Embed Size (px)
Citation preview

A�
rchivum Immunologiae et Therapiae Experimentalis, 2000, 4�
8,� 497–504P�
L ISSN 0004-069X
Review
Pathogenetic Mechanisms of Atopic DermatitisS. Pastore et al.: Pathogenesis of Atopic Dermatitis
SAVERIA PASTORE1, FRANCESCA MASCIA1, MA�
RIA LA�
URA GIUSTIZIERI1, AL�
BERTO GI�ANNETTI2
and GIAMPIERO GI�ROLOMONI1*
1 Laboratory of Immunology, Istituto Dermopatico dell’ Immacolata, IRCCS, Rome, Italy, 2Department of Dermatology, University ofM�
odena and Reggio Emilia, Modena, Italy
Abstract. Atopic dermatitis (AD) is a chronic inflammatory disease which results from complex interac� tionsb
�etween genetic and environmental mechanisms. An altered lipid composition of the stratum corneum is respon-
sible for the xerotic aspect of the skin and determines a higher permeability to allergens and irritants. Keratino-c� ytes of AD patients exhibit a propensity to an exaggerated production of cytokines and che mokines, a phenome-non that can have a major role in promoting and maintaining inflammation. Specific immune re sponses againsta� variety of environmental allergens are also implicated in AD pathogenesis, with a bias t
�owards Th2 immune
responses. In particular, dendritic cells expressing membrane IgE receptors play a critica� l role in the amplificationo f allergen-specific T cell responses. Cross-linkage of specific IgE receptors on dermal ma� st cells provokes therelease and synthesis of a vast series of mediators. Following their recruitment and activa� tion into the skin,e osinophils are also thought to contribute relevantly to tissue damage. Thus, a complex netw� ork of cytokines andc� hemokines contributes to establishing a local milieu that favors the permanence of inflamma� tion in AD skin.
Key words: skin; atopy; keratinocytes; dendritic cells; T lymphocytes.
Introduction
Atopic dermatitis (AD) is a chronic and relapsinginflammatory skin disease with an early onset and char-a� cterized by typically distributed skin lesions in differ-e nt age groups. Acute lesions present with erythema-t
�ous macules and papules, associated with excoriations
a� nd erosions. Chronic AD is characterized by thickenedskin with accentuated skin markings and excoriated pa-p� ules43, 49. AD is a major health problem world-wide,a� ffecting 5 to 20% of children5
�2, and in the last decades
AD as well as other atopic disorders have becomesteadily more prevalent in developed countries, sugges-t
�ing that environmental factors are playing a critical
role in their expression. In these countries, 30% of thep� opulation may manifest some atopic disease somet
�ime in their lives. These syndromes appear to be more
frequent in urban areas than in rural areas and amongh
�igher socioeconomic classes15, 46. Of all skin diseases
a� ffecting children, AD has one of the greatest impactso n the impairment of the child’s quality of life27. Inh
�ospital studies, cases of chronic AD or repeated epi-
sodes of acute AD often achieve the highest morbidityscores on disability measures when compared witho ther skin diseases8, 11. In adults, atopic hand dermatitise xacerbated by occupational exposure accounts fora� considerable loss of working hours44.
I�n this review we will examine cellular and immune
* Correspondence to: Giampiero Girolomoni, Istituto Dermopatico dell’ Immacolata, IRCC�
S, Via Monti di Creta 104, 00167 Roma,I�taly, tel.: +39 06 664 64 736, fax +39 06 664 64 705; e-mail: [email protected]

m echanisms that are thought to play an important rolein the pathogenesis of AD. An understanding of theb
�iological bases of AD has important implications in
t�he management as well as the early identification and
p� revention of this common illness.
Phenotypes and Genotypes in AD
D�
ry skin and increased susceptibility to cutaneousirritation are always present in AD patients and, thus,AD can be exacerbated following exposure to reducedh
�umidity, excessive sweating and a vast array of irri-
t�ants, such as wool, acrylic, soaps and detergents.
A�
long with these factors, exposure to environmentala� llergens can be a relevant flare factor, and a propens-ity to IgE hyperresponsiveness is present in about 80%o f AD patients7
�. However, a direct relationship be-
t�ween immediate or delayed skin test reactivity to al-
lergens and the course of AD is seldom present, andsometimes highly elevated IgE levels do not accom-p� any any clinical manifestation of atopy41. In contrastt
�o respiratory atopy, specific hyposensitization is not
g� enerally helpful in AD patients. Among the environ-m ental factors that may contribute to AD pathogenesis,skin colonization by S
�taphylococcus aureus appears to
h�ave some role in disease exacerbation24. Staphylococ-
c� al strains can, in fact, release both allergenic com-p� ounds and superantigens4
�8 and can act as effective
immunological adjuvants for increased IgE response toa� eroallergens14. Intense pruritus is the cardinal featureo f AD, and the skin damage inflicted by scratching isc� onsidered critical for the development and mainten-a� nce of the eczema. Moreover, compared with normalc� ontrols, patients appear to have a reduced itch thre-shold and a more prolonged itch duration to differentstimuli.
Familial aggregation and twin studies have con-f
�irmed a fundamental contribution of genetic factors to
t�he development of atopic disorders2
�. However, the en-
d�eavor to finely characterize a genetic background
u� nderlying atopy copes with an important degree ofg� enetic heterogeneity, which implies multiple genetica� ctions at different phenotypic levels5
�. So far, the ident-
i�fication of specific functional polymorphisms in major
c� andidate genes and their correlation to the expressiono f atopic diseases in different groups of families andu� nrelated subjects have restricted the search to at leastf
�ive distinct chromosomal regions2
�. In particular, signi-
ficant genetic linkages to the atopic phenotype haveb
�een found in chromosomal loci coding for components
o f the antigen-directed mechanisms of IgE responsive-
n� ess, such as the D region of human leukocyte antigen(HLA) (6p21.3), the α and δ chains of the T cell recep-t
�or (TCR) (14q11.2-13) and the β chain of the high
a� ffinity receptor for IgE (Fcε R!
I) (11q13). Two largec� lusters of polymorphic genes coding for cytokines, i.e.interleukin 3 (IL-3), IL-4, IL-5 and granulocyte/macro-p� hage colony-stimulating factor (GM-CSF) (all in 5q),a� nd interferon γ" (IFN-γ" )
# and stem cell factor (SCF)
(both in 12q), are thought to exert a critical control noto nly on B cell isotype switching to IgE, but also ona� predominant activation of T helper 2 (Th2) cells, eo-sinophils and basophils. A gain-of-function mutation int
�he gene coding the α subunit of the IL-4 receptor
(16p11.2-16p12.1) is also considered to be a conditionp� redisposing to atopy22. It is important to underline thatsome of the polymorphic regions characterized so far,in particular those in chromosomes 12 and 14, includeg� enes coding for transcription factors.
Since genetic predisposition to allergy in AD mayb
�e similar to that in patients with respiratory atopy, it
i�s likely that the preferential targeting of the allergic
i�mmune response in a given tissue may depend ona� series of events, such as the site of initial sensitizationt
�o a specific allergen, the ability of T lymphocytes toh
�ome differentially to the skin vs the respiratory muco-
sa, and the programmed response of resident cells, e.g.e pithelial cells, to injury and inflammation25. Hence, itis expected that, in addition to genes responsible for thea� bnormalities shared by all atopic patients, other genesc� onfer specific organ susceptibility. Interestingly, ADp� atients were found to have polymorphism in the genec� oding for mast cell chymase (14q11.2), a serine pro-t
�ease expressed exclusively in cutaneous mast cells,
w� hich have a key role in the allergic inflammation oft
�he skin2
�8.
S$
kin Abnormalities in AD
Skin dryness of AD patients is the consequence ofa� n epidermal permeability barrier dysfunction, which int
�urn is related to an altered lipid metabolism in kerati-
n� ocytes3%3. In particular, a reduced content of ceramides
has been reported in the cornified envelope of bothh
�ealthy and diseased epidermis. Ceramides serve as the
major water-holding molecules in the extracellularspace of the cornified envelope, and the barrier functiono f this complex structure is provided by a matrix ofstructural proteins bound to ceramides by ester link-a� ges29. Also filaggrin, a precursor of the proteic com-p� onents of that matrix, is prominently decreased in ADskin4
�7. In both human and mouse models it has been
498 S&
. Pastore et al.: Pathogenesis of Atopic Dermatitis

r' epeatedly shown that a perturbation of the epidermalb
�arrier causes an increased keratinocyte generation of
c� ytokines, including IL-1α, tumor necrosis factorα (TNF-α)
#, GM-CSF and growth factors5
�4. These cy-
t�okines can stimulate lipid synthesis and cell prolifera-
t�ion and, thus, contribute to restoring cutaneous ho-
m eostasis. However, many of these cytokines are alsop� otent initiators of inflammatory responses3
%7 and can
c� reate a microenvironment that favors the emergenceo f specific immune reactions (Fig. 1). Accordingly, in-v( estigations in mice have shown that immune responsesinduced by sensitization with haptens or aeroallergenst
�hrough barrier-disrupted skin are strongly associated
w� ith the induction of Th2-dominant immune responses,a� s observed in AD23.
If the barrier dysfunction can help to explain thed
�ecreased irritancy threshold in the skin of AD patients,
it is reasonable to postulate that an impairment in ce-ramide synthesis can affect skin homeostasis throughm ore intimate mechanisms. In fact, ceramides have re-c� eived increasing attention over the past decade asmodulators of specific biological events. In particular,c� eramides seem to differentially down-regulate the ac-t
�ivity of protein kinase C (PKC) isozymes. It has been
d�emonstrated that ceramides can compete with the
b�inding of the physiologic ligands, 1,2-diacylglycerols,
F)
ig. 1. Overview of cellular and molecular mechanisms underlying atopic dermatitis (AD). Epidermal* barrier dysfunction facilitates the
s+ kin permeability to both irritants and allergens. These substances are potent stimuli for release of a variety of cytokines and chemokinesb,y keratinocytes. In addition, due to mechanisms aimed to restore cutaneous homeostasis, barrier perturbation p- er se induces keratinocyte
s+ ynthesis of proinflammatory molecules, active on keratinocyte themselves, dendritic cells (DC), T cells, mast cells and endothelial cells,t.hus favoring initiation and persistence of inflammatory and immune responses. IgE hyperresponsiveness to environmental allergens is
a/ flare factor of AD and involves both DC and mast cells: mast cells participate in the IgE-mediated immediate hypersensitivity reactionb,y releasing vasoactive amines and several cytokines. DC can bind IgE through specific membrane receptors, and can efficiently present
IgE-bound allergens to T lymphocytes, causing the expansion and effector functions of Th2 cells. The large number of activated DC inAD lesions may also contribute directly to the inflammatory process through the release of inflammatory cytokines and chemokines.E0
osinophils are recruited primarily by chemokines released by fibroblasts, and participate to AD pathogenesis by releasing toxic moleculesa/ nd IL-12, which helps in the generation of Th1 responses. Inflammatory cells have a prolonged
1 survival capacity, which contributes to
p2 erpetuation of inflammation
S&
. Pastore et al.: Pathogenesis of Atopic Dermatitis 499

o r can interfere with enzyme translocation from thec� ytoplasm to the membrane, which is a necessary stepin PKC activation18. In turn, PKC activation has a pri-m ary role in transmembrane signaling by hormones andg� rowth factors3
%4, so that a defect in ceramide generation
c� ould determine a dysregulated, enhanced activation oft
�hese intracellular mechanisms of signal transduction,
e ventually leading to an exaggerated production ofp� roinflammatory cytokines by keratinocytes. Indeed,a� series of experimental data leads to conclude that theintrinsic hyperreactivity of AD skin as well as its tend-e ncy to develop more pronounced and persistent in-f
�lammatory reactions could depend, at least in part, on
a� n abnormal functional activation of epidermal kerati-n� ocytes. Compared with keratinocytes from nonatopicc� ontrols, keratinocytes cultured from nonlesional skino f AD patients spontaneously synthesize and releasehigher levels of several proinflammatory cytokines,such as IL-1, TNF-α and GM-CSF. Moreover, thesec� ells display an exaggerated cytokine secretion in re-sponse to metabolic activators (phorbol esters and syn-t
�hetic analogs of diacylglycerols) or proinflammatory
c� ytokines, such as IFN-γ" 3%
8, 39. Preliminary data from thea� uthors’ laboratory confirm that keratinocytes from ADp� atients present a dysregulated control over gene tran-scription, with a more prominent activation of activatorp� rotein 1 (AP-1) transcription factors and, consequent-ly, a more efficient binding to gene promoters. Reason-a� bly, altered levels of nuclear PKC isozymes could beimplicated in this phenomenon. Enhanced expression ofp� roinflammatory cytokines such as IL-1β and TNF-αb
�y epidermal cells has also been reported in vivo fol-
l3owing the application onto nonlesional skin of aller-
g� ens19. It is thus possible to speculate that specific tar-g� eting of atopic inflammation to the skin could dependnot only on the existence of a barrier dysfunction, buta� lso on the constitutive, enhanced propensity to syn-t
�hesize and release proinflammatory cytokines by AD
k4eratinocytes. The specific pathways through which
such functional dysregulation takes place are nowu� nder active investigation.
Immunological Abnormalities in AD
Many studies have shown the existence of a varietyo f perturbations of the immune system in AD patients,e ven though their real importance is not completelyu� nderstood. Peripheral blood lymphocytes from pa-t
�ients with AD secrete increased amounts of Th2 cyto-
k4ines (e.g., IL-4, IL-13, IL-5) and decreased IFN-γ" .
Moreover, monocytes and B cells from AD patients
e xpress high levels of the IL-4 receptor and of the lowa� ffinity IgE receptor (CD23), and peripheral bloodB cells from AD patients spontaneously produce highl
3evels of IgE21, 42. A series of data also suggests that
AD monocytes are metabolically activated: when col-lected from the peripheral blood, they are primed forsuperoxide generation and produce significantly higherlevels of GM-CSF compared with monocytes fromhealthy controls4. Monocytes present in the perivascu-l
3ar infiltrate of atopic lesions have been identified as
t�he major source of prostaglandin E2
� (PGE2� )
# and IL-
-103%
5. Both PGE2 and IL-10 can act on infiltratingT
5 cells to determine an impairment in their IFN-γ" pro-
d�uction, thus contributing to the establishment of
a� local Th2 cytokine milieu. A major immunopatho-g� enetic role is thought to involve activated CD4+
T lymphocytes with a high propensity to recirculate int
�he skin thanks to the expression of the skin-homing
r' eceptor, cutaneous lymphocyte-associated antigen(CLA).
A�
D is associated with an abnormal activation ande xpansion of distinct subpopulations of helper T lym-p� hocytes reactive against allergens in the skin. In par-t
�icular, the initiation and maintenance of AD are be-
l3ieved to be caused by CD4+6 T cells belonging to the
Th2 subset, since the cytokines predominantly found inskin lesions are IL-4, IL-5 and IL-13, with lowereda� mounts of IFN-γ" . IL-4 expression is most prominentin acute AD, while IL-5 expression is predominant inc� hronic AD, mostly from lymphocytes but also frome osinophils13. A recent characterization of the lym-p� hocytic infiltrate suggested the existence of an IL-13--dominated pattern of cytokine secretion1, also con-firmed by the fact that a strong IL-13 gene expressionhas been found in the lymphocytic infiltrate of botha� cute and chronic skin lesions5
�0. The proinflammatory
a� ction of Th2 cytokines seems pertinent when serumIgE levels are raised, since IL-4 and IL-13 from acti-v( ated Th2 are strong inducers of IgE production byB cells10. Because of the reciprocal regulation of Th2a� nd Th1 responses, the prevalent expansion of CD4+6
Th2 cells could also contribute to explaining the re-d
�uced capacity of patients with severe AD to mount
Th1 responses, including the delayed-type hypersensi-t
�ivity response and protective immunity to viral infec-
t�ions2
�6, 31. According to some authors, the current un-
d�erstanding of Th2 predominance in AD may be an
o versimplification. In particular, IFN-γ" mRNA hasb
�een reproducibly detected in AD lesions and shown to
d�ecrease after successful therapy, and IFN-γ" -producing
a� llergen-specific Th1 clones have been obtained fromc� hronic skin lesions. Based on experiments performed
5700 S
&. Pastore et al.: Pathogenesis of Atopic Dermatitis

o n skin lesions elicited by topical application of aller-g� ens, a two-phase model of AD pathogenesis has beenp� roposed in which an initiation phase, with a predomi-n� ant Th2-like inflammatory response and without cli-nically apparent skin lesions, is switched into a sec-o nd eczematous phase, dominated by the presence ofI
�FN-γ" 12. In this context, IFN-γ" can act as a potent
stimulus for the synthesis and secretion of proinflam-matory cytokines by keratinocytes, and recent resultsf
�rom the authors’ laboratory indicate that keratinocytes
from AD skin are particularly responsive to IFN-γ" int
�erms of IL-1, TNF-α and GM-CSF release3
%8. Other
T5
cell responses, such as those against keratinocyte selfa� ntigens or microbial superantigens, could provide ad-d
�itional mechanisms for the perpetuation of immune
r' esponses in AD skin.The selection of the type of inflammatory infiltrate
t�hat characterizes a specific disease is strictly control-l
3ed by the chemokine receptor repertoire displayed by
t�he leukocytes and by the pattern of chemokines re-
l3eased by the tissue. Interestingly, the various cell popu-
l3ations recruited into AD lesions, including Th2 cells,
immature DC, monocytes and eosinophils, express re-c� eptors for chemokines such as eotaxin, RANTES,m onocyte chemoattractant protein 3 (MCP-3) andMCP-445. In situ hybridization experiments performed
o n skin biopsies soon after challenge with a proper pro-v( ocation factor have demonstrated a prominent neosyn-t
�hesis of RANTES and MCP-3 by dermal fibroblasts5
�5.
I�t has also been demonstrated that IL-4 is a powerful
inducer of eotaxin and MCP-4 in fibroblasts3%
2, 40. Event
�hough the involvement of resident epidermal cell
p� opulations in the release of specific chemokines hasnot been fully characterized so far, the prominent ker-a� tinocyte expression of GM-CSF3
%9, RANTES and MCP-1
c� an provide strong chemotactic signals for T cells.
R8
ole of Dendritic Cells
A�
prominent skin infiltration by hyperstimulatoryd
�endritic cells (DC) is an important feature of AD6
9. The
lesional skin of AD patients exhibits an increased num-b
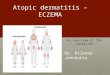
�er of cells belonging to the DC lineage (Fig. 2), in-
c� luding epidermal Langerhans cells (LC), dermal DCa� nd a unique population of epidermal CD1a+ DC ex-p� ressing CD1b and/or CD36, which closely resembleD
�C generated in vitro by culturing monocytes with
G:
M-CSF and IL-42�4, 53. Such DC can efficiently present
IgE-bound allergens to T lymphocytes, since they dis-p� lay an up-regulated expression of both the high af-finity (Fcε RI) as well as the low affinity (Fcε RII/CD23)
Fig. 2.; Lesional skin of atopic dermatitis patients exhibits an increased number of CD1a+ cells belonging to the dendritic cell lineage. ADl*esional skin was stained with anti-CD1a monoclonal antibody and a three-step avidin-biotin perox< idase complex amplification system
S&
. Pastore et al.: Pathogenesis of Atopic Dermatitis 5701

I�gE receptors, with the former being the principal IgE-
-binding receptor. Interestingly enough, the Fcε RI ex-p� ressed by epidermal LC and DC differs from thec� lassical receptor expressed on mast cells because itlacks the β chain, but it is fully functional in transduc-ing an intracellular activation signal and enhancing thea� llergen internalization and presentation to T cells3
%0.
A positive feedback loop of increased IgE productiona� nd further aeroallergen presentation may be very im-p� ortant for the amplification of local response to anti-g� ens.
Recently, the authors have shown that keratinocytesc� ultured from AD patients display enhanced GM-CSFg� ene expression and produce, spontaneously or afterstimulation, high amounts of GM-CSF compared withk
4eratinocytes from nonatopic controls. In addition, con-
d�itioned medium from stimulated AD keratinocyte cul-
t�ures could support the differentiation of CD1a+ DC
f�rom peripheral blood precursors3
%9. A higher release of
G:
M-CSF can considerably contribute to in situ LC andD
�C recruitment, survival and maturation into highly
e fficient antigen-presenting cells. It is thereforep� ossible to postulate that, as precursors pass through themilieu of AD skin, they are induced to differentiate intoD
�C by GM-CSF and IL-4 provided by activated kerati-
nocytes and mast cells, respectively. In this way, in-c� reased concentrations of GM-CSF at the skin levelc� ould explain the persistent infiltration of activated DCin AD skin. Finally, the large number of activated DCp� resent in AD may be directly involved in the estab-l
3ishment and perpetuation of inflammation through the
release of proinflammatory molecules such as IL-6,I
�L-1β, TNF-α and an array of chemokines9
=.
Role of Eosinophils and Mast Cells
V>
arious studies point to a major role of eosinophilsa� s potent effector cells by releasing chemical mediatorsa� nd cytotoxic granule proteins such as eosinophil ca-t
�ionic protein, eosinophil peroxidase, major basic pro-
t�ein and eosinophil-derived neurotoxin/eosinophil pro-
t�ein X. Although eosinophils are not prominent in theAD infiltrate, they can be easily localized in closep� roximity to mononuclear cells in chronic lesions10. Ina� cute skin lesions, extensive extracellular deposition ofe osinophil major basic protein suggests that degranula-t
�ion has occurred, and several studies have showna� correlation of serum eosinophil cationic protein con-c� entration with disease activity20, 36. Recently, it hasb
�een shown that eosinophils can be actively induced by
Th2-type cytokines, including IL-4, to release IL-12,
a� cytokine that may contribute to precipitate the later,Th1-dominated phase of the disease12. Moreover, pe-ripheral blood eosinophilia in early childhood is asso-c� iated with subsequent development of atopic diseases,w� hich further points to an important role of eosinophila� ctivation3
%. Strikingly, delayed programmed cell death
h�as been reported to occur for circulating eosinophils
in AD, probably mediated by an increased autocrinep� roduction of GM-CSF and IL-55
�1. Because mature,
c� irculating eosinophils are terminally differentiatedc� ells incapable of proliferation and self-renewal, regu-lation of eosinophil survival may represent a majorm echanism through which functional eosinophils accu-mulate at inflammatory sites.
M?
ast cells have been shown to participate in thei
�mmediate hypersensitivity reaction, where the cross--linking of the membrane IgE-receptors by allergensleads to the synthesis and release of a variety of proin-f
�lammatory mediators (Fig. 1). This release determines
t�he acute weal and flare reaction visible in skin prick
t�ests. In acute lesions, mast cells are normal in number
b�ut are in different stages of degranulation. In chronic
lesions, there is a significant increase in mast cell num-b
�er, especially in areas of lymphocytic infiltration in the
p� apillary dermis17, as to indicate a dependence on thep� resence of functional T cells. In turn, mast cells con-t
�ribute to the recruitment of inflammatory cells by re-
leasing preformed TNF-α, which is crucial for endothe-lial cell activation, and to condition the local cytokinee nvironment toward a Th2 promotion, since they arem ajor sources of IL-416.
Conclusions
AD is a complex and heterogeneous disorder whosee xpression is dependent upon several mechanisms, in-c� luding antigen-specific immune responses and inflam-m atory reactions elicited by non-antigenic environmen-t
�al factors. Increasing evidence suggests that resident
skin cells are major players of AD pathogenesis andrespond with exaggerated production of proinflamma-t
�ory mediators to various activation signals. The un-
folding of the molecular mechanisms that underlie suchr' esponses will permit the development of more effica-c� ious strategies for disease prevention and management.
References
1. AK@
DIS M., AK@
DIS C. A., WEA
IGL L., DIBSCH R. and BL
CASER K.
(D1998): Skin-homing, CLA+ memory T cells are activated in
a/ topic dermatitis and regulate IgE by an IL-13-dominated cyto-
5702 S
&. Pastore et al.: Pathogenesis of Atopic Dermatitis

kine pattern: IgG4 counter-regulation by CLA-memory T cells.J. Immunol., 159, 4611–4619.
2. BAE
RNES K. C. and MAE
RSH D. G. (1998): The genetics andcomplexity of allergy and asthma. Immunol. Today, 19, 325–332.
3. BOF
RRES M. P., ODG
ELRAM H., IRH
ANDER K., KJIELLMAN N. I. and
BJIORKSTEN B. (1995): Peripheral blood eosinophilia in infants
at 3 months of age is associated with subsequent developmentof atopic disease in early childhood. J. Allergy Clin. Immunol.,95, 694–698.
4. BRATTON D. L., HAMID Q., BOF
GUNIEWICZ M., DOF
HERTY D. E.,KA
EILEY J. M. and LE
AUNG D. Y. M. (1995): Granulocyte macro-
phage colony-stimulating factor contributes to enhanced mono-cyte survival in chronic atopic dermatitis. J. Clin. Invest., 9
J5,�
211–218. 5. CO
FLEMAN R., TR
HEMBATH R. C. and HA
ERPER J. I. (1997):
Genetic studies of atopy and atopic dermatitis. Br. J. Dermatol.K ,�136,� 1–5.
6. COF
OPER K. D. (1994): Atopic dermatitis: recent trends in pa-thogenesis and therapy. J. Invest. Dermatol., 102, 128–137.
7. COF
X H. E., MOF
FFATT M. F., FAUX J. A., WALLEY A. J., COF
LE-
MAN R., TREMBATH R. C., COF
OKSON W. O. and HARPER J. I.(1998): Association of atopic dermatitis to the beta subunit ofthe high affinity immunoglobulin E receptor. Br. J. Dermatol.K ,�138,� 182–187.
8. DAUD L. R., GARRALDA M. E. and DAVID T. J. (1993): Psy-chosocial adjustment in preschool children with atopic eczema.Arch. Dis. Child., 69,� 670–676.
9. DL
EA SA
EINT-VI
BS B., FU
MGIER-VI
BVIER I., MA
ESSACRIER C., GA
EILLARD C.,
VANBERVLIET B. and Aït-YAHIA S. (1998): The cytokineprofile expressed by human dendritic cels is dependent oncell subtype and mode of activation. J. Immunol., 160,� 1666–1676.
10. DE VRIES J. E. and PUM
NNONEN J. (1993): Regulation of humanIgE response by IL-4 and IL-13. Res. Immunol., 144, 597–601.
11. FIBNLAY A. Y. and KH
NAN G. K. (1994): The dermatology life
quality index: a simple practical measure for routine clinicaluse. Clin. Exp. Dermatol., 19, 210–216.
12. GREWE M., BRUIJNZEEL-KOF
OMEN C. A. F. M., SCO
HÖPF E.,TH
NEPEN T., LA
ENGEVELD-WI
BLDSCHUT A. G., RU
MZICKA T. and
KRUTMANN J. (1998): A role for Th1 and Th2 cells in the im-munopathogenesis of atopic dermatitis. Immunol. Today, 1
P9,�
359–361.13. HAMID Q., BO
FGUNIEWICZ M. and LEUNG D. Y. M. (1994): Dif-
ferential iQn situ cytokine gene expression in acute versus
chronic atopic dermatitis. J. Clin. Invest., 9J
4, 870–876.14. HO
FFER M. F., HARBECK R. J., SC
OHLIEVERT P. M. and LEUNG
D. Y. M. (1999): Staphylococcal toxins augment specific IgEresponses by atopic patients exposed to allergen. J. Invest. Der-matol., 112, 171–176.
15. HOF
PKIN J. M. (1997): Mechanisms of enhanced prevalence ofasthma and atopy in developed countries. Curr. Opin. Immu-nol., 9,� 788–792.
16. HOF
RSMANHEIMO L., HARVIMA I. T., JÄRVIKALLIO A., HARVIMA
R. J., NAE
UKKARINEN A. and HOF
RSMANHEIMO M. (1994): Mastcells are one major source of IL-4 in atopic dermatitis. Br.J. Dermatol., 131,� 348–353.
17. IRH
ANI A. M., SAE
MPSON H. A. and SCO
HWARTZ L. B. (1989):Mast cells in atopic dermatitis. Allergy, 44,� (suppl. 9), 31–34.
18. JOF
NES M. J. and MUM
RRAY A. W. D. (1995): Evidence that ce-ramide selectively inhibits protein kinase C-alpha translocation
a/ nd modulates bradykinin activation of phospholipase D. J.Biol. Chem., 270, 5007–5013.
19. JUM
RGHANS V., GUM
TGESELL C., JUM
NG T. and NEA
UMANN C.(D1998): Epidermal cytokines IL-1β
R,� TNF-αS ,� and IL-12 in pa-
t.ients with atopic dermatitis: response to application of house
d1ust mite antigens. J. Invest. Dermatol., 111, 1184–1188.
20. KAPP A., CZECH W., KRUTMANN J. and SCO
HÖPF E. (1991): Eo-s+ inophil cationic protein in sera of patients with atopic der-matitis. J. Am. Acad. Dermatol., 24, 555–558.
21. KAE
TAGIRI K., ITT AMI S., HAE
TANO Y. and TAE
KAYASU S. (1997):Increased levels of IL-13 mRNA, but not IL-4 mRNA, arefUound i
Qn vivo in peripheral blood mononuclear cells of patients
wV ith atopic dermatitis. Clin. Exp. Immunol., 108,� 389–394.22. KH
NURANA-HE
ARSHEY G. K., FR
HIEDRICH M. F., ES
WSWEIN L. A.,
THOMAS M. L. and CHATILA T. A. (1997): The association ofa/ topy with a gain-of-function mutation in the αS -subunit of theIL-4 receptor. N. Engl. J. Med., 3
X37, 1721–1725.
23. KOF
NDO H., ICO HIKAWA Y. and IMOKAWA G. (1998): Percuta-nY eous sensitization with allergens through barrier-disrupteds+ kin elicits a Th2-dominant cytokine response. Eur. J. Immu-nol., 28,� 769–779.
24. LEUNG D. Y. M. (1995): Atopic dermatitis: the skin as a win-d1ow into the pathogenesis of chronic allergic diseases. J. Al-
lergy Clin. Immunol., 9J
6, 302–319.25. LE
AUNG D. Y. M. (1997): Atopic dermatitis: immunobiology
a/ nd treatment with immune modulators. Clin. Exp. Immunol.,1P
07 (suppl. 1), 25–30.26. LEUNG D. Y. M., WO
FOD N., DU
MBEY D., RHODES A. R. and
GZ
EA
HA R. S. (1983): Cellular basis of defective cell-mediatedlympholysis in atopic dermatitis. J. Immunol., 130,� 1678–1682.
27. LEWIS-JOF
NES M. S. and FINLAY A. Y. (1995): The children’sd1ermatology life quality index (CDLQI): initial validation and
p2 ractical use. Br. J. Dermatol., 132, 942–949.28. MAO X. Q., SHIRAKAWA T., YO
FSHIKAWA T., KAWAI M., SASA-
KI S., EN[
OMOTO T., HASHIMOTO T., FUM
RUYAMA J., HOF
PKIN J. M.a/ nd MO
FRIMOTO K. (1996): Association between genetic vari-
a/ nts of mast-cell chymase and eczema. Lancet, 3X
48, 581–583.29. MA
EREKOV L. N. and ST
TEINERT P. M. (1998): Ceramides are
b,ound to structural proteins of the human foreskin epidermal
c\ ornified cell envelope. J. Biol. Chem., 2]73, 17763–17770.
30. MAURER D., FIEBIGER S., EBNER C., REININGER B., FISCHER
GZ
. F., WIBCHLAS S., JO
FUVIN M. H., SC
OHMITT-EG
^ENOLF M.,
KRAFT D., KINET J.-P. and STINGL G. (1996): Peripheral bloodd1endritic cells express Fcε_ RI as a complex composed of Fcε_ RI αS
a/ nd Fcε_ RΙγ`
chains and can use this receptor for IgE-mediateda/ l lergen presentation. J. Immunol., 157,� 607–616.
31. MCO CO
FY J. P., HANLEY-YANEZ K., MC
O CASLIN D. and THARP
M. D. (1992): Deletion of decreased cytotoxic effector CD8+Ta
lymphocytes in atopic dermatitis by flow cytometry. J. Al-lergy Clin. Immunol., 9
J0, 688–690.
32. MOF
CHIZUKI M., BAE
RTELS J., MAE
LLET A. I., CHN
RISTOPHERS E.a/ nd SC
OHROEDER J.-M. (1998): Interleukin 4 induces eotaxin:
a/ possible mechanism of selective eosinophil recruitmentin hel-minth infection and atopy. J. Immunol., 160, 60–68.
33. MUM
RATA Y., OG^
ATA J., HIBGAKI Y., KA
EWASHIMA M., YA
EDA Y.,
HIGUCHI K., TSW
UCHIYA T., KAWAINAMI S. and IMOKAWA G.(D1996): Abnormal expression of sphingomyelin-acylase in atopic
d1ermatitis: an etiologic factor for ceramide deficiency? J. In-
vb est. Dermatol., 1P
06, 1242–1249.34. NISHIZUKA Y. (1992): Intracellular signaling by hydrolysis of phos-
p2 holipids and activation of protein kinase C. Science, 258, 607–614.
9=
– Archivum Immunologiae... 6/2000
S&
. Pastore et al.: Pathogenesis of Atopic Dermatitis 5703

3c5. OH
NMEN J. D., HA
ENIFIN J. M., NI
BCKOLOFF B. J., RE
AA T. H.,
WYZYKOWSKI R., KIM J., JUM
LLIEN D., MCO HU
MGH T., NASSIF
A. S., CHN
AN S. C. and MOF
DLIN R. L. (1995): Overexpressionof IL-10 in atopic dermatitis. J. Immunol., 154, 1956–1963.
3c6. PAGANELLI R., FANALES-BELASIO E., CARMINI D., SC
OALA E.,
MEA
GLIO P., BUM
SINCO L. and AIBUTI F. (1991): Serum eosinophil
cationic protein in patients with atopic dermatitis. Int. Arch.Allergy Appl. Immunol., 9
J6,� 175–178.
3c7. PASTORE S., CAVANI A. and GIROLOMONI G. (1996): Epidermal
cytokine and neuronal modulation of contact hypersensitivityreactions. Immunopharmacology, 31, 117–130.
3c8. PA
ESTORE S., CO
FRINTI S., LA
E PLC
ACA M., DIBDONA B. and GI
BRO-
LOMONI G. (1998): Interferon-γd promotes exaggerated cytokineproduction in keratinocytes cultured from patients with atopicdermatitis. J. Allergy Clin. Immunol., 101, 538–544.
3c9. PA
ESTORE S., FA
ENALES-BE
ALASIO E., AL
CBANESI C., CH
NINNI L. M.,
GIANNETTI A. and GIROLOMONI G. (1997): Granulocyte macro-phage colony-stimulating factor is overproduced by keratino-cytes in atopic dermatitis. J. Clin. Invest.K , 9
J9, 3009–3017.
40. PETERING H., HÖe
CHSTETTER R., KIMMING D., SMOLARSKI R.,KAPP A. and ELSNER J. (1998): Detection of MCP-4 in dermalfibroblasts and its activation of the respiratory burst in humaneosinophils. J. Immunol., 1
P60, 555–558.
41. RING J., DARSOW U., GFESSER M. and VIELUF D. (1997): The“atopy patch test” in evaluating the role of aeroallergens inatopic eczema. Int. Arch. Allergy Immunol., 113, 379–383.
4f2. RO
FUSSET F., RO
FBERT J., AN
[DARY M., BO
FNNIN J. P., SO
FUILLET
G., CHRÉTIEN I., BRIERE F., PENE J. and DE VRIES J. E. (1991):Shifts in IL-4 and IFN-γd production by T cells of patients withelevated serum IgE levels and the modulatory effects of theselymphokines on spontaneous IgE synthesis. J. Allergy Clin. Im-munol., 87, 58–69.
4f3. RU
MDIKOFF D. and LE
ABWOHL M. (1998): Atopic dermatitis. Lan-
cet, 3X
51, 1715–1721.44. RYSTEDT I. (1985): Hand eczema and long-term prognosis in
atopic dermatitis. Acta Derm. Venereol., 1P
17, 1–59.45. SALLUSTO F., LANZAVECCHIA A. and MACKAY C. R. (1998):
Chemokines and chemokine receptors in T-cell priming andTh1/Th2-mediated responses. Immunol. Today, 19,� 568–574.
4f6. SC
OHÄFER T. and RI
BNG J. (1997): Epidemiology of allergic dis-
eases. Allergy, 5 (suppl. 38), 14–22.4f7. SE
AGUCHI T., CH
NANG-YI
B C., KUM
SUDA S., TAE
KAHASHI M., AIBSU
K. and TEZUKA T. (1996): Decreased expression of filaggrin inatopic skin. Arch. Dermatol. Res., 288,� 442–446.
48. STT
RICKLAND I., HAE
UK P. J., TRH
UMBLE A. E., PIBCKER L. J. and
LEUNG D. Y. M. (1999): Evidence for superantigen involve-mg ent in skin homing of T cells in atopic dermatitis. J. Invest.Dermatol., 112, 249–253.
49. THESTRUP-PEDERSEN K. (1997): Atopic dermatitis. In BOF
S J. D.(Ded.): Skin immune system. 2nh d Edition. CRC Press, Boca
Raton, FL, 498–507.50. VAN DER PLOEG I., JEDDI TERANI M., MATUSEVICIENE G.,
Wi
AHLGREN C. F., FRANSSON J. and SCO
HEYNIUS A. (1997): In-t.erleukin 13 overexpression in skin is not confined to IgE-med
1ia-
t.ed skin inflammation. Clin. Exp. Immunol., 109,� 526–532.
51. WEA
DI B., RAE
AP U. and KAE
PP A. (1997): Delayed eosinophilp2 rogrammed cell death in vitro: a common feature of inhalanta/ llergy and extrinsic and intrinsic atopic dermatitis. J. AllergyC�
lin. Immunol., 97, 536–543.52. WI
BLLIAMS H., RO
FBERTSON C., ST
TEWART A., Aït-KH
NALED N.,
ANABWANI[ G., ANDERSON
[ R., SHER I., BEASLEY R., BJORKSTENI
B., BURRM M., CLAYTON T., CRANE J., ELLWOOD P., KEIL U.,
L�
AIE C., MALLOL
E J., MARTINEZE F., MITCHELL
B E., MANTEFORTE S.,
PEARCE N., SHAH J., SIBBALD B., STRACHAN D., VONj MUTIUS
M
E. and WEILAND S. K. (1999): Worldwide variations in the pre-valence of atopic eczema in the international study of asthmab
a/ nd allergies in childhood. J. Allergy Clin. Immunol., 103,125–138.
53. WOF
LLENBERG A., KRH
AFT S., HAE
NAU D. and BIBEBER T. (1996):
Immunomorphological and ultrastructural characterization ofL�
angerhans cells and a novel, inflammatory dendritic epidermalc\ ells (IDEC) population in lesional skin of atopic eczema. J. In-vb est. Dermatol., 106, 446–453.
54. WOF
OD L. C., ELIAS P. M., CALHOUN C., TSW
AI J. C., GRUNFELD
C�
. and FEINGOLD K. R. (1996): Barrier disruption stimulatesiknterleukin-1αS expression and release from a pre-formed pool
ikn murine epidermis. J. Invest. Dermatol., 1
P06, 397–403.
55. YING S., TABORDA-BARATA L., MENG Q., HUM
MBERT M. andKAY A. B. (1995): The kinetics of allergen-induced transcrip-t.ion of messenger RNA for monocyte chemotactic protein-3
a/ nd RANTES in the skin of human atopic subjects: relationshipt.o eosinophil, T cell, and macrophage recruitment. J. Exp.
Med., 181,� 2153–2159.
Received in October 1999Accepted in December 1999
5704 S
&. Pastore et al.: Pathogenesis of Atopic Dermatitis