Embed Size (px)
Citation preview

AUTONOMIC PHARMACOLOGY
SYMPHATETIC NERVOUS SYSTEM
Magdalena Šustková

NERVOUS SYSTEMPERIPHERAL CENTRAL
AUTONOMIC NERVOUS SYSTEM SOMATIC NERVOUS SYSTEM
BRAINSPINAL CORD
Afferent part
Efferent part Senzoric part
(=effe-rent)
Moto-ric
part(=affe-rent)
Sympathetic
(adrenergic nervous system)
Parasympathetic
(cholinergic system)


ganglions periphery

Sympathetic and parasympathetic

Activation of sympathetic NS – phylogenetically old adaptive reaction
„fight-or-flight“

Sympathetic activation
State of maximal work capacity as reguired in „fight or flight“ situations
- activity of skeletal muscles and CNS - supply of oxygen and nutrients – increased blood flow - increased heart rate and contractility, peripheral (splanchnic blood vessels) vasoconstriction - enhanced bronchodilatation
- GIT – restrained and slowed – peristaltic dimishes, sphincteric tonus increases
- Etc.

parasympathetic nervous system sympathetic

Sympathetic stimulation• initiating mechanisms – stimulation of CNS
cortex and suprarenal medulla
• neurotransmitters – adrenaline (epinephrine),
noradrenaline (norepinephrine), dopamine
• target organs – skeletal muscles and CNS
• energy sources – aerobic glycolysis
• substrate transport – heart, vessels, lung and
airways

Catecholamines
Biosynthesis

Catecholamines
Degradation

Adrenergic synapse


Consequences of sympathetic stimulation
organ effect consequences
heart (β1)increased contractilityincreased heart rateincreased conduction velocity
increased heart output and blood circulation maintenance
vesselsperipheral vasoconstriction α1/skeletal vasodilatation β2 /
sufficient blood pressure maintenance
kidneysstimulation of reninsecretion
homeostasis and sufficient blood pressure maintance
lungs (β2) bronchodilatation improved ventilation
sweat glands (ACh)
sweatthermoregulation
GIT (α, β) inhibition of peristaltic blood redistrubution
eye (α1) mydriasisimproved vision in the dark
penis (α1)uterine (β2)
stimulation of ejaculationtocolytic effect
preservation of tribe/population

Acute sympatoadrenergic activation participates
in maintenance of vital important organs
vasoconstriction – blood pressure - perfusion
increased contractility and frequency – increased heart output
reduction of renal perfusion - blood redistribution
metabol. changes – activation of glycolysis – increased glycaemia
↑A IIacute stress
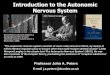
Chronic sympatoadren. activation participate in harming/damage of vital important organs
ictus
heartfailure
infarctum
renalfeilure
Na+ and water retention
aterogenesis a destabil. platesvasoconstrictionhypertrophy and remodelationligament prolipherationendothelial dysfunctions
hypertroph. a remodel. left ventricledamage of cardiomyocytes
thrombus activation
hypertension
arrhytmias↑A II

-adrenergic stimulatory effect
rec. effector consequences1 Smooth muscles
(vessels, genitourin.) contraction (↑ tension sphincters)
heart ↑ contractility, hyperthrophy
liver glycogenolysis
eye mydriasis, ↑ absorption of intraocular liquid
2 smooth-vessel muscles
contractions
pancreas (-bb.) insuline secretion

α adrenergic stimulation
• Stimulation and maintenance of blood circulation
• glycogenolysis and decrease insuline secretion – increased glucosis and its decreased storage → increased offer of glucose for glycolysis
• increased sphincter tonus

α receptors subtypes
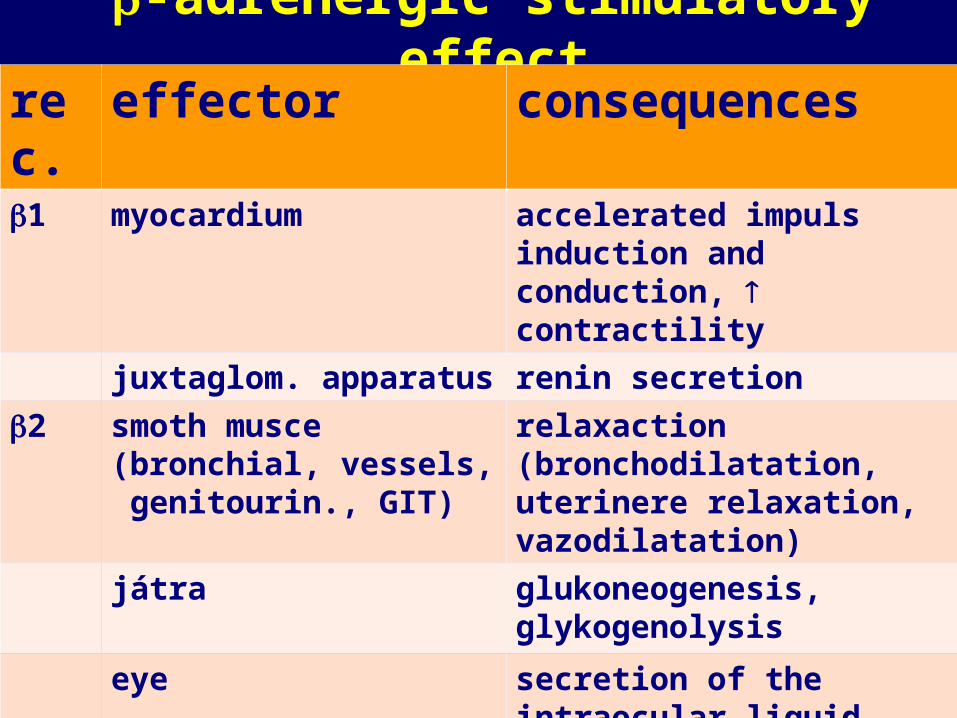
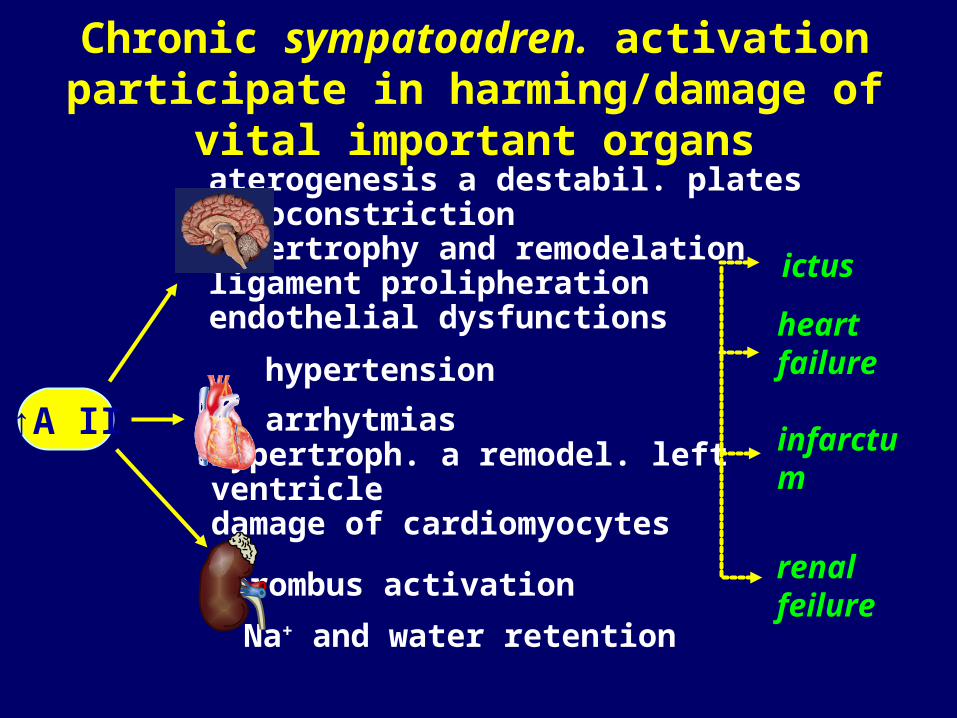
-adrenergic stimulatory effectrec. effector consequences1 myocardium accelerated impuls induction
and conduction, contractility
juxtaglom. apparatus renin secretion
2 smoth musce (bronchial, vessels, genitourin., GIT)
relaxaction (bronchodilatation,uterinere relaxation, vazodilatation)
játra glukoneogenesis,glykogenolysis
eye secretion of the intraocular liquid
skin sweating
3 lipidic tissue lipolysis

β adrenergic stimulation
• blood circulation maintenance
• blood perfusion maintenace
• increased glycaemia → increased offer of glucose for glycolysis
• lipolisis – increased source of adjuvant energy

Dopamin/dopaminergic stimulation
rec. effector consequencesDA vessels (renal, coronary,
brain and splanchnic) dilatation (low doses)
gout decreased motility

Effect na target organs -
• catecholamines have low lipophilicity - low passage into the CNS
• relatively low impact of adrenergic stimulation on brain activity
• tremor, anxiety, euphoria, insomnia, rarely psychosis

Effect na target organs -
• Potenciation of circulation, increased blood pressure, against shock/trauma („anti-shock“ effect), tachycardia, tachyarrythmia, hypertrophy (β1+1)

Effect of sympathetic and parasympathetic NS on the myocardium
sympathetic parasympathetic
noradrenalin acetylcholin
β1 β2 M2
chronotropic eff.dromotropic eff.inotropic eff.bathmtropic eff.

Effect na target organs -
• Vasoconstriction especially in splanchnic circulation –increasing of blood pressure and circulation, vessel spams 1+ 2
• improved sceletal muscles perfusion β2

Effect na target organs -
• stimulation of renin release - β1
• increased blood pressure, Na and water retention, hypertension
• sphyncter contraction, detrusor relaxation - 1 -
• urine retention, prostatic complications

Effect na target organs -
• glycogenolysis - 1
• increased glycaemia,
diabetogenic effect
• reduced insuline secretion - 2
• glucose storage reduction,
diabetogenic effect

Effect na target organs -
• decreased secretion, relaxation, slower passage - dopamine rec. a rec. β2
• blood redistribution, obstipation

Effect na target organs -
• bronchodilatation- β2
• inhibition of mastocytes degranulation, histamine reduction - β2
• vazokonstriction the tissiue - 1
• antiasthmatic effect, antialergic efgect, mucosa decongestion

Effect na target organs -
• increased intraocular fluid secretion - β2
• increased intraocular fluid resorption - 1
• pupil dilatation - 1
• mydriasis, intraocular pressure regulation

Effect na target organs -
• thermoregulatory sweat
glands throughout the body –
release ACH act on M rec.
• stress, anxiety - increased sweating on palms, soles, ampits – release NE – act on mostly α1>β2 rec.
• prevention of hyperthermia, sweating, so called „gous skin“

Pharmacologicalusage - stimulation - inhibition
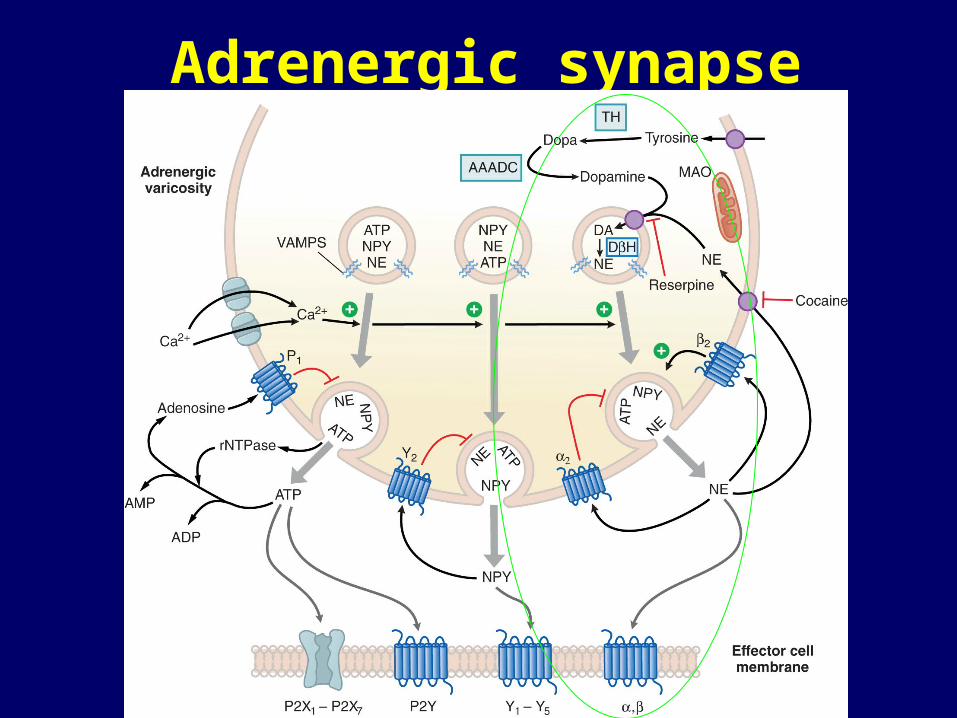
Adrenergic synapse
Direct and indirect effects
direct effects- on the receptors α (1,2) and β (1,2,3)
indirect effects- precursor for synthesis of the neuromediators (NEP, EP, DOP)- inhibition of degradation (IMAO, ICOMT)– increased release of the neuromediator from the neural ending- re-uptake inhibition- retention inhibition- combinations

SYMPATHOMIMETICS
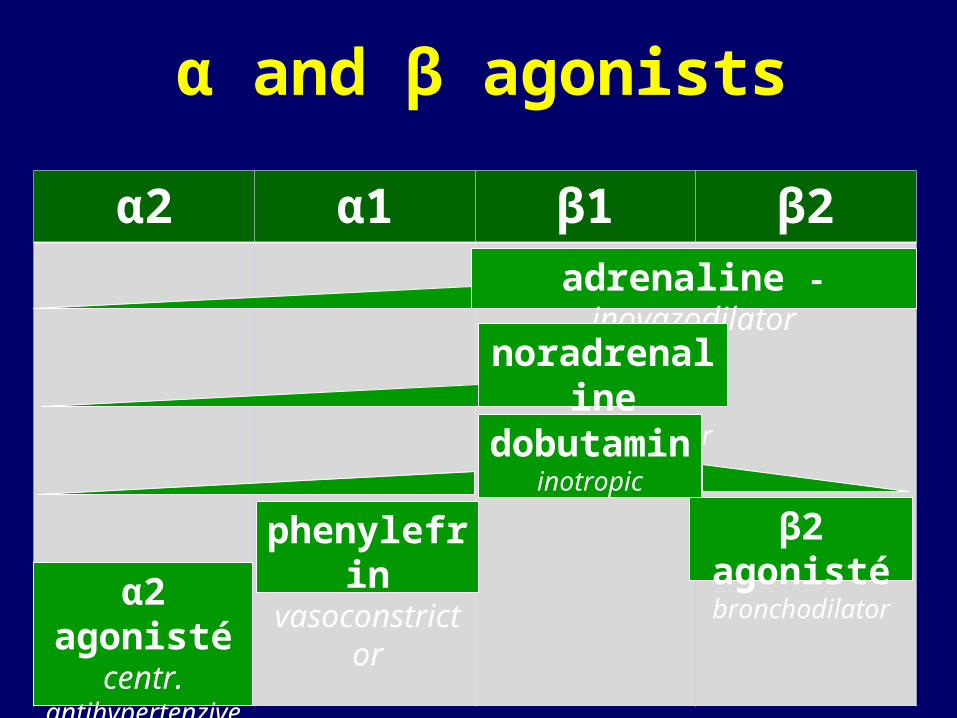
α and β agonists
α2 α1 β1 β2
adrenaline - inovazodilator
noradrenaline inovasoconstrictor
β2 agonisté bronchodilator
dobutamin inotropic
α2 agonisté centr.
antihypertenzive drug
phenylefrin vasoconstrictor

Sympathomimetics contractility (1)
• vasodilatation (2)
• vasoconstriction (1)
• used only parenteraly for treatment of acute states
• indication: shock, resuscitation, acute heart failure selhání, alergy
• CAVE: proarrhythmic effect + accelerating of ischemia

Sympathomimetics in treatment of chronic heart failure
• inovazodilators - 1,2 mimetcs with inotropic and slight vazodilatory effect - (adrenalin, epinephrine)
• inotropics - 1 mimetics (selective) (dobutamine)
• peripheral and renal vazodilators - DA agonists with renal and peripheral vasodilatation (dopamine)
• inovasoconstrictors - 1 mimet. - contractil., vasoconstr.
- mimetics - vasoconstr. (noradrenaline, norepinephrine)

Myocardial receptores and vessel receptores controlling contractility of vessal tonus
glukagon. receptor
1 - receptor 2 - receptor - receptor dopamin. rec.
adenyl-cyclasis
ATP cAMP
PDE inactivation
1 in
2 in perif.
•inotropic•chronotropic•arrhythmogenic
peripheral vazodilatation
renal and peripheral vazodilatation
vazoconstriction

ADRENALINE (EPINEPHRINE) - inovazodilator
1+2 agonist: contractility, vasodilatation mild heart rate agonist: vasoconstriction
Remarkable contractility increase + mild vasodilatation
increased heart metab. consumption, proarrhythmic effect
indication:increased heart output in heart failure of the left
ventricle

1 - receptor - receptor
ADRENALINE
1 in
•inotropic•chronotropic•arrhythmogenic
vasoconstriction
2 - receptor
2 in periphery
systemic vazodilatation
NORADRENALINE (NOREPINEPHRINE)- inovasoconstrictor
1agonista: contractility, vasoconstriction mild heart rate agonist: vasoconstrictor
signifficant contractility increase + signifficant vasoconstr.
indication: increasing of heart output in heart failure of left ventricle with serious hypotension, shock („peripheral analeptic“)

1 - receptor - receptor
NORADRENALINE
1 in
•inotropic•chronotropic•arrhythmogenic
vasoconstriction

DOBUTAMINE - 1 inotropic
1 agonist (main eff.): contractility,
mild heart rate
agonist (side. effect): vasoconstriction 2 agonist (side. effect): vasodilatation
Secondary effect - increased contractility - increased metab. myocardial requirements - proarrhythmic effect
indication:decreased heart output in acute failure of the left heart ventricle

1 - receptor 2 - receptor - receptor
DOBUTAMINE
1 in 2 in periphery
•inotropic•chronotropic•arrhythmogenic
systemic vasodilatation
vasoconstriction

DOPAMINE - renal vasodilatans • stimul. DA rec. (direct) : renal and peripher. vasodil.
1 agonist (indirectly in doses stimul. NA):
contractility + heart rate
agonist (indirectly increases NA) : vasoconstriction
signifficant vasodilatation (in doses): renal perfsionincreased contractility (in doses - stimul. noradren.)
increases metab. myocardial consumption, proarrhythmic
effectindication: increases heart output in heart failure without
hypotension improves renal perfussion potentiates diuret. effect

1 - receptor - receptor dopaminergicDA1 a 2 rec.
DOPAMINE
renal and peripheral vasodilatation
noradrenaline release
1 in
•inotropic•chronotropic•arrhythmogenic
vasoconstriction

Combination treatment with dopamine and dobutamine
clinical requirements: • increased heart output (periph. vasodilat. + increased
contractility)
• blood presure maintenance (increased contractility + vasoconstriction)
• renal perfussion maintenance (renal vasodilatation)
„golden standard“ – combination with dobutamin (increased contractility + mild vasodilatation) with dopamine (in low doses - increased renal perfusion)

2- sympathomimetics• direct effect on 2 of the bronchial smooth muscles -
bronchodilatation - speed up of sputum outflow - regul. of antiinflammatory mediators,
mastocytes local aplication in the form of aerosol or systematically (p.o. or inj.)
• long-lasting administration induces reduction of the mimetic effects - tolerance due to reduced 2 rec. expression
• glucocorticoids reduce the risk of tolerance (reasonable combination)

2- sympathomimetics
relatively frequent adverse effects :• tachyarrhythmia•tremor, spasms, insomnia •hypocalemia
contraindications:•subvalv. aortal stenosis, hypertr. obst. cardiomyopat. •thyreotoxicosis •tachyarrythmia, repolarisation disturbances (prolonged. QT interval)

-adrenergic effect
1 – receptormyocardium
2 – receptor (bronchial, vessels, urogenit. tract)
adenyl-cyclasis
ATP cAMPin
bronchialvessels
inotropic a chronotropic effect
bronchial relaxation and vazodilatation
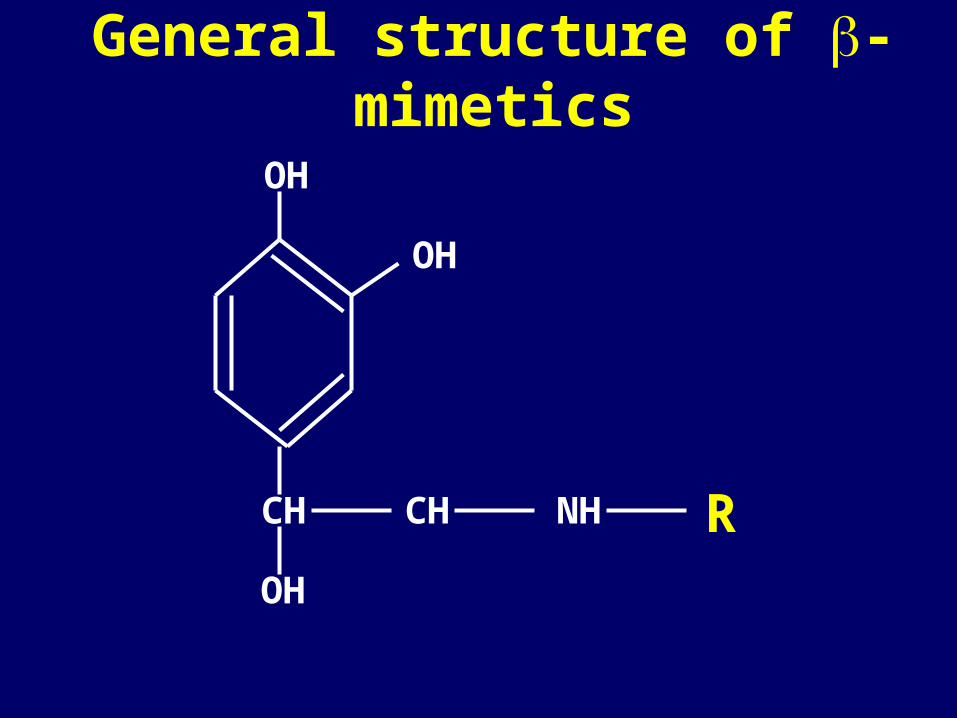
General structure of -mimetics
CH CH NH
OH
OH
OH
R

Structure and function of sympathomimetics
adrenalin
isoprenalin
albuterol
salmeterol

Fast and short-acting 2- sympathomimetics (RABA)
• fast onset of short-lasting bronchodilatation after
inhalation, inhalation more safe
• acute use in exacerbation of attack
• onset of effect in 5-10 min (inhal.), 15-90 min (p.o.)
• lasting for 4-6 hod
• salbutamol /Ventolin/
• fenoterol (Berotec)
• terbutalin (Bricanyl)

Long-lasting 2- sympathomimetics (LABA)• bronchodilatation 12 h, onset of effect in one week • not useful for treatment of acute attacks, only
prophylaxis • preference of inhalation (20x higher effect in
comparison to p.o. + systemic side effects• used for combination with inhal. glucocorticoids• medium and serious asthma in comination with
glucocort..
• salmeterol /Serevent/
• formoterol /Oxis/
• procaterol /Lontermin/
2-mimetics – adverse effects
• tremor (in higher doses)
• palpitation (heart), tachycardia, arrhythmias
even sudden death
• headache
• paradoxical bronchospasms (in inhalation)
• rarely allergy

SYMPATHOLYTICS

α and β antagonists
α2 α1 β1 β2
phentolamin - vazodilatation
antag. α1 dilat. prostat.
musc.
β1 blokátory cardioselective
karvedilol nonselective α+β blockernegat. chrono-, dromo-, inotropic, vazodilation, bronchoconstr.
β1+β2 blokátory non-cardioselective

α-BLOCKERS
- treatment of benign hyperplasia of the prostate - treatment of hypertension

α1-adrenergic receptor blockers
• treatment of benign hyperplasia of prostate – reduced sphincter tonus and increased detrusor contraction
• treatment of hypertension - vasodilatation• doxazosin, terazosin – less selective α1 blok. • alfuzosin, tamsulosin – more selective α1A blok.
Adverse eff. - hypotension, disturbed ejaculation, oedema of nasal mucosa

-BLOCKERS- one of the most
important drug groups in treatmant of
cardiovascular diseases

sir James BlackNOBEL PRICE (1958) development of
betablocker (propranolol)

Mechanism of -blocker effects
block of β1 rec.
•slowdown of SA impuls formation
•slowdown of impuls conduction
•reduced myocardial contractility
(reduced heart rate and heart output, myocardial stabilisation – reduced myocardial automacy/irritability)
•reduces renin output (reduced blood pressure)
Mechanism of -blocker effects
block of β2 a β3 rec.•increased tonus of arterial vessel smooth muscles (vasoconstriction)
•increased bronchial tonus (bronchoconstriction)
•metabolic effect (lipolysis, hyperglycaemia in diabetics
•diminuation of insuline release)

Mechanism of effect- competitive blockade of postsynaptic activation
noradrenaline
metoprolol
bisoprolol

Mechanism of -blocker effects
effect of β1 rec. blockade• Slowdown of impuls formation in the SA nodus • Slowdown of impuls conduction • Reduced myocardial contractility• Reduced myocardial irritability
reduced heart rate and heart output, myocardial stabilisation - reduced fibril. threshold
• Reduced renin output reduced blood pressure

Mechanism of -blocker effects
Effect of β2 and β3 blockade
• vasoconstriction
• bronchoconstriction
• lipolysis, hyperglycaemia

Pharmacology of blockade
affinity to the 1 a 2 rec. (selectivity)
possible parcial rec. stimulation (ISA)
lipophylic x hydrophylic
length of the effect
vasodilat. effect (rec. 2 stimulation, rec. blockade , NO release, Ca chanells blockade)

CARDIOSELECTIVITY - influence of 1 and 2 blockade
a) cardioselective
- specifically on myocardial receptors 1
- betaxolol, bisoprolol, metoprolol, esmolol, atenolol...
b) non-selective
- participating of extracardial receptors 2 (or 3)
(broncho- a vasoconstriction, reduced lipolysis and inzuline secretion)
- metipranol, pindolol, bopindolol...

CARDIOSELECTIVITY
greater impact on reduced mortality and morbidity
in the secondary prevention of heart failure
less adverse effects
well tolerated (vaso- and broncho-constriction)

Indexes of selectivity in basic cardioselective -blockers
0,9
1,7
2,4 2,4
0,8
1,6
1,1
0
0,5
1
1,5
2
2,5
acebutolol atenolol betaxolol bisoprolol celiprolol esmolol metoprolol
%

HYDROPHILICITY versus LIPOPHILICITY
a) lipophilic molecules - penetration into the CNS (insomnia, depression) - metabolised in liver ( biol. availability) - variable blood concentrations (polymorfism of CYP) - metoprolol,...
b) hydrophilic molecules - less adverse effects (not central..) - excreted through kidney (prolonged effect,
availability) - atenolol, bisoprolol...
NOT SIGNIFFICANT DIFFERENCES IN THE CLINIC
- BLOCKERS non-specific ANTAGONISING RECEPTORS
rec. blockade :mild vasodilatation
reduced negative metab. impact reduced bronchoconstriction stronger effect in heart failure therapy not sufficient data about secondary preventive
effects karvediol, (labetalol)...

DURATION OF -BLOCKER EFFECTS
it is important to keep sufficient -block. concentration during the maximal sympathicotonia – in the morning i.e. at the time of most acute coronary syndromes occurence
short-lasting non-retarded metoprolol is not suitable

Comparison of T1/2 in basic cardioselective -blockers
7-13
6-9
14-20
12-17
53-4
0
5
10
15
20
25
acebutolol atenolol betaxolol bisoprolol celiprolol metoprolol
%
BETAXOLOL, BISOPROLOL- remarkably cardioselective, withouth ISA, hydrophilic- long T1/2 (15-20 h)- little variability in biodegradation
- remarkably cardioselective, withouth ISA, lipophilic- short and variable T1/2 (drug forms with prolonged effect)- well supported clinical effect
METOPROLOL

NEBIVOLOL• medium cardioselective, hydrophilic, withouth
ISA • T1/2 8-27 h (polymorphic. metabolism)• remarkable vazodilat. effect nitrate-like effect
CELIPROLOL• highly cardioselective, hydrophilic with ISA• longer T1/2 (6-8 h)• vaso-,bronchodilat. effects (2 rec. stimulation)

KARVEDILOL (+β block.)
• mild cardioselective, medium T1/2 (6-8 h)• remarkable vasodialt. effect (-lytic eff.)• does not increase insulin-resistance• most effective drug in heart failure therapy
• prefered in heart failure and always when no hypotension and bronchoconstriction occure

-BLOCKER CARDIOVASCULAR INDICATIONS
• arterial hypertension• ischemic heart disease:
• acute myocardial infarction (IM)• stp IM – secondary prevention• angina pectoris, „mute“ ischemia
• heart failure• arrhythmia (tachyarrhythmia)

select. -BLOCKERS ADVERSE EFECTS
- heart conduction disturbances,
bradycardia
bronchial obstruction
- vasoconstriction
- reduced contractility
- dyslipidemia
- insomnia, depression, hallucination
- obstipation, diarrhoea, flatulency

-BLOCKER ADVERSE EFFECTS
- heart conduction disturbances, bradycardia
- bronchial obstruction - vasoconstriction- reduced contractility - dyslipidemia - insomnia, depression,
hallucination-obstipation, diarrhoea,
flatulency

Contraindication of selective -blokers
valid
• heart conduction
disturbances
• signifficant
bradycardia:< 55 for put on BB, < 45 for stopping BB
• phaeochromocytoma
abandoned• limb ischemia signs• Raynaud´s sy.• diabetes mellitus• depression • dyslipidemia
careful • asthma, chronic bronchitis

VARIOS CHARACTERS OF -BLOCKERS
- IMPACT ON TOLERANCE AND CONTRAINDICATIONS:
in central adverse effects - hydrophilic (e.g. bisoprolol)
in limb ischemic signs - with vazodil. activity and selective
(nebivolol, betaxolol, bisoprolol) in diabetes – non-inducing insuline-resistence
(karvedilol, nebivolol), or highly cardioselective (betaxolol, bisoprolol)
u bronchial obstruction - 2 stimul. (celiprolol) or highly cardioselective (betaxolol, bisoprolol)
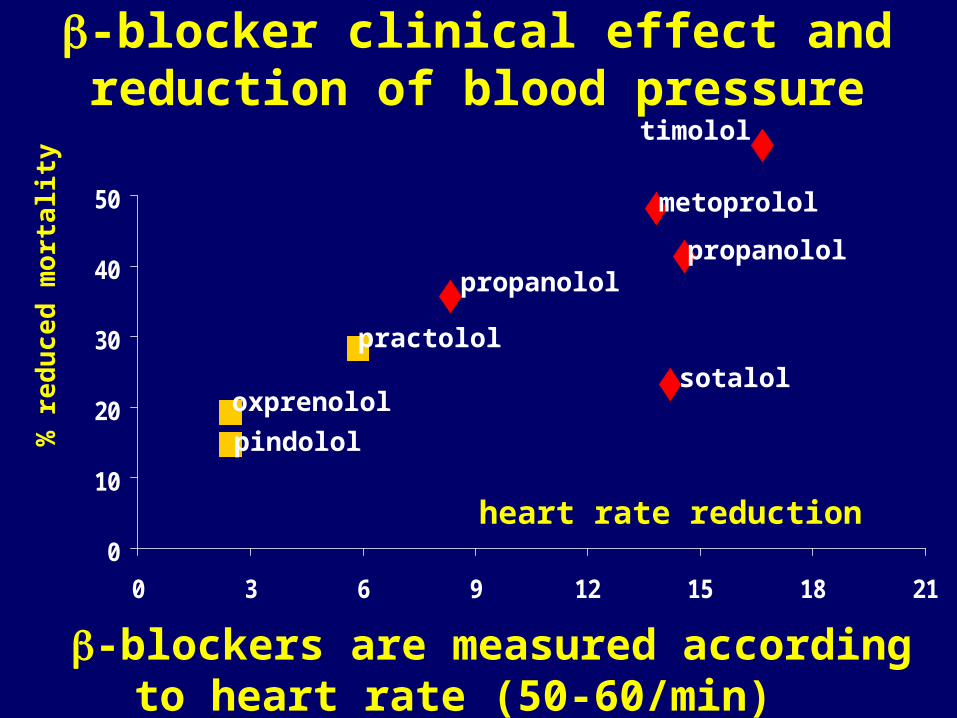
-blocker clinical effect and reduction of blood pressure
0
10
20
30
40
50
0 3 6 9 12 15 18 21
pindolol
oxprenolol
practolol
% r
edu
ced
mor
talit
y
heart rate reduction
timolol
metoprolol
propanololpropanolol
sotalol
-blockers are measured according to heart rate (50-60/min)

Thank you for your attention.