Embed Size (px)
Citation preview

Atypical Chronic MyeloidLeukemia
Fabio Pires de Souza Santos
Hematologist
Hospital BP
Hospital Israelita Albert Einstein, Hospital Sao Camilo

Disclosures
• Speaker: Novartis, Janssen, Celgene, Amgen
• Research Funding: Novartis
• Advisory Board: Novartis, Amgen, Abbvie

Myeloproliferative Neoplasms Myelodysplastic/Myeloproliferative Neoplasms
Chronic Myeloid Leukemia, BCR-ABL1 positive Chronic Myelomonocytic Leukemia
Chronic Neutrophilic Leukemia Atypical Chronic Myeloid Leukemia, BCR-ABL1 negative
Polycythemia Vera Juvenile Myelomonocytic Leukemia
Primary Myelofibrosis Myelodysplastic/Myeloproliferative Neoplasm with Ring Sideroblasts and Thrombocytosis
Essential Thrombocythemia Myelodysplastic/Myeloproliferatyive Neoplasm, Unclassifiable
Chronic Eosinophilic Leukemia, NOS
Myeloproliferative Neoplasm, Unclassifiable

Atypical Chronic Myeloid Leukemia, BCR-ABL1 Negative
• MDS/MPN BCR-ABL1 negative granulocytosis with intense granulocytic dysplasia
• Incidence 1-2% of BCR-ABL1-positive CML
• Median survival 15 months
• Median age 60-70 years; Slight male predominance
• AML evolution in 30-40%
• No standard of care

HISTORY

WHO 2017 Diagnostic
Criteria
White Blood Cell count ≥ 13.000/mm3
Neutrophil precursors ≥ 10% of WBC
Dysgranulopoiesis
<2% Basophils
<10% Monocytes<20% Blasts PB and BM
Hypercellular BM with granulocytic dysplasia
Absence of rearrangements of PDGFRA, PDGFRB,
FGFR1 and PCM1-JAK2
No WHO criteria for BCR-ABL1-positive
CML, MF, PV, ET

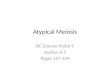
Atypical CML - Morphology

Abnormal Chromatin Clumping Syndrome

Atypical CML – Clinical FeaturesVariable Breccia Drozd‐Sokołowska Wang
Age, Median 62 64 72
Sex (M:F) 0.77 2.6 1.76
WBC, median (x109/L) 23.7 97 40.8
Hemoglobin, median (g/dL) 11.4 8.6 9.4
Platelets, median (x109/L) 319 66 87
Blood myeloid precursors ≥10% Median 13% Median 27.5 % 100%
Bone Marrow Blasts ≥5% Median 2% Median 3% 34%
Organomegaly 54% 67% 45%
Increased LDH NA 100% 84%

Molecular Features of Atypical CML (i.e. What’s Under the Hood)

Cytogenetic Abnormalities
in aCML
• Frequency variable 20-89%
• 30% of cases aneuploid changes
• Most commonly Trisomy 8
• -5
• -7/del(7q)
• del(20q)
• i(17q)
• Older case series include rearrangements of PDGFRA, PDGFRB, PCM1-JAK2 these should be classified as other neoplasms, not aCML!

Gene Mutations in aCML

SETBP1 mutations in atypical CML
Piazza R et al, Nat Genet 2012

SETBP1 mutations in atypical CML
Makishima H et al, Nat Genet 2013

SETBP1 mutations in atypical CML
Piazza R et al, Nat Commun 2018

Other Mutations in aCML
• Common but not specific ASXL1, TET2, SRSF2
• Possible therapeutic targets NRAS, CSF3R, JAK2, KIT
• Rare but very specific ETNK1
• CSF3R Mutations• Originally described in both CNL and aCML• Frequency in aCML may have been overestimated • Much more common and specific for CNL (~80% of cases)

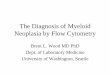
Differential Diagnosis of
aCML

CNL and CMML
Chronic Neutrophilic Leukemia
• Increased WBC
• Predominantly mature neutrophils and band cells
• Granulocyte precursors <10% of WBC
• Molecular: CSF3R mutations found in 60-70% of cases; high specificity
Chronic Myelomonocytic Leukemia
• Presence of increased monocytes in both absolute (>1000/mm3) and relative frequency (>10%)
• Molecular profiling may help differentiate role for AI approaches (see Faisal et al, Cancer Medicine 2019)
• TET2 more common in CMML (78%) vs aCML (20%)
• SETBP1more common in aCML

MDS/MPN-U
0,00%
10,00%
20,00%
30,00%
40,00%
50,00%
60,00%
70,00%
80,00%
90,00%
Organomegaly Increased LDH WBC >40x109/L Hb <10 g/dL Platelet<100x109/L
PB Blasts >5%
aCML MDS/MPN-UWang et al Blood 2014

Prognostic Factors in aCML
• Older age (>65 years)
• White Blood Cell Count >50x109/L
• Female gender
• Presence of >10% Circulating Blasts
• SETBP1 Mutation
Breccia M et al, Haematologica 2006; Piazza R et al, Nat Genet 2012

Therapy of Atypical CML
• No Standard of Care
• Patients should be evaluated for transplant eligibility eligible patients should proceed to HSCT as soon as possible
• Multi-Gene NGS Panel to Screen for Targetable Lesions JAK2 (Ruxolitinib), CSF3R (Ruxolitinib or Dasatinib), NRAS(Trametinib)
• Conventional Therapy Hydroxyurea, Interferon-alfa, ESA, Hypomethylating drus

Hypomethylating Agents
From Schwartz LC and Mascarenhas J, Blood Reviews 2019

HSCT in aCML
46 patients submitted to EBMT Registry between 1997 and 2006
Prognostic Factors for Outcome pos-HSCT
• Older Age
• EBMT Score
• Donor Type
RFS in 5 years is 36%
OS in 5 years ˜50%
From Onida F et al, Br J Haematl 2017

Algorithm for Therapy of
Atypical CML
From Gotlib J, Blood 2017

Conclusions• Atypical CML is a form of MDS/MPD characterized by leukocytosis,
granulocytic hyperplasia with severe dysplasia and increased immature precursors
• Several mutated myeloid genes are found in aCML; SETBP1 and ETNK1 are the most specific ones
• SETBP1 mutation associated with poor survival in aCML
• NO standard therapy eligible patients should be offered HSCT; NGS panels should be used to determine presence of targetable lesions