Embed Size (px)
Citation preview

AUTOIMMUNE HEMOLYTIC
ANEMIA
Jennifer Eads
January 23, 2008

Learning Objectives Review epidemiology and pathophysiology
of autoimmune hemolytic anemia
Understand the difference between warm and cold antibody mediated disease
Review treatment optionsWhich treatments are most effective?What work has been done thus far?

Early History of Hemolysis Term “hemolytic” first used in 1888 by
William Hunter in London“excessive blood destruction”
How long does a red cell live?Winifred Ashby (1919) used serologically
distinct red cells—determined RBC to live for approximately 100 days
Radioactive chromium studies—RBC life span of 110 days

Warm AIHA Due to development of an IgG antibody Antibody active at warm temperature of 37°C May be either primary or secondary in
etiologyPrimary-idiopathic in natureSecondary-due to an underlying disease
○ Lymphoproliferative disorders○ Autoimmune diseases○ Infection○ Immunodeficiency disorder○ Tumor

Epidemiology-Warm AIHA Incidence of 1-3 cases per 100,000 per year
Favors females 2:1
Age at time of occurrence dependent on causePrimary more common in women during the 4-
5th decades of lifeSecondary occurs in association with underlying
disease

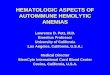
Mechanism of destruction Primarily due to extravascular hemolysis
Antibodies bind to surface of RBC membrane
Fc portion of antibody binds to macro-phagesInteraction → spherocytes
Spherocytes become trapped in spleen and are destroyed

Extravascular Hemolysis

Cold agglutinin disease Due to development of an IgM antibody Antibody active at cold temperature (4°C)
and not usually physiologically significant Either primary or secondary in etiology
Primary-idiopathic in natureSecondary-due to an underlying disease
○ Lymphoproliferative disorders○ Infection○ Autoimmune diseases○ Immunodeficiency disorder○ Tumor

Epidemiology-Cold agglutinin Disease Accounts for 16-32% of cases of AIHA
Affects older adults approximately 70 years of age
Slight female predilection

Mechanism of destruction Intravascular hemolysis
IgM antibodies activate the compliment system resulting in cytolysis
Extravascular hemolysisC3b and iC3b rather than the Fc portion of
IgM are recognizedHemolysis occurs in the liver via action of
Kupffer cells

Diagnosis Clinical signs and
symptomsFatiguePallorJaundiceShortness of breathHeart failure
Raynaud’s phenomenon, vascular occlusions/necrosis in cold agglutinin disease
Lab dataCBC with peripheral
smearLDHHaptoglobinBilirubin

Diagnosis Disease severity depends on degree of hemolysis
Antibody characteristics○ Quantity○ Specificity○ Thermal amplitude○ Ability to fix compliment○ Ability to bind tissue macrophages
Antigen characteristics○ Density of antigen on cell surface○ Degree of antigen expression○ Patient age

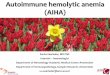
Diagnosis
Serologic evidence of the presence of an antibodyDirect antiglobulin test
○ Patient’s RBC’s mixed with antiglobulinSpecific focus on IgG and C3d
○ Positive in almost all cases○ Non-specific for a RBC autoantibody
Indirect antiglobulin test○ Positive in approximately 80% of cases○ Autoantibodies likely to be panreactive as
compared to alloantibodies

Direct and Indirect Coombs Tests

Treatment-Role of Blood Transfusion Limit to life threatening situations or high
risk patients
Best to use most compatible units
Often difficult to match
Transfusion may stimulate further formation of autoantibody

Treatment-Warm AIHA
Folic acid supplementation Glucocorticoids Splenectomy Cytotoxic drugs Rituximab Plasmapheresis IVIg

Glucocorticoids
Dameshek et al (NEJM, 1951)5 patients given ACTH for acquired AIHAAll showed remission of diseaseWithdrawl of ACTH resulted in recurrence
Subsequent studiesWhat doses are appropriate?Which steroids should be used?How long should treatment continue?

Glucocorticoids Initial therapeutic intervention for warm AIHA
Initial prednisone dose of 1-1.5mg/kg/day
Response rates20-30% have a lasting remission50% require low dose maintenance10-20% do not respond
Considered a failure if 15mg or greater of prednisone is required to maintain a Hct of at least 30%

Glucocorticoids
Multiple possible adverse effectsOsteoporosisAvascular necrosisIncreased risk for infectionCataractsGlucose/lipid abnormalitiesBehavioral changesPeptic ulcer diseaseMyopathy

Splenectomy First done in patients with either ITP or
congenital spherocytic anemias
Welch et al (NEJM, 1950)Splenectomy performed in 220 patients with “blood
dyscrasias” at NEMC between July 1939 and June 1949
First evaluation of role for hemolytic anemia○ 34 cases with primary etiology
“Good results” in 50%
○ 18 cases with secondary etiology “Good results” in 33%

Splenectomy Second line treatment
Has multiple benefitsRemoves site of hemolysisDecreases antibody production
Response rate of 60-75%Often will still require steroids
Requires immunization

Cytotoxic Drugs
Moyo et al (Blood, 2002)9 patients with severe refractory AIHA
○ Includes both warm and cold antibodiesTreated with high dose cyclophosphamide
for 4 consecutive days (50mg/kg/day)6 patients achieved a complete response, 3
a partial response

Cytotoxic Drugs
Includes cyclophosphamide, azathioprine and cyclosporine A
Results in a 40-60% response rate
May cause bone marrow suppression

Rituximab
An anti-CD20 monoclonal antibody
Results in B cell destructionComplement mediated cytotoxicityAntibody dependent cytotoxicityInhibition of B cell proliferationInduction of apoptosis

Rituximab Zecca et al (2003)
15 children with AIHA/Evan’s syndrome looked at prospectively
All children had failed two lines to treatmentFound to have an 87% response (13/15)
○ Increase in hemoglobin level by 1.5g/dL○ Decrease in reticulocyte count by 50%○ Fewer patients with positive DAT
All other immunosuppressants stoppedAny patient to relapse (3) had subsequent
remission with further treatments

Plasmapheresis
Current data based on case reports
Has been difficult to assess effectiveness in setting of other treatments
May be useful in fulminant cases until other therapies can take effect

Intravenous immunoglobulin Tried in AIHA after it was found to work
well for patients with ITP
Second line therapy for steroid non-responders
When used, requires higher doses than used for treatment of ITP

Treatment-Cold agglutinin disease Avoidance of cold temperature Folic acid supplementation Cytotoxic drugs α-interferon Plasmapheresis Rituximab
Efforts should be made to limit transfusionDifficult to matchTransfusion worsens hemolysisBlood warmer may reduce the risk of further hemolysis

ReferencesBussel, J.B. et al. Intravenous Treatment of Autoimmune Hemolytic Anemia with Very High
Dose Gammaglobulin, Vox Sang, 1986, 51:264-269
Buetens, O.W., Ness, P.M. Red blood cell transfusion in autoimmune hemolytic anemia, Current Opinion in Hematology, 2003, 10:429-433
Dacie, J.V. The immune hemolytic anemias: a century of exciting progress in understanding, British Journal of Haematology, 2001, 114:770-785
Dameshek, W. et al. The treatment of acquired hemolytic anemia with adrenocorticotrophic hormone (ACTH), The New England Journal of Medicine, Jan 1951, Vol 244, No 4
Gehrs, B.C. and Friedberg, R.C. Autoimmune Hemolytic Anemia, American Journal of Hematology, 2002, 69:258-271
Moyo, V.M. et al. High-dose cyclophosphamide for refractory autoimmune hemolytic anemia, Blood, July 2002, Vol 100, No 2
Perrotta, S. et al. Anti-CD20 monoclonal antibody (Rituximab) for life-threatening autoimmune haemolytic anaemia in a patient with systemic lupus erythematosus, British Journal of Haematology, 2002, 116:465-467
Petz, L. Treatment of autoimmune hemolytic anemias, Current Opinion in Hematology, 2001, 8:411-416
Welch, C.S. et al. Splenectomy in blood dyscrasias, The New England Journal of Medicine, Apr 1950, Vol 242, No 16
Zecca, M. et al. Rituximab for the treatment of refractory autoimmune hemolytic anemia in children, Blood, 2003, Vol 101, No 10









![Reference ID: 4163684 · 2017-10-06 · Autoimmune hemolytic anemia and autoimmune pancytopenia [see Warnings and Precautions (5.8)], undifferentiated connective tissue disorders,](https://img.pdfslide.us/doc/110x75/5e6c3053a4cd0f4cd9724d58/reference-id-4163684-2017-10-06-autoimmune-hemolytic-anemia-and-autoimmune-pancytopenia.jpg)








![HISK 10 ANemia HEMOLITIK.ppt [Read-Only] - ocw.usu.ac.idocw.usu.ac.id/course/download/1110000096-hematology-and-immunology... · Autoimmune hemolytic anemia caused byAutoimmune hemolytic](https://img.pdfslide.us/doc/110x75/5c7c94c409d3f23a2a8b4fbf/hisk-10-anemia-read-only-ocwusuacidocwusuacidcoursedownload1110000096-hematology-and-immunology.jpg)