Embed Size (px)
Citation preview

Fax +41 61 306 12 34E-Mail [email protected]
Acta Cytologica 2011;55:526–530 DOI: 10.1159/000333227
Atypical Follicular Cells with Equivocal Features of Papillary Thyroid Carcinoma Is Not a Low-Risk Cytologic Diagnosis
Martin H. Luu a Andrew H. Fischer a Thomas J. Stockl a Latha Pisharodi b
Christopher L. Owens a
a Department of Pathology, University of Massachusetts Memorial Medical Center, Worcester, Mass. , and b Department of Pathology, Rhode Island Hospital, and Warren Alpert Medical School of Brown University, Providence, R.I. , USA
tion and 33 having confirmed malignancies. Atypical follicu-lar cells, cannot exclude PTC, have a significantly higher risk of malignancy than atypical follicular cells, other patterns (45.8 vs. 13.9%, p ! 0.01). Conclusions: Atypical follicular cells with equivocal features of papillary carcinoma is not a low-risk cytologic diagnosis. Copyright © 2011 S. Karger AG, Basel
Introduction
The proposed Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) is intended to standardize re-porting terminology by offering specific cytologic cate-gories [1] . The acceptance of a universal terminology for thyroid fine-needle aspiration (T-FNA) reporting will improve the communication and knowledge of the risk of malignancy of each category and optimize rational man-agement decisions [2–4] . In order to maintain the sensi-tivity of T-FNA TBSRTC described categories including
Key Words
Thyroid cytology � Bethesda System for Reporting Thyroid Cytopathology � Atypical follicular cells
Abstract
Objective: To determine whether or not significant differ-ences in the risk of malignancy exist between subgroups of atypical follicular cells in The Bethesda System for Reporting Thyroid Cytology (TBSRTC) in patients who underwent surgi-cal resection. Study Design: Between 2004 and 2009, con-secutive thyroid fine-needle aspirates at our institutions with a cytologic diagnosis of ‘atypical follicular cells’ were retrieved and subclassified using the diagnosis and diagnos-tic comment as: (1) atypical follicular cells with equivocal fea-tures of papillary carcinoma [cannot exclude papillary thy-roid carcinoma (PTC)] and (2) atypical follicular cells, other patterns. The risks of malignancy for excised nodules were calculated and comparisons were made between these sub-groups. Categorical analysis was performed using a 2-tailed Fisher’s exact test, and p ! 0.05 was considered statistically significant. Results: A total of 7,072 thyroid fine-needle aspi-ration cases were retrieved, with 1,542 (21.8%) having a his-tologic follow-up. There were 222 (3.1%) cases of ‘atypical follicular cells’, with 127 (57.2%) having a histologic correla-
Received: May 11, 2011 Accepted: June 23, 2011 Published online: December 9, 2011
Correspondence to: Dr. Martin Luu Department of Pathology, University of Massachusetts Memorial Medical School 3 Biotech, One Innovation Dr Worcester, MA 01605 (USA) Tel. +1 508 793 6100, E-Mail martin.luu @ umassmemorial.org
© 2011 S. Karger AG, Basel0001–5547/11/0556–0526$38.00/0
Accessible online at:www.karger.com/acy
Part of this work was presented in poster format at the 2011 United States and Canadian Academy of Pathology Annual Meeting in San Antonio, Tex., USA.

Atypical Follicular Cells – Cannot Exclude PTC
Acta Cytologica 2011;55:526–530 527
‘suspicious for malignancy’, ‘suspicious/positive for fol-licular neoplasm’, and ‘atypia of undetermined signifi-cance/follicular lesion of undetermined significance’ (AUS/AFLUS or AFLUS).
The AFLUS category was created recognizing that some T-FNA are not easily classified as benign, suspi-cious, or malignant. The Bethesda authors noted that this category is heterogeneous and described 9 cytologic pat-terns that may lead to an AFLUS diagnosis. The Bethesda authors also cautioned against overuse of this category and estimate the overall risk of malignancy to be around 5–15% for this category. A recent study observed that this wide range of frequencies may account for an actual ma-lignancy risk ranging from 7 to 38% depending upon the specific pattern observed in the AFLUS aspirate and sug-gested subclassifying AFLUS to better reflect the risk of malignancy [5] . Specifically the AFLUS pattern contain-ing equivocal features of papillary carcinoma was report-ed to be of higher risk than the other common AFLUS patterns. Other studies have suggested a higher risk of atypical T-FNA with focal features of papillary thyroid carcinoma (PTC) compared to other atypical cases [6, 7] .
In this study we sought to determine the risk of malig-nancy among excised nodules following a referring cyto-logic diagnosis of AFLUS with equivocal features of PTC and to determine if it is different from the other patterns of AFLUS by analyzing consecutive T-FNA and record-ing histologic follow-up at two tertiary care centers.
Materials and Methods
This study was approved by the institutional review boards of both institutions [project No. 4006-08 at Rhode Island Hospital, and project H-10396 at the University of Massachusetts Memo-rial Medical Center (UMass)]. Computer searches were used to identify all T-FNA at Rhode Island Hospital, a tertiary care aca-demic medical center that uses ThinPrep � (Hologic Corporation, Bedford, Mass., USA) processing as a sole modality for all of its T-FNA material, and UMass, another tertiary care academic medical center that processes T-FNA material into conventional smears and ThinPrep slides. Consecutive T-FNA during the years 2004–2009 at UMass and those during the years 2005–2008 at Rhode Island Hospital were included in this retrospective study. The original cytologic diagnosis was noted to be one of the fol-lowing categories: benign, atypical follicular cells, indeterminate, suspicious for follicular neoplasm, suspicious for malignancy, positive for malignancy, or unsatisfactory.
For this study, a computer search identified T-FNA containing the word ‘atypical’ or ‘atypia’ in the line diagnosis. The diagnoses were reviewed and cases further qualified as ‘suspicious for fol-licular neoplasm’, ‘suspicious for malignancy’, or ‘suspicious for PTC’ were excluded from further analysis. Cases of AFLUS that
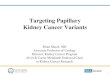
had a repeat fine-needle aspiration yielding a different cytologic diagnosis were also excluded from further considerations. The remaining atypical cases (including cases with two consecutive atypical FNAs – counted as one case) formed the AFLUS cohort and these cases were sub classified (by M.L. and C.O.) based on the diagnostic comments into two categories. The first category in-cluded cases with equivocal nuclear features of PTC (AFLUS – cannot exclude PTC) and the second category lacked nuclear fea-tures of PTC (AFLUS – other patterns). As an example of a case that we subclassified as AFLUS – cannot exclude PTC, the corre-sponding diagnostic comment was ‘atypical follicular cells – thy-roid follicular cells with focal nuclear membrane irregularities, nuclear enlargement and open chromatin, hemosiderin-laden macrophages, and dense colloid’ ( fig. 1 a). As an example of a case that we subclassified as AFLUS – other patterns, the correspond-ing diagnostic comment was ‘atypical follicular lesion – debris, macrophages, and few clusters of follicular cells with microfol-licular arrangments’ ( fig. 1 b). The risk of malignancy following a referring T-FNA with AFLUS cytodiagnosis in patients who un-derwent surgical resection was calculated and a comparison was made between the two subgroups. Categorical analysis was per-formed using a 2-tailed Fisher’s exact test, and p ! 0.05 was con-sidered statistically significant.
T-FNA biopsies at UMass were procured under ultrasound guidance by an endocrinologist or radiologist using a 22- to 25-gauge needle. Between 2 and 6 passes were performed (typi-cally 5). In the majority of cases, material from the first 2 to 4 passes was expressed on one glass slide and one alcohol-fixed smear was made. Residual material that could not be expressed was rinsed into CytoRich Red fixative (Thermo Scientific, Ka-lamazoo, Mich., USA). Typically the last one or two passes were entirely expressed into CytoRich Red fixative without making smears. In a subset of cases all passes where entirely expressed into CytoRich Red fixative. The CytoRich Red needle rinse was centrifuged, the supernatant decanted, and the pellet resuspend-ed in PreservCyt solution (Hologic). One ThinPrep slide was pre-pared and stained using the Papanicolaou technique with a Saku-ra Tissue-Tek Prism (Sakura Finetek, Torrance, Calif., USA) auto-mated stainer. If the sample was not ‘dilute’ or if 4 or more particles were evident in the PreservCyt container, a Cellient TM cell block (Hologic) was prepared.
T-FNA biopsies at Rhode Island Hospital were procured by a clinician or a radiologist via the palpation technique or with ultra-sound guidance using a small caliber needle (22–27 gauges) with suction in some cases. Multiple passes were performed (typically 5), with all material immediately rinsed into buffered fixative Cy-tolyt solution (Hologic). Specimens were centrifuged, decanted, and resuspended in Preservcyt solution, and ThinPrep slides were prepared using a ThinPrep 2000 (Hologic) automated slide pro-cessor and stained with the Papanicolaou stain using a Shandon Varistain XY (Thermo Electron Corporation, Waltham, Mass., USA) automated staining instrument. Additional centrifugation steps with resuspension in Cytolyt solution were performed for bloody specimens. Cell blocks were prepared by centrifuging and decanting residual solution to yield a cell pellet in cases with suf-ficient residual material. HistoGel (Thermo Scientific), a hydroxy-ethyl agarose processing gel, was used to suspend the cell pellet as per the manufacturer’s guidelines. The suspended cell pellet was embedded in paraffin wax, sectioned, and stained with hematoxy-lin and eosin using the standard technique.

Luu /Fischer /Stockl /Pisharodi /Owens Acta Cytologica 2011;55:526–530528
Results
A total of 7,072 T-FNA were examined during the pe-riod of 2004–2009; 1,542 (21.8%) resections were histo-logically examined and 389 (5.5%) were found to be ma-lignant. A total of 222 (3.1%) of all T-FNA were classified as AFLUS in this cohort, with 127 (57.2%) had a histo-logic correlation and 33 (26.0%) of the excised nodules had a confirmed malignancy. The patient characteristics and the distribution of the types of thyroid carcinoma among AFLUS cases having a histologic follow-up are summarized in table 1 . Among 222 AFLUS cases, 68 were subclassified as AFLUS – cannot exclude PTC, and the remaining 154 were subclassified as AFLUS – other pat-terns. Of the 68 cases subclassified as AFLUS – cannot
a b
Table 1. P atient characteristics and distribution of carcinoma types among histologically examined AFLUS cases
AFLUS subgroup M:F ratio Mean age (M/F)years
Mean nodulesize, cm
PTC(classical type), n
PTC(follicular variant), n
Follicularcarcinoma, n
AFLUS, cannot exclude PTC 1.1:1 67/60 1.8 8 14 0AFLUS, other patterns 0.9:1 55/46 2.1 3 5 3
M :F = Male to female.
Fig. 1. a Morphological features of ‘atypical follicular cells with equivocal features of papillary carcinoma’ showing two sole clus-ters of follicular cells with mild chromatin clearing and equivocal nuclear membrane irregularities. The remaining follicular cells in the aspirate (not shown) have typical benign features without other diagnostic features of papillary carcinoma. b Morphologi-
cal features of ‘atypical follicular cells, other patterns’ showing few clusters of follicular cells in microfollicular arrangements (one of these clusters is shown). No features of nuclear chromatin clearing or nuclear grooves are seen in these atypical follicular cells or in the rest of the aspirate. Papanicolaou stain. ! 400 orig-inal magnification.
Table 2. T hinPrep� compared to ThinPrep plus conventional smear in the number of cases subclassified as AFLUS cannot ex-clude PTC and AFLUS other patterns in patients who underwent surgical resection
ThinPrep + smears (n = 52)
ThinPrep(n = 16)
p
AFLUS cannot exclude PTCBenign, n 20 6 1.00Malignant, n 17 5
(n = 82) (n =72)
AFLUS other patternsBenign, n 7 4 0.52Malignant, n 33 33

Atypical Follicular Cells – Cannot Exclude PTC
Acta Cytologica 2011;55:526–530 529
exclude PTC, 48 or 70.6% were resected compared to 79 or 51.3% of the AFLUS – other patterns cases (p ! 0.01). The positive predictive value for malignancy amongexcised nodules following a cytologic diagnosis ofAFLUS – cannot exclude PTC is 45.8% compared to 13.9% for cases with the AFLUS – other patterns referring cytologic diagnosis (p ! 0.01; fig. 2 ). The ThinPrep alone and ThinPrep plus conventional smear cohorts have a similar number of cases diagnosed as AFLUS – cannot exclude PTC and AFLUS – other patterns ( table 2 ).
Discussion
Our results add to the knowledge of the AFLUS cate-gory of TBSRTC by demonstrating that among excised nodules the referring aspirates with equivocal features raising concern for PTC have a significantly higher risk of malignancy than aspirates that do not have these fea-tures. Our results confirm the heterogeneity of the AUS/AFLUS group regarding the risk of malignancy which has been noted by other investigators. The variability of risk within this category constitutes important knowl-edge for cytopathologists and clinicians.
In our practice we find aspirates within the AFLUS category to be some of the most diagnostically challeng-
ing cases. In our cohort, most of the cases of AFLUS with equivocal features of papillary carcinoma showed some chromatin clearing or nuclear irregularity and some mi-crofollicles, but had insufficient cellularity for a diagnosis of ‘suspicious for papillary thyroid carcinoma.’ Thus we are left with an atypical aspirate insufficient for a diagno-sis of ‘suspicious for follicular neoplasm’ and insufficient for a diagnosis of ‘suspicious for papillary carcinoma’ and therefore best subclassified as AFLUS with equivocal fea-tures of papillary carcinoma. Most of the cases of AFLUS with other patterns showed some microfollicular groups without significant chromatin clearing or nuclear irregu-larity and without sufficient cellularity for a diagnosis of ‘suspicious for follicular neoplasm.’ Also, within the cat-egory of AFLUS are aspirates with an overall low cellular-ity and benign nuclear features with some architectural abnormalities, such as a microfollicular predominance, that make it difficult to assign a benign diagnosis. Fol-lowing the TBSRTC guidelines both of these examples are classified into the same general category of AFLUS. For the AFLUS category in our institutions we typically include a diagnostic description that will convey our con-cern for papillary carcinoma if present, and such cases are shown to multiple cytopathologists and tend to be dis-cussed in multidisciplinary conferences. By using thisapproach we are able to classify smears according toTBSRTC and effectively communicate the risks of the common patterns of AFLUS to our clinical colleagues and thus assist as much as possible in making sound treatment decisions.
An opponent of the AFLUS category could make a rea-sonable argument to eliminate this category entirely and classify AFLUS with equivocal features of papillary car-cinoma as ‘suspicious for papillary carcinoma’ and to classify AFLUS – other patterns into either a benign cat-egory or ‘suspicious for follicular/Hürthle neoplasm’ de-pending upon the degree of suspicion. We oppose this notion because it would diminish the positive predictive value of the ‘suspicious for malignancy’ category, which in our experience is often followed by a total thyroidec-tomy. Such a strategy would also decrease the sensitivity of T-FNA, and as the Bethesda authors noted the major-ity of participants voted in favor of this category in order to maximize the sensitivity of the test.
The next logical question is how to best treat a nodule diagnosed as AFLUS with equivocal features of papillary carcinoma. We would advocate for a consideration of lo-bectomy in such a patient depending upon the clinical situation, such as an unchanged diagnosis on repeat FNA. In the current study the risk of malignancy for AFLUS
Total AFLUS cases(% of total T-FNA)
222 (3.1)
AFLUS R/O PTC(% of total AFLUS cases)
68 (30.6)
AFLUS, other patterns(% of total AFLUS cases)
154 (69.4)
p < 0.01
Total T-FNA7,072
Number (%) of cases excised48 (70.6)
Number (%) of malignant cases22 (45.8)
Number (%) of malignant cases11 (13.9)
Number (%) of cases excised79 (51.3)
Fig. 2. Risks of malignancy of AFLUS with equivocal features of papillary carcinoma compared to AFLUS – other patterns in pa-tients who underwent surgical resection. AFLUS R/O PTC = AFLUS with equivocal features of papillary carcinoma.

Luu /Fischer /Stockl /Pisharodi /Owens Acta Cytologica 2011;55:526–530530
with equivocal features of papillary carcinoma was 45.8%. Although there was a significant difference between the number of patients who underwent surgical resection fol-lowing AFLUS with equivocal features of papillary carci-noma diagnosis and patients with a referring AFLUS – other patterns diagnosis, we suspect this difference may in part be due to the ‘concerning language’ used in the diagnostic comment of the former. Importantly, the ob-servation that all of the histologically proven malignancy in the referring AFLUS with equivocal features of papil-lary carcinoma diagnosis was papillary carcinoma re-flects the consistently recognized aspirate features that prompted this cytologic diagnosis. In addition, subse-quent discussion of AFLUS cases with equivocal features of papillary carcinoma at multidisciplinary conferences may bias the decision to refer these patients to surgical re-section. Nonetheless, our results are comparable to a pre-viously reported risk of malignancy of 38% in cases with a referring cytologic diagnosis of this subcategory [5] . On
the other hand, cases of AFLUS – other patterns may be managed conservatively, especially if a repeat fine-needle aspirate yields a benign cytologic diagnosis. It is also im-portant to monitor the rate of AFLUS to ensure it is not overused and to correlate cases with histologic follow-up to fine-tune the threshold for this diagnosis.
In summary our findings demonstrate that the ‘AUS/AFLUS’ category in TBSRTC is heterogeneous and that aspirates with equivocal features of papillary carcinoma harbor a greater risk of malignancy in patients who un-derwent surgical resection than atypical aspirates lacking these features. Conveying this risk to clinical colleagues is important and will facilitate optimal patient care.
Disclosure Statement
The authors have no relevant conflict of interest with any of the companies or products mentioned in this article.
References
1 Cibas ES, Ali SZ: The Bethesda System For Reporting Thyroid Cytopathology. Am J Clin Pathol 2009; 132: 658–665.
2 Rabaglia JL, Kabbani W, Wallace L, Holt S, Watumull L, Pruitt J, Snyder WH, Nwariaku FE: Effect of The Bethesda System for Re-porting Thyroid Cytopathology on thyroid-ectomy rates and malignancy risk in cyto-logically indeterminate lesions. Surgery 2010; 148: 1267–1272.
3 Theoharis CG, Schofield KM, Hammers L, Udelsman R, Chhieng DC: The Bethesda thyroid fine-needle aspiration classification system: year 1 at an academic institution. Thyroid 2009; 19: 1215–1223.
4 Luu MH, Fischer AH, Pisharodi L, Owens CL: Improved preoperative definitive diag-nosis of papillary thyroid carcinoma in FNAs prepared with both ThinPrep and conventional smears compared with FNAs prepared with ThinPrep alone. Cancer Cyto-pathol 2011; 119: 68–73.
5 Renshaw AA: Should ‘atypical follicular cells’ in thyroid fine-needle aspirates be sub-classified? Cancer Cytopathol 2010; 118: 186–189.
6 Renshaw AA: Focal features of papillary car-cinoma of the thyroid in fine-needle aspira-tion material are strongly associated with papillary carcinoma at resection . Am J Clin Pathol 2002; 118: 208–210.
7 Weber D, Brainard J, Chen L: Atypical epi-thelial cells, cannot exclude papillary carci-noma, in fine needle aspiration of the thy-roid. Acta Cytol 2008; 52: 320–324.
8 Yassa L, Cibas ES, Benson CB, Frates MC, Doubilet PM, Gawande AA, Moore FD, Kim BW, Nose V, Marqusee E, Larsen RP, Alex-ander EK: Long-term assessment of a multi-disciplinary approach to thyroid nodule di-agnostic evaluation. Cancer Cytopathol 2007; 111: 508–516.
9 Yang J, Schnadig V, Logrono R, Wasserman PG: Fine-needle aspiration of thyroid nod-ules: a study of 4,703 patients with histologic and clinical correlations. Cancer Cytopathol 2007; 111: 306–315.
10 Baloch ZW, Fleisher S, LiVolsi VA, Gupta PK: Diagnosis of ‘follicular neoplasm’: a gray zone in thyroid fine-needle aspiration cytol-ogy. Diagn Cytopathol 2002; 26: 41–44.
11 Gharib H, Goellner JR: Fine-needle aspira-tion biopsy of the thyroid: an appraisal. Ann Intern Med 1993; 118: 282–289.