Embed Size (px)
Citation preview
Axillary Vein Puncture without contrast venography for pacemaker and
defibrillator leads implantation.Dante Antonelli MD, Alexander Feldman MD,
Nahum A. Freedberg MD, Yoav TurgemanMD.
Dept of Cardiology, Ha Emek Medical Center, 18100 Afula
DISCLOSURE OF INTERESTS
There id no conflict of interests related to the study.
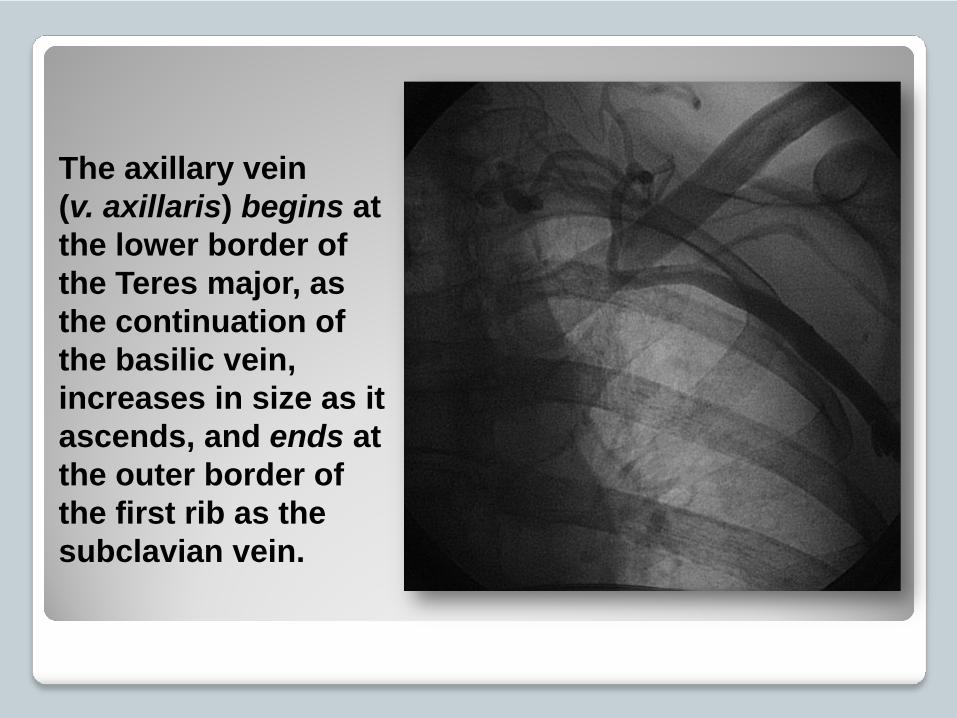
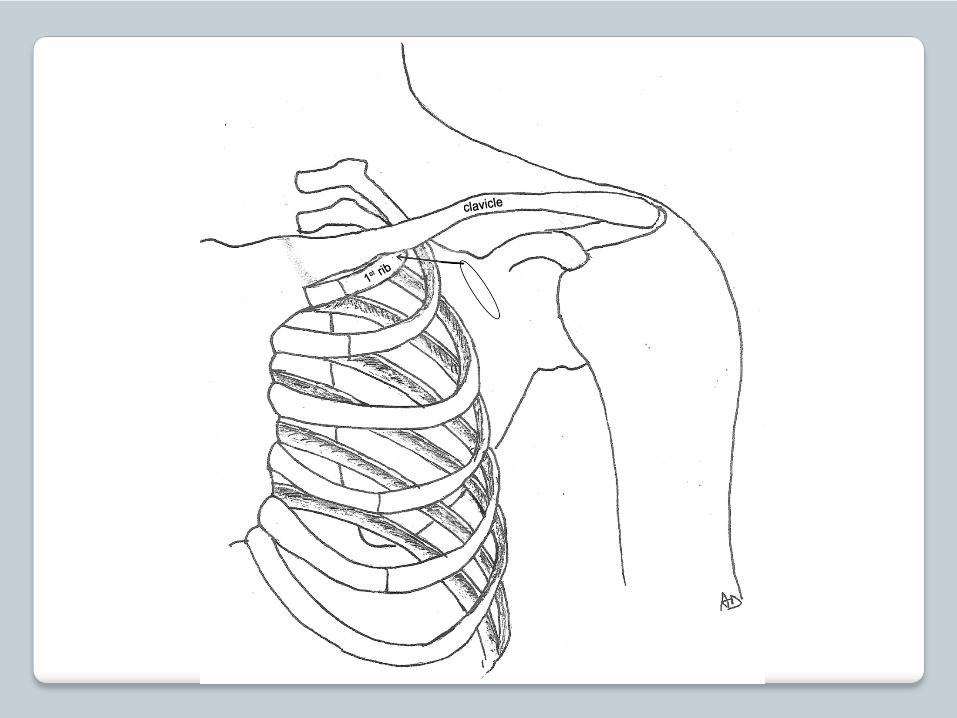
The axillary vein(v. axillaris) begins at the lower border of the Teres major, as the continuation of the basilic vein, increases in size as it ascends, and ends at the outer border of the first rib as the subclavian vein.

Percutaneous blind intrathoracic puncture
of the subclavian vein has gained a wide
acceptance because of its speed and
simplicity; however pneumothorax, and
"Subclavian Vein Syndrome" may
complicate this approach.
Consequently it has been recommended to puncture the axillary vein. The use of anatomical landmarks, contrast venography, echo and Doppler guidance techniques were developed to facilitate these vein approaches.
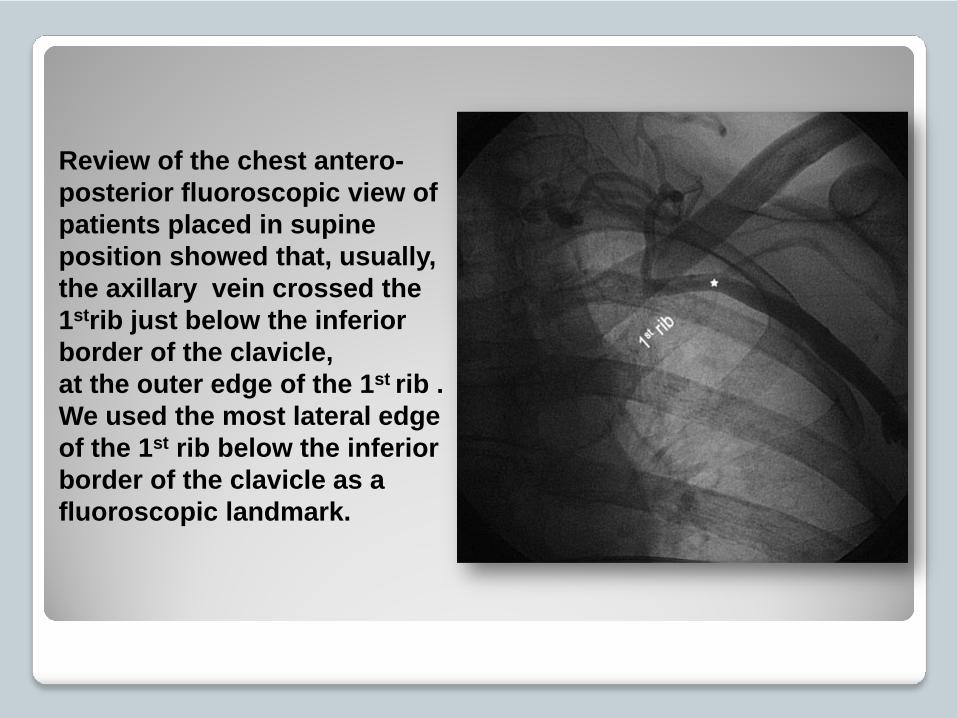
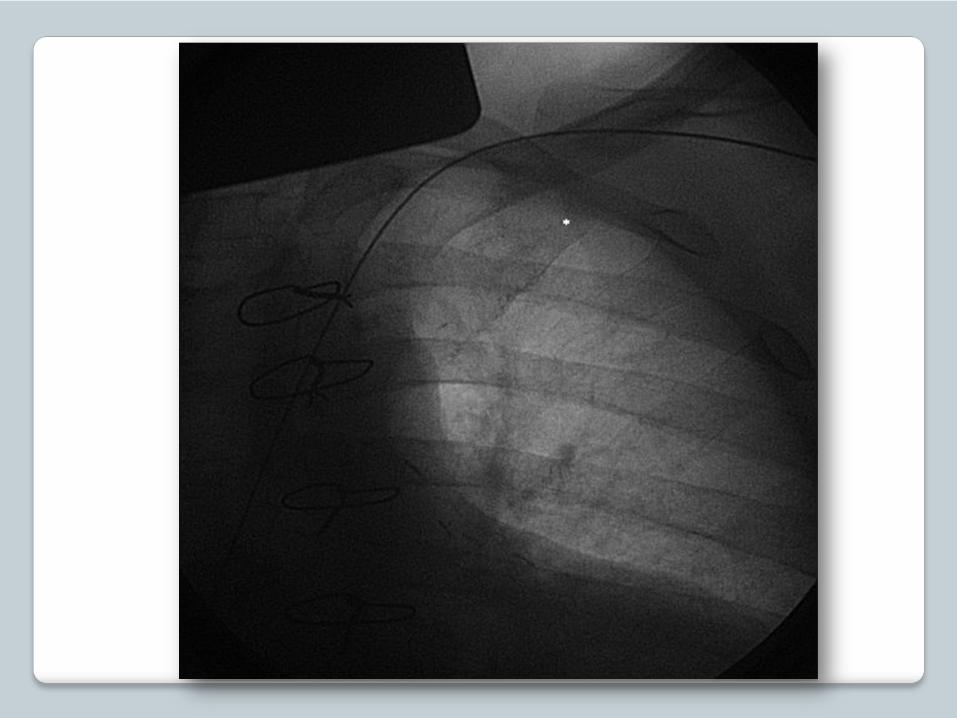
Review of the chest antero-posterior fluoroscopic view of patients placed in supine position showed that, usually, the axillary vein crossed the 1strib just below the inferior border of the clavicle, at the outer edge of the 1st rib .We used the most lateral edge of the 1st rib below the inferior border of the clavicle as a fluoroscopic landmark.

Results:
Our study population included 182 consecutive patients referred for permanent pacemaker or implantable cardioverter defibrillator implantation; there were 64 women and 118 men with a mean age of 69.8±12.4 years (range 39-101).

Implanted Devices Type
PM Single Chamber 23 (12.8 %)PM Dual Chamber 100 (55.5%)ICD Single Chamber 2 (1.1 %)ICD Dual Chamber 32 (17.8 %)ICD Biventricular 23 (12.8)
Total implanted leads = 362
Left sided implantation was preferred in most of
the cases.
Right sided procedure was preferred in 8 patients
(4.4 %) because the patients were left- handed,
after left mastectomy and had left sided skin
ulceration.

The axillary vein was successfully cannulated in all patients. In 172 patients (94.5%), the vein was cannulated without the use of venography. Venography was required in 10 patients (5.5%): 6 women (9.4%) and 4 men (3.4%).
The venography showed that axillary
vein did not cross the 1st rib in its
most lateral edge below the inferior
border of the clavicle in 8 of these
patients (80%).
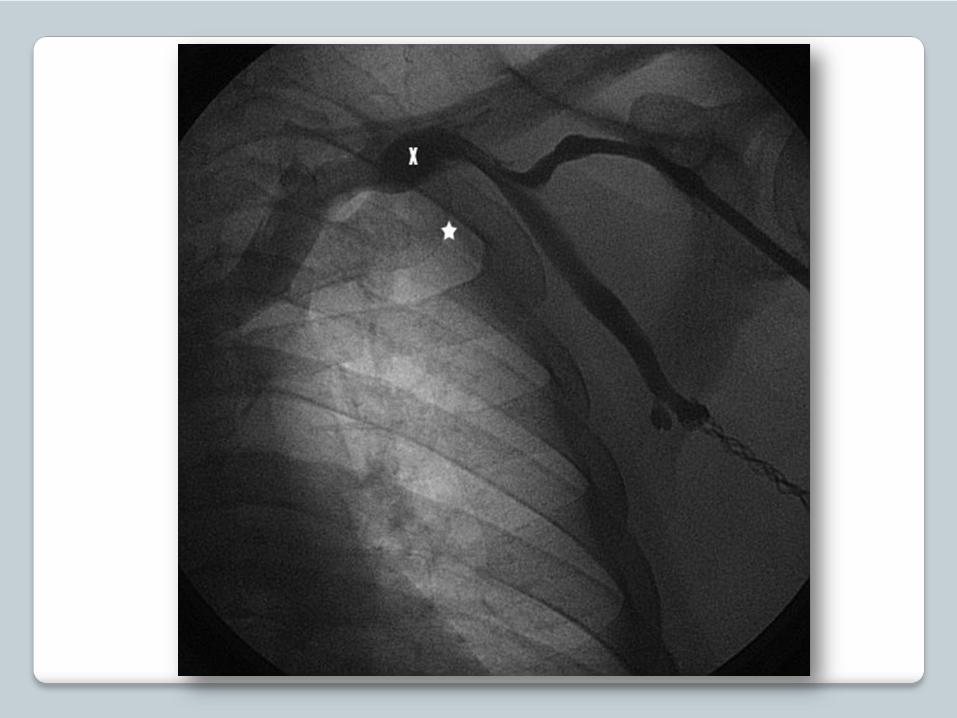

Severe vein spasm has been reported during contrast-guided axillary vein puncture in 8.1% of cases and was an independent risk factor of puncture failure.Venography showed no axillary vein course abnormalities or spasm in our 2 patients with failure of vein access. The veins were successfully cannulated after administration of intravenous fluids.We suggest that the axillary vein cannulation failed because of vein collapse, most probably due to the mechanical effect of the needle.
Unintentional puncture of the artery occurred in 6 patients (3.3%): local pressure was applied for 1-2 minutes and no significant hemorrhage was observed.There was no clinical evidence of venous thrombosis and no leads failure. No pneumothorax, hemothorax or brachial plexus injury occurred.
Conclusions:
The approach of axillary venipuncture using our
fluoroscopic landmark, without prior contrast
venography, is simple to perform, safe and
effective.





























