-
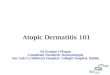
Atopic dermatitis: Chronic and relapsing disorder
Nestor Cisneros MD FRCPC
Assistant professor Allergy and Clinical immunology
Training Program Director Allergy and Clinical Immunology
-
Conflict of interest
• Shires: speaker
-
Objectives
➢At the end of this session,
➢ participants will be able to recognize the prevalence of
atopic dermatitis.
➢ Review the current management of atopic dermatitis
➢ Recognize the psychosocial impact of atopic dermatitis.
-
Atopic Dermatitis: Epidemiology.• Chronic and relapsing
disorder
• AD is the most common skin condition. • Affect 20 %
children.
• 20-33% of AD patients have moderate to severe disease
• AD first manifestation with allergic disorder.
• Impact QoL to patients & their families
-
Burden of AD.
-
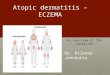
Infants with Eczema, sleeping problems and mental health at 10
yrs of age
Variable Odds ratio (95 CI)
• Emotional problemsInfant eczema with
sleep problems 2.63 (1.20-5.78)
• Conduct problemsInfant eczema with sleep problems 3.03
(1.01-9.2)
• Hyperactivity -Infant eczema 1.78 (1.02-3.09)- ever eczema
2.12 (1.34-3.37) Schmitt et al Allergy 2011Schmitt et al Allergy
2011
-
InfectionURI/OMBacterial, fungalViral infection
AllergensFood (egg)Environmental (mites)Contact dermatitis
(Nickel)
Heat, drynessAnxiety
Triggers for atopic dermatitis
Itch-scratch cycle AD flares
-
How to treat Atopic Dermatitis
Education
Maintenance and repair of skin barrier
managing infectious triggers
Minimizing triggersSkin directed TXAntihistamines ( caution)
TCSTCI
/Bleach bath
-
Maintenance skin care
• Foundation of the AD management ( soaking bath)• Bathe
daily
• Soak 10-15 minutes in lukewarm water
• Use moisturizing cleanser where needed
• Apply medication &moisturizing after bath
• Lubrication/moisturization:• Reduce the needs for topical
steroids.
• Help to repair the skin barrier
Nicol NH, Boguniewicz M .Dematology Nursing Oct 2008
-
Topical therapy: emollient
Clark A et al J Drugs Dermatol 2011;10(5):531-7
Day 7
Day 21
N:392-17 year with mild to moderate AD
-
Topical Treatment of inflammation: TCS and TCI• Goal of therapy
to treat inflammation
• Topical steroids: effective and extremely safe when use
correctly
• Topical Calcineurin inhibitor: ( second line)• Acute therapy
for inflammation and proactive therapy
• Key-give skin break.
Use of anti-inflammatory therapy to "put out the fire”
-
Topical corticosteroids
• First line treatment
• Potency classification• Class I –most potent
• Class VII – least potent
• Potency differ and can be confusing
• Address the steroid phobia.
-
Topical Corticosteroids
Vehicle or form of the products
-
TCI: topical calcineurin inhibitor
• Do not cause the side effects of TCS
• Beneficial to treat AD • Concern about long term use of
TCS
• In areas on the face, eyelids
• Side effect: burning and stinging
• Higher cost
• FDA:• Black box warning (2006) due to the theoretical risk of
lymphoma.
• Pediatric eczema elective registry :no increase in the risk of
eczema (2014)
Black warming
-
Topical steroids-pearl
For patient saying
“As soon as I stop , it comes RIGHT BACK”
OR
“I HAVE TO USE IT EVERY DAY”
Then steroids potency is probably too low
Provided that all other areas of the treatment are being
maximized
-
Management of the AD exacerbation
Zubierbier et al JACI 2006
-
Anti-inflammatory treatment
AD flare
Topical steroids application
Day 7-14;Low potency _faceMid high potency
Daily useEOD Emollients
Recovery
Aim for rare flares up
-
Proactive therapy for AD
Preventing eczema flare up William HC BJD 2011
-
How much to dispense
Area treated* Once BID x 1 week
Hands, head, face 2 g 88 g
Leg 4 g 56 g
Entire body 30 g 420 g
* 70 kg adult
-
Bleach bath
• Randomized• 31 patients ( 6 m-17 year with
moderated to severe eczema and bacteria infection)
• All treated with cephalexin 14 days prior.
Mean EASI score at one month and 3 month.
Huang J et al Pediatrics Vol. 123 No. 5 May 1, 2009
Mupirocin oint.Bleach bath
Intranasal petroleum ointPlain water bath
EASI: Eczema area and severity index score
-
Step care management.