Embed Size (px)
Citation preview

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 1/213

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 2/213
Atlas
of
Neurosurgical Anatomy

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 3/213
John L
Fox
Atlas
of
Neurosurgical
Anatomy
The
Pterional Perspective
With a Contribution
by
Bengt Ljunggren
Illustrated
by
David M. Klemm
With 171 Illus
tr
a
ti
ons in 329 Parts, 133 in
Full
Color
Springer-Verlag New York Berlin Heidelberg
London Paris Tokyo

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 4/213
JN tN L. Fox,
M.D.
Clinical Professor of Surgery. Division of Neurosurgery, Uni"ersity of Nebraska Medical
Center, Omaha, NE68105,
USA
H
ENG
T LJUNGGREN, M.D.
Professor. Department of Neurosurgery, Uni,'ersity Hospital, Uni,'crsity of Lund, 22185
Lund,Sweden
Illttilmtor
D
AV
ID M.
K LEMM
Medical lIIustralOr.
Ed
ucational l\led ia Production and Services. GeorgelOwn University
Medical Center, Washington, DC 20007, USA
Portions of the work on this atl
as
were carried OUI by
Dr.
J.L.
Fox
at the following institu
tions: University
of
Zurich, Zurich, Swiuerland (1973-1974
);
West Virginia University Med·
ical
Center. Morgantown. West Virginia (1975-1982); King
Faisal
Specialist
Hosp
ital and
Re
search Centre, Ri
ya
dh, Saudi Arabia (1983-1985); Georgetown Unil'ersity Medical Center,
Wa shington. D
.C.
(1985-1987); and University
of
Nebraska
1-.ledic
al Center. Omaha,
Ne
braska (1987 -1988). The senior author is grateful for their suppor t in this academic en·
deavor.
On IM/TQnl coveT: Fig. 7. 13/p. 138.
Library of Congress Cataloging-in-Publication Data
F
ox,
John L.
,
1934-
Atlas of neurosurgical anatomy: the plerional perspective f John
L. Fox with a contribution by Hengl Ljunggren ; illustrated by David
M. Klemm.
p. cm.
Includes bibliographies and
in
dex.
\. Brain-Anatomy-Atlases. 2. Brain-Surger
y -
Atlases.
[. Ljunggren, SengI.
II.
Title.
[D
NLM:
. Nervous Syslem-anatomy
&
histology -atlases.
2. Nen'ous Sys tem-surgery-atlases. WL 17 F792aJ
QM
455.
F6
5
1989
61
18-dcl9
DNLMIDLC 88·39319
Printed
on add·free
paper
o3:l 1989 by Springer-Verlag New \or
lo:
I
nc.
Softcovcr repri
nt oTlllc
hardcover
1st edition 1989
All rights reserved. This work may not
be
translated or
co
pied
in
wbole or
in
pan without
the writlen permission
or
the publisher (Springer-Verlag, 1
75
Fifth A"enue,
New York
,
NY
100
[0. USA),
except for brief excerp
ts
in connection
with
reviews
or
scholarly analysis.
Use
in
connection
with
any form of information storage and retrieval, electronic adaptation,
computer software,
or
by similar
or
dissimilar methodology
now
known
or
hereafter de·
"e1o
ped is forbidden.
The use of general descriptive names, trade names, trademarks, etc.
in
this publication,
even if the former are not
e s p e i
identified, is not to
be
taken
as
a sign that such names,
as
understood
by
the Trade Marks and Merchandise Marks Act , m
ay
accordingly
be
used
freely
by
anyone.
While the advice and information
in
this book are believed to be trueand accuratealthe date
of
go
ing to pre
ss,
neilher the authors nor the editors nor the publisher can acce pt any legal
responsibility for any errors or omissions that
ma
y
be
made.
Th
e publisher makes no ,,'ar·
ranty, express
or
implied. with respect to the material contained herein.
Typeset, printed, and bound
by
Universitatsdruckerei H. Sturtz AG. Wunburg, Federal
Republic of Germany.
9 8
7 6 5
4 3 2 1
lSBN- 13: 978 -1-4613-8825-8
00[:
10 .1007/978-1-4613-8823·4
e
-[
SBN -1 3: 978-1-4613-8823-4

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 5/213
Dedicated
to James Winston
Watts,
M.D.,
Professor
Emeritus,
Department
of
Neurological
Surgery, George
Washington University
Medical
Cente'r,
Washington,
D.C.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 6/213
Foreword
During the past 15 years, several publications
on
neurosurgical tech
niques, often with special emphasis
on
surgical
ana
tomy. have
appeared
in the literature. Howevel; this book by J
ohn L.
Fox goes far beyond
an
ordinary
effort.
Thi
s extraordinary work,
Allas ofNeurosurgical Anat011o/:
The
Pte1'ional
Perspective, has its or igins in the author's many years of devo
tion, exhaustive labors, and experience
as
a teacher in the operating
theater (to
wh
ich
hi
s many residents
will
attest). This surgeon, born in
Bill ings, Montana, in the ycar of 1934, a
uthore
d
one
of his first publica
tions as a seni or resident in 1964. The tide, "Differentiation of Aneurysm
from Infundibulum of the Posterior Communicating Artery," presaged
his future recognition as an intracran i
al
aneu rysm surgeon. Now Profes
sor Fox is known throug h
out
the world not only for his many publica
tions
on
su
bj
ects in neuroscience
and
clinical neurosurgery,
but
also for
his teaching methods, which utilize both television demonstrations and
color slides
of
live neurosurgical anatomy in realistic
depth and
clarity.
Such talents as a teacher have led J ohn Fox to be ca
lled
forth as an in
structor
and
lecturer in many neurosurgical seminars
and
courses both
here and abroad, East and West. His presentations with color photo
graphs showing true visual images now are capt
ure
d with perfection in
this atlas. Such
photograp
h
s,
wit h accompanying instructions
and
de
scriptions on
approaches
to aneurysms and tumors, have left a promi
nent
and
lasting impression on everyone who has had the opportunity
to
attend his lectures.
This
book gives us images in living color, images curremly unsur
passed by any other work and well illustrated as the su rgeon actually sees
them.
The
excellent accompanying and instructive drawings help
car
ry
the reader and
observer step
by
step through the
intricacies
of
cis
ternal
anatomy
and
pathways of intracranial s
urger
y.
Thi
s publication is di
vided into eight chapters, starting with the history of the pterional ap
proach in neurosurgery. The inclusion of this interesting and instructive
chapter
gives us an added evolutionary insight. It is co-
authored
by Pro
fessor B
engt
Ljunggren, whose interest
and expert
ise in neurosurgical
history
and
aneurysm
surgery are
well known. Professor Ljunggren,
from the University Hospital of Lund in Sweden, fascinates the
reader
with his accounts of the early evolut ion of techniques for
turning
the cra
nial
fl
ap. The next
three
c
hapler
s by Dr. Fox carry us
through
inst
rum
en
tation
and
positioning, photographic technique,
an
d cran ial anatomy.
His final
four
c
hapter
s take us from the sylvian fissure into
and th r
ough

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 7/213
VIII
Foreword
the carotid, chiasmatic, and inter pedu ncu lar cisterns and their en virons.
Such anato my could never be so we ll illustrated before the days of the
o
per
ating microscope.
I have fo llowed the career of john
Fo
x for nearly
30
years, including
the time since his days as a student
and resident at the George
Wash
ington
Un
i
ve
rs
it
y
Me
dical Cent
er
throu gh his appointment
as
Pro
fessor
of
Neurological Surgery at the same institution in Washington,
D.C., on Ju ly I, 1974. Subseque nt yea rs have shown that Professor Fox
not
only is singularly and eminently qualified and gifted
as
an author of
such an a
tl
as,
but
also continues to h
ave
the
ene
r
gy
and
dr
ive to give fu
ture students, anatomists, neurologists, and neurosurgeons such a
la
st
ing work on intracranial s
urgery via the pt
er
ional perspec ti ve.
L UDWIG G. K EMPE, M.D.
Professo r of Ne urol
og
ical Surgery and
Research Professor of Anatomy
UniversityofSouth
Caro
lina
Charleston, South Carolina

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 8/213
Preface
After completing a three-volume book entitled
inlmcranial Aneurysms
published by Springer-Verlag in 1983, this authorcominued to compile a
set of
surg
ical photographic s
li
des
that
served
we ll
for teaching anatomy
at neurosurgical rounds, meetings, and workshops. But preservation
of
these images for future
sLUden
ls required their publication in a more
permanent form. The plerional approach to cenain imracranial prob
lems is being used with increasing frequency, and the photographs pre
sented here give us the plerionai,
or
frontolateral, perspective - a per
spective that is turned upside-down and obliqued
in
comparison with
most standard anatomical illustrations.
Yet
, th is is the vlew as seen by the
neurosurgeon. For ease
of
comparison, all photOgraphs are oriemed as
if a right-sided operation
is
being performed.
In one sense, this atlas becomes "volume 4"
of
Intracmnial
Aneury
sms.
However, em phasis
is
on live anatomy and its va riations rather than on
pathology. h is for this reason that this author omitted cases with basal
tumors, for such masses often distort and compress the vessels and cra
nial nerves beyond dear recognition.
The earthly finality
of
death
is
m
it
igated
by
the deeds one does during
hi s or her lif
e.
One then leaves behind the results
of
interaction with
others. As physicians
we
hope to have mostly benefined our patients.
Sometimes we
fail. This atlas
nOl
only is
in
memory
of
those failures. but
also is a photographic epitaph
of
some of those very patiems, however
few
in number. For the many patients who survive the neurosurgeon's
hand and return home to family, the sur geon can gain more than any
ephemera l fame,
fonune
,
or fe
eling
of
"well done."
The
neurosurgeon,
more importantly, can be both a catalyst inspiring younger surgeons to
greater heights and a teacher leav ing behind works upon which others
can build.
The
a
uthor
, the con tributor to the c
hapt
er
on
hi
story, and the
ar tist hope that this atlas will serve such lasting purposes.
J owe a debt
of
gratitude to my friend and colleague Professor Bengt
Ljunggren at the Departmem
of
Neurosurgery of the University Hospi
tal,
The
University
of
Lund, Swede
n.
Beginning with the 1889 work
of
the German surgeon
Wi
lh elm Wagner. Professor Ljunggren contributes
a vital perspective to the history in Chapter 1. Special credit is
due
to
David
M.
Klemm, medical ill
ustraLOr
at the Georgetown University Med
ical Cemer in Washington, D.C., where I carried out
part
of the work on
this book. He drew and labeled a ll the illustrations that accompany the
color photographs.
JOHN L. Fox

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 9/213
Contents
Foreword
by
LUDWIG C. KEMPE.
Preface . . . . . . . . .
History of
the
Pterional
Approac
h
BENGT
LJUNCGREN and JOHN L. Fox
2 Instrumentation and Positioning
3 Photographic Technique . . .
4 Cranial Anatomy and the Cranial Flap
5 The S),lvian Fissure
6 The Carotid Cistern and Environs.
7
The
Chiasm
at
ic Cist
ern and
Environs
8
The
Ambient and I nterpeduncular Cisterns
In d ex
VII
IX
11
33
37
55
93
123
165
20
1

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 10/213
1
History of the Pterional Approach
BENGT LJUNGGREN and
JOHN
L.
Fox
Introduction
Many surgical a
pproach
es have
been
proposed
in order to facilitate
exposure
of lesions in
the
skull-base reg ion wi th a minimum of brain re
traction [I, 3, 12, 15, 18, 19,24,29,32-34,37,
39, 40, 49]. The pterional approach [ the cir
cle ofW
illi
s
and
its environs is routinely used by
many surgeons. A
pt
erional ap proach implies
that a small skull flap is raised with the pterion
(Creek
pterion,
wing [ II
])
- the craniom
et
ric
point located undern eath the tcmporalis mus
cle a
nd
formed by the junction of
the
frontal,
parietal, and te
mpor
al bones with the grea t
s
ph
enoid
wi ng
bone
-
in
the ce
nt
er
of
the base
of the flap (Fig.
1.1
). Additional drilling
do
wn
of
the
sphenoid ridge allo
ws
a
lo
w basal expo
s
ure
along the skull base. Equipped with
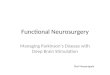
Fig. 1.1. Close-u p view of left
side of
dr
y sku ll with sutu
res
betwee
n the frontal (F),
parietal
(P),
temporal (1),
sphenoidal (S), and zygomatic
( l) bones outli ned by black
ink .
today's microsur gical instruments, the
neurosurgeon finds that the pterional ap
pr
oach to skull-base lesions is a more natural
and easier procedure
than
earlier-day
opera
tions. Yet, there is a fascinating hiSlOrica l back
ground over the last 100 years, that forms the
basis of the present-day
pteriona
l approach.
There are
several pi
onee
rs w
ho
made mo
nu
mental contributions to the development of
this access to deep-seated cran ial-base lesions.
Wilhelm Wagner and His
Osteoplastic Method
following studies on human cadavers for sev
er al years, Wilhelm Wagner (1848-1 900)
be
came the first su rgeon in the world to raise a

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 11/213
2
I. Hi
slOry of the Pterional Approach
bo
ne flap (temporal in site)
out
of the cra
ni
al
vault in a l
iv
in g
per
son , kee p
it
attached to the
o
ve
rly
in
g s
of
t
tiss
ue (per
io
steum, te
mpor
al
mus
cl
e,
and
scalp
),
and then re
pl
ace the
fl
ap
(a
fter evacuation of a la rge ep idural
hematom
a)
[4, 44
].
Wagner used hamm
er
and
chisel to raise the bone flap.
Th
e patient , a 27-
year-old man with skull-base frac
tu r
es and the
clinical pic
tu r
e of increas
in
g intracranial pres
sure, under
we
nt surgery on the second d
ay
fol
lo
wing a severe head
in
jury. He
was in
a p
oo
r
condition prior
to th
e operation. Following
evacua
ti
on of the hematoma,
it was
apparent
thal the int racranial
pr
essure had become nor
ma
lize
d ,
bUl
the patient did not recover and
d
ie
d
24
hou
rs
af
ter
surger
y.
At autop
sy
Wa
gner found no signs of
di st ur
bed
nut
r
iti
on
in the temporal, om
eg
a
-s
haped
fl
ap that he
had rai
se
d to allow e
va
cu
at
ion of the now-ab
se nt hematoma. He conclude d that h is osteo
pl
as
ti
c method
was
an exce
ll
ent proce
du
re that
res
ul
ted in a good exposure
of
lacerat ions
of
the middle me
ni
nge
al
a
rt
ery in the middle cr
a
ni
al fo ssa. He
al
so suggested that
hi
s osteo
plas
ti
c method could be used to ex pl ore and re
sect other intracranial lesions such as brain
abscesses, epileptic scar
s,
and brain tumors
[44
].
T
wo
years later (1891 ) Wagner rightly
cl
aimed prio rity for the intro
du
ction of the u
se
of
the above-described, intrao
per
at
ive osteo
plastic bone flap to ex
pl
ore intracranial le
sion
s.
He emphasized that such
fl
aps
ap
peared
to heal quic
kl
y and without complications
when attachment
to
the
so
ft tissue
was
retained
durin
g surgery [45]: The osteopl
as
tic method
of
tr
epanat ion is no morc difficult or da nger.
ous than an explo rat ive l
ap
aroto
my.
"
In 1895 Wagner publi shed t
wo
cases
of
suc
cessful evacuation of e
pidur
al hematom
as
t
hrou
gh h
is
then innovati
ve
osteoplastic proce
dure
. In this paper
[4
6) he again emphasi
;r.e
d
the ad
va
ntages associated with te
mp
ora
ry re
section of a large bone fl
ap for cx
pl
orat
io
n of
the middle meningeal branches.
In 1909 Harvey Cushing
[5]
described
Wagne r
's
original
pr
oce
dur
e to explore and
deco
mp
ress cere
br
al lllmors, w
hi
ch otherwi
se
pro
ve
d to be inopera
bl
e, using the usual os
teo plas tic method of exploration
.
He sum
m
ar
ized [5]: osteo
pl
ast
ic
resec
ti
on, what
ev
er
tools m
ay
be employed , has doubtless
come to be made, in the hands of a ll , under
some form of
tourniquet, with the om
eg
a
shaped
fl
ap broken off across the thin squa
mous win g of the temporal bone .
Wagner
was
a self-edu cated surgeon who,
like his great contemporary co lleague from
Be rlin, Ernst von Bergmann
1907),
had been in volved in the Franco-Pru
ss
ion
Wa
r
in 1870. He devoted h is life to working in the
local hospita l
of
Kon igs
hou
e, a sma
ll tow
n in a
mining d is trict in Upper Silesia, w
hi
ch in 1880
cou nted 27,600 inhabitant
s. Si
l
es
ia at this time
was
incorporated into the newly founded Ge
r
man Reich. In thi s sma
ll
place Wagn
er
became
an absolute master s
ur
geon, and like
vo
n
Bergmann he exhibited a particul ar interes t in
cranial and sp inal surgery. While von
Be rg
mann st
rong
ly o
bj
ected to the use of
opening the skull with chisel and ma
ll
et. t
hi
s
was
the technique s
up
erbly prac
ti
ced by
Wagne
r. T he l
attcr
al
so
pu
bl
is
hed importa
nt
contributions concerning the opera
ti
ve man
agement of compli
ca
ted sku
ll
fra
ctlll"
es
[4
3]
and on fracture
di
slocations in the cervi
ca
l
sp in e [47]. Hi s re port on the cli nical diagnosis
and operati
ve
evacuation of e pidural
he matomas is a master piece [46] .
Th
e sa me ca n
be said
of
the remarkable
vo
lume, "
Di
e
Ve
rlet
zu
ngen der Wirbelsaule und des Rocken
marks" [47] which he pub lished in collabora
ti
on
with
hi
s co
lleag
ue Stolper from nea
rb
y
Br
es
lau (Wroclav). D
espi te
a heavy clini
ca
l
da
il),
practice, he not o
nl
y kep t abreast with the
surgical
li
terature of the lim e
but
also followed
the
li
tera
tu
re in
ge
neral med ici ne and other re
lated branches . Wa gner was belo
ve
d by hi s pa
tients, for he radiated security and goodness
and was wide ly recogni zed in the whole of
S
il
esia not o
nl
y for
hi
s supreme s
kill
but also
for
hi
s vast medical kn
ow
ledge and h
is
good reo
s
ui ts
in the treat
me
nt of nons
ur
g
ic
al d iseases.
C
rani
a] Saws
In 1891 Professor
("
professe
ur
a la
Fac
uitc
libr
e
) Jean Toison from
Lill
e in France re
poned on h is use of a chain
saw
to divide the
bone between b
urr
holes from within
ou t
w
ard
to fac
ili
tate raising of
os
teopl
as ti
c sku ll
fl
aps
[38]. Th is saw could repl ace hammer and
c
hise
ls
pr
eviously used
in
opening the cran
ia
l
va
ult. I n
hi
s pape r Toi
so
n paid much attention
to
Wagner (already
in
his t
itl
e) as the true

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 12/213
de Martel's Sku
ll
Trephine a
nd
Meta l Gu ide
3
pi
onee r behind the revolutionizing method of
raising cranial flap
s.
He de
sc
ribed Wagner's
"
hi
stori
ca
l contribution w
hi
ch he first per
formed on a liv
in
g human on October 1st
1889" and continu ed [38], .. Aussi la nou ve
ll
e
methode opCraloire inaug
ur
ee
par
W Wagne r
(de Konigshuue) qui
permetde
creer
une
vaste
ouverture a a boite ossellse
du
crane
et
de re
fermer, a la fin de I'operation, avec de I'os,
J'ouverture r
endue
tcmporaire de la trepana
tion, constilUe-t-cile un grand progres chirur
gical. Ce chirurgien a donne a celle methode
opera toire Ie nOIll de rcseClion temporaire du
crane ..
Toison's saw
was
fairly cl um
sy
and
was
there
fore not much used [48]. T hree years later
(1894) Leonardo Gigli from Florence, Italy, de
scribed
hi
s
si
mple yet clever
in
s
trumem
, a wire
saw to
di
vi
de bone between two open
ings, Thi
s
tool has come to bear his name, being called the
Gigli saw [16, 17). Origina ll
y,
Gigli imemed
hi
s
wire saw to facilit.·
ue
symph
ys
iotomy in obste tri
cal surgery. He finished hi s o
ri
gi nal repo
rt
{16],
emphasizin g that one dozen saws could be or
dered from the Hermann HarLel Company in
Bres lau at the price of 3 German marks plus
40
pf
ennig for shipp
in
g
com
to an
)'
foreign
co
unt ry.
He also added that c
hi
efs of clinics
could obta in free samples by ju st sending in a
request.
Professor Alfred Obalinski from the
Ja
gi
cl
Ionian University of Cracow in Galicia (the
have n
of
Polish culturc at the time, although
under the government
of
Vienna) had in
tended to describe the use of the Gigli saw for
cranial trepanations at the
Im
ernational Con
gress
in
Mo
scow
in August 1
897.
However, he
was
prevemed from going and instead
pub
lish
ed hi
s innovative application in the Cen
tro/blatt [ilr Chimrgie that same
),ea
r [30]. In his
paper Obalins
ki
stat
ed
that it had
occ urred
to
him that by using a slightly bcnded cannu la as
an
inse
rter
,
the
fl
ex
ibl
e Gig
li
s
aw
was
ideal f
or
introduction between burr holes. He em
phasized that the use of the Gigli saw permits
the safest method of dividing the skull bone
from the inside to the outside without the type
of
trauma usually seen from the use of ham
mer and chi se l [30]. In
Mo
scow, Emile Doyen
from Paris demonstrated
hi
s
ow
n m
et
hod for
perform ing a cra
ni
ectomy in front of many
prominent professors
of
surger ) including
vo n Bergmann from Berlin, Czerny from
Heidelberg, Cermany, Kocher from Bern,
Swi
tzerland,
Simp
son from Edinburgh, Scot
land, and Sk lifassowski from
SL
Petersburg,
Ru ss ia. In his pioneer paper Obalinski gives
credit
to
Ka rl Da
hl
gren
(1864
- 1924), a
Swedish pioneer who, in 1896, had designed a
new bone-cuttin g forceps fo r making lin ear
cuts in the skull
bone
and which cut from the
i
ns
ide out [6]. With the increasing interest in
cranial surgery in the first decade
of
this cen
tu ry. the Cigli saw later became recognized also
in the United States by Harvey Cushing, who
adopted the use of this simplc instr
ument
to di
vide the skull
bone
between two
burr
hol es
[36].
de Martel's Skull Trephine
and
Metal Guide
In 1908 Co
unt Thi
erry de Manel (1875- 1940)
pre
se nted lhe perfect
so
lution to the rest of the
problem of trephining wi thout risk of produc
in g intracranial damage. As a bo)' de Martel
was already very inquisitive and e
nj
oyed taking
mechanic
al
things apart to learn how the ), op
erated [31]. Frequently he dissected the fowl
being prepared in the kitchen, and he bought
a skeleton that he displayed as an amiable com
panion, de Martel, a dcscendant of the
Mirabeau
fa
mil
)'
who played an olltstanding
role in the French Re volu tion, was an
ar
istocrat
f
ull
y conscious of
hi
s ancestry. At fi rst he
was
enrolled in a school for the training of en
gi neers and later
was
trained by several French
master surgeons. He became especially in
terested in neurosurgical instrumentation. At
the age of 33 he published an article [28] de
scribing
two
new neurosurgical ins
tr
uments.
Today, 80 ),ears later, both are in dail y use by
many thousa nds of neurosurgeo ns a ll over the
world.
In hi
s milestone paper the two instru
ments he described were
(a)
a motor-dr
iv
en
trephine equipped with an automatic di se n
gaging ge
ar
that stopped the trephine
as
soon
as
it h
as
penetrated the skull and (b) the metal
gu id e for the introduClion of the Gigli saw
be
tween se parate burr holes.
Wh en in Pa ris, de Martel presented his n
ew
automatic trephine, but it was received with de
ri
sion. He then performed a demonstration
lI
si
ng a dried skull with a balloon 0 11 the inside
as an im itaLo n of the dura mater. With his au-

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 13/213
4
I.
History of
the Pt
erional
Ap
proach
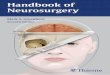
Fig. 1.2. The " hypoph yseal 0 a pproach of Heu er and
Dand
y.
F
rom
Dandy WE (1936)
The
braill, in Lewis
D (cd): WF Prior,
Proc/ice of SUrgfly,
vo l 1
2.
LOmatic tr
ep
hin
e he drilled a hole
in
this sk ull
without
puncturing
the balloon and com
mented
[31 ], "Well , as
yo
u call see, this
treph ine can
be
operated
by
an imbecile" ("ct
bien comme va lis voycz, Messieurs, cc trepan
pellt manie meme par un imbeci le"). Amer
ican ne
ur
osurgeons were even
more
reluctant
to accept de
Mart.e1 's
e lectric dri ll. By the late
1930$ it was used rout inely in Scandinav ia,
France, Germany, and Central Europe. Yet in
Bo
ston in 1948 its lise
was
rejected even at the
Massachuseus General Hospita
l.
The burr
ho les
we
re d
one
manually (and laboriously )
with Hudson drills. It was said that electric
drills were not used because Cushing had once
st
at
ed th
at
such drills caused too much vibra
tion transmitted to the brain (Bakay L, per
so nal communication, 1974).
Hagerstown, Maryland,
pp
145,
583-585. Re
printed
wit
h permission of Practice of Surgery
Ltd
.
[71 .
de Martel also had designed a hemostatic
forceps, a self-reta ining cerebral retractor, and
a special surgi
ca
l ch
air
supporting the patient
for
operat
in g on posterior fossa
tumor
s
wi
th
the p
at
ie
nt
in the siuing position. He was the
pioneer
neurosurgeo
n in France who foug
ht
and overcame the difficulties
of
blood lo
ss
and
inadequate posterior
Fossa
visuali
za
tion com
mon to neurosurgery during the first qua rter
of this centu ry. He had los t his only son in
Worl
d War I. In 1938, at the Annual Congre
ss
of the Deut
sc
he Gese ll
sc
haft
fUr
Chirurgie. de
Martel gave
an
impassioned speech
about
the
necessity
of
continued friendship between
French and German surgeons, a speech
that
was followed by thunderous applause. Two
yea
rs
later, on
Ju
ne 14 , 1940,
as
Hitler's troops occu
pied Paris, de Martel commited suicide [3 1
].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 14/213
From a "Hypophyseal" to a More Pterional Approach
5
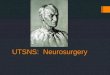
Fig. 1.3. Another view of the "concealed incision"
(be hind the hairline) of Heuer and Dandy. From
Da
nd
y WE
(1936
) The brain, in Lew is D (ed): WF
From a .. H ypophyseaJ" to a More
Pterional Approach
In
1918
Waller Dandy took the liberty
to
report
for George Heuer, one of his yo unger col
leagues, on a "
hypoph
yseal" a
pproach to
pituitary tumors [23]. Heuer later described
this
approach
in
more deta
il
and
used it
for
sel
IaI' and suprasellar LUmors [21, 22]. In the
1940s Dandy made some modifi cations [7
-
10
]
and
this lype of cranial
opening
became
popu
larly known in
the
United States as
the
" D
andy
na p " (Figs.
1.2-1.4).
This hypophyseal ap
proach used a skin incision concealed behind
the hairline.
Prior, Practice
of
Surg
ery,
\'01 12. Hagerstown, Mary·
land, pp \45.583-585. Reprinted
with
permission
of Practice of Surgery Ltd . [7].
In
19
62 George "{ayes,
one of
Dandy'S stu
dents and former chief of neurosurgery at The
Walter Reed Army Medical Center 111
Washington, D.C., briefly illustr
ated
his fron
totemporal
approach
in
a publication with
Slocum [20]. One of their figures showed " ...
the
visualization of an ane
ur
ysm of
the
an
terior
communicating artery
as exposed
through
a small Dandy pituitary lype of flap. "
Hayes
and
his colleagues commonly used this
approach to the base of the brain (Hayes GJ ,
personal communication, 1974).
In 1963,
before
the period of micro
neurosurgery, Lougheed and co-workers [27]
stated that their operative procedure was car·
ri
ed out through
a
front
o temporal bone flap

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 15/213
6
L History
of
the Plerional Approach
A.
I
Openo nS .r.·chnldl
e t w ~ ~ ,
optic
n.
ad
GJrotid
L
Fig.
1.4. Dandy
's
ap
proach
to
an intracra
ni
al
aneurysm. From Dandy WE
(19
44, reprilHcd
1969
)
Intracranial Arterial Aneurysms. New
York, H
afner
.
Skin irn:: i$i
on
Fig. 1.5. The ptcrional craniotOmy flap as outlined
by Kempe. From Kempe LG [25] .
mal\cr
Copyright ]944
by
Comstock Pu b
li
shing Co
mp
an
y,
In
c. Re printed by permission of Corne
ll
U
ni
versity
Press [9].
with removal of the pterion and a bit of the
outer third of the lesser wing o
hh
e sph enoid. "
Ludwig Kempe. w
ho
succeeded Ha
yes
at
T he
Walter Reed Army Medical Center,
Ili
cely illus
trated various features
of
the plcrional ap
proach (Fig. 1.5) in his 1968 two-volume
alias,
OPerative Neurosurgery [25].
Of
interest is the de
scription g
iv
en to the critical
burr
hole placed
at
the junction of the temporal line, the
zygoma tic process of the frontal bone, and the
orbita l ridge. At The Walter Re ed Army Hosp i
tal this became known as the " psyc
hopat
hic
p
oi
m " [14, 26, 41],
pr
obably in reference to the
dispos ition of the s
urgeon
should the res
idem
fail
to
pla
ce
th
e
burr
hole correctly Sub
seque mly Fox
learned
the
pt
erion
altcc
hnique
of
cran ial ope ning [ 13 , 14] by observing
or
as
sisting George Hayes, Ludwig Kempe, and
Hu
go Ri
zzo
li
, Dand
y'S
las t
neurosurg
ica l res
i
demo Barnes Woodhall, another of Dand y'S
trainees, simila r y used the
pt
erional approach
at
Duke Uni
ve
rsity (Woodha
ll
B, per sonal com
munication, 1980).
With the
imroduct
ion of mic
roncuro
s
ur
gi
cal techniques, Gazi a ~ a r g i l illus
trat
ed his

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 16/213
Bi b
li
ograph y
7
Fig. 1.6.
D
iag
ram
of s
kull
w
ith
area
us
ua
ll
y includ
ed in
a pterio
nal fl
ap
a
lt
hough modified
by
var iou s surgeons.
F
ro
m F
ox
JL
[14] .
microtechnical pterional approach [51, 54
],
which was a refinement of hi s 1969 frontotem
poral description [50]. He emph
as
ized the
sma
ll
, low basa l expos
ur
e
by
drilling down the
sphenoid bone. At that time the basic differ
ence between hi s published description and
that of Kempe's [25] was the use
of
micro
technique, sphenoid bone drilling, a w
id er
opening of the
sy
lvian
fi
ssure, the
pl
acement
of
the posterior
burr
holes more ant
er
iorly
(making it a frolHos phenoidal craniotomy),
and the avoidance
of
r
et
raction
on
the tem
por
allobe [54].
and co-workers used
the pterional approach for lesions in the inter
peduncular cistern [52], in which situation the
poster ior clinoid process is a landm ark that, on
occasion, may hind
er
a clear ex pos ure [35].
The
skin incision likew ise has changed with
the needs and
pr
eference ofthe indi
vi
dual sur
geon. Dand
y's or
iginal incision is illustrated
in Fig
s.
1.
2 th r
oug
h
1.4.
Kempe's incisi
on
(Fig.
1.5)
permitted greater exposure
of
the
temporalis muscle as
well
as
a more basal exp
o
sure. Various s
urg
e
on
s
at
tim
es
extend the
fronta l limb a s
hon
distance into the skin of the
forehead above the junction
of
the medial
twO
thirds and lateral one third of the eyebrow.
Th is
mi
ght permit a sh
orter scal
p incision,
but
itdid
make part of the surgical sca r
visi
ble after
hair regrowth. incision was long
er
but rema in ed concealed beh in d the hairline
w
hil
e descending lo w enough to permit a
lo
wer, basa l a pproach [53, 54
].
The pterional
approaches at times can injure the fromalis
"
branches
of
the facial
nerve,
a point of recent
di
sc
uss ion [2, 55].
Throug
hout the ye
ar
s n
euro
logical s
ur
geons have altered and modified the a
ppr
oach
to the middle fo ssa and se llar region. In one
form
or
anOlher the p te rion has been incorpo
rated within the reflected bone fl
ap
in modifi
cations
of
the
pter
ional
fl
ap" (
Fig
.
1.6).
Its
evolution from the Heuer-Dandy flap to the
Hayes- Kempe flap posteriorly and basa
ll
y and
then to
th e
Yaprgil nap anteriorl y and basally
has been accompanied
by
par
a
ll
el ad
va
nces
in
imagi n
g,
anesthesia, magnification,
li
ghtin
g,
retraction, in str
um
entation, and intraopera
tive ene
rg
y transfer
(by
lase r, ultrasound, elec
trocautery, and the like
). The
pterional ap
pro
ach is n
ow
finding its place as an important
surgical route to t he
ci
rcle
ofWilli
s
and
itsenvi
rons. The pioneers who laid the fundamental
cornerstones to th
is
procedure include
Wilhe
lm
Wagner, Leona
rd
o Gig
li
, Alfred
Obalins
ki
,
Thierr
y
de
Martel, George Heuer,
and
Walter Dand
y.
T hese
are
the m
en of
years
long past to be remembered
by
a
ll
ne
uro
sur
geons who today regard the pterional ap
proach to the sku
ll
base as an elementary and
most obvious and fundamental principle.
Bibliography
1.
AI-Me f
ty
0
(1987)
Supraorbital-ptcrional ap
proach
to skull
base
I
csions. Ne
ur
os
ur
ge
ry
21: 474-477
2.
Ao
ki N
(1987)
I
ncision
offacial nerve b
ra
nch
al

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 17/213
8
I. History of the Plerionai Approach
aneur
ysm surgery.
(Leuer
to the Editor) J
Neurosurg 66: 482
3. Brock M, Dietz H (1978) The sma ll frontolateral
approach for the microsurgical treatment of
intracranial aneurysms. Neu r
ochirurg
ia
(Stultg)
21:
185-
191
4. Buchfeldcr
M,
Lj
unggren B (1988) Wilhelm
Wagner
(1848-
1900).
Surg
Neural, in press
5.
Cushing
H (1909) A met hod of combiningexplo
ra tion and decompression for cerebral tumors
which prove to be inoperable. Surg Gynecol
Obstet
9:
1-5
6.
Dahlgren K (1896) Ein neues Trepanations
in strument. Centralbl Chir 23: 217 -220
7. Dandy ,-\,IE (\936) The brain, in Lewis 0 (ed):
PracliceofSurgery,
Hagerstown, Md, WI<- Prior, vot
12, pp 145,583-585
8. Dan
dy
WE (1938) I
ntracranial
aneurysm of in
ternal carotid artery.
Cured by operat
ion. Ann
Surg
107:654-659
9. Dandy
WE
(1944, reprimed
1969)
Intracranial
ArterialAneurysms. New York, Hafner
10.
Dandy WE (1945) Intracranial arterial
aneurysms, in:
The Brain.
New
York,
H
arpe
r
&
Row (Reprinted 1969 from WF Prior, Lewis Prac
tice o/Surgery, Hagerstown, Md)
II. Dorland's
Illustrated Medical Dictionmy
(1974) cd
25. Philadelphia, WB Saunders Co, p 1284
12. Dotl NM (1933) Intracranial aneurysms: cere
bral arterio-radiography: surgical treatment.
Edinb Med J 40:
219-234
13. Fox
JL (1979) Microsurgical exposurc of intra
cran ial ancurysms. J Microsurg I: 2-31
14.
oX
JL
(1983)
Intracranial
Aneurysms.
Ncw Yor
k,
Springer-Verlag
15. Frazier CH (1913) An approach to the
hypophysis through the anterior cranial fossa.
AnnS
urg57: 145-150
16. Gigli L (1894) Ober ein neues Instrument wm
Durchtrenncn dcr Knochen, die Drahtsage.
Centra lbl Chir 21: 409-411
17. Gigl i L (1897) Z
UI"
praktischen Vcrwertung der
Drahtsage. Cemral
bl
Chir 24: 785-788
18. Hakuba
A,
Liu
S, Ni
sh
imu ra S (1986) The or
bitozygomatic infratcmporal approach: A new
surgical technique. Surg Neurol 26: 271
-276
19.
Harris
P,
Udvarhely i GB (1957) Aneurysms aris
ing at the internal carotid-postcrior com
municating artery junction. J Neurosurg
14: 180- 19 1
20. Hares GJ , Slocum HC (1962) The achievement
of
optimal brain relaxation
by
hypervemilation
technics
of
anesthesia.] Neurosurg 19: 65-69
21. Heuer GJ (1920) Surgical experiences with an
intracrallial approach to chiasmalles ions. Arch
Surg I: 368-381
22. Heuer G] (193 1) The surgical approach
and
treatment of tumors and other lesions about the
optic chiasm. Surg Gynecol Obstet53:
489-5
18
23. Heuer C] , Dandy WE (1918) A new hypo physis
operation.]ohns HopkillS Hosp Bu
ll
29:
154
24.
Jane
JA, Park
TS,
Pobereskin LH et al (1982)
T he supraorbital approach: Technical
no
te.
Ne urosurgery 11:537-542
25. Kempe
LG
(1968)
Operative Neurosurgery,
wl/
Cranial,
Cerebral,
and
Intracm71ial Vascular Disease.
Berlin, Springer-Verlag
26. Kcmpe LG, VanderArk GO (197 1) Anteriorco
m
municating artery aneurysms. Gyrus rectus ap
proach. Neurochirurgia (Stult
g) 14:
63-70
27. Lougheed WM. BOltereH EH,
r..
lo rley TP (1963)
Results
of
the direct attack in the surgical man
agement of internal carotid and mid dle cerebral
aneurysms. Clin Neurosurg9: 193-200
28.
de
Martel T (1908) Un point de technique
operaLOire dans la craniectomie. Presse Med
16:641-643
29. McArthur
LL
(1912) An aseptic surgical access to
the pituitary body and its neighborhood. J
AMA
58:2009-2011
30.0balinski A (1897) Zur Technik del' Schadel
trepanation. Centralbl Chir 24: 857-859
31. Pec ker ] (1980) T hierry de Martel, 1875-1940.
Surg Neurol
13:
40 1-403
32. PiteHi SO, Almeida GGM, Nakagawa EJ etal
(1986) Basilar aneurysm surgery. The subtem
poral approach with section of the zygomatic
arch. Neurosurgery 18:
125-
128
33. Pool] L (196 1) Aneurysms of the anterior com
municating artery. Bifrontal cranioLOmy
and
routine use of temporary dips. ] Neurosu rg
18:98-112
34.
Pool
] L (1962) T iming
and
techniques in the
intracranial surgery
of
ruptured aneurysms of
the anterior communicating artery.] Neurosurg
19:
378-388
35. Samson
OS,
Hodosh RM, Clark WK (1978)
Microsurgical evaluation
of
the ptcrional ap
proach to aneurysms
of
the distal basilar circula
tion. Neurosurgery 3: 135- 141
36. Seeger W (1973) Allgemeine neurochirurgische
Operations tech nik,
in
Sailer
FX,
Gierhake
FW
(cds): Chirurgie histQrisch gesehen. Deisenhofen bei
t.
H.inchen, Dustri Verlag: pp 237 -238
37. Sugita K (1985) MiC1"01liurosurgical Atlas. Berlin,
Springe r-Verlag
38.
Toison]
(189 1) De la trepanation
du crane
p
ar
resection temporaire d'un lambeau osteoplas
tique (procede
de
Wagner et procede person
nel). Co ng Fr Ch ir 5: 325-338
39.
To
nnis W (1936) Erfolgreiche Behandlungeines
Aneurysma der Art. commun. ant. cerebri. Zen
tralbl Neurochir I: 39-42
40. Tonn isW, Walter W (1960) Ein neuer operativer
Zugang zu den sackrormigen Aneu
rys
men de r
basalen Hirngef.isse. Wien med Wochellschr
11
0:
145-147
41.
VanderArk CD, Kempe LG, Smith DR (1974) An-

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 18/213
Bibliogr
ap
hy
9
terior communicating aneurysms: the gyrus
rectus approach. Cl in Neurosurg 21:
12
0- 133
42. Wagner W (1885) Uber Halswirbellu xationen.
Ard,iv fur klinische Chirurgie . Be
rl
in, Ver lag von
August Hirschwa ld ,
pp
192-2 16
43. Wagner W (1886) Die Behandlung der komp
li
cirten
Sc
hadelfrakturen. Centralbl Chir
26: 2405-2510
44. Wagner W (1889)
Die
temporare Resekti
on
des
Sc hadeldaches an Stelle der Trepanation. Ein
Vorschlag. Ce lllra
lbi
Chir 1
6: 833-838
45. Wagner W (
1891
) Zwei Fa
il
e von temporarer
Schadelresektion. Ccmra lbl Chir 18: 25- 29
46. Wag ner W (1895) Z
wei
Faile
vo
n HaematOm der
Du ra mater geheilt durch temporare Schadel
resektion. Berl klin \-I/ochenschr32 (7) : 1
3i
- 140
47. Wa gner W, Stolper P (1898) Die Verletzungen der
Wirbelsa ule und des Riicke
nmar
ks, in vo n
Bergmann E, von Bruns P (eds): DeutscM
Chirur
gie,
No
40,
Stutt
gar
t,
Ve
rl
ag
vo
n F
er
dinand Enke,
pp 1-564
48. Walkcr EA (1951) A Hs/ory ofNeu.rological Su.rgery.
Baltimore, Williams & Wilkins Co, p 50
49. Wolff J (1863) Die Osteoplas
ti
k in ihren Be
ziehungen zur Chirurgie und Ph ys iologic. Arch
klin Chir 4: 1
83-29
4
50.
~ a r g i l
MG (1969) Microsurgery Applied
10
Neurosurgery. Stuttgart, G
Thieme
, pp 119-
14
3
51. r g i MG (
19
84) Microneurosurgery. Stuttgart,
GT
hieme
52.
MG
, AnticJ , Laciga R et a1 (1976) Micro
s
ur
gical pterional approach to aneurysms of the
basilar bifuf(:ation. S
ur
g Neurol6:83-9 1
53.
Y a ~ a r g i l MG,
FoxJL(1975)The microsurgical ap
proach to intracran ial ane
ur
ysms. S
ur
g Ne
ur
ol
3:7-14
54.
a ~ a r g i MG,
FoxJL,
Ray MW
(1975)
Th
e
ope
ra
tive approach to aneurysms
of
the anterior com
municating artcry, in Krayenbiihl H
(cd):
Ad
vances
and Technical Standards in Neurosurgery.
Vienna-New York, Springer-Verlag, pp 113 - 170
55. Yaprgil
MG,
Reichman
MV,
Kub
ik
S (
19
87) Pre
servation
of
the frontotemporal
br
anch
ofth
e
fa
cial ner
ve
using the inter
fasc
ialtcmporalis nap
for pter ional craniotOmy. Technical ar ticle. J
Neurosurg 67: 46
3-466

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 19/213
2
Instrumentation and Positioning
Introduction
This chapter describes the surgical instru
menlS and equipm
ent
utilized by the author
during the plcrional approach to intracranial
lesions. Since part
of
the instrumentation is
used to maintain the proper position and align
ment of
the patient, positioning
is an
inti
mately related
sub
jec t.
The Japane se samumi was a dedicated and
courageous warrior skilled in
batt
le. He and his
sword or bow-and-arrow were a si ngle fighting
unit. They were such an integral p
an
of
each
other that activation
of
cerebral and muscle
memory effected rapid and nearly subcon
sc ious communication, resulting in precise,
"computeri
zed" de live
ry of the weapon
upon
its
targeted foe.
The
above simile is meant to emphasize the
conceptual and real changes occur ring in the
modern neurosurgical operating room.
The
neurosurgeon (samurai), the instrumentation
(bow-and-arro
w),
and the patient's lesion (foe)
are no longer separa te en tities. Through ex
tensive laboratory and clinical training, un
learning old habits, and learning new methods
of
hand-brain-eye coordination, the
modern
neurosurgeon now develops cerebr
al
and mus
cle memory akin to
that of
the
sa
murai.
The
operating microscope and microsu rgical in
struments become an
in
tegral part
of
the sur
geon who must deftly deliver his
therape
utic
a
rrow on
target. If this is
to be
done with mini
mal disturbance to the patient's brain, the
arrow's trajectory is limited to narrow path
ways
between cranial and intracranial structur
es.
It n
ow
can be appreciated that,
in
addition to
being a
bl
e to work
in
small, op tically magnified
spaces with de licate and long dissecting instru
ments, thc position
of
the neurosurgical pa
tient nowadays
is
critical to the "s tereotax ic"
alignment
of
the su
rgeon's eye, the micr
o
scope, the dissecting
in
struments, and the
ta rgeted lesion.
The
surgeon must supervise
the positioning of the p
at
ie
nt
so
that
when the
target
is
reached later
in
the
day,
the surgeon is
comfonably situated for delicate dissection
of
the tumor
or
vascul
ar
anomaly within
ve
ry nar
row spaces. As the patienland instrumentation
are being se t
up
, the surgeon reviews a mental
check list(much as an air
pl
ane pilot does) based
on past experience and endeavo rs
to
control in
terlocking events with
in
the
operat
ing room.
Inexact patient posi tioning or imperfect align
ment of
the patient's h
ead in
the historical pas t
could be compensated by more br
ai
n retrac
tion or by rotation
of
the patient's head rest
in
g
on a cranial "donut."
Nei
ther is acceptab le in
most modern-day microneurosurgical proce
dures where the patient
'S
cranium is im
mobilized
by
a skull-fixat ion apparatus and the
brain
is
supported
by
se lf-retaining retractors
usually attached to the operating table. Thus,
an incorrect positioning
of
the skull-fixation
apparatus, f
or
ex.a
mple,
may
cause
part of
this
a
ppar
atus to
intcrfer wi
th later pl acement
of
a
sma
il
,
se
lf-retaining retractor
0
11 the in ternal
carotid artery
and
thereby hinder the sur
geon
's
line-of-sight to the interpeduncul
ar
ci
s
tern.
It is in
this context th
at
"interlocking
events" must be well thought out and control
led.
Because the neurosurgeon is working within
very narrow confines, it is even more incum
bent
upon
the surgeon not only to have a
thorough knowledge
of
normal and aberrant

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 20/213
A
B
c
12
2.lnstrumemation and Positioning
Fig.
2.1
. A. Top of skull with
burr
hote at ri
ght
coronal su
ture and sma ll hole
(arrow)
ju s
t behind burr hole. B.
View with cam
era
lens
at
burr hole. Anterior clinoid
processes
(triangle
s
),
poste
rior clinoid processes,
and
left foramen ovale (wroed
arrow) are
, ,'ell seen
at
sku
ll
base. Small arrow lies on
right
posterior clinoid processand
poims toward metal pin pro
jecting up\\'
ard
from n
oorof
sella turcica.
C.
Similar but
morc restricted view with
camera l
ens
at smaller cra
nial hole (behind burr hole
in A). Arrow crosses left
pe
trous pyramid
and
intracra
nial opening of carotid canal
and p o i n ~ LO the
for amen
ovale. Figures 8 and Care
rotated 90
0
counter clock
wise compared with
A.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 21/213
Head Holder
13
neuroanatomy but also to be able to concep
tualize the anatomy in its three dimensions
(stereoimage concept).
The
tomographic plan
es
of
computed tomography (CT) and magnet
ic
resonance imaging (MR I) detract from such
conceptua lization (whereas stereosco
pi
c im
ages and pneumoencephalography [45J en
courages it
). The
medical student learns hi s
anatomy from standard cadaver dissections
and textbooks.
The
surgeon,
at
least in the
pterional approach illu st rated in this atlas,
must view the p
at
ient's anatomy from an ob
lique and
up
side down oriemation (wi th re
spect to the patient).
Cranial openin gs have become smaller as
microsurgical techniques have advanced. In
theory, an intracranial lesion could be operated
on via a tiny (eg, I mill) cra ni al opening
(F
i
g.
2.1). In a sense, the operat ing microscope
brings the surgeon's eye closer to the cran
ial
opening. If the surgeon's eye were at the open
ing like peering through a keyhole, a full view
of
the intracranial spaces could be seen - if re
tractors cou ld fit
through
the opening - and
the lesion cou
ld be removed
or
corrected - if
dissectOrs, like a laser beam, could fit through
the opening. Thus, among the factors limiting
the u
se of
very sma
ll
cranial openings
in
most
cranial operations are intracranial instrumen
tation and maneuverability.
Instrumentation continues to change, de
pending on s
ur
gical needs. There are
va
ri
ations
among
specific types
of
instruments (eg,
retractor systems, cranial-fixation systems,
operating tables), and an individual surgeon
often uses the system that he was trained in or
that fits his particular approach. The instru
ments and equipmem herein described ha
ve
been the
au t
hor's personal preference for the
pterional approach to various intracranial le
sions. Much
of
the following
is
reproduced
from a previous publication
[16].
External Instrumentation
Operating Room Table
We
place the patient on the Amer ican Sterilizer
operating room (OR) table so that the patient'S
head is at the foot end
of
the table (Fig. 2.2).
This has several advantages: (a) the table ped
als are not
in
the way
of
the sitting s
urg
eon's
feet (the anesthesiOlogist
or
circulating nurse
manipulates these as needed); (b) there
is
more
room for the base
of
the mi croscope (w hich we
position to the left
of
the sur geon); (c) the nor
mal opening in the OR tab
le
lies under the lum
bar region
of
the patient's back, facilitating
lumbar cerebral spinal fluid (CSF) drainage
without turning the patient. The only disad
vantage
of
this alignm
ent
is that the main
weight of
the patient
is off
the center
of
gravity
for the OR table. An assistant often must assist
in elevation of the surgeon's end
of
the table
by
lifting lip the table
under
the patient's shou
l
ders when the patient
'S
head is raised (table
fl exed) to
its
final position (aboma 10- to 15-de
gree elevation of the patient'S head).
Thi
s ac
lion lightens the unbalanced
lo
ad on the table
wh ile the table is flexed. One must becareful to
avoid sliding the bUllocks into the opening,
which would risk sciatic nerve pressure
in
short
patients.
Head Holder
In this
era of
minosurgical technique and self
retaining retractors, it usua
ll
y is essential that
the head be immob ilized
by
three-poim skull fi
xation.
We
use
the
Mayfield-Kees skull clamp
(Kees Surgical Specialty Company). T his clamp
(F ig. 2.3) is inserted into the normal foot end
of
the American Sterilizer table.
The
horizon
tal part
of
the head holder should be nearly
parallel wi th the fl oor. We prefer to have the
two-point
si
de of the clamp
on
the side
of
the
surgery, as the opposite one-point side may
project Out tOO fal: All joints are tightened se
curely (from above downward), and the head is
immobilized throug
hout
the operation.
A study group stated (17):
Unde r the sur
gica
l microscope, the
slig
htest
movement
of the patient's head
is
magnified con
siderably. Microsurgery demands a precisely
maintained position of the
firmly fixed cra
nium
throughout the entire opel'ation, whe
th
er one op
crates with the patient in the sitting. supin
e,
or
prone position. This is
beS
t
achieved
by
a
pillion
head
holder in which the essclllial clemem is a
clamp made to accommodate three relatively
sharp p
ins.
The pins penetrate the
scal
p a
nd
are
then firmly fixed to the outer (able of the sku
ll.
\Vhen
placing the pins, the sur geoll shou ld take
care to
avoid
a spinal
fluid
shunt, surface
vessels,
thin bone
(such as
over the frontal and
mastoid
sinuses),
and the thick temporal muscle where the
pos ition of the pin tends to remain unstable, how
ever
tightly
the clamp
is
applied. A
pin on th
e
forehcad s
hould
, of course,
be we
ll away from
th
e
eyc; and whe n the clamp
is
positioned too
close
to

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 22/213
14
2.
Instrumentation
and Positioning
A
"
B
c

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 23/213
fi g. 2.3. A. Mayfield-Kees head
holder
with demon
stration sku
ll
(bone flap removed) in position
for
right fron(Oiatcrai craniotomy. 8 . Pa tie nt in position
A
B
wi
th head turned 40° to left, tilted 15° to left. and
d ro p
ped
bac k 15°, From F
ox
[16].
Fig. 2.2. A. Sketch
of
American Steri
li
ze
r OR table.
Th
e usual head end is
to
the observer
's
lefl.
The
head rest has been rCII1O\'cd from th
is
end
and
placed at the normal foot end on the observer's
right. T he
patient'S
head in it
ia
lly rests on the head
rest on the observer's right with that end c evated
10°_
1
5°
and
wit
h the
lu
mbar region o
fl h
e patient's
back resting
Me
r the
ope
ning
(arrow)
in the table.
B.
Same
after
specia
ll
y mad e maltress
is
in place with
ope
ning f
or
l
umbar
CSF
dra
inage. A model skull
(see Fig. 2.3) is held
by
the sku
ll damp
(replacing
the
h
ead
rest). An
ether
screen" (bar w
it
h k
no
b project
ing toward observer) p rojects away from the left sidc
of
the paticlll to later ho ld the d ra p
es
alld suction
tubes.
The
Leyla sel
f-
r
eta
i
ni
ng
retrac
t
or
b
ar
(see
Fi
g.
2. 11
)
atl<lc
hcs (aITow) to
the
O R table ju st
cephalad to the
ether
scr
ee
n attach me n
t. The
micro
scope stands JUSt cephalad to lhe et her screen, and
the anesthesiologist
is
position
ed
caud al LO lhe ether
screen. C. Preli mina ry dr aping of paticnt. In st
ru
me nts
are
placed on the overh ead instrument ta
bl
e
(Phelan
Ma
nu fact
urin
g Co r
porat
ion, Minnea polis).
Note
the
steralized "C-clam ps" at each end with rub
ber
tubi
ng
stretch
ed
between. T hese
are
covered
after
fi na l draping
and
prel'cnt instruments from
falling offinto the ancsthesiologist's nonsterilc field.
From Fox [ 16].
15

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 24/213
16
2. Instrumenta tion and Positioning
the incision, a pin·casing can
be
a hinderance.
Special sma
ll
er pins available for infants can also
be used f
or
patients who have thin skulls. Particu
l
ar
attention should
be
given to p
at
ients who have
had a lo ng history of hydrocephalus. Having se
cured the clamp .
the
surgeon holds the head
in
the de si
red position while the final attach ment
to
the operating table is made. Man ipulation of the
head holder accurately and with
safe
ty may bcdi f·
ficull at first,
but
with experience any obstacles en
counlcred can
us
ually be surmounted. This
method of skull fixation avo ids the
pr
essure in
juries
th
at may occur
to
t
he
scaJp or face w
hen
the
head has been resting on rubber pads for lo ng
pe riods.
Th
e time
of inse
rtion
of
the poinlS imo the
scalp and skull is a critical period . T he head
must be perfectly posiLioned according to the
approac
h u
se
d by the surgeon .
Any
deficiency
wi ll cause defective a
li
gnment
of
the target,
cranial
ope
nin
g,
mi croscope, and surgeon
's
eyes.
The
alignment must
be
such that there
will be a dear view
of
the aneu rysm at the focal
poim
of
the microscope with the surgeon in a
comforta
bl
e position. Upon inserti
on of
the
Fig. 2.4. Pneumatic lift chair (C.C.R. Medical Corpo
ration, Pittsburgh). The dark cushion is added for
extra height. From Fox [16] .
poinlS, the patient's blood pressure and intra
cranial pressure
wi ll
rise unless he is properly
anesthetized and his blood pre
ss
ure is under
control.
Th
e sur geon must notify the anes
thesiologist before he inserlS the poims. Colley
and Dunn
(6]
recommended local anesthesia
in the
sca
lp at the point-insertion sites.
Surgeon's Chai r
Surgeons' chairs are
ava il
able from
va
rious
companies, eg, Storz Instrument Company,
Aesculap Company, Stryk
er
Corporation, and
V. Mueller Company. e l al [57] re
ported on their spec
ial
chair; we have found
the recent modification so
ld by
the Aesculap
Company to be qu ite sa tisfactory. \Ve also have
used the pneumatic lift chair (style P390244)
ava
il
able from lheC.C.R.
Me
dical Co
rp
oration
of
Pit lS burgh (Fig. 2.4). A hard cushion may be
pl aced on the seal to gi
ve
the surgeon a bit
more height. The stool h eight
is
adju stable by
press ing on the foot bar.
Operating Microscope
After years of experience with neuros
ur
gery
sa ns microscope fo llowed by microneurosurgi
cal experience in hi s operating room, Cha
rl
es
Drake concluded [
12]:
Th
e
remarkable
new surgical world revealed
under the operating microscope and the beaut i
ful instruments ava ilable to work in it have un
doubtedly played a m.yor role in placing the
sa fety and scope
of
aneurysm surgery
\\
'here they
are
tod ay.
And Gazi ~ a r g had advised [55]:
However, it should never
be
forgotten that there is
much
mo
re to microtechniquc in ne urosurgery
than the possession of a highly pe
rf
ectcd optical
instrumen
t. Thi
s al
one
is of
litt
le
valu
e without
special methods of bipolar coagulation, carefully
adapted in struments,
and,
above all, atraumatic
operation techniques.
In 1865
Bi
schoff [4] published his work on
dissections
of
the cranial nerves. He began
wi
th
lou pes and later graduated to the dissecting
microscope with up to
50x
power.
The
evolu
tion of the u
se
of the operating mi croscope in
surgery is detailed in other publications [9, 17,
36,41, 43 ,55].
In
19
78 a stud y gr
ou
p concluded the foll ow
;ng
[In

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 25/213
Operating
Microscope 17
The
use
of
th
e operating mic
roscope
and
micro
technique is onl y
on
e part of the modern trend in
the surgi
ca
l treatment of certain cerebrovasc
ul
ar
probl
ems. Co in
c
identally,
a
team
of experts
has
evoh'cd, each of
whom
is s
pecially
trained
to
carry
Out his or her wsk
in
this type of surgery ...
Al
th
oug
h
we
pl
ace
major empha
sis
upon
the micro
surgi
ca
l tedmi<lues, advances h
ave
occurred as
we
ll in anesthesiology, nu rsi ng
care, radiol
ogical
di ag
nos
ti
c methods, pharma
cology,
a
nd avai
l
ab
le
monitori ng
syste
ms. Certainly t
he
judicious
use
of
vascu
lar h
ypote
n
sion and
of techniques
to co nt ro
l
intracranial pressure
has
hel
pe
d grea tly
o
redu
ce
pa tient morbidity. Some operations would
be
ex
tremely difficult if not
impossib
le
to
pe
rform
without
tod ay s so
phisticated personnel ...
Both
re
ports
in th
e recent literature and the in
creasi
ng
use of the microscope by neurosurgeons confirm
the o
pin io
n a
nd
experience of study group
mem
bers
that
th
e application of
the
operating
micro
scope and
m
ic
rotechnique
has
markedly reduced
the
mortality and
morbidi ty assoc
iated w
ith
intra
cranial aneur
ysm
sur
ge
r
y.
Para llel improveme
nts
in
equipm ent
have co
ntributed additiona
ll
y
to
these results. The cardinal factors,
ho weve
r, arc
the train in g, expe rience, and expertise of the
operating surgeon who
util
i
zes th
ese
new
tech
niqu es and
the capabilities of h
is
ope
ra tive
team.
Some
of
the techni
ca
l
as
pects
of
optics, su
p
ports, accessories, use, care,
and
sterili
za
tion
of
the
mi
croscope and i
ts
accesso
ri
es
are
given
elsewhere
[10,
14
,
15
,
17
,3
1,
35, 37, 40, 43, 55,
57
]. The
Zeiss operating microscope (Carl
Zeiss, Inc) is the unit most commonl y used at
this time (Figs.
2.5-2
.
7).
We have been usin g (he counterbalanced
Zeiss-Contraves unit (
Fig
s. 2.6 and 2.7) with
ele
ct
ron
ic sw
itches
that
release magnetic locks,
immobilizin g the
mi
croscope in any desired po
sition [57].
Our prefere
nce has been the OPM I
No.
I
Ze
i
ss
magnification system rather than
the zoom lens sys tem attached to the Contraves
stand. We also prefer the floor
mount
to the
ceiling mount. In o
ur
OR the television camera
is attached to the left
si
de
of
the beam splitter,
and the binocular observation lUbe or sti
ll
cam
era is attached to the right sid e.
The
newer in
clinable binocular tube (Fig. 2.8) has impro
ve
d
the
ve
rsatilityof this in strumenl.
With exper ience, the counterbalanced Zeiss
Contra
ves mi
c
ro
scope and the surgeon be
come a
si
ngle entity, wo rking comfortably
"hand-in-g love" in attacking the lesion. Nor
mally
we
ha
ve
one s
ur
gi
ca
l a
ss
ista
nt
on the
right s
id
e of a right-handed s
ur
geon.
Thus,
this surge
on'
s left hand is his first a
ss
ista
nt and
the other s
ur
geon, in
ef
fect, is
hi
s second assis
tant.
The
counterbalanced Zeiss-Contraves
microscope, first used by
[57] in
Zurich,
ca
n be auached to laser systems
or
u
se
d
in
conjunction with
an
ultrasonic aspirator.
With the
former
, the mobile microscope comes
over the left should
er of
the surgeon while the
at tached laser unit is
off
to the surg
eo
n's dire
Ct
left and s
iLS
between the
mi
croscope stand and
the anesthesiologis
t'
s equipment.
Other
exce
l
lent operating microscope
sys
tems arc avail
a
ble.
For example.
Keni
chiro Sugita in Mat
sumoto,
Jap
an, h as developed a hi ghl y sophi
s
ticated system [48].
Although agreement
is
not uni
ve
rsa l as to
when the microscope should be
brought
into
the operative field, experience sh
ows
that a
more
gent
le,
ac
c
urat
e, and rapid dissection can
be carried out if, once the dura is opened, the
entire ap proach to the aneur ysm and its dissec
tion
ar
e
carr
ied
out
und
er
the microscope.
With the pat ient supin e, the angled position
of
the incl in a
bl
e binoc
ul
ar
lUbe
is used most
often. Thi s now can be easily altered to a
straighter position when
dr
illing the sphenoid
wing and to a sh
ar
p
er
angle when dissection is
in
the
sy
lvian
fi
ss
ur
e
or antcri
or perforated
substance. With
ex
p
erie
nce, the su rgeon often
finds that he routinely uses the same higher
magnification (eg,
6x
or
8x
t
ru
e magnifica
tion) for the
ap
proach to the tumor
or
aneurysm
as
he does for i
ts
dissection.
Several
disadvantages
to the operating micro
scope have been mention ed [ 17]: Spec
ial
train
in g is requir
ed
for usin g the microscope.
microtools. and microsllture; it necessitates
operating in a dee p, narrow gap; it requires
longer adaptation time; it does not permit
good tissue palpation (i nstruments are used ,
not fingers) and requires visual manipula tion ;
work is indirect; work
is
tiring to the eyes; stiff
neck, shoulders, and back generally result; dis
tractions
are
poorly toleraLCd; eq uipme nt and
training are expensive; it la
ke
s
up
space in the
operating room; and the operating time for
most surgeons
is
longer.
The advantages
for the ne
ur
osu
rgeo
n far a
outweigh any drawbacks, however [17]: Fewer
parallax problems occur because the objective
lens brings the largetcloser to the surgeon's vi
sion; binocular vision is improved; i
ll
umination
is incrcased; the focus is s
harper
; and magnifi
cation permits a smaller craniotom
y,
less brain

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 26/213
18
2. Instrumell lation and Posi
tioning
retraction, a smaller cortical incision, and bet
ter
delineation of normal and abnormal
anatomy. Structures
that are
beller idcmified
by
the microscope
are
the arachnoid space,
compartments,
and
bands; the perforating
ar·
tcries; vascular variat ions in the circle
of
Willis;
aneurysmal
anatomy; microaneurysms; the im
pending rupture of an aneurysm; small bleed
ing points for bipolar coagulation; and the
nerves [17]. The advantages to the patienlarc a
smaller wound, beller repair or nerves a nd ves
sels, the fact that some inoperable lesions be
come operable, optimal hemostasis, fewer sur
gicallcsions, and fewer postoperative compli
cations [ 17 ]. Educational advantages include
Fig. 2.5. Standard Zeiss operating micro
scope wi
th
zoom lens system. f\lounted on
Zeiss Universal S3B noorstand.
Counesy
of Carl Zeiss, In
c.
use of the observer tube, television with tape
recording,
and
cinematogra phy
or
st
ill
photo
graphy. I
n
addition, the television system al
lows
the
scrub nurse and
anes
the
siologist to
know the state of the surgery from
moment
to
moment.
As the mi crosu rgical era began, Drake in
1965 stated [11]:
The ability to see the minute details of the struc
tures about an aneurysm has been, in my opini on,
the source
of
much
trouble in this as ill
other
fields of neurosurgery . . . There is a new
wo
rld
waiting
fo
r us.
The
dissecting microscope with its
superb
illumination is
ideal.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 27/213
A
Operaling Microscope
fig. 2.6. A.
CoUi
ltcrixliallccd
7..ciss-Co
lltra\cs
ollCrat i
ng
micrOKope. B. Close·up of microscope.
From Fox [16]:cou
rlCsy
ofC:lrI Zeiss. Inc.
19
B

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 28/213
20
2. Inst rumenta tion
and
Positi
on
i
ng
A
B
Fig. 2.7.
A.
Zeiss-Contravcs op
era
ting microscope in
position at surgery. The bo ne flap has been turned.
Note the rubber wbing that holds the drapes firmly
down
and
cauda
lly.
Abo\'c
arc
two suction tubes in
readiness. In the background is a telc\·is ion monitor.
B. Close-up of microscope
and
alLach ments. Left:
Sony lclc\·ision camera and microph one. Cn Ur:
bi nocular system and beam-spiller. RighI: assistant's
observation tube.
Th
e l
auer
is rcmo\'cd when st
ill
camera photographs arc made. From Fox [16].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 29/213
Operating i r o s o p e
21
B
Fi g. 2.8. Inclinable billoclliartube (Carl Zeiss. Inc) flanked by SonyT Vcamerit on left and Contax st
ill
camera
on right. A. I n straight positiull . B. 111 angled positiun.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 30/213
22
2. Instrumenta tion and Positioning
Gillingham cautioned , however [22]:
This is
a moment
1O
reflect
on
the use
of
magnifi
cation. [\ may make us len times morc gentle but
it
leads to obsessive over dissection
in
an endeavor
to find
the
neck
ofa
sac which is nonexistent
orcx
cessi
vc
manipulation
in
the
region
oftbe
neck.
Television
As memioned above, television has imponant
ed ucational adv3mages (live visualization of
microanatomy and taping procedures for fu
lure teaching) as well as practical advantages
[
17
,32]. Operati
ng
room physicians and nurses
alter their anesthe
ti
c techniqu
es
and ongoi
ng
activities
as
well as morc efficiently prepare for
anticipated operative CVClllS based on informa
tion received from
the
television monitor.
Color television systems (see Fig.
2.7
B) for
the microscope arc in a state of rapid evolution
in
terms of image clarity and brighmess,
weight, durability,
and
freedom from need f
or
frequem
repairs. Hence, il is pointless to rec
ommend specific systems allhis time.
Many
of
the newer television cameras can
operate at a lower light level. Yct it is still advan
tageous to obtain good lighting to allow a smal
l
er
diaphragm opening and consequently a
greater depth
of
fie
ld
and sharpe r focus.
Table
2.1
summarizes some methods to im
prove lighting for the s
ur
geon
and
for
the
tele
vis ion or pho1.Ographic cameras.
Overhead Table
In our
experience, the overhead table (sec
Fi g. 2.2 C)
made
by the Ph elan Manufacturing
Corporation (Minneapo
li
s) has provided
maxi mum advantages for the surgeon, anes
thesiologist, scrub nurse, and patien t. The cra
nial end of the table should bejustcaudal to the
patient's shoulder (more caudal if the cervical
carotid arter y needs
1.0
be
exposed).
The
table
height is easily adjusted, and the nurse or tech
nician has clear
and
rapid access to instr
u
mems and the su rgeon 's hanet.
I ntraoperative Instrume ntation
Fishhooks
The use
of
improvised
ti
ssue-retraction hook
s,
or "fishhooks," connected to rubber bands h
as
Table 2
.1
. Methods
of
mprovi ng lighti ng for the sur
geon an d/o r camer<ts."
I. I ncrease voltage in transformer
(s
hortcns bu lb life).
2. Use an cfficiem lighting sys tem (currently
in
state ofim·
pnll'ement).
3.
Keep
hull>s
and
op
tic
al
system clean.
4. Discard bulbs ",it h blue or dark spots
in
light image.
5. Usc
add -on light sources.
6. Usc short focal length objecti\'e lens.
7. Avoid zoom ens system. which absorl>s more light.
8.
Turn
off
bright lights in opcr.lting room (bener con
u'ast; surgeon's pupils arc dil'lIcn. rcrruiring less lig ht ).
9. use of inlernal rencctions in surgical wound;
a,-oid rencclion s back
in
to the microscope.
1_
Remo" e black paint border aruund glass light dencctor
behind objecti
ve
lens (present
in
some microscopes).
II.
Usc
30-70
beam splitrer (70% to side arms. onl),
30%
(0 surgeon) inslead of 50-50 beam spliuer.
1
2.
Use greater magnification
in
e)'cpicces. thercby requ i
r
less rnagn
.i
fic3tion (hence less light loss) inside
mrr.ros<;ope
unll.
13. OllCn diaphragm to camera (with loss
of
sharpness and
depth of focus).
14
. l'rollCrI}, adjust
TV
camera power supply and TV
monitor.
15. SeleCl
efficient
TV
camera
or
film that can OllCrale
wit
h
less light.
Certain mClhods li sten ha\'e particular \'"Iue
in
some cir
cumstances, whereas
in
others they may pro\'e unneces
sary or impractical.
It
ems I through 10 also increasc
brightness for the surgeon. Item II d e c r e s e ~ image
brightness
to
the surgeon. From
Fox
et
al [ 17 1.
been used by many surgeons to retract scalp,
muscle,
an
d du ra. More recently a fi shhook re
tractor devi
ce
usi
ng
springs (Aesculap Instru
melll Co.) instead
of
rubber bands has been
suggested [57
].
We prefer the "disposable"
Week
Durahoo
ks (Edward
Week
and Com
pany), although one can remove their rubber
bands for repeated usc.
The hooks are used to retract the froillolem
poral scalp flap tlIrned over the patient's
forehead as follows (Fig.
2.9):
The sterile
dr
apes between the overhead ta
bl
e (neu
ro
sur
gical instrume ll t table; Phelan Manufactllring
Corporation, Minneapo
li
s) and the patient's
head are-held firmly downward and cauda lly
by
st
andard rubber
suction tubing of appro
priate length. The looped end s of thi s tubing
arc secured LO stirrup clamps on each side
of
the OR table. This lube
(a)
firmly h
ol
ds the
drapes in place and (b) allows a convenient site
of
allachmem fo r the
rub
ber bands th
at
retract
both the scalp hooks
and
the bone flap. I n this
way
the drapes of the pcrioperalive field are

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 31/213
Intraoperati\ e Ins trumentation
23
Fig. 2.9. Close-up view of ru bber tube holding
drapes firmly (sec Fig . 2.7
A).
H
ere
the samc tubing
is
used to attach the rubber
b..1nds ho
ld ing thc fish
hooks. T hese fis hhooks retract thc oxrccllulose-co-.
vcred scalp
nap
forward.
The
ri
ght fromolateral
smooth, firm , and dear
of
unnecessar ydamps
and other retractors.
SUClion an d SUClion- l
rrigat
i
on
Devices
SUClion tubes usually are sized (diameter) by
the "French" (Fr) designation: a 3- Fr size has
an oLlterdiame ter of 1 mm; a9-
Fr
size is 3 mm ;
ct
c.
Standard si
zes
for ane
ur
ys
m s
ur
gery are
3-
Fr
, 7-Fr, 9-Fr, and II -
Fr
, al though there are
many other va riatio n
s.
There are a multitude
of types of suc
ti
on lubes with variations in
length. ang
ul
ation, tip con figuration, and
vac
uum pre
ss
ure [3, 5, 17,28,29,44,56, 57J.
A S
UCl
ion system wi th a mechanism to con
trolthe negative pressure at ve ry l
ow
levels is
essential.Th e suction should be finel yadjusled
to eliminate the ha7
..1n
l of small anatomical
structu res be
in
g entrapped and damaged.
Many neurosurgical suction tubes are con-
bo nc nap is attachcd
to
the l
cm
p
ora
l
is
musclc (a t
cemcr of figure). Dural lack-up sutures and bonc
nap
sutures are in place in the cranium before the
dura is opened. From Fox
[ 16].
slruCled to allow reg ulation
of
suction strength
by adjust ing the degree to w
hi
ch the
thumb
occludes the air ho le. T h
ese
holcs can be en
larged [5, 29]. and/or ventin g needles can be
placed in rub
ber
suc
ti
on tubes. T he trap bot
tles can have press
ur
e- regulating gauges.
When di ssecting delicate Slnl
ClUres,
it may be
helpful to use special smooth-tipped su
ct
ion
tubes and negative pre
ss
ur
es of about 2 m
of
Wale I' (a pproximatel y 0.2 alln ) [57]. I n place of
wa ll sllction, s
ome
sllrgeons prefer an electric
suction pump, easily regula ted by adjus ting the
d ia ls on the pum p.
Irri
b'<lt
in g fluid in cunjunction with the suc
tion apparatus is essential during the surgical
proced
ure
. In addition to keeping tissues from
drying and t he an
eu
r
ys
m wa ll from becom in g
briule, it disco
ura
ges the formalion of small
blood clots and their.adherence to the dissect
ed surfaces; it also increases the effectiveness

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 32/213
24
2.
Instrumentation and Positioning
of bipola r coagulati
on and
re
du
ces tissue adhe
siveness. Co nsta
nt
bathing with CSF has the
same effect. Some s
ur
geons
pr
efer a comb ina
tion suction-irrigation unit.
We usually use an angu latcd Frazier suction
tube of va ryi ng leng ths. The II-Fr and
g-Ff
sizes are used for cra nial wo rk
and
the 7-Fr for
aneurysm dissection. We use the 7-Fr size
r
at
her than sma
ll
er sucti
on
tubes because of
its
usc as a dissector and retractor as we ll as a suc
tion device. Moreover, the la rger diameter pro
vi
de
s less air a
nd
liquid ve loci ty for the same
vacuum
pr
essure.
The
metal sucti
on
tube can
also
be
used for resting micro
sc
issors or
other
instruments to reduce tr
emo
r when making a
delicate dissection. The suction lube is held in
the su
rgeo
n's left hand , often with his ha nd or
fifth finger resting
on
the Leyla retractor bar
of
the sku
ll.
(T
his
rest
i
ng fi
nger" serves
more
to provide
pr
oprioceptive feedback
rather
than comfol"( to the surgeon. ) The
SUCl
ion is
often used against sma ll dental cotton balls
(Ri chmond Denta l Colton Co
mp
any, Char
lotte, North Carolina) or sma ll cottonoids for
su
ct
ion protection and retraction. Rubber tub
ing is
pr
ef
erred
to plastic tubing, the latter
being too stiff for com
fo
rta
bl
e usc.
We
routinely put 1,000
unit
s
of
heparin in each
liter of irrigating solution
1.0
limit
dotting
,
which could cause obstru
ct
ion within the tub
ing; this practice may r
etar
d undesirable d
Ol
ting in
the
basilar cisterns as well. The
on
ly
time we use a suction-irrigation apparatus
(House-Radpour unit) is
during
bone
(s phenoid wing or clinoid
pro
cess) drillin g.
Bone-Remova l
Instrum
ents
In
19
30 Rogers [46] gave
an
excelle
nt
historica l
account of cra niotomy m
ethods.
He noted th
at
the
Hor
sl
ey tre
phine h
ad
its
or
igins in
the
time
of Hippocra tes (ca 400 years Be). The
technique
of
bone flap removal made a si
gn
ifi
cam adva nce with Cigli's
ap p
lication of the
wi re saw (the Cigli saw) in 1894 [19, 20]. This
saw
is still routinely used by many s
ur
geons -
especially in elderly pat ients w
her
e the dura
may be stuck to the inner table of the skull. T he
prese
nt
-d
ay
use of
powe
r (pneumatic or elec
tr
i
c) dr
i
ll
s and
cran
iotomy for lifting skull flaps
is
we ll
known
and
requires no
further
discus
sion here.
Rongeurs for biting a
way
the base of the
bone flap
are
stand
ard
in any cranio
lOm
y set.
We commonl y use the Le ksell, Echlin, and
Le
mpert
r
ongc ur
s for fronto
tempo
ral
crani
olO
my, wh
ere bone is
ronge
ured
away
at
the
base.
The
flat-jawed Le
mpert rongeur
is
especially helpful for removing that portion of
the sp henoid wing sticki ng Out as a ridge to
wa
rd
the
sylv
ian fissue.
The
neurosurgeon
needs a sma ll , high
speed electric
or
pneumatic drill f
or
removing
the sp henoid ridge, the clinoid
pr
ocess,
and
other
protrusions of the cranial base; however,
only
after
he has become acquainted with and
skilled in its application in
the
laboratory
should he use a high
-s
p
eed
drill in a ne
uro
s
ur
gica l
operation
[17J . A drill that ca n reve rse its
dir
ection is pre fe rred by some to
one
th
at
cuts
in only
one
direction. A constantsuctioll-irriga
tion sys t
em
with physiological saline ca n be
used to cool the
dr
ill
; o
ther
wise, h
ea
t is trans
mitted to nearby ne
ur
al structure
s.
One ob
mins a m
ore
acc
urat
e and controlled use of the
drill when it
is operated at
high speeds; onl y
very slight pressure should be used to remove
the bone. Dan
ge
rous skiddi ng may OCClll"
at
slow speed sor with dull drill bi ts because of the
greater
pr
essure needed to cut bone. When
using
li
ghtweig
ht
dr
ill
s
or bur
rs, steel
burr
s are
used when the drilling is remote
fr
om the
dura. Diamond burrs are safer close to the
du ra or vital stru ctures, for they tend less to
tea r SOflli
ss
ue.
We
use oxycellulose
rather than
cotton s ponges to cover the n
ear
by galea, mu
s
cle, and bone flap, as no ha rm occurs if these
get caught in the drill. Co
uon
, on the mher
hand
, may cause serious damage if caught in
the drill.
When using bonewax
under
the micro
scope,
we
have fo
und
the fo llowing to
be
help
ful:
The
sc
rub nu
rse
app
lies a sma
ll
bit of
bonewax to
one
side of a sma
ll
, d
ry COllo
noid
and hands it by bayon
et
forceps
to
the
center
of
the surgeon
's
op erative field. The surgeon
then can use his bipolar forceps
(w
it
hout
cur
rent applied) or h is finger to pu sh the C01-
tonoid against the wax, which is pressed into
the bl
eeding bone. Usua
ll
y
we
use this
technique on the sph enoid wing after drilling
it
und
er magnification.
Electrocautery
Electrocautery for coagulation of vessels
and
vascular
ti
ssues has been
an
in1.egral pa
rt
of
neurosurger
y
ever
since the
advent
of the

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 33/213
Im
r3oper.uivc Instrumentati
on
Fig. 2.10.
Fox
bipolar elec
trocautery f
orceps in
three
len
gt
hs: 16, 18,
an
d 20
em.
Eac
h of
th
e straight force ps
cO l11
es
in
0.5-
and
1.0-111
111
diamete r t
ip
s; curved and
angled tips al
so
are
availa
bl
e.
From Fox [16]; counesy of V.
Mue
ller
Compau)'.
Chicago.
..
B
ov
ie electrosu
rg
i
cal
un i
t,
repo
ned
by
Cus
hi
ng and Bov ie in 1928 [7]. Light [38] gave
a good histor
ica
l overview of the subject in
1945. In 1967 Malis [39] reviewed the de,'elo
p
men
ts
and evolution of bipo
la
r cl
e<.:
trocoagula
tion since thc
ti
me of Grcenwood in 1940 [2 3].
" Monopola r" elcctrocoagulation has be en
and continues
to be
commonly used to coagu
late or c
ut tissues. (Of course, it is really bipo
lar: On e pole is the ground plate and the
other is the hand-hcld electrode.) Bi polar elec
trocoagulatio n
of
the type whcre both poles
arc
in the forceps
was
d
ev
eloped by Grcen
wood [23-26]
to
caute rize sma
ll
blood vessels
on the spinal co
rd
, whcre minimal heat and
electr ical spread ,.,re re essentia
l.
Accordingly.
the bipolar forceps basically consis
ts
of a mod
ification
of
ordinary
bayo
net forceps or jewe l
er
s' fo rce ps in wh
ic
h each blade of the forceps
is one of the electrodcs or po
le
s; the blades are
i
so
l
at.e
d from each Other by insula
ti
on, whi ch
se parates them at thei r base.
For microvascular and intracranial
aneurysm surgery and ford issection of tumors
from the brainstc
lll
, bipol
ar
electroc
aut
ery
units have become essential. Th ere h
ave be
en
many mod ifica tions in both the fo rceps and the
po crs
upp
ly [8, 13, 1
8,23-27,33,3
4
,3
9,47,
52.53, 5
6,57].
Ma
li
s [39] improved
th
e powe r
supply ( 0 prov id e a damped wave spark unit
that
was
electrica lly bener
iso
lated.
Thi
s unit
(Cod man and Shurtleff Company) has been
one of the more popular and reliable un its for
neurosurge ry (a nd is prefe rred by us).
Th
e
unit was designed spec
ifi
cally to prov ide the
be st coagul ation at the lowest
vo
ltage with the
least mu
sc
le stimula
ti
on. At the same
ti
me, it r
e
stricts the cur rent to the shon cst path bet
wee
n
the tips of the twO blades of the forceps, with
no currenL of consequence now ing from tip to
gro
und
or tip to pa
ti
ent. Th e greater sa fety of
bipolar coagulation compat'ed
wi
th monopolar
coagul ation around bra
in
stem structures was
demonstrated by Gestr ing
et
al [18].
So
me t ried to
pr
ovide a single unit f
or
both
mono polar and bipolar electrocoag
ul
ation [ 18,
27]. Sugita
et
al (52, 53] uscd a ther
mi
ster at
the tip of
their forceps to
aUlo
maticaliy cut o rf
the eleclri
ccur
ren t when a preset temperature
was rcached. Others developed a suctio n [47]
or irri
ga
tion [13, 34] sys tcm attached to one
blade of their forceps. Del ong and Fox
[8]
d
e
scri
be
d an automalic
cy
cling on-off bipolar
electrocautery powe r supp ly.
We
used to
pref
er the bipolar for
cc ps [56, 57] (Mat hys & So h
n,
Zur ich
),
but we
now use the stain less-steel Fox bi polar bayo net
forceps (V. Mu eller Co
mp
an
y,
Chicago)
(Fig. 2
.10
). T hesc forccps come in 16-, 18-, and
20-cm lengths and with 0.5- and
I.
O-mm tip
diametcrs.
Ot
her popular bipolar forceps
fo
r
sur
ge
ry include the Rh oton
round
-handled
forceps and the Malis forc
ep
s with the blades
slightly angled dow nw
ard
rathe r than parallel
lO the hand le. Ti tanium
or
st
ai
nless steel are
comm only us
ed
metals, the fo rmer being
liglllcr. We pref
er
the heavier
weig
ht of the
sta in less-steel forceps for bettcr balance, com
fo rt, and p ropriocepti
ve
feedback.
It
is impor
tant n
Ol
to sterilize titanium and stainless-steel
instruments in the same pac kage, for the dif
fere
nt. metals in close proximity m
ay
create an

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 34/213
26
2. Instrurnenta
ti
on
and
Positioning
electrical potcmial conductive
to
rusting and
co rr osive activit),.
De Long and Fox [8} recommended the fol
lowing
care
of these forceps to limit
thc slicking
oftisslICS to
their
tips:
I.
Do
not
short-circuit the elect
ri
c c
urr
ent
by
touching the forceps lips together.
2.
Clean the
lips
frequem ly only with a
damp
d
ot
h (not with the scalpe )
3. Po
li
sh the lips periodically (
or
obtain new
forcep
s)
when the tips become pitted and
rough.
4." Knead " the tissue between the forceps tips
by gelltly squeezing and releasing the for
ce ps blades.
5. Lift lhe forceps from tissue contact fre-
quentl y.
6. K
ee
p
the
ti
ssue moist with CSF
or
sa
line.
7. Avoid high current settings.
8.
Apply
the
currCIll
in shon
bur
sts
to
allow
heat dissipation.
Wc usc the bipolar forccps as the principal
d isscCling a nd tissuc-separating instrument
intracraniall
y.
For this reason the blades of the
forceps mu st have
pr
oper s
pr
eading tcnsion,
yc t n
ot be
so tense as to ma ke tip approxima
tion un comfortable. T h
ey
must not rotatc in
appropriately in the s
ur
gcon's hand. In terms
of tim c, its actual application for e lec
tr
ocautc
ri
zation is quite sh
ort
compared with
its use
as
a
tiss
ue dissector, pcrforator,
spreader, se
par
atet; and grasper. It is uscd to
place and remove cotlonoids , cotton balls, gela
tin sponge, gelatin paste, oxycellulose, and I'LIb
bel' or
plastic sheclS.
On
tcrms of frequenc ),
and duration of usc, for us the suction lube (in
the surgeon 's left hand) and the bipolar elec
trocautcry forceps (in the right hand) havc be
come thc main micros urgical inSlrulllcnlS dur
ing intracranial s
urg
cr)',
For most of o
ur ext
racranial cauterizati
on
we
u
sec
ither
the mon
o
polarorth
e bipolar unit
with the
Mali
s powcr supply dial set at 30 or 35.
On
cerebral cOrtcx wc use the Malis bipolar
power supply dial al the 25
to
30 seuings: on
the brainstem
we
use the 15 to 25 setting
s.
"ine r-tipped forceps increase thc cun'ent den
sity
at the tips. I f
hi
gher settin
gs
are
required,
lhe spark ga p in the unit probabl y needs reset
tin
g.
With faulty spark gap distances or other
electrical problems, one can use hi gher power
settin gs to obtain
mor
e current, but the quality
(waveforms)
of
the electrical OLitput w
ill be
pOOl
; resulting in p
oor
coagulat ion and a tcn
den
cy
for vcssels to explode or be incised. Pro
longed or illlensh'C use, even in one patient,
may res ult
in
a need for an elCClrical overhaul.
Thcrefore, twO or more such bipolar powcr
supplies should be available.
We
use a 15-foot
cord between the power supply and the for
ceps. Longer cord s may cause defective electri
ca
l output at the forcep
s. We
set the pow
er
sup
pl
y at the foot
of
the
OR L:'l
ble. I n this position
it does not add to
th
e instrument cluneI' near
the surgeon, and ilS electromagnetic noise
emission is a sufficient di stance from the televi
sion sys tem so as to not c"eatc any significalll
audiovisual in t
cr
ference. For the same reason,
the wa
ll
socket plug-i n sites for the television
and the bipolar I)()\\'er supply units should be
at a considerabl e di stance from each other. The
"
mono
polar" a
nd
bipolar electrocautery cords
should not be dose to each other.
Retractors
In past yea rs m
OSt
brain retrac
ti
on
wasdonc
by
assistant surgeon
s.
Such retraction
was
often
in
consistcnt , inaccurate, and dangerou
s,
as
brain retraction prcss urc exceeded cerebral
pcrfusion pressure. In 1958 Gi llingham
[21]
warned that bleeding from an aneurysm at
s
urger
y (causing reversal of blood now from
vital brain tissues and a
drop
in blood pressure)
may res ult in ischem ia of nearby brain tissuc.
He wa rned that this would be aggravated
by
ex
cess or prolonged brain retraction. Addition
all y, he ca ution
ed
th
at
inacc urate o r excessive
retraction may place traction on vital per
forators, produc
in
g vasospasm and in
adequate cerebral perfusion. Albin et al
[ I.
2,
17 ] havc sh
ow
n
that
brain retraction pressures
exceeding 20 I.orr cause underlying brain dam
age. I f induced hypotension is used, evcn Icss
brain retraction prcssUl'e
is
IO
lerated.
A num
ber
o f authors have described t he use
of self-rel.aining brain retractors [17,29,30,40,
42,57], Various t )'pes, eit her in the literature
or in co
mmer
cial catalogs, have included the
de Mane l , Dolt (Edinburgh
),
Hamby, Green
berg, (Le yla), Dohn-Carton.
Malis,
Cloward, Enker, Mi skimon, and Jannclta re
tr
actor
sys
tem
s.
Self-retaining retractors also ha
ve
become
indispensablc to aneur
ys
m surgery because
they allow th e surgeon to work in a relatively

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 35/213
Othe r Microsurgical Instruments
27
confined space unhinde red by the presence o
f'
an assistant's hands, whi ch are less dependable
for maintaining constant retraction
of
the
brain.
Sel
f-reta
in
ing brain retractors arc
of
two
basic types [17].
One
is composed of a series
of
straight shafts attached
by
small clamps to gi
ve
the co rrect arm length
and
con
fi
guration re
quired for holding the brain spatula in place.
The oth
erco
nsislS
of
a series
of
ba
ll
-and-socket
un its resembling a chain of peads wi th an inter
n
al
cable th
at
when tightened, remains
in
the
desi red position.
Of greatest impo n ance in intracranial
surgery
is
the minimal brain re trac
ti
on neces
sary (Table 2.2), ascribable not only to u
se of
the su rgical microscope and microtechnique
but also
to
improvemenls in exposure tech
n
iq
u
es
that a
ll
ow
a lowel; basal, and ta ngential
approach to the base
of
the sk ull and the circle
of
Wi llis, which is partly aided
by
removal
of
a
portion
of
the sphenoid wing and lhe use
of
special self-retaining brain retractors. How
ever, these aids wo u
ld
be tota lly useless without
a relaxed brain effected
by
proper timing
of
surgery and
by
supe
ri
or anesthetic and life
support methods.
The selection
of
a self-retaining retraClo r
system is up to the individual surgeon's prefer
ellce and habi
t.
Many prefer systems that at
tach only to the sku ll. T hey
are
concerned that
table- mounted retractors may move relative to
the brain even if the skull is immobilized
by
three-point fixatio n
[40].
We have found that
the
a ~ a r g i
(Lcyla) retractor system
(Fig.
2. 11) is ideal for most cases
of
intracranial
aneurysm surgery. We auach the bar to the left
Table 2.2. Minimal brain retraction.
I
crmincd by:
I. Usc of microS(ope. mi<;rotC(;hnique
2.
Low
oosal. tangemial approach
3. Self-retaining br.lin retractor
4. CSF drainage
:1. Neumanest hetic techniques
Avoids:
I. Removal
of
significant brain for exposurc
of
lesion
2. CUlling
of
Olfactory nCf\'c
3. Dil'iding
of SOIllC
bridging I'eins
4. Secondary brain contusion o r edema, vascular spasm
5. Vascular compression
by
retractoror stretched arachnoi
dal bands
6.
Tr.letion on aneurysm
7.
UnnC(;essary exposure
of
A·I and
M-I
arterial segmcl11s
From Fox et
al
r 7 1
side
of
the O R table
just
cranial to the "ether
screen" attachment (which holds drapes that
separate the microscope from the anes+
thesiologist; see Fig. 2.2 B) . Two or three
fl
exi
ble (unless tightened) retract
or
ar
ms
are at+
tached to the connectors on the bar.
All
joints
must be firmly tightened to
avo
id drif
t.
Fi rst, se t the retractor blade (in the flexible
arm)
neal"
the planned retraction site. T hen
tighten the flex ible bar by turning [he sc r
ew,
which pu lls the internal wire tau l. Last, "toe
in" the retractor blade to its desired position
and retraction pressure and then tighten its
win g nut. Drift
is
minimal or absent if done
prope
rl
y.
Al
ways
have the poilll
of
connect
io
n
between the retractor blade and flexible bar
away
from the
cra
n
ial
opening. This requires
auaching the flexible arm
ncar
the
end
of the
re tractor blade and bending the blade at its
proper point for descent in to the c ranial cavi ty.
T hi s maneuver gives better
in
tracranial expo
sure wi
thout the ends of the
fl
exible retractor
arms being in the
way.
Alth
oug
h these retractors are usua lly
ap plied against brain tissue
or
its coverings, on
occasion a narrow retractor ca n be used to
gently retract nerves, aneurysms, or
ane
ries
such as the internal carotid anery or the mid
dle cerebral artery during frontotemporal ap
proaches to the interpeduncular cistern [16,
48,50,51]. Such retraClion requires d
is
pl ace
ment and protection
of
these arteries \I'jthout
occluding the
m.
O ther Microsu rgical Instruments
T h
ere
are n
ow
a large number
of
microsurgi
ca l instruments in the fie ld of neu rosurgery.
We cannot review
all
of
them in th is rapidly
changi ng field .
Fig
ures
2.
12
and
2.
13 i
ll
ustrate some
of
the
instr uments we most commonly use for micro
dissection.
The
jewelers'
fo
rceps is used to pick
up the arachno id over the
sy
lvian
fiss
ure to
in
i
tiate opening of this fissure. T he Aescu lap
bayonet sc issors (curved and straigh
t)
come in
three lengths (16 cm for surface wo r
k,
18
cm
f
or wo
rk
about
the ante rior circle of
Wi
llis, and
20 cm for deeper work, eg, abou
lthe
posterior
circle
of Wi
llis). T here is also a 22-cm scissor.
The bipolar forceps have been described in the
ea
rl
ier section on electrocautery. T he Rhoton

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 36/213
28
A
B
c
2. Instrumemation and Positioning
....
-
Fig.
2.11. A- D. Leyla
gil) re
tractor system.
Cour
tesy of Aescul ap-
\'\
'
er
ke AG,
TUlliingen, \Vest Ge rmany.
B. Close-up view of auach
mCIlt
head between the bar
(left)
and retractor arm co
n
nector (right). C. Close-up
view
of
connector bell,'ceo
b
ar
and OR table.
D.
Retrac
tor h.1r and attachment head
in prcliminaryposition.Above
is the draped sca lp wit h an
outline
of
a righl
froruolat
eral craniotomy incision.
From Fox [ 16] .

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 37/213
Olh
er
Microsurgical Instruments
29
fig.
2.
11
instruments show n
in Fig.
2.13 are the four
types most commonly used
by
us.
Th
e "Iong
flat instrument"
(a ,.
micro-Penfield No.4
")
is
used
to
retract nerves, arte
ri
es, and the
aneurysm. The short
fl
at instrument" is ideal
for se parating adhesions between an aneurysm
and adjacent tissues because the edges
of its
angled, flat end are somew hat sharp.
The
40°
hook is
sa
fer to use than the rig
ht
-angled hook,
for it w
ill
not
catch and tear tissues
upon
iLS
re
moval from the field. A ba ll-tipped hook also is
helpful.
I nstruments
and
suture for reanastomosing
or
repairing blood vessels and nerves should
be available along wit h the expertise to do so.
These are detailed in many articles on micro
vascular anastomosis.
These microsurgical instruments require
some trai ning and experience in their use and
manipulation through a small opening and in
sid e a deep narrow cavi ty. The surgeon can rest
hi s hand on the skull
oron
the Ley la retractor
bar (named after the daughter
of
which holds the self-retain
in
g retractors.
Often the surgeon rests only his fifth finger as
a point of propr io
cept
i
ve
feedbac
k.
This allows
sensory orientation and reduces tremor.
One
in
strument can also be rested on the suction
tube
of
the surgeon's left hand to reduce tre
mor in critical moments.
On occasion a
mirro
r at the tip
of
a probe
can be useful for seeing behind and around
va rious structures. Wilson and Spelzler 154]
used a dental mirmr, Sugita et al [49] a 5-mm
mirror, and a ~ a r g i l and colleagues [57J a mir
ror that changes positions when the grip han
dle
is
squeezed.
There
now are many types, sizes, and config
urations
of
vascular and aneurysm dips and
clip-appliers. These are in a continual state
of
evol Ulio n, and lhe reader is referred to oth
er
articles on the subject
[14, 16
]. T he technology
D

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 38/213
30 2. Instrumentation
and
Positioning
fi g. 2.12.
uft:
Jc\\'clc l'
s'
forceps (Ed ward Week &
Co .).
C ~ l I l f r ; Bayonet sha ped m icroscissors (Aes
culap Instruments). Rig"': Ua),oncI shaped bipolar
electrocautery forceps (Math)'s & Soho
).
From Fox
116].
of
energy transfer (la
se
r, ultrasound)
in
the
operating room is a large and changin g field
that will not
be
a
ddr
essed her
e.
Bibliography
I. Al
bi
n MS, Bun
cg
in L, Be n nc lt MH et 31 (19i7)
Clinical and experimemal brain retraction pres
sure monitoring. Ac ta Ncurol Scand (supp 64)
56: 522 -523
fi g. 2.13. En larged view of microsurgical dissecting
instr
um en
ts
(Rhoton ty pe: V. Mueller
Co
mpany).
Ltft
nld:
No. 7,
or
"Iong
nat
ins
tru
ment."
ufl
1 l ~ r :
No.2, o r "short nat
instrument,"
RigJllullter: No.
II
,
or
"40
0
h
oo
k."
Righi tl,d:
No.
10,
o r right angle
hook." From Fox l I6].
2. Albin MS, Bun
eg
in
L.
Dlti
OV
IlY M et al ( 1975)
Brain retraction preSS urC
dur
ing
intra
cranial
pr
ocedu rcs. S
ur
g
,"b
rum 26: 499 - 50 0
3. ll.1d cr DCH (1975)
i c r o - s r g i c a l
trea tmen t of
intracranial an cur
ys
ms. J Neurosurg Nurs
7:25
- 27
4. Bischoff EPE ( 1865)
M i k r r u w J ~ h
Analys
t
der
ArwstomoStn der Kopfr trot
rl.
Mun ich , Vc rlag der
JJ Lentncr'schen Buch
handlun
g. See 'H
icroscopic
Arw{ysis
of
tht Allas/olllos;s
U
p/weer
/IU
emllia{
Nerves, translated by Sachs EJr, Va ltin £W (1977 )
Hanover, NH, Uni\'ersity Press o r New En gla
nd
5. Bo
nd u
ra nt CP (1977) Altera tion or su
ct
ion lip
prcssure. J Neurosurg 46: 559
6. Co lley PS, Du n n RC J r (1979) P
re \
'ent ion or
bl
ood
pr
essu re responsc
10
sku ll
-p
in head
ho
ld
er
by
local
anest
hesia. Anesth
Ana
lg (C le\'e)
58:241-243
7.
Cushing H, BO" ie WT ( 1928) Electro-su rgery as
,III aid to the rcmoval or im racra nial tu
mor
s.
Surg G}' llccol Obstel 4 7: 751- 784

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 39/213
Bibliography
31
8. De lo ng \VB, Fox J L (1977) Automatic q-cling
bipola
rcoag
ul ator. Surg Neurol8: 15 - 16
9. Donaghy R
fo.
·IP (1979) The history
of
micro
surgery in neurosurgery.
Cli
n Neurosurg
26:619-625
10. Donaghy Y a ~ a r g i l MG (1967) MicrQ-WSW
lar
Surge/yo
Stungart, G T hieme
II. Drake
CG
(1965) On the surgical treatment
of
ruptured intracranial aneurysms. Cl
in
Ne
urosurg 13: 122 -
155
12. Drake CG (l976) Ccrcbral aneurysm surgery
an u
JXI
atc, in Sc h
ei
nberg P (cd):
Cerebrqvascular
Disease. Tenth Prineeton Conference. New ' ork,
Ral'en Press, pp 289- 310
13. Dujovny M, Vas R, Osgood CP et al (1975) Au
tomatically irrigated bipolar forceps. Technical
note. J Neurosurg 43: 502-503
14
.
Fox
J L(1976) a ~ c u l a r c l i p s forthe microsu rgical
(reat melll of stroke. Stroke 7: 489-500
15.
Fox
J L (1979)
Mi
u osurgical cxposure
of
intra
cranial aneur ysms. J Microsurg I: 2- 31
16. Fox
J L (1983)
Intracranial Aneurysms.
New Y
or
k,
Sprin
ger-Ve
rl ag, pp 678 - 707
17. Fox .I L, Albin MS, Bader DCH et a1 1978) Micro
surg ical treatment of neurovascul ar disease.
Ne
urosurgery
3: 285-337
18. Gestring FG,
Koos
WT, Boeck FW (1972) Bipolar
coagul ation with modified cOtl\'emi onal elec
trocoagulators. Tec hnical note .I
Ne
llrosurg
37:50 1- 504
19. Gigli L (1894) Ober ein neues I nstr ument zum
Du rchtrcnnen der Knochen , die Drahtsage.
Centralbl ChiI' 21: 409 - 4 11
20. Gigli L (1898) Zur Technik
der
temporaren
Schadelresektion mit meiner Drahtsiige. Cell
tralbl Chir 25: 425- 428
2
1.
Gi
ll
ingham
fJ
(1958) Th e management
of
ru p
tured intracran
ia
l aneurysm. Ann R Co
li
Surg
23:89-1 17
22. Gi lli
ng
ham FJ (1976) Twent)'-five
exper
i
ence wit h mi ddlc ccrcbral aneu rys ms. Rev Ins[
Nac Ncurol (Mcx) 10; 16-21
23. Gree nwood J J r (1940) 1 \\'0 point coagulation. A
new p ri nciple and instrument for applyi
ng
coagul ation current in ncurosurgery. Am J Surg
50:267-270
24. Grecnwood
.I
JI"
(194
2)
1
\\'0
point coagulation. A
fo ll
ow-u p r
eport
on a new techni<l
lI
e and instru
ment for electrocoagulation
in
neurosurgcry.
Arch Ph
ys
T her 23: 552- 554
25. Greenwood J J r (1955) Two-point or interpolar
coagulation. Review after a twelve-}'car period
wit h lotcs on add ition of sucker tip. J Neul"Osurg
1
2:
196- 197
26. Greenwood J
.I
I'
(1974) ElcClrocaag ul ation in
n
eurOSUl-gcry.
Surg Ne urol 2: 4
27. Gurdjian
ES,
Thomas L
M,
Gurdjian
ES
(1968) A
sin glc unit for bipolar, rnollopol
ar
coagu
la
tion,
and cutting / Nc urosurg 29: 567 -568
28. Hamby
\V
B (1952) Intracranial Anellrysms.
Sprin gfield , IL. Charles C
Th
omas Pu blisher
29. Hamby \VB (1969) Intracra nial surgery for
aneurysms. P
rog
Neurol Surg 3: 1
-65
30. Hamby \VB (1970) Remark
scoll
cerni ng intracra
nial aneurysm
sU
I·gery. Clin
Ne
urosurg 17: 1- 17
3
1.
Hocrenz P
(1980-
1981) The
opera
ting micro
scope. J Microsurg I: 364-369, 419-427;
2:
22-26, 126-139: 3: 179- 182
32. Housepian EM, Ungcr \VH. Scharff
TB
et al
(1975) Expericnce with videotape monitOring of
mi
croscopic neurosurgical proce
du
res. J
Nc urosurg 42: 204 - 208
33. Jacques S, Bullara L
A,
rudcnz
RH
(1976) Micro
vascul
ar
bipolar coag
liJ
ator. Technical note. J
Ne urosurg 44: 523 - 524
34. King
TT,
Worpo e R ( 1972)
Sel
f-irrigating bi
lar diather
my
forceps . J Neurosurg 37; 246-
247
35.
K
riege
l'
A (1978)
The
Use
of
the Operating Micro
scope. New York, Carl Zeiss
36. Kurze
T
(1964) Microtechniques in neurological
surgery. Clin Neurosurg I I : 128-137
37. Kurze T, A puzzo M q , \ \'eiss M H e t aJ (1977) E
x
pericnces with sterilization of the operating
microscope. J Neurosurg 47: 861
-8
63
38. Lig ht RU (1945) Hemostasis
in
neu
l"Osurge
r
r·
.I
Neurosurg
2:
414-434
39. Malis
LI
(1967) Bipolar coagulation in micro
surgery. in Dtmaghy RMP, Ya§argil
MG
(cds):
Micro-vascular Surgery.
Sw ug;m , G Thieme,
pp 126- 130
40. Mal is Ll (1979) Ins trumentation and techniques
in microsurgery. Cl
in
Ne
uros
ur
g 26:
626-636
41.
Ny
len CO ( 1954) Th c microscope
in
aural
surgery. I S first use and l
ater
development.
Ac
ta
O[olaryngol [Supp l] (Stockh) 116: 226- 240
4
2.
Peerless
SJ
(1974)
The
surgical approach to mid
dle cerebral
and
posterior commu ni cating
,IllC\lI·ys ms. Clin Nc urosurg 21: 151- 16.?
43. Rand RW (1985) Micronellrosmgel)i cd 3 SI Lo u
is,
CV Mosby Co
4
4. Kh
oton AL, Merz W (1981) Suction lU
beS
f
or
con
\'eI1lional a
nd
microscopic neurosurgery. Surg
Neurol 15:
120
- 124
45. Robertson GE (1967)
Pllellmoenuphalogm//hy,
ed 2 Springfi
el
d, 1L, Charles C T hom
as
Pu
b
li
sher
46. Rogers L (1930) T he history
or
craniotomy: an
account of the methods which have been prac
ticed
and
the instruments used f
or
openi
ng
the
huma
ll
sk ull
du r
ing life. Ann
Med
Hist 2:49:)-
514
47. ScarffTB
(197
4) A nell' bipol
ar
suction-camery
forceps fo r microncurosurgical use. Surg
Neurol
2:
213
48. Sugita K (1985) Mic1"01Ie1lrOSlagicai
Atlas.
Be rli n,
Springer-Verlag
4
9.
Sugita
K,
Hirota T , Tsugane K (1975) Appl
ica-

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 40/213
32
2. Instrumenta tion and Positioning
lion of
nasopharyngeal mirror
for aneurysm op
eration . Technical note. J Neurosurg 43: 244-
246
50. Sugita K, Kobayashi
S,
Shintani A el
al
(1979)
fl. licroneurosurgery for aneurysms o f tile basilar
artery.] Ncurosurg 51: 61
5-6
20
51.
Sugita K, Kobayashi
S.
TakemaeT et al
(
19
80)
Di
rect retraction method in aneurysm surger
y.
J
Neurosurg 53:
41
7
-419
52. Sugita K. Tsugane R (1974) Bipolar coagul
ator
with
automatic
thcrmocomrol. Technical note.
J
Neurosurg 41:
777
- 779
53. Sugita K, Tsuganc R,
Kagcyam3
N (1975) Bipo
lar coagulator
wit
h automatic thcnnocontrol
and some impro\'cmciltsofmicrosurgicai insl
"
u-
melliS, in Handa
H (cd):
Microneurosurgery.
Balti
more, University Park Pre
ss,
p 17
54. Wilson CB, Spetzler RE (1979) Operative ap
proaches to aneurysms. Clin
Ne
urosurg
26:232 - 247
55.
a ~ a r g i l Me (
19
69) MicrosUlgery
Applied
to
NeuroSllrgery. StUttgart, G Thieme, pp 119 - 143
56. a ~ a r g i MG. FoxJL, Ray MW (1975)
Th
e opera
tive approach
to
aneurysms
oflhe
anteriorcolll
municat in g artery, in
Kr
ayenbiihl H (cd): Ad
Milas
and Technical
Stlllu/mtis
in
Neurosurgery,
vol
2.
New York, Springer-Verlag, pp 113- 170
57. Y 1 ~ a r g i l MG , Vise WM, Bader DCH (1977) Tech
nical adjuncts
in
neurosurgery_ Surg Neurol
8:33 1-336

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 41/213
3
Photographic Technique
I
ntrodu
ction
The col
or
illustrations of live microsurgical
anatomy as shown in th is atlas were repro
du
ce d from photograp hic color sl
id
es .
Th
e
photogra phs were taken du ring actual opera
tive proced
ur
es performed
by
the au th
or
since
1975.
Th
ey
re pr
escnL
vis
ual r
eco
rds of selected
su
rg
ical cases treated at the
West
Virginia Uni
ve rsity Medical Center in
I'v
lorgant
ow
n, West
Vi
rgini a; the
Ki
ng Faisal Specialist Hospi tal
and Research Centre in Ri
ya
dh , Saud i Ara
bi
a;
and the Georgetown Unive rsity Med
ica
l
Cen
ter
in
Was
hington, D
.C.
T he maj
or
ity
of
these cases we re pal
ie
nt5 with illlracra
ni
al
aneurysms,
bu
t th e e mphas is here
is
o n live
ana tomy such as may be seen in the p
te r
ional
approach to many oth
er lypeS of
ne urosurgical
pr
oblem
s.
Photograph ic slides
we
re selected
for demonstration on the basis of illustrating
clarity of fea
tu r
es, h
av
ing absence of si
gn
ifi
cant t
iss
ue distortion by tumor o r hemorr hage,
showing normal anato
mi
c va riations, an d/or
portraying special neuroana lOmi cal points.
From a recent
hi
storical stand poin t, the au
thor learned the ph
otogra
phic technique de
scribed herei n from trial-and-error expe ri
ence and from lec
tur
es give n by Leo
nar
d
Ma
l
is,
Chairman of the Depar tment of
Neur
osurgery,
Mo
unt
Si
nai
Sc
hool of
Medici ne, New York City. Earl y in hi s experi
ence the author VLF)
was
und
er
the miscon
ception that increased lightin
g,
a wi
de
opening
of the ca mera d ia ph ragm (s ma ll I-s top
num
ber
),
and sho rt time exposur es were neces
sary lO gain sufficient exposure of the
im
age
on the film in the presence of movement of
ne
ur
al and vascul
ar
intracranial tiss ues re
fl
ected
by
cardiac pulsa
ti
ons (direc
tl
y on the
bl
ood vessels)
and
r
es
pi
ra
tor
y pulsations (indi
rec
tl
y via the venous circulation). Ma ny surgi
cal
photog
ra phers still photogr
ap
h through
the operating mi croscope with these concepts
in mi nd. However, in many instances, ph
olO
graphs taken with such techniques have lacked
shar
pn
ess of image. appeared somewhat flat,
and fa iled to provide a good de pth of field.
The key lO improving the quality of the color
photograph
s is to na
rr
ow the lens apera
tu r
e
(we use an f -
St
Op o f 44). T his results in a signif
icant improvement in clarity and sharpness of
images
and
in dep th
of
focus (re
du
cing the
fl
at
ness of image eff
ect). To accomplish this one
must increase the br ightness of the
li
ghtsour
ce
and/or increase the du ration of film exposure.
The light intensity can be increased to so me ex
tent by ove rloading (increasing the voltage) the
transformer of the 30- or 50-W tungsten bulb.
Stronge r halogen o r xenon li
ght s
ou
tcescan
be
used. Bu t excess light energy, even wi th the use
of fi berop tic
dr
ies out intracran ial tis
sues rapidly and reasonab le limits are finite.
One can, however, extend the film exp
os
ure
time la, for exa
mp
le. 1 seco
nd
. Because a
rt
e
rial systolic pulsations are qu ite br ief com
pared wi th the entire dura
ti
on of one pulse.
th is m
ovi
ng (blu
rr
ed ) image is not detected by
thc hu man eye observing the resulting photo..
graph . In otherwords, th is systolic movemem
(o
r " noise") is ave raged out by the stable image
of
re lat ively much longe r dura
ti
on [4].
Th
e sur
gical photograp her mu Sl ta ke care to avoid any
respir
at
ory- i
ndu
ced movement by as king the
anesth
es
iologist
to
hold the pat
ic
m
's
respira
tions du ring the du rat ion
of
fi lming if possible.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 42/213
34
3. Photographic Tcch
ni<Jue
In
the author
's
early years
of fi
lming with
narrow lens aperature and I-second exposure
limes, excellent col
or
slides were obtain
ed
with
any sim pl e camera bacK (film hol
de
r) and with
30-\V incandescent lighting (givi ng a 2,800° to
3,
100
° K color te
mp
erat
ur
e). Recen t and
mo
re
sophisticated cameras, optics, and microscope
lighting systems have not improved the quality
of the phoLOgraphs, and in many situations the
quality
deteriorated.
Th
e co nversion of
some
Ze iss
mi
croscopes to the usc
of
halogen,
tungsten-filament lam ps (giving a 3,200° to
3,400° K color temperalUre) has improved the
light intensity without noticeable deg radation
in the photographic image
on
tun gsten (ASA
or ISO No.
160)
Kodak Ektachrome film (ba
lanced for color temperatures of 3,200° K [4,
5]). We have been sa tisfi ed with th is light.
More recently
we
temporarily sw itched to
the use of the much brighter xenon light
so
ur
ce (shown on microscope in Fig. 2.5). How
ever, its color temperature is around 6,000° K.
ils e
miued
liglll energy is stronger in the blue
green spect
rum
(com
par
ed wi th light from
tungslen-filamentlamps), and hence one
mu
st
use day light color slide film (Kodak
's
Ekta
chrome fi lm, ISO No. 200, is ba lanced at a
color
tempera
ture of 5,500° K). U
nfortu
nately, the heat-absorbing (red-absorbin
g)
path ways of the microscope's optical system
further
reduced the red speClrum in the
li
ght,
and the r
es
ulting photograph (even with da
y
light film) port rayed defective col
or
reproduc
tion. White
or
gray tissues had a yellow-green
cast and red blood vessels had a brownish cast
(due to the red and green color mi xture). Al
though proper filters may improve the color,
the liglllioss may resultin no signi ficant netim
pro
vem
em
in brightness with the xenon light
source compared
wi
th the tungsten-halogen
light so
ur
ce. Accordingly, we have r
et
urned to
the tungsten-halogen la
mp
on the Zeiss-Con
lI
'aves op
erat
ing microscope.
Current Techniques
Except for the Zeiss cam
era
adap ter and 2x
mag nification attac
hm
ent, the optics is that
which is contained within the Zeiss operating
microscope system [3]. The still ca mera (cam
era
back to hold and move the film; Fig. 3 .1 )
can be any good-quality model and is attached
to the right or left side of the beam splitter (we
use the right; the
TV
camera is on the left; see
Fi
g.
2.7). We have tried using special adapters
a
ll
ow in g the TV camera and still camera to be
attach
ed
to the same side of the microscope's
beam spl ineI' (pe rmitting an observer's tube to
be attached
LO
t
he
o
ther
side),
but the
ca
m
era
lens a
per
ature had to be widened (sma ller [
stop number) with a res ulting degradation of
the photographic image.
As reported previously [I, 2], the following
we
re utilized by the author. For
photograp
h y,
we
used a
Ze
i
ss
OPM I- I oper ating microscope
equipped wi th a 275-mm objective lens, a 160 -
mm focal-length binocular tube , 12.5X
eyepieces, a 30-70 beam spli tter (70% of the
light is deflected and divided equa
ll
y between
the film on the righ t and the camera on the left;
30% goes to the s
ur
geon's eyes), a Zeiss camera
adapter
and 2x magnification auachment, a
Contax camera body, and ISO (f
orme
rl y called
ASA)
No.
160 (tungsten) Ektachrome 35-mm
fi l
m.
The tun gsten-halogen light so urce was
used without auxiliary lighting but with the
transformer
co
nstantly on "overload "
th roughout the operation. (If the heat is al
lowed to escape
direct
ly into the room, the light
bulb usua
ll
y la sts
throughout
several opera
tions.) Before 1980 no drapes we re used, but
the microscope, camera, film, and T V system
were cold-gas-sterili
ze
d for 12 to 18 hours wit h
pure
ethyl
ene
oxide gas. (New federal regul
a
tions have now restricted this m
et
hod of sterili
zation.) Any black-paint border aro
und
the
glass prism deflecting the light
thr
ough the ob
jective lens was removed. Overhead lights in
the
operating
room were turned o
ffLO
provide
beller contrast and LO facilitate dilation of the
surgeon's pupils.
Photographs \·
..
ere made
wit
h respirations
temporarily stopped or during the expiratory
phase of the automatic respirator and wi th the
[ s top on the Zeiss photoadapter set at44 . With
nonautom
at
ic cameras,
the
expo
sure
time
was
set
at
I second. Wi th automatic cameras the ex
posure time ap proxi mates t
hi
s duration. We
use the del
aye
d sh utter-release mode so that a
ll
camera
an
d microscope movements have
ceased by exposure
ti
me occurring about
12 seco
nd
s after pressing the exposure button.
Self-retaining retractors and while cottonoids
we re positioned to provide light reflcClions
within the wo
und
while avoiding re fl ections to
wa
rd
the microscope. Unl ess otherwise indi
cated, the photographs presented we re made

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 43/213
Currenl Techniques
35
Fig. 3. 1. Contax camera at
tached 10 microscope beam
splitter via ad
apter
(not
seen) alld 2x magnification
attachment
(arrow).
with the
Ze
iss magn ification dial se t at its third
magnification
se
lling (the old
No.
16 01' the
new No. 1). providing a true 6x magni fication
for the surgeon. Although lhe photographs
lhemsel
ves
do not provide stereoscopic vision
and sufficient depth
of fi
eld, which may be
6 em from the sku
ll
surface, the reader's know
ledge
of
analom),
wi
ll
compensate for this.
Bib
li
ography
L Fox J L
(1979)
r.,I ic rosurgical exposure
of
i
mr
a
crani
al
aTleurysms .
1
Microsurg
I: 2-
31
2. Fox J L (1983)
llitracranial
Al1
e
Ul
ysms.
New York,
Springer-Verlag,
vol 2
3.
Hoerenz
P
(1980- 1981) The operating micro
scope, J Microsurg I:
364- 369,
419-427;
2: 22 - 26 ,
126
- 139;3:
179
- 182
4.
Ma lis LI
(1981)
Neurosurgical photography
through the mic roscope. Clin Neurosurg
28: 233- 245
5. MartIn-Rodriguez JG (1985) Colol' still and mo
tion pholOgraphy and color tcle\·
is
ioll recording
through the
operating
microscope, in Rand
RW
(00):
Mi
crQrlclI.rosllrgery. SI
Louis,
CV
Mosby Co.
ed 3, pp
83-9)

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 44/213
4
Cranial Anatomy and
the Cranial
Flap
Anatomy
The
pterion
ha
s
been
defined
in
Chapter
I.
Figure 4. 1 illustrates
that
the pterion
is not
a
speci
fic
point
but rather
a
genera
l region
of
the
skull lying under the tcmporalis muscle and in
do
se prox im ity to the frontal, parietal, tem
poral,
and
sphenoid bones.
The
frontoparietal
(coronal) suture and the sphenoidotemporal
suture do not meet at a common point but in
stead come
to
a T' intersection
(Fig.
4.1) with
the parietotemporal, parietosphenoidal. and
frontosphcnoida l sutures (the latt
er
two form
ing a relatively straight posterior-ta-anteri
or
extension
of
the parietotemporal sut
ur
e).
This
anatomical arrangement allows a sh
ort
com
mon boundary between the parietal and
sphenoid bones and causes a separation
be
tween the frontal and temporal bones.
Fig.
4.1_
View of left side of skull model .
TI le sutu re lines between JX)rtions
of
the
sk ull arc outlined in ink. F, frontal;
P
parietal;
T, tempora
l; S, sphenoidal; and
Z,
zygo mat ic bones.
Figure 4.2 shows the anatomical arra nge
ment
of
these bones at the inner base
of
the
skull
[I].
Although
not
prominent on
the out
side, the sphenoid bone represents the "key
slOne" of cranial-base analOmy.
The
word
sphenoid
is
derived from the Greek word
sphenoeides,
meaning wedge-like
[6].
From its
body this interesting struclllre
(F
i
g. 4.3)
sends
out
lalerallesser
and
greater wings, appearing
rather
like a butterfly in flight [2]. For the sur
geon operating at the base of the skull and
brain, this hidden keystone contains land
marks
of
orientation
as well
as structures that
may have to be removed by rongeurs and high
speed drills.
The
latt
er
structures include the
sphenoid wings, anterior clinoid process, pos
terior clinoid process,
roof of op t
ic canal,
tuberculum sellae, floor and septum
of
the
sphenoid sin us, and floor of the se lla turcica.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 45/213
38
Iw
gw
"
"
o
d.
Fig.
4.
2. Base of skull, upper surface. Note that
Ihe anlerior clinoid process is a posterior pro
jection of
the
origin of
the
lesser wing of
the
sphenoid oone.
Components
of the sphenoid
wi
ng include
lu,
lesser wing;
gu'.
greater
wi
ng;
ls, tuberculum sellae;
ae,
alilcrior cli noid pro
cess;
s
, sella lUrcica; pc. posterior clinoid pro
ccss;fo, foramen ovate; ds, dors u m sellae. Re
drawn from Clemente CD (ed)
(198S)Al alomyoj
tht H/lInol Body by Hem)' Gmy, 30th American
ed. Philadelph ia, Lea &
l< eb
igcr, p
17
1 [ IJ.
"
Fi
g. 4. 3.
Vicw
of disaniculatcd sp henoid bone of
sku ll as seen from behind. The
dorsum
se llae hides
the sella turcica (pituitary fOS5<1) seen best from
aoc·vcin Fig. 4.2. Note the relationship of the
greater
and lesser wings
separated by
thcsupcriororbi
l.al
fis·
surc. A
n o
pt ic
strut separates the
supe
ri
or o,'hital fis·
su
re
from the op tic canal. From E
tter
L E (1955) Atlas
of
Roentgen AI/atomy
of
the Skull.
Sp
ri
ngfield, 1L ,
Charles CThomas Publisher. p 17 [2).
V

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 46/213
The Cranial
Fl
ap
39
By whatever approach to basal struct
ur
es, the
surgeon must ha
ve
intimate know ledge
of
the
sphenoid bone.
Th
e basal cran ial anatomy takes on a differ
ent perspec tive when viewed in the surgica l up
s
ide-
d
ow
n, oblique position (see
Figs.
2.3 and
4.8).
Fi
gures 4.4
an
d 4.5 illustrate a skull model
with a sma
ll
pterional cranial opening. T hesc
show the value
of
remov ing much of the
sphenoid wi ng (ie, lesser and grea ter win
gs)
[3,
4]. Before the sphenoid w
in
g is remo
ve
d , the
s
urg
eon
's
view
of
the supras
ell
ar region is
blocked by the latcral projcClio n
of
the win g
unless greater and haza rdous brain retraction
is appl
ie
d. Partial removal
of
thc sphcnoid
wing, practiced for years
by
Walter Dand y's dis
ciples, pcrmits a
low
cr, basal, tangential a p
proach
to
the circle of W
illi s.
Once the s
ur
geon
u
ses
this tcchniquc rOUl
in
ely and then omits it
from an operative case, he will appreciate its
significant value for permitting easier visuali
zation of basal cistern s. This technique,
coupled with the s
kill
ed u
sc of
sel f-ret.'lining
retractors and
of
the operat
in
g microscope on
a relaxed bra
in
, a
ll
ows thc sur geon to manipu
late microinstruments in small but sa tisfactor
il
y visuali
ze
d spaces.
I f
we
take the same
dry
sku
ll
model shown
in
Figs. 4.4 and 4.5, one can see the relat ionship
of the ba silar artery to the anterior and pos
terior
cl
inoid processes as visua
li
zed throug h a
pterional exposu re (
Fi
gs. 4.6 and 4.7).
One
ca n
understand from
Fi
g. 4.7 that removal
of
much
of
thc sphcnoid win g on one side and a
widely opened sy lv
ia
n
fi
ssure on the othcr side
arc necessary to approac h the midbrain, pons,
and inlerpeduncul
ar
cislern wilh
mi
ni mal
brain retraction. T he posterior clinoid process
of
the sphenoid bone then becomes a critica l
landmark, lying medial to the oculomotor
nerve passing for
wa
rd from the midbrain.
The Cranial Flap
All surgical photogra phs in th
is
atlas arc show n
as a right-sided pterional craniotomy. Those
th
at
originally
we
re left-sided h
ave
been re
ve
rsed to per mit consistency in anatomical il
lu
strat ion. Muc h
of
the following in this chap
ter
is
modified from a previous publication
of
the auth
or [4
].
For a right frontolatcral cra niotomy, the
head is held
in
a skull-
fi
xa tion ap
paratus (see Fig.2.3) and lUrned approxi
mately 30
0
t045° to the left, tilted 15
0
to the left ,
and dropped back about 15
0
(Fig. 4.8). This
brings the "p
syc
hopat
hic point" (see Chap
te r I) into the center and to thc highest point
of
the opcrat ive field .
(W
hen a rig
ht
-handed
surgeon operates on the left side
of
the head , a
40
0
to 45
0
rotation to the riglH is used.) For
aneurysms
of
the middle cerebral artery or the
internal carotid artery bifurcation, the head
is dropped back further so that thc surgeon's
line of vision
is
as perpendicular as poss ible
to the M-I portion
of
the middle cerebral ar
tcry.
T he skin incisio n is kept behind the hairline
rather than curvi ng for wa rd into the exposed
forchead.
Thi
s requi res a long incision, but the
cosmetic resul t
is
better
after
the hair grows
back. T he incision (Fig. 4.8) be gins at the mid
line. curves laterally be
hi
nd the hairline, and
terminates
one
fingerbreadth
in
front
of
the
ear at the level of (or s
li
ghtl), below) the
zygomatic arch. T he skin flap and galea are
stripped from the temporal is fasc ia and
teum, covered with oxycellulose gau
ze
(co lton
may get ca ught in the hi gh- speed drills), and
pu
ll
ed fo rward with
fi
shhook retractors.
An incisio n
is
made in the anterior and pos
tcrior
lim
il of the expo
se
d lemporalis muscle.
T he ante rior portion of the temporalis muscle
is
stripped posterioriy from the zygomat ic pro
cess
of
the frontal
OOne
. Herc one may have to
clectrocoagulate
one or
two branches
of
the an
terior deep temporal artery (from the imcrnal
maxillary arter y). Also. tiny art.eries perforat
in
g the frontal bone just behind its zygomatic
process may have to be coagulated (w ilh cut
tin g current) and
/or
sealed with bonewax.
Th
e
periosteum is stripped along the line
of
inci
sion from the exposed frontal, parietal, and
lemporal bon
es.
Howe,'e
r,
a triangle
of
perios
leum (Fig. 4.9) is preserved anteriorly for later
suturing
to
the te mporalis fascia, thereby cov
er in g the anterior frontal burr ho le at the end
of
the opera tion. This piccc of periosteum,
with its base
anter
iorly,
is
laid on the galea
of
the skin flap, covered with oxycellulose, and
held
by
a fi shh
oo
k retractor.
The frontotemporal bone
fl
ap itself
is
simi
l
ar
to th
at
illustrated
by
Ludwig Kempe (sec
Fig.
\.5) with the
fo llow in
g modifications
(Fig. 4.10),

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 47/213
40
4. Cranial Anatomy and the Cran
ial
Flap
I.
The first burr hole is
ju
st behind the
"psychopathic
point"
and its anterior ed
ge
touches
on
that point.
2. The
second burr hole is also
in
the frontal
bone. This hole lies mo re medial than that
il
lustrated
by
K
empe
(see
Fi
g.
1.
5).
Th
ere
are
three advantages to this:
(a)
It a ll
ows
more
room for frontal lobe retraction without the
retractor striking the fron tal bone. (b) It per
mils plenty
of
room f
or
maintenance oftem
poralis mu
sc
le attachment to the
frontOlcm
perosphenoparietal bone flap, thereby re
ducin g the incidence
of
later temporalis
muscle atrophy. (c) T here is enough ex
posed bone flap for placement of flap-edge
holes for suturclrubber band retraction of
the bone flap.
3. The
third
burr
hole
is
placed
in
the parietal
bone just inferi
or
to the temporal line.
4. The fourth burr hole is dr i lled in the tem
poral
bone
ju
st
in
front
of
the ear a nd above
the zygomatic arch. If placed too far back,
temporal bone air cells may be encountered.
The bone dust
is
saved an d used to fill the
burr holes
after
clos
ur
e
of
the bone flap,
thereby helping to preve
n1.
any future inde n
tations of the scalp into the burr holes.
In patients yo unger than 55 yea rs, the
dur
a
is not usually tightly adherent to the skull bone.
In these cases we often uti
li
ze the ai r-driven
craniotome to cut the sk ull
fl
ap in a similar de
sign between two holes: only the most anterio r
and the most inferoposterior
bur
r holes.
Otherwise a Gigli
saw
is used to
cut
the skull
bone between the four burr holes. Prior
to
either of these techniques
of
craniotom
y,
rongeurs are used
(we
usually u
se
the Echlin
rongeur)
to
bite away as much of a channel
in
the fronto-spheno-temporal bone as possible
between the two basal burr holes under the
te
mp
oralis muscle. Doing this before saw ing
the bone between the
upp
er calvarial
burr
holes a
ll
ows this inferior bony channel
to
be
cut
without the bone flap inadvertently fracturing
too hi gh above the base.
After the bone
fl
ap
is
cut free, its inferior
edge is rongeured (Leksell rongeur) until
it
pr
esents a smooth, n
onpr
ojecting s
urf
ace.
Heavy si lk sutures are passed t
hr
ough two of
the small edge holes (already drilled f
or
future
reattachment
of
the bone flap to the cal
varium).
The
sutures are each connected to a
rubber band that has been wrapped around
the rubber tubing show n previously in
Figs. 2.7 A and 2.9. In this manner, the bone
fl
ap, still attached to the temporalis muscle,
is
re tracted over the zygomatic arch, thereby ex
posin g the dura
(Fig.
4.11). The bone flap is
waxed
at
i
ts
edges and then covered with wet
oxycellulose. T he calvarial edges are also
waxed .
The dura
is the n tacked up with sutures
that are passed through the calvarial edge
holes (also
to
be used for reattachment
of
the
bone
fl
ap. T he sph enoid wing is rongeured in
fe
ri
orly as far as possi ble and then waxed. In
cases where an even more basal expos ure is re
quired, we cut the zygomatic arch anteriorly
and posteriorl
y.
I t can be left attached to soft
tissues while the b
ul
k of the temporalis muscle
is displaced inferiorl
y. The
zygoma is reat
tached at the end
of
the surgery.
The superficial temporal a
rt
ery runs in
front
of
the
ear
and just su perficial to the
galea. Preservation
of
this artery
is
useful,
especia
ll
y if the su rgeon plans an
ext
racrania
l
to- intracranial anastomosis. This may
be
neces
sary if one plans on a trapping proce
dure
or an
arterial occlusion. In such a circumstance,
meticulous techniqu e is needed to prevent su
perficial temporal artery injury.
The frontalis branches
of
the facial nerve
pass forward between the galea and lemporalis
fascia and are usually seen passin g anteroin
fe
rior to the first burr hole. They can some
tim
es
be preserved
by
turning a s
up
erfical
layer
of
the
tempora
l s fascia forward over the
zygomatic
pr
ocess
of
the front
al
bone before
incising the tcmporalis musc le anteriorly. Elec
trocoagulation in the area must be kept at a
minimum. T he ne
rves are
ofte
n
injured, and
the patient m
ay
have an immobile forehead
on
the ipsilateral side foll owing surgery. In most
such cases, frontalis muscle function returns
wi thin 6 month s.
Sphenoid Wing Removal
The
operating microscope is n
ow brought
into
the s
ur
gica l field and used until dural closure.
The Ley la se lf-retaining retractors
are
at
tached to the
operating
table (see fig. 2.1
1).
The dura of
the frontal and temporal lobes are
retracted gently from the sphenoid bone and
the lateral roof
of
the orbit. If necessary, some
cerebrospinal fluid (CSF) ca n be drain ed
by

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 48/213
Sp
henoid
Wing
Removal
41
lumbar puncture to relieve pre
ss
ure on the
bra in. Release only a suffici
ent amount of CS
F
to permit a relaxed brain, as excess removal
risks premaLUre rupture
of
an ane
ur
ysm, tear
in
g
of vc in
s bridging th e
dura
and the brain,
or
downward hern iation
in
cases with ma
ss
le
sions.
The dur
a of the temporal lobe is often
quite
vasc ul
ar and w
ill
require bipolar ele
c
trocoagulation, oxycellulose application,
an
d
occasionally the u
se of
malleable dips.
With a suction-irrigat
io
n apparatus
in
the
left hand and a high-speed drill in the
ri
ght
hand (of a right-handed surgeon), the surgeon
removes
projections
of
the sphenoid w
in
g and
lateral
or
bital roof.
Ke
ep all couono
id
s o
ut of
the immediate field to avoi d
in
ju ry
by
their
being caught in the drill.
The
steel drill bit is
used in i
ti
ally because ofiLS more rapid removal
of
bone.
As
the base
of
the
anteriordinoid pro
ce
ss
is approached, the drill bit is changed to
the d
ia
mond type, which tends less to tear the
n
ear
by dura.
Th
e Lemp
ert
rongeur is ve
ry
helpful in removin g slive r-like projections
of
the sphenoid wing. A tiny
bi
t
of
bonewax on a
small , dry couonoid is applied aga
in
st the bone
with the bipolar forceps to stop bone bleeding.
One mllst be careful to avoid drilling into the
orbital cavit
y.
I f this occurs, the p
at
ient
will
have greater temporary swe lling and ec
chymosis of orbital ti
ss
ues during the pos
t
operative period. In some pati
ellLS
there
is
a
partial, congenital absence
of
the greater wing
of the sph
eno
id bone behind the o
rbi t.
The
sphenoid w
in
g is removed with a
rongeur and then burred down with the hi gh
speed drill
dose
to the base
of
the anterior
clinoid process, a medial depth
of
about 5 cm
(Figs.
4.12
an
d 4 .13).
As one ap
proaches this
point, the men in go-orbital artery (su praorbital
branch
of
middle men in geal arter y) is a land
mark seen in the dura;
it
passes from the mid
dl
e meningeal a
rt
ery through
it
s own "lacri
mal" foramen (Hyrtl
's
canal)
in
the sphen
oi
d
wing
or
through the lateral corner of the
superior orbital fissure to communicate with
the lacrimal artcry in the orbit. (This artery is
on
e
of
the remnanLS
of
the embryo nic stapedial
arterial system
[5]). The
meningo-orbital ar
tery usually is electrocoagulated and severed,
allowing further drilling ofthe sphenoid win g.
At
this point the fast
er
steel drill bit is swi tched
fo r a diamond bit.
Th
e base
of
the amerior
cl
in
oid process appears as a glistening while
bone o ften contain
in
g a single sma
ll vasc
ular
channel (Fig. 4.13).
Th
e dural opening
is
cons
id
erabl y smaller
than the craniotomy defect. The bony open ing
is
la
rger for the reasons stated earlier in this
chapter.
The
dura is permitted to cover the
brai n as much as po
ss
ible to
pr
otect the brai n
from the drying effecLS
of
air and light. The
du ra is opened in a modified, sha
ll
ow horse
shoe-shaped man ner (Fig.
4.
1
4). The dural
nap is retracted o
ve
r the smoothed-out
sphenoid bone
by
suturing it to the galea.
Often a secondary
dur
al incision over the syl
vian fissure is needed if the
fi
ssure is to be
opened widely. At this point, some CS F can be
remo
ve
d by
lumbar
dr
ai
nage
or
by
aspiration
from the chiasmatic and
ad
jacent cisterns
under a minima
ll
y elevated frontal lobe
(Figs.
4.14
and 4.15). Auention must be paid to
the one or more ve ins bridg ing the temporal
lobe and the sphenoparietal sin us. Although it
is good practice to preserve ve nous drainage
where possible, we have not seen any complica
tions from electrocoagulating and severin g
these
vei
n
s.
I n cases where minimal temporal
lobe retraction is necessary, these veins may be
preserved.
The
fo llowing chapter details the
anatomy of the
sy
lvian
fi
ssure
in
the approach
to
the basa l cisterns.
Bibliography
I. Clemente C D (ed) ( 1985) Anatomy
of
Ille Human
Body
by
Henry
Gmy,
30th
American e
d.
Philadel
phia, Lea & Febigcr, p
171
2. Etter Lf. ( 1955) A/las of Roentgen Anatomy of lhe
Skull.
Springfield, 1L, Charles C Thomas Pu
b
lisher,
pp 16-44
3.
FoxJL
(1979) Mi
crosurgical exposure of intracra
nia
l aneurysms.J
Microsurg
I : 2-31
4. Fox
JL (1983)
Intracranial Aneurysms,
vol 2. New
York, Springer-Ver lag, pp 877-887, 1030
5.
Lie
TA (1983) Variat
ions in cerebrovascular
anatomy, in Fox J1. (ed): Intracranial Aneurysms,
\'01 I. New
Yo
rk, Springer-Verlag, pp 432-489
6. Sin/man's Medical DicliOl l1ry, ed 24. (1982) Balti
more
,
William
s
& Wilkins Co,
p
1312

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 49/213
42
4. Cranial Anatomy and the Cranial Flap
Fig. 4.4. View of dry skull in
the
same surgical pos
i
tion as in figs. 2.3 and 4.8 prior to removal of the
sp heno id \ ~ i l \ g
Th
e right orbit is at the upper left
corner. spit, L1.leral aspect of greater sphenoid
wi
ng;
pel,
pClrous pyramid;
ac,
anterior clino
id pr
oces;
pc,
tip of ]X>sterior clinoid process; crossed an-ow, ex
posed lOp of red rubber eraser
("lUm or
or
",
j l lcurysm").

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 50/213
Analomy 43
""'It
Fig. 4.5. Same dry skull as in Fig. 4.4. Th e sphenoid
w
in
g
(sPh)
h
as
been drilled away.
Crossed arraw:
red
r
ubbe
r eraser
("
tumor" or "aneurysm")
si
tting on
lhe tuberculum se llae nanked by both ame ri
or
clino id processes. ac, Rig
ht
am
er
ior clinoid
pr
ocess;
pel, ri ght petrous pyra mid ;,,£;, righl post
er
ior clino id
process. From
Fo
x [3].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 51/213
44
4. Cranial Anatomy and the Cranial Flap
Fig. 4.6. Same dr y skull as in '-igs. 4.4 and 4.5. Skull
is in upright, oblique position with view over lateral
roof of orbi
l.
zy. Frontal processofzygoma;pet. right
petrous pyramid;
ac,
anterior clinoid processes
flank ing tubercu lum
se
llae
(ts);
PC. right posteriur
clinoid process;
00,
red pen representing basilar ar
ter
y.
(Be hind the latter would be the midbrain and
pons.)

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 52/213
AnalOmy
45
Fig.
4.7.
Same dry skull as in Figs.
4.4-4.6.
Sku ll
now is in
surgical upside-down, oblique position.
Thesurgeon's view is more caudal to view the region
of
the "basilar artery" (00, a red pen) as seen via the
pterional approach.
Th
e
orbit
is in th e
upper
left
corner of the figure. pc, Right posterior clinoid pro
cess;
pel,
petrous pyramid; *, right anteri
or
clinoid
process: sph, drilled down sphenoid wing. From Fox
[3).

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 53/213
46
4. Cranial Anatomy and the Cranial Flap
Fi g. 4.8. Pa tient's head in a skull clamp. The incision (triallgle) iso udin cd to stay behind the hairline. ret allows
the bone
nap
to remain
auac
hed to
the
temporalis mu
sc
le. From
I-ox
[3).

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 54/213
Th
e Cranial Flap
47
Fig. 4.9. Scalp
nap
turned for right pte
ri
onal
craniotomy. Paticnt in position show n in Fig. 4.8.
G a ~ a
exposed. Crosstd
01'7'01/,\ junct
ion of tcmpo
dl
line wit h orbital ridge and zygomatic proce
ss of
f ron-
tal bo ne; fb. frontal bone;
If,
tClllporalis fasc ia; pt.
perios te
um
;
re,
raney clips on scal p edgc;
s,
suction
tube:
If,
thumb forceps
el
evat
in
g triangul
ar
patch
of
periosteum offfrontal bo ne Vb).

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 55/213
48
4. Cranial Anatomy and the Cranial Flap
Fig. 4.10. The oxycellulosc
(ox)
covered galea and
scalp flap
arc
held
by
fishhook
retraCLOrs (fit).
A re
tractor
(ret)
is pulling the incised lcmporalis muscle
forward. One parietal (P). one temporal (I), and lWO
frontal if)
burr
holes have been drilled and covered
with bonewax. fe, Periosteum; el, elevator; if, tern
poral
is
fascia.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 56/213
The
Cranial Flap
49
Fig
.
4.11.
The
bone flap
(bj),
covered byoxyce
ll
ulose
(ox), has becn turned latera lly o\·er the zygomatic
arch. It rcmains attached to the temporalis muscle
(t1ll). lph,
Sphenoid
....
,ing;td. temporal
dura;fd.
fron
tal dura : su, suture for later reattachment of the
bone flap.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 57/213
;0
4. Cranial AnatOmy and the Cranial Flap
I
,
/CO
Id
.1
Fig. 4.12
. The sp
henoid
wi
ng
(sph)
prior to removal.
hII,
Amcrior frontal
burr holc;fd,
fron tal dur<t;sf,
dura
over sy lvian fissure; It , temporal
dura.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 58/213
Sp henoid Wing Removal
51
Fig. 4.13.
The
right sphenoid wing (spl ) h
as
been
burred
away.
Crossed
arrow, vascul ar channel ill lesser
wing
of
sp henoid wing near base of ante rior clinoid
process; mo, mcningo-or
bi
tal artery.
On
righ t is a re-
tractor on the dura of the tempo ral lobc (/d). On le ft
is a suction tube
(5)
and retractor (ret) 0 11 the dura of
the right frOlllallobe ifd). Ze iss dial
SCl
at magnifica
tion
Hu
mber 0.6 (old no. 10). From Fox [3].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 59/213
52
4. Cranial Anatomy and the Cranial Flap
Fig.
4.14. Initial
exposure
of
carotid cistern.
Ma
gnifi
ca
ti
on reduced. Re
tractor
s (rtt) elc\'ating the right
Icmporallobe (about') and frontal lobe
(below)
I em
frO Il1 right spheno id wing
co\
'c red by the turned-
down dural flap
(dura), The sy
lvian fi
ss
ure
(sf)
is not
ye t opened. 2, Optic nerve; ica, imernal carotid af
tcry. Zeiss magnifica tion dial set at number 0.4 (old
no
.
6).
From Fox [3].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 60/213
Sphenoid Wing Removal 53
Fig.
4.15. View
along spheno
id
wing to the right an
teriorclinoid process
(*). ti.
"I"emporal lobc;j1, fronlai
lobe. The internal carotid artery (ica) and optic
nerve
(2)
are covered by arachnoid. J, Right olfac
tory tract;
s.
suction lube.
Zeiss
dial set at
0.6
(old
no. 10 ). From Fox (3).

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 61/213
5
The Sylvian Fissure
Introduction
E
ve
n though the pterional approach to skull
ba
se
le
sions has become more
w
id
ely
used
by
neurosurgcons, significam separation of the
frontal and tcmporal lobes
by
opcning the
sy
l
vian fissure is often not
done
. However, as
we
have gained morc experience.
we
hav e opened
the
sy
lvian fissure more and morc. This has
several benefits [3, 5): (a) small vessels arc not
compressed
by
arachnoid al bands
durin
g re
traction of the brain; (b) there is le ss resistance
(and hence less bra in-ret ractor pressure) to re
traction
of
the fronta l lobe;
(c)
traction
011
onc
lobe does not pull and
injure Lh
e other lobe;
(d) fewer bridging
ve in
s need
be
sacrificed;
(e)
the olfactory nerve usually can be preserved;
and
(f)
there is minimal traction on perforatin g
arteries an d on an aneur
ys
m.
Fig.
5.1.
CT
scan
after
injec
ti
on
of
iopamidol into CS F.
Arrow runs from posterior
cerebral artery (at junction of
ambient cistern with inter
pedu ncular cistern) to optic
tract. Arrowhead. middle cere
bral artery in sylvian fissure.
Section is at level
of
midbrain
and optic chi asm. Note an·
tcrior cerebral arteries in
chiasmatic cistern (trianglt)
and interhemispheric fissure.
Fi
gure 5.
1 is a computed tomography (CT )
scan that
ni
cely
ill
ustrates the significant cere
bral
spinal fluid (CSF) space
(sy
lvian cistern)
between noncom pressed frontal
and temp
oral
lobes. Thi s space, containing the midd le cere
bral a
rt
ery and its branches. is quite prominent
in the old
er
01" the atrophied brain. h m
ay
be
minimal in the edematous
or
compressed
brain.
Th
e sy lvi
an
cistern is larger near its basal
zone, as seen
in Fi g.
5.1. and becomes smalle r
in
the more peripheral
zo
ne
s.
At the surface the
sy
lvian fi ssure may appear to be absent (i t is
no
t)
owing
to
the close approximation of the
fromal
pi
a and temporal pia mater. This zone
is covered by fi rmly adhering arachnoid
s
tr
elched over the pia,
and
at
first observation
the
untut
ored observor m
ay be
mislead into
be
l
iev
in g that an
opening
of the
sy
lvian
fissur
e
is
too difficult
to wa rr
ant performing. Indeed.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 62/213
56
5. The Sylvian Fissure
the difficulties encountered with
opening
the
sylvian fissure co
mp
ressed
by sofland
ede
mat
ous
br
ain cont
ai
ning friable,
nonautoregu
lat
ing vessels may make the procedure LOa
haza rdou
s.
But in most circumstances the fis
s
ure
can be widely
opened,
t
hu
s permitting ex
ce llent exposure of basal anatomy between a
drilled-down sp henoid wing and a widely ex
posed sy lvian fissure.
Anatomy
Fig
ure
s 5.2 th rough 5.8 illustrate the initial
opening
of the
sy
lvian
fi
ss
ur
e
in
five cases
(a ll
photographs in this a lias are presented as vi
ew
ing the right side). With initia l elevation of the
frontal
an
d temporal lobes
(Fi
g. 5
.2),
the sur
geon
w
ill see fine arachno id bands passing in
the s
ubdur
al space between
the
arachnoid a
nd
dura
(both being meso
dermal
leptomeningeal
tiss ue of similar embryonic origin). I n some
cases the arachnoid over the sy lvian
fi
ssure is
distended by contained CS F (Fig. 5.3). Th is
often occurs when the brain has been mildly
shrunken as wa ter is transfe rred from the
brain into the
CS
F space owing to controlled
hyperventilation [7].
The sylvian fissure is usually opened on the
frontal lobe side of the sylvian veins (Figs.
5.4-5.8). Initially, we use ajeweler's forceps to
pick
up
the arac
hn
oid (Fig. 5.6), which
is
incis
ed
wi
th microscissors. The self-retaining re
tractor
bl
ades
are
employed
to separa
te the
frontal and tempora l lobes, thus gently s
tr
e tc
h·
ing the arachnoid in the
fi
ssure. This facilitates
ex posure of the next, deeper layer of arach
noid and i
ts
contained peripheral branches of
the middle cerebral a
rt
ery (Fig. 5.7). Close i
n
spection via the operating microscope revea ls
the ever-present, fine
arac
hnoid bands or
fi
bers s
upp
orting the arteries within their bath
of CS F.
This
anatomical
phenomenon,
to be
emphasized
throughout
this atlas, has been
stressed by Arutiunov and colleagues in th eir
drawings
[1]. They related mechanical disto r
tion of these s
up
porting
fi
bers to the evolution
of vasospasm after
ane
urysmal s
ubarac
hnoid
hemorrhage.
We no lon
ger
hesitate to coagu late and incise
veins
and
su perficial
arter
ies passing between
the two lobes. In this manner the surgeon, with
the suction tu be in his left hand and the bipolar
forceps or microscissors in his right hand ,
works his
way
down toward the base of the sy l
vian fissure (
Fi
gs
.
5.8-5.12).
Meticulous
ca
re is
taken
wi
th the small arachnoid a
dh
esions
and
band s adjacent to middle cerebral ar tery
branches d
eeper
in the fissure. When released ,
these band s will not compress and compromise
vessels as the lobes are separa ted, and the sur
geon w
ill
find
the
fissure
sud
denly
ope
ning
up
to
significant advantage. A sma
ll
cotton paddy
or dental cotton ba ll (counted) is helpful for
co
mpr
essing bleed ing vessels with the suction
tube prior to their electrocoag ul ation.
One
finally reaches the mu ch
tougher
arachnoid fibers
at
the base of
the sy
lvi
an
fis
sure
(F
igs. 5.9-5.1 1
).
When these arc cut, the
surgeon gains immedia te entrance into the
carotid cist
ern and
more CS F is re leased. Dur
ing this approach, the surgeon mu st decide
wh
et
her or not to electrocoagu late and cutone
or
more bridging veins between the sylvian
vei ns of the l
emporal
lobe and the dural
sphen
opa
rietal sinus (F igs. 5.1
0 -5 .1
3). Preser
vation of bridging veins generally is a good pol
icy, bUllheir presence may limit adequa te expo
sure in some cases. Also, these veins may lear,
resulting in ve no us bleeding
at
a difficult time
durin
g the operation.
We
rarely, if ever, had a
complication
due
to removal of these particu
l
ar
ve in
s.
Figure 5 .1 3 shows the preliminary
anatomy in
one
patient
after ope
ning the syl
vian fissure.
The following figures illustrate va riatio ns in
s
ur
gical
anato
my
of
the
rig
ht
sy
l
via
n fissure.
Figures 5 .14 and 5.15 are
twO
separate cases
where
on
ly the d istal zone of the
sy
lvian fissure
(simil
ar
to site of jeweler's forceps in
Fig.
5.6)
has been opened. In each case branches of the
middle cerebral artery project
out
and
arachnoid bands are noted. In Fi g. 5.15 the
morc superficial
part
of the sy lvi
an
fissure has
been oblit
era
ted la terally by adh esions (from
prev
ious hemorrhage) between the fronta l and
t
empora
l lobes. Figures 5.16 and 5.17 are illus
trations (at
different
magnifications) of middle
cerebral arterial
br
anches projecting outward
after the lateral portions of the frontal and
temporal lobes in Fig. 5.1 5 have been scpa
rated. Emphasis
is
placed
on
the arachnoid
bands of
Ar
ut
i
un
ov
( I], which
are
clearly re
vealed in these photographs. Of course, nor
ma
ll
y they
are bat
hed in CSF within the sylvian
cistern .
Figure 5 .18 indicates a later state of dissec
tion where the tough arachnoid between the
base of the frontal lobe and the base of the tem
poral lobe is being severed by microscissors
(compare
with Fi
g.
5.
11
).
Figure 5. 19 s
ho
ws
a

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 63/213
Anatomy
57
va
riation in the M-I and M-2 arterial anatomy
after cutting basal arachno
id
fibers.
Fi
g
ure
5.20 is an example
of
a long M-I artery project
ing laterally through an early superfi cial open
ing of the sy lvian fissure. Figure 5.21 illustrates
another long M-I artery taking the m
ore
usual
course deep in the sy lvian fissure. Figures 5.22
and 5.23 are exam ples
of
a long M-l artery and
a short M-l artery, respectively. In both in
stances, the
M-1
artery
is
best seen with the
su
r
geon's view a
im
ed perpendicular to the axis of
the artery, and this is best obtained
by
a greater
than-usual extension
of
the patient's head
when lesions along the M-l artery and internal
ca rotid
anery
bifurcation are treated surg
i
ca
ll y.
As
the
sy
lvia n fissure is opened more widely
at the base, the bifurcation of the internal
ca
rotid artery into
its
M-J
and
A-
I branches
comes into view. A structu re often seen but not
common ly recognized here
is
the optic tract
(Figs. 5.23-5.29) . In this region the optic tract
fo
rm
s the lateral border
of
the lamina ter
minalis and its cistern,
is
crossed
by
the A-I ar
tery, and
li
es d
eep
to perforators passing to the
anterior perforated substance from
A- J,
M-I,
and the carotid bifurcation vasc ulature.
Fig
ures 5.24 and 5.25 are good examples
of
im
portant anatomy seen
at
and just
be
yond the
widely opened sylv ian
fi
ssure. In addition to
that described above. this anatomy includes the
anterior choroidal artery, stria thalamic per
forators. reCUITen t artery
of
Heubncl; and the
anterior temporal artery. Figures 5.
26an
d 5.27
are additional examples wh
ere
the internal
carotid artery is short.
The
multitude
of
stria
thalamic perforators as seen
in Fi
gure 5.28 will
be obscured
by
an aneurysm at the bifurcation
of the internal carotid artery (
Fi
g. 5
.2
9).
In an occasional case, gentle retraction to
separate the fromal an d temporal lobes will
ex
pose middle ce rebral artery branches usually
deeply hidden in the
sylvi
an fissure (Fig. 5.30
).
With microlechnique to open the arachnoid
membrane and to sever the fine arachn
oi
d
bands supportin g the arteries, the a rte ries (dis
tended and pulsating with blood)
may
project
outward toward the surgeo n (Fig. 5.31). Usu
ally a second layer
of
arachnoid membrane is
found covering the lar
ger
M-2 branches and
must be removed to see these branches clearly
(
Fi
g. 5.32). These arteries then can be followed
down to the M-I artery and its perforators
(Fig.
5.33).
It
is thi s author's opinion that the
brain
is
covered by a double layer
of
arachnoid
as if the brain had settled down onto a balloon
made
of
arachnoid membrane.
As
the brain
settled, the opposing arachnoid wa lls ap
proximated, leav ing an inner layer (wrapped
around and supporting the arleries at the base
of
the brain) a
nd
an
outer
layer (covering the
brain and stretched between neu ral protru
sions so as to form CS F-co maining cisterns and
fi
ss
ures). Ju st as fine arachnoid band s and fib
ers run between the dura and the arachnoid
(see Fig. 5.2), similar
ba
nds and fibers (of
Arutiunov) run from the inner arachnoid
la
yer
(surrounding arteries) to other nearby inner or
outer arachnoid layers (see
Fig.
5.17). Often
the inner laye r of arachnoid el1\'elops not only
the conduit arteries but also the perforators
running in the CSF space between the artery
and the brain (the anterior thalamic per
forators from the posterior communica ting
ar'
tery shown in Chapter 8 being the best exam
pl
e). Thus, these perforators appear to be
lined on both sides by a layer
of
inner
arachnoid membrane [4]. This membrane be
comes stretched, perforated, and discontinu
ous with growth of the child.
Figures 5.34 and 5.35 are two illustrations of
a leash
of
stria thalamic perforators passing
from the M-I
ar
tery,
through
the base
of
the
sylvian cistern , over t he optic tract, and into the
amerior perforated substance. Figure 5.36 is
an angiographic example
of
such perforators.
The nex t chapter will ta
ke
the obse rver deeper
into the carotid a
nd
adjacent cisterns.
Bibliography
I. Arut
iun
ov A,
Baron
MA, Majorova NA (1974)The
role
or
mechanical
ractors in the pathogenesis or
short-term and prolonged spasm or the cerebral
ancri
es.
J Ne urosurg40:
459
-
472
2.
Fox
JL (1979) Microsurgical exposure orintracra
nial
aneurysms.] Microsurg I:
2-31
3.
Fox
JL
(1983) Intmcrallial Aneurysms.
vol 2. New
York,
Springer-Ver
la
g,
pp
877
-
10
69
4.
Fox
JL, J
erez
A (1
974) An
unusual
aCOus
tic
neurinoma loca lized betwee n brain
stem
and basi
lar arlery using emulsified Pantopaque cisternog
raphy.
Surg Neurol 2:
329
-
332
5. Fox JL, A
lbin
MS, Sader DCH et al (1978)
Micro
su
rgical treatment of neurovascular disease.
Neurosurgery
3:
285-337
6. )<
ox JL, Nugent GR
(1976)
R
ecent advances
in
intracranial aneurysm surgery. \V Va
Me
d J
72:
104-
106
7.
Hayes
GJ , Slocum HC (1
962)
The
ac
hieveme m of
opt imal brain relaxation by hypervcntilation
technics
or anesthesia.J Neurosurg
19:
65-69

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 64/213
58
5. The Sy lvian Fissure
Fig. 5.2. Initial intradural exposure down right
sphenoid wing.
dum,
Dura rencctcd over drillcd
dowlJ sphenoid wi ng: tlr, arachnoid
hand
s between
dura and arachnoid mcmbranc;jf, frolllal lobe; 1l1,
brain rClraClOrs; II. tcrnporall obc; \'cin.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 65/213
Anatomy 59
r·
•
"
.
.
-.
<
,
fig. 5.3. Arachnoid mem
bra
ne
(ar) in
sylvian
fi ssur
e
distended
by
CS
F.
Prom in ent sylv ian vein (v) cov·
ered by this arachnoid
and
divides periphera lly into
twO bra
nches
(single-crossed
arrows) entering
•
,
....
•
. '
•
-
•
.
"..
••
f-
,
•
,
.....
.
.
) .
sphenoparie tal
si
nu
s. clp.
Malleable clips on d ural
edge;
If.
lem porallobc;jl. frontal lobe;
(lolJbie-crossed
r r u ~ a rachnoid on fronta l lobc side
of
sylvian veins.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 66/213
60
5.
Th
e Sylvian
Fis
s
ure
Fig.
5.4. Initial incision into sy lvian fissure
(arrows).
This is
0
11 the fronta l lobe (jl) s
id
e of the syl\·
ja
n veins
(v). Arachnoid membrane
(ar, lOP) is
stretched over
the
sy
lvian fissure. A rachnoid bands (ar. bottom) cross
a peripheral branch
(a, bottom) of
the middle cerebra l
artery. Abo\'c is a surface branch
(a, toP) of
the mid
dle cerebral artery o n th e temporal lobe.
rei,
Retrac
LO
r ;cot, cOllonoid.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 67/213
AnaLOmy
61
Fig. 5.5. Same case ("ig. 5.4). Distal ponion
of
right
sy lvian fissure widely
opened,
exposing a large fron·
tal M-2 ar lery
(m-2, bottom)
and a sma
li
lemporal
M-2
an
ery (rn -2, loP). ica , Imernal carolid ancry (oU(
of
focu s) ;
co
l,COltonoid under
rClracLOr;j1,
frontal lobe;
If, lc
mporal
lobe;ar, arachnoid band .

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 68/213
62
5. The Sylvian Fissure
II
Jf
(
"-
dura
- '
Fig .
5.6. Another case illustrating jeweler"s forceps
(jj)
grabbing arachnoid over
Syh,j.Ul fiss
ure
(arrow). fl.
Fromallobe; II, temporal Jobc;d1lra, dural margi n;$, suction
lU
be;
t',
vein. From to x [3).

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 69/213
Anatomy
63
fI ret
Fig. 5.7. Fu
rthe
r
opening
or sy Jvian fissure coma
in
in
g entwining vessels.
ar (toP),
Arachnoid
on
at herosclerotic inte rnal carot
id
artery
(ica); Ie,
tento
rial edge;
li·ret, temporal
lobe rei ractor;jl-rel, rrontal
tl-ret
(
,
JolJe retral:tor;
v, sy
l vian ve ins. N
ote
arachnoid bands
(ar, bottom) octween sy lvian vessels and pia. From
Fox
[3].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 70/213
64
5. The
Sy lvian
Fi
ssure
I \
II-ret
Fig.
5.8. Anoth
er
case to illustrate u
se of forcep
bla
de
s
ifcPl
to open and separate arach
no
id (ar) on
fr
ont
al lobe s
id
e of
sy
l\'ian veins.
/l-ret,
Temporal lobe
tl.f et
rct
rac to r;jl-rel,
fr
ontal lobe re tracLOr; col,
sma
ll cot
t
Oil
ba
ll
(from dental supply house).

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 71/213
Amllomy
65
Fi
g.
5.9. Arachnoid at base
of sylv
ian
fiss
ure is usu·
ally th
ic
kened
(ar)
and needs to be cut to expose basal
cisterns.
gr,
Gyrus rectuS;
2, opt
ic ne
..
. ej
ita,
illlernal
carotid artery;
dum, du
ra o,'cr sphen
oi
d wi ng; 3,
oc
ul
omotor nerve;
v, ve
ins;ti, temporallobe;fcp. for
ceps.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 72/213
66
5. T he Sylvian fissure
Fig.
5.10. Anot her case after
partial opening
of
arachnoid
(ar,
lOP)
over sylvian fissure. Arachnoid
ba
nds (ar, hottom) connect branch (a)
of
m
id
dle cere·
br
al
artery
wit
h pia. cot, Cottonoids under retractors;
fl.
frontal lobe; 2, optic nerve; ica, internal carotid ar
tery; pc, poste rior clinoid process; v, sy lvia n ve ins; It,
temporal lobe. T he vei n
(v, lOP)
is entering the
sphenoparietal sinus.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 73/213
Anatom),
67
Fig. 5.11 . Same case (Fig. 5.10) after further separa
tion
of
arachnoid
(ar,
below) b
)'
blades
of
forceps
ifcp}, or (toP), Arachno
id
band
O\
'er optic ne n'eJ
carotid arrer)' ju ncuon;pc, I>ostenor cli no id process;
V, vein;
I'll,
retracto r on tcml>oraiiobe.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 74/213
68
5. The
Sylvian Fissure
\
--
Fig. 5.12. Same case (Fig. 5.10) after clearocoagula
lion
of
vei n (v) to sphenoparietal
sin
us. dura,
Du
ra
over drilled-down sphenoid wing; te, tentorial edge;
mem,
membrane
of Liliequisl ill background (pointer
crosses more supe rficial frontal lobe and internal
carotid artcry) ;sc, microscissors.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 75/213
Anatomy
69
Fig. 5
.1
3. S
.
me case (Fig.
5.
10) arter rur ther separa
lion or rrontal lobe
(j1)
and te
rn
pordl lobe.
Th
e
arachnoid membrane or Li licqu iSl
(mem)
has beC I1
partially opened. re\'ealing the basi lar artcry (ba) in
the interpeduncular cistern. T he uncus (un) is sti
ll
ad hercnt to thc oculomotor nerve (3). s. Suction
tube; 2, optic nervc;pt:. posterior cli noid process; at ,
ante
ri
or
cli
noid process.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 76/213
70
5. The
Sylvian Fissure
fig. 5.14. Another case after opening per ipheral
part
of
right
sylv
ian fissure. Note arachnoid bands
(ar) between arteries and between arterial branches
and pia.
The
temporal (I) and frontal
if)
branches
of
(
I
/1- t
r
•
,
fJ
I
,
the middle cerebra l artery are projecting out of the
depths
of
the sylvian fissure and toward the ob
server. rei, Retractor;
Il,
temporal lobe;
fl.
frontal
lobe.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 77/213
Anatomy
71
Fig. 5
.15.
Another
cas
e after partial opening
of
right
sy lvian
fis
sure
(crossed arrow).
Branch
(a)
of middle
cerebral arter y lies on island of Reil
(*)
and co mes
from depths
of sy
lvian
fi
ssure.
ad,
Adhesions (elec-
trocoagulated) between frontal
lo
be
(jl)
and tem
porallobe (If). col, Coltonoids under brain retractors;
ar,
arachn
oi
d band.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 78/213
72
5. The
Sylvian Fissure
Fig. 5.16. Same case (Fig. 5. 15) after
furt
h
er opening
of sy
l
vi3n
fissure.
dura,
Dura over drilled-down
sphenoid wing; or, arachnoid membrane stretched
between frontal and temporal lobes;
Ii-ret,
tempor
al
lobe re
tr
actOr;
floret,
frontal l
obe
retractor. Note
many arachnoid bands between branches (a) of lhe
middle cerebral artery and between arteries and pia
(shown
unde
r
greater
magnification in the next fig
ure).

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 79/213
AnalOmy
73
Fig. 5.17. Same case (Fig. 5.16) and vicw
undcr
grcat
er
magnification (o ld Zeiss dial No. 25 or new Zeiss
dial No. 1.6). Crossed arrows, examples
of
the many
arachnoid bands: col, coltonoid
under retraclor;fl.
frontal lobe.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 80/213
74
5. The
Sy lvian Fissure
Fig
.
5.18. Another case where arachnoid at base
of
sy
l
via
n
fis
sure is being cut by microscissor
s.
A suc
lion
tube
(s) is in
the surgeon's
Jcrt hand and mi
cro
scissors are in his righl.
Th
e optic nerve (2)
and
the
i/Hernal ca rotid artery (ica) arc still covered by
arachnoid.
cot,
Sma
ll cOlton
ball;
rtt,
retractor on
frontal lobe; v, ve in from temporal lobe to
sphenoparietal
si
nu
s; II,
temporal lobe. From
Fox
[2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 81/213
Anatomy 75
Fig. 5.19. Example of 1\\'0 fron
t..a
l (I:Mmom) and one
temporal (top) M
-2
branches
(m-2)
arising from the
M-I artery (m-/). on,
Ba
se of aneu rysm with dome
buried in temporal lobe
(If); ala,
anteri
or
temporal
arte
ry;
v. \·eins;j1. fronta l lobe.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 82/213
76
5.
The
SyJ
vi
an
Fi
ssure
Fig. 5.20. Exampleof middlecerebral arter y pmject
ing through partial opening of sy lvian fi ssure.
cot,
Coltonoids
under retractor;jl. frontallobc; an
,
twO
microanc
urys
ms of
1\'1-1
artery (m -I) bifurcation; pia,
posterior temporal ar tery: fl, temporal lobe;
I,
tem
pol-al M-2 branch;
G,
small artery;
v,
vcins;f, frontal
1\'
1
-2
brauch.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 83/213
Anatomy
77
Fig. 5.21. Vi
ew
along a widely opened right sylvian
fissure uncler le
ss
magnification (old Zeiss dial
No. 10
or
leI,' Zeiss dial No. 0.6). fl·rel, Frontal lobe
retranor; 2, optic nerve; ica, imerna l carotid artery;
double-crossed
arrfJUl, origin
of
anterior choroidal ar
tery; single-crossel{ arrow. crosses dome of ica
aneurysm and poims to poste rior commu nicating a r-
-
tcry dcep to aneurysm; ala, antcrior tcmporal ar
tcry; Il-,.et, temporal lobe retractor; cot, couono id ; 1/1-
2, M-2
arter
ies
ar
isi ng wit h multilobulated
aneurysms at bifurcation of the M- I artery (m-/); ox,
ox),ce
ll
ulose (Surgicel);ar, arachnoid band
s;a-I,
A- I
artery. From "ox [3].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 84/213
78
5.
T he Syl\'ian Fissure
Fi
g.
5.22. Example of lo ng M-l artery (m-/) buried
deep
in right
sylv
ian fissure. rei, Retractor on the
tempor
al
lobe;
cot,
cOltonoid; v, \'cins;
an,
small
aneurysm flanked by tempo l'a] M-2 artery
(loP)
and
,,'
(
r
onlal M-2
artery
(bottom).
NOle
perforators sUlek
to
dome
of
aneurysm.
ala ,
Anterior tempo ral artery.
From
Fox
[2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 85/213
AnaLOmy
79
Fig.
5.
23. Example
of
short M· I artery (m.I) at base
of
sylvian fissure.
slw,
Superior hypophyseal artery;
ica, bifurcation of internal carotid artery; ala, an·
terior temporal artery;
an,
small aneur
ysm
nanked
by temporal M·2 artery (t) and frontal aner), (j);
ar, arach noid fibers enveloping perforators;
p,
per
forating arteries arising from the
A-I
artery (a-I)
and entering the a nterior
per
forated substance; at,
optic tract. The M- I perforators are mostly hidden
be
hind the M-l ar te ry. From Fox [2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 86/213
80
5. The S)'lvian Fissure
Fig. 5.24. Example of atherosclerotic internal
carotid a rlery (*) bifufcation seen after a wide open
in
g of the sy lvian fiss ure .
mem,
Dceply located mem
br
ane
of Liliequist; a-I, A- I anery; mol, M-I arter),;
ach, am criorchoroidaJ artcry;ar, arachnoid band be-
I
\
. r?-
u
C?,
,
tween artery
and
tempora l lobe; I, temporal
M-2
af
ter
y;f,
frontal M-2 artery; p, perforators from A-I
and M-l an e rics;o/, optic tract;
v,
veins;
110.,
ret:
ur
reru
artery of Heu
bner;
ch, optic chiasm.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 87/213
Anatomy
81
Fig. 5.25. Internal carotid artery (ica) bifurcation at
base
of
syl
via
n
fis
s
ure
(at higher magnification: old
Zeiss dial No. 25 or new Zeiss dial No. 1.6). hp,
hypothalamic perforators from internal carotid ar·
lery (ica); acll, anterior choroidal artery; mem, deeply
located arachnoid membrane
of
Liliequist;
m-l,
M-I
artery entering
sy
lvian fissure; p, perforators from
internal carotid and M-J ar teries; ho., artery
of
Heubner; a-J, A-I artery; ret, frontal lobe retractor;
ot,
optic tract; eh, opticchiasm;ar, arachnoid bands.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 88/213
82
5. The Sylvian Fissure
\
."
. -,
.,
'"
gel
f[-ret
Fi
g. 5.26. Transsylvian view of M-J (m-l)
and
A-I (a
J) origins from internal carotid artery (ica). CrOSJed
arrow, or
igin
of
anterior
choroida
l
anery;
pea, minis
cule posterior communicating artery whose anterior
thalamic perforaLOrs (p) are notable; 00, basilar ar
tery in background; sea, right superior cerebellar ar-
terYi 1'-1, large P_I
artery;
/l.ret,
tcmporallobe
retrac
torian, base ofaneu rysm (from bi furcation o f basilar
artery);
ot,
optic tract (see a<ljacent
perforato
rs from
A-I
l;jl-ret,
frontal lobe retractor; gel, gelatin sponge
(G
cl foam); ch, optic chiasm; 2, optic nerve;
Pit, piLUil
ary stalk. From Fox [3].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 89/213
Anatomy 83
Fig. 5.27. Another exam p
ic of
transsylvian view
of
A-I (a-I)
and M-I
(m-l)
origins from short internal
carot
id
artery
(iea).
Note anterior thalamic per
forators and arachnoid bands coming
of
f posterior
communicat
in
g arlcry (pea) . Retraction
of
the uncus
(unc)
causes angulation
of
the oculomotor nc
l '-'
c (3)
lateral to the poste l-ior clinoid process (pe).fib, Fibrin
from previous hcmorrhage;
ala,
anterior temporal
arlery; m-2, M-2 a
rt
ery; 01, op
tic
tract; p, perforator
from
anery of
Heu
bner;jl-ret,
frontal
lobe
retractor;
cit,
optic ch
ia
sm;
2,
optic nerve; ac, anterior clinoid
process. From "ox (3].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 90/213
84
5. T he Sy lvian Fissure
Fig.
5.28. An
other
case where the interna l carotid
ar
lCr
y bifurcation
(crQSMd
arrow)
is well
seen
af
ter the
sylvian
fiss
ure
is
widely opened. Note leash
of
arachnoid bands
and
perforators (p) passing from A-
I
(a-I) to
the
anterior
perforated substance.
ell, opt
ic
chiasm;
Qt,
optic tracl;
00,
basilar artery;slm, superior
hypophyseal arlcry;o7l, aneurysm
orica
at
rakeoffof
anteri
or
choroidal aftery;
m-I,
M-l artery.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 91/213
Anatomy
85
Fig. 5.29. Base of aneurysm (an) at bifurcation of in
lernal carotid artery
(ica),
transsy lvian
view
. Artery
of Heubner (1m) is adherent to aneurysm. a-I,
A-
I ar
tcry; If, lamina terminal is; ot, optic tract; adm, an-
ter io r ch
or
oidal artery; pea, poste rior communic
.1.t
ing artery; If, temporal lobe; m_l. M- J aner)';cof, cOt
tonoid ;
1111,
rctractoTs;j1, frontal lobe . From
Fox [3]
.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 92/213
86
5.
The Sylv
ian Fissure
Fig. 5.30. Another case illustrating the anatomy of
the right syJv ian fissure. Arachnoid sti ll CQ\ 'crs the
sy
lvia n fissure (between crossed
arrows) in
which the
ar teries arc exposed
by
separation
of
the frontal
(jl)
and temporal (tf) lobes. rei, Retractor; spit, dura rc
nected over s
phenoid
wing; v. ve in.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 93/213
Anatomy
87
Fig. 5.31. Same case
(Fig.
5.30) after the arachnoid
(ar)
over the
sylv
ian fissure has been opened.
Periphera l branches
(a)
of the middle cerebra l arte ry
project themselves toward the surgeon. Deeper
M-2
branches rem
ai
n covered by a deeper layer of
arachnoid (crossed
arrow).
Note strands
of
arachnoid
fibers su
ppor
ting the arteries.
*,
Unseparated
deeper portions
of
the fromal and tempora l lobes.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 94/213
88
5.
Th
e Sy h'ian Fissure
Fig. 5.32. Same case (Fig. 5.30) after removal of the
deeper arachnoid layer.
Th
e frontal M·2 branch
(single-cros.sed arrow) and the temporal
M-2
branch
(dQuble-trOSMd an-ow)
are seen. ala, Aillcri
or
temporal
ar tery.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 95/213
Anatomy 89
".
Fig. 5.33. Same easc (Fig. 5.30) aflcrcxposurc of the
M-
I
arte
r}'
(m-l) deep
in the sylvian fiss ure. The M-I
division into the frontal (single-crossed arrow) and
tempor
al
(double.crossed arrow) is seen. Note leash of
stria thalamic perforators (perf) passing from M-l.
cr
ossi
ng the right op
tic
tract (ot), and enter ing thc an
tcrior perforated substance
under
the frontal lobc
retractor
(ret).
fl, Temporal lobe; an, giant intern al
carotid aneurysm; ala, anterior temporal
arte
r y.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 96/213
90
5.
The
Sy lvian Fissure
}
Fig. 5.34. Samccase (Fig. 5.30) wit h more magnifi
ed
view
of
]\,1· I
1/1+
1) perforators. pel[.
One
of man)' M-l
perforaLOrs; m-2, M-2 arteries;
rei,
fromal lobe re-
tractor;
01,
optic t
ra
ct;
an,
aneu
rys
m;
(1.1;
linc
arachnoid fibers
from
art.eries.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 97/213
Anatomy
91
Fig . 5.35. Another case showing arterial anatomy
of
base of right
sy
l
via
n fissure. Note unusually large
perf
or
ator (double-crossed arrow) arising from the M-
1
ar t
e ry
(m-/).
II, Temporal lobe;
ala,
an t
er
i
or
tem
poral artery;
lia,
ar tery of Heubner; 01, op tic tract
;j1,
.I
fmnla1 lobe;
aI;
arachnoid fibers;
a- I, A-
I artery; eh,
optic chiasm; iea, internal camtid arter
y; pea,
pos
t
er
i
or
communicating artery; single-crossed arrow. an
terior choroidal anery.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 98/213
92
5.
The Syh"ian Fiss ure
Fig . 5.36.
Left
internal carotid
ancriogram
illustrating stria thalamic perforators
frolll lhe
M- I and
A-I
ar
teries. Patient had aneurysm
(arrow)
alorigin of A- I and al or igin ofantcl"ior choroidal artery. From
Fox
and
Nugent [61 with permission from the West Virginia State l\Iedical Association.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 99/213
6
The Carotid Cistern and
Environs
Introduction
The
carotid cistern,
the
chiasmatic cistern,
and
the cistern of the lamina lcrminalis lie rostral to
the arachnoid membrane
of
Liliequist (mem
brane of Key
and
Retzius). Surgical observa
tions regard ing the cerebra l sp inal nuid (CSF)
cisterns and their
companmental
divisions arc
de
scribed elsewhere [3]. Fi g
ure 6.1
is a coronal
com pUled tomography (CT) image
(a
cistern
ogram) that nicely illustrates the rela tionship
of the illlcrn
al
carotid
ar t
ery to the carotid c
is-
tern bounded late rallyby the medial portion of
the temporal lobe.
Po
steriorly the carotid
cis
tern
is
se
par
ated
from
the
in ter peduncular
ci
s
t
ern
(see C
hapter
8) by the arachnoid mem
brane of Lilicquisl; mediall y the carot id cistern
joins the chiasmatic
and
lamina terminalis cis
terns and superi orly it joins the sy lvian ciste
rn
(
fi
ssure). In Fig. 6 .1 note the bifurcation of the
internal carotid
arte
ry into the middle cerebral
artery (r..'I-1 segment)
and
the
anterior
cerebral
artery (A- I segment). Th is occurs
altheconflu
ence of thc
upp
e r pan of the carotid cistcrn,
Fig. 6.1. Cisternogram with iopamidol in CS Fimaged by coron
al
CTscan
LO
show anatomyofimernal carotid
arte
ry
(
black (/),-ow) wilh cisterns
and
brain. Open arrow, A-I arter),; black
arrowhead,
optic chiasm;
while arrow
head,
uncus of temporallobc; wltill' (j/TOU \ contrasl medium in s)'Jvian fissure
(c
istern ). See text.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 100/213
94
6. Th e Carotid Cistern
and
Environs
Fig.
6.2.
Tomographic image after ai r has replaced some CSF
by
pneu moencephalography (pati
eoti
n sitting
position). Closed G/'rQW, lies in interpeduncular cistern
and
poims to arac
hn
oid membrane of Liliequisl (Key
and
Retziu
s). Open arrow,
ai r in aqueduct ofSylvius. Sec text.
the lower-medial
pan
of the sylvian cistern
(co
ntaining the
M-
I origin
),
and the
upper
-lat
eral part
of
the chiasm
at
ic
ci
stern
(c
ontaining
the A- I orig
in ).
This confluence is bounded
superiorly
by
the an terior perforated sub
stance of the frontal lobe.
In earlier years when pneumoencephalog
raphy
was
a co
mmon
intracranial
im
aging
pr
o
ce
dur
e, th e injected gas (u
sua
ll y air), which re
pl aced or di
sp
laced some of the CSF often was
tempo
rarily trapped
in
the int
er peduncular
ci
stern (Fig. 6.2).
The
air
was pr
evented from
pa
ss
in g through membrane openings and into
the anterior cisterns by the membrane
of
Liliequist until a sufficient
pr
ess
ur
e
diff
ere
n
tial developed to overcome adhesive forces be
tween the air bubbles and the moist arachno id
membran
es
.
The
membrane
of
Liliequist. known origi
nally as the membraneof Key and Retziu s. isan
important arachnoid landmark [2]. The mem
brane run s from the
dor
sum
sella
e and po
s
terior clinoid processes up
wa
rd toward the
mammillary bodies
of
the hypothalamus. It
passes from
si
de to side between both
oculomotor nerves (see
Fig.
8.1).
No
rm ally
it
is
eith
er
a solid, translucent sheet with openings
on either side
or
a multi perforated membrane
allowing passage of CSF from the posterior
fossa into the anterior cistern s, from whence
CSF circulation continues over the surface of
the brain. After subarachnoid
hemorrha
ge
or
meningitis, adhesions along this membrane
m
ay
seal offCSF passageways and ca use a com
municating h
yd
roce
ph
alus.
Opening
either
this mem
br
ane
or
the lamina t
er
minalis at
s
urger
y releases much CSF and may be a per
manent cure for patients wi th hydrocephalu
s.
U
nl
ess
one
is
approaching
a lesion
in
the inter
peduncular
ci
ste rn
or
attempting lO release
CS
F from the posterior cisterns,
it
is better to
leave the
Lili
equ
is
t membrane intact.
It
acts
as
an effe
Clive
barrier to
surg
ical blood entering
the posterior basal cistern s. Further details are
given in another textbook [2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 101/213
Anatomy
95
Anatomy
Th
e surgical anatomy prc
sc
mcd
in
this alias is
oriented as the surgeon sees it through the
operating microscope at surgery.
I t
is
always
de
pi
cted on the right
si
de
of the patient for ob
server consisten
cy, and
the
reader
may
ne
ed to
refer to the figures
in
Chapter 4 (especially
Fig.4.8) for occasional orientation of the
supine p
at
ient's head. T he
ri
ght o
lf
actory tract
wi
ll
al
ways
head toward the uppe r- left corner
of
the figure (towa rd the paticm's nose), and
the
ri
g
hl
lcmporallobc (usually its uncu
s) wi ll
li
e und er a ribbon re
tr
ac tor 011 the right s
id
e of
the field (toward the
p
al
iem's
riglll ear).
Now
that the
sy
lvian fissure has been
opened
(C
hap
ter
5), the surgeon recognizes
normal
(o
r abno
rm
al)
va ri
at
ions
in
s
ur
gical
anatomy as seen between the ba sc
of
the sy lv
ia
n
fissu re and t he dura reflccted ovcr the drilled
d
ow
n and surg ica
ll
y
fl
attcncd sphenoid w
in
g
i g s 6.3 and 6.4). The
fi
rst visible branch
of
the internal carotid artcry is usuall} not lhe
ophth
al
mi c artery, f
or
the
or
igin of the
ophthalmic artery invariably
is
hidden by the
superiorly and medially overlapping optic
nerve.
The
ophth
al
mi c artery usually
ar
ises on
the medial side
of
the carotid artery ju st below.
above. or at the level
of
the exit
of
the carotid
artery from thc cavernous sinus. Most com
monly the surgeon first recogni zes the ori gin
of the posterior communicatin g artery on thc
latcral, poste
ri
or, or posterolateral side
of
the
ca rotid
ar t
ery; but on close inspection onc can
see more proximal (ie. toward the heart ) arte
rial
br
anches, which are the superior hypo
physea l artery (
Fi
g. 6.4) and hypophyseal per
forators. Throughollt this cha pter the reader
will note how close the
in
ternal carot
id
artery
comes to the posteri
or
clinoid process. and at
times its bifurcation is behind the level
of
the
dorsum
se ll
ae.
The
oc
ul
omotor nerve (third
cran
ia
l nerve) al
ways
l
ies
external to the pos
terior
cl in
o
id
process. as th is nerve passes fo
r
ward
under
thc anterior reflcc
ti
on of the ten
torium and into the to p of the cavernous sinus
(sec Fi gs. 8.2 and 8.3).
The intracranial portion
of
the internal
ca rotid artery may be fairly long, as noted in
Figs. 6.3 and 6.4,
or
sho rt , as demonstrated in
i g s
6.5 and 6.6. T he shorter this internal
carotid artery segment. the more readily the
surgeon can expose the
or
ig
in
s
of
the
A-I
and
M I branches.
A leash
of
vi tal perforating ar tcries arises
from the posteroinferior s
id
e
of
the internal
carotid artcry and the posterior communicat
in
g artery (
Fi
gs.
6.7 and 6.8). Often
one
has to
retract the carotid artcry medially
or
latera lly
to sce thcm. Thcse perforators include the
superio r hypophyseal artcry. hypophyseal per
forators, and anterior thalami c p
erforato
r
s. As
the s
urg
eon ret racts the fro ntal lobe. the olfac
tory tract and gy ru s rec tus come into v
ie
w.
Commonl
y,
thc r
ecurrc
nt artery
of
Hcubner
(pc
rf
orator from the antcrior cerebral artery)
is seen in the Cl"cvicc betwee n the retracted
frontal lobe
and
the optic nerve (Fig. 6.7).
Wh cn large, this may be mi staken for the A-I
artery, which
li
es
be
hind
(o
r in front) and
below the artery of Hcubner.
As
one retracts the temporal lobe, a major
i
nt
ernal carotid artery branch with
in
the
carotid cistern will be the antcriorchoroidal ar
tcry
or
arteries (
fr
equently there may be two
or
evcn three) as illustrated
in Fi
gs. 6.9 and 6.10.
This artcry arises latera
ll
y, postcrio
rl
y, or pos
t
erolatera
ll
y from the internal carotid artery
and passes posterio
rl
y under the uncus
of
the
temporal lobe.
II
.
ente
rs the choroid fi
ssur
e
and
pa
sses thence into the temporal horn .
As
this artery travels bac
k,
it m
ay
come
in
close
proximity to the bifurcation of the internal
ca rotid artcry and i
ts
perforator
s.
The
posterior communicating
ar
tery may be
seen decp to the space between the carotid
ar·
tery and the optic ncr
ve
(see
Fi
gs. 6.6 and 6.9).
or
it
may bowolltlatcraliy as show n in Figs . 6.11
and 6 .12 . Eve n when the posterior
CO Il l
municating ar tery is small (Figs. 6. 13 and 6 .14),
it will contain v
it
al anterior thalamic per
forators to the brai nstem. Often an infun
dibulum
of
the posterior communicating ar
tery is seen, and its appearance suggests a
prcanc
ur
ys
m
al
anomaly (
Fi
g. 6
.1
5)
dcveloping
at the distal angle
be
tween
in
tern al carotid a r
tery and the poster ior communicatin g artery,
the classical si tc
of
such aneurysms (
Fig.
6.16).
Although the pituitary stalk
li
cs
in
the
ba
ck
of
the chiasmatic cistcrn, it often is readily
identificd upon exposure
of
the carotid cis
tern. As show n in Figs. 6.7 and 6. 11 , for exam
ple, the ptcrional approach renders the pituit
ary stalk
visi
ble through the space betwecn thc

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 102/213
96
6.
The
Carotid Cistern and Environs
Table 6.1. Structures contai ned within the carotid 6sterns',
1.
Internal carotid artery
2. Origin of the ophthalmic artery (not always)
3. Origin of the superior hypophyseal anery
4. Origin
of
the posterior communicating
anery
5. Origin of the anterior choroidal artery
6. Origin orlhe middle cerebral artery (M- I)
7.
Origin orthe anterior cerebral artery (A·l)
8. Origins of the hypothalamic perforator s from the carotid
artery
9. Origins of the more rostral anterior thalamic perforators
10. Some stria thalamic perforatorll
II.
A portion orthe
artery of
Heubner
12.
A portion
of
Ihe ante rior perforalCd substance
of
the frontal lobe
13.
Medial surface orthe temporal lobe
14. Lateral border orlhe optic nerve
15. Sympathetk fibers on the internal carotid artery
16. Rostral edge of the poster ior clinoid process (dural covering)
17. Anterior cli noid process (du ral covering)
18. A portioll
of
the tentOrial edge between the anterior
and
postcriorclinoid
processes
Items 12-14 and 16-18 can be considered to form portions
of
the margins
of the carot id cistern. Sec Fig. 6.1.
oplic apparatus and the carotid arter
y.
The
sla
lk
li
es
be tween the arachno id membrane
of
Liliequisl posteriorly and the o ptic chiasm an
teriorl
y.
It appears as a reddish, vascularized
projection pa
ss
ing inferiorly through the
op
ening
in
the
diaphragm
se
ll
ae. T he superior
hypophyseal artery and hypothalamic per
forators pr
ov
ide a rich
ane
rial blood supply,
an d the ponal plexus
of ve
ins also are visible
under micro
scope
.
Regard
less of
the locati
on of
the lesion,
we
not
on
ly open the sy lvian fi
ss
ure substantiall y
but
we
also lyse a
dh
esi
on
s and arachnoid
(which separates the carotid and chiasmat
ic
cisterns) betwee n the ips
il
atera l optic nerve
and the base of the frontal lobe when usi ng the
pter ional ap proach (Figs. 6 .1 7 and 6. 18). This
allows: (a) gentle retraction
of
the frontal lobe
without adhesions pulling on the
op ti
c nerve,
(b) less brain retraction pre
ss
ure, (c) occa
sional inspeClion
of
the anterior communicat
ing complex
in
aneurysm cases, (d) exposure
of
the lamina tc rmina
li
s in cases with hydro
cephalu
s,
and (e) assessment
of loc
al anatomi
cal variations and enha
nc
e
ment of
the su
r
geon's knowledge of surgical anatom
y.
In our
experience the latter is done at no risk [Q the
patient and has
be
en extremely important
in
honing the surgeon's s
kill
s. in patients without
lesions in the
anterior
communica ting region,
actual exposure
of
the anterior communicat
ing a
ner
y is not
done in
pa tients who would re
quire significant frontal lobe retrac tion .
Figures 6.19 and 6.20 illustrate how,
in
some
cases, the internal ca rotid artery ca n extend
or
project above
and
behind the level
of
the pos
terior clinoid processes and the dorsum se llae.
H
ere we
are l
oo
king med
ia ll
y behind the
op
tic
apparatus (nerve, chi asm, and traCl); the lOp
and side of the do rsum se
ll
ae are brought into
vIew.
Although not proved hi stologically
in
this
case (Fig. 6.21), we believe that sy
mp
athetic fi
bers are seen traveling on the adventitia of the
internal carotid
aner
y in the carotid cis t
ern.
T hey ca n
be
mi staken for arachnoid bands and
vIce versa.
Upon elevation
of
the frontal lobes
in
the
nons
wo
ll
en brain , a
view of
the medial side of
the opposite carotid cistern can be visualized
(Fig. 6.22) . Note h
ow
the medial s
id
e of the
temporal lobe forms the lateral
boundar
y
of
the caro tid cistern. Figures 6.23 and 6.24 aga in
show how the carotid cistern is bounded be
hind
by
the arachnoid membrane of
Lil
iequist,
above by the anterior perforated substance,
laterally by the tem poral lobe, and medially by
the chiasmatic cistern. T he membrane
of
Lili
equist
appears
blue when CSF remains be
hind it
in
the interpeduncular cistern.
Th
e

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 103/213
Anatomy 97
color turns black when the CS F is drained (eg,
by aspiration or
lu
mbar puncture) so as to leave
only a shadowed space without the reflecting
and refracting water (CSF ). Note the unusual
ve in
s (bilateral) from the unseen cavernous
sinus to the unseen ba si lar vein
of
Ro senthal,
the unusual position of the pituitary gland in a
shallow pituitary fossa, the portal veins on the
pituitary sta
lk
, and the opposite posterior com
municating artery seen
through
the space be
tween the optic nerves.
Figures 6.25 and 6.26 represent another
exam
pl
e
of
the carotid cistern and environs.
No te the superior hypo
ph
yseal artery, pituit
ary sta
lk
, and anterior thal amic perforators
with hypophyseal perforators (dis
pl
aced me-
dially
by
giant aneu rysm). Table 6
.1
sum
maries the
va
rious structures fo
und in
the
carotid cistern.
The
next chapter will take us
i ~ t o the more medial chiasmatic and adjacent
cIstern s.
Bibliography
I. Fox JL
(19
79)
Microsurgical exposure ofintracra
nial ane urysms. J Microsurg
I: 2-3 1
2. Fox
JL
(1983) IntmcranUiI Aneurysms. New York,
Springer-Verlag, frontispiece,
pp 877
- \069
3. a ~ a r g i l MG, Kasdaglis K, Jain KK et al (1976)
Anatomical obser
va
tions
of
the subarachnoid cist
erns
of
the brain during surgery. J
Ne
urosurg
44:298-302

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 104/213
98
6. The Carot id Cistern
and
Environs
Fig. 6.3. View of right carotid cistern and environs.
aI', Arachnoid membrane between the optic nerves;
1, olfactory trdct; gr, gyrus rcctus; 2,
ri
ght optic
nerve;
Ttl,
retractor
on
frontal lobe;
crossed arrow,
ori
gin of the posterior communicating artery; ica, inter
nal carotid arter
y;
3, oculomotor nerve passing for
ward uncler the morc lateral tentorial edge (Ie), by
the more medial posterior clinoid process (PC)
and
thence imo the C3 \'e
rn
OUS si
nu
s; mem, a refleClion of
Liliequisl's mcmhl<tlle. Between the oculomotor
nerve and Liliequisl's
membrane
is a black,dear CSF
passageway into the interpeduncular cistern. Note
the attachment of Li liequist's arachno
id
al mem
brane to the posteri
or
clinoid and adjacent do rs um
sellae. Opening this membrane between the
oculomotor nerve and the internal carotid
arte
ry
is
the usual frolllolatcral route
to
the interpeduncular
cistern. From
x
[ I].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 105/213
Anatomy 99
Fig.6.4. Carotid cistcrn in another patient.
or,
Arachnoid between optic nerves; 2, right optic
nerve;
slUJ,
superior hypophyseal arter y; ica, internal
carotid artery; Ie, anterior reflection
of
tentorial
edge, 3, oculomotor nerve passing late ral
to
duraon
posterior d inoid process (PC
); pea,
posterior com·
municating anery;
mem,
membrane
of
Liliequis
t;fl·
rei , froma
ll
obe retractor; 1, ol factory tract; v, ve in 011
gyrus rectus (gr). From Fox
[2
].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 106/213
100
6. The Carotid Cistern
and
Environs
Fig. 6.5. Right carotid cistern with shon internal
carotid artery
(ica).
2, Optic nerve;
ac,
anterior
clinoid process; mem, membrane of Lil
ie
quisl (cover.
ing posterior clinoid process); pea, origin of pos
terior commu nicating artery; ), oculomotor nerve;
ad,
adhesions between aneurysm
(an)
and temporal
lobe (/l);cot, couonoid;ata, anterior temporal artery;
crossed
arrow, origin
of
anterior choroida l artery; bif,
bifurcation of carotid artery; fr i , origin of A-I ar
tery;ft. frontal lobe. From Fox [2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 107/213
Anatomy
101
Fig. 6.6. Anotherexample
of
a short internal carotid
artery (ica)
.
Note yellow atherosclerotic plaque. pea,
Or igin of post
er
ior communicating artery (lateral
pea)
passing behind carotid artery and reappearing
deep to space betwcen optic nerve
(2)
and carotid ar·
{cry;
gel,
Gelfoam on optic nerve;
a-I,
right
A-
I
ar
tcry; bif, bifurcation of carotid artery; ret, temporal
lobe re tractor; an, aneurysm; ad, adhesions between
aneurysm and tentorium
(te).
From F
ox
[ I
].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 108/213
102
6. Th e Carot
id
Cistern and Environs
Fig.
6.7.
Example
of
long atherosclerotic internal
carotid artery (ica) and environs. Many
hypothalamic (including superior hypophyseal ar
tery) and anterior thalamic perforators (enclosed in
an envelope
of
arachnoid)
arc
seen passing back and
media lly from the carotid artery and the posterior
communicating artery
(pea). peif, One
of these per-
rorators comingoff he carotid
ancry
; , oculomotor
nerve, tl, uncus
of
temporal lobe;jl. frOlltal lobe; ret,
retractOr; J, olfaClory tract;
ar,
arachnoid between
opt
ic
nCfI'
CS;
2, right optic nerve;
JUl,
recu rrent ar
tery
of
H
eubner;pil
, vascular pit
ui
tarystalk;pc, d ura
on posteri
or
clinoid process. f rom Fox [2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 109/213
Anawmy
103
1( /
, ,
I ,
/
Fig. 6.8. Greatly magn
ifi
ed
view
between
ri
ght optic
t
ra
ct
(ot)
and internal carotid artery
(ica). Ze
iss d ial
set at
No.
2.5
(ol
d
No.
40). Anterior thalamic per
fOTawrs(jJeifj
from carotid
aneryand
posterior com-
municating artery
(pca)
are see
n. 2,
Optic n
en
-e;
mem ,
membrane
of Lili
equist; pro probe retracting
carotid artery laterally. From
Fox
[I
].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 110/213
104
6. The Carotid Cistern
and
Environs
Fig.
6.9. Carotid cistern with origins
of
posterior
communicating artery
(pea)
and anterior choroidal
artery (acha) from internal carotid artery (jea). mem,
Membrane of Liliequist;
an,
aneurysm; 3, oculo-
',
mOLOr ncrvc;ad , adhesions between frontal lobe
and
optic tract (ot); pit, pituitary stalk; 2, optic nerve; 00,
origin
of
ophthalmic artery; ret, retractors. From
Fox [2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 111/213
Anatomy
105
ha
Fig
.
6.10.
View
of
carot
id
cistern showi ng relation
ship
of
anterior choro
id
al
anery (acha)
to the uncus
(tine)
of the temporal l
obe./I(1.,
Anery
of
Heubner;
J,
olfactory tract;
gr.
gyrus rectu
s; 2,
optic nerve;
iea.
i
n
lel'llal ca rot id
ar
ler
y; pea,
origin of posterior com·
muni
ca
tin g anery;
Ie,
tentorial edge;
all,
aneur
ys
m
(shrunken and elongated by bipol
ar
electrocoagula
tion);
ad,
adhesions and fibrin between aneurysm
and temporal lobe and tentorium. Deep to the an
terior choroidal anery
(adUJ)
li
es the arachnoid
membrdne
of
Li liequisL From Fox [I].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 112/213
106
6, The Carotid Cistern and Environs
Fig.6. 1I . View of carotid cistern with laterally di·
rected posterior communicating artery
(pea). mol,
M-l origin;peif, perforators from A-I (a-I); ot, righ t
optic tract; Jryp, hypothalamic
per
foraLOrs from
carotid artery; pil, pituitary stalk; ch, optic chiasm; 2,
l
eft and
right optic nerves; (-ica, medial side
ofleft ill-
lernal carotid artery; dia, diaphragm
se
ll
ae;
pc,
left
posterior clinoid process; crossed arrow, superior
hypophyseal artery; r-ica, right internal carotid ar
tery; r-pc, right posterior clinoid process; ), oculo
motor
len"e. F
rom Fox
[2J.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 113/213
An alO my
107
Fig. 6.12. A very athcrosclerOlic imcrnal carotid ar
tery
(ica)
with the posterior co mmunicating artery
(fxa) goi
ng latcrall
y. Crosud
r r ~ crosses dome
or
atherosclerotic aneurysm and points to
perf
orator.
adm,
Ante rior choroidal artery; 00, basitar
arter
),
lying
in
imerpedunc
ular
cistern and seen
ar
t
er
re-
mova l
of
membralle
or
Li licquist
(In. m)
sti
ll
attached
to oc
ul
o
mO lOr ncn 'e
(J) and posterior clino
id
pro
cess
(PC),
rtt, Retractor on
ri
ght tempora l lobe;
e
, ten
lorial edge; at:, anterior clinoid process; 2, optic
nerve,

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 114/213
1
08 6. The
CarOlid Cistern and Environs
cot
--=- ---
Fig.
6.13.
Example of small, sh
ort
posterior com
mun icating artery (crossed arrow) connecting internal
carotid artery (ica) with posteri
or
cerebral artery (p-
2). cot,
Cotlonoid;
unc,
uncus
of
temporal lobe;
an
,
small aneurysm at takeoff of anterior choroida l artery ;
m-
I, origin
of
M-I
ar
tery;
a-
I, origin
of A-J
artery;lUl,
artery
of
Heubner;
01,
optic tract;
2,
optic nerve;
ac,
anterior clinoid process;
pc,
posterior clinoid pro
cess;
te,
tentorial edge;
),
oculomotor nerve. From
Fox (2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 115/213
Anatomy
109
Fig.
6.14.
Same case as Fig. 6. 13 with probe
(pr)
dis
placing carotid artery medially.
Crossed arrow,
site
of
anterior thalam ic perforators from posteriOl· com-
""'
\
municating artery;
01,
optic tract;
pc,
posterior
clinoid process;
p-J,
P
-l
artery; 3, oculomotor nerve;
unc, uncus;p-2, P-2 artery.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 116/213
110
6.
Th
e Carot id Cistern and Environs
Fig.
6.15 . Ex
ample of prcaneur
ys
mal
type
of infu n
dibulum
(cro
SM
d
af7"ow) of posterior communi
ca
ting
artery
(pea).
perf. Anterior thalamic pe rfor.uors;
adm,
aillcrior choroidal anc )';
V,
vein;
a-l,
A-I ar
tery;
Qt,
OPlic tract;
fl-rt/,
frama l lobe retractor;
pro
pr
obe retracting carotid artcl1'i Pit, pituitary stalk; 2,
optic nc n'c;llC, anlc rior di no id process; un, inte
rna
l
ca rotid artery;
Ie,
tentorial edge;
pc.
postcriordinoid
pr
ocess; J, ocul omotor Ilcn'c; II-rei, temporal lobe rc
tractor. From
,"ox
[2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 117/213
Anatomy
I
II
mom
Fig.
6.16.
Carotid cistern after bipolar eleclrocoagu·
lalion of aneurysm
(an)
with ad hesions
(ad)
to
oculomotor nerve
(3)
and uncus
(unc) of
tcmporal
lobe.
col,
Cottono
id
s;
mem,
membrane of Li liequist
oot
(or Kcy
an
d Retzius); ac, autc
rior cl
inoid proccss;
ica,
internal carotid artery;
pc,
posterior clinoid process;
pea, origin of postcl'ior communicating artcr
y.
From
Fox [2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 118/213
112
6.
Th e Carotid Cistern and Environs
Fig.
6.17.
Anatomy
of
carotid cistern
and
environs.
Arachnoid membrane of
Lili
eq
ui
sl(mem) is we ll seen
deep to
and
between the internal carotid artery
(ica)
and oculomotor nerve (3). Crossed arrow, anterior
choro idal
arte
ry;
IInc,
uncus; m·l, origin
of
M
-l
ar
tcr),; an, base of aneurysm at bifurcation of ca rotid
artery; a-1, righ t A-I al "ter}';
a-a,j
unction
of
ri ght A-I
and unseen right
A-2
and ante
ri
or communicating
(aea) arteries; gr, right gyrus rectu
s; perf,
perforators
from anterior communicating artery;
hr,
bridging ar
tcry from anterior comm
un ica
ting artery to
left A-2
artery (connection out of view);
a-2, Icrt
A-2 artery;
2, optic nerves;
ch.
optic chiasm; ft, lamina termi nalis;
ot
,
right opt ic tract;
a
c, ante
ri
or clinoid process;
ds,
diaphragm sel lae;
pc,
posterior clinoid process; pea,
post
erior
communicating artery.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 119/213
Anatomy
11
3
Fig. 6.18 . Sa me case as Fig. 6.17. Upper in ternal
carotid artery (ica) and the
M-
I origin (m-
/)
are re
tracted by a probe (pr) to \'iew perforators (crossed ar
rows) and optic tract
(ot)
behind aneur
ys
m
(an)
and
bifurcation
of
carotid artery.
pea, Po
sterior
COIll-
municating artery; -UIIC. uncus; acha, anteri
or
choroi
dal artery;s, suction lube;
perf.
perforators;00, recur
r
em
artery
of Heubner;jl
, frontal lobe;
a-I,
A-I
ar
ter
y; Ma.
anterior communicating artery;
it,
lamina
termina
lis.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 120/213
114
6. The Carotid Cislern and Envi
ro
ns
Fig.
6.19. Ano th er case with view of carOlid
ci
stern
and e nvi rons, looking morc medially. Appearing deep
between
ri
ght internal carotid artery
(
r-iea) and o ptic
apparatus a re seen perforators (peif). pituitary stalk
(Pit),
right posterior clinoid process
(PC),
lOp of lhe
dor
sum se
ll
ae (ds), left
superior
cerebellar artery (l
sell),
and
left oculomotor nerve (3). Lateral to the
right carotid artery 3rc noted the tentorial edge (te ),
side of the
dor
s
um
sellae
(ds),
a
dural
ve
nous
si
nus
(us)
be
hi
nd the dorsum sellae, the posterior com
municating artery
(pea)
and
its
adjacent aneurysm
(crosud arrow),
the P-2 artery
(p.2).
basilar artery
(00),
and right oculomotor l
en'c
(3). 2, Optic nerves; ch,
optic chiasm; 01,
right
optic tract;foo. right (bottom)
and l
ef
t (toP) fronto-orbital
arterie
s;gr, right (bottom)
and left
(lOP)
gyri recti; l-ita, med ia l side of left inter
nal carotid artery; a.-I,
A-
I arte ry_

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 121/213
Anatomy 11
5
Hg
. 6.20. Same case as
Fig
.
6.19
emphasizing r
eo
lationship
of
intcrnal carotid artc ry (ica) and pos
teri
or
cl inoid proccss
(PC). Ids.
Top of dorsum se
lla
c
covcrcd bydura ;fds, front ofdOT5um
seU
ae;sds. side
of dOT5u m
se
llae; vs, vcnous sinus in dura behind
dOT5u
m se
ll
ae;
J,
oculomotor ncrve;
col,
cottonoid
s;
P01l
S, rostral pons;
se
a, right superior cerebell
ar
ar
tery be hind 3rd ncrvc;p-2. P·2 artcry
in
front
of3rd
ner
ve; une,
uncu
s;a
1l
. second ane
urys
m at tak
eo
ff of
anterior choroidal arlery (hidden);
CTossed
arrow, first
aneur
ys
m at takeoff of posterior co mmunicating ar
tcry (hidden); rtf, right temporal lobe re t
ra
ctor;
m·J,
M- I arte
ry
o
rigi
n;
00,
bas il
ar
artery;
Iry,
hypophyseal
perf
or
ator from ica;
a-I,
A-I arter
y; 01,
optic trac
t.
Note Icft lateral m
edu
llary per
fo
rator from basil
ar
;lrtC
I
),
and
in
shadows behind d
or
sum s
ell
ae.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 122/213
116
6. The Carotid Cistern and Environs
,.,
Fi
g. 6.21. Ano ther case illu.nra ting sympathetic fi·
bers (5)'"') on internal carotid artery (ica). ar (]
alen
]),
Arachnoid band ; Ie , tcnlorial edge; an, aneu rysm
at
takeoff
of
[.N)Sterior commun ica ting artery (hidden:
most
of
aneurysm is below lc
nlo
rium);cot, cottonoid:
Il t, frontal lobe rclrdctQr; ar (medial), arachnoid
membrane between optic nerves; 2, right optic
ncn'c;
mem,
membrane of Li liequist;
ac,
anterior
clino id process. Fro m Fox [ I].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 123/213
Anatomy
117
Fig. 6.22. Another tase showing
view of
medial side
of
opposite
(kfl)
carotid cistern. reI, Retractor on
right frontal lobe
(fl); ch,
optic chi
as
m; 2, both optic
nerves;
cot,
cotton ball; clp, shank of aneurysm
cl
ip;
ac, right anterior clinoid process;
ar,
arachnoid fi-
bers;
1.5,
tuberculum sellae;
unc,
medial side
of
left
uneus;foa, left fronto-orbital artery on left frontal
lobe;
m-I,
origin
oflef
t
M-
I artery; v. vein;
ica,
left in
ternal carotid artery (medial side near bifurcation);
a- I, origin
ofle
ft A-I artery.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 124/213
liS
6. The
Carotid Cistern and Environs
Fig.
6.23. Another case with
vi
ew
of
carotid and
chiasmatic cistern
s.
The pituitary g land (pit) projects
superior to
the
level of
the
diaphragm sellae.
Sing/to
crossed arrow,
portal veins of pituitary stalk ; 2, optic
nerves; ell, optic chiasm; r-ica,
right
internal carotid
arter
y;
hy, hypothalamic perforators from internal
carotid artery; pc. dura
of
posterior clinoid process;
mem
o
membrane
of Liliequist; v, unusual
vei
n a
ri
s
in
g
from cav
ernou
s sinus; double-crossed arrow, posterior
communicating a
rt
ery; aella,
one
of two alllerior
choroidal arteries;t l-ret, temporal lobe retractor ;
111-1,
M- l pordon
of
middle cerebral artery;
fmi,
per
forators from bifurcation
of jea to
alllcrior perfo
rated substance; ot, right optic tract; a-I, A-I portion
of
anterior cerebra 1artery;fl-rel, fro mal lobe retrac
tor; l-ica, left
imernal
carotid arter
y;
l-pea, left po
s
terior communicating artery. From Fox [2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 125/213
Anatomy
119
Fig. 6.24. Some case as Fig. 6.23. View is looking me
dia
ll
y
tow ar
d the le
ft
inte
rn
al
Gl.r
otid artery
(i-ica). 2,
Optic nerves;
Pit,
pituitary
st.a
lk; l-pea, left posterior
communicati
ng ar
tery;
ch,
optic ch iasm; a-1
, A-
I por
tion
of
left anterior
cere
bral artery;
cot,
COtton strip;
1/j.-1, M-l portion of left middle cerebral artery;jl-ret,
frontal lobe retractor; v,
unu
sual vein
on
left arising
from cavernous sinus; pr, probe retracting the vein;
cr
ossed
arrow, medial left tempora llobc. , 'rom Fox [2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 126/213
1
20
6.
The Caro
tid Cistern and Environs
Fig. 6.25. Another case illustrating internal carotid
artery (ita)
and
environs.
pc,
Posterior clinoid p ro
cess;
an,
giant aneurysm of right P·1 artery;
tl,
right
tem poral lobe; mol, M-I artery;
a-i,
A-I artery; ret, re
tractor on frollla lobe;a-2, right
A-2
ar tery;gr, gy
ru
s
rectus;
am,
anterior communicating artery;
2,
optic
nerves; ch, optic chiasm;
sha,
superior hypophyseal
artery;
crossed
arrow,
one
of several hypophyseal and
anterior thalamic per fo rators in an arachnoid
shea th;
Qt,
optic trac
t.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 127/213
Anatomy
121
Fig. 6.26. Same case as
Fig.
6.25. Probe
(pr) is
retract
ing right optic
ne n
·c (2) mcdia lly to show pituitary
stalk
(pit). pc ,
Posterior
cl
inoid proces
s; all.
giant
ancurys
m;
te,
telltorial edge;
UIIC,
uncus;
),
oculomOlOr
llen
'c; I'll, temporal lobe retractor; bif,
bifurcation
of
right internal carotid artery.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 128/213
7
The
Chiasmatic Cistern
and
Environs
Introduction
As
the s
ur
geon d issects media
ll
y from the ptcr
iona l exposure, he or she encounters a conflu
ence of cistern s
in
the ccnt
er of
which is the
chiasmatic cist
ern
. T he computed tomography
(CT) scans with cerebral spinal fl uid (CSF) con
trast enh ancement show the ch iasmatic cistern
and
adjacent cisterns (Figs. 7. 1
and
7.2).
The
ca rotid cisterns are lateral, the cistern of the
Fi
g. 7.
1.
Axial \·icw
of
CT scan after injection
of
iopamidol into the CSF
by
lumbar puncture: cister
nogram of chiasmatic cistern containing
op
tic
chiasm (black
arrowhead) and
medial poI-lions
of
optic
nerve.
Closed black
arrow crosses ant.el-im-clinoid pro
cess and poin ts to lateral portion of optic nerve in
carotid cistern; open arrow lies
in
confluence of
upper
lamina
ter
minalis is behind and above, and the
olfac tory cisterns pass anterior to the chi
as
mat
ic cistern. T he o lfactory ci
stern
lies
be
tween the gyrus rectus and medial
orb
ital
gyrus. In the mid line between the fronta l lobes
is the perica llosai cis t
ern and
interhemispher ic
fiss
ur
e (cistern).
carotid cistern with med ial chiasmatic cistern from
wh ich arter
ial
shad ows of A-I (mediall
y)
and M-I
(laterally) can be seen 10 originate; white arrow points
to optic tract lyi
ng
lateral to the laleral portion
of
the
cistern of the lamina terminalis and medial to the
confluence of the two cisterns (ca rotid and sylv ian);
while triangle lies
on
lamina termi nalis.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 129/213
124
7. The Chiasmatic Cistern and Environs
Fig.
7.2. Coronal (fromal) view
of
CT scan after in
jection of iopamidol into the CSF by lumbar
punctu re: cistcrnogram of olfactory cistern. Black ar
ruws
lie
in
olfactory cistern and poim to olfaClory
tracts; while triangle,
gy
ru s
rec
tu s; while dosed arrow,
Anatomy
As
the surgeon elevates the frontal lobe, the ol
fa
ctory tract m
ay be
stretched
if
the brain is
vcry rel
axed
.
If
this ha
ppen
s,
vei
ns n
ea
r the
midline
and
trav
er
s
in
g bcnveen the frontal
lobe (gyrus rectus or adjace
nt
medial orbital
gy
ru
s)
and nearby dural
si
nuses
may lear
and
bleed . When such occurs,
it
w
ill be
necessary to
expose the olfactory cist
ern
(
Fig
s.
7.3
and
7.4)
.
This maneuver is not necessary unle
ss
bleed
in
g occurs, req
ui
ring bipolar elec trocoag
ul
a
tion
of
these
ve
in
s.
The
olfactory tract appears
as
a white band
lying in the olfactory cistern. P
os
teriorly, it
arises from the medial and lateral olfactory
stria , forming the
from border
of
the anterior
perforated substance.
Th
e tract is
adherent
to
the froma
llobc
between the gyrus rectus (me
dially) and the medial orbital gyrus (laterally).
further anteriorly the olfactory tract se parates
from the brain (figs.
7.2
and
7.5)
and passes to
ward the olfactory bu lb lateral to the crista ga
lli
(Fig. 7.6). From this olfactory bulb pass the hid
den fil aments of the olfactory nerves d
ow
n
th
roug
h the cribiform plate and into the mu
cosa
of
the nose.
As
the dissection proceeds medially from
branch of anterior cerebral artery in
int
erhemis
pheric
fiss
ure;
open arrow, co nt
rast medium in sub·
arachno id space (optic cistern) surrounding optic
nerve
in
orbit.
the carotid cistern
and
into the chiasmatic
cis
tern toward the
anterior
communicatin g com
pl ex, the surgeon m
ay
fo ll
ow
the A- I
ar
tery ifit
is eas ily seen.
Th
is usua
ll
y occurs if the internal
carotid artery
is
fairly short.
In
cases where the
internal carotid a rtery
is
long and the
A-
I ar
tery is hidden
po
steriorl
y,
the s
urg
eon shou
ld
avoid retraction
of
the frontal lobe to expose
the A- I artery. If an anterior communicating
artery
aneurys
m is the target. the ap proach is
then
di r
ec
tl
y through the gyrus rectus [2-4].
The landm
ar
ks for the I-cm incision in the
gy
ru
s rectus are illustrated in Figs.
7.7
and
7.8.
The
tr iangular or
quadran
gu l
ar
zone inferior
and lateral to the franta-orbita l artery lying on
the gyrus rectus is described in the legends f
or
the
se
figures.
I f the
sy
lvian fissure has been widely
opened, elevati
on of
the frontal lobe
will
bring
the optic c
hi
asm,
op t
ic tract,
and
lamina ter
minalis (be
twe
en the
opt
ic trac
ts)
into vi
ew in
cases with a prefixed optic c
hi
asm (ie, sh
ort
opt ic
ner
ves intracran ia
lly).
Figures 7.9and
7.10
are t
wo
examples
of
a prefixed chiasm.
The
lamina termina
li
s a
ppear
s as a thin, translu
cent membrane retain in g third ventricul
ar
CS
F inside. The CSF on its outer, visible side
li
es in the cistern of the lamina terminal is ,

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 130/213
Anatomy
125
which contains the medial portion
of
the A- I
arteries, their interconnecting anterior com
municating artery, and the recurrent artery
of
Heubner (Figs. 7.10-7.12). The cistern
of
the
lamina ter minalis merges with the chiasmatic
cistern be low and anteriorly and with the in
terhe mi spheric
fiss
ure (
ci
stern ) superiorl
y.
Laterall
y,
the cistern of the lamina termina lis
merges with the confluence
of
the sy lvian and
carotid cisterns lateral to the optic tract.
Figures 7.13 and 7.14 are intraoperative
photographs
of
the sa me patient. In I-ig
ure 7.13 we see through the right carotid
cis
tern and the lam in a te rminal is and ch iasmatic
cistern s into the left (o pposite) carotid cistern.
The
tented lamina tenninalis is prominent.
Th
e medi al s
id
e
of
the left internal carotid ar
tery is seen superior and inferior to the image
of the l
ef
t optic nerve.
The
left posterior com
municating artery is visualized deep to the
pituitary stalk. Pani cularly important are the
hypophyseal perforators from the carot
id
a
r
teries. If the
A-
I arteries are
fo ll
owed medially
and
superiorly, the anterior communicating ar
tery is seen lying in the cistern above and an
terior to the tented-
up
lamina terminalis
(Fig. 7. 14).
Figures 715 through 7. 18 are four exam
pl
es
of
variations in the anatomy
of
the chiasmatic
and lamina t
er
minalis cisterns. In each case the
inferoanterior zone o f the lamina terminalis
is
visua
lize
d . In
Figs.
7. 15
an
d 7. 16 the r ight lateral
margin
of
the pituitary stalk is see
n.
This pitu
itary stalk , along
wi
th the optic nerves and
chiasm,
li
es
in
the chi asmatic cistern (bounded
caudally
by
the arachnoid membrane of
Lili
equist). Howeve r,
in
many cases the mem
brane
of
Liliequist, which lies caudal to the
pituitary stalk, sends an ante
ri
or reflection of
arachnoid membrane in front of the pituitary
stalk .
Th
is situation puts the pituitary stalk in
side
it
s ow n hypophyseal cistern (Fig. 7.16). In
l'ig.
7.16
note
that
the frontal lobe retraction
is
stre tching arachnoid bands at the lateral mar
g
in of
the cistem
of
the lamina terminalis.
Figu res 7.1 7 and 7.18 additionally illustrate
the many
va
riations in the pathway
of
the recur
rent
artery of Heubner. Generall
y,
this artery
a
ri
ses from the A-I artery
or
the A-2
ar
tery
near the a nterior communicating ar tery (refer
to Fig. 7.40). There may
be
two arteries of
Heubner
on one
s
id
e.
The
artery passes later+
a
ll
y and lies super ior to and behind
or
in front
of
the
A-I
and medial
or
igi n
of
the
M-
) arteries
and se nds branches into the anterior perfo
rated substance.
Fr
equently the
anery
o f
Heubner is seen before the
A-
I artery is
id
en+
tified, and it may bequite large (as in Fig . 7.11
).
Fi
gures
7.19
and
7.20
are photographs
of
the
same patient before and after p
er
foration
of
the lamina terminalis to treat hydrocephalu s.
One
of
the many variations in the anteriorcom
municating artery complex inside the lamina
terminalis cistern is shown here. Such vari
at ions, with dupl ica tions and cross-bridges, are
common (refer to Fig. 7.39).
Th
is is a tripli
cated anterior communicting artery complex
with a bridge between two
of
the arteries.
The
ar tery
of
Heubner is we
ll
see
n.
Figures 7.2 1 through 7.24 demonstrate two
patien
ts
in whom the artery of Heubner is the
sa
me diameter as the A- I artery (Figs. 7.21 and
7.22)
or
larger than the A- I artery (Figs. 7.23
and 7.24) . In Fig. 7.21, the A- I a rtery
is
almost
t
.. .::
si
ze of
an adjacent large M-I
perforator
,
and the
M-
I artery is equal
in
si
ze
to the inter
nal
cal"Otid
artery. In Fig. 7.22 the pituitary
stalk
is
surrounded
by
arachnoid (
Lili
equist's
membrane behind and an anterior reflection
of the same membrane
in
front). Hence the
pituitary struc
tu r
es are 111 their own cistern
(hypophyseal cistern).
The same is tru e
In
another patient
(Fig.
7.23)
where pa
rt
of
the anterior ar achnoid
enclosing this ciste
rn
has been opened by the
surgeon.
Th
e pituitary sta
lk
is redd ish due to
the marked arte rial and portal
ve
nous vascul ar+
ity (which partly accounts for i
ts
enhancement
on
CT
scans with contrast medium).
Fi
g
ure 7.24 in the sa me patient shows a
ve
ry
hypoplastic right A-I artery and a large right
artery of Heubner. Ad ditional anomalies are
the low takeoffof the frontopolar arteries.
The
large left A- I artery supplies this unusual an
terior commu nicating complex. Because the
anterior communicating a rtery is lifted
up
by
an ane
ur
ysm
in
the cistern
of
the lamina tel'
minali
s,
descending "hypothalami
c"
per
forators are well shown .
Figure 7.25 is an example
of
a pa tient wi th a
pr
efixed chiasm and
short
internal carot
id
ar
teries. Without the sur geon go in g through the
gy ru s rectus, the right A- I, anterior com
mun icating, and left A- I
arter
i
es
are seen upon
elevation of the frontal lobe. Im
ponan
t per
forators from the right A- I a rtery to the right
optic tract, chiasm, and nerve are seen.
I-i
gure
7.26 also is a photograph
of
a shon internal

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 131/213
126
7. The
Ch
ia
smatic Cistern
and
Environs
Thble
7.1. Structur
es
contained within the chiasmatic cistern '.
I. Optic chiasm
2.
Optic ner\'es. medial borde r
3.
Surface of the gyrus rectus of the frontal lobe
4.
Tuberculum sellae (dural covering)
5. Arachnoid membrane of Liliequist (Key and Retzills), rostral surface
6. Arachnoid between optic
neTl
'
es
i. Superior hypophyseal artery
8. Hypothalamic perforators
9.
A portion of the fronto-orbital artery
10. Pituitary stalk (often lies within its own cistern)
Items
2-5
can be considered to form portions
of
the margins of the chias
matic cistern.
Table 7.2. Struc
tur
es contained ... ithin the lamina terminalis cistern' .
I. Outer surface of the lamina terminalis
2. Surface of the optic tracts
3. Surface
oflhe gy
r
us
rectus of the frontal lobe
4. Anteriorcommunicatingartery
5. Anterior cerebral artery, A-I portion
6.
Anterior cerebral artery, origin
of A-2
portion
7. Origin of the fronto-orbital artery
8. Artery of Heubner, proximal portion
9. Hypothalamic perforators from A-I and anterior communi catinganeri
es
1
0. St.r
ia thalamic perforators from the A-I arte ry
II . Origin of an occasional accessory anterio r ce re
br
al
artery
• Items 1-3 can be considered to form portions of the margins of the lamina
terminalis cistern.
carotid artery and a prefixed chi asm . An un
usual arterial anomaly is also illustrated: the ar
tery of Heubner and the frolltopolar artery
arise from a common trunk.
Thi
s arterial
trunk origi nates at the right A- IIA-2 arterial
junction. Branches from the ascend in g fron
topolar artery suppl y the territory
of
the ab
sent franta-orbital arte ry.
Fig
ur
es
7.27
th rough 7. 30 reveal a common
variation in the amerior communica ting artery
complex. In Figs.
7.27
through 7.29 the an
terior communica ting artery forms a "Y" with
one
limb on the right and two limbs
on
the left.
the superior
one
anastomosing higher
up on
the left A-2 arter
y.
In
Fig.
7.30 the anterior
communicating artery is duplica ted ; the
superior one is hidden by a layer
of ar
achnoid.
Fi
gures 7.31 and 7.32 illustrate another
example of a V-shaped ante rior communicat
ing
ar
tery with the common trunk on the right
and the two limbs on the lefl. Additiona
ll
y a
large per foralor and an accessory amerior
cerebral artery (a third, midline A-2 artery)
arise at the division
of
this Vs haped anterior
communicating arte ry.
The common ly dup
li
ca ted anterior com
municating ar tery again is seen in Fig. 7. 33. Fi
g
ure
7.34
sho
ws th
e
und
erside
of
an
anter
i
or
communica ti ng artery and nearby perfo rator
s.
Th
e optic tract is rarely well seen unle
ss
the
sy lvian fiss ure has been opened. Figures 7.35
through 7.38
are
examples i
ll
ustrating this
tract in two patients. I n fi gure 7.35 the origin
of
an accessory anterior cerebral artery is seen
(sometimes mistaken for the base of an
aneurys m) . Figure 7.36 (sa me patient) isa more
magnified
view of
the lamina terminalis seen
between a large arte ry o f Heubner and the A- I
ane
ry. A l
arg
e
ve
in
turns posteriorly and pa
ss
es along with the optic tract to join the unseen
basilar
ve
in
of
Ro senthal.
Fi
gures
7.37 an
d 7.38 are
tw
O views
of
the
right optic t ract and chiasm.
Th
e
A-
I arteries
join the anterior communicating artery
we ll
above the lamina terminalis, and the left A- I ar
tery has an unusual bridging
arter
y returning
back to the le ft A-I. Note the arachnoid band
(compare with th
at in Fig.
7. 16) over the rig
ht
A-I ar tery at the lateral border
of
the cistern
of
the lamina terminalis. Tables 7.1 and 7.2 sum-

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 132/213
AnalOmy
127
marize the various stru ctures found in the
chi asmatic and lamina terminalis cisterns.
The
duplications and bridges
of
ten seen as
the anterior communicating artery complex
were illustrated by Bremer [1] in 1943
(Fig. 7.39).
But it
was
only with routine use
of
the
ope
rating m
ic
roscope th
at
surgeons saw
how commonl y such
va ri
ations occurred.
Fig
ure 7.40 is Westberg's representation of the
usual course of the recurrent artery
of
Heubner [5]. This large perforator
se
nds
branches illlo the anterior perforated sub
stance along with the stria thalamic perforators
from the A- I and M- l arteries.
Bibliogr
ap
hy
I.
Bremer J L (1943) Congen ital aneurysms
of
the
cerebral arteries. An embryologic study. Arch
Pathol35: 8 9 ~ 8
2. Fox J L (1979) Microsurgical expos
ur
e
of
intracra
n
ia
l ane
ur
ysms. J Microsurg
I: 2-
31
3. Fox J L ( 1983) Intracranial Aneurysms,
vol
2. New
York , Springcr-Vc
rl
ag, pp 877 -
1069
4. Kempe LG (1968) Operative
Neurosurgery, vol
I : Cra
nial,
Cerebral,
ami Intracranial Vascular Disease. New
York, Springer-Verlag, pp 1- 75
5. Westberg G
(196
3) The recurrent artery of
Heubner and the arteries of the central ga ng lia.
Acta Radiol (Diagn) 1:
949-954

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 133/213
128
7. The
Chiasmatic Cistern
and
Environs
'0'
Fi
g. 7.3. Lowe r portion of olfactory tract (1). gr,
Gyrus rcclus;2, right optic nerve;dura, dural margin
of optic canal;
ar,
arachnoid covering internal
carotid artery (carotid cistern);
ac,
anterior clinoid
process;
v,
vein on
temporallobe;
s,
Sliction
lube;
ret,
retractor on frontal lobe.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 134/213
Anatomy
1
29
Fig.
7.4.
Same case as
Fig. 7.3
. Midd
le
portion
of
right olfactory tract
(1)
in olfactory cistern. V, Vein in
sulcus bet
wee
n frontal lobe
(jT)
and olfactory tract;
dura,
dura
coveri
ng
orbital roof (floor
of
anterior
fossa) projections;
nt,
retractor on frontal lobe.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 135/213
130
7. The
Chiasmatic Cistern and Environs
Fig. 7.5. Same case showing olfactory tract
(1)
pass
in
g through subarachn
oi
d space from frontal lobe
(jl)
toward cribiform plate and nose. v, Vein;
a,
ar
tery;cg, dura
of
crista galli.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 136/213
Anatomy 131
Fig. 7.6.
Another case demonstrating olfactory bulb
(ob)
and upper olfactory tract (I). cg, Crista ga
lli
;
ret,
retractor;jZ, base
of
frontal lobe ;dura,
dura
covering
orbital roof projections.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 137/213
132
7. The Chiasmatic Cistern and Environs
Fig. 7.7. Initial exposure of gyrus rectus (gr) during
an approach to an amerior communicating artery
aneur
ysm
where the A-I artery
is
not followed me
dially. Note the quadrangular zone bounded
by
the
edge of the frontal lobe retractor blade (jl
-
ret), the
fTOlllo-orbital a
rt
ery
fjo),
the frontallobe/optic nerve
junction (dQuble-crossed arrow), and the olfactory tract
(/). T he incision in the gyrus
rcelusis
made here and
the fronto-orbital artery is followed to the aneurysm.
v, Vein;
ar,
arachnoid between optic nerves; 2, ri gln
optic nerve;
ica,
interna l carotid artery;
Ie,
ant
er
i
or
reflection of tentorial edge; Ii , temporallobc; II/em,
membrane of Lili equ isl; cot, cotton st rip lying on syl
vian fissure. From Fox [3].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 138/213
AnaLOmy
1
33
Ag.7.8. Another case illustrating the initial expo
sure of gyrus rectus on the right
(r-gr)
where the
right
A-I anery
(a-I, hottom) is
fo
llowed medi
ally.
Crossed arrow, interhemi spheric fissure. Note quad
rangular zone oounded
by
the frontal lobe
and
right
A-I
j unction, the olfaclOry tract (/) , the front.allobc
retractor blade (jI-ret), an d the f "OO lo-orbital artery
I/o). The initial incision
is
made within this zone. r-gr,
Right gyrus rectus; lIa, left artel-Y of Heubncr; i-gr,
medial surface
of
left gyrus rct:lus; i-10, left fronlo
orbital artery; aT, arach noid between optic nerves; 2,
le ft
and
right optic nerves; Ii, temporallobc;
ch,
optic
chiasm;it, lamina terminalis;o/, right optic tract;mca,
branch
of
middle cerebral aner}, in sy lvian fissure;
a-l, left (toP) and right
(hoI/om)
A-I arteries converg
ing lOward the hidden anlerior communicating ar·
ter y. From
Fox
[3J.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 139/213
1
34
7. The Chiasmatic Cistern and Environs
Fig. 7.9. Another case
ill
ustrating prefixed optic
chiasm (ch). Lamina terminalis (it) and i
ts
cistern be·
tween the
op
t
ic
tracts
(ot) arc
seen. With
in
the cistern
oft
be lami na terminalis is pari of the
A-
I ane
ry(a-J)
and a duplicated amerior communica ting artery
(aca). ar, Arachnoid between optic nerves (2); ica, in
terna
l carotid
arte
r
y; ac, anterio r dinoid
process;
pc,
poste rior clinoid process; »Mm, arachnoid mem
brane of Liliequist; te, tentorial edge; ata, anterior
temporal ar tery; It, temporal lobe; hij, bifurcation of
iea; tUmble-crossed arrow, origin of hidd
en anter
ior
choroidal artery;
single-crossed arrow,
origin of hid
den
posterior communicating artery;
/w.,
artery of
Heubner.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 140/213
Anatomy 135
Fig. 7.
10.
Another case
with
prefixed chiasm
(ch)
and
short intracran
ia
l optic nerves (2). T he carotid,
chiasmatic, and lamina terminalis cisterns appear
here without identifiable boundaries after dissec·
' .
tion.
ica,
Imernal carotid artery;
Ii.
temporal lobe;
a·l,
A·I
ar
tery;
Ia,
artery
of
Heubner;j1, frontal
lobe;
1$,
tuberculum
se ll
ae;
it,
lamina terminal
is; ot,
optic tract. From Fox [2).

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 141/213
136
7. The Chiasmatic Cistern
and
Environs
Fig. 7.11. Same case as
Fig.
7.10. A short imernal
carotid artery has permitted exposure of the an
terior communicating arte ry (aca) by following the
right A- I artery
(a-I,
bottom).
The
upper chiasmatic
cistern and
the
cistern of
the
lamina tcrminalis are
exposed.
ch,
optic chiasm; It, lamina terminalis;
ot,
optic tract; ha, right (bottom) and left (toP) arteries of
Hcubner; gr,
right
gyrus rectus; a-J
(lOP),
left A-I ar
terYi/o, left [ront()-orbital artery
on
left gyrus reclus.
From
Fox
[2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 142/213
Anatomy 137
Fig. 7.12.
Same case after removing about I·em
length
of gy
rus rectus to expose an anterior com
mun icating artery aneurysm
(an)
surrounded
by
left
(lap) and riglll
(bottom)
A
-2
arteries
(a-2).
Above are
the left and below are the right
A-
I arteries
(a-I),
ar-
teries
of
Heubner
(ha),
and fr
orlLO-orbita
l arteries
1/0).//,
Lamina lerminatis;gr, teft gyrus rectus. These
st ructures l
ie
within the lamina terminalis and in
terhem ispheric cisterns. From Fox
[2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 143/213
13
8
7. Th
e Chiasmatic Cistern and Environs
Fig. 7.13. Another
case with expos
ur
e of a ll the an
terior cisterns bounded by the left
and
ri ght tem
poral lobes
(l-Il, r-el).
s, Suction tube above bifurca
tion
oflef
t internal
ca
rot id
ar
tery
(l-ica); (1- 1,
both A-I
arteries; ii, lamina terminal is; ot, ri ght optic tract;fl.
right frontal
lo
be; 2, both oplic nerve s; ky. left and
right hy
poph
yseal perf
or
ators; Pit, pituitary stalk
(a nd its hypoph
yse al
cistern) surrounded by
arachnoid (ar), which splits and surround s it; pc,
posterior clinoid process; mem, membrane of
Li liequist;
l-ica and
r-ica, both internal carotid ar
terie
s;l-pca
and r-pea,
both posterior communicating
an erie
s. The
left one
(i-pea)
lies in fro
Ol of
Liliequist
membrane and is seen through the s
pa
ce between
the pituitary stalk (pit) and [he rig ht carotid artery
(r-ica).
From Fox [3].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 144/213
Anatomy 139
fl ret
Fig.
7.14.
Same case after exposure ofrwo aneurysms
(an) on the anterior communicating artery.
The
small one projecting upward is obvious.
Th
e large
one projects downward and is hidden
by
the anterior
communicating artery
(aca). Above
and below arc
the left and right A-I arteries (a-I) and A-2 arteries
Olf
-l
(
(a-2) . 111.
left frontal lobe,
Lt,
lamina terminalis,
01,
right optic tract; bif, bifurcation
of
right internal
carotid artery;
col.
couonoid;
JUl,
ri
ght ar
tery
of
Heubner; fl-ret, right frontal lobe retractor. From
Fox
[3].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 145/213
140
7. The Chiasmatic Cistern and Environs
Fig. 7.
15. Another case
showing chiasmatic cistern
both rostral
and
abo\'c (to observer's left)
and
caudal
and behind (to observer 's right) the optic ap paratus.
$, Suction
tube
; l-fl, left frontal lobe; ar, arachnoid be·
tween left oplie nerve and frontal lobe and separat
ing
left
carotid cistern from c
hi
as
matic cistern;
2.
bolh optic nerves;
fo,
left fronto-orbital anc l
} '; ha,
l
ef
t arteries of H
cub
ncr;
ell,
optic chiasm;
01,
right
op
tic tract;
ac,
right anterior clinoid process; Pit,
pituitary gland projecting above (with
rc
spca
to
pa
liem) sella lUl'eica; ita, inte
rn
al carmid artery;
frs,
pituitar y stalk; ft, lamina term in alis;
rei, rctractoron
right fromal lobe; an, aneurysm ar ising from an
terior commun ica ting artery;
a-I
and a-2, left (toP)
and right (bol/om)
A-
I and A-2 artcrics:fp, low .akrofr
of le n f
ro lH
opo l
ar
artcr)';col, sma ll coHon hall.
Fr
om
Fox
[3}.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 146/213
Anatomy
14 1
Fig. 7.16. Anoth
er
case sh
ow
ing surgica lly induced
commun ica tion between chi asmatic cistern rostra
ll
y
and interpeduncular ciste
rn
caudall y. T he latler con
tains the basilar ar tery
(ha)
seen after opening the
membrane of Liliequisl (mem). Note Li liequist's
membrane
se
nds an ant
er
ior reflection around
pi tuitary sta lk (pit), th
us
enclosing the hypophysea l
ciste
rn
. Double-crossed arrow, reflections of light from
CS
F in int
erpe
duncul
ar
cistern;
ji"gle-crossed
an-ow.
lies on sho
rt
internal carotid ar tery
and
points 10 ori
gin of posterior communicating artery; /l-ret, tem
poral lobe retractor ; m·}, M- I arter
y;
perf, largest of
several perforatOrs from A-I ar tery (a-1); ot, right
op
tic tract;
ar,
arachnoid ba nds at lateral margin of
cistern
of
the lamina tennina l
is;
fl, lamina termina l
is
(covered by A- I artery);j1-rel, frontal lobe retractor;
ell,
optic chiasm; 2, both optic nerves; ac, anterior
cl
inoid process.
FrOIll Fox [2]
.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 147/213
142
7. The Chiasmat
ic
Cistern and Environs
Fig. 7.17
. An
other
examp
le of structures in chiasmat·
ic , carotid, and lamina lerminalis cisterns. 2, both
optic nerves; ch,
op
tic chiasm; ii, lamina terminalis;
Q/,
right
optic tract; ac,
ailler
ior clinoid process;
d()U
ble-cro5Sed
arrow, origin
of
posterior communicating
artery from internal carotid artery;
)/1--/,
M-l artery;
perf, perforator from A-I artery (a-I); ha, artery of
Heubner;fo, franto-orbital artery;
rei,
retractor on
frontallobe;sillgle-crossedarrow, interhem ispheric fis
sure; gr, left gyrus rectus.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 148/213
Anatomy
143
Fig. 7.18. Another example
of
the lamina terminal is
(It). A bi lobed anterior communicating artery
ane urysm (an) is surrounded by the lert
A-2
artery
(a-2,
loP),
the anterior communicating artery
(aca),
and the
ri
ght
A-2
artery (a-2, boltom). Th
e
termina
tion
of
the lert A-I artery (a-I,
toP) is
see
n.
2, both
op
tic nerves; ell, optic chiasm;
ot,
right optic tract;a-I
(bottom), right A- I artery;ha, artery
of
Heubner; r-[o,
right fronto-o rbi tal artery;Jl, right frontal lobe;
ret,
retractors; V,
vei
n on lert gyrus rectus (gr); l-fo, left
fronto-orbital artery.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 149/213
144
7.
The
Chiasmatic Cistern and Environs
Fig. 7,19 . Another case illustrating lamina tcrminalis
(ll),
its
cistern, and a variati
on
of the anterior com
municating complex with 3 arteries
(uca)
and a
bridge (brl between 2
of
them. a-I,
Left
(lOP) and
right (bollom) A- I arteries; eh, optic chiasm; ot, right
optic tract; single-crossed arrow, origin
of
posterior
commu nicating artery:
douhle-crrused arrow,
origin of
anterior
choroidal artery; mol, M-I artery;
v,
vein; r-
JUl,
ri
ght artery of
Hcubncr;
ju,junction of anterior
communicating artery and hiddell right A-2 artery;
r-fo,
right
franto-orbital artery; an, microaneur
ysm
on
anterior communicating artery;
a-2,
left A-2 ar
tery;
ar,
arachnoid in interhemispheric fissure ; l-fo,
left frollto-orbita.l artery;
t-fla,
Icrt artery of
I-Ieubnc r. From Fox [3].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 150/213
Anatomy
145
Fig. 7.20. Same case as Fig. 7. 19 after putt ing muslin
(mu)
on microaneurysm and open
in
g
(singk-U05Std
arrow)
the lamina terminalis
(It); ica,
internal carot
id
artery;
doublt-cro.s.std arrow.
anterior choroidal
anery;
nt,
frontal lobe retractor;
ot,
opt
ic tract ;3v, third
ven
tr
icle;
tot, small
cotton
ball .

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 151/213
146
7.
The
Chiasmatic Cist
ern
and Environs
Fig. 7.21.
Chiasmatic cistern
in
case with
hypoplas
ti
c
right A-I artery
(a-l). The
recurrent artery
of
Hcubncr
(ha)
is as large as the A-I artery.
p.
Per
forators;
mol, M-I
artery;
m-2,
frontal
(bottom)
and
temporal (top) M-2 arteries; aT, arachnoid over syl
viall fissure; II, temporallobe;jl, frontal lobe; cot, cot-
tonoid;
rei,
frontal lobe retractor;
ft,
lamina lcr
minalis;
ot,
right optic trac ljch, opticchiasm;gr, right
gyrus rectus; 2, both optic
nen
'es; l-ica, left internal
carotid artcrYipit, pituitary stalk; mem,
membrane
of
LiliequisljT-ica,
right
internal ca rotid artery.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 152/213
Anatomy
147
Fig. 7.22. Magnified
view of Fig. 7.2 1.
Arachnoid
membrane of Liliequist (num) sends anterior sheet in
front of pituitary stalk (pit). ac, Anterior clinoid pro
cess; r-ica, atherosclerotic right internal carotid ar
tery; cot, cottonoid; aM, anterior temporal anery
from internal carotid artery;
ret,
temporal lobe re-
tractor; m-I, M-l artery; a-I, hypoplastic
A-I
artery;
p, perforator;
IUl,
artery of Heubner;foa, fromo-or
bital anery;
r-
gr, right gyrus
reClUS; ihf,
interhemis
pheric fissure; l-gr, left gyrus rectus; l-ica, left inter
nal carotid anery; 2, both optic nerves;
ch,
optic
chiasm; ft, lamina tenninalis; ot, right optic tract.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 153/213
148
7.
The
Chiasmatic Cistern and Environs
Fig. 7.23.
View
of opposite imcrnai carotid cistern
and
chiasmatic cistern. 2, both optic nerves;
{-gr,
left
gy
rus reclUs;
i.oa, left ophthalmic
artery going
unde r left optic nerve;
l-iea,
atherosclerotic left inter
nal carotid artery (medial sidc);is, tuberculum se llae;
r-oo, origin
of right
ophthalmic artery; r-ica. right in-
lernal carotid artery; mem, part of membrane of
Liliequisl (opened) passing in front
of
pituitary stalk
(pit); p, hypothalamic perforator;
ot,
right optic tract;
it, lam ina terminalisj ch. optic chiasm;
ar,
arachnoid
between optic nerves. From Fox [3].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 154/213
Anatomy 149
Fig.
7.24.
Same case as
Fig.
7.23
after
removal of
,I
small amount
of
right gyrus rectus (r-w) to
view
cist
ern
of
the lamina terminalis.
Another
example
of
a
hypoplastic ri ght A-I artery
(a-I. mllom)
and a large
right artery
of
He
ub
ner
(r-ha).
The left A-2 artery is
hidden by the right A-2 artery (a-2). an. Ane urysm
projecting back against the lamina termi llalis (It);
p.
hypothalamic perforators stuck to allleri
or
COIl1-
1T1unicat
i
ng
,1I·tcry aneurysm; *, anterior com
municating artery; r-/pa, right frontopolar artery
(unusually low takeoff from the
A-2
artery);
I-[pa,
left frontopol
ar
artery; l-gr, left gyrus rectus;[oa, left
fronto-orbital artery; I-ha, left artery of Heubner;
a
I (loP), left A-I artery; 2, both o ptic nerves; ch, optic
ch
ia
sm;
Pit,
pituitat·y stalk;
ot,
right optic tract. From
Fox
[3].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 155/213
150
7. The Chiasmatic Cistern and Environs
Fig.
7.25.
Example of chiasmatic cistern with pre
fixed oplic chiasm
(s
hort intracrania l optic nerves).
gel, Gelfoam
on
left optic nerve; 2, both optic nerves;
ch, optic chiasm; iCG, internal carotid anery; elp,
shanks of two aneurysm
dips
; 01, oplic tract; a-I,
right (bottom)
and
left
(toP) A-I
arteries;
aca,
anterior
communicating artery; it, lamina terminalis; ha,
right artery
of
Heubner;
T-fl,
right frontal lobe;
ihj,
interhemispheric fissure (cove
red
by arachnoid);
l-fl,
left f rontal lobe; l-foa, left fronta-orbital artery.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 156/213
Anatomy
151
Fig.
7.26.
Another case revealing an unusual com
mon trunk (*) from which arise the right frontopolar
artery
(r-fpa)
and the artery
of
Heubner
(ha). gr,
Right gyrus rectus; a-2, right A-2 artery from which
the above-mentioned trunk arises;
l-fpa,
left fron
topolar artery; 2, left optic nerve;
ch.
optic chiasm;
a-I,
left (toP) and right
(bottom) A-
I arteries;
it,
lamina
terminalis;
01, op
tic tract; mem, membrane
of
Liliequist;
ac,
anterior clino
id
process;
ica,
internal
carotid artery;
col,
coltonoid. Note xanthochromic
pigment (bilirubin) from hemoglobin
of
recent sub
arachno id hemorrhage.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 157/213
152
7.
T he Chiasmatic Cistern
and
Environs
Fig.
7.27. Allother example where chiasmatic,
carotid,
and
interpeduncular cisterns arc all seen
(from observer's left to righ t) . 2, Bo th optic nerves;
ch,
optic chiasm; 01, right optic tract;
ito,
internal
carotid artery; single-crossed
arrow,
hidden or igi n of
poste r ior co m m u nica
ti
ng
artery; dQu.ble-crossed arrow,
hidden ongm of anterior choroidal artery; ac, an
terior clinoid process; pc. posterior clinoid process;
bo,
basi lar artery;3.oculomotor nerve; un, uncus;
rei,
fron tal lobe retractor;
00,
artery
of
H
eub
ner;
a-I,
right (bottom) and left (toP) A- I arteries_ See next two
fi gures for anterior communicat ing artery complex.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 158/213
Anatomy 153
Fig. 7.28. Same case as in Fig. 7.27. T}'pical variation
in anterior communicating artery complex illus
trated.
a-I,
L
eft (toP)
and right ( mllom) A
-I
arleries;
a-2,
left (top) and right (bol/o
.
m)
A-2
arleries; aea, an
terior communicating arlcry;
co,
connecting b
ri
dge
from anterior communicating arler}, to left
A-2
ar-
tery; in , arachnoid over interhemispher ic fissure;
lIa,
arler}'
of
Heubner; ar, arachnoid fibers; iea, inter
nal
carotid artery; sillgle-crossed
arrow,
origin
of
pos
terior communicating artery; *, bifurcation
of
inter
nal
carotid artery.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 159/213
154
7. The
Ch
iasmatic Cistern
and
Environs
fig. 7.29. Same case as in Figs. 7.27 and
7.28.
An
terior communicating artery complex magnified.
foa,
Franto-orbital artery;
ilif,
arachnoid over i
n
terhem ispheric fissure; a-2, left (toP) and right
(bot
-
10m) A-2 arteries; a-1, left (lOP) and right (hoI/om) A-I
2
arteries; Ma, ante
rior
communicating artery; co, con
necting branch to the left A-2 artery; 2, both optic
nerves; ch,
op
tic chiasm;
ot,
op
tic tract; 1m, artery of
Heubner.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 160/213
Anatomy
155
)
1' I
"
,.1
Fig. 7.30. Another case illustrating relationship
of
anterior communicating artery
(aca)
to chiasmatic
and lamina terminalis cisterns.
a-I,
Left
(toP)
and
right
(bottom)
A-I arteries;
a-2•
left
(lOP)
and right
(bot-
10m)
A-2
arteries;
00,
artery
of
u n e r and
branches covered
by
arachnoid and blood;
ar,
arach noid over interhemispheric
fi
ssure and cover-
a-I
ing a second anterior communicating
ar
ter
y; r-gr.
right gyrus rectus; rtl, frontal lobe retraClOr; I, olfac
tory tract;jl ,
ri
ght frontallobe ;fpa, left frontopolar
artery (low takeoff); foa, left f ronto-orbital artery;
l-gr,
left
gy
rus rectus;
2,
both optic ner
ves;
ts, tuber
culum sellae;
ch,
optic chiasm; 01, right optic tract;
It,
lamina terminalis.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 161/213
156
7.
The
C
hiasmat
ic
Cistern
and Envil"Ons
Fig. 7.31. Another va riation of the anterior com
municating ar tery complex. Fr
om
the an
ter
ior com
municating artery (aca) arises both a connecting
br idge (co) to the left A-2 (sec
Fig. 7.32)
and an acces
sory
(t hi
rd) anter ior cerebral artery (ace) ascending
between the two
A-2
arteries. a·· I , Left
(toP)
and right
(bottQm) A- I ar lc i-ies; a-2, left (lOP)
and
right (OOllom)
A-2
arte
ries;
r-foa,
right
fronto-orbital
artCl-Y; I,
right
olfactory tract; r-gr, ri ght gyru s rectus; l-gr, left gy ru s
rectus; i-roa, left fronto-orbital artery; ar, arachnoid;
2, both optic nerves;
at,
a
nterior
clinoid process;
ica,
internal carotid arte ry;
*', bi
furcation of the internal
carotid artery (from
wh ich
unseen aneur
ysm
arises);
ot,
right optic tract; cit, optic chiasm; It, lamina ter
minalis.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 162/213
Anatomy
157
Fi
g. 7.32.
5."lme
case as
in Fig. 7.31 wit
h right frontal
lobe d isplaced by retractor (rei). a-1, Left (lOP) and
ri
ght (hottom)
A-I
arteries;
a-2,
left
(loP)
and right
(bot-
10m) A-2 arter ies; aca, anterior commun
ica
ting ar
ter
y;
p, perforatOr;
co,
connecting branch from an
terior commu nicating artery to the left
A-2
artery;
V,
\'
ei
n;
ace
, accessory (third) anterior cerebr
al
artery;
foa,
left fronto-orbital arter
y; I-JUl,
l
ef
t artery
of
Heubner; 2, right optic nen'c; ac, right anterior
cl inoid process;
ch,
optic chiasm (lateral s
id
e);
ot,
right optic tract; it. lamina termina
li
s;
*,
bifurcation
of
internal carotid artery from w
hi
ch arises base of
aneurysm
(an); m-2, M-2
artery;
r-Iw,
right a rtery of
Heubncr.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 163/213
158
7. The Ch iasmatic CiS lern and En"irons
Fig.
7.33. AnOlher case of anterior
communicating
artery (aca) duplication. a-I, Right A-I artery; M. ar
tery
of
Heubner; 0-2, right (bottom) and left (top) A-2
arteries; Ttl, right frontal lobe retractor;
ihf,
in
terhemispheric
fi
ss ure;gr, left gyrus rectus; I , left 01-
faclO ry tract; 2, both optic nerves; i-loa, left frolllo
orbital artery;
an,
aneurysm; Pit, pituitary stalk ; ica,
in ternal carotid a rtery;
. ,
bifurCllion
of
inlernai
carotid artery; 01, right optic tract; ii, lamina ter
minalis; ch, optic chiasm; p. perforator.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 164/213
Anatomy
159
Fig
.
7.34. View of
underside
of
an anterior com·
municating artery co mplex in chiasmatic and lamina
terminalis cistern
s. s,
Suction tube;
ua,
internal
carolid artery;
ot, ri
ght optic tract;
fI,
lamina
ter·
minal
is;
p, hypothalamic perforators; a-J, right
(001-
t
om) and left (toP) A· I arte
ri
es;
a-2,
orig
in of
left
A-2
artery;
(Ua,
anterior communicating
ar
ter
y; ha,
left
artery
of
Heubner;
1-[00,
le
ft
fronto-orbital artery;
1,
left olfactol}' tract; 2, both
op
t
ic
nerves;
ts,
tuber
cul
um
sellae.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 165/213
160
7. The Ch iasmatic Cistern and Environs
Fig. 7.35.
AnaLOmy
of lhe lamina terminalis and
chiasmatic cisterns. 2, B
ot
h optic nerves;
ar,
vascul
ar
arach noid betweell optic nerves; cit,
oplicc
hiasm;all,
aneurysm a
ri
sing from most of the internal carotid
artery; a-I, right (bottom) and left (lOP) A-I arte
ri
es; it,
lamina tcrminalis;
JUI,
artery
of
Heubner;
ret,
frontal
lobe retrano}";
0-2,
right (boltom)
and
left (lOP) A-2 ar
teries; ace, origin o f accessory anterior cerebral ar
tery; i/l[,
arachnoid
over interhemisphe ric fissure.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 166/213
Anatomy
161
Fig.
7.36.
Same case as in Fig. 7.35 with magnified
viel\' of the lamina terminalis (It) between the right
A-I
artery (a-I) and artery of Heubner
(ha). The
lamina terminalis is bordcred latcrally by the optic
tract
(vi).
Note arachnoid bands
(or) and
many
P I ~
forating arteries (P). v,
Vein:
gr, gyrus reclus; all,
aneurysm.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 167/213
162
7.
The Chiasmatic Cistern and Environs
Fig,
7.37.
Another example
of
carotid, ch iasmatic,
and lam ina tcnnina
li
s ciSlCrnal analOmy. ica,
in t
cr
nal carotid
artcry; Ie,
edge
of
anterior reflection
of
tentorium;
pc.
posteri
or
clinoid proccss; /KO, pos
terior co mmunica
ti
ng artcr
y; oclw,
anterior choroi
dal
artcry; m-I,
M-l
anc
r
)'; QI,
optic tract;
(1 1,
right
(hollom) and Icft (loP)
A-
I arteries; dr, arachnoid
b<
uld; II, lamina lerminalis;
dCd,
anterior com
municating artery;
hr,
bridging artcry from
left A-
I
loanterior cornmuni catingancry:Joo, left fronto-OI '
bital
ar
tery;
gr,
left gyrus rectus; lUi,
le ft anery of
Heubner;
eh,
optic chiasm; 2, both optic ncn'CS; p,
perforator
s.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 168/213
Anatomy
163
Fig. 7.38. Same case as
in Fig.
7.37, different vi
ew. iea,
Internal carotid artery;
pea,
posterior communicat
ing artery: aelta. anterior choroidal
aner
y: mol, M- I
arter
y;
I-
I,
right (bottom) and left
(lOP)
A- I arteries;
P,
perforator ; ill; arachnoid band;
I··IUI,
right artery
of
H
eubner
and branches; r{oa . right fronLO-orbital
ar·
tery;a-2, origins
of
right
(bottom
) and left
(lOP)
A-2 ar
teries;
v, ve
in;
aea,
anterior communicating arter),; {-
100, left fronto-orbital arte ry;gr, left gyrus reclUS; 2,
bOlh
optic nerves; '·IUl, left artery of H
eubner
; 01,
optic
tr
act; fl, lamina tenninalis.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 169/213
,
Fi
g. 7.3
9. A histor
ic, diagrammatic example
of
an
alllerior
com
municating ar ter
ial
complex form ing duplications and br id ges. On
( ither side
are
the right and left A-IIA-2junctions. Fl"Om BremerJL
(1943) Conge nital aneurysms of the cerebral
ancr ics.
An em
bryologic study. Arch Pathal 35: 81
9-83\;
copyright 1943, Amer
ican fo.'leclieal Association [I].
Fi
g. 7.40. Photograph
of
a plastic cast
(toP)
and d ia
gram
(bottom)
of the rec
ur
rent artery of Hcubnc r as
seen in front with two somewhat different projec
tions. In the diag ram the artery Heubncr is shown in
interrupted lines. From \Vcstbcrg C (1963) T he re
cur rent artery of Heubner and the ancrics of the
central ganglia. Acta Radiol (
Oi
agn) I:
949-954
[5].
164

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 170/213
8
The Ambient and Interpeduncular
Cisterns
Jntroduction
Thi
s chapter focuses
on
the pterional ap
pro
ach toward the amb ient
an
d inte
rpeduncu
lar cistern
s.
Th e surgica l orientati
on
of th e pa
tient's head (sec Fig. 4.8) is similar to th
at
for
the plerionai approach to the syivian, carotid,
and chiasmatic cisterns. However, the operat
ing microscope is s
hif
ted from a m
ore
rostr
al
direc tion (see Fig. 4.5) to a more ca ud al line-of
sight
(see Fi
g. 4.7).
T he amb ient ciste
rn
is a
ce
rebral spinal fluid
(CS
F)
compartment
made up of the
body
a
nd
wing
of the ambie
nt
cistern on each
si
de. T he
bo
dy is
bor
dered laterally by the medial su r
face of the temp
ora
l lobe and the med ial ed ge
of the tentorial notch. It is bordered media
ll
y
by
the latera l surface of the mi
dbr
ain and the
pont
omesencepha
li
c
jun
ction. T he wing (n
ot
seen ana tomi ca lly in this atJas) is a la teralexten
sion
of t
he
body a
nd
lies betwecn the pulvin
ar
of the thalamus
anter
iorly and the temporal
lobe pos ter iorl y. The body of the ambient cis
te
rn
as seen in this atlas contains those struc
t
ur
es foll
ow
ing the te
nt
orial e
dg
e and lying
within the space between the car
ot
id cistern
rostra
ll
y
an
d the interpe
dun
cul
ar
cistern cau
da ll y. Some of these structu res (such as th e an
te rior cho roidal arter
y)
arc assigned to a sepa
rate c
ru
ral cist
ern
by some authors [8}. T he
basilar ve in of Rosenthal and the ter minus of
the optic tract ca n be considered either to
li
e
within the ambient ciste
rn
or to make
up
pan
of the med ial wa ll of the cistern . The third
(oculomotor) nerve
li
es within both the inter
peduncu lar cist
ern
and the amb ient cist
ern
since the arac
hn oi
d memb rane of
Lil
ie
qu is
t
(sep
ara
ting the rostral chiasma
ti
c ciste
rn
from
the c
aud
al inte
rp
e
du
ncular
cis
tern) usua
ll
y is
adh erent along its latera l margin to the medial
and caud al side o f the oculomotor nerve. This
membrane m
ay
stop
at
or bef
ore
the
ocul
omo
t
or
nerve so that CS F in th e inter
pedu ncul
ar
ciste
rn
mixes with
CS
F in the am
bient cistern at a confluence lateral or medial
to the oculom
otor
nerve (
Fig.
8.1; also sec
Fig. 6.3). In some cases the Liliequist mem
brane extends lat
era
lly to the t
ent
orial edge
(see Fig. 8.
10
), a
nd
CS F fl
ow
must be t
hr
ough
per forati
on
s in th is ar ach
no
id me
mbr
ane. T he
poste
ri
or
co
mmuni
cating artery a
nd
the P-2
port ion of the posterior ce reb ra l a
rt
ery as we ll
as the f
ourth
(
tr
ochlea r) nerve and s
up
erior
ce rebe
llar ar
tery also are par
tl
y within the
body of th e ambie nt ciste
rn
.
Fig
ur
e 8.2 shows the anato my
at
the le,'e l of
the tentorial notch and midbrain. Figu re 8.3
diagrams the
anato
my of the auachmcnts of
the t
entorium a
nt
erio
rl
y to the posterior and
anter ior cl ino id processes. Dur ing the pter
iOlla l app roach to the inter pedun cul ar ciste
rn
,
the posteri
or
cli no id process is an
impon
ant
lan
dma
rk lateral
to
w
hi
ch is the oculomotor
nerve.
Within the inter pe
dun
cular cistern lie the
origins of the oculomotor ner ves, the tip of the
basilar artery (Fig. 8
.4),
the origins of the P-I
segments of the posterior cerebral a
rter
ies and
their poste
ri
or th alamic perforators (
Fi
g. 8.4),
and the origins of the s
up
erior cerebe llar ar
te ries. I n the case of a shor t P- l artery, the
caud al end of the posterior communicating a r
tery also may lie m
ore
medially and within the
interped uncu lar cistem.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 171/213
1
66
8.
The
Ambient and Interpeduncul
ar
Cisterns
5u.p
lY
NeT""
(m.b
..
"
p.duncl.
Qu.adriq.mi
MI
pio.t.
Fig.
8.2. Incisura of the tentorium. The midbrain
was sectioned transversely, and the hemispheres
have been removed. Note r
el
ation
of
the bifurcation
of the basilar arte ry to the environs in terms
of
a pIer·
iO
llal
approac
h lO lhis region. From Taveras Jr ..[
Fig. 8.1. Diagram of sagittal sections of a normal
brain and the se llar region , looking to the right. M,
Mammillary body; LM, Lilicquist's mernbranc(mcm
brane
of
Key and Retzius); 3.
right
ocu lomOlOr
Ilene;
PC, right
p o ~ t c
i o l
clinoid process; DS, dor
sum sellae;
arrow, normal now
of CSF th
ro
ugh the
prepontine and inter peduncula r cisterns. From
JL, 0
(1980)
Suprasellar arachnoid
c)
's\s:
an extension
of
the membrane of Liliequis
l.
Neurosurgery 7: 615 -
618
(4).
"
opt.< <hi"""
1 ,{u.
ru\.. bulwn.
Ne:rve.
i-Bo.,ilor r u t . , . ~
, , - , -0, ," (.e:rt1.Cro..l
a:ftV" :I
ou.du.c.t
of
(1960) T
he
roentgen diagnosis of
intracra
ni al in
cisural space occupying lesions. Am
J
Roentgenol
84: 52-69 [7]. Copyright by American Roentgen
R'ly
SocielY. 1960.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 172/213
A
Anatomy
167
Fig. 8.3. Rel ationship of posterior
cl
in oid process on
the left
(A)
and right
(B)
to the oculomo
tor
nerve
and circle of W
il
lis.
No
te relat
io
n
ofpo
steriorclino
id
process. posterior cOlllm un icating artery. 1'-
1
a rt er
y,
and oculomotor nerve t.o tip
of
bas ilar ar tery in
terms of the pter ional app roach \0 the interpedun
cul ar
cis
tern. Reproduced by per mi ss ion from Mal
kasian I) R. Rand
RW (19i8) 1\
'licrosurgi
ca
l anato
my,
in Ra nd R W (cd): Microl1tllroslllgtry. cd
St Lo uis,
CV 1\
losby Co, PI'
3i
-
iO
[6]. A. Superior
view
view
of the left se llar and p,uasell
ar
region de monstra t
ing the d ura l reneClions and the "ocul omotor
trigolle."
/.ines wilh adjaunl OfN'11
arrOW.J. bo
und
aries
of
the ocul
omotor tr
igone:
.t ,
medial renections of
the tentorium cerebc
lli
:
y..
poste
ri
or cl
inoid process;
ante
r
io
r clino
id
process; d. d ia phragm s
el
lae;
lal
tra/ slmighl
black
arrow. ostium
of
the ilUern al carotid
artc )':
cw"Vtd
(lITOU\
O\
'cr optic n
en
'e and
und
er fal
ci
form ligamcnt;dolltd Ii/It. ope ning to the optic fora
m
cn; m
td
ial slmiglit arrow
(b
l
ack
cMcurt'd),
opening in
d i:lphragm se
ll
ac for pituitary sta
lk
; broke71
r r ~
oculomotor ostium; long black arrOW/lead, ostium
of
the fou
rth
cran ia l ner\"c;
l'lI/all
black
arrows.
"Y" du ral
fold. B. Supe ri or
view of
the sella illustrating the reo
lationship of the a n ler
io
r cl i
no
id process
(11 ),
middle
cerebr:11 art
er
y (C). poste rior communicating arte ry
U), ocul omotor
Il
c n e (fl , trochlear nerve (D), pos·
ter
io
r cerebr
al
a
ne
ry
(C)
and tentorium cerebclli
Illed i<l l renectio ll ( :- /
). No
te that the oculomotOr
nerve is s
li
ghtly lateral and
inf
erior to the poster ior
communicating
an ery
at the oculomotor ostium as it
penetrates the du ra in the oculomo
tor
trigone. Ho
w
e\ 'er. as the oculomot
or
nerve
P.
1SseS inferior to the
post
erior
communicating artery (proximal to the
m
id
brain), it m
ay
be im med iat
el
y i
nferior
or slightly
medial to the poste
ri
or cerebral artery-postcr ior
communicaling
artery
ju
n
ct
ion.
Th
e ant
erior
choroid,ll artery has not been included. Unl1UJrked
falciform ligamell t o\"er the
op t
ic nen'c as
it
enters the optic ca nal; E, frce edge of the tentorium
cerebc
ll
i and its medial renection;
H,
basilar artery;
I , post
erior cl
i
no id
process;
K.
antc rior cerebral ar
tery.
8

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 173/213
168
8.
T he Ambient
and
Interpeduncular Cisterns
A
Fig. 8.5. Diagrams illustrating various r
el
ationships
of
the basilar
arter
y terminat ion to the dorsum se
lla
e
(A) and the th ird ventricle (B). From Greitz T,
1...O
f5-
Fig. 8.4. Lateral
vicw
of vertebrohasilar arteriogram
(s ubtraction techn ique) to show example of pos
terior thalamic pel-foratofs
(arrow)
arising from the
p
ol artery and the basilar ancry bifurcation. From
Fox
[2 ].
ted S (1954)
Th
e relationship between the third ven
tr icle and the basi l
ar
artcry. Acta Radiol4 2: 85- 100
[5].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 174/213
Anatomy
169
Fig
. 8.6.
Two
cxampl
csofiopa
midol cislcrnography
wil
h axial
cr
sections at lel·eI
of
midbrain.
Thc
cis
tcrnal CSF is whitc. A. UIV)' black OrTout. from in·
tcrhcmisphelic fissure
to
cistern
of
thc lamina lcr'
millalis (poims
to
lamina tcrminalis behind which is
bla
ck unenhanced CSF
in
third ventricle):
sim igllt
solid black OITOW
lies at union
of
syl\'ian. chiasmatic
and ambient cisterns and points to optic tract;
wavy
wllile aITow p< lSses
from lateral syl\'ian cistern (fis
sure) to medial
sy
lvian cistem;
jlmigllt
solid
wllile
aITow lies
on medial temporal lobc and points
to
th e
body
of
the a
mbi
ent cistern lateral to midbra in :slum
.wiid wllilt Qrrow
lies on
vc
rm is
of
cercbellum and
pOill lS
10 (illad rigcmilia l cistern:
shorl o/lell
Muck
arrow
li
cs in interpcdunc
ul
ar
cis
tern and poims to mam-
A
8
mill
al
l '
body
of
hYj>othalamu s.
B. BfackaITuwhead li
cs
in j unction
of
ambient and intcrpedullcul
ar
cisterns
and poillts 10 oculomotor ner
ve
that separates the
se
cisterns;
doubit-headtd
aITOW lies in interpeduncular
cistcrn and points (a) anteriorly to pituitary stalk
(sur r
ounded
by
arachnoid enclosing less enhanccd
CS
F in hypophyscal cistern) and (b) posteriorly 10
ol1e of
the two ascending P_I afleries;so/id black aITOW
lies
in intcrpeduncular cistcrn and extends from
othcr asccnding P·l artery
to
postcrior clinoid pro
cess (whit
er
than
tllC
enhanced
CSF);solid whitton'OW
lies 011 peduncle of midbra
ill
and points to
bod y of
ambient cistern;
opm arrow lies
on anteri
or
cl inoid
process aud points to internal carotid artery.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 175/213
170
8.
The
Ambienl and In terpedu ncular Cis terns
Within the interpeduncular cistern , the ter
minus
of
the ba
si
l
ar
a
rt
ery
may
have
va
rious
relat ionships wi th the dorsum se
ll
ae and its
posterior clinoid
pr
ocesses
as we ll
as with the
brainstem (
Fi g.
8.5).
The
imaged anatomy of
the str
uctur
es
about the ambient and inter
peduncular cisterns can be seen in cross-sec
tion on the computed tomography (CT) scan
after
instillation of
wa
ter-soluble
cont
rast
medium into the CSF (Fig. 8.6).
Fi
gure 8.7 is a
photogra
ph of
a plastic model of the brain
or
iented as the
neuro
s
ur
geon w
ill
sec the
brain stem, basilar an ery, superior cerebellar
arte
ry, oculomotor nerve, and posterior cere
bral a n e ry (P- I segment) .
In Ihis
view fro m the
plc
ri
onal perspective,
Lhe
right temporal lobe
and cerebellar hemis
ph
ere have been removed
(a
lso see
Fig
. 4.7).
Anatomy
Th
e s
urg
eon fo
ll
ows the posterior com
municating artery cauda
lly.
A
dhes
ions be
tween the uncus
of
the temporal lobe and
oculomotor nerve are removed.
The
tempora l
lobe and i
ts
uncus are retracted. After opening
the arachnoid membrane of
Li
licqui st (mem
brane
of
Key and Retzius), the surgeon sees the
follow in g in a
ca
udal-to-rostral direction
(Figs. 8.8 and 8.9): the rostral pon
s, su
p
er
io r
cerebellar artery, oculomotor nen'e, posterior
cerebral
arte
r
y,
posterior communicating ar
tery and its anterior thalamic p
erfora
tors, an
I.erior choroidal artery. inl.ernal carotid artery.
and o
pt ic
nerve.
The
oc
ul
omotor nerve wi
ll be
seen passing imo the dura
of
the oculomotor
tr
igone (Fig. 8.3)
just
latera l to the
po
sterior
clinoid
pr
ocess. From there the oc
ul
omotor
nen
'e en ters the cavern ous
si
nu
s.
At
this stage
oft
he expos
ur
e, only the lateral
termination
of
the
P-I
artery wi ll be seen at its
ju n
ction with the
P-2
artery
and
the post
er
ior
communicating artery (Fi
g.
8.8).
Us
ually the
P-I artery is obscured
by
the ant
er
ior thalamic
perforators as the artery curves ca udally and
media
ll
y
away
from the s
ur
geon and lOward
the basilar a
rt
ery tip.
The
upper trunk
of
the
basilar a rtery may come into vi
ew
(Fig. 8.9).
At
times the
membrane of
Lili
equist w
ill be
thickened
and
imper
fo
rate from a previous
subarachno id hemorrhage
or
mening
iti
s
(
Fig.
8
.10),
resulting in an obstruction to the
fl
ow
of CSF and subsequent hydrocephalus.
An
in
cision in t
hi
s thickened membrane
(Fi
g.
8.
11
) w
ill
result in a s
udd
en
flow
of CSF
and relaxation
of
the brain. Note thal now the
amel'ior thalamic p
er
forators are seen on their
lateral
si
de whereas views of the carotid cis tern
earli
er
showed these sma
ll
arteries on their me
di al
si
de (sec Figs. 6.7 and 6.8).
In a rare patie nt the post
er
i
or
clinoid pro
cess and i
ts
dural cover ma y project up between
the caudal surfaces
of
the internal carotid ar
tery and optic nerve
or
chiasm
(F
i
g.
8 .1 2). In
the majority
of
patients the posterior clinoid
process projects
up wa
rd in
a parasagiual plane
late ral to the in ternal carotid artery (
Fig.
8
.1
3).
On
occasion both posteriorc linoid processes
and the top
of
the do
rs
um
sel
lae
ca
n be seen
(Fig. 8. 14).
Thi
s same figure shows the right
posterior communicating
ar
tery clipped wi th
sma
ll
ma lleable clips (avoiding perforator
s)
prior to severing this
ane
ry between the
cl
ips.
The P·
2 artery passes laterally between the
temporal lobe an d oc
ul
omotor nerve.
The
P- I
artery takes its typical course
away
from the sur
geon; it loops superiorly, caudall
y,
and me
di a
ll
y lO
wa
rd the rostral tip of the b
asi
lar ar
tery. In
Fi g.
8.14 the middle half of the P- I ar
tery is hidden by the P-2 artery.
Figure 8
.15
is the
sa
me case after severing
of
the right posteri
or
communicating artery.
Th
is
is an
unu
su
al
view
of
both P- I arteries, both
1'
-2
arteries, and the left (opposite) posteri
or
com
municat ing a rtery.
Fig
ures
8
.16
a
nd 8. 17
are t
wo
se
parate exam
ples of previo
ll
s
su
barachnoid hemo
rrha
ges
that have caused adhesions in
the arachno
id
sh
eat
h encl
os in
g the a
nt
erior thalamic per
forators. T hese adhesions have
ca
used many
of
the perforators
to
stick together. This situa
ti
on
requires sl
ow,
delicate dissec
ti
on to
pr
event
p
erforator
injury.
Figures 8 .18 and 8 .19 are two se parate exam
pl
es
of ap pr
oaches to the int
erped
uncular
cis
tern where the intracranial internal carotid ar
tery is short. Retraction of the frontal lobe
brin
gs
A- I and M -I pe
rfor
ator s into "iew at the
bifurcation
of the
internal carot
id
artery. In
Fi
g.
8. 18 the uncus, which hides the P·2 artery,
is still ad herent to the oculomotor nerve. In
Fig.
8.
19 the
interna
l carotid artery hides the
posterior communicating arte r
y.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 176/213
Anatomy
I i i
Fig.
8.7. Plas
tic model of brain: viewed as from a
right pterional appro.1ch to the anatomy around the
interpedunc
ul
ar cistern (see Fi gs. 4.6
and 4.i). The
right temporal lobe and ri ght cerebellum have been
removed, btu the view is similar to that after
wi
de
opening
of
sylvian
fiss ur
e. r-fl. Right front.allobe; J,
both olf.lclory tracts;
1-1l,
medial side of left (o ppo
she) temporal lobe;
p-J,
le ft Pol artery; i-sea, l
ef
t
supe rior cerebe
ll
ar artery; ), rig ht oculomotor
lIerve; ba,
b;:
lsilar
arter
y; '·va. le ft vertebral arte ry:
va
.
ri
ght I'enebral
artery;
//lcd,
medulla
ob
lon
ga
ta;
aiea, right anterior inferior cerebellar
ar
ter
y;
7 and
8. origins of facial and acoustic nerves; 6, right abd u
cent nerve ; 5. right t
ri
ge minal nerve arising from
POllS:
mep. sectioned middle cerebellar peduncle;
ebllll, medial surface of le ft cerebellum (right side cut
awa y);
r-
se
a,
right superior cerebellar artery; p·2,
right
1'
-2 ;1I·tel}'; I'ed. pedu ncle (pyram idal tract) of
midbrain: il'[. interpeduncular fossa
of
midbrain;
pea, right posterior communicating artery; pil, pitu
itary bod y; 2. right optic n
en
'e; lIIam, mamill
ar}'
bod
y.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 177/213
172
8. The Ambient and Imerpeduncular Cisterns
Fi
gures 8.20 through 8.23 are examples of
the righ t latcral zone, middle zone, and left
eral zo ne
of
the inter peduncular cistern as
viewed progre
ssiv
ely from the right pterional
approach. In each res peClive case the micro
scope is tilted from a p
ar t
i
al
cauda-medi
al
di
reclion (ie,
direction
of
the
surge
on '
s view) to a
caudal, yet morc medial, direction. At thc sa me
time the right internal carOlid artery and the
proximal M-J arte ry arc displaced gently to the
l
eft
(media lly)
by
a l la lTOW self-retaining re
tracto
r.
Care is taken not to occlude the carotid
artery (especially i f vascular hypotension is
used) or fracture atherosclerotic
pl
aques in the
arte ry.
In
some cases
it
may
be
necessary to clip
(with sma
ll
ma
ll
eable
cli
p
s)
and sever the post
e
ri
or communicatin g artery (see
Figs
. 8
.1
4
an
d
8.
15), avoiding occlusion
of
anteri
or
thalamic
perforato rs by the clip
s.
In Fig. 8.20 a clear view
of
the oculomotor
nerve separat
in
g the super ior cerebe
ll
ar artery
and the P-2/posterior communicating junClion
is present. T his th ird crani al nerve begins, as it
typically does, as a broad neural band fro m the
midbrain in the interpeduncular fo
ss
a. This
broad band
gather
s together rostral to the
pons and passed forward
under
the tentorial
edge and into the oculomotor trigone (see
Fi
g. 8.3) ju st late ra l to the posterior clino
id
pro
cess. The midbrain, from whence the
oculomot
or
nerve originate
s,
is
hidden from
view owing to the buck
li
ng
of
the brainstem
during the embryoni c stage
of
development.
The forward buckling
of
the de
ve
loping pons
accoun ts fo r the ros tral pons being seen by this
surgica l ap
pr
oach.
With retraction
of
the in temal carotid
anery
and a more medial
til
t
of
the a
im of
the micro
scope
, the center of the interpeduncul
ar cis
tern
ca n be seen
in
Fi
g.
8.2
1.
An even s
harp
er
medial angulation
of
the microscope aimed
caudal to the carot
id
a
ner
y and hypotha lamus
permits the s
ur
geon to see beyond the inter
ped uncular midline as is revealed in Fig s. 8.22
and 8.23. In this circumstance the observer is
look
in
g
th r
ough the space between the back
of
the
dor
sum sel
la
e and clivus (see Figs. 4.7 and
8. 1) and the front
of
the brainstem (see
Fi
g. 8.7). With this
ri
ght pterional approach,
the
do
rsum se
ll
ae (Fig. 8.
14
)
li
es in the upper,
left-hand field
of
the observer's view, and the
basilar artery and ros tral pons
li
e
in
the lowe r,
right-h
and
field
of
the observer's vie
w.
De-
pending on the exaCl direction
of
the opti
cs
of
the microscope, the surgeon now sees bo th
superior ce rebellar arteries (origins), both
oculomotor nerves, both P- I arte ri
es (o
rig in s),
and the l
ef
t mesencepha
lic
peduncle (pyrami
daltract),
T he
anterior
(frolltobasal) surface
of
the up per basilar artery is viewed
by
the su
r
geon.
Figures 8.24 and 8.25 represent another
example
of
the transition from a view
of
the
junClion
of
the ambient and inte
rp
eduncular
cistern s (
Fig.
8.24) to a view
of
the center
of
the
interpeduncular
ci
stern (Fig. 8,2
5)
, Note how
the
P-1
artery on the right tul"llS caudally away
from the s
urgeon
whi le the P- I artery on the
left takes a more lateral co
ur
se. Large and vital
ante
ri
or and posterior thalamic perforators
are presen
l.
Figure 8.26 gives a view
of
the anatomy of
the lamina termi nal s, chiasmatic, carotid , am
bient, and interpeduncular cis tcl"Ils
in
one pa
tient. Figme 8.27 demonstrates anatomy about
the carotid, ambient, and prepontine cistel"lls.
Figures 8.28 through 8.30 represent
another example
of
transition from viewing
the lateral zone to viewi ng the central
zo
ne
of
the interpeduncular cistern in a case
of low
lying ba
si
lar artery bifmcatio
n.
Figures 8.31
through 8.33
il
lu
strate the many anterior
thalamic perforators arisin g from the internal
carotid and posterior communicating arte
ri
es.
They
lie
ensheat hed wi thin their own filmy
arachno id envelope. Th e anter ior choroidal ar
tery takes a pro
minent
course from the inte
r
nal carot
id
artery an d' disappears be hind the
uncus.
Fig
ur
e 8.33 additionally gives a panoramic
view
of
the anatomy
of
the lamina termina lis,
chiasmati
c,
carotid, ambient, and interpedun
cular cisterns. The relationshi p of the pos
terior communicming artery to the
P-I
and P-2
arteries is illustrated. Figure 8,34 gi
ves
a dear
vi
ew
from the bifurc
at
ion
of
the internal
carotid and adjacent optic tract to the bifmca
tion of the ba silar arter
y. The la
st two fi g
ur
es
dea
rl
y demonstrate that the pterional a p
proach permits access to lesions situatcd an y
where about the circle
of
Willis,
I t
is ideally
suited for multip le lesions (eg, aneurysms) pre
sent in diffcrent loci, ye t within reach from the
chiasmatic to the i
nterpedun
cular
ci
sterns.
The
approach req ui res significant removal
of
the sphenoid wing and , in many cases, a wide

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 178/213
Anatomy
173
opening of the sy lvian fissure. Additional de
ta
ils
of
the neurosurgical techniques used by
the author for lhis approach are given else
where [2].
B
ibli
ogra
ph
y
I. Fox J L (1979) f\Iicrosurgical exposure of intracra
nia l aneurysms.J Microsllrg I:
2-3
1
2. Fox J L (1983) Intracranial
Ancwysms, vo
l 2.
New
York.
Springer·Verlag, PP 877 -
1069
3. Fox JL (1985) Microsurgical exposure of vene
brobasi l
ar
aneurysms, in Rand RW (ed):
Micra'
neurosurgery,
cd
3.
St Louis, CV
]\
'Iosby Co,
PI' 589-599
4. "
ox
J L, AI-Mefty
0
(1980) Suprase llar arachnoid
cysts: an extension of the membrane of Lil iequisl.
Neurosurgery 7: 615-618
5. Greilz
T,
Uifsled S (1954) The relationshi p be
tween the third ventricle and the basilar anery.
Acta Radiol42: 85 - 100
6.
Ma
lkasian
DR,
Rand
RW
(1978) Microsurgical
anatomy, in Rand RW (ed):
Micronfuroslllgcry,ed 2.
St Louis, CV Mosbr Co, pp 37- 70
7. l avaras J M (1960) The roentgen diagnosis
of
in·
cis ural intracranial space occupring lesions.
Am
J
Rocntgenol84: 52- 69
8.
a ~ r g i l
MG, Kasdaglis
K,
J ain KK el al ( 1976)
Anatomical observations of the subarachnoid
cis
terns
of
the brain
during
surgery.
J
Neurosurg
44: 298- 302

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 179/213
174
8.
The
Ambient
an
d Interpeduncu lar Cisterns
Fig. 8.8.
Pl
crion
al approac
h
to
ambient and inter
peduncular cisterns (see
Fig
. 8.7 and Fi
g.
4.7). pr,
Probe retracting the ill ternal carotid artery
(ica); 2,
right
optic nerve; ac, anterior cl inoid process; aI',
arachnoid: pc, posterior clinoid process; Ie , tentorial
edge;), oculomotor nc n
c
at lateral oordcr
of
inter
pedu ncular cistern and emering cavernous sinus
through oculomotor ostium (see FIg. 8.3);
sea,
s
uper
"
jo l
"
cerebe
ll
ar
artery;
col,
cononoid:
rei,
tem-
\Xlra
lobe retractor;
pons,
rostral pan of pon
s; pea,
posterior communicating anery entering posterior
cerebral artery at the
pol (P- /)/P2(P-2)
junction;
p,
anterior
thalamic perforators;
lIIC, urlCUS:
adw, dup
licated anterior choroidal artery; v, \'cin. Note: P
-2
ar
tery
and
basal vei n
of
Rosenthal lie ill ambient cis
tcrn between pontomesencephalic region and tem
porallobe. From F
ox
lll.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 180/213
A
na
to
m
y
1
7
fi
g .
8
.9
. S
a
m
e ca
se
a
s
i
n f
oig
8.
8.
P
ro
b
e (p
r)
isr
et
r
c
t-
i
ng
po
s
te
rio
r
c
om
m
u
n
ic
ati
n
g
a
r tc
"
y p
ea
)
to
s
ho
w
o
ri g
i
n o
f
su
p
er
i o
r
ce
re
b
el
la
r a
rt
e r
y
.s
ta
) f
ro
m
b
as
il
ar
a n
e
ry
ha
)
in
i
m
cr
p
cd
u
n
cu
l
r
cis
tc
l l
.
m
; A
r
ac
h
no
id
:
po
rl
S
r
o
st r
a
l
pa
rt
o
f
p
o n
s
; J
b
as
e
o
f
oc
u
lo
m
o t
or
ne
r
ve
n
r
in
g
o
u t
t
its
m
i
db
ra
in
or
ig
in
: /
1-
/,1
-
1
a r
-
t
er
) ;
p-
2
-2
a
r
te r
),
e
n t
c
rin
g
a
m
b i
en
t
c i
s t
e r
n
: Ii
-re
i
te
m
po
r
al
l
o b
e
re
tr
ct
o r
: a
c}
w
d
u p
li
ca
te
d
a
n t
er
io
r
c
h
or
oi
da
l
a
rte
r
y ;
Im
e
,
un
c
u
s;
V,
v
ei
n :
fl-
rr
t,
f
rO
ll
tal
lo
b
e
rc
tr a
c
t
O
l';
2,
o
p t
ic
n
er
v
c :
e
a,
in
te
rn
a
l c
ar
o
t id
r
t
cr
y:
pc
, p
o
s
te
ri o
r
c l
in
oi
d
p
ro
ce
ss
.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 181/213
176
8.
The Ambient
and
Interpeduncular Cisterns
Fig. 8.10 . Path
of
posterior communicating anery
(pea) in another case.
The
thickened
(horn
pre
vio
us
subarachnoid bleed) arachnoid membrane of
Liliequist
(mem)
se parates unseen interpeduncular
cistern from carotid cistern.
Th
e posteri
or
com
municating anery (pea) follows posterior extension
of
carotid cistern
to join
(*) the posterior cerebral ar
tery
(p-2)
in the ambient cistern.
The
1'-2 anery
(P-2)
ascends
in
the wing
of
the ambient
cistern. ica,
Internal carotid artery; at, alllerior clinoid process;
Ie, tentorial margin: 3, oculomotor nerve; /l·rel, tem
poral lobe retractor; p, anterior tha la mic per
forators;
ar,
arachnoid membrane ensheathing pos
terior communicating artery and its perforators (p);
rei,
re lr
actor
displacing M·l artery and carotid ar·
lery bifurcation median),;
a /,
ol 'igill of A·] ,trtery; 2.
right optic nerve; at, anterior clinoid process. From
Fox
[2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 182/213
Anatomy 177
Fig. 8.11. Same case as in
Fig
. 8.
10
. Membrane
or
Liliequist
(mem)
has been opened, revcaling intcr
peduncular cistern.
), Ri
ght oc ulomotor
ne n
'e;
p,
lateral medu
ll
ary perforators: bo, basilar artery; r-
sea,
right superior cere
be llar
artery;
p-2 , P-2
artery;
pea,
posterior communicating artery; INd, medial
side
or
lert (opposite) pedu ncle
of
midbrain. From
Fox [2).

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 183/213
178
8. The Ambiem and
Im
erpeduncular Cisterns
Fig. 8.12. Another case illustrating an unusual pre
sentation of the posteriordinoid proce
ss (PC) pr
oject
ing up between optic nerve (2) and internal carolid
artery
(ica). gr,
Gyrus rectus;
a-J, A-
I
ar
tery;
v,
vein;
unc,
UIlCUS;
J,
oculomotor nerve;
an,
collapsed
aneur
ys
m at posterior communicating artery; clp,
clip
on
aneurys
m; Ile, a
nter
io r clinoid
process.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 184/213
Anatomy
li9
Fig. 8.13. Another case with view
through
ca rotid
cistern into interpeduncular cistern. m-l, t.
·I-1
arte ry;
a-
l ,
A- I artery;
ot,
op t
ic
tract; p, hypothalamic
and
anterior thalamic perfor,llors; ch,
opLic
chiasm; 2,
right optic nerve; ac,
am
erior clinoid process; ica, in
ternal carotid arterY;CTossed arrow, origin of posterior
communicating artery (pea); ac/uJ., anterior choroida l
artery; pol, P
_I
arte ry;
p-2,
P-2 arte ry; 3, oculomotor
nerve;
br, branch
from s
uperior
cerebellar
arte
ry
(sea); PO/IJ, rostral pons; an, aneurysm
of
basilar ar
tery (00) at ori
gi
n
of
s
uperior
cer
ebe
llar artery (sea);
pe, posterior cl inoid process;ds, lOp of dorsum sellae.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 185/213
1
80
8. The Ambient and Interpeduncular Cisterns
Fig. 8.14. Same case
as in Fig.
8.13, looking leftward
across interpeduncular cistern.
fl.
Frontallobc;
ret,
retractor on internal cal"Olid artery
(ica)
and its bifur
cation; p, ilnte ri
or
thalamic perforators; 2, right
optic nerve; ac, amcrior clinoid process; l-pc, left
(op'
posite) posterior clinoid process; tis, LOp of dorsum
sellae; pc. right posterior clinoid process; I-sea, left
supe
ri
or cerebcll,ll" artery; ped, medial side of left
I·sea
peduncle of midbr.aiu; 3, left and right oculomotor
nerves; cmssed Ulnm',
one
of
twO
malleable clips on
posterior communicating an c
ry
(pea); b-Ul . base of
bifurcation aneurysm
of
basilar
anery
(00); /1-1,
right
pol
anery; /1-2, right
P-2
artery;
UIlC, uncus; If-ret,
tern
porallobe retractor; pons. rostral pon s;
an,
dome or
aneurysm at hidden origin
or
I'ight supcl·iorcerebcl.
lar artery (r-sea).

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 186/213
Anatomy lSI
Fig. 8.15. Same case asin Fig
s.
8.13 and 8.14. showing
posterior circle
of Willis
in
interpeduncular
cistern.
2, Right optic nerve;
iea,
internal carotid al· tery; ae,
anterio
r clinoid process;
i-pea
, left posterior com
municating ane ry:
p-2,
left and right P-2 arteries;
p-I.leftand
right - 1 aneries ;J, left (labeled twice)
and
right oculomotor nerves: l-pc, left posterior
clinoid process;
r-
pc, right posterior clinoid
pr
ocess;
00,
tip of basilar
artery;
an,
aneurysm at bifurcation
of hasilar artery;
p,
posterior thalamic perforators;
ped, medial side
of
left peduncle of midbrain;
sea,
right superior cerebellar artery: pons. rostral pons;
crossed r r ~ malleable clip on caudal
end
of severed
right posterior communicating arte ry; Inc, uncus.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 187/213
182
8. The Ambient and Interpeduncular Cis terns
Fig.8.16. Another case illustrating the posterior
communicating artery
(pea)
and its amerior thalamic
perforators (p)
st
uck together by adhesions from
previous hemorrhage. WIC, Uncus; aeM, anterior
choroidal artery;
mol,
M-I artery;
pr,
probe retract
ing internal carOlid ar tery (ica);
a-I,
A-I artery; 2,
optic nerve; pc, posterior
cl
inoid process; mem, thick
ened membrane
of
Liliequist;;, ocu lomotor nene .

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 188/213
AnalOmy
183
Fi
g.
8.17.
Anothcr case wherc the
amer
i
or
thalamic
perforalOrs (p) are stuck IOgether by adhesions in
their c
ncl
os ing arachno
id
sheath. pr, Probe retr
ac
t
ing intcrnal carotid artcry (ita); acha, duplicated an·
terior choroidal artery and p
er
forators;
crossed arrow,
origi n of antcriorchoro idal
aner
),jan, aneurysms at
origin antcrior c
horoi
dal artcry (bottom) and pos·
terior co mmunicating artery (toP):
2,
optic
nc n
'c;
boo,
bif
ur
ca
ti
on
of
basilar artcry:
00,
tr
u
nk of
basilar
artcry;), oculomotor ncrve;sca, superior ccrcbellar
artcr),;
p-2,
P
-2
an ery; po
l,
P_I artcr
y; pea,
posterior
communicating
artcr
y;
II",
uncu
s.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 189/213
184
8.
T he Ambient and I
nterpeduncular
Cisterns
Fig. 8.1 8. Following
posterior
comm unicating
artery
(pea) toward interped uncul ar cistern hidden behind
mem
brane
of Lil iequisl (mem). col, Coltonoicl;
rei,
tempora l lobe retraCLQr; J, oculomotor nerve; unc,
uncus;p, anterior thalamic perforators and A-I per
forators;
akl,
anterior temporal artery; mol, M-l af -
col
" I
tery;
a-I,
A-I ar tery; 2, optic nerve;
aeM,
atHerior
choroid al artery;
ica,
internal carotid artery; crossed
arrow,
origin of posterior co mmunicating artery
(pea); all,
aneurysm at
or
i
gi
n
of
posterior com
municating artery; It, tentorial margin;pc, post
erior
clinoid process.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 190/213
Anatomy
185
II ret
Fig. 8.
19.
View ofrightlatcra
J portion of intcrpcdun
cular cistern after opening membrane
of
LiliequisL
jl-rtl.
Frontal lobe retractor;
p,
perforators from
bi
fu
rcation
of
internal ca rotid artery (iea);
01,
optic
tract; a-I, A-I artery; mem, medial
jX>rtion of
mem
brane
of
Liliequist;
pc,
posterior
cl
inoid process; 00,
basi
lar artery;
an,
aneurysm of basilar
ar
tery at ori
g
in of
superi
or
cerebe ll
ar
artery
(sea);
p-l, P
_I
artery;
p-2, P-2 artery; m-J, M-l artery; m-2,
M-2
artery; It-nl,
temjX>ral
lobe retractor; unc, uncus; 3, oculomotor
nerve;
fe,
tentor
ial
margin.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 191/213
186
8. The Ambient
and
Intt:rpWuncular Cisterns
Fig. 8.20. Anothe r case with view
of
right lateral por
tion of interpeduncu lar cistern after remm'
al
of
mcmbr.mc of Liliequisl. Notc how oculomotor
nerve (J) gathers together from a broad band exiting
the midbrain. pons. Ro stral pons; sea, su perior cere
bellar artery;
00,
basilar artery near
its
bifurcation: Ie,
margin of tentorium;
/1,
temporal lobe;
col,
cot
lO
no
id
;
rei,
retractor:
p-2,
P·2 artery;
p, perforat
ors;
111-2.
M
-2
artery:
mol,
M-l
ar
ter
y;
ot, optic tract; a-I.
A-I artery; 2, opt ic nerve; mem, membrane
of
Liliequisl (anterior re nectio
ll around
pituitary
stalk); ial, internal carotid artery; pea, posterior com
municating artery;
aciUl,
anterior choroidal ar tery;
pol, P_I artery. Reproduced by permission from Fox
JL (1985) Micros
ur
gical expos
ure ofve
rtebrobasilar
ane
urysms, in Rand RW (cd): Micr
mleUrQS1I1gery,
cd 3.
Sf Louis, CV Mosby Co, pp
589-599
[3].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 192/213
Anatomy
187
Fi
g. 8.21 . Same case as in Fig. 8.20. Internal
caro
tid
artery
(ica
), mid dle cerebral
ar
tery (m-I), and pos
teriorcomm unicating ar tery (pea) retracted medially
by
narrow retractor (rtt) to expose cemer or imer
peduncular cistern containing aneu rys m (an) at
bi rurcation
or
bas ilar
ar
tery (ba). Except at its base,
aneurys m is covcred by a
carpe
t or
fi
brin. p-I. Left
(loP) and
ri
ght (bottom) P-l arte
ri
es;sca, right superior
cerebe
ll
ar a
rt
ery: Ie, margin or tentorium : J,
oculomOlOr nen'C; pons. rostral pons; p. one or sev
eral anterior thalamic perrorators rrom postcrior
communicaling art.ery; 2.
opt
ic nerve; /le, anterior
cl
inoid process:pc, posterior
cl
inoid process. Repro
d uced by perm
is
sion rrom Fox
J L (1985)
Micro
neurosurgical exposu
re or
verte
br
obasilar an
eurysms. in Rand RW (cd): M icrotll'UfOsmgery,ed 3. 51
Louis. CV Mosby Co, pp 589- 599 [3).

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 193/213
188
8. The
Ambient and
Interpeduncular
Cisterns
Fi
g.
8.22. Example of ventral surface of
bas
ilar ar
lcry
(ha) in interpedunc
ular cistern flanked
by
oculomotor nerves (3). The membrane of Liliequist
has been removed. t-sea,
Left
superior cerebellar af
tef),; r-sea, right superior cerebellar artery; ], right
and left
oculomotor nerves; lie, right posterior
clinoid process; pol, left and right P-l arteries;
I),
cot
posterior thalamic perforators from
pol;
*, base of
basilar
tip aneurysm; ica,
internal carotid artery;
ret,
rClraClOr displacing iea bifurcation medially; aelia,
anterior choroidal
arter
y; fl. frontal lobe;
col,
cot
tonoid;
/l-ret,
right temporal lobe re tractor; crossed
arrow, malleable dip on caudal end of severed right
posterior
communicating arte
r
y.
From
Fox [2J.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 194/213

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 195/213
190
8. Th e Ambient
and
Interpeduncular Cisterns
,.1
'01
Fig.
8.24. Another case
illustrating anatomy at j unc
tion of carotid,
interpeduncular
, and ambient cis
terns after removal
of
arachnoid mem brane
of
Lilicquist. rei, Retractor displacing internal carotid
a
rt
e l
)'
media
lly; CQl,
couono
id
s;
p,
perforators; mol,
M- I artery;aw, duplicated anterior temporal artery;
v, veins; pons, rostral
pons;),
oculomotor nerve;sco,
superior cerebe llar artery; 00, basilar artery; pea,
post
erior
communica ting artery in carotid cist
ern;
p-2, P-2 artery emering
wing
of ambient
cistern
be·
tween pons and lemporallobe ;p-J, p
ol
artery going
medially in interpeduncular cistern. From Fox [2J.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 196/213
Ana{Qmy 191
.
co.
J
r
)
I
/
Fig. 8.25. Same case as in
Fig.
8.24. View of ventral
aspect
of
bifurcation of basilar artery (boo) and inter·
peduncular cistern between ocul
omO{Qr
nerves (3).
00, Basilar artery: sea. right superior cerebe llar ar
tery; p-l, right (labeled twice) and lef P_I arteries;
p-
2, right P-2 artery; pons, rostral pons; v, ve ins; ala, an-
terior temporal artery;
mol.
M-I artery; col, (ot
{Qnoid;
rel, retra({Qr on ica; p, posterior thalamic per
forators; i-sea, left superior cerebellar artery;
an,
aneurysm
of
tip
of
basilar
artery;crossed
arrow, caudal
end
of
severed posterior communicating artery
(with malleable dip s on
it).
From Fox
[2]
.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 197/213

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 198/213
Anatomy
193
fi
g.
8.
27
. A vicw through carotid and interpeduncu
lar ciste
l'll
s into prepoilline cistern anterior to the
pons
(PO"s). ll·
rt
t ,
Temporal lo
be
retractor; co
l,
cot·
tonoid;
fl ·ret,
frontal lobe retrac
tor
;
clp.
shank of
aneurysm clip on an 3mcrio
rco
mmunicat ing artery
anc
urys
m;
a·l.
A-I artcr
y;
mol. M-l an ery;
tmc,
1I
.t
00'
uncus; sea, superior cerebe llar
anery
; an , aneurysm
of bas ilar artery
(1M)
at takeoff of amerior inferior
cerebellar anery ;J, oculomotor nerve;
pc
. posterior
cli
noid process; ic
a.
internal carotid artery. From
Fox
[2].

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 199/213
194
8. The Ambicni and Jnterpeduncular Cisterns
Fig. 8.28. Another case with view of carotid, inter
pe
dun
cular, and rostral
prepontine
cisterns.
Ie,
Mar
gin of tentorium; mem, remainder of membrane of
Lilicquisl (most removed): rti,
tempora
l lobe retrae
LO
r ; pons, rostral pons; J, oculomotor
ncn'c;jK.
post-
crior clin oid process; ac, anteriorclinoid process; ica,
jlllcrnal
carotid
artery; 2, optic nCl've; QI. optic tract;
a-I, A-
I
artery; m-l,
M-I
artery; p-2, P-2 artery;p-J. p.
I artery; crossed
arrou,
origin of posterior com
municating artery.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 200/213
Anatomy 195
fig. 8.29. Same case as in 8.28 with medial re
traction
(1"(/)
of
the internal carotid artery
(ica).
2.
Optic ne
rv
e:
ac,
anteri
or
clinoid process;
pc, pos
terior clinoid process;p·l, left (obscured with blood)
and right P-
J
arteries; " bifurcation
of
basilar artery;
an, aneurysm
of
b.1si lar artery at takeoff
of
hidden
right su pcrior cerebella r artery;
),
oculomotOr n
en
'e
entering cavernous sinus;
POtU,
rostral pons;
p,
per
forator;
p-2,
right
P-2
artery:
pea,
posteri
or
com
municating artel")'; m-l, M·J artel")'; 0-1, A- I artery;
01, optic tract.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 201/213
196
8. The Ambient and Interpeduncular Cisterns
Fig.
8.30. Same case as in Figs. 8.28
and 8.29.
View of
bifurcation
of
bas ilar artery (boo) in center
of
imer
peduncular cistern. pol,
Left
and right po l arteries;
J, ocu lomotor ncn"c;
all,
aneurysm at o
ri gi
n of
superior cerebe llar artery (sea); Ie, margin of ten
LOr
ium; pons. rostral pons; *, bifurcation of imernal
carotid artery; ret, retractor d isplacing imernal
carotid artery media ll
y.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 202/213

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 203/213
198
8. The Ambient and Interpeduncular Cisterns
Fig. 8.32. Same case as in Fig. 8.31
at higher
magnifi
cation to show
anterior
thalamic perforators
(p)
from
postcfiorcommunicating
artery (pea) and thei r
ensheat
hi
ng arachnoid. ar, Thickened arachnoid
bands within envelope of arachnoid about per
fo
rators and posterior communicating arter
y; un"
uncus of right tern poral lobe; adm , anterior choroi
dal arter
y; ica,
interna l carotid
arter
y;
QI ,
optic tract.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 204/213
AnalOmy
199
Fig.8.33. Same case as in Figs. 8.31 and 8.32.
Arachnoid membrane
of
Lil
ie
qu ist has becn dissect
ed
away.
Note how pterional approach can g
i\
·c
panoramic vicw
of
chiasmatic, lamina terminalis,
carotid, ambielll, and interpeduncular cisterns. 2,
Both optic nerves;
eh,
optic c
hi
asm;
It.
lamina ter
mi
nalis;
01,
right optic tract;
a.-I,
A-I arter
y;
p, pe r-
forators;
m-J, M-l
artery;
m-2,
M
-2
artery;
ar,
ar
achnoid sheath; aeM, anterior choroidal artery;
ita,
internal carotid artery;
an,
aneurysm;
pea,
po
s
terior co mmunicating artery;
00,
basil
ar
artery;
p-
l ,
P-I
artery; p-2 ,
P-2 arter
y:),
oculomotor nerve;
sea,
orig
in
of
right superior cerebell
ar
artery.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 205/213
200
8.
T he Ambient and Interpeduncular Cisterns
Fig. 8.34. Anoth
er
case illustrating bifurcation of
basi lar artery (boo) in interpeduncular cistern.
I-sea,
Left
superi
or
cerebell
ar
artery;
pc
. posterior clinoid
process;
),
left
(hid
den
in
shadows) and right
oculomotor nerves;
v,
vein;
r-sea,
origin of right
superior cerebellar artery;
{1-J,
right and left
pol
ar-
teries in interped uncular cistern;
pea,
posterior com
municating artery;
p-2,
origin
of
right P·2 arter
y; p,
perforators;
Il-ret,
temporal lobe retractor; unc,
uncus;
mol, r.1- 1
artery; ot, optic tran;
ha,
artery
of
Heubncr;jl, frontal lobe;
a-I,
A- I artery; aCM, an
terior choroidal artery;
ica,
internal carotid artery.

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 206/213
A
Abducens nerve, 171
Acoustic nerve, o
ri
gi
n of, 17 1
Adhesions
arachnoid membrane, 94
between frontal and temporal
lobe
s.
56,
71
ca rotid ar lery aneurys m to
oculomotor ne
rv
e,
111
fr
on
t
al
lobe
to
oplic tract,
10.
Ambient cistern, 165-200
anatomy of, 172, 199
body of, 169
junction with ca rotid and i
n
t
erped
unc
ul
ar cistern
s.
169, 172, 190, 192
junction
wi
th
sy
lvian and
chiasmatic
cis
terns, 169
Aneurys m
anterior cerebral ar te ry A-I,
92, 161
anlerior choro
id
al artery. 92.
108
at o rigin, 84, 115, 183
anterior co mmun ica ting ar·
lery, 124, 132, 137, 139,
140, 1
43-
144, 193
hypothalamic perfo rators
stuck to, 125, 149
basilar arte r
y_ Stt
Bas
ilar
af
te r
y.
aneurysm of
internal carotid a
rt
er y.
See
Caro
ti
d artery, in
terna
l,
a neurys m of
middle cerebral a
rt
ery M- I
al b
if
urcation, 76-77
dome in temporal lobe, 75
fl
anked b y tempora l and
frontal M-2 arte ries, 78 -
79
Index
posterior cerebral an ery P-I ,
120
posterior co
mmun
icating ar·
tery,
11
4. 178
at o rigin. 11
5-
11 6, 183-
184
,197
at
supe
ri
or cerebellar artery
ori gin , 180. 185, 196
Aqueduct of
Sy
lv
iu
s, 166
Arachnoi d, 156, 174- 175
anterior re fl ec
ti
on at pitu
itary sta lk , 125, 186
between frontal and temporal
lobes, 72
sc \'ered by microscissor
s,
56,84
between left
op
tic nerve and
frollta
l l
obe. 140
bet
wee
n op t
ic
nerves,
98-99.
10
2,
116, 132-134, 148,
160
covering internal carotid ar
tery and o pt ic ner
ve,
53,
74
disten
ded
by cerebrospinal
fl uid , 56.
59
at interhemisphe
ri
c
fi
ssure,
144, 150, 153-155, 160
at pituitary stalk, 138, 169
s
ur
gica l ope ll ing of, 57, 87-
88, 177
and se paratio n
by
fo rceps
blades, 64-65, 67
at sy lvia n fissure. 146
Arachno id bands or fibers, 57,
87.90-91,
11
7. 153
at anterior cerebral ar tery
A- I , 84, 127, 161- 163
in arachnoid envelope of tha
lam
ic
per
fo
rators and
posterior communica ting
artery. 198
be
tw
een hypothalamic
per
forators
and
o p
tic
tract,
81
between m id dle cerebral ar
tery branches, 56, 70-
73
betwee n middle cerebral M-l
a
rt
ery and te
mpor
al
lobe. 80
between sy lvia n vessels and
pi a, 63
at illlernal carotid artery, 67.
11 6
at lamina terminalis cistern,
125.14
1
at optic nerve/carotid artery
j unc
ti
on, 67
at posterior communicating
ar tery, 83
in subd ura l space, 56, 58,
60-6
1
at sy lvia n fissure base. 56,
65-66
Arachnoid membrane of
Lili
e
quist, 68-69, 93-94, 98-
100, 103-104. 107, 111 -
112, 116. 11 8. 125, 134,
138, 141 , 146- 148, 151,
165-166, 184
adhesions of, 94
attac
hm
ents of, 98
colorat ion of. 97
medial portion of, 185
at pituita ry sta lk , 125, 138.
147 - 148, 1
86
re flection of, 98
removal of, 188
surgical
ope
ning of. 177
thickening after hemorrhage.
170, 176, 182

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 207/213

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 208/213
tentorium of. See Tentorium
cerebe
lli
ve rm is of, 169
Cerebral arteries, anterior, 124,
1
67
A-
I artery, 77, 85, 91, 93- 94,
10
1,
11
0,
11
3-
115. 118,
120, 123, 124, 133-135,
178-179, 182, 1
93-195,
197, 199-200
ane urysm of, 92, 16 1
arachnoid band over, 84,
127, 161- 163
hypoplasia of, 125. 146-
147, 149
left,
11
9, 125, 126,
136-
140,143-
144,149- 157,
159-160. 162-163
bridgin g artery to anter-
IOr
communicating
artery, 127, 162
or i
gi
n of,
82-83.
100, 108.
11
7,176
perfo rators from, 57.
79 -
80,82,84,92,106.141-
142, 161 - 163, 170, 184,
186, 199
rel
at
ion to artery of Heub
ner, 95
right. 125. 126, 136- 140,
143-144, 1
50-
163
junction wit h right A-2,
11
2
tran ssy lvia n view of, 82-83
A-2 arter
y,
126, 156-157
and
common tru nk for ar
tery of Heubner and
ri
ght
frontopolar ar tery,
126, 15 1
left. 137. 139- 140, 144,
153
- 158, 160
bri
dg
in g artery from an
t
er
ior communicating
artery. 112, 126,
154, 157
or
igin of, 159. 163
right, 120, 137. 139- 140,
143,
149. 153-158, 160
junction wit h ante rior
communicating ar tery,
144
ju nction with right A- I ,
11 2
origin of, 163
accessory. 126, 1
56-
157
o
ri
gi n of, 127. 160
in
c
hi
asmatic ciste
rn
, 55
Index
Cerebral arteries, middle. 55
branches of, 56, 57,60,66,
70-71,75,86-90,133
M- I artery. 84-85, 93, 94,
118, 120, 123, 14 1- 142,
144, 1
62-163,
179,182,
193-195, 197, 199-200
aneurysm of
at bifurca tion, 76-77
dome in temporal lobe,
75
nan
ke
d by temporal and
frontal M-2 arteries,
78-79
deep in
sy
lvian fissure,
89
emering sylvian fissure, 81
frontal artery from, 75, 89
l
ef
t, 11 9
long, 67, 78
orig
in
of,
82-83,
106, 108,
112- 11 3,
11
5, 117
perforators from, 57.79-
8 1
,89-92,125,1
46- 147,
170, 181, 1
84-
187, 190-
191,200
short, 57, 79
tran ssy lvian view of, 82-83
vari
ations in, 57 ,
75
M-2 artery, 83,
90,157,
185-
186,199
aneu rysms at bi fu rcatio n at
M- I
.77
dee
p branches of, 87
frontal artery from, 61, 76,
80,88, 146
variations in, 57, 75
Cerebral arteries, posterior.
108-109, 1
66-
167
1'-1 artery, 1
75
, 179, 183,
185-186, 194
aneurysm of, 120
ascending. 169
course of, 170, 172, 190
left, 171, 181, 187- 189,
191. 195-196,200
ori gi n of. 165
perforators from, 165, 168,
1
81,188,195
right, 180-18 1, 187-189,
191, 195-196,200
short, 165
P-2
artery, 109, 114-1 15,
165, 176- 177,179. 183,
185, 192. 194
course of. 170
entering ambient cistern,
175, 190
l
ef
t, 181
perfo rators from, 186,
190--191
203
right, 171, 180- 18 1. 19 1,
195
origin of. 200
relation of
P-
1 and
1'
-2
to
posterior communicating
artery. 170, 172, 174.
186,199
Cerebral peduncle, 166
Cerebrosp in al fluid
circulation of, 94
in distension of arachnoi d
membrane, 56, 59
drainage by lumbar punc
tur
e,
40-4
1
flow through interpedu ncu
lar cistern, 165, 166
in
m
id
brain
se<:t
ions, 169
Chair, surgeon's, 16
Chiasmat
ic
cistern. 93, 1
23-
164
anatomy of, 123-127. 172,
199
struc
tu r
es in. 126
union with
sylv
ian
and
am
bie nt cisterns, 169
Choroidal artery, anterior. 57.
77,80--82,85,91,107,
110, 112- 113,
11
8, 145,
1
62-
163, 179,182,184,
186, 188, 192. 198-200
aneurysm of, 92, 108
at origin , 84. 115, 183
cou rse of, 172. 197
duplicated, 174, 175, 183
origin of, 95, 100, 104, 134,
144, 152, 1
83
perforators from, 183
relation
to
uncus of temporal
lobe, 95, 105
Circle of Willis
posterior,
18
1
relat
io
n to poste
ri
or clinoid
process, 167
Clinoid process
of
sphenoid
bon'
anter
ior, 37-38, 4 1-44. 5 1,
69,83, 100, 107- 108,
11 0- 11 2. 116- 11 7. 123.
128, 1
34,141-142,
147,
1
51-
152. 156, 167, 169.
174, 176,178-18 1, 187,
194- 195
attachment to t
entor
ium,
165
righ
t,
140, 157

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 209/213
204
Clino id process (to'I/.)
posterior,
37-38, 42
-45,
66-
67 ,69,83,98,100, 106 -
10
8,
110-1
11
, lJ
8,
[20-
121, 1
38,152,
162, 167,
169 , 174-175, 179, 182,
1
84-185,
187, 193- 195,
200
attac
hment
to tCllloriutn,
165
dura on, 99, 102. 118
left , 170, 180--18 1
relation to internal carotid
artery. 96, 114- 115
right, 114, 166, 170, 180-
18 1, 188
unu
sual
pr
esentation or.
170, 178
Communicat in g artery. anter
io r, 11
3. 120, 150, 159,
163
aneurysm of,
124, 132, 137,
1
39-
140, 14 3- 144 , 193
hypothalamic perforators
stuck
to,
125, 149
bridging artery from left A·I,
127, 162
bridging ar tery to left A-2.
112 . 126 , 153 - 154, 157
duplicating, 126, 127, 134,
ISS, 158. 164
ju nction
with A·I
and A-2
arteries,
112, 144
perforators from , 11
2, 157
triplicating complex of, 125,
144
variations
in
complex of,
126.
127 , 1
53-
157
V-shaped. 126. 152- 154.
156-157
Communica ting artery. poster·
io r, 77, 85, 91, 99.
11
2-
11
3, 162- 163. 175,177.
195, 200
adjacent aneurysm, 114
aneurys
m
of
collapsed, 178
at origin, 115- 11
6, 183-
184, 197
in
carotid cistern, 190
caudal end in interpeduncu·
lar ciste
rn
, 165
clips on, 170, 178, 180- 18 1,
188, 1
91
course of, 176
ensheathed by arachno
id
membrane, [76
Index
hidden by internal carolid ar
tery, 192
junction with P· I and P·2 ar·
teries, 170, 17
2,
174 , 186
lateral direction of, 95, 106-
107
left ,
11
8- 119, 138
origin of. 95.
98.100-10
1,
104- 105.11 1. 134, 141-
142, 144,152- 153,179,
1
84,194
perforalOrs fr
Om
hypophyseal,95, 102
hypothalamic, 95. 102-
10
3
thalamic, anterior, 82-83,
95, 102- 103, 109- 110,
172.174,176
, 180, 184,
187.190, 192 , 1
97-
198
adhesions in arachnoid
sheath of. 170. 182-
183
in arachnoid sheath. 198
preane
ur
ysma l type of infun
dibulum. 95. 1[0
relation to P· I and P-2 arter
ies, 170 , 172. 174. 186,
199
right , 138, 17 1
sma
ll
, 95, 108
Cranimomy, right frontolateral,
39
Cribriform plate, 124, 130
Crista
ga lli
,
124
, 130-13 1
Cushing, Harvey. 2, 3. 4
D
Dahlgre n. Karl, 3
Dandy, Walter, 4, 5-6
De Martel, Thierry. 3-4
Diaphragm sellae, 106. 1
12
,
118
ope
ning for pituitary sta
lk
,
167
Dissecti ng instruments, 29, 30
Dorsum se
ll
ae,
166
front of. 115
relation to b
asi lar artery ter·
mination, 168
side of, 114- 1
15
top of, 114- 11 5, 170, 179-
180
Doyen, Emile,
3
Drake, Charles, 16, 18
Drills and bur r
s,
24, 41
Dura
of
crista g'd
lli
. 130
exposure o
f.
40, 49-50
frontal,49-50
margin of, 62
as optic c
ana
l margin, 128
of
orbital roof projections.
129, 13 1
of posterior
cli
noid process,
99, 102, 118
of
sphenoid wi ng, 65, 68, 72,
86
of sy lvian
fi
ssure , 50
tempordl, 50
venous
si
nus in , 114-115
Dural
flap,
4 1
E
Electrocautery, 24-26, 39. 40-
41
F
Facial nerve
fron talis branches of, 40
origin o f. 17 1
"alciform ligament, 167
Fi shhook retractors. 22-23, 39,
48
"1aps
cranial.
39-40
dural,41
scalp.
39. 47-48
Foramen ovale.
38
Forceps
electrocautery, 24-26
jewelers, 27, 29. 56. 62
to open and se parate arach
noid, 64-65, 67
" rontal M-2 arteries, 61, 70,
75-76.
88-89
microaneurys
llI
s of. 76
frolll middle cerebral M-I ar
tery. 75. 89
from middle cerebral M-2 ar
tery. 6
1,
76, 80, 88, 146
aneurysm flanked
by
,
78 -
79
Frontal
du r
a. 49-50
Frontal lobe. 53, 58-59, 6 1-64,
66,69.72,74-75,77,
81-83,85-87,91,180.
188.192
ad hes ion 10
op
tic
tr
acl,
104
adhesion to temporal lobe,
56,71
ba
se of,
131
c1 evillion of, 52, 124

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 210/213
left, 1
39-
140, 150
in quadrang
ul
ar
zo
ne of
chiasmatic cistern, 132-
133
righi , 139, 143, 150, 155, 171
Frontolaleral craniotomy, right,
'9
Fronto-orbita l arteries, 114,
124 , 1
32-
133, 13
7,
14 2,
14 7, 154
l
ef
t, 117, 133, 140, 143--144.
149- 15 1, 155-159,162-
163
ri
gh t, 14 3- 144, 156. 163
fo-rontoparieta l sutu re line, I , 37
Frontopolar arteries
left. 140, 149
low takeoff of. 155
low takeoff of. 125, 149, 155
right,
14
9
common trunk with anery
of H
eub
ner, 126, 15 1
Frontosphenoid al suture li ne,
1,37
Frontotemporal bone
nap
,
39-
40
G
Gigli saw, 3, 24, 40
Gyrus rectus, 65, 98, 105, 120,
123, 124. 128, 161, 178
initial exposure o f,
124
,
132-
13'
H
le f
t,
114 , 137, 142, 14 7-149,
155-156, 158. 162- 163
medial surface of, 133
right, 112, 11 4. 133, 136,
146- 147,151. 1
55-
156
vein on, 99, 143
Hayes, George, 5
H
ead
ho ld er, 1
3-16
H
emor
rh
age, subarachnoid
and adh esions in arachn oid
shea th of thalamic per
foralOrs, 170, 1
82-
183
th ic kened arach noid mem
brane
of
Lil iequist from,
170. 176
and xanthochromic pigment
from hemoglobin, 15 1
Heubner recurrent artery, 57,
80-8
1,9 1. 102, 1
05,108,
113, 134- 135, 142- 143,
Index
14 7, 1
52-
155, 158. 170 -
171
,200
adherent to aneurysm al ca
rotid ar ter y bifurcatio n,
85
cOlllmon trunk with right
fr
omopo
lar
ar
ter
y.
126.
15 1
co
ur
se o f, 127, 164
varia tions in, 125
large size of, 125, 14 6, 149
lef
t,
133, 136- 137, 140, 144,
149, 1
57,159,
162-163
perfo rator from, 83
rela tion to
anter
i
or
cerebral
artery. 95
righ
t,
136- 137. 139, 144,
150, 157, 163
Heuer, George,
4 , 5
Histo
ry
of pte
ri
ona a
pp
roach,
1-7
cranial saws in,
2-3
hypophyseal nap in , 5-6
osteoplastic method of Wag-
ner, 1-2
skin incisions in , 7
trephine and melal guide of
de Mar tel in, 3-4
Hydrocephalus. commu nicat
ing,
94
Hypoph
y.sea
l app roach of
Heucr and Dandy. 4,
5-
6
Hypophyseal artery, superior,
79,84, 95, 99, 102. 106,
120
Hypophyseal
ci
stern , 125. 138,
14 1,
169
Hypophyseal
per
forators
from imern
al
carotid artery,
95,99,
11
5, 125, 138
arachnoid sheath o f, 120
from posterior c
ommuni
ca t
in g ar tcr
y,
95, 102
Hypothala mic perforators
from
in
terna
l carotid artery.
81,95, 102- 103, 106,
11 8, 14
8, 159, 179
from post
er
io r commun ica t
in g artery, 95, 10
2-103
stuck to
anterior
communi
ca ting artery aneurys m,
125, 149
Hypothalamus. mammillary
body
of, 166, 169,
171
Hyrtl's ca nal, 41
205
I
Incisions in skin,
7.
39, 46
Instrumentat
io
n, 11-30
bone-re
mo
va
l, 24
dissccting, 29, 30
electrocautery, 24-26, 39,
4
0-4
1
external, 1
3-22
fishhook retractors, 22-23,
39, 48
intraoperat
iv
e,
22-30
jewel
ers'
fo rceps, 27, 29, 56,
62
mirrors, 29
opcrating microscope, 16-22
overhead table, 22
retf3clOrs, 26-27. 28. 48. 5 1-
52,56,58
scissors, 27, 29, 68, 74
suct
io
n
and
suct
io
ll
-i
rriga
ti
o n
devices, 23- 24, 41
surgeon's chai r, 16
television sys tcms. 22
Interhemispher ic fiss ure
(c
is
tern ), 123, 124. 133, 142,
14
7,
158, 169
arachnoid covcring of, 144,
150, 153-- 155. 160
Interpeduncular cistern, 69,
9l-94, 14 1, 152, 165-
200
anatomy of, 165- 173, 199
ap
pr
oaches to. 170. 1
84-
185
basilar artery bifurcation in.
189
center of, 172, 187, 194 -
196
fron
lO
latera l route
10,
98
j un
Ct
ion
wi
th ambient and
C.t rOlid cisterns. 169.
172,190, 192
right l
at
eral po
ni
on of, 1
85-
186
Interpeduncular fossa of mid
brain, 171
Irri
gat
in
g flu id, 23--24
J
J ewelers' forceps. 27, 29, 56, 62
K
Kempe. Ludwig, 6, 39
Kcy and Retzius membran
e.
Set
Arachnoid me
mb
rane of
Li li
equist

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 211/213
206
L
Lacrimal artery, 51
Lamina lerminalis, 85, 112-
11 3,
123.
124
,
12
5, 1
33-
14 8, 15 0- 151 , 155- 160,
1
62-
163, 192, 197
anatomy 0[, 172, 199
Lamina terminalis cistern, 93,
125
, 134- 136,
144
, 149,
16
9
anatomy of, 160-- 162
arachnoid bands
at marg
in
of, 125, 141
struc
ture
s in, 126
Liliequist membrane.
See
Arach
noid membrane of
Li li
e
quist
M
Mammillary body of hypothala
mu
s,
166,
169
, 171
Medu lla oblongata, 171
Medu llary perforators from
basilar artery. 115, 1
77
Meningo-orbital artery. 41, 51
Microscissors. 27.29.68,
74
Microscope, opera ting,
16-
22
advantages of, 17- 18
disadvantages of, 17
Midbrain
anatomy of, 165, 166
interpeduncular fossa of, 171
peduncle
of
(pyramidal
tr act), 169, 171 - 172, 189
left. medial side of, 177,
180- 181
Mirrors at tip of probes, 29
o
Obalinski, Alfred, 3
Oculomotor nerve
s,
65, 69, 94,
98-100,
102 . 104, 10
6-
1
10, 11
2,
11
5, 121, 152,
169, 176, 1
78-
1
79.182-
183. 185. 187, 190, 1
93-
194, 196, 199
adhesion to carotid artery
ane
ur
ysm, III
adhesion to uncus of tempo-
ral lobe, 170, 184
angulation of, 83
base of, 175
course of, 172
entering cavernous sinus,
170,174,192,195
Ind
ex
le ft ,
114
. 180-18 1, 188,200
origins of, 165
oSl ium of, 167, 174
relation to basilar artery bi
furcation. 19 1
right, 114 , 166. 171, 177,
180- 18 1, 1
88,200
separating superior cerebe
ll
ar
artery. 172, 186
Oculomotor trigone, 167, 172
Olfactory bulb, 124,
131
O lfactory cistern , 123, 124,
129
Olfactory nerves, 1
24
Olfactory stria, medial and lat
eral, 124
Olfactory trace, 53, 95, 98--99.
102, 105, 124, 132-133,
155, 17 1
lower portion of, 128
left. 158-- 1
59
middle portion of, 129
right, 156
upper
port ion of, 130, 13 1
Operating
microscope, 16-22
Operating room table.
13
Ophthalmic artery, 95
left, 148
origin of, 104, 148
Optic ca nal, 38, 167
dural
margin of, 128
Optic chiasm, 80-84, 9 1, 106,
112, 114, 11 7- 120, 123,
133, 136, 14
0-
144, 14
6-
152. 154-156, 158, 160,
162, 1
66,179,192,197,
199
lateral side of, 157
pr
e
fi
xed,
124
, 125-126, 134-
135, 150
Optic cistern , 124
Optic nerves, 52, 66, 69, 77,
82-83, 100-101, 103-
105, 107-
108,
110, 112,
11 4, 11 8--120, 167.175,
1
82-
184. 186-187,
194-
195
arachnoid band over, 67
arachno
id
between, 98--99,
102, 11 6, 132- 134,148,
160
arachnoid covering of, 53. 74
latera l portion in carotid cis
tern, 123
left, 106, 117, 133, 138, 140-
143, 146- 152, 154-156,
158--160,162, 192, 199
in orbit, 124
right, 98-99, 102, 106, 11 6-
117.121, 128,133.138,
141
-
14 3,
146--1
50,152,
154- 160,162,171, 174,
176, 179 - 181 . 19
2,199
unusual relation to posterior
cl inoid process, 170, 178
Optic tract,
79-85, 89-9
1, 106,
1
08-
110, 11 5, 120, 123,
135-136,
145 ,150-
15 1,
154, 1
61-
163, 169,179,
185-186, 194-195, 197-
198, 200
adhesion to frontal lobe, 104
right,
112
,
114
, 118, 133,
138--1 44, 146--149, 152,
155-159, 192, 199
terminus of, 165
view to internal caro tid ar
tery, 103
Or
bit
dura covering roof projec
ti
ons, 129, 13 1
in surgical position, 42-45
Orbital fissure,
super
ior. 38
Orbital gyru s, m
ed
ial. 123, 1
24
p
Parietosphenoid al suture line,
1,37
Parictotemporal suture line, I,
37
Peduncles
cerebe llar , middle, 17 1
cerebral, 166
interpeduncular cistern . Set
Interpeduncular cis tern
midbrain.
16
9, 1
71-172,
189
Perforated substance, anterior,
9.
front border of, 124
perforators to, 57, 79, 84, 89,
118
Perforat
in
g arteries
on a
neur
ysm dome, 78
from anterior cerebral
A-
I
ar tery, 57.
79-80,
82, 84,
92,106, 141- 142, 16 1-
1
63,170,184,186,
199
from anterior choroidal ar
tery, 183
from anterior commun icating
arter
y, 11
2, 157
to anterior perforated sub
stance, 57, 79, 84, 89,
11
8

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 212/213
arachnoid fibers from, 57,
90
from artery of Heubner, 83
hypophyseal. Su Hypophy
seal perforators
hypothalamic. Su Hypotha
lamic perforatOrs
from internal carotid artery.
Su Carotid artery. inter
nal, perforators from
medu llary, from basil
ar
ar
tery, 115, 177
from middle cerebral M-I ar
tery, 57, 79-81, 89-92,
125
,
146-147,170,181,
184-187, 1
90-191,
200
from posterior cerebral arter-
''''
_I, 165, 168, 188, 195
P-2, 186,
190-19
1
from posterior communicat
ing artery. Su Commu
nica ting artery, posterior,
perforators from
stria thalamic, 57, 89-92
thalamic. See Thalamic per·
foralO rs
Pericallosal cistern, 123
Periosteal patch elevated from
frontal bone, 39, 47
Petrous pyram id , 42-45
PhoLOgraphy, 33-35
curre
nt techniques in,
34-35
Pituitary gland, 97, 118, 140,
1
71
in
fu
ndibulum of. 166
Pituitary sta lk , 82, 95-96, 102.
104, 106,
11
0,
114
, 119,
12
1,125, 138, 1
40-
14 1,
146,149
opening for, in diaphragm
se
ll
ae, 167
portal veins of, 11 8
surrounded by arachnoid,
125, 138, 147-148, 169
Pons
rostral paft of, 115, 170, 172,
174-175,179-1 8 1,186-
187, 190-192, 1
94-
196
trigeminal nerve ar i
si
ng
from, 171
Positioning
of
patient, 39
importance of, II , 16
Prepontin e cistern, 193,
194
Psyc hopathic point, 6, 39
Pte rion, de finition of, 1,37
Pterygoid
pl
ates, 38
Index
Q
Quadrangular zone in chias·
matic ciste rn , 124. 133-
163
Quadrigeminal cistern , 169
Quadrigeminal plate, 166
R
Raney
dips
, 47
Recurrent artery of Heubner.
Set Heubner recurrent
artery
Reil is lan
d,
7 1
Retractors, 26-27, 28, 48, 5 1-
52, 56, 58
fishhook, 22-23, 39, 48
self· retaini ng. 26-27
Rongeurs, 24, 40
Rosenthal
ve in
, bas
il
ar, 165,
174
S
Saws, crania l, development of,
2-3, 24, 40
Scalp nap, 39.
47-4
8
Scissor
s,
types of, 27, 29, 68,
74
Sella turcica, 37-38
Ski n incisions, 7, 39, 46
Skull fixation, three·poim,
13-
16,39
Sphenoid wings, 37, 38,
42-43,
45
dura over, 65, 68, 72. 86
prior to removal,
49-50
removal of, 39, 40-41
Sphenoid otemporal su ture line,
1
,37
Sphenoparietal sinu
s,
bridging
veins to temporal lobe,
41,56,66.74
electrocoagulation of. 56, 68
Stria thalamic perforators, 57.
89-92
Subarachno
id
h
emor
rhage
and adhesions in arachnoid
sheath of thala
mi
c per
foralOrs, 170, 182-183
thickened arachnoid memo
brane of Liliequist from,
170, 176
and xanthochromic pigment
from hemoglobin. 151
Suction and suc
ti
on.irrigation
devices, 23-24, 4 I
Suture lines of sku ll , 1,37
207
Sy lvian aqueduct, 166
Sylvian fiss
ur
e (cistern), 52, 55-
92.93-94, 123
anatomy of. 56-57
arachnoid over, 146
dura over, 50
lateral, 169
medial, 169
s
ur
gical openin g of, 56-91
union wit h chiasmatic
and
ambient ciSlern, 169
veins in, 63, 66, 75-76, 78
branches of, 59
Sympathetic fibers on internal
carot
id
artery, 96, 116
T
Table
operat
ing room,
13
overhead, 22
Televis ion systems, 22
Temporal arteries
anterior, 70, 75, 77-79, 83,
88-89,91, 100, 134, 147,
184,19 1
dup
licated. 190
from middle cerebral arter
ies, 70
M·I, 75, 89
M-2. 61,76,80,88, 146
aneurysm nanked by, 78,
79
posterior, 76
superficial. 40
Temporal
lobe, 53, 56, 58-59,
6 1
-62,65-66.69-70,7
4,
85-87,9 1,186
adhesions
with carotid artery, 100
wit h frontal
lobe,
56, 71
aneurysm dome in, 75
br idging veins to sphe
nopa
.
rictal
si
nu
s, 41,56
.66,74
el
ectrocoagulation of. 56,
68
dura of, 49-50
elevation of, 52
left, medial side of,
11
7, 119,
171
medial , 169
right, 120
uncus of, 69, 102, 108-109,
11 2-113, 115, 121, 152,
174-1 75, 178, 180-183,
185, 192-193, 197-198,
200

7/23/2019 Atlas of Neurosurgery Anatomy.pdf
http://slidepdf.com/reader/full/atlas-of-neurosurgery-anatomypdf 213/213
208
Tcmporal lobe (conI.)
adherence to oculomotor
nerve, 170, 184
left, media l side of, 117
relation to
anterior
choroi
dal artery, 95, 105
retraction of, 83
vei
n on, 1
28
Tempora
l
is
muscle. incision of,
39,47
Tentorium cerebcUi, 166
anterior reflection of, 99, 162
attachments to clinoid pro
cesses, 165
caro
ti
d a rtery aneurysm
adhesion
to,
101
Index
Third ventricle, 145
cerebrospinal fluid in,
169
relation to b
as
ilar artery,
168
Toison, J ean,
2-3
Tre
mor. reduct i
on
of,
29
Trephin
es, development of, 3-
4
Trigemin
al
ne
rv
e.
ri
g
ht
, ar is
in
g
from pon
s,
171
Trochle
ar
nerve,
165, 166
ostium of,
167
Tubercu
lum se
lla
e, 37-38, 43-
44,117,135, 148, ISS,
159
in
interpeduncular cistern ,
190 - 1
91,200
in
lamina terminalis cistern,
127 , 161
portal, of pituitary stalk, 118
in
sulcus belween frontal lobe
and olfactory cistern,
129
in sylvian fissure, 59, 63, 66,
75-76, 78
on temporal lobe, 128
Venous d ra
in
age,
pr
eservation
of,41
Venous sinu
s,
dura
l,
114-115
Ventricle, third, 145
cerebrospinal fluid
in
,
169