Embed Size (px)
Citation preview
Aznan Lelo & Zulkarnain Rangkuty
Dep. Farmakologi & Terapeutik,
Fakultas Kedokteran
Universitas Sumatera Utara
22 Oktober 2009, KBK, TROPMED
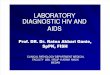
The tree of antibiotics
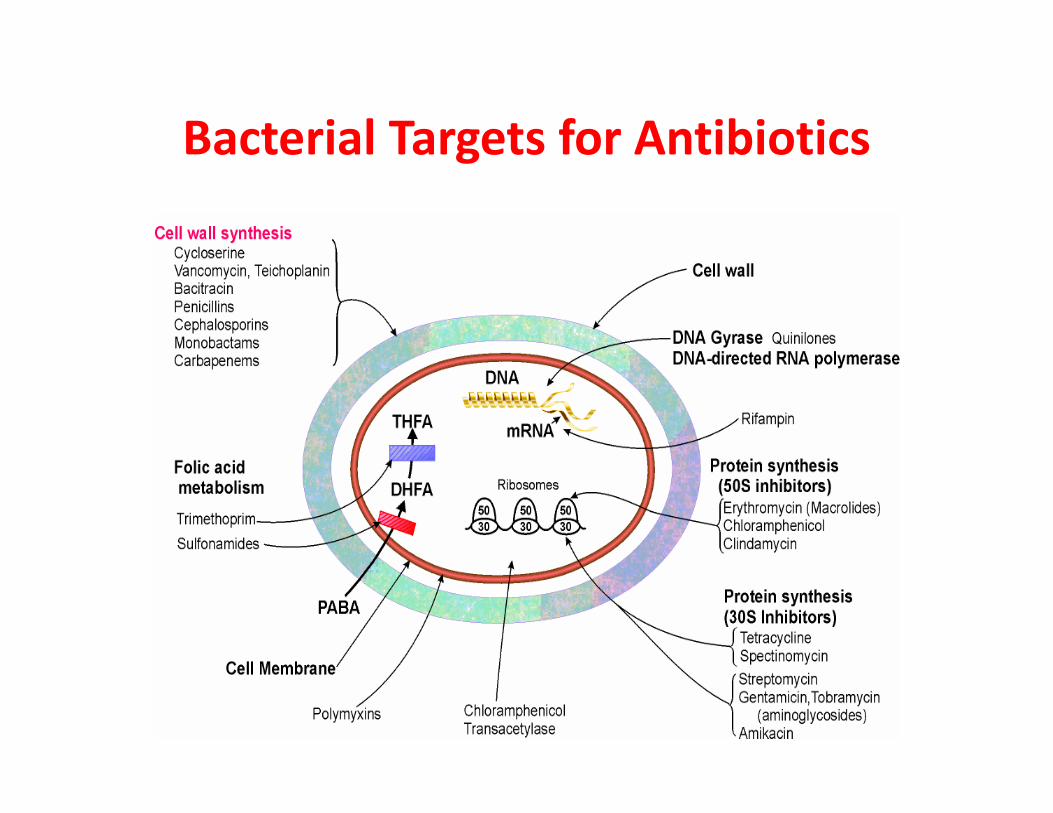
Bacterial Targets for Antibiotics
Inhibitors of Cell wall synthesis
bactericidal, time dependent killing
1. Beta-lactams (penicillins,
cephalosporins, carbapenems,
monobactams)monobactams)
2. Cycloserine
3. Glycopeptides (vancomycin,
teicoplanin)
4. Bacitracin
Cell Wall Active Agents
• B-lactams bind to “penicillin binding proteins” (PBP)
-PBP are essential enzymes involved in cell wall
synthesis
-weakened / distorted cell wall leading to cell lysis
and deathand death
• Glycopeptides bind to the terminal D-ala of nascent
cell wall peptides and prevents cross-linking of these
peptide to form mature peptidoglycan
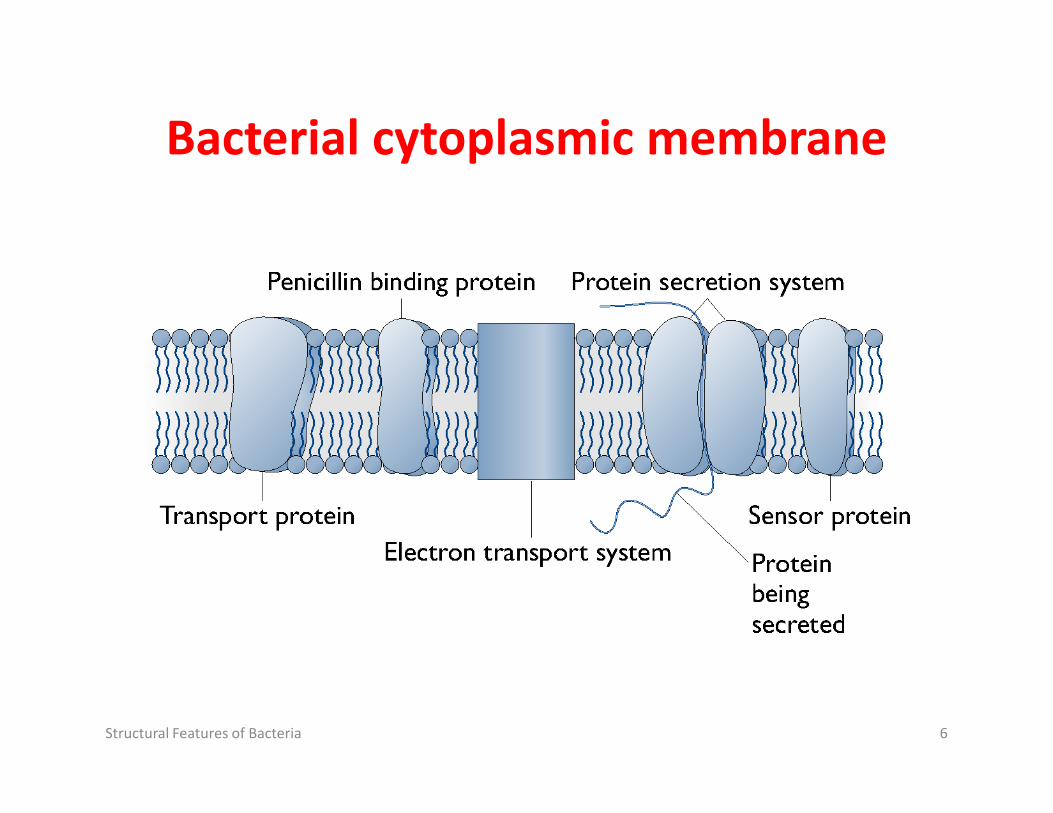
Bacterial cytoplasmic membrane
Structural Features of Bacteria 6
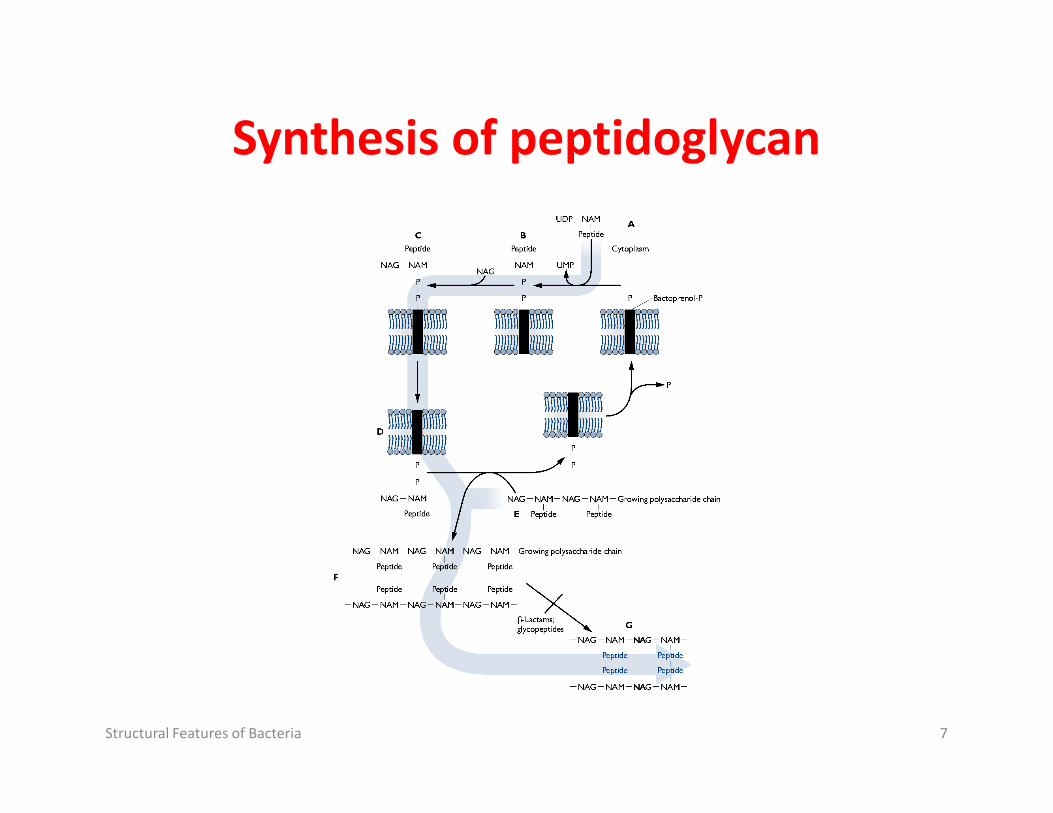
Synthesis of peptidoglycan
Structural Features of Bacteria 7
Antibiotics that inhibit PG synthesis
• Fosfomycin (Monurol) – inhibits formation of PG subunit
• Bacitracin – binds lipid carrier, inhibits externalization of PG subunit (toxic, usually used topically)
Structural Features of Bacteria 8
of PG subunit (toxic, usually used topically)
• Penicillins and cephalosporins (β-lactam antibiotics) -inhibits PG crosslinking
• Vancomycin (glycopeptide antibiotics; Vancocin) –inhibits PG crosslinking
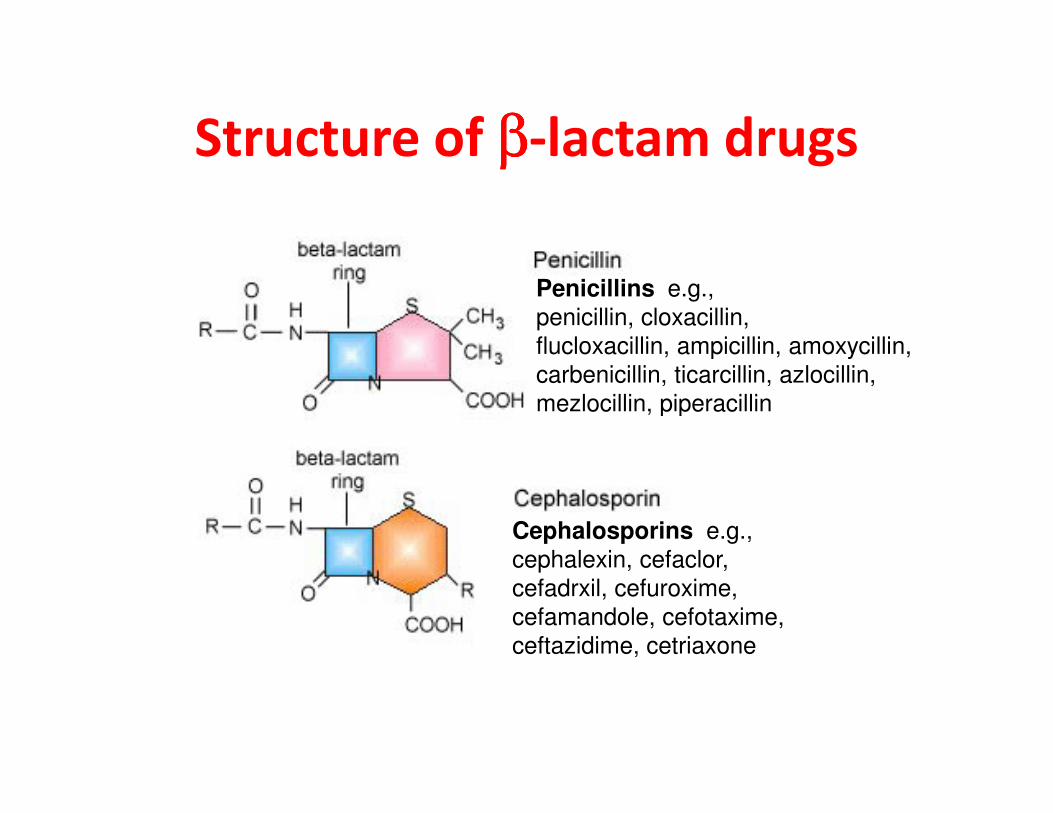
Structure of ββββ-lactam drugs
Penicillins e.g.,
penicillin, cloxacillin,
flucloxacillin, ampicillin, amoxycillin,
carbenicillin, ticarcillin, azlocillin,
mezlocillin, piperacillinmezlocillin, piperacillin
Cephalosporins e.g.,
cephalexin, cefaclor,
cefadrxil, cefuroxime,
cefamandole, cefotaxime,
ceftazidime, cetriaxone
Penicillins
• Penicillin G / V
- good gram positive (not Staph)
-moderate anaerobic activity
• Synthetic penicillins (Ampicillin)
- good gram positive (not Staph)- good gram positive (not Staph)
- moderate gram negative (not Pseudomonas)
• Anti-staphylococcal penicillins
- Cloxacillin
• Anti-pseudomonal penicillins
- Piperacillin
PENICILLIN
• First antibiotic
• Active for coccus gram negative and positive
• Side effects � allergy, anaphylactic shock,
toxic reaction, and local irritation.toxic reaction, and local irritation.
• Excreted by urine
• High resistancy rate

Activity of ß-lactams against common organisms
PenicillinsBenzylpenicillinFlucloxacillinAmoxycillinPiperacillin
Staphylococci++++
E.coli
RR++
Streptococci++++
EnterococciRR++
PseudomonasRRR+
Gram (+)ve Gram (-)ve
Piperacillin
CephalosporinsCephalexinCefuroximeCeftriaxoneCeftazidime
+ ++ + +
++RR
++++
RRRR
RRR+
Urine only+++
CarbapenemsImipenem + + + + +
CEPHALOSPORINS
• Produced by Cephalosporium acremonium
• Inhibit the 3rd step transpeptidase reaction in microbial membrane synthesis.
Type of Cephalosporin :
� 1st Generation (Cefadroxil, Cefazolin, Cephalexin, etc)
� 2nd Generation (Cefaclor, Cefoxitin, Loracarbef, etc)� 2nd Generation (Cefaclor, Cefoxitin, Loracarbef, etc)
� 3rd Generation (Cefixime, Cefoperazone, Cefotaxime, Ceftazidime, Ceftriaxone, etc)
� 4th Generation (Cefepime)Administration : Oral, Intravenous, Intramuscular.
• Cross the placental and blood brain barrier.
• Excretion : kidney and bile.
• Side Effects : Allergic reaction, anaphylactic reaction with bronchospasme and urticaria, diarrhea, bleeding, etc.
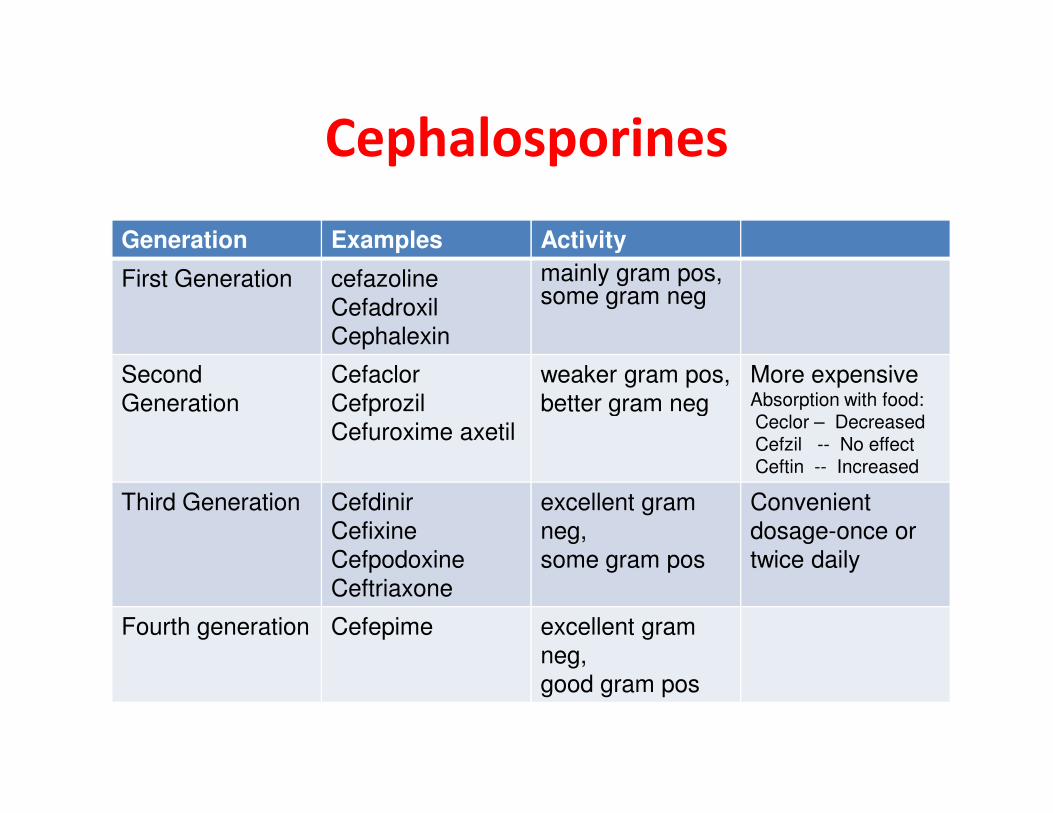
Cephalosporines
Generation Examples Activity
First Generation cefazoline
Cefadroxil
Cephalexin
mainly gram pos, some gram neg
Second
Generation
Cefaclor
Cefprozil
weaker gram pos,
better gram neg
More expensiveAbsorption with food:Generation Cefprozil
Cefuroxime axetil
better gram neg Absorption with food:Ceclor – DecreasedCefzil -- No effectCeftin -- Increased
Third Generation Cefdinir
Cefixine
Cefpodoxine
Ceftriaxone
excellent gram
neg,
some gram pos
Convenient
dosage-once or
twice daily
Fourth generation Cefepime excellent gram
neg,
good gram pos
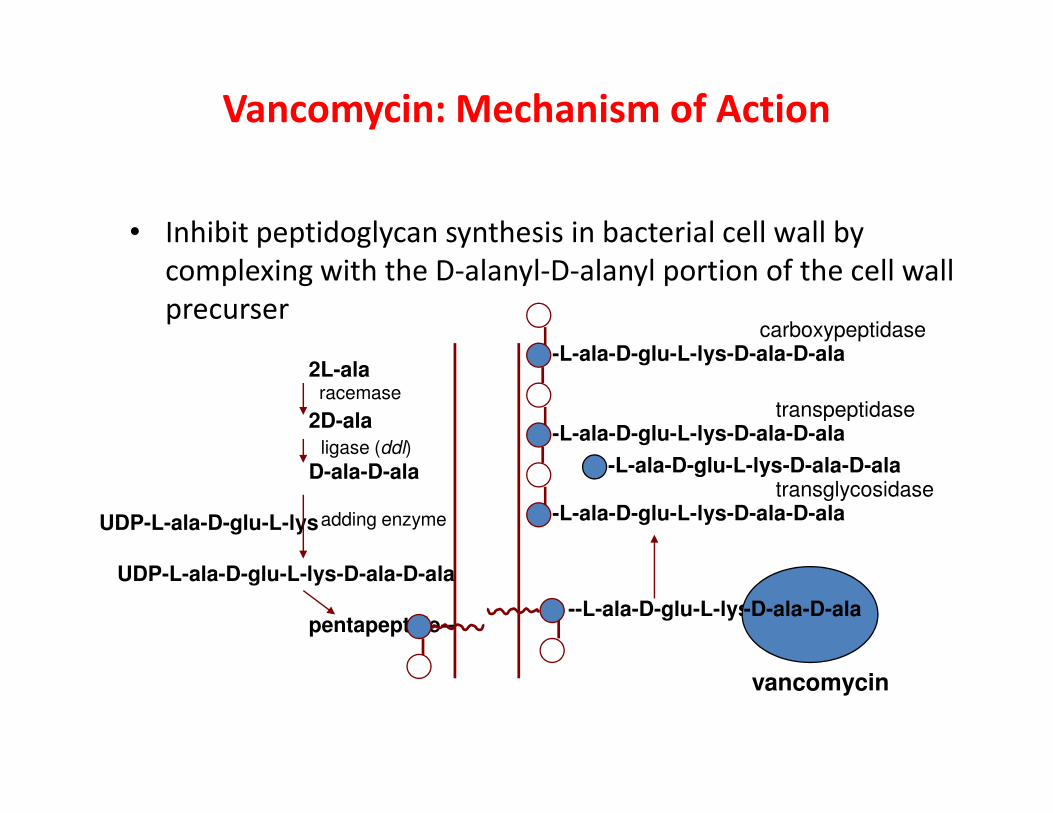
Vancomycin: Mechanism of Action
• Inhibit peptidoglycan synthesis in bacterial cell wall by
complexing with the D-alanyl-D-alanyl portion of the cell wall
precurser
2L-alaracemase
transpeptidase
-L-ala-D-glu-L-lys-D-ala-D-alacarboxypeptidase
2D-ala
D-ala-D-ala
UDP-L-ala-D-glu-L-lys
UDP-L-ala-D-glu-L-lys-D-ala-D-ala
pentapeptide--
ligase (ddl)
adding enzyme
--L-ala-D-glu-L-lys--D-ala-D-ala
vancomycin
-L-ala-D-glu-L-lys-D-ala-D-alatransglycosidase
-L-ala-D-glu-L-lys-D-ala-D-ala
-L-ala-D-glu-L-lys-D-ala-D-ala
transpeptidase
Cell Wall Active Agents
• B-lactam resistance
1. Production of a B-lactamase (most common)
2. Altered PBP (S.pneumoniae)
3. Novel PBP (MRSA)
4. Altered permeability
• Glycopeptide resistance
- primary concern is Enterococcus / S.aureus
- altered target
- bacteria substitutes D-lac for D-ala
- vancomycin can no longer bind
Beta-lactamase inhibitors
• Clavulanic acid:
- used with amoxycillin (Augmentin®)
- used with ticarcillin (Timentin®)
• Sulbactam:• Sulbactam:
- used with ampicillin (unavailable in UK)
• Tazobactam
- used with piperacillin (Tazocin®)
Inhibitors of protein synthesis
• Ribosomes are the site of protein synthesis
• many classes of antibiotics inhibit protein
synthesis by binding to the ribosome
• binding may be reversible or irreversible• binding may be reversible or irreversible
1. Aminoglycosides
2. Macrolides
3. Tetracyclines
4. Chloramphenicol
5. Fusidic acid

Macrolides
Aminoglycosides - general properties
• Major weapon in treatment of severe sepsis
– Gram negative, rapid bactericidal effect
• Fat insoluble and not absorbed orally• Fat insoluble and not absorbed orally
– Effective by the parenteral route
• Entry into cells depends upon oxygen-dependent
transport (lacked by streptococci & enterococci)
• Toxic to the kidney and inner ear - imperative to
measure levels
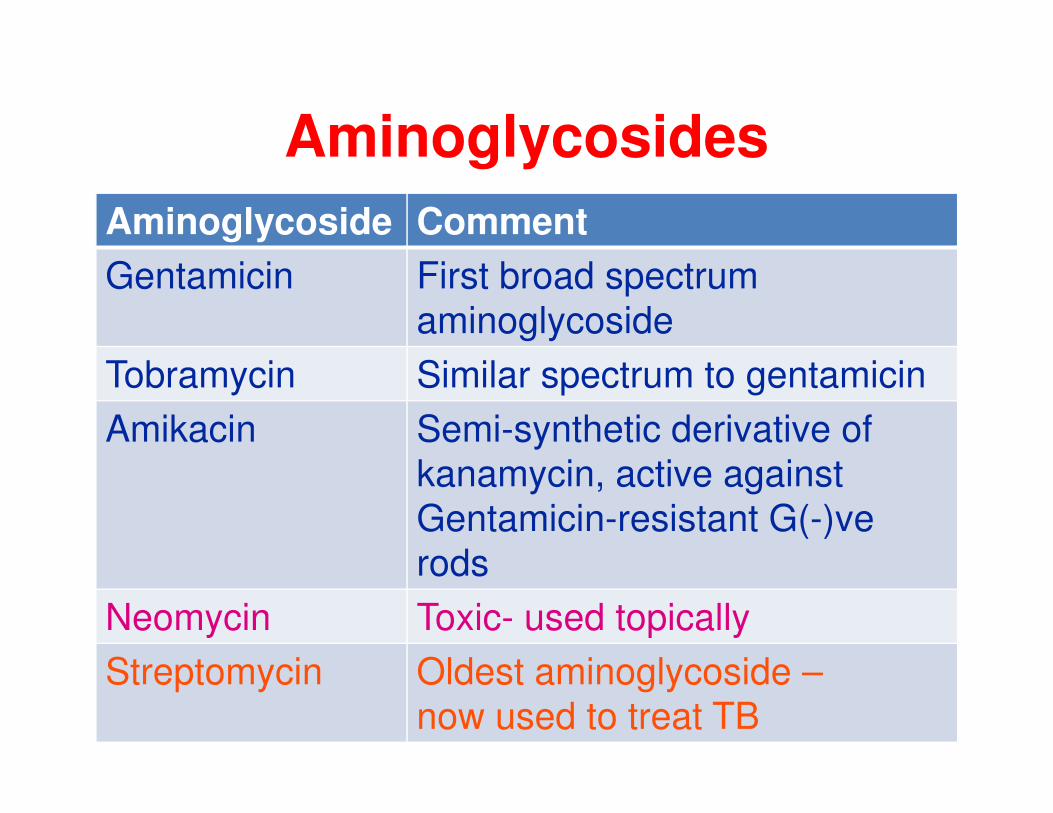
Aminoglycosides
Aminoglycoside Comment
Gentamicin First broad spectrum
aminoglycoside
Tobramycin Similar spectrum to gentamicin
Amikacin Semi-synthetic derivative of
kanamycin, active against
Gentamicin-resistant G(-)ve
rods
Neomycin Toxic- used topically
Streptomycin Oldest aminoglycoside –
now used to treat TB
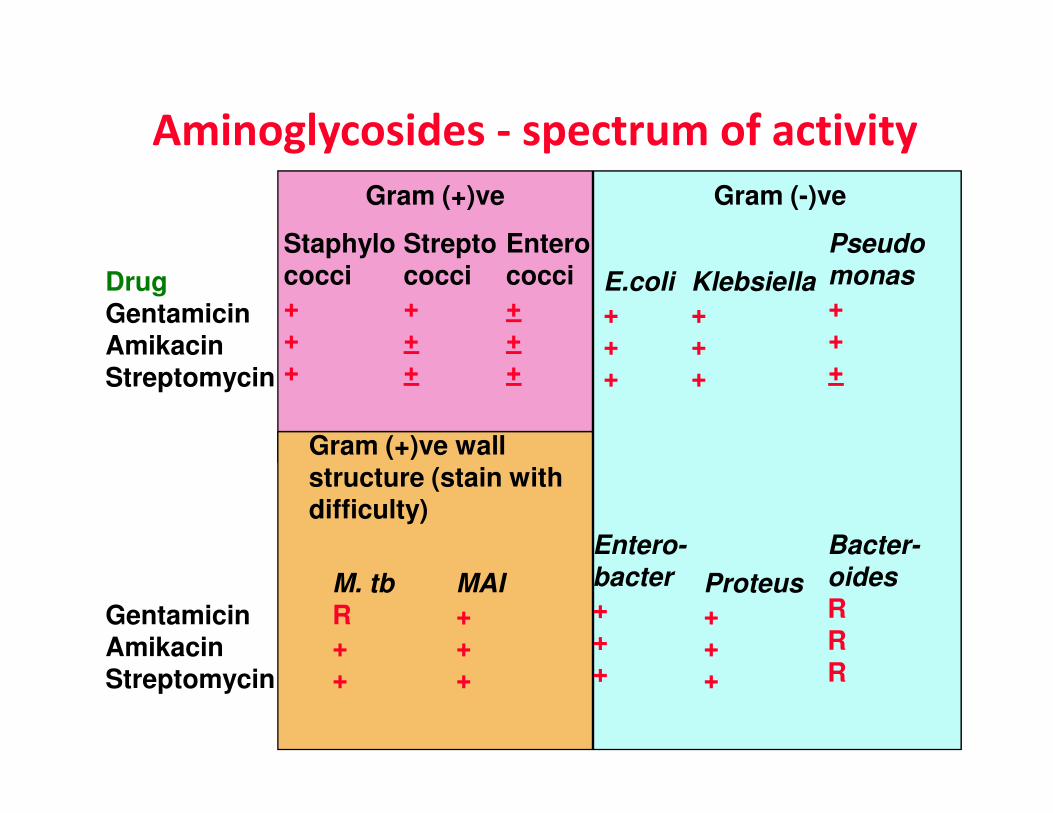
Aminoglycosides - spectrum of activity
DrugGentamicinAmikacinStreptomycin
Staphylococci+++
Klebsiella
+++
Streptococci+++
Enterococci+++
Pseudo
monas
+++
Gram (+)ve Gram (-)ve
E.coli
+++
Proteus
+++
Bacter-
oides
RRR
Entero-
bacter
+++
GentamicinAmikacinStreptomycin
Gram (+)ve wall structure (stain with difficulty)
M. tb
R++
MAI
+++

Macrolides
• Erythromycin
• Azithromycin
• Clarithromycin
Large structures:
CH3
OH
CH3
OHO
H3C
O
OH N(CH3)Large structures:
14- (Erythromycin &
Clarithromycin),
15- (Azithromycin),
or 16-membered
rings.
CH3
O
CH3
O
OH5C2
H3CHO O
OH N(CH3)
CH3
O
OCH3
OCH3
OH

Macrolides - general properties
• Newer macrolides inhibit Mycobacteria,
protozoa (T. gondii, E. histolytica, P.
falciparum), Campylobacter, Helicobacter, falciparum), Campylobacter, Helicobacter,
Borrelia, Neisseria & other genital pathogens
• GI complications, mostly with erythromycin
• Given orally, but absorbtion & bioavailability
variable from one macrolide to another
Macrolides
• Erythromycin is inactivated by gastric acid.
• Erythromycin esters are less susceptible to acid
inactivation and are better absorbed
• It inhibits cytochrome P 450
• Erythromycin and Azithromycin are excreted in • Erythromycin and Azithromycin are excreted in
bile.
• Clarithromycin appear in urine and bile.
• Azithromycin has large Vd – high tissue
distribution – concentrated in neutrophils,
macrophages.
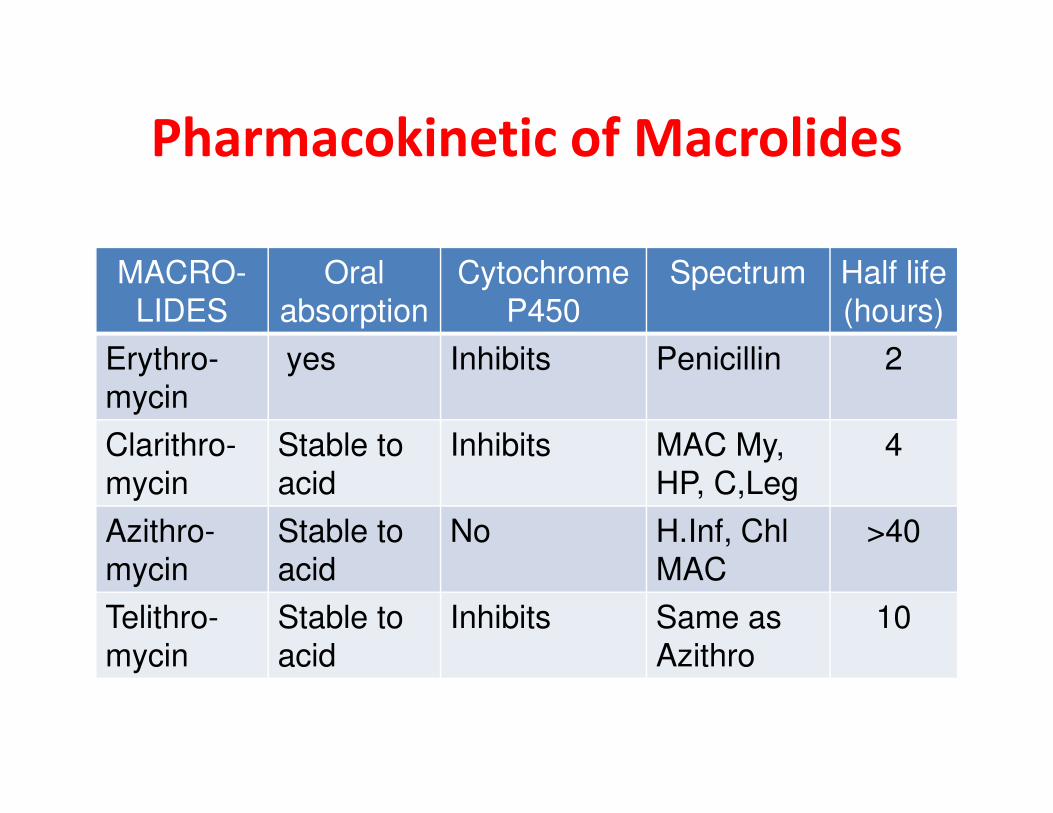
Pharmacokinetic of Macrolides
MACRO-
LIDES
Oral
absorption
Cytochrome
P450
Spectrum Half life
(hours)
Erythro-
mycin
yes Inhibits Penicillin 2
mycin
Clarithro-
mycin
Stable to
acid
Inhibits MAC My,
HP, C,Leg
4
Azithro-
mycin
Stable to
acid
No H.Inf, Chl
MAC
>40
Telithro-
mycin
Stable to
acid
Inhibits Same as
Azithro
10
Macrolides
Adverse effects :
• Epigastric distress - erythromycin
• Cholestatic jaundice (mainly with erythromycin
estolate)
• Ototoxicity – erythromycin at high dose.• Ototoxicity – erythromycin at high dose.
Drug - drug interactions
• Erythromycin, Clarithromycin and Telithromycin
inhibit the cytochrome P450 system and so
potentiate the activity of theophylline and
terfenadine
ClindamycinPharmacodynamic
• Active against gram +ve and anaerobes
• Good activity against bacteroides (including B. fragilis) and Penicillin resistant streptococcus.
• No activity against most gram -ve bacteria
Pharmacokinetic Pharmacokinetic
• Well absorbed orally
• Distribution in most tissues including bone.
• Excretion is mainly biliary and also in urine.
Adverse effects
• Gastrointestinal super-infections – potentially fatal pseudo-membranous colitis by C. difficile.
• Oral Metronidazole and Vancomycin are used for the treatment of the fatal pseudo-membranous colitis.
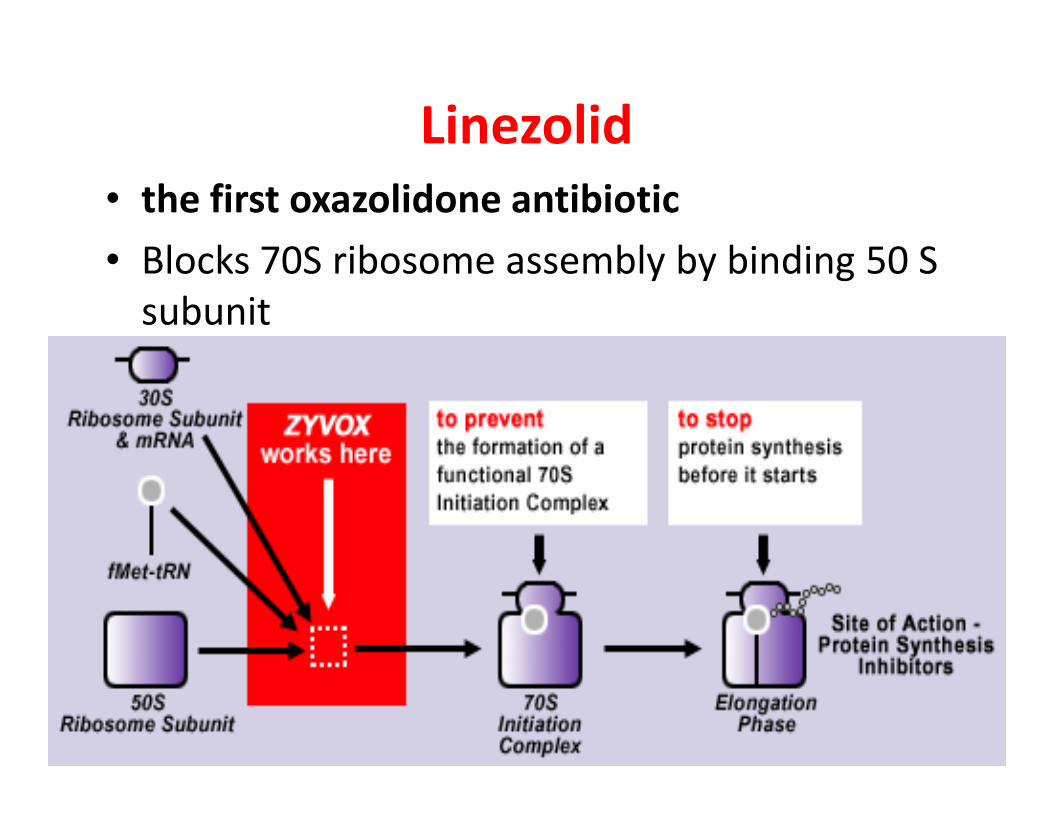
Linezolid
• the first oxazolidone antibiotic
• Blocks 70S ribosome assembly by binding 50 S
subunit
Linezolid
Anti-bacterial spectrum :
• Gram positive bacteria only
– Penicillin resistant streptococci
– Methicillin and Vancomycin
Pharmacokinetics :
• Orally absorbed
• Well distributed
• Excreted by renal and non-renal routes
staphylococcus
– Vancomycin resistant enterococcus
– Lister monocytogenes, Corynebacterium spp
• Also active against mycobacteria tuberculosis and Clostridium
Adverse effects :
• Nausea and diarrhea
• Thrombocytopenia
• Inhibits MAO, avoid tyramine containing foods
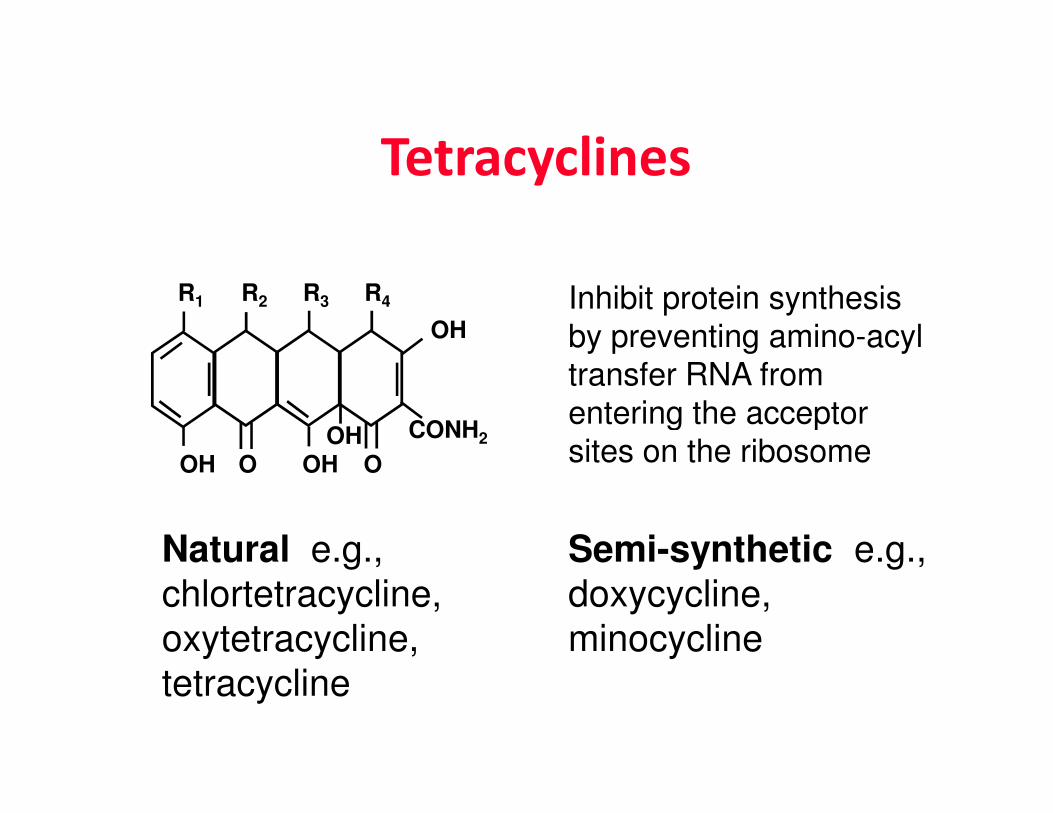
Tetracyclines
OH
R1 R2 R3 R4 Inhibit protein synthesis
by preventing amino-acyl
transfer RNA from
entering the acceptor
Natural e.g.,
chlortetracycline,
oxytetracycline,
tetracycline
Semi-synthetic e.g.,
doxycycline,
minocycline
OH O OH O
CONH2OHentering the acceptor
sites on the ribosome
Tetracyclines – general properties
• Active against many common Gram (+)ve & (-)ve
bacteria, chlamydiae, rickettsiae, coxiellae,
spirochaetes, some mycobacteria, E histolytica, &
plasmodia
• Adiministration : oral, intravenous, intramuscular• Adiministration : oral, intravenous, intramuscular
– Given orally, absorption affected by food
• Effect on dentition (chelates Ca)
• Contraindication : pregnancy, lactating, growing child, liver and renal insufficiency
• Side effects : Allergic, anaphilactic, toxic reaction, diarrhea (GI intolerance common)
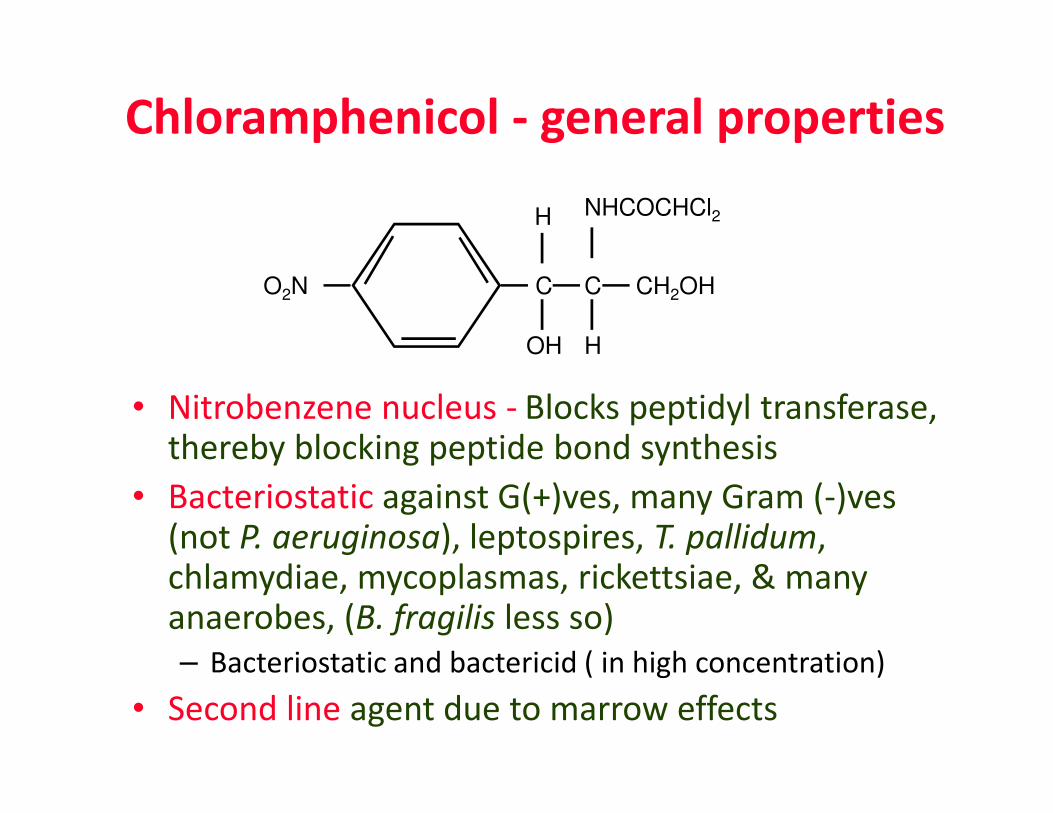
Chloramphenicol - general properties
• Nitrobenzene nucleus - Blocks peptidyl transferase,
C
OH
H
CH2OHCO2N
H
NHCOCHCl2
• Nitrobenzene nucleus - Blocks peptidyl transferase, thereby blocking peptide bond synthesis
• Bacteriostatic against G(+)ves, many Gram (-)ves (not P. aeruginosa), leptospires, T. pallidum, chlamydiae, mycoplasmas, rickettsiae, & many anaerobes, (B. fragilis less so)
– Bacteriostatic and bactericid ( in high concentration)
• Second line agent due to marrow effects

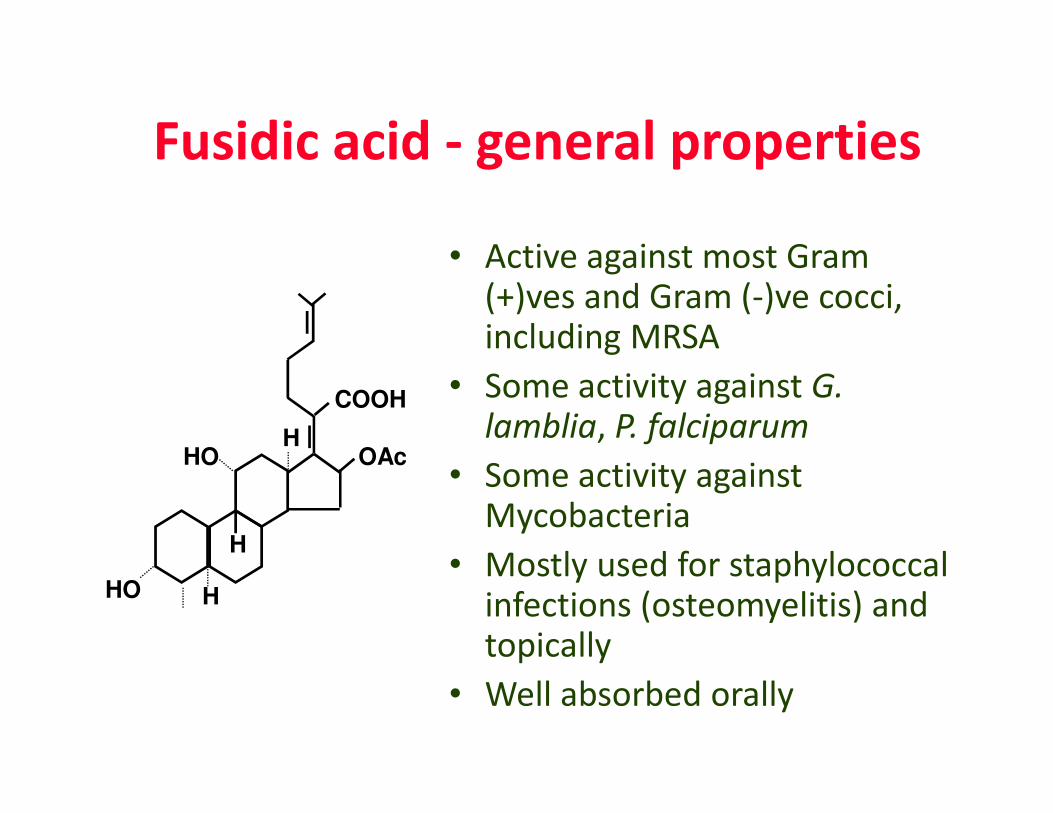
Fusidic acid - general properties
• Active against most Gram (+)ves and Gram (-)ve cocci, including MRSA
• Some activity against G.
lamblia, P. falciparumCOOH
lamblia, P. falciparum
• Some activity against Mycobacteria
• Mostly used for staphylococcal infections (osteomyelitis) and topically
• Well absorbed orally
COOH
HHO
H
HHO
OAc
Inhibitors of Nucleic acid synthesis
• Inhibition of synthesis of precursors
Sulphonamides
TrimethoprimTrimethoprim
• Inhibitors of DNA replication
Quinolones
• Inhibitors of RNA polymerase
Rifampicin

Inhibition of synthesis of precursorsDrugs acting on microbial folate synthesis
• Trimethoprim - inhibits folate
required for the synthesis of purines required for the synthesis of purines
and pyrimidines by enzyme inhibition
• Sulphonamides - also inhibit folate
synthesis by enzyme inhibition
Trimethoprim- Sulfamethoxazole
(TMP-SMX)
• Prepared as a fixed 5:1 ratio of SMX to TMP
• MOA - inhibits two steps in the folic acid pathway – optimal antibacterial effects occur at a ratio of 1:20
(TMP:SMX) which is also the peak concentration following
oral and IV administrationoral and IV administration
• Pharmacokinetics:– Oral bioavailability > 90%
– Widely distributed into body tissues and fluids
– Metabolized in liver (Acetylated and glucuronide
conjugated ) - then renally excreted
– SMX: 70% in protein bound• It displaces bilirubin, so it can cause newborn jaundice or make it worse if
used in third trimester.

Mechanism of action ofTMP-SMX
Sulphonamides - general properties
• First chemotherapeutic
• Broad spectrum activity– Restricted in use by resistance
– Side effects � allergy, anaphylactic shock, toxic
reaction, and local irritation.reaction, and local irritation.
• Many interactions with other drugs due to
plasma protein binding
• Principal use has been for treatment of UTIs– Excreted by urine
• Useful in treatment of PCP, Nocardia, &
Toxoplasma gondii
Untoward effects of sulfonamides
• Hematopoietic system:
– Hemolytic anemia (in glucose-6-phosphate dehydrogenase deficient patients);
– aplastic anemia; thrombocytopenia; eosinophylia.
• Urinary tract:
– Occlusions due to precipitates and hypersensitivity reactions.
• Drug interaction:
– Due to the high affinity to plasma proteins.
– These include anticoagulants, hydantoin and hypoglycemic agents of
sulfonylurea group.
• Therefore, the patient must be given sufficient amount of
water to produce 1.2 liter/day of urine (i.e. 3-4 liter of
water/day).
Inhibitors of DNA replication
• Quinolones (eg ciprofloxacin - a fluoroquinolone) large family of synthetic agents that affect DNA gyrase synthetic agents that affect DNA gyrase
• DNA gyrase required to supercoil bacterial DNA (it is also important in DNA repair) – bacteria unable to ‘pack’ DNA into cell

Quinolones
• These are synthetic anti-microbials.
• The member of this group –
– Old quinolon (unfluorinated quinolone; first
generation)generation)
– Fluoroquinolones
• Bactericidal and concentration dependent.
• Long post-antibiotic effect on enterobacteriacea
FLUOROQUINOLONES
• Fluoroquinolones (ciprofloxacin, norfloxacin, levofloxacin, moxifloxacin)
- bactericidal, concentration dependent
- bind to 2 essential enzymes required for DNA
replication
- DNA gyrase and topoisomerase IV- DNA gyrase and topoisomerase IV
- gram pos and gram neg
- atypical bacteria, some have anaerobic activity
• Farmakokinetic : well absorbed by oral administration
�widely distributed�Excreted by urine
• Clinical use : UTI, RTI, STD, arthritis, bone infection
• Side effects : Nausea, vomite, headache.
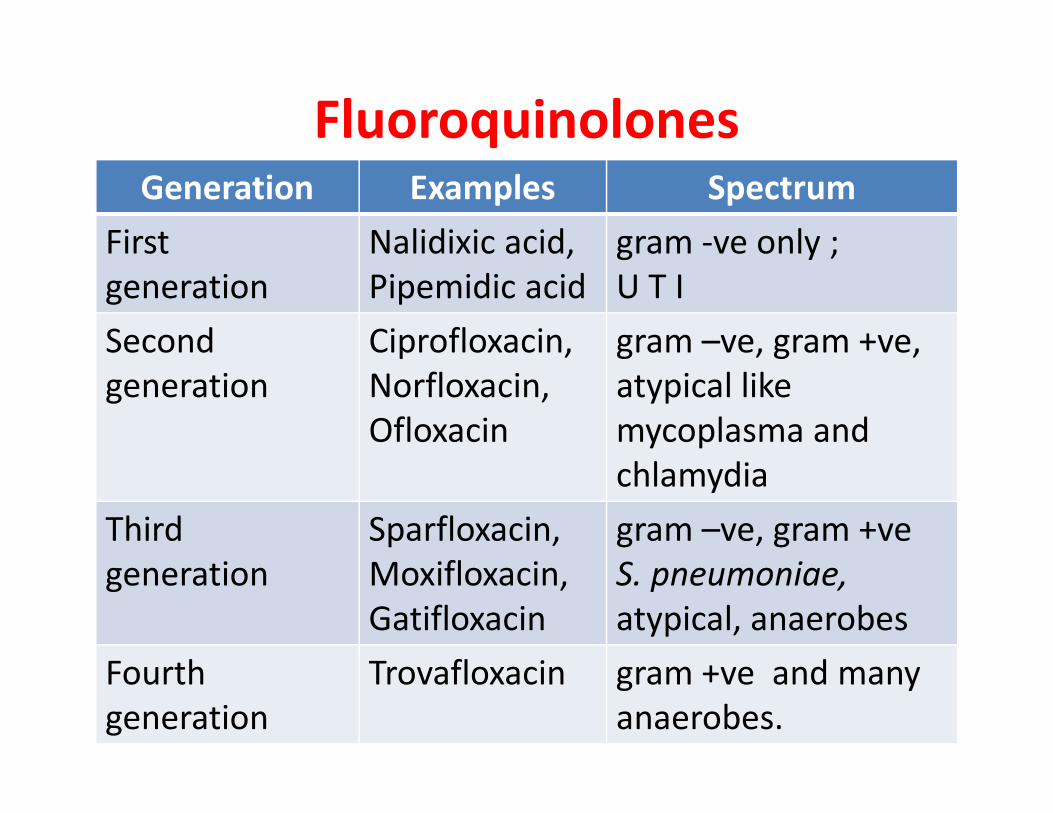
FluoroquinolonesGeneration Examples Spectrum
First
generation
Nalidixic acid,
Pipemidic acid
gram -ve only ;
U T I
Second
generation
Ciprofloxacin,
Norfloxacin,
Ofloxacin
gram –ve, gram +ve,
atypical like
mycoplasma and Ofloxacin mycoplasma and
chlamydia
Third
generation
Sparfloxacin,
Moxifloxacin,
Gatifloxacin
gram –ve, gram +ve
S. pneumoniae,
atypical, anaerobes
Fourth
generation
Trovafloxacin gram +ve and many
anaerobes.
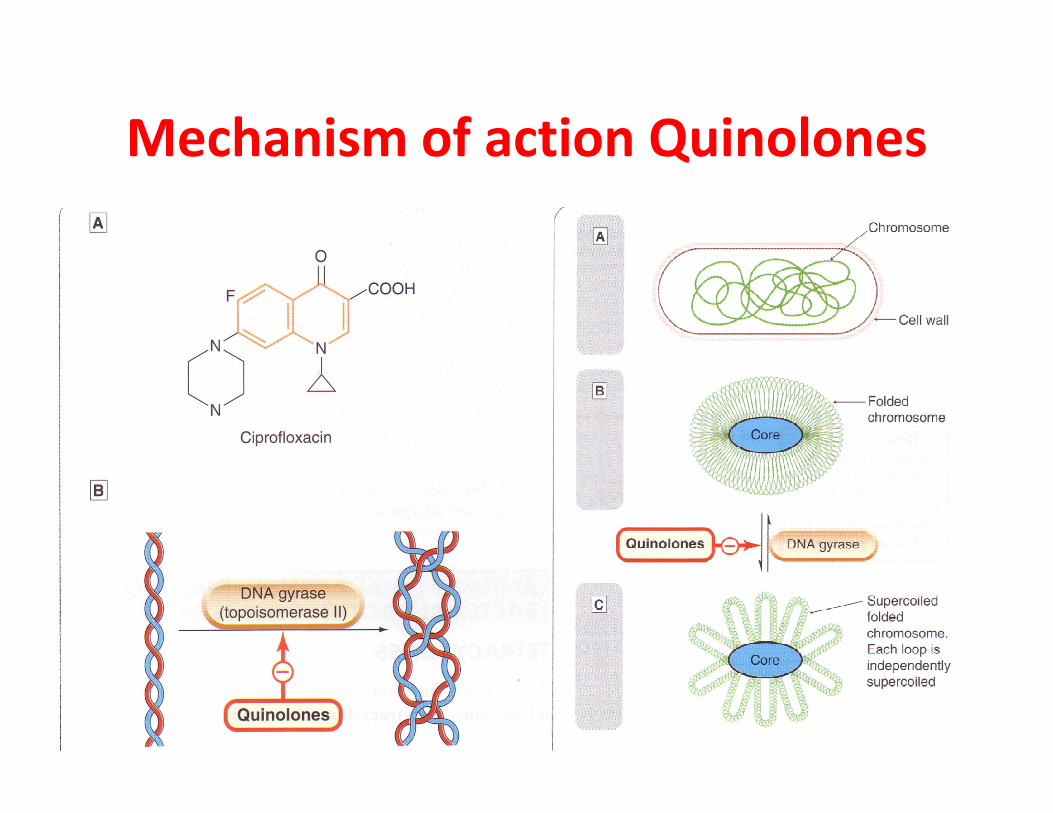
Mechanism of action Quinolones
Fluoroquinolones
Pharmacokinetics :
• Orally well absorbed, metabolism in liver
• FQ chelate Ca, Mg, Fe and Zn
• High tissue penetration – bone, lungs and • High tissue penetration – bone, lungs and phagocytes exceeds that in plasma
• Excreted primarily in urine –(Trovafloxacin and Sparfloxacin are predominantly eliminated by non – renal route)
Fluoroquinolones
Adverse effects :
• CNS : dizziness, confusion, seizures threshold
is decreased.
• Cartilage damage • Cartilage damage – Quinolones are not recommended for
prepuberal children and pregnant woman due to possible arthropathy in children
• Liver failure – Trovafloxacin
• QT prolonged – Sparfloxacin and Moxifloxacin
• Phototoxicity – Sparfloxacin
Fluoroquinolones
Drug interaction
• Plasma concentrations of theophylline,
Warfarin, Caffeine are increased by FQ due to
inhibition of metabolism of these drugsinhibition of metabolism of these drugs
• FQ enhance the CNS toxicity of Caffeine and
seizures are reported.
Inhibitors of RNA polymerase
that affect bacterial DNA and RNA
• Rifamycins (eg rifampacin) specific
inhibitors of bacterial DNA-dependent
RNA polymerase – blocks mRNARNA polymerase – blocks mRNA
• Metronidazole (a nitroimidazole)
When reduced it can react with DNA,
oxidizing it and causing strand breaks
METRONIDAZOLE
• Active for the anaerob
• Well oral absorption
• Effect on CNS
• Drug of choice for � paracytic infection (G. • Drug of choice for � paracytic infection (G.
lamblia), amoeba, and bacterial vaginosis.
Characteristics of a good antibiotic
• Kills or inhibits the growth of bacteria at low concentrations
• Broad spectrum
• Minimal side effects
– Due to direct effects of antibiotic itself
Structural Features of Bacteria 52
– Due to direct effects of antibiotic itself
– Due to effects on the normal microflora of the body
• Appropriate pharmacokinetic properties
– Must get to the site of infection in high concentrations
– Distribution influences mode of administration (oral, injected)

![Baru Kuliah Malaria Blok Tropmed-2.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000141-tropical-medicine/tmd175... · Affinity of Parasite to Erythrocytes P.vivax P.malariaeP.malariae](https://img.pdfslide.us/doc/110x75/5b4cc87d7f8b9a481a8bab0f/baru-kuliah-malaria-blok-tropmed-2ppt-read-onlyocwusuacidcoursedownload1110000141-tropical-medicinetmd175.jpg)






![MEASLES ((campakcampak,, rubeolarubeola,, gabakgabak ...ocw.usu.ac.id/course/download/1110000141-tropical-medicine/tmd175... · Microsoft PowerPoint - CAMPAK.ppt [Read-Only] [Compatibility](https://img.pdfslide.us/doc/110x75/5bc96d4009d3f2ca288cff62/measles-campakcampak-rubeolarubeola-gabakgabak-ocwusuacidcoursedownload1110000141-tropical-medicinetmd175.jpg)
![tetanus kbk-2.ppt [Read-Only] - ocw.usu.ac.idocw.usu.ac.id/course/download/1110000141-tropical-medicine/tmd175... · light, reduced noise, and stable temperature) may be recommended](https://img.pdfslide.us/doc/110x75/5b5d42797f8b9aa1428dc5f3/tetanus-kbk-2ppt-read-only-ocwusuacidocwusuacidcoursedownload1110000141-tropical-medicinetmd175.jpg)
![swine flu kbk-1.ppt [Read-Only]ocw.usu.ac.id/.../1110000141-tropical-medicine/tmd175_slide_swine_… · MAP of H1 N1 Swine Flu. Swine Influenza (Flu) Swine Influenza (swine flu) is](https://img.pdfslide.us/doc/110x75/5f5a2f7aee204b1010391ac9/swine-flu-kbk-1ppt-read-onlyocwusuacid1110000141-tropical-medicinetmd175slideswine.jpg)