Embed Size (px)
Citation preview

Atul Grover, M.D., Ph.D.September 17, 2015
Medical Education: The Foundation of the Futureof Medicine
Future of Medicine Summit IXWest Palm Beach, FL
[email protected]@AtulGroverMD

AAMC: Med. Schools, Hospitals, MDs
• Membership includes: 144 U.S. medical schools (MD programs) Nearly 400 major teaching hospitals and health systems
Includes 51 VA medical centers Nearly 90 academic and scientific societies
• Over 300,000 “Voices:” 141,000 faculty members
Clinical and basic science (research) faculty Staff the physician practice groups and hospitals
83,000 medical students 115,000 residents
2

Extraordinary clinical careCOTH hospitals comprise only 5% of all hospitals but account for:
37% of charity care 23% of all hospital care
24% of all Medicaid in-patient days 20% of all Medicare in-patient days
88,577 full-time MDs work in medical school clinical departments
Cutting edge researchOver half of NIH Extramural Research Awards go to an AAMC medical school and/or teaching hospital
Education and training74% of all residents train at an AAMC hospital
AAMC Hospitals’ 3 Missions Advance Health
3

© 2015 AAMC. May not be reproduced without permission.
AMC Missions Rely on Multiple RevenueStreams; Revenue Cuts Mission Cuts
Clinical Revenue
IMEDSH
Residents,Students Research
Community Benefits
4

© 2015 AAMC. May not be reproduced without permission.
5
The Small “p” Politics of Medical Education: Adapting to Change
The Big “P” Politics of Medical Education: Advocating to Congress

© 2015 AAMC. May not be reproduced without permission.
Medical Education Enterprise: Numbers
830,000 doctors, including 750,00 in patient care• 32.6% = women; 24% = IMGs; 8.9% = minorities; 36% = age 55+
6
144 MD schools and 30 DO schools• 80,000 MD students; 24,000 DO students
9,600 ACGME certified residency programs• 120,000 residents; 5,000 more in AOA certified programs
• 46.1% = women; 25.9% = IMGs; 10.5% = minorities

Society’s Changing Health Care Needs
Outcome Focused: Health care delivery, payment measured by quality, outcome metrics.• Volume or cost no longer drive payment.
7
Cost Conscious: Health care designed to – • Maximize each health care team member’s contribution.
• Members include multiple different health professionals.
Population Health Focused: Emphasis on improving, maintaining health, not just treating illness.• Workforce size, distribution, demographic & specialty composition all
matter.
• Organization, financing of care matter, too.

© 2015 AAMC. May not be reproduced without permission.
What’s Changing:
How Medical Education Is Responding to Society’s Changing Needs
8

Small “p” Politics of Medical EducationMajor Changes at Every Step in the Process
New MCAT + New Competencies to Demo + Life-long Learning
Achieving Competencies to Meet Society’s Changing Needs: Better Quality, Lower Cost, Population Health
The Match
9

Core Competencies in Premedical Students
Resilience and AdaptabilityCapacity for ImprovementCritical ThinkingQuantitative ReasoningScientific InquiryWritten CommunicationKnowledge of Living SystemsKnowledge of Human Behavior
Service OrientationSocial SkillsCultural CompetenceTeamworkOral CommunicationEthical ResponsibilityReliability and DependabilityResilience and Adaptability
10

www.AAMC.org/MCAT
A New MCAT Exam
In the first 14 hours, 14,000 applicants registered for the new MCAT

Diversity
Holistic Review
Pre-professional Readiness
Holistic Review
Academic Readiness
www.AAMC.org/admissions
12

Enhancing Medical School
13

Translating Competencies to Observable Behaviors
The Physician
Patient Care
Knowledge for Practice
Inter-professional Collaboration
Personal and Professional Development
Systems-based Practices
Practice-based Learning and Improvement
Professionalism
Interpersonal and
Communication Skills
Recommend and interpret
common diagnostic and screening
tests
Gather a history and perform
a physical examination13 Core Entrustable
Professional Activities
Prioritize a differential diagnosis
following a clinical encounter
14

Refocusing Residency and Fellowships
15

AAMC Vision for Optimizing GME
#2. Optimizing the Environment for Learning, Care, and
Discovery
#1. Investing in Future Physicians
#3. Preparing the Physician and Physician
Scientist for the 21st Century
1716

Optimizing GME: AAMC Priorities
1. Investing in Physicians:
17
• Refine GME accountability metrics.
• Align residency training with societal needs, students’ aspirations & desires.
• Make case for public funding of GME.

Optimizing GME: AAMC Priorities
2. Optimizing the Environment for Learning, Care, and Discovery:
18
• Define, foster optimal learning environments.
• Improve environment for teaching faculty.

Optimizing GME: AAMC Priorities
3. Preparing the physician & physician scientist for the 21st Century
19
• Elevate performance of entering
residents & new practitioners.
• Develop models, demonstrate ways to optimize duration of education and training.

20
What Hasn’t Changed:
The Match Is Increasingly a Big Squeeze

Match 2015:
1,093* US MDs without a position before SOAP
606** US MDs without a position after SOAP
27,293*PGY1 Positions
18,025*US MD Seniors =
Applicants
Match
Data from the 2015 Match and 2015 SOAP
16,932 Matched US MDs*
Match DayMarch 20, 2015
21 Data: Results and Data 2015 Main Residency Match, NRMP, & NRMP CEO Presentation to April 2015 Group on Student Affairs

Primary Care Continues to Over Shadow Specialties in Match: 2015 Picture
This year, 27,293 residencies offered nationally. Potential primary care residencies = 46.3%.• Family medicine: 3,195
• Internal medicine: 6,770
• Pediatrics: 2,668
Total: 12,633 = potential primary care = 46.3% of all residencies offered
In contrast:*• Child neurology – 104 residencies offered = 0.38% of all offered
• Thoracic surgery – 35 residencies offered = 0.13% of all offered
• Dermatology – 22 residencies offered = 0.08% of all offeredSource: NRMP * = PGY-1 positions
22

23
Why Is the Supply of Slots on Match Day so Tight?
The Big “P” Politics of GME

Two Points of ContentionIs there a physician shortage?
• Many, including AAMC, believe nation faces serious shortage by 2025
• Not all agree – e.g., IOM committee
Should Medicare fund more residency slots?
• In 1997, Congress capped # of residents for which Medicare pays GME at 1996 #. Virtually no change in cap in 18 years. But med school grads up nearly 30%.
Result = bottleneck.
24

In 1997, Congress Capped # Residents Eligible for Medicare GME at 1996 LevelsNumber of applicants exceeds cap; big loss of $
25 Source: NRMP, Results and Data: 2014 Main Residency Match

The Big “P” Politics of GME: What Challenges Face the Physician Workforce
Projected shortages.• Significant shortages in primary & specialty care.
Growing health professionals workforces.• Rapid increases in NPs, PAs.
• Team-based delivery of care.
Political obstacles to lift Medicare GME cap.• $10 billion/10 years cost to add 3,000 resident slots/year.
• Some want to use GME $ for other purposes.
26

New Workforce Projections Look at Multiple Scenarios: Shortages in AllScenarios run for AAMC: Demographic Changes: Growth, aging. Insurance Status Changes: ACA impact. Physician Behavior Changes: Work hrs, yrs. Staffing Pattern Changes: NPs Health Care Organization Changes: ACOs.
27

New Projection Findings: What the Graphs Will Show You
Time
Ph
ys
icia
ns
DemandSolid line = Demand
Dotted line = Supply
Supply
28

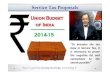
Supply Versus Demand: All Physicians
700,000
750,000
800,000
850,000
900,000
950,000
2013 2014 2015 2016 2017 2018 2019 2020 2021 2022 2023 2024 2025
Full
Tim
e Eq
uiva
lent
Phy
sici
ans
Year
Demand (ACA + MC)
Demand (ACA)
Demand (ACA + RetailClinics)Demand (Demographics)
Demand (APRN Moderate)
Demand (APRN High)
Supply (Retire Later +2)
Supply (GME Growth)
Supply (Status Quo)
Supply (Millennial Hours)
Supply (Retire Earlier -2)
29

All Physicians: Continued Shortages in 2025
New Projections for 2025:46,100 – 90,400 Shortage
30

Primary Care: Cont’d. Shortages in 2025
New Projections for 2025:12,500 – 31,100 Shortage
31

New Projections for 2025: 28,200 – 63,700 Shortage
“Med/Surg Specialties:” Cont’d. Shortages
32

Why a Physician Shortage? Demand Is Growing Faster than Supply
• Many factors, but demographics = biggest
33
• Population = growing larger, older
Elderly have greater health care needs 46% projected growth in elderly; 5% for young Medicine keeps people alive but with more illnesses Next 20 years: 36 million people added to Medicare
• Even best prevention delays disease, does not eliminate it.

34

A Growing, Aging Population Matters
35
HHS/HRSA The Physician Workforce: Projections and Research into Current Issues Affecting Supply and Demand, December 2008 at http://bhpr.hrsa.gov/healthworkforce/reports/physwfissues.pdf
Physician utilization/100,000 people by age

36

Because of Growth/Aging: Supply Also Not Likely to Keep Pace with Demand
Number of physicians per capita = flat/decrease in next decade if we don’t train more.
37
# of hours /week worked makes big difference. Older physicians work longer hours than younger
“Millennials” – Will that continue?
Age of retirement also a big factor. 36% of doctors now = age 55+. Most will retire in the next decade. But will they retire sooner or later Even a year or 2 delay makes affects future supply.

Indicators of Physician Shortages
Longer waiting times for an appointment Both primary care and specialists Most vulnerable – low income, complex patients
38
Backlog of unfilled positions for doctors – e.g.: 19% of WY population lives in underserved area 31% of MS population
Classic examples: VA, Medicaid Long waiting times for veterans became big new MacPac reports difficulty getting specialist
appointments for Medicaid, CHIP recipients
Source: http://hrc.nwlc.org/status-indicators/people-medically-underserved-areas

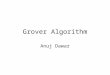
Example: In July 2015, 67% of VA Physician Vacancies = Specialists
Source: AAMC Analysis of Job Postings from VA Physician Careers Website, as of July 2015http://www.vacareers.va.gov/careers/physicians/index.asp
30%
67%
Percent of VA Physician Vacancies
Prim. Care Specialists
Other
3%
Other = Non-Care Givers
39

What Do Shortages Mean for Patient Care Delivery?
Increasing pressures for changes in care delivery: Non-physician providers Team delivery New technologies New reimbursement strategies Focus on outcomes, cost Population health promotion
40

© 2015 AAMC. May not be reproduced without permission.
41
The Power of Advocacy: Your Advocacy

Where Do We Go from Here? AAMC Advocates a Four-Pronged Strategy
No one tactic is enough. A multi-pronged strategy is needed to avoid a physician shortage.
42
Advance health care delivery reform to achieve more cost-effective care. AMCs are leaders.
Champion accountability for GME – bipartisan bills.
Pass legislation to lift cap on number of residents for which Medicare will pay for GME – also bipartisan.
Strengthen federal investment in programs to address maldistribution, such as NHSC and Title VII.
We’re advocating for all of them. Please join us.

Reduce the Physician Shortage
Bill Nelson (D-FL)
Charles Schumer (D-NY)
Harry Reid (D-NV)
S. 1148: Resident Physician Shortage Reduction Act of 2015A bill to amend title XVIII of the Social Security Act to provide for the distribution of additional residency positions, and for other purposes114th Congress, 2015–2016. Sponsor and 12 cosponsors.
43

© 2014 AAMC. May not be reproduced without permission.
Reduce the Physician Shortage
44
Joe Crowley (D-NY)
Charles Boustany, M.D. (R-LA)
H.R. 2124 : Resident Physician Shortage Reduction Act of 2015A bill to amend title XVIII of the Social Security Act to provide for the distribution of additional residency positions, and for other purposes114th Congress, 2015–2016. Sponsor and 76 cosponsors.

© 2014 AAMC. May not be reproduced without permission.
Encourage Your Members of Congress
Please Thank:
45
Sen. Bill Nelson for sponsoring the Senate bill.
Rep. Alcee Hastings for cosponsoring the House bill.

© 2014 AAMC. May not be reproduced without permission.
Encourage Your Members of Congress
Ask to Them Cosponsor GME Bills:
46
Sen. Marco Rubio
Rep. Lois Frankel
Rep. Patrick Murphy

Grassroots Advocacy Is Essential
“Now more than ever the people are responsible for the character of their Congress. If that body be ignorant, reckless, and corrupt, it is because the people tolerate ignorance, recklessness, and corruption."
James Garfield, "A Century of Congress" published in Atlantic, July 1877
47

What You Can Do: Join AAMC ActionPower AAMC’s Grassroots Advocacy
• Nearly 156,000 people are part of AAMC Action – over 10,000 new members in ‘15
• Over 29,000 responded to calls to action – 16+% of the community.
• Join the community at www.aamcaction.org
• Encourage friends, family, colleagues to do the same
www.aamcaction.org48