Embed Size (px)
Citation preview

Atypical mycobacteria keratitis after laser in situkeratomileusis unresponsive to fourth-generation
fluoroquinolone therapyJose de la Cruz, MD, Irmgard Behlau, MD, Roberto Pineda, MD
We report a case of post-laser in situ keratomileusis atypical mycobacteria infection unresponsiveand resistant to fourth-generation fluoroquinolones, which highlights the importance of a highlevel of suspicion and the need for multidrug therapy for effective eradication.
J Cataract Refract Surg 2007; 33:1318–1321 Q 2007 ASCRS and ESCRS
CASE REPORT
Atypical mycobacteria infections have frequently beenassociatedwith interface keratitis after laser in situ ker-atomileusis (LASIK). The typical course of infectionhas been delayed onset and response to antimicrobialmonotherapy. In recent years, there has been a de-crease in the incidence of atypical mycobacteria infec-tions after LASIK. Several reasons have been proposedfor the decrease, which is probably multifactorial.One intervention can be improved: sterilization ofequipment with mandatory spore testing. Anotherpossible reason for the decrease is the introduction ofbroad-spectrum fourth-generation fluoroquinolones(8-methoxyfluoroquinolone), which have good activ-ity against atypical mycobacteria; they are widelyused for perioperative prophylaxis for LASIK andused empirically to treat LASIK-associated infections.
Accepted for publication March 8, 2007.
From the Cornea and Refractive Surgery Service (de la Cruz, Pineda)and the Infectious Disease Service (Behlau), Department ofOphthalmology, Massachusetts Eye and Ear Infirmary, HarvardMedical School, Boston, Massachusetts, USA.
No author has a financial or proprietary interest in any material ormethod mentioned.
Alexander Sloutsky, PhD, Director, Mycobacteriology Laboratory,Massachusetts Department of Public Health, Jamaica Plain, Massa-chusetts, and The University of Texas Health Center, Department ofMicrobiology, Mycobacteria/Nocardia Research Lab, Tyler, Texas,performed the microbiological studies.
Corresponding author: Roberto Pineda MD, Director, RefractiveSurgery Service, Department of Ophthalmology, MassachusettsEye and Ear Infirmary, Harvard Medical School, 243 Charles Street,Boston, Massachusetts 02114, USA. E-mail: [email protected].
Q 2007 ASCRS and ESCRS
Published by Elsevier Inc.
1318
We report a case of post-LASIK atypical mycobacteriainfection unresponsive and resistant to fourth-genera-tion fluoroquinolones. The case illustrates the impor-tance of a high level of suspicion and the need formultidrug therapy for effective eradication.
CASE REPORT
A 25-year-old man had bilateral myopic LASIK in 2004. Oneyear after surgery, he experienced regression (�1.25 diopters[D] sphere) in the right eye and requested an enhancement. ALASIK retreatment was performed in the right eye, resultingin uncorrected visual acuity (UCVA) of 20/15. Topical com-mercial gatifloxacin (Zymar) 4 times daily was used as post-operative prophylaxis.
Approximately 2 weeks following the enhancement, thepatient began to experience a foreign-body sensation inthe right eye, without a significant change in vision. Threedays later, due to the lingering symptoms, he was seen bythe refractive surgeon, who noted a 3.0 mm intralamellarinfiltrate with significant hyperemia. The LASIK flap waslifted, the intrastromal bed was scraped for cultures, andthe interface was irrigated with balanced salt solutionand commercial gatifloxacin before the flap was reposi-tioned. Gatifloxacin every 2 hours and ciprofloxacin oint-ment at bedtime was begun. There appeared to be aninitial improvement of the infiltrate 3 days after the flapwas lifted, but then indolent-appearing diffuse lamellar ker-atitis developed. Topical prednisolone acetate was added,with a transiently improved interface haze that worsenedwith redevelopment of the infiltrate. The UCVAdeterioratedto 20/400, with progressive pain and photophobia. Due tothe deteriorating clinical course, the flap was relifted, recul-tured, and the intrastromal bed was reirrigated with com-mercial gatifloxacin.
One day postoperatively, positive growth for atypical my-cobacteria from the initial cultures was reported. Topicalamikacin every 2 hours was added to gatifloxacin, and top-ical corticosteroids were terminated. The density of the infil-trate decreased initially with this change in medicalmanagement, but eventually deteriorated, with a diffuse‘‘cracked-windshield’’ pattern of infiltrate throughout thecornea.
0886-3350/07/$dsee front matter
doi:10.1016/j.jcrs.2007.03.035

1319CASE REPORT: MYCOBACTERIA KERATITIS AFTER LASIK
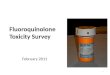
Three weeks after the onset of symptoms, the patient wasreferred to the Cornea and Refractive Surgery Service at theMassachusetts Eye and Ear Infirmary for evaluation andmanagement. Examination revealed counting finger visionin the right eye, diffuse intrastromal haze with stromal melt-ing, and multiple infiltrates involving the visual axis witha cracked-windshield appearance (Figure 1). Because thiswas known to be an atypical mycobacterial infection andprogression with penetration of the flap by the infiltrate,the LASIK flap was lifted and amputated. The rationale forflap amputation was to lower the bacterial load, remove ne-crotic as well as infected tissue, and permit better antibioticpenetration. During the flap amputation, the stromal bedwas soaked in gatifloxacin 0.3% solution for 5 minutes. Thetherapy was changed to topical clarithromycin every houralternating with moxifloxacin (Vigamox). The tissue speci-men was cultured and grew abundant atypical mycobacte-ria, identified as Mycobacterium chelonae (Figure 2) bypolymerase chain reaction-specific probe (data not shown).The patient’s course improved markedly after the above in-tervention, with reduced haze, resolving epithelial defect,and a best corrected visual acuity of 20/50 with a C5.0 Dcontact lens 3 weeks after flap amputation. Susceptibilitytesting to M chelonae reported 3 weeks later showed initialintermediate resistance to gatifloxacin but on repeated sus-ceptibility testing, showed complete resistant to gatifloxacinand also moxifloxacin.
DISCUSSION
Atypical mycobacteria (Mycobacterium fortuitum) wasfirst identified as a human pathogen in 1938 froma cold abscess in a Brazilian woman.1 The first ocularinfection caused by atypical mycobacteria, also identi-fied as M fortuitum, was reported in 1965 and wasassociated with a corneal foreign body.2
With the advent of LASIK, reports of atypical myco-bacteria keratitis increased significantly until the lastsurvey of members of the American Society of Cata-ract and Refractive Surgery in 2005, when there was
Figure 1. Slitlamp image showing the cracked-windshield appear-ance of the stromal infiltrate.
J CATARACT REFRACT SU
a dramatic decrease in the number of reported casesafter LASIK (E.D. Donnenfeld,MD, ‘‘Report on Surveyby ASCRS on Infectious Keratitis After LASIK,’’ pre-sented at the World Cornea Congress V, Washington,DC, USA, April 2005). One possible reason forthe decline is the introduction of fourth-generationfluoroquinolones, which have improved susceptibilitycompared with second- and third-generation fluoro-quinolones.3–6
Most ocular infections caused by mycobacteria(nontuberculous) are from the atypical mycobacteriagroup. Four of the 6 mycobacteria that have been in-volved in LASIK infections are rapid growers,M chelo-nae and M fortuitum (both Runyon type IV) being the2 most common.7 In contrast to the acute or subacuteonset of symptoms generally seen with bacteria andfungi, respectively, rapid growing atypical mycobac-teria may present with a slower onset of clinical dis-ease (3 to 14 weeks) after LASIK surgery. Sincenearly all reported cases of atypical mycobacterial ker-atitis have antecedent physical trauma, surgery, orcontact lens use, a breakdown in natural host defensesappears to be an important factor in the pathogenesisof corneal disease. Infection results in multiple foci ofdisease at various levels within the corneal stroma.The presence of organisms stimulates a mixed acuteand chronic inflammatory response. The developmentof granulomatous inflammation performs a valuablerole in preventing the spread of atypical mycobacterialkeratitis and clearing mycobacteria from infected tis-sue. It has been postulated that suppression of granu-lomatous inflammation by topical corticosteroids mayaccount for the severe and prolonged keratitis.8
In cases of identified mycobacteria infection, there isconsiderable benefit from combination antibiotic use
Figure 2. Ziehl-Neelsen stain of amputated flap tissue showingabundant acid-fast bacilli.
RG - VOL 33, JULY 2007

1320 CASE REPORT: MYCOBACTERIA KERATITIS AFTER LASIK
since atypical mycobacteria have a slower growth ratethan other bacteria and may become resistant to a sin-gle antibiotic class during the course of extended treat-ment. For this reason, the use of 2 or even 3 antibioticagents is recommended for atypical myobacteriakeratitis to reduce the possibility of resistance duringthe treatment period.9–11 Amikacin sulfate is themost frequently used agent.10,11 Clarithromycin (10to 40 mg/mL), a macrolide antibiotic, is reported tohave better penetration through intact epithelium12
and is recommended as initial therapy by Fordet al.13 in their study of antibiotic therapy against my-cobacteria. However, in other studies, clarithromycinis reported to have a poor response despite better pen-etration and improved corneal concentrations.14–16
Most important, resistance is an emerging problemwith these antimicrobial agents; up to 60% of atypicalmycobacteria are unresponsive to amikacin anda higher percentage is reported to be unresponsive tociprofloxacin.13 In the study by Ford et al.,13 a seriesof 24 cases of atypical mycobacteria in South Floridashowed that these organisms were sensitive to amika-cin and clarithromycin but resistant to second- andthird-generation fluoroquinolones. Other studieswith rabbit models have shown no significant differ-ences between treatment groups.17
The introduction of fourth-generation fluoroquino-lones provides an additional agent against rapidlygrowing mycobacteria.18 In vitro studies of the mini-mum inhibitory concentration (MIC) at which 90% ofisolates were inhibited with the use of fourth-genera-tion fluoroquinolones showed they are effectiveagainst atypical mycobacteria.7,19–21 Fluoroquinoloneantibiotics are concentration-dependent killers, requir-ing theMIC to be reached to be effective. Furthermore,the molecular structures of moxifloxacin and gatiflox-acin have a greater binding affinity for 2 of the en-zymes necessary for bacterial deoxyribonucleic acidsynthesis (deoxyribonucleic acid gyrase [also calledtopoisomerase II] and topoisomerase IV) in bothgram-negative and gram-positive microorganisms.The older fluoroquinolones adequately inhibit deoxy-ribonucleic acid gyrase in gram-negative organismsbut are not as effective as fourth-generation agents ininhibiting topoisomerase IV in gram-positive organ-isms.3 The improved effectiveness of fourth-generation fluoroquinolones is reportedly due to theirsuperior bactericidal activity, higher corneal concen-tration, and better resistance pattern.5
Note that the study results cited are from in vitrotesting and have not been replicated in vivo. Thiscase reports the emergence of a fourth-generation-fluoroquinolone–resistant atypical mycobacteriapost-LASIK surgery. Combined with other recent re-ports (Hofling-Lima et al.22 and Freitas et al.23), our
J CATARACT REFRACT S
report may herald an emerging ominous trend offourth-generation fluoroquinolone resistance. Factorsthat may contribute to the emergence of this resistanceare their increasingly widespread use and, specifically,their extensive use perioperatively in LASIK and otherophthalmic surgeries.
In our institution, there was another case of a patientstatus post-penetrating keratoplasty on chronic sup-pressive therapy with fourth-generation fluoroquino-lone who presented with similar emergence ofresistance to all antibiotics except amikacin and clari-thromycin (unpublished data). Because of the diffi-culty of treating mycobacteria infections and theextent of the disease, a combined medical and surgicalapproach was taken. The flap amputation, which re-duced the bacterial burden and allowed betterpenetration, along with effective multiple antibiotictherapy were the keys to successful treatment of thisinfection. The development of resistance to fourth-generation fluoroquinolones in M chelonae under-scores the importance of multiple antibiotic therapy.Therefore, the refractive surgeon must maintaina high level of suspicion despite coverage withfourth-generation fluoroquinolones after refractivesurgery procedures.
We suspect, as does the author of the report fromBrazil,22,23 that we will see more fourth-generationfluoroquinolone resistance in atypical mycobacteriawith the widespread use of fluoroquinolones inophthalmic procedures. We suggest initial combinedantibiotic therapy that includes at least 2 of the 3most susceptible agents (clarithromycin, amikacin, andfourth-generation fluoroquinolones) for rapidly grow-ing mycobacteria. In addition, susceptibility testingshould be done at laboratories with mycobacteria ex-pertise. Most important, when there is ongoing infec-tion in the face of empiric therapy, the surgeon needsto suspect drug resistance and apply aggressive surgi-cal intervention to halt and cure slow but often severeatypical mycobacteria ocular infections.
REFERENCES1. Cruz JC. Mycobacterium fortuitum un nuovo bacillo acido-resis-
tente patogenico para o homem. Acta Med Rio de Janeiro 1938;
1:297–301
2. Turner L, Stinson I. Mycobacterium fortuitum as a cause of cor-
neal ulcer. Am J Ophthalmol 1965; 60:329–331
3. Schlech BA, Alfonso E. Overview of the potency of moxifloxacin
ophthalmic solution 0.5% (VIGAMOX�). Surv Ophthalmol 2005;
50(suppl):S7–S15
4. Mather R, Karenchak L, Romanowski EG, Kowalski RP. Fourth
generation fluoroquinolones: new weapons in the arsenal of oph-
thalmic antibiotics. Am J Ophthalmol 2002; 133:463–466
5. Hamam RN, Noureddin B, Salti H, et al. Recalcitrant post-LASIK
Mycobacterium chelonae keratitis eradicated after the use of
fourth-generation fluoroquinolones. Ophthalmology 2006;
113:950–954
URG - VOL 33, JULY 2007

1321CASE REPORT: MYCOBACTERIA KERATITIS AFTER LASIK
6. Brown-Elliott BA, Wallace RJ Jr, Crist CJ, et al. Comparison of in
vitro activities of gatifloxacin and ciprofloxacin against four taxa
of rapidly growing mycobacteria. Antimicrob Agents Chemother
2002; 46:3283–3285
7. John T, Velotta E. Nontuberculous (atypical) mycobacterial ker-
atitis after LASIK; current status and clinical implications. Cornea
2005; 24:245–255
8. O’Brien TP, Matoba AY. Nontuberculous mycobacterial dis-
eases. In: Pepose JS, Holland GN, Wilhelmus KR, eds, Ocular
Infection & Immunity. St. Louis, MO, Mosby, 1996; 1033–1041
9. Daines BS, Vroman DT, Sandoval H, et al. Rapid diagnosis and
treatment of mycobacterial keratitis after laser in situ keratomi-
leusis. J Cataract Refract Surg 2003; 29:1014–1018
10. Bullington RH Jr, Lanier JD, Font RL. Nontuberculous mycobac-
teria keratitis; report of two cases and review of the literature.
Arch Ophthalmol 1992; 110:519–524
11. Dalovisio JR, Pankey GA. In vitro susceptibility of Mycobacte-
rium fortuitum and Mycobacterium chelonei to amikacin. J Infect
Dis 1978; 137:318–321
12. Gross RH, Holland GN, Elias SJ, Tuz R. Corneal pharmacoki-
netics of topical clarithromycin. Invest Ophthalmol Vis Sci
1995; 36:965–968
13. Ford JG, Huang AJW, Pflugfelder SC, et al. Nontuberculous
mycobacterial keratitis in south Florida. Ophthalmology 1998;
105:1652–1658
14. Chung MS, Goldstein MH, Driebe WT Jr, Schwartz B. Myco-
bacteria chelonae keratitis after laser in situ keratomileusis suc-
cessfully treated with medical therapy and flap removal. Am. J
Ophthalmol 2000; 129:382–384
15. Solomon A, Karp CL, Miller D, et al. Mycobacteria interface ker-
atitis after laser in situ keratomileusis. Ophthalmology 2001;
108:2201–2208
16. Fulcher SFA, Fader RC, Rosa RH Jr, Holmes GP. Delayed onset
mycobacterial keratitis after LASIK. Cornea 2002; 21:546–554
J CATARACT REFRACT
17. Hu F-R, Luh K-T. Topical ciprofloxacin for treating nontubercu-
lous mycobacterial keratitis. Ophthalmology 1998; 105:269–
272
18. Khardori N, Nguyen H, Rosenbaum B, et al. In vitro susceptibil-
ities of rapidly growing mycobacteria to newer antimicrobial
agents. Antimicrob Agents Chemother 1994; 38:134–137
19. Leibowitz HM. Clinical evaluation of ciprofloxacin 0.3% ophthal-
mic solution for treatment of bacterial keratitis. Am J Ophthalmol
1991; 112(suppl):34S–47S
20. Hwang DG, Biswell R. Ciprofloxacin therapy of Mycobacteria
chelonae keratitis [letter]. Am J Ophthalmol 1993; 115:114–
115
21. Abshire R, Cockrum P, Crider J, Schlech B. Topical antibacterial
therapy for mycobacterial keratitis: potential for surgical prophy-
laxis treatment. Clin Ther 2004; 26:191–196
22. Hofling-Lima AL, de Freitas D, Mello Sampaio L, et al. In vitro
activity of fluoroquinolones against Mycobacterium abscessus
and Mycobacterium chelonae causing infectious keratitis after
LASIK in Brazil. Cornea 2005; 24:730–734
23. Freitas D, Alvarenga L, Sampaio J, et al. An outbreak of Myco-
bacterium chelonae infection keratitis after LASIK. Ophthalmol-
ogy 2003; 110:276–285
First author:Jose de la Cruz, MD
Cornea and Refractive Surgery Service,Department of Ophthalmology,Massachusetts Eye and Ear Infirmary,Harvard Medical School, Boston,Massachusetts, USA
SURG - VOL 33, JULY 2007



![Final Rule: Lost Securityholders and Unresponsive Payees · [Release No. 34-68668; File No. S7-11-11] RIN: 3235-AL11 . Lost Securityholders and Unresponsive Payees . AGENCY: Securities](https://img.pdfslide.us/doc/110x75/5f0815c27e708231d420429c/final-rule-lost-securityholders-and-unresponsive-payees-release-no-34-68668.jpg)