Embed Size (px)
Citation preview

Autoimmune diseases
• Chronic inflammatory conditions• Repair mechanisms cannot compete with tissue
destruction caused by the immune system• Variety of symptoms and of target tissues
• Mechanisms of recognition and effector functions are the same as those acting against pathogens and environmental antigens
AUTOIMMUNE DISEASES
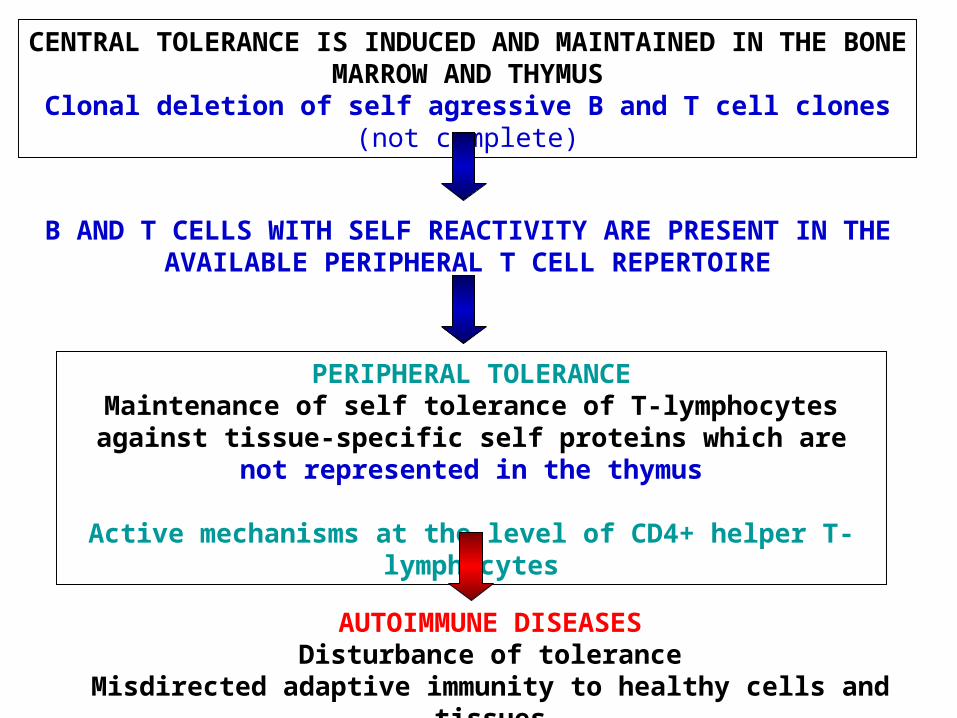
CENTRAL TOLERANCE IS INDUCED AND MAINTAINED IN THE BONE MARROW AND THYMUS
Clonal deletion of self agressive B and T cell clones (not complete)
B AND T CELLS WITH SELF REACTIVITY ARE PRESENT IN THE AVAILABLE PERIPHERAL T CELL REPERTOIRE
PERIPHERAL TOLERANCEMaintenance of self tolerance of T-lymphocytes against tissue-specific self proteins which are not represented in the thymus
Active mechanisms at the level of CD4+ helper T-lymphocytes
AUTOIMMUNE DISEASESDisturbance of tolerance
Misdirected adaptive immunity to healthy cells and tissues

Deficiency in establishing central T-cell tolerance:
Autoimmune PolyEndocrinopathy- Candidiasis-Ectodermal Dystrophy (APECED),
AIRE deficiency. AIRE: transcription factor inducing expression of many tissue-specific genes normally not expressed in the thymus.
Rare disease, but more frequently seen in inbred populations Finnish, Iranian Jews and in the island of Sardine
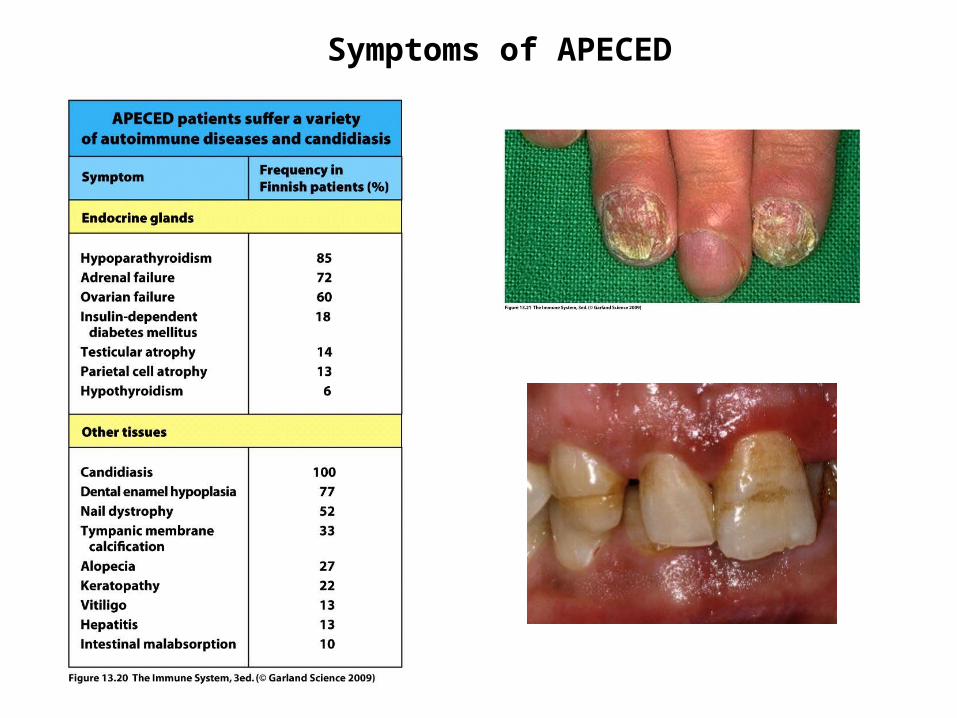
Symptoms of APECED
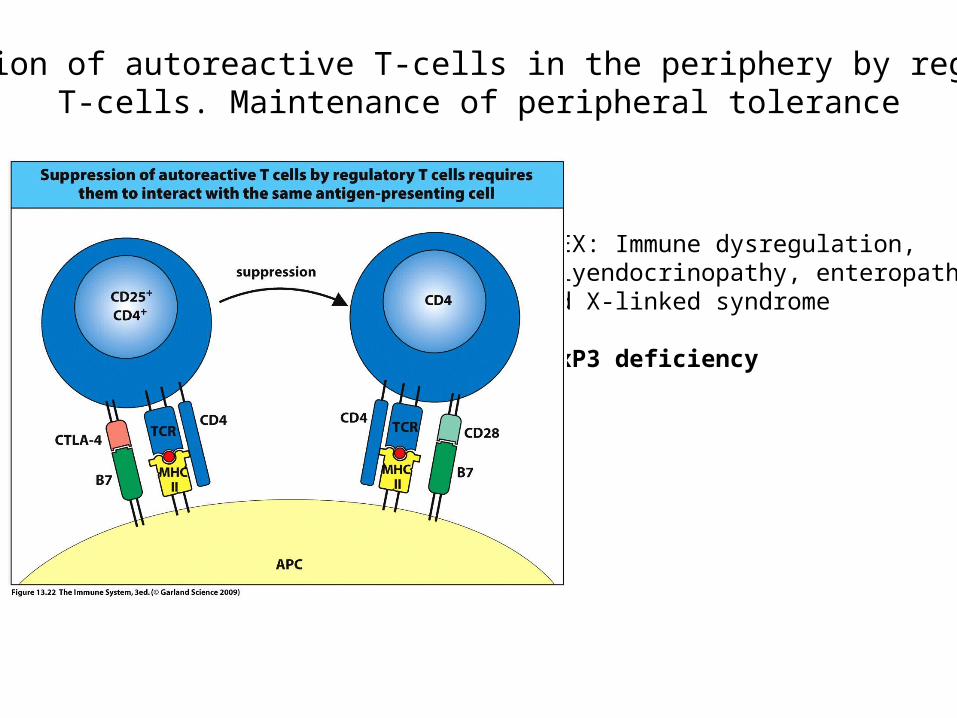
Inhibition of autoreactive T-cells in the periphery by regulatoryT-cells. Maintenance of peripheral tolerance
IPEX: Immune dysregulation, Polyendocrinopathy, enteropathy, and X-linked syndrome
FoxP3 deficiency
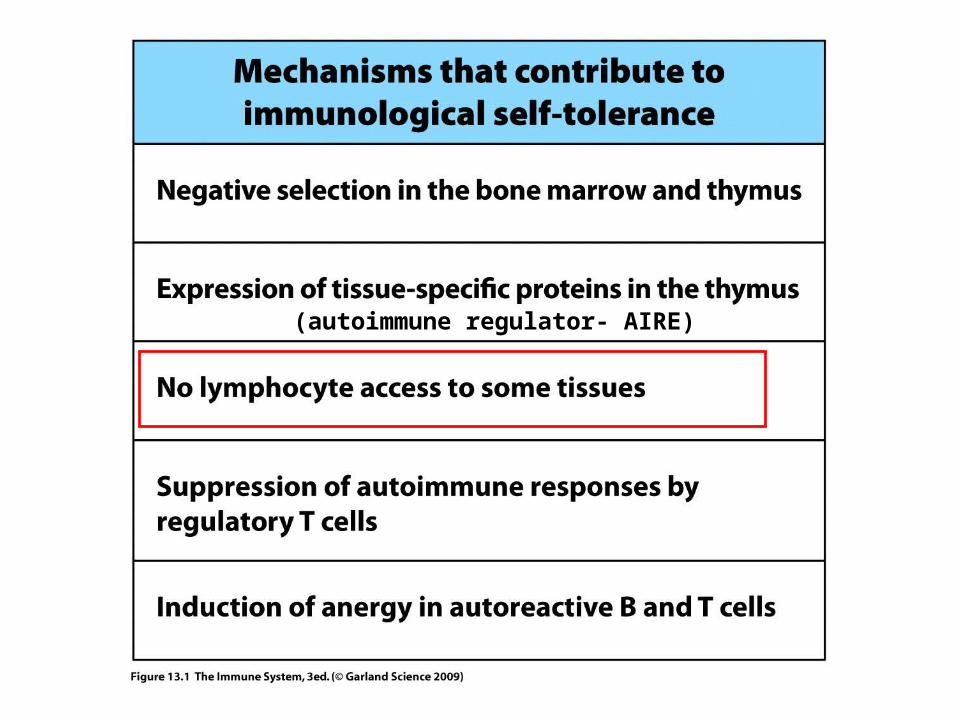
(autoimmune regulator- AIRE)
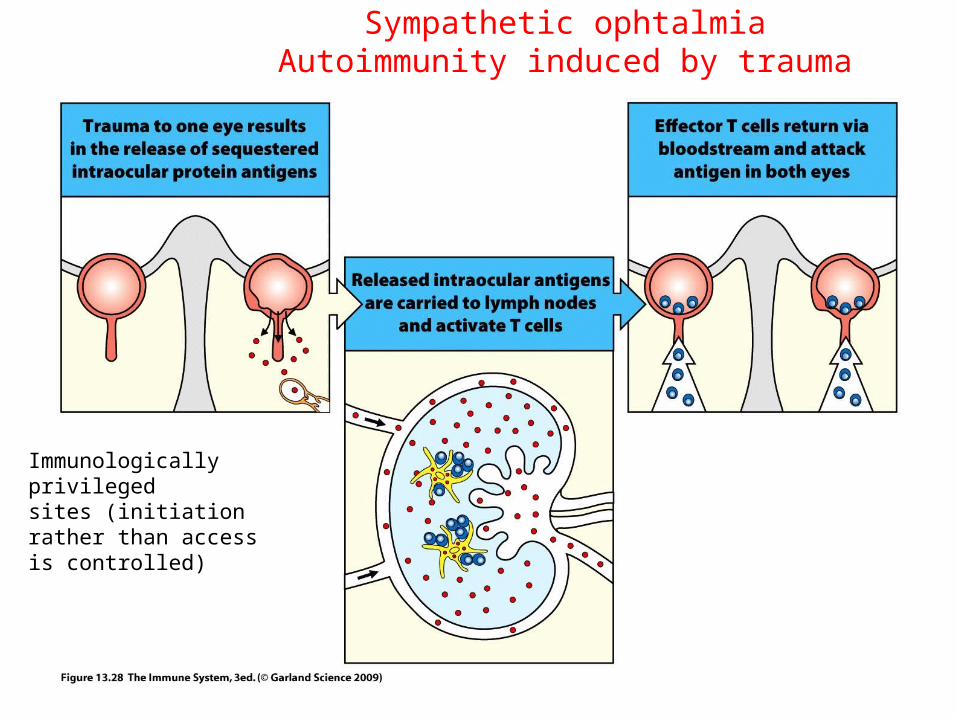
Sympathetic ophtalmiaAutoimmunity induced by trauma
Immunologically privilegedsites (initiation rather than access is controlled)
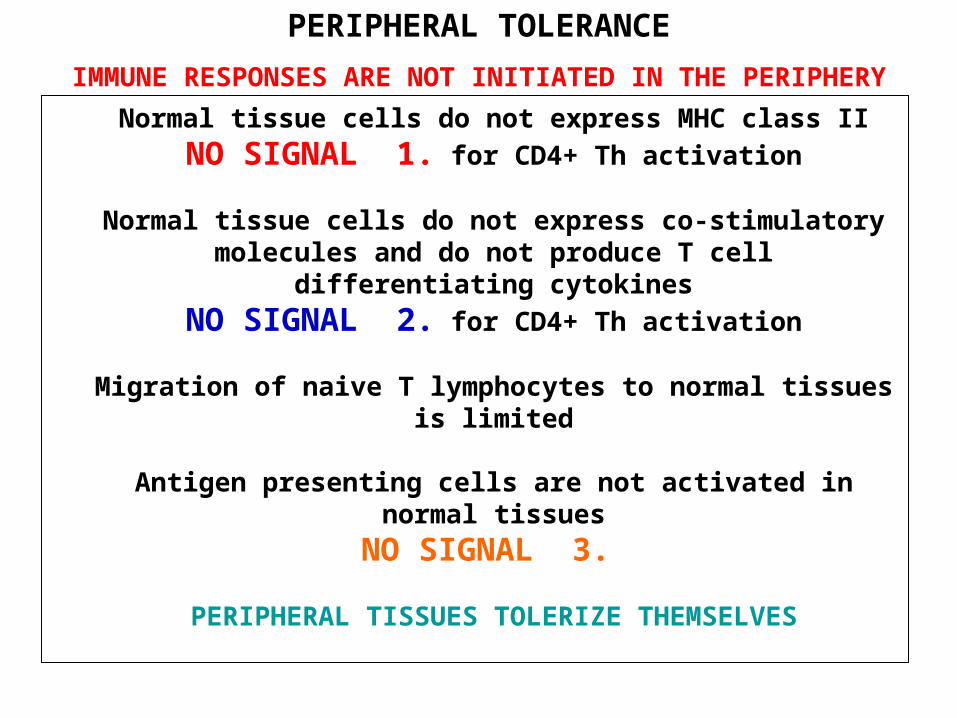
Normal tissue cells do not express MHC class II
NO SIGNAL 1. for CD4+ Th activation
Normal tissue cells do not express co-stimulatory molecules and do not produce T cell differentiating cytokines
NO SIGNAL 2. for CD4+ Th activation
Migration of naive T lymphocytes to normal tissues is limited
Antigen presenting cells are not activated in normal tissues
NO SIGNAL 3.
PERIPHERAL TISSUES TOLERIZE THEMSELVES
PERIPHERAL TOLERANCE
IMMUNE RESPONSES ARE NOT INITIATED IN THE PERIPHERY

Autoantibody production is dependent on the availability of autoreactive T cells
Practically all autoimmune diseasesInvolve some T-cell defects
In the absence of T cell help autoreactive B cells ate trapped in the T-cell zone and die

Expression of MHC-II on non-immune cells may contribute to autoimmunity
• in response to IFNγ MHCII expression is induced on thyroid cells, on the β cells of the pancreas as well as on microglia.
• Insufficient for the activation of naive T-cells (not normally present in the periphery anyway), BUT effector T-cells crossreacting with autoantigens may be activated

Molecular mimicry may lead to severe autoimmune reactions(T-cell epitopes)

Molecular mimicry may lead to severe autoimmune reactions(T-cell epitopes)
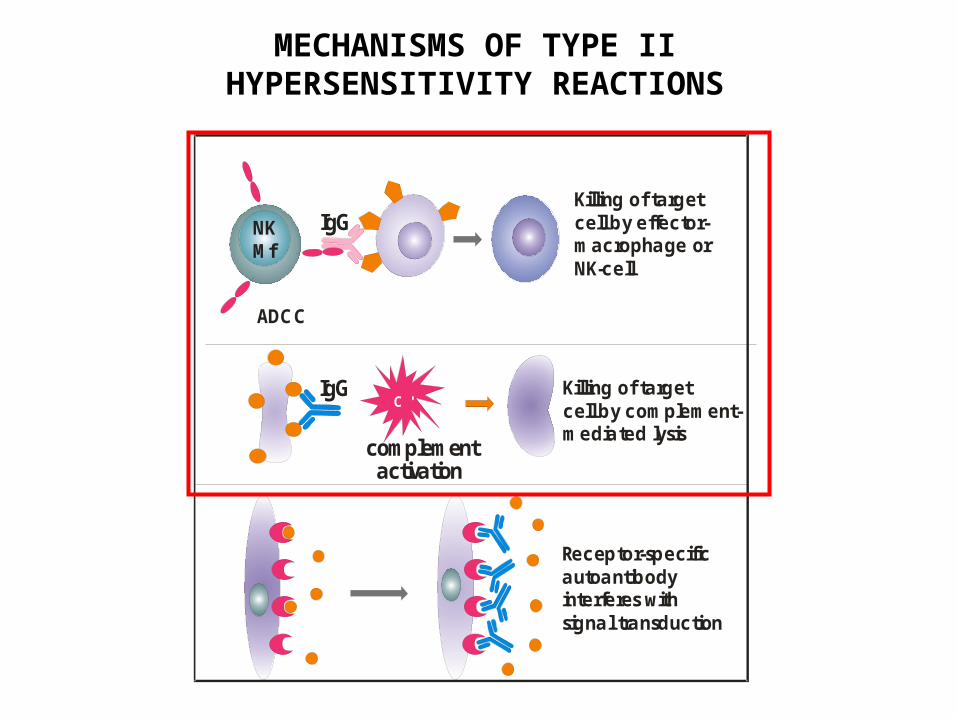
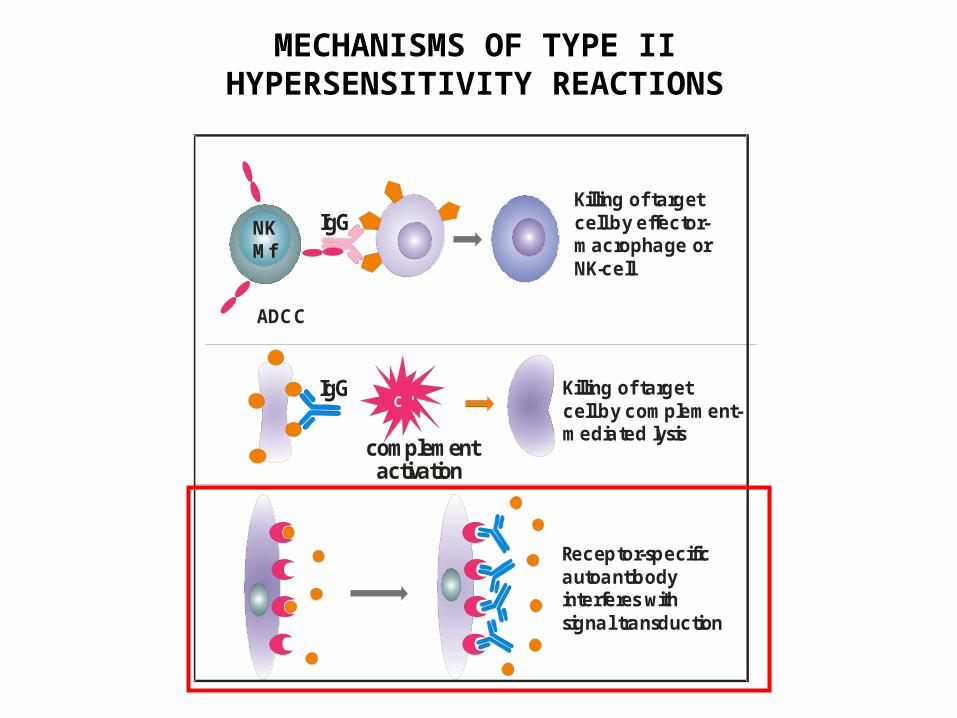
MECHANISMS OF TYPE II HYPERSENSITIVITY REACTIONS
Killing of target cell by effector-macrophage orNK-cell
Killing of targetcell by complement-mediated lysis
complement activation
IgG
IgG
Receptor-specific autoantibodyinterferes withsignal transduction
NKMf
C '
ADCC
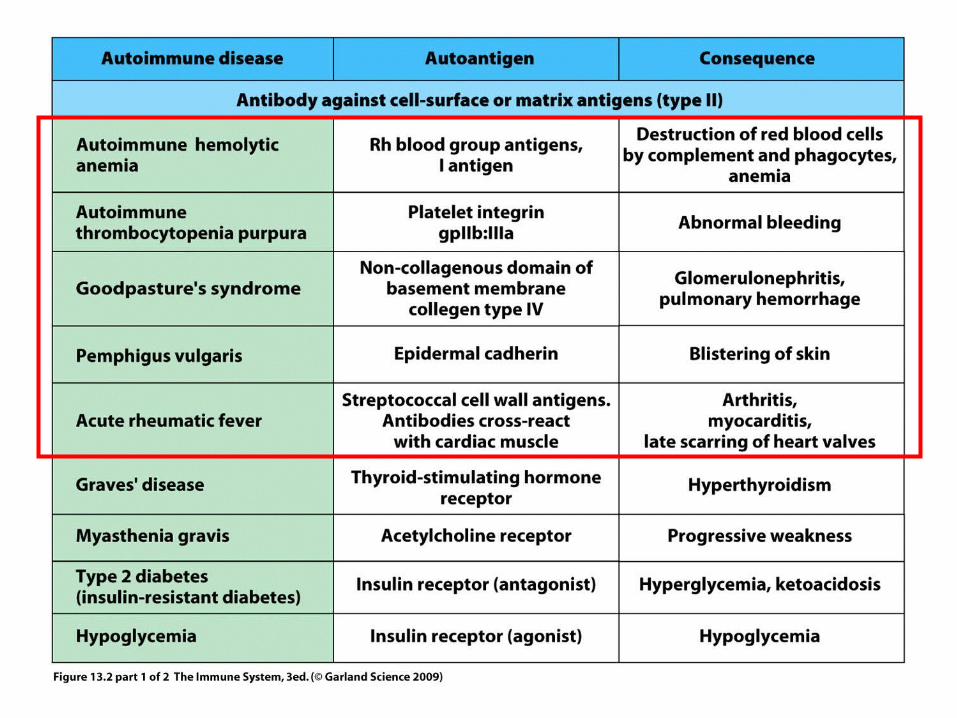
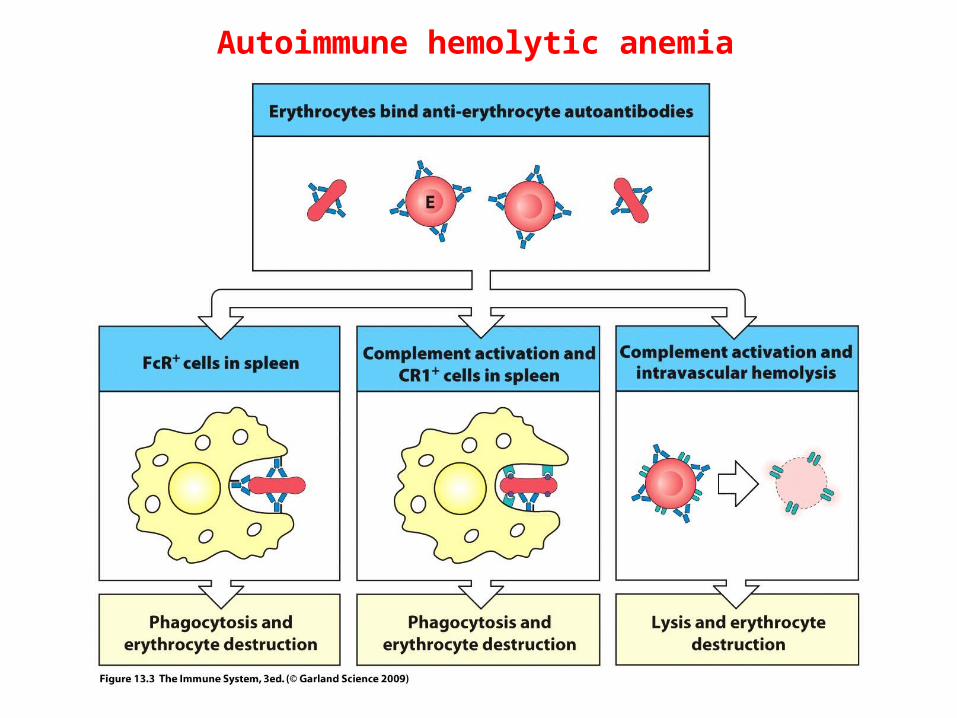
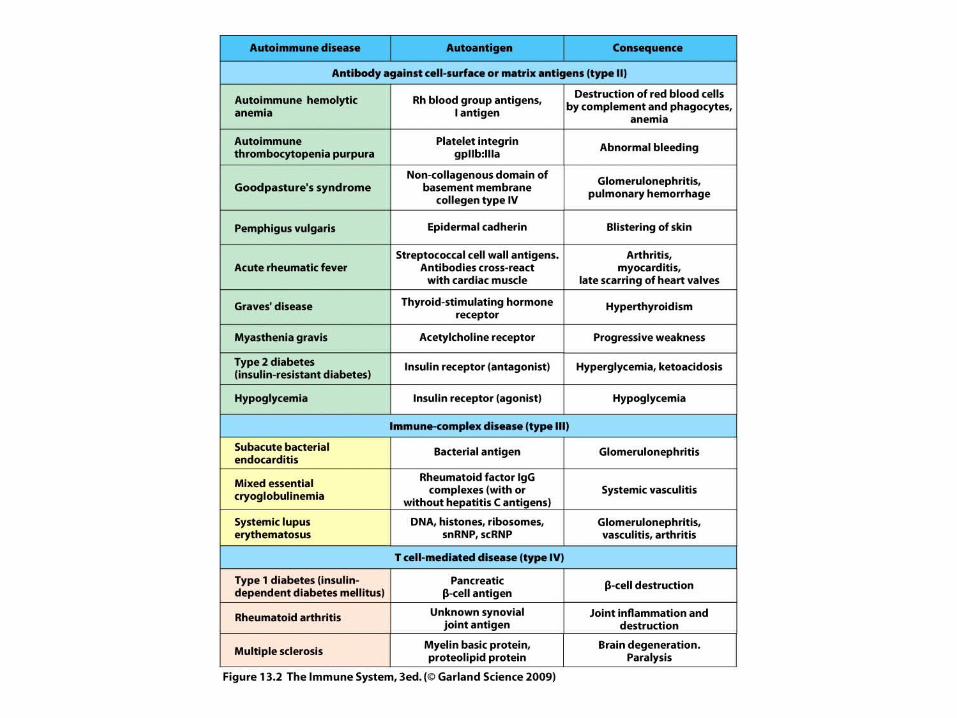
Autoimmune hemolytic anemia
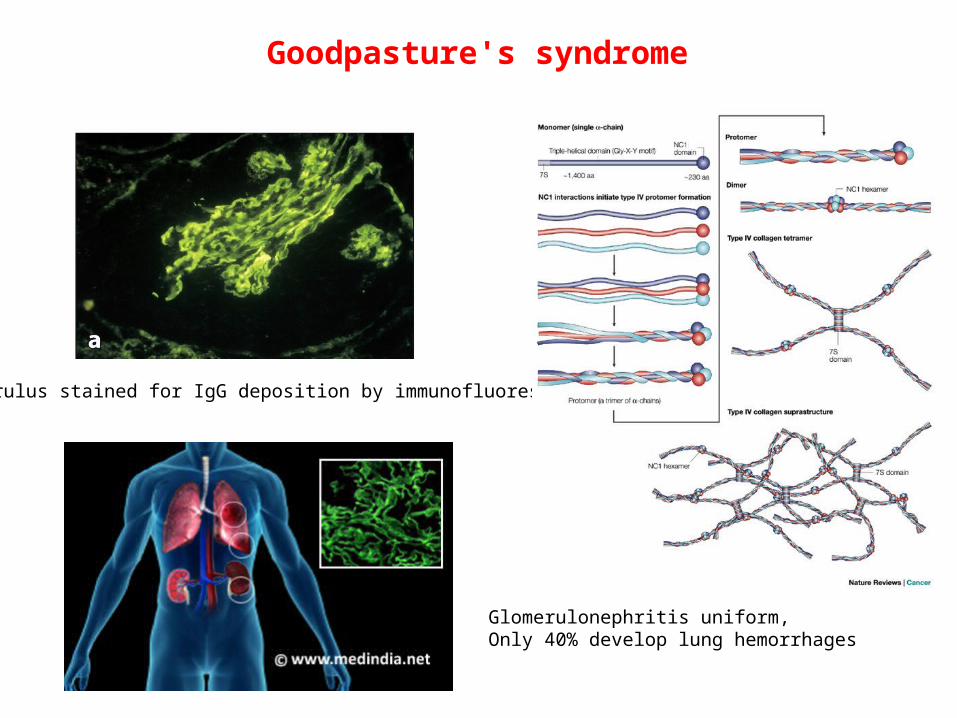
Goodpasture's syndrome
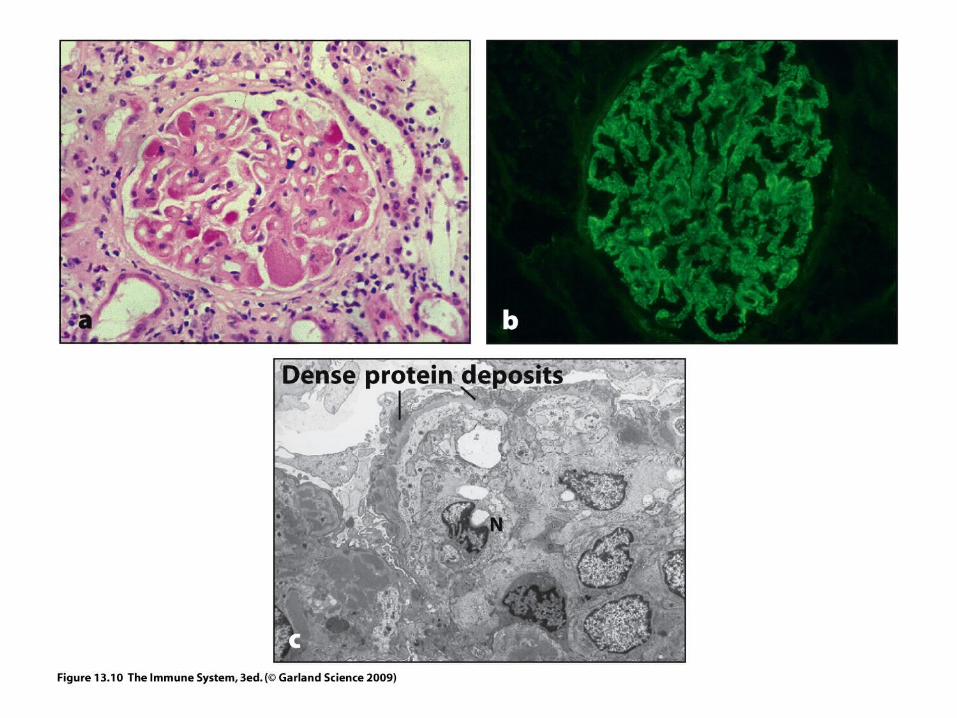
Glomerulus stained for IgG deposition by immunofluorescence
Glomerulonephritis uniform,Only 40% develop lung hemorrhages
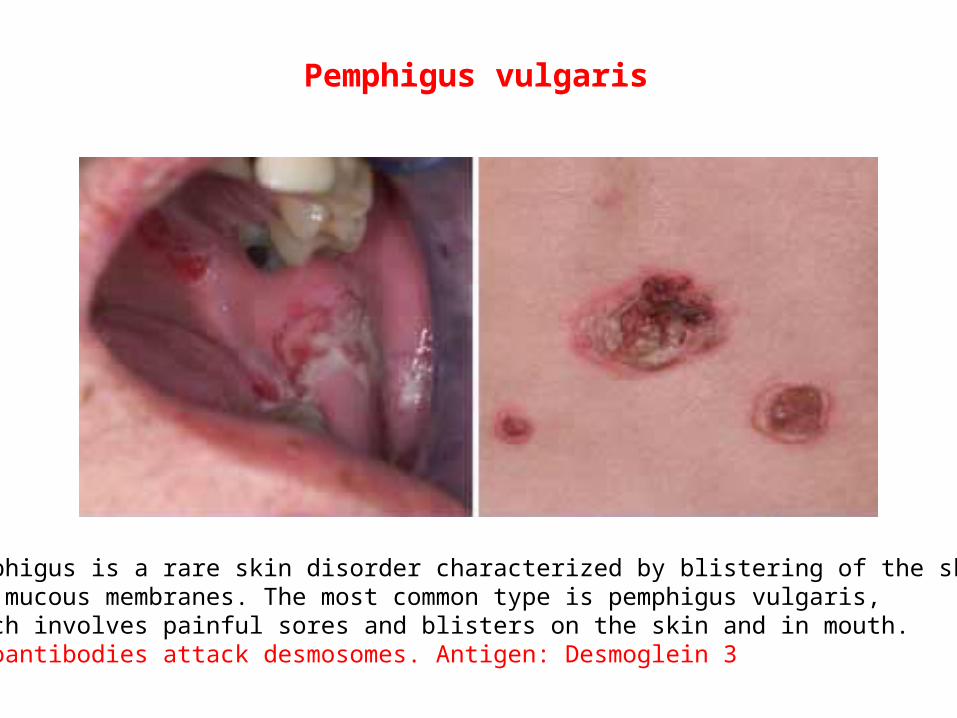
Pemphigus is a rare skin disorder characterized by blistering of the skin and mucous membranes. The most common type is pemphigus vulgaris, which involves painful sores and blisters on the skin and in mouth. Autoantibodies attack desmosomes. Antigen: Desmoglein 3
Pemphigus vulgaris

Epitope spreading ( pemphigus foliaceus)
desmoglein
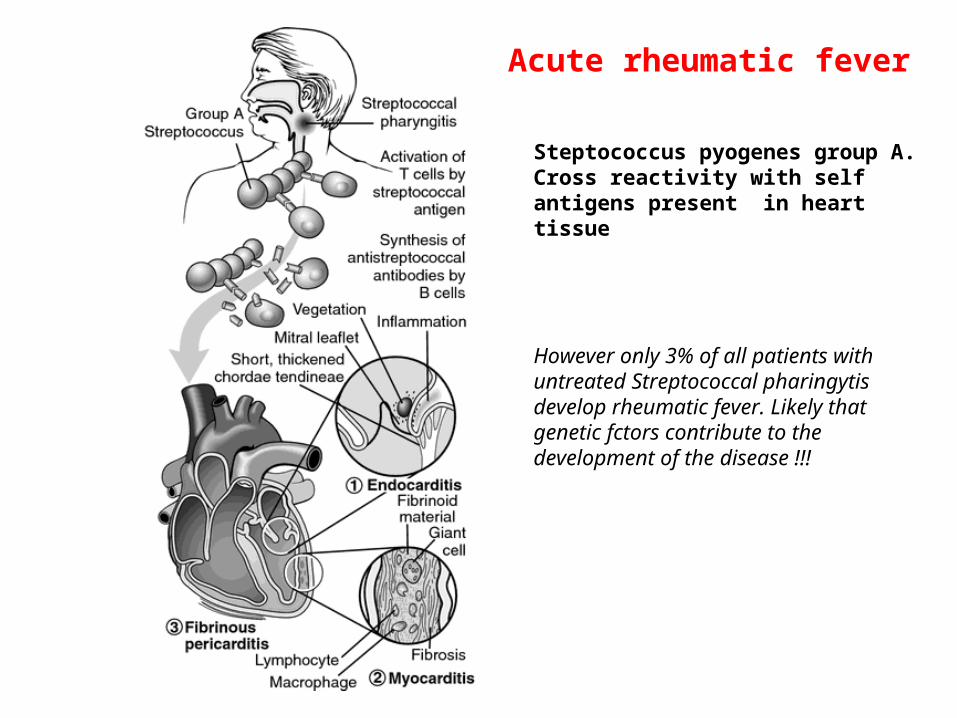
Acute rheumatic fever
Steptococcus pyogenes group A. Cross reactivity with self antigens present in heart tissue
However only 3% of all patients with untreated Streptococcal pharingytis develop rheumatic fever. Likely that genetic fctors contribute to the development of the disease !!!
MECHANISMS OF TYPE II HYPERSENSITIVITY REACTIONS
Killing of target cell by effector-macrophage orNK-cell
Killing of targetcell by complement-mediated lysis
complement activation
IgG
IgG
Receptor-specific autoantibodyinterferes withsignal transduction
NKMf
C '
ADCC
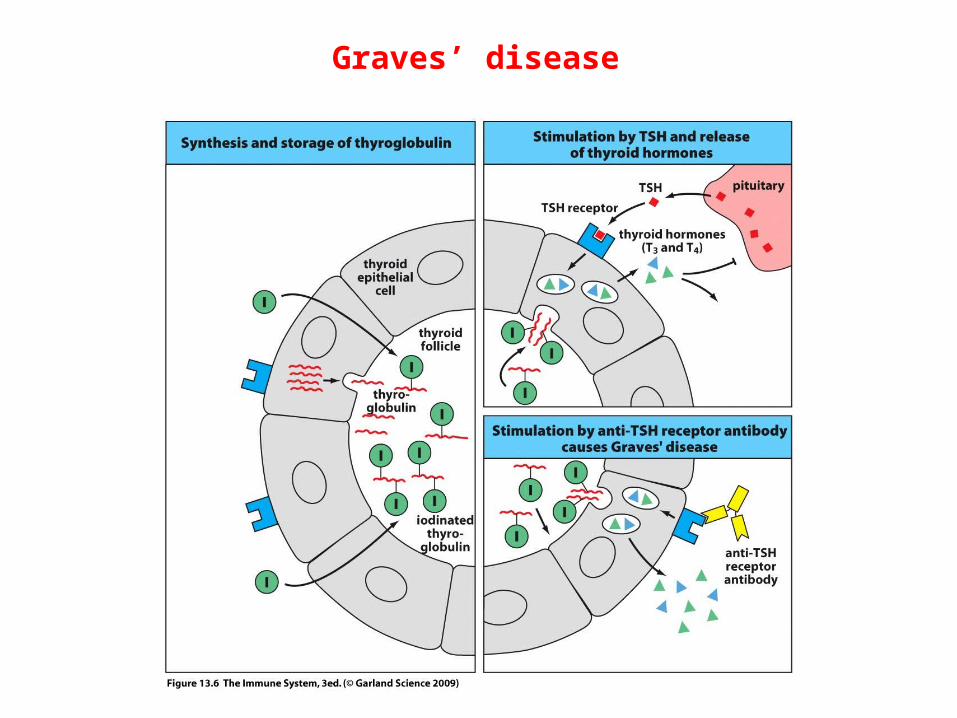
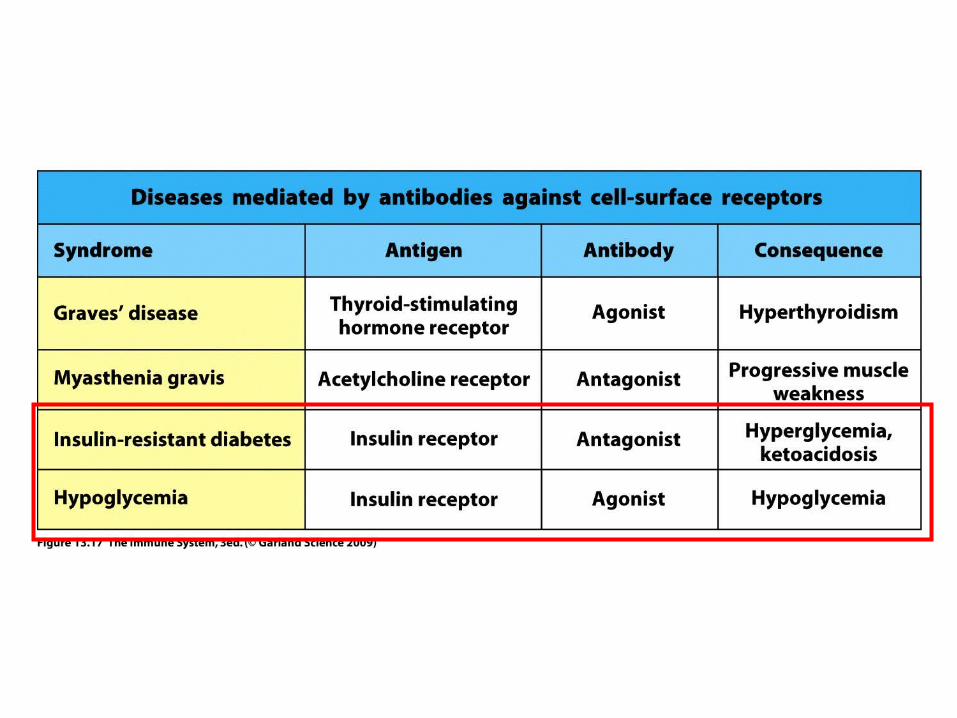
Graves’ disease

Graves' ophthalmopathy
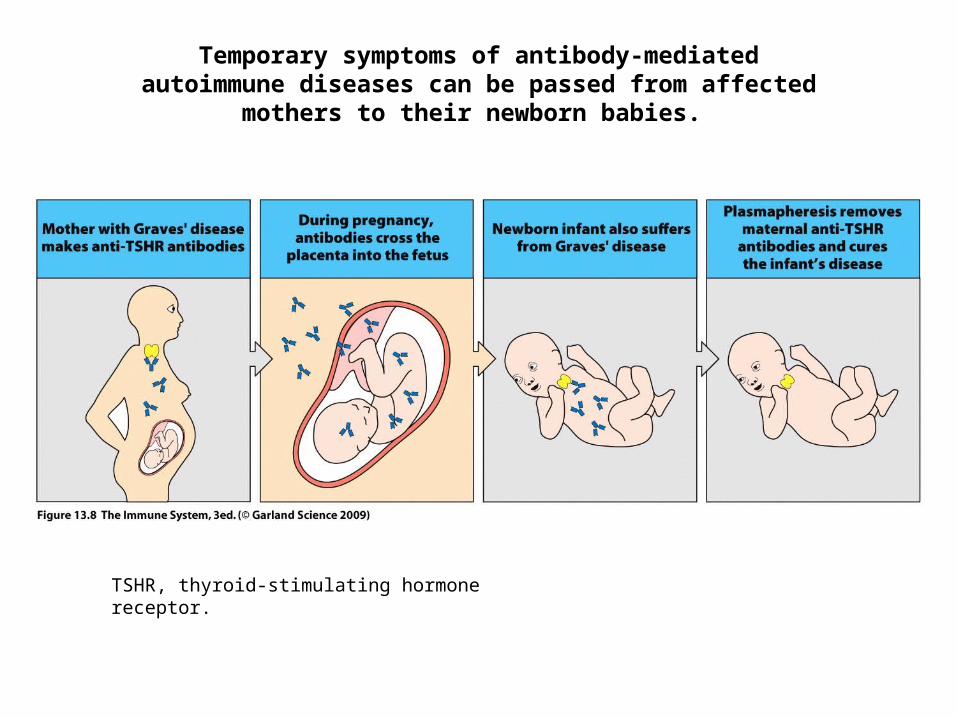
Temporary symptoms of antibody-mediated autoimmune diseases can be passed from affected mothers to their
newborn babies.
TSHR, thyroid-stimulating hormone receptor.
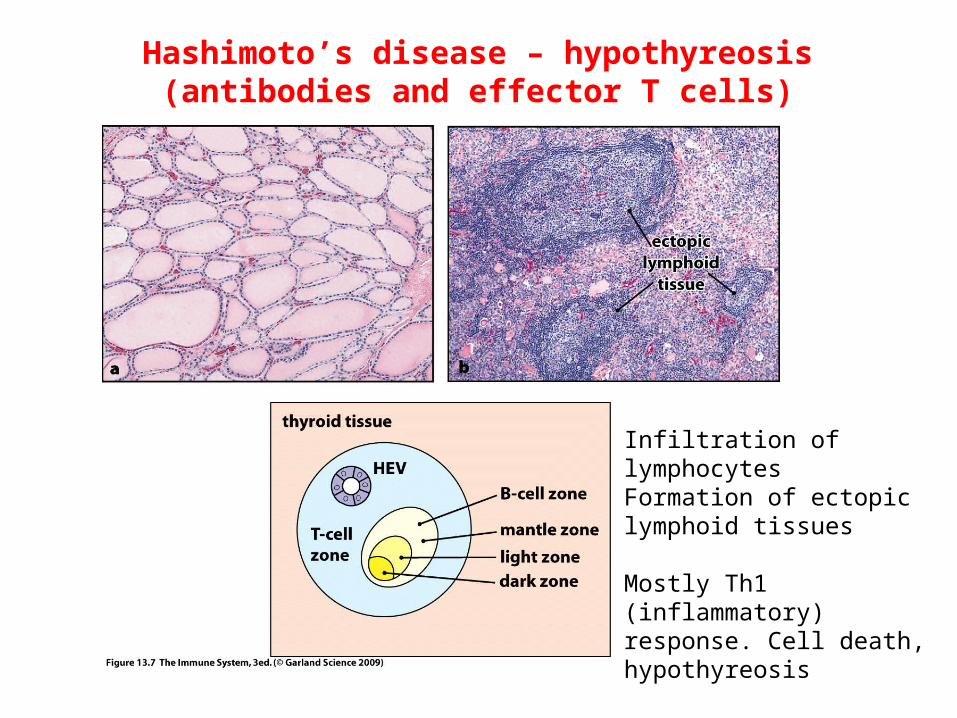
Hashimoto’s disease – hypothyreosis(antibodies and effector T cells)
Infiltration of lymphocytes Formation of ectopic lymphoid tissues
Mostly Th1 (inflammatory) response. Cell death, hypothyreosis

Nerve impulse
Nerve impulse
InternalizationNO Na+ influx
NO muscle contraction
MYASTENIA GRAVIS
AUTO – ANTIBODIES IN MYASTENIA GRAVIS
NEURO-MUSCULAR JUNCTION
Muscle
Acetilcholin receptor
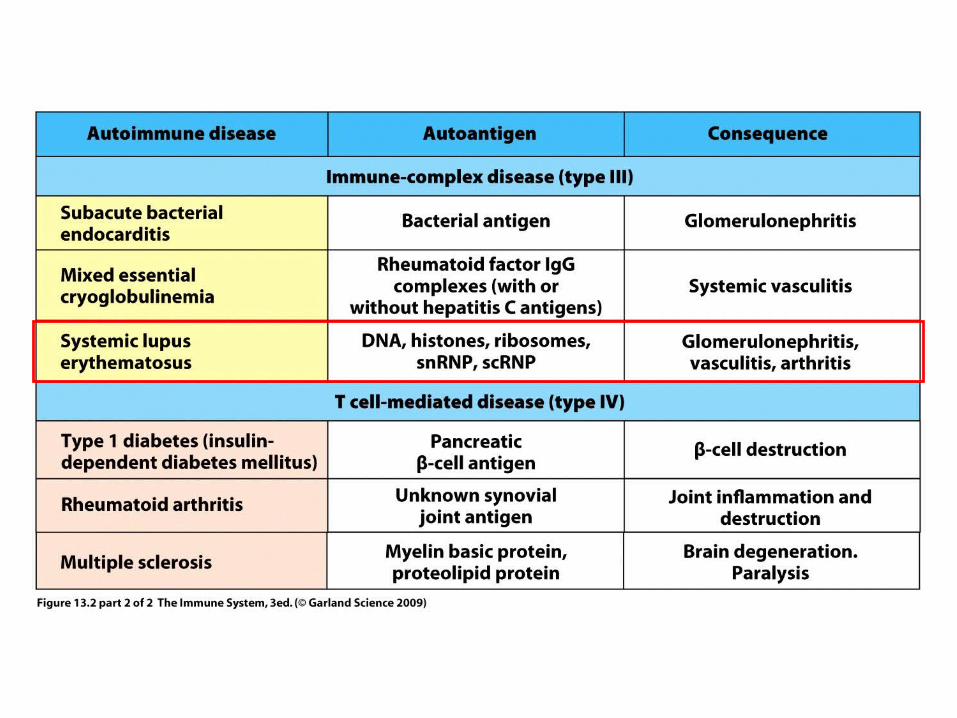
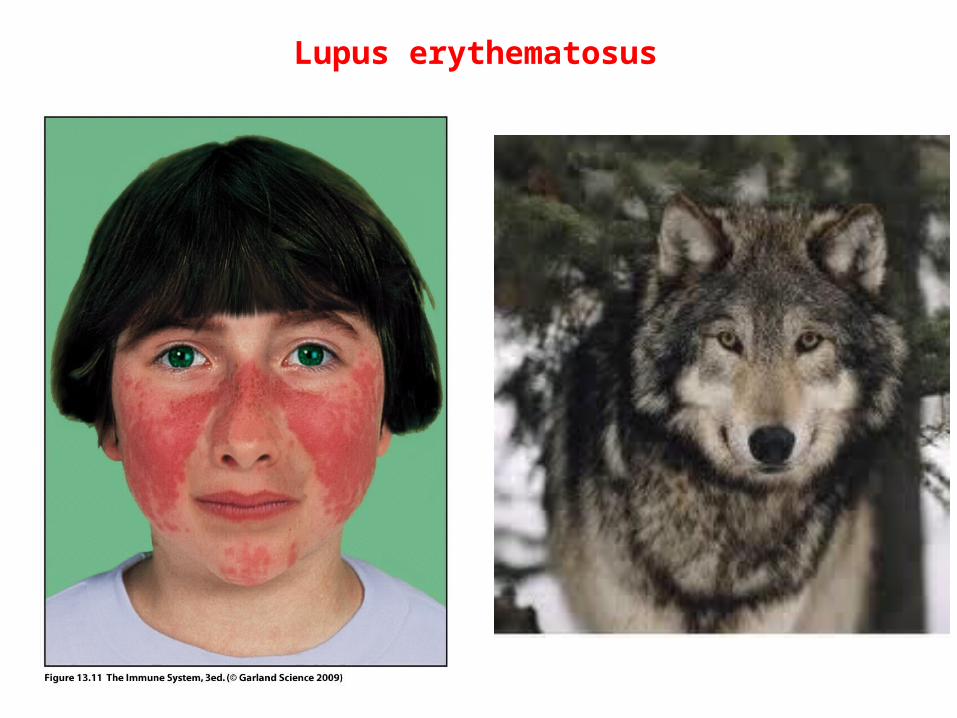
Lupus erythematosus
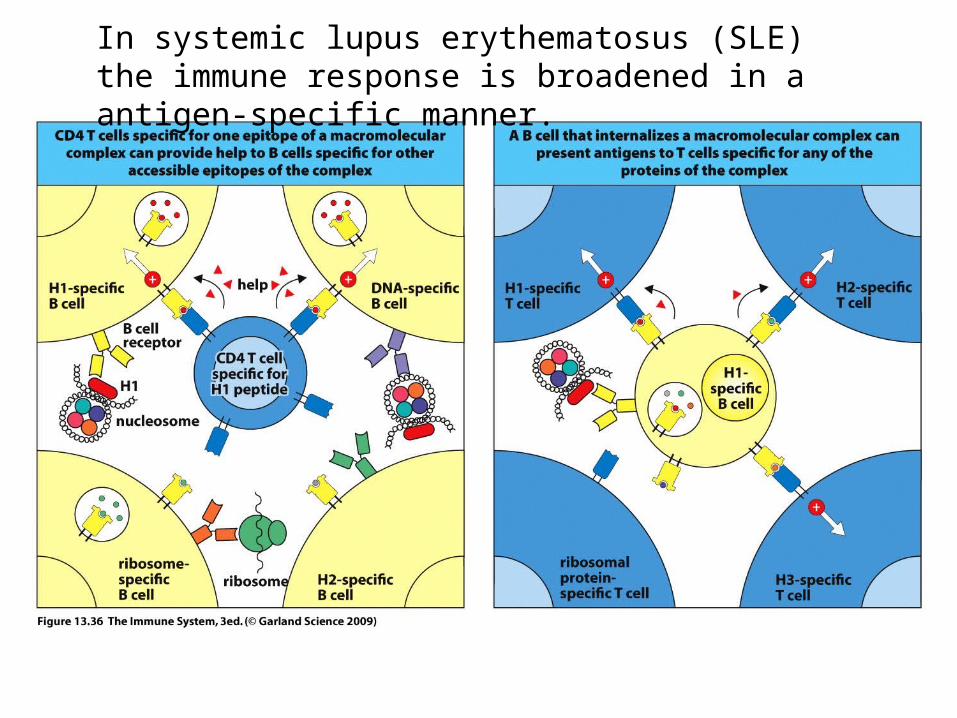
In systemic lupus erythematosus (SLE) the immune response is broadened in a antigen-specific manner.
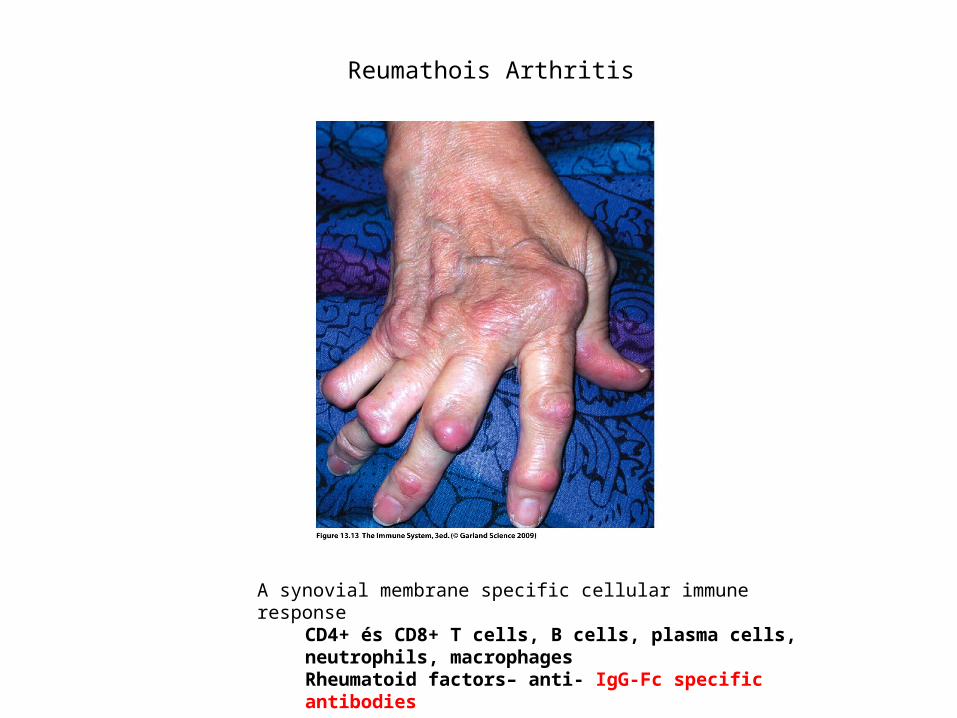
A synovial membrane specific cellular immune response CD4+ és CD8+ T cells, B cells, plasma cells, neutrophils, macrophagesRheumatoid factors– anti- IgG-Fc specific antibodies
Reumathois Arthritis
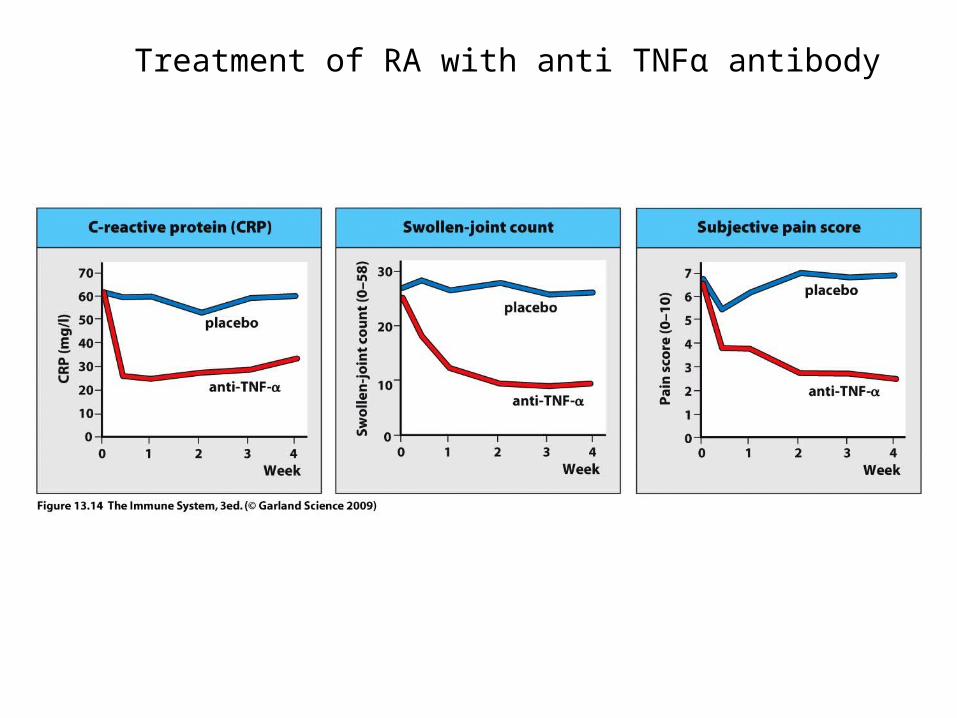
Treatment of RA with anti TNFα antibody
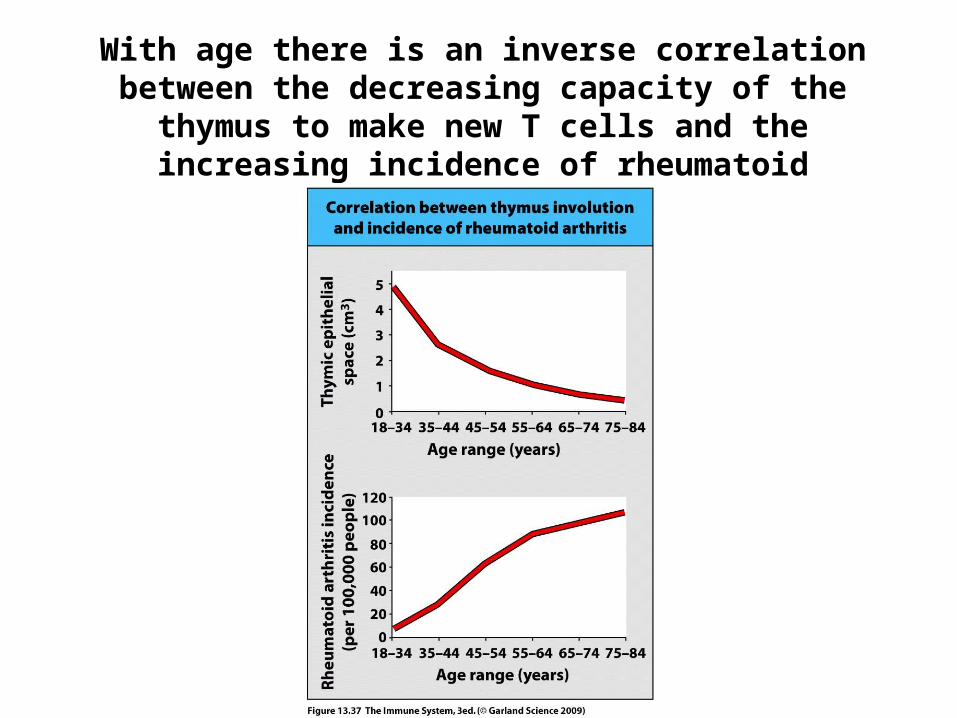
With age there is an inverse correlation between the decreasing capacity of the thymus to make new T cells and the increasing incidence of rheumatoid
arthritis.
InsulinInsulin
cell cell cell cell cell cell
PPaancreatic islet cellsncreatic islet cells
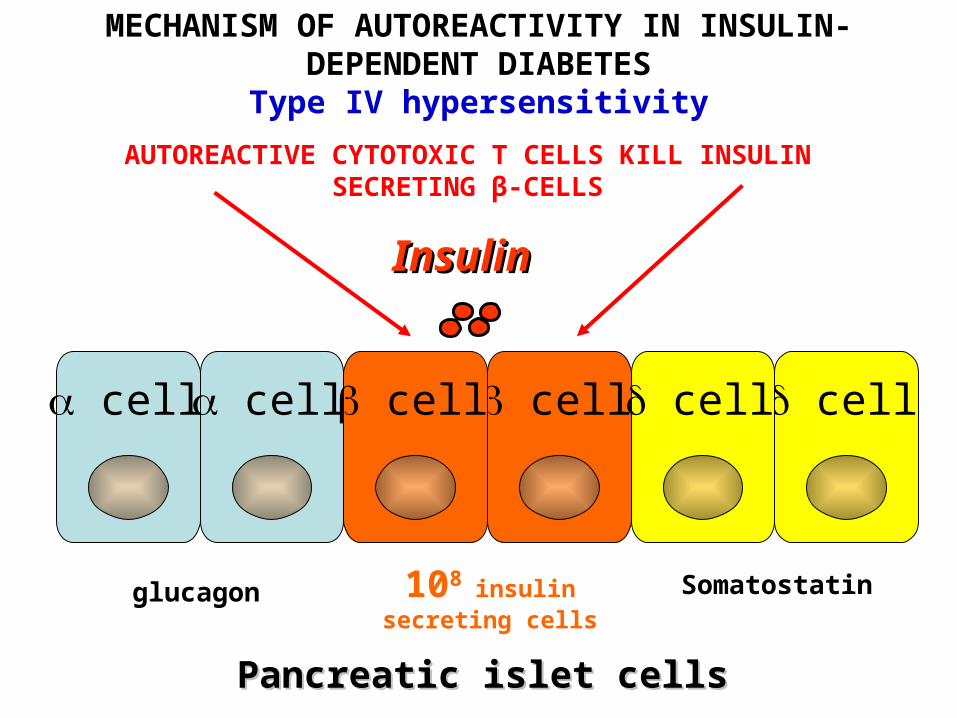
MECHANISM OF AUTOREACTIVITY IN INSULIN-DEPENDENT DIABETESType IV hypersensitivity
AUTOREACTIVE CYTOTOXIC T CELLS KILL INSULIN SECRETING β-CELLS
glucagon Somatostatin108 insulin secreting cells
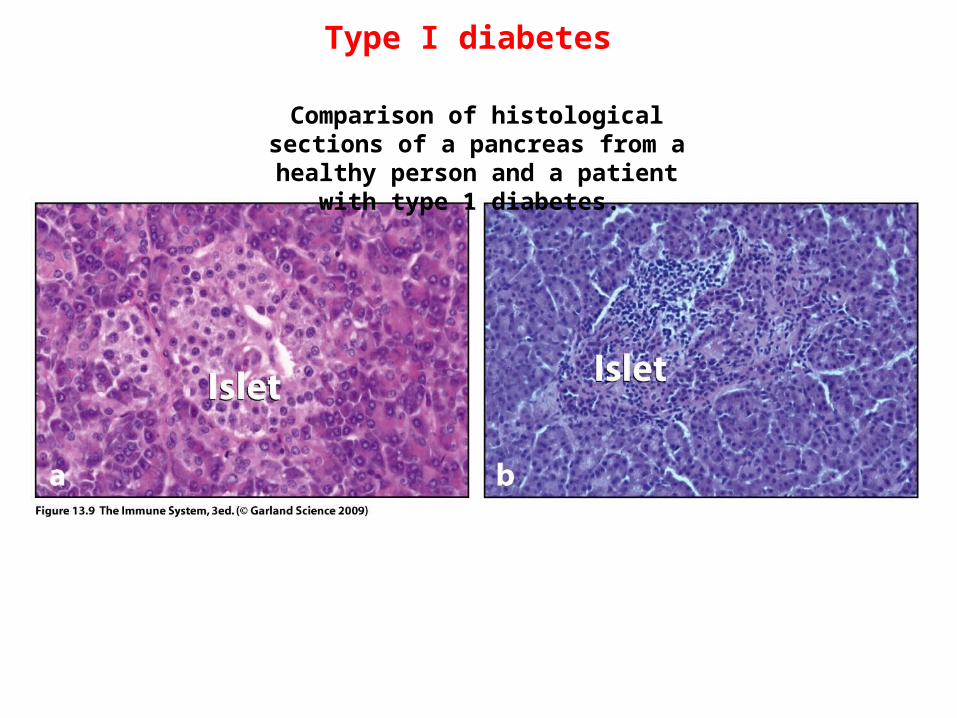
Type I diabetes
Comparison of histological sections of a pancreas from a healthy person and a
patient with type 1 diabetes.
FACTORS INVOLVED IN THE PATHOMECHANISM
OF AUTOIMMUNE DISEASES
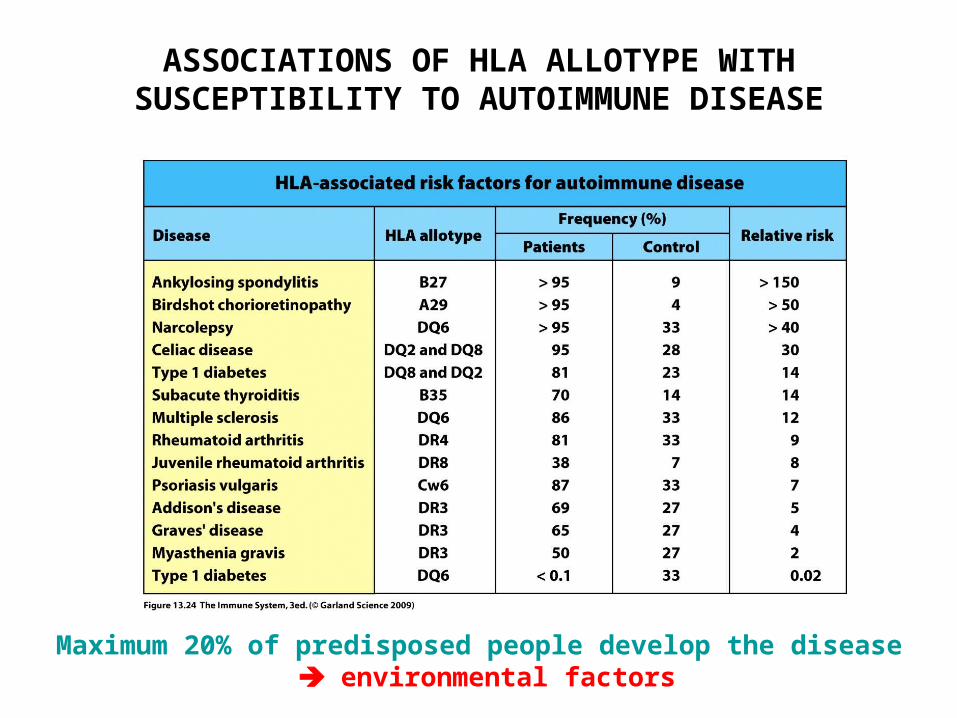
ASSOCIATIONS OF HLA ALLOTYPE WITH SUSCEPTIBILITY TO AUTOIMMUNE DISEASE
Maximum 20% of predisposed people develop the disease environmental factors
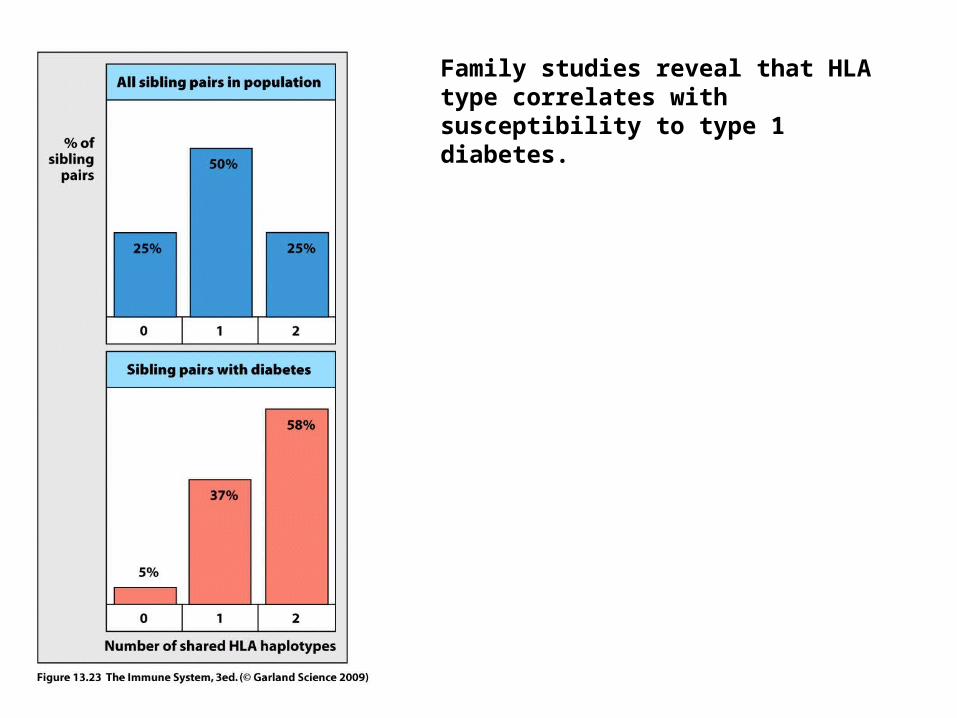
Family studies reveal that HLA type correlates with susceptibility to type 1 diabetes.
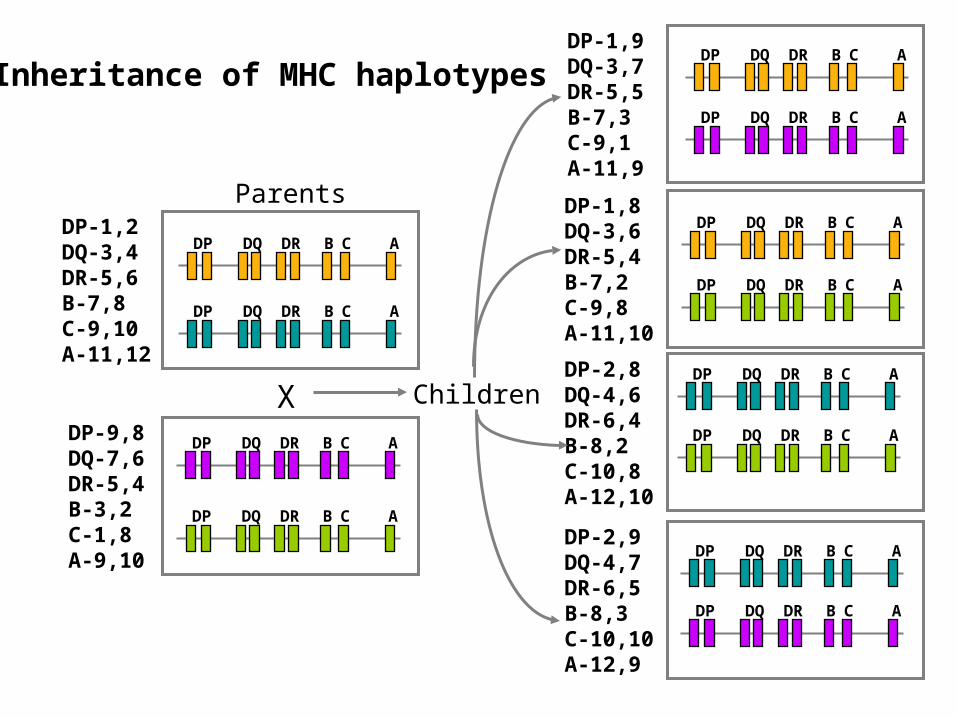
Inheritance of MHC haplotypes
B C ADP DQ DR
B C ADP DQ DR
B C ADP DQ DR
B C ADP DQ DR
X
ParentsDP-1,2DQ-3,4DR-5,6B-7,8C-9,10A-11,12
DP-9,8DQ-7,6DR-5,4B-3,2C-1,8A-9,10
DP-1,8DQ-3,6DR-5,4B-7,2C-9,8A-11,10
DP-1,9DQ-3,7DR-5,5B-7,3C-9,1A-11,9
DP-2,8DQ-4,6DR-6,4B-8,2C-10,8A-12,10
DP-2,9DQ-4,7DR-6,5B-8,3C-10,10A-12,9
B C ADP DQ DR
B C ADP DQ DR
B C ADP DQ DR
B C ADP DQ DR
B C ADP DQ DR
B C ADP DQ DR
B C ADP DQ DR
B C ADP DQ DR
Children
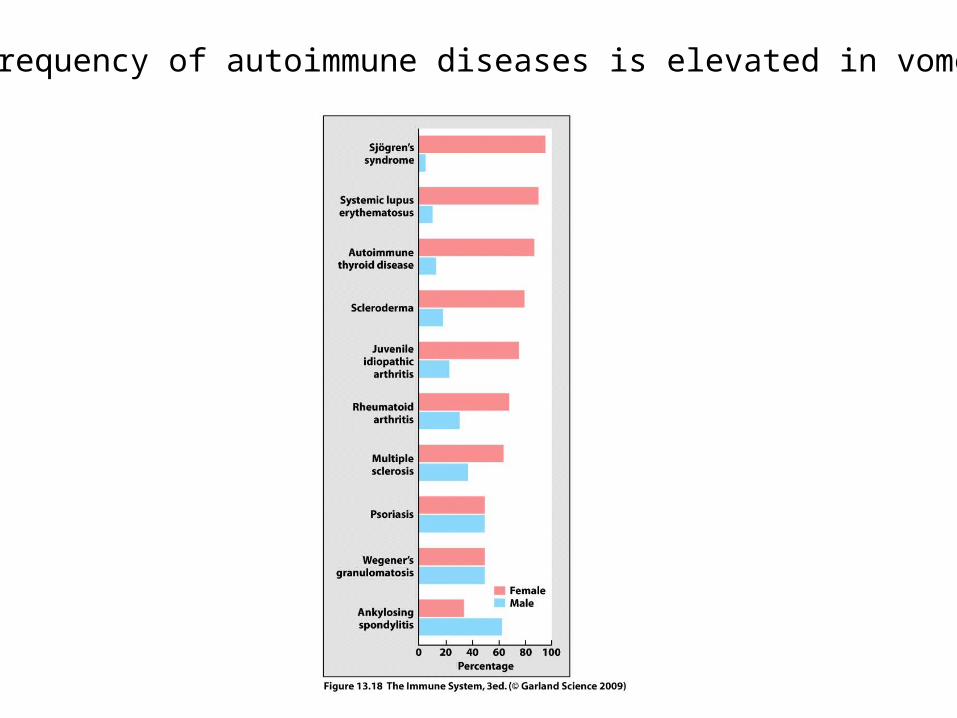
Frequency of autoimmune diseases is elevated in vomen