Embed Size (px)
Citation preview

Atypical hemolytic uremic
syndrome
Prof. Dr. med. Lars Pape

Definition HUS:
hemolytic anemia
Thrombocytopenia
acute renal failure

• main cause of acute renal failure in children
• Incidence 1 – 2 / 100 000 children
• highest incidence in Argentinia
• 90 % by Shigatoxin producing E.coli (EHEC)
• 10 % „atypical“ HUS

Thrombotic Microangiopathies1. Infection
a. Shiga-Toxin producing bacteria(EHEC, Shigellen, Citrobacter) = STEC-HUS
b. Strep. pneumoniae
2. Dises of the complement system (and others) = aHUSa. genetic causeb. caused by antibodies
3. ADAMTS13 deficiency = TTPa. Genetic causeb. Caused by antibodies
4. others (HELPP, post-Tx, iduced by medication...)

The complement system: always on, strongly amplified, dependent on natural regulators
The complement system is a vital component of the natural (innate) protective immune systemComplement is activated by three mechanisms (classical, alternative and lectin) which allow the system to respond to inflammatory, infectious, ischaemic and necrotic insult, as well as foreign and self-antigens•Always ‘on’ to allow rapid immune response
– Rapid amplification leads to powerful and destructive immune reactions
– Natural inhibitors of complement keep amplification in check and prevent uncontrolled complement activation

Factors that amplify complement activation
Infection Surgery
Autoimmune Pregnancy


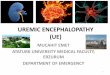
Ongoing research in the field of complement inhibitors• Most genetic mutations have been discovered in the past 20 years• 30–50% of patients with aHUS have no identifiable genetic mutation
Link with low C3
Homozygous CFH deficiency
CFI mutations
C3mutations
Link with RCA –CFH mutations
(SCR20) Thrombomodulin mutations
Hybrid (CFH-CFHRI)
Heterozygous CFH deficiency
Association with low CFH
MCPmutations
Anti-FH auto-antibodies
Homozygous MCP deficiency
CFB mutations
1973 1981 1994 1998 2003 2004 2005 2006 2007 2009
DCFHR1 / DCFHR3 deletion

Noris & Remuzzi, NEJM 2009
aHUS

AnaphylaxisInflammationThrombosis
ConsequencesCell destruction
InflammationThrombosis
Consequences
Prox
imal
Term
inal
Lectin pathway Classical pathway Alternative pathway
Immune complex clearanceMicrobial opsonisation
C3a
iC3b
C3
C3bWeak anaphylatoxin
C3 + H2O: always active (chronic)Amplification
Gain of Function Mutations: C3, CFB
+
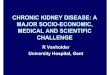
Chronic uncontrolled complement activation leads to devastating consequences in aHUS
C5a
Potent anaphylatoxin Chemotaxis Proinflammatory Leukocyte activation Endothelial activation Prothrombotic
C5b-9Membrane attack complex
Cell lysis Proinflammatory Platelet activation Leukocyte activation Endothelial activation Prothrombotic
C5C5b
C6C7
C8C9
C5-convertase
Natural Inhibitors: Factor H, I, MCP
Thrombomodulin

Endothelial cells: - Activation - Swelling and disruption
Platelets:- Activation- Aggregation
Leukocytes:- Activation
Platelet consumptionMechanical haemolysis
Blood clotting Vessel occlusion
InflammationIschaemia
Systemic multi-organ complications
Clinical consequences:
Red cells:-Haemolysis
Uncontrolledcomplement
activation on cells
Chronic uncontrolled complement activation leads to endothelial and end organ damage

aHUS
aHUS is asystemic disease !
• Kidney
• CNS
• Lung
• Heart
• Vessels

Plus one or more of the following:
Differential diagnosis for TMAs: aHUS, TTP and STEC-HUS
Evaluate ADAMTS13 activity and Shiga-toxin / EHEC test
ThrombocytopeniaPlatelet count <150,000 or
>25% decrease from baseline
Renal impairmentElevated creatinineand / orDecreased eGFR and / or
Elevated blood pressure and / or Abnormal urinalysis
Neurological symptomsConfusion and / orSeizures and / or
Other cerebral abnormalities
Gastrointestinal symptomsDiarrhoea +/– blood and / or Nausea / vomiting and / or
Abdominal pain and / orGastroenteritis
Microangiopathic haemolysisSchistocytes and / orElevated LDH and / or
Decreased haptoglobin and / orDecreased haemoglobin
AND


Serum creatinine level ≤200 µmol/L or platelet count ≤30×109/L had the stronger association with a severe ADAMTS13 deficiency
Patient characteristicsADAMTS13
Deficiency group (n=160)
ADAMTS13Detectable group
(n=54)p value
Platelet count, ×109/L 17.4 (14.2) 66.6 (49.3) <0.0001Creatinine level, µmol/L
mg/dL114 (68.4)1.29 (0.77)
454 (326)5.13 (3.68)
<0.0001
Patient characteristics Adjustedodds ratio 95% CI p value
Platelet count ≤30×109/L 23.4 3.4–24.2 <0.001Creatinine level ≤200 µmol/L(2.26 mg/dL) 9.1 8.8–62.5 <0.001
Creatinine and platelet count can support a differential diagnosis of aHUS

First diagnostic steps
Hb, LDH, freee Hb, PLT, Haptoglobine, FragmentocytesGOT, GPT, GlDH
Creatinine, BUN, Cystatine C
Renal Ultrasound (RI 1) !
Eventually: EEG / CCT

Exclusion TTP




Terminal complement complex
Faktor H, B, I
Faktor-H antibodies
Status of complemet system


PE / PI is not associated with positive long-term outcomes regardless of mutation
Affected protein Short-term outcome to PE / PI*
Factor H 60%
CFHR1, R3 70–80%
MCP No definitive indication for therapy
Factor I 30–40%
Factor B 30%
C3 40–50%
THBD 60%
Long-term outcome to PE / PI*
Death or ESRD: 70–80%
ESRD: 30–40%
Death or ESRD: <20%
Death or ESRD: 60–70%
Death or ESRD: 70%
Death or ESRD: 60%
Death or ESRD: 60%

Eculizumab blocks terminal complement
C5
Prox
imal
Term
inal C5a
Eculizumab
• Proximal functions of complement remain intact– Weak anaphylatoxin– Immune complex clearance– Microbial opsonisation
• Terminal complement –C5a and C5b-9 formation blocked
• Eculizumab binds with high affinity to C5
Complement cascade
C5b-9C5b
C3 C3a
C3b

Rapid and Sustained Improvement in Platelet Count under Eculizumab
164 x 109/L: Mean Change from Baseline in Platelets at Week 27
*P<0.0001
0
25
50
75
100
125
150
175
200
225
250
275
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Plat
elet
Mea
n C
hang
e fr
om B
asel
ine
Weeks
**
*
* **
**
* *
Plat
elet
Cha
nge
from
Bas
elin
e†(x
109 /L
)
Study Week

Significant and Continued Improvement in eGFR under Eculizumab
64 mL/min/1.73m2: Mean Change from Baseline in eGFR at Week 27
-15
5
25
45
65
85
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
eGFR
Cha
nge
from
Bas
elin
e†(m
L/m
in/1
.73m
2 )
*
** *
*
**
*
*
Study Week
*P<0.001#P<0.05#

82% of Patients Eliminated Dialysis under Eculizumab
% Discontinued Dialysis
Patients Not on Dialysis at Baseline:
Of the 11 patients not on dialysis at baseline, all patients (100%) remained dialysis-free through the end of the study evaluation period
9/11
Patients on Dialysis at Baseline

Adverse Event Findings
C10-003 (N=22) AEs occurring in ≥20% n (%)
Pyrexia 11 (50)
Cough 8 (36)
Abdominal pain 7 (32)
Diarrhea 7 (32)
Upper respiratory tract infection 7 (32)
Vomiting 6 (27)
Nasopharyngitis 6 (27)
• Most AEs were mild or moderate• No meningococcal infections in this
trial• One patient was noted to have low
positive values for neutralizing antibodies to eculizumab
– Overall, there had been no observed correlation of antibody development to clinical response or adverse events
• No new safety concerns• No deaths

aHUS caused by factor H antibodies• an immunsuppressive therapy with Steroids, Mycophenolatmofetile
and/or Rituximab can be tried.• Cave: Rituximab can not be administered in parallel with Eculizumab,
because Eculizumab inhbits the complement need for destruction of B-cells
• In case of negative factor H ab after immunosuppressive tretament Eculizumab may be discontinued.
• After transplantation mosty no recidives under maintanance immunosuppression, therefore no long-term Eculizumab therapy needed.
• Factor H-antibodies can develop, if in patients with factor H-deficieny or mutation, factor-H is regularily administered by plasma infusion or plasmaexchange therapy.




What to do initially?• If differential diagnosis is unclear, immediate start of plasma-exchange
therapy as this is therapy of choice in TTP.• In children with clear diagnosis of aHUS immediate treatment with
Eculizumab• If the diagnosis of TMA is unclear: renal biopsy• After exclusion of TTP and typical HUS: immediate administration of
Eculizumab• If there is a massive complement activation in complement diagnostics
(i.e. highly elevated terminal complement complex): immediate treatment with Eculizumab
• If anti-Factor H Ab are diagnosed: Switch from Eculizumab to intensive immunosuppressive treatment