Embed Size (px)
Citation preview

Ac
YBEa
b
c
d
e
f
a
ARRAA
KAASIV
1
mtbcat(vsim
0d
Atherosclerosis 203 (2009) 387–394
Contents lists available at ScienceDirect
Atherosclerosis
journa l homepage: www.e lsev ier .com/ locate /a therosc leros is
ttenuation of inflammation and expansive remodeling by Valsartan alone or inombination with Simvastatin in high-risk coronary atherosclerotic plaques
iannis S. Chatzizisisa,b,∗, Michael Jonasb,∗, Roy Beigelb, Ahmet U. Coskunc, Aaron B. Bakerb,enjamin V. Stoneb, Charles Maynardd, Ross G. Gerritye, William Daleyf,lazer R. Edelmana,b, Charles L. Feldmana, Peter H. Stonea,1
Cardiovascular Division, Brigham and Women’s Hospital, Harvard Medical School, 75 Francis Street, Boston, MA 02115, United StatesHarvard-MIT Division of Health Sciences & Technology, Massachusetts Institute of Technology, Cambridge, MA, United StatesMechanical and Industrial Engineering, Northeastern University, Boston, MA, United StatesDepartment of Health Services, University of Washington, Seattle, WA, United StatesDepartment of Pathology, Medical College of Georgia, Augusta, GA, United StatesNovartis Pharmaceuticals Inc., East Hanover, NJ, United States
r t i c l e i n f o
rticle history:eceived 20 April 2008eceived in revised form 10 July 2008ccepted 22 July 2008vailable online 5 August 2008
eywords:therosclerosis
a b s t r a c t
Aims: We investigated the role of Valsartan (V) alone or in combination with Simvastatin (S) on coro-nary atherosclerosis and vascular remodeling, and tested the hypothesis that V or V/S attenuate thepro-inflammatory effect of low endothelial shear stress (ESS).Methods: Twenty-four diabetic, hyperlipidemic swine were allocated into Early (n = 12) and Late (n = 12)groups. In each group animals were treated with Placebo (n = 4), V (n = 4) and V/S (n = 4) and followed for8 weeks in the Early group and 30 weeks in the Late group. Blood pressure, serum cholesterol and glucosewere similar across the treatment subgroups. ESS was calculated in plaque-free subsegments of interest
ngiotensin receptor blockerhear stressnflammationascular remodeling
(n = 109) in the Late group at week 23. Coronary arteries of this group were harvested at week 30, and thesubsegments of interest were identified, and analyzed histopathologically.Results: V alone or with S reduced the severity of inflammation in high-risk plaques. Both regimensattenuated the severity of enzymatic degradation of the arterial wall, reducing the severity of expansiveremodeling. V alone or with S attenuated the pro-inflammatory effect of low ESS.Conclusions: V alone or with S exerts a beneficial effect of reducing and stabilizing high-risk plaque
nt of
aao
iathwl
characteristics independe
. Introduction
Therapies that reduce the adverse metabolic and proliferativeilieu within an atherosclerotic lesion would be likely to reduce
he progression of atherosclerosis. Angiotensin II receptor type 1locking agents (ARBs), like Valsartan (V), may enhance a vas-uloprotective environment by normalizing endothelial functionnd reducing low density lipoprotein-cholesterol (LDL-C) oxida-ion and inflammatory cell infiltration [1,2]. Statins, like SimvastatinS), in addition to their effects on lowering LDL-C, also exert a
ariety of pleiotropic effects on many components of atherosclero-is, including endothelial function and nitric oxide bioavailability,nflammatory cell migration, and plaque thrombogenicity, ulti-ately promoting plaque stability [3]. Since the mechanisms of
∗ Corresponding author. Tel.: +1 617 732 5692; fax: +1 617 732 7134.E-mail address: [email protected] (P.H. Stone).
nfieeri
l
021-9150/$ – see front matter © 2008 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.atherosclerosis.2008.07.032
a blood pressure- and lipid-lowering effect.© 2008 Elsevier Ireland Ltd. All rights reserved.
ction of V and S are different, it is possible that the anti-therosclerotic effects of these two agents will be complementaryr even synergistic [4].
The nature and clinical significance of an atherosclerotic plaques dependent not only on the formation and progression oftherosclerosis, but also on the vascular remodeling response tohat atherosclerosis [5]. Expansive remodeling is associated withigh-risk plaques, whereas constrictive remodeling is associatedith stable fibrous plaques [5–7]. A dynamic process of extracellu-
ar matrix (ECM) protein synthesis and breakdown modulates theature of the vascular remodeling response to plaque growth. Therst two aims of the present work were to test the hypothesis that Vither alone or in combination with S (a) exerts a plaque stabilizing
ffect by attenuating the high-risk plaque characteristics, and (b)educes the severity of expansive remodeling by attenuating thenflammation and the ECM degradation within the arterial wall.Low endothelial shear stress (ESS) is a major determinant of theocalization and progression of atherosclerotic lesions [8,9]. Recent

3 roscler
hEdttt
m[ntautapiei
2
L(omdtbwamptwtS(ona2psI
golmEeairestmEai(s
naii(itatfirtlawircIbamii
arr[ea
2
Ium2ndsat(guIAficwfiayuil
88 Y.S. Chatzizisis et al. / Athe
istopathology studies have indicated that the magnitude of lowSS, as well as changes in ESS and the rate of change in ESS alsoetermines the severity of plaque inflammation leading to forma-ion of high-risk plaques) [5–7,10]. The third aim of our work was toest the hypothesis that V alone or in combination with S attenuateshe local pro-inflammatory effect of low ESS.
We utilized a well-established diabetic hyperlipidemic swineodel capable of developing human-like atherosclerotic plaques
11]. Two complementary approaches were employed to assess theatural history of atherosclerosis and the effects of V and V/S onhat natural history: (a) Serial in vivo vascular profiling, which ismethodology utilizing coronary angiography and intravascular
ltrasound (IVUS) as described below. Vascular profiling enabled uso identify regions of interest with low baseline ESS, which providesn efficient and effective means to focus on areas where high-risklaque will form. (b) Ex vivo histopathology of those regions of
nterest at the time of animal sacrifice enabled us to investigate theffect of the active agents on vascular inflammation and remodel-ng.
. Methods
The investigation conforms to the Guide for the Care and Use ofaboratory Animals published by the US National Institutes of HealthNIH Publication No. 85-23, revised 1996). A detailed descriptionf the methods is presented in Online supplement. Briefly, 24ale Yorkshire swine were rendered diabetic and fed a high-fat
iet supplemented with sucrose in quantities titrated to main-ain serum total cholesterol (TC) and blood glucose (BG) levelsetween 500–700 and 150–350 mg/dl, respectively [11]. The pigsere allocated into two groups: Early Atherosclerosis group (n = 12)
nd Late Atherosclerosis group (n = 12) to study the early and lateanifestations of atherosclerosis, respectively (Fig. I, Online Sup-
lement). In each group the animals were assigned to one ofhree treatment subgroups: four were given placebo (P), fourere treated with 320 mg Valsartan (V) daily, and four were
reated with the combination of 320 mg Valsartan with 40 mgimvastatin (V/S) daily. Intracoronary vascular profiling methodsi.e. IVUS and angiography) [8] were performed for assessmentf local ESS along the lumen surface of 3D-reconstructed coro-ary arteries at weeks 4 and 8 after the induction of diabetesnd initiation of high-fat diet in the Early group, and at weeks3 and 30 in the Late group (Fig. I, Online Supplement). Therogression of plaque burden and severity over time in the recon-tructed arteries of each treatment subgroup were estimated byVUS.
To investigate the effect of medication on lesion formation, pro-ression, and differentiation to more advanced plaques, we focusedn the Late group. In these arteries, we calculated ESS at base-ine (week 23) to identify arterial regions where future plaque
ay develop and 3 mm long subsegments of interest of differentSS magnitude were selected. To be considered in the analysis,ach subsegment of interest was required to be free of apparenttherosclerotic plaque at baseline, defined by IVUS as maximumntima–media thickness (IMT) ≤ 0.5 mm6 [6]. The animals were sac-ificed immediately after the follow-up vascular profiling, and thepicardial portions of the major coronary arteries were harvested,nap frozen in liquid nitrogen and maintained at −80 ◦C. To locatehe subsegments of interest on the harvested arteries two to three
ajor and readily visible side branches were identified on the
SS and IMT maps, which were derived by the 3D-reconstructedrteries, and used as references [6]. The same branches were alsodentified on the harvested arteries by utilizing magnifying lenses2×). Using these branches as landmarks the exact location of eachubsegment of interest was then identified on the preserved coro-3
bg
osis 203 (2009) 387–394
ary arteries. Subsegments of interest were frozen cut at the middlend cryosectioned (7 �m). Verhoeff’s elastin, oil red O, and picrosir-us red staining, as well as CD45 immunostaining were performedn each cryosection for the assessment of intima-to-media ratioIM), lipid accumulation, collagen content, and inflammatory cellnfiltration, respectively. Oil red O, picrosirius red and CD45 posi-ive intimal areas are presented either as absolute areas (mm2) ors percent of the intima. To investigate the effect of medication onhe heterogeneity of the natural history of atherosclerotic lesions atollow-up (week 30), the lesions were histopathologically classifiednto three categories [6,12]: (a) minimal lesions with IM < 0.15, rep-esenting minimal depositions of lipids and inflammatory cells intohe intima, (b) intermediate lesions, representing larger masses ofipid-laden inflammatory cells without fibrous cap and IM ≥ 0.15,nd (c) FAs, representing severely inflamed atherosclerotic plaquesith a thin fibrous cap overlying a large necrotic lipid core. The
ntegrity of the internal elastic lamina (IEL) beneath the atheroscle-otic intima was assessed in Verhoeff’s elastin-stained sections andategorized into four grades [6] (grade 1: intact, well-organizedEL; grade 2: IEL with a few breaks; grade 3: IEL with many breaksut intact media; grade 4: IEL with severe fragmentation associ-ted with underlying media degradation). Gene expression of theajor ECM degrading enzymes (MMPs and cathepsins) and their
nhibitors (TIMPs, cystatin C) was measured in each lesion by apply-ng real-time PCR.
The nature of the remodeling response to plaque growth in eachrterial subsegment of interest was assessed by comparing the localemodeling behavior of each individual subsegment with the globalemodeling response of the entire artery, as previously described6,13]. Three local remodeling patterns were defined: (a) excessivexpansive remodeling, (b) compensatory expansive remodeling,nd (c) inadequate remodeling.
.1. Statistical analyses
All analyses were performed with SPSS 15.0 (SPSS Inc., Chicago,L) and Stata 10.0 (StataCorp LP, College Station, TX). Contin-ous variables with normal distribution are summarized asean ± S.E.M., non-normally distributed variables as median and
5th and 75th percentiles, and categorical variables as actualumbers and percentages. To correct for systematic error intro-uced by the clustering of arterial subsegments within animals,everal statistical methods were used. First, to investigate thessociation of continuous variables (e.g. histopathologic charac-eristic, normalized gene expression) with categorical variablese.g. treatment subgroup, lesion category, remodeling pattern, IELrade) mixed-effects ANOVA with the animal as random effect wassed. Second, for analyses in which the dependent variable (e.g.
MT) was measured at baseline and follow-up, repeated-measuresNOVA was employed, and the animal and artery were speci-ed as random effects. Finally, where the dependent variable wasategorical (e.g. remodeling pattern), ordered logistic regressionas implemented and the standard errors of the regression coef-cient were adjusted for clustering of arterial subsegments withinnimals with the Huber White Sandwich Estimator. In all anal-ses, p values were adjusted for multiple comparisons of datasing either the Scheffe or modified Bonferroni methods. Find-
ngs were considered to be statistically significant at the 0.05evel.
. Experimental results
One pig in the Early group and one pig in the Late group diedefore the completion of follow-up. Two additional pigs in the Lateroup were excluded from the study because their plasma TC con-

rosclerosis 203 (2009) 387–394 389
cT9i(o2n
mTat
3s
bilmVawi3
3
maaCbltaid
3p
atidiwciimr
3
wIs
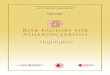
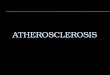
Fig. 1. (a) Effect of Valsartan and Valsartan/Simvastatin on the progression ofatherosclerotic burden in each medication subgroup. (b–d) Effect of Valsartan andVgt
3
Y.S. Chatzizisis et al. / Athe
entrations fell outside the 95% CI of TC distribution at follow-up.hus, 11 pigs (4 on P, 3 on V and 4 on V/S) in the Early group, andpigs (4 on P, 2 on V and 3 on V/S) in the Late group were stud-
ed. Thirty-two coronary arteries were profiled in the Early groupleft anterior descending, LAD, n = 10; left circumflex, LCx, n = 10;btuse marginal, OM, n = 1; right coronary artery, RCA, n = 11), and5 coronary arteries in the Late group (LAD, n = 8; LCx, n = 8; OM,= 1; RCA, n = 8).
Baseline and follow-up characteristics of the animals in eachedication subgroup are shown in Table I (Online Supplement).
here was no significant difference with regard to weight, TC, BGnd systolic blood pressure across the medication subgroups withinhe Early and Late groups.
.1. Effect of V and V/S on the progression of plaque burden andeverity
Regardless of the medication assignment, the atheroscleroticurden by IVUS significantly increased after week 8 (Fig. 1a). Max-
mum IMT by IVUS was classified into four grades, and the percentength of the reconstructed artery occupied by each grade was esti-
ated in each medication subgroup (Fig. 1b–d). Pigs on V and/S developed very few grade 2 plaques, and no grade 3 plaquest weeks 23 and 30. In marked contrast, plaques in pigs treatedith P progressed to more advanced grades after week 8, lead-
ng to marked heterogeneity in plaque severity at weeks 23 and0.
.2. Effect of V and V/S on plaque histopathologic characteristics
In the Late group 109 subsegments of interest (n = 46 in P ani-als, n = 28 in V animals, and n = 35 in V/S animals) were identified
t week 23 (approximately four to five subsegments per artery)nd were cryosectioned and histopathologically stained at week 30.ompared to P animals, lesions in animals treated with the com-ination V/S were of comparable size (IM) but with significantly
ower lipid deposition, plaque inflammation, and collagen con-ent (Table II, Online Supplement). Compared to P-treated animals,nimals treated with V only exhibited significantly less intimalnflammation, while no effect was observed on plaque size, lipideposition, and collagen content (Table II, Online Supplement).
.3. Effect of V and V/S on the development of inflamed high-risklaques
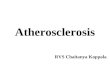
Based on histopathology characteristics atherosclerotic lesionst follow-up were classified into three categories, representing dis-inct stages of their natural history: minimal lesions (n = 25, 22.9%),ntermediate lesions (n = 53, 48.6%), and FAs (n = 31, 28.4%). FAs thateveloped in animals treated with V or V/S had significantly less
nflammation than those FAs that developed in P-treated animals,hereas there was no significant difference in terms of lipids and
ollagen content across the medication subgroups (Fig. 2). Accord-ngly, in the intermediate lesions there was no significant differencen plaque size, lipids, inflammation and collagen content across the
edication subgroups (Fig. 2). These results suggest a stabilizingole of drugs especially in inflamed high-risk coronary plaques.
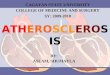
.4. Effect of V and V/S on IEL integrity
The IEL integrity was classified into four grades and correlatedith the severity of inflammation in each medication assignment.
n plaques with severe IEL disintegration (i.e. grade 3) V and V/Significantly limited the inflammation compared to P (Fig. 3a).
s2i
alsartan/Simvastatin on the progression of plaque severity in each medication sub-roup. Error bars represent the standard error of mean and p values are provided forhe statistically significant results only.
.5. Effect of V and V/S on vascular remodeling
Three local remodeling responses were identified in the sub-egments of interest, i.e. excessive expansive remodeling (n = 23,1.1%), compensatory expansive remodeling (n = 56, 51.4%), andnadequate remodeling (n = 30, 27.5%), and were correlated with

390 Y.S. Chatzizisis et al. / Atherosclerosis 203 (2009) 387–394
Fig. 2. Effect of Placebo (P), Valsartan (V) and Valsartan/Simvastatin (V/S) on the histopathologic characteristics of intermediate lesions and fibroatheromas (FAs). Photomi-crographs (a–f) of oil red O- and CD45-stained FAs with inflamed thin fibrous cap at the shoulders (black arrowheads; L = lumen, F = fibrous cap, NC = necrotic core, M = media,A nflamo
ttvrt
at(Ve(hpsw
3e
aeeit(M
= adventitia, C = calcification). V either alone (c and d) or with S (e and f) reduced if mean and p values are provided for the statistically significant results only.
he histopathology in each medication subgroup. Ordered logis-ic regression analysis with remodeling pattern as the dependentariable showed that subsegments with excessive expansiveemodeling were associated with more severe IEL disintegrationhan subsegments with inadequate remodeling (p = 0.002; Fig. 3b).
In subsegments with excessive expansive remodeling V eitherlone or in combination with S reduced the severity of inflamma-ion; in addition V/S only reduced the lipid and collagen contentFig. 4a–d). Likewise, in subsegments with inadequate remodeling
and V/S reduced the severity of inflammation without, how-ver, affecting the plaque size, and the lipid and collagen content
Fig. 4a–d). There was no significant effect of V and V/S on theistopathologic characteristics of subsegments that exhibited com-ensatory expansive remodeling (Fig. 4a–d). These results reveal atabilizing role of V alone or in combination with S in subsegmentsith excessive expansive remodeling.wiewe
mation at the necrotic core and fibrous cap. Error bars represent the standard error
.6. Effect of V and V/S on gene expression of ECM degradingnzymes
In subsegments with excessive expansive remodeling V eitherlone or in combination with S tended to attenuate the genexpression of MMP-9 (Fig. 5). This effect of medication on thexpression of MMP-9 was associated with a significant reductionn the MMP/TIMP ratio, indicating that both regimens decreasehe ECM degradation within excessively expanded subsegmentsFig. 5). No significant effect of V and V/S on gene expression of
MP-2, TIMP-1, TIMP-2, cathepsins K, L, and S, and cystatin C
as observed in subsegments with excessive expansive remodel-ng. Likewise, there was no significant effect of V and V/S in genexpression of the ECM degrading enzymes and their inhibitors, asell as on the MMP/TIMP ratio in subsegments with compensatory
xpansive or inadequate remodeling (Fig. 5).

Y.S. Chatzizisis et al. / Atheroscler
Fig. 3. (a) IEL disintegration in relation to inflammation in each medication sub-group; P = Placebo, V = Valsartan, V/S = Valsartan/Simvastatin. Error bars representthe standard error of mean and p values are provided for the statistically significantresults only. (b) Frequency distribution of each IEL grade in inadequate remodel-ing (Inad), compensatory expansive (Comp), and excessive expansive remodeling(Excess).
Fig. 4. Effect of Placebo (P), Valsartan (V) and Valsartan/Simvastatin (V/S) on the his-tomorphometric (i.e. intima-to-media ratio) and histomorphologic characteristics(i.e. lipids, inflammation, collagen) of inadequate remodeling (Inad), compensatoryexpansive (Comp), and excessive expansive remodeling (Excess). Error bars rep-resent the standard error of mean and p values are provided for the statisticallysignificant results only.
3a
listed
dtEssmTu
4
icosnlaolfslViIolaoattwptptaid
4h
tta[aar
osis 203 (2009) 387–394 391
.7. Attenuation of the pro-inflammatory effect of low ESS by Vnd V/S
Baseline ESS of the subsegments studied was 1.0 (0.7–1.4) Pa,imits: 0.0-3.5 Pa. To assess the role of medication on the pro-nflammatory effect of low ESS, local ESS was calculated in theubsegments of interest at baseline (week 23) and classified intowo categories: low ESS < 1 Pa and moderate/higher ESS ≥ 1 Pa. Theffect of medication on the severity of inflammation in lesions thateveloped in each ESS category was investigated.
In animals treated with P subsegments with low baseline ESSeveloped plaques with significantly more intense inflammationhan subsegments with moderate/higher baseline ESS (Fig. 6). LowSS subsegments in V and V/S subgroups exhibited lesions withignificantly less inflammation than low ESS subsegments in Pubgroup, whereas there was no difference in the severity of inflam-ation in low ESS subsegments between V and V/S animals (Fig. 6).
hese results indicate that V alone or in combination with S atten-ates the pro-inflammatory effect of low ESS.
. Discussion
In this study we explored in detail the effect of V alone andn combination with S on the early and late natural history oforonary atherosclerosis, as assessed by IVUS and histopathol-gy. The diabetic, hyperlipidemic swine model we used in thistudy has proven to be an excellent model for studying coro-ary atherosclerosis in that swine develop regional atherosclerotic
esions similar to humans [11]. We observed, as anticipated, thattherosclerotic lesions are highly focal and develop independentlyf each other, driven by local hemodynamic factors, in particularow ESS. Using vascular profiling, a well-validated methodologyor the assessment of local ESS in vivo [8], we were able to locateubsegments of interest with various severities of atheroscleroticesions and then study the effect of medication on these lesions.
alone, as well as in combination with S, decreased the sever-ty and complexity of coronary plaques as identified by serialVUS studies. Histopathologically, we observed a broad spectrumf atherosclerotic lesions after 30 weeks of diabetes and hyper-ipidemia including minimal fatty streaks, intermediate plaques,nd severe thin cap FAs. V alone or with S reduced the severityf plaque inflammation, particularly in the high-risk FAs. Also, Vnd V/S reduced the severity of inflammation and subsequentlyhe enzymatic degradation of IEL and the arterial wall reducinghe severity of excessive expansive remodeling. V, either alone orith S attenuated the pro-inflammatory effect of low ESS, therebyreventing the escalation of the vicious cycle of low ESS, inflamma-ion, excessive expansive remodeling and formation of high-risklaque. Notably, the levels of TC, BG, and blood pressure acrosshe medication subgroups were similar, suggesting that the anti-therosclerotic effect of V alone or in combination with S wasndependent of the lipid- or blood pressure-lowering effect of therugs.
.1. Stabilizing role of V alone or in combination with S onigh-risk plaques
We demonstrated that V alone or in combination with S reducedhe recruitment of inflammatory cells into the intima. Althoughhe anti-inflammatory action of ARBs has also been studied in
therosclerotic plaques of the aorta in the mouse [14–17], rabbit18], and monkey [19,20], the present study is the first showing suchn effect in the coronary arteries. Furthermore, the ability of ourtherosclerotic model to develop high-risk coronary atheroscle-otic plaque with intense inflammation, large necrotic cores and
392 Y.S. Chatzizisis et al. / Atherosclerosis 203 (2009) 387–394
F acelluc Placet
trcbpdpttaI
odtne
4v
trSripmp
ig. 5. Effect of Valsartan (V) alone or with Simvastatin (S) in gene expression of extrompensatory expansive (Comp), and excessive expansive remodeling (Excess); P =he statistically significant results only.
hin fibrous caps gave us the unique opportunity to focus on theole of V alone or in combination with S in the histopathologicharacteristics of those plaques. We showed that V alone or in com-ination with S reduce the severity of inflammation in high-risklaques, without affecting the plaque size, indicating that theserugs exert their stabilizing effect by altering the composition of thelaques. The anti-inflammatory effect of V is probably regulated byhe blockade of the pro-inflammatory angiotensin II type 1 recep-ors (AT1), as well as over-stimulation of the anti-inflammatoryngiotensin II type 2 receptors (AT2) by the uncoupled angiotensinI [15,21].
Another interesting finding in our study is that the combination
f V with S decreased plaque lipid accumulation, whereas V aloneid not exert such an effect. This effect is presumably attributable tohe complementary pleiotropic effects of S, supporting the combi-ation of ARBs with statins for more powerful anti-atheroscleroticffect [3,4,22,23].tsiaq
lar matrix degrading enzymes and their inhibitors in inadequate remodeling (Inad),bo. Error bars represent the standard error of mean and p values are provided for
.2. Stabilizing role of V alone or in combination with S onascular remodeling
To the best of our knowledge this is the first study investigatinghe effect of V alone or with S on IEL degradation and atheroscle-otic wall remodeling in coronary arteries. V either alone or withsignificantly reduced the severity of IEL disintegration, through
eduction in severity of inflammation, suggesting a synergistic anti-nflammatory role of V and S [22,23]. Increased IEL disintegrationrovides the gateway for the extension of atherosclerosis into theedia, where the inflammatory cells produce matrix degrading
roteases, which degrade the medial extracellular matrix, leading
o excessive expansive remodeling of the wall [6,24]. We demon-trated that V and V/S exert a stabilizing effect by reducing thenfiltration of inflammatory cells through the disrupted IEL, therebyttenuating the severity of vascular wall degradation and subse-uent excessive expansion.
Y.S. Chatzizisis et al. / Atherosclerosis 203 (2009) 387–394 393
Fcrs
bpmiewaleIehrprTofiemttso
4a
pnflpFaVi
ndiwl
Fp
ccrTeli[tstaVhoocpt
4
lolriw
imsoasmE
ig. 6. Severity of inflammation in relation to local baseline ESS in each medi-ation subgroup; P = Placebo, V = Valsartan, V/S = Valsartan/Simvastatin. Error barsepresent the standard error of mean and p values are provided for the statisticallyignificant results only.
The molecular mechanisms through which V alone or in com-ination with S attenuates expansive remodeling had not beenreviously studied. By performing transcriptional profiling of theajor ECM degrading enzymes (MMPs and cathepsins) and their
nhibitors (TIMPs and cystatin C) our study showed in vivo that Vither alone or with S reduces the mRNA expression of MMP-9,hich is actively involved in the ECM degradation [24,25], as well
s the MMP/TIMP ratio, thereby shifting the ECM balance towardsess degradation. However, V or V/S was not found to exert anyffect on the amount of collagen in intermediate lesions or FAs.n vitro and in vivo investigations have demonstrated that ARBsxert an anti-growth and anti-fibrotic effect [1,26]. On the otherand ARBs and statins can reduce the collagen degradation througheduction in inflammation, which is a potent matrix degradingrocess. Furthermore, a recent study in aortas of atheroscleroticabbits revealed that candesartan increases plaque collagen [18].herefore, the net effect of ARBs and statins on collagen contentf a plaque is likely dependent on the balance between the anti-brotic effect through inhibition of growth factors and pro-fibroticffect through inhibition of inflammation. In our atherosclerotic pigodel the V- or V/S-mediated anti-fibrotic effect was not enough
o destabilize the plaques since this may be counterbalanced byhe anti-inflammatory (pro-fibrotic) effect of the drugs. Additionaltudies are needed to further clarify the true role of ARBs and statinsn plaque collagen.
.3. Attenuation of the pro-inflammatory effect of low ESS by Vnd V/S
Another novel finding in our study is the attenuation of thero-inflammatory effect of local low ESS by V alone or in combi-ation with S. Low ESS is a major determinant of the localization,
ormation and progression of atherosclerotic lesions. In addition,ow ESS is associated with the localization and severity of high-risklaques [5–7,10]. In the present study we observed that inflamedAs preferentially developed in arterial regions with low ESS innimals treated with P, while in the same low ESS regions, V or/S prevented this effect by reducing the severity of local plaque
nflammation.On the basis of these finding we propose the following mecha-
isms of interaction between local hemodynamic environment andevelopment of high-risk plaque which can be perturbed or inhib-
ted by the systemic intervention with V alone or in combinationith a statin (Fig. 7): low ESS promotes endothelial dysfunction,
ipid accumulation, production of oxidative stress, inflammatory
wosih
ig. 7. Proposed effect of Valsartan alone or in combination with Simvastatin on theathobiology of atherosclerosis and vascular remodeling.
ell recruitment into the intima and plaque development [5]. In theontext of inflammation, the IEL underneath the plaque undergoesegional disruption and leads to local expansion of the arterial wall.he expansive wall remodeling perpetuates the initially low ESSnvironment, thereby fostering a self-perpetuating cycle amongow ESS, inflammation and wall expansion, eventually transform-ng an early lesion to a high-risk plaque with proclivity to rupture5–7]. As we demonstrate in the current study, V and V/S may blockhe abovementioned cycle by reducing lipid infiltration, oxidativetress, and inflammation [27], thereby preventing local IEL disrup-ion and excessive expansive remodeling. At the vascular level thettenuation of the excessive local remodeling response by V and/S may restore the initial pro-inflammatory low ESS stimulus toigher, more physiologic, levels, thereby attenuating the severityf inflammation and plaque rupture. Although the stabilizing effectf V alone or combined with S has not been investigated in humanoronary atherosclerotic lesions, our findings may provide a patho-hysiologic insight into the reduction of acute coronary syndromeshat has been observed in large clinical trials [28].
.4. Limitations
There are several limitations within the present study. A majorimitation is that the independent role of S was not investigated inur model. However, the primary purpose of our study was to shedight into the independent role of V alone in coronary atheroscle-osis, as well as into the potential synergism of V with S, and not tonvestigate the anti-atherosclerotic properties of S alone, which are
ell-documented in many experimental and clinical studies [3].Our study was also limited by the small number of animals stud-
ed. However, the power of the study increased by investigatingultiple subsegments in each coronary artery (average four to five
ubsegments per artery). In addition, despite the limited numberf animals statistical significance was still achieved. Also, there wasselection bias since subsegments of interest were not randomly
elected. This bias was limited by intentionally selecting subseg-ents of different ESS magnitude, so that the entire spectrum of
SS values and atherosclerotic plaques was represented.Although the anti-atherosclerotic effect of V found in this study
ould be likely to exert an important clinical effect in man as well,ur findings may not be directly applicable to human atherosclero-is, since our experimental model of atherosclerosis was based onnduction of diabetes and intense hyperlipidemia to achieve veryigh levels of plaque inflammation.

3 roscler
dmapie
bavacwtt
5
etshtbarpt
C
fe
A
AtFm
IHF
A
i
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
94 Y.S. Chatzizisis et al. / Athe
In this study we measured only the mRNA expression of matrixegrading enzymes and their inhibitors. While gene expression isost often accompanied by protein expression and activation we
re well aware that gene expression by PCR is not synonymous withrotein expression. Some genes may not be translated to proteins or
f translated the proteins may be inactivated or denatured withoutvident effect.
The results of the current study refer to V and could note generalized on the entire class of ARBs. Although it is wellccepted that all ARBs exhibit blood pressure-lowering action andascular protective effects, different ARBs may exhibit differentnti-atherosclerotic effects in various experimental models andlinical studies. In this study the experimental animals were treatedith the highest recommended dose of V (320 mg daily) [2], and
hese results cannot necessarily be extrapolated to lower doses ofhe drug.
. Conclusion
In this animal study we utilized in vivo vascular profiling tofficiently identify and follow-up coronary artery regions likelyo develop high-risk plaques, and assessed the local impact ofystemic anti-inflammatory pharmacologic interventions on theistopathologic characteristics of those plaques. We demonstratedhat V alone, as well as in combination with S, independently oflood pressure- and lipid-lowering effects, reduces the initiationnd progression of severe plaque, and exerts beneficial effects ofeducing and stabilizing characteristics associated with high-risklaque, even in atherosclerosis susceptible regions of the coronaryree with low ESS.
onflicts of interest
Drs Peter H. Stone and Charles L. Feldman receive research grantsrom Novartis Pharmaceuticals Inc. Dr William Daley was priormployee of Novartis Pharmaceuticals Inc.
cknowledgments
We are grateful to Michelle Lucier, Gail MacCallum, Philip Seifert,nna Maria Spognardi, and Adam Groothuis for their invaluable
echnical assistance. We also thank the Molecular Genetics Coreacility at Children’s Hospital in Boston for providing us the equip-ent for the PCR analyses.Funding. This work was funded by the Novartis Pharmaceuticals
nc., Boston Scientific Inc., George D. Behrakis Research Fellowship,ellenic Heart Foundation, and Alexander S. Onassis Public Benefitoundation.
ppendix A. Supplementary data
Supplementary data associated with this article can be found,n the online version, at doi:10.1016/j.atherosclerosis.2008.07.032.
eferences
[1] Cheng ZJ, Vapaatalo H, Mervaala E. Angiotensin II and vascular inflammation.Med Sci Monit 2005;11:RA194–205.
[2] Burnier M, Brunner HR. Angiotensin II receptor antagonists. Lancet 2000;355:637–45.
[3] Werner N, Nickenig G, Laufs U. Pleiotropic effects of HMG-CoA reductaseinhibitors. Basic Res Cardiol 2002;97:105–16.
[
osis 203 (2009) 387–394
[4] Nickenig G. Should angiotensin II receptor blockers and statins be combined?Circulation 2004;110:1013–20.
[5] Chatzizisis YS, Coskun AU, Jonas M, et al. Role of endothelial shear stress in thenatural history of coronary atherosclerosis and vascular remodeling: molecular,cellular and vascular behavior. J Am Coll Cardiol 2007;49:2379–93.
[6] Chatzizisis YS, Jonas M, Coskun AU, et al. Prediction of the localization of high-risk coronary atherosclerotic plaques on the basis of low endothelial shearstress: an intravascular ultrasound and histopathology natural history study.Circulation 2008;117:993–1002.
[7] Chatzizisis YS, Coskun AU, Jonas M, et al. Risk stratification of individual coro-nary lesions using local endothelial shear stress: a new paradigm for managingcoronary artery disease. Curr Opin Cardiol 2007;22:552–64.
[8] Stone PH, Coskun AU, Kinlay S, et al. Effect of endothelial shear stress onthe progression of coronary artery disease, vascular remodeling, and in-stent restenosis in humans: in vivo 6-month follow-up study. Circulation2003;108:438–44.
[9] Wentzel JJ, Krams R, Schuurbiers JC, et al. Relationship between neointimalthickness and shear stress after Wallstent implantation in human coronaryarteries. Circulation 2001;103:1740–5.
10] Cheng C, Tempel D, van Haperen R, et al. Atherosclerotic lesion size andvulnerability are determined by patterns of fluid shear stress. Circulation2006;113:2744–53.
11] Gerrity RG, Natarajan R, Nadler JL, Kimsey T. Diabetes-induced acceleratedatherosclerosis in swine. Diabetes 2001;50:1654–65.
12] Virmani R, Kolodgie FD, Burke AP, Farb A, Schwartz SM. Lessons from sud-den coronary death: a comprehensive morphological classification scheme foratherosclerotic lesions. Arterioscler Thromb Vasc Biol 2000;20:1262–75.
13] Feldman CL, Coskun AU, Yeghiazarians Y, et al. Remodeling characteristics ofminimally diseased coronary arteries are consistent along the length of theartery. Am J Cardiol 2006;97:13–6.
14] Tsuda M, Iwai M, Li JM, et al. Inhibitory effects of AT1 receptor blocker, olme-sartan, and estrogen on atherosclerosis via anti-oxidative stress. Hypertension2005;45:545–51.
15] Wu L, Iwai M, Nakagami H, et al. Roles of angiotensin II type 2 receptor stim-ulation associated with selective angiotensin II type 1 receptor blockade withvalsartan in the improvement of inflammation-induced vascular injury. Circu-lation 2001;104:2716–21.
16] Doran DE, Weiss D, Zhang Y, Griendling KK, Taylor WR. Differential effectsof AT1 receptor and Ca2+ channel blockade on atherosclerosis, inflammatorygene expression, and production of reactive oxygen species. Atherosclerosis2007;195:39–47.
17] Suganuma E, Babaev VR, Motojima M, et al. Angiotensin inhibition decreasesprogression of advanced atherosclerosis and stabilizes established atheroscle-rotic plaques. J Am Soc Nephrol 2007;18:2311–9.
18] Johnstone MT, Perez AS, Nasser I, et al. Angiotensin receptor block-ade with candesartan attenuates atherosclerosis, plaque disruption, andmacrophage accumulation within the plaque in a rabbit model. Circulation2004;110:2060–5.
19] Strawn WB, Chappell MC, Dean RH, Kivlighn S, Ferrario CM. Inhibition of earlyatherogenesis by losartan in monkeys with diet-induced hypercholesterolemia.Circulation 2000;101:1586–93.
20] Takai S, Jin D, Sakaguchi M, et al. Comparative effects of candesartan andamlodipine in a monkey atherosclerotic model. Hypertens Res 2004;27:517–22.
21] Sales VL, Sukhova GK, Lopez-Ilasaca MA, et al. Angiotensin type 2 receptor isexpressed in murine atherosclerotic lesions and modulates lesion evolution.Circulation 2005;112:3328–36.
22] Li Z, Iwai M, Wu L, et al. Fluvastatin enhances the inhibitory effects of aselective AT1 receptor blocker, valsartan, on atherosclerosis. Hypertension2004;44:758–63.
23] Yamamoto E, Yamashita T, Tanaka T, et al. Pravastatin enhances beneficialeffects of olmesartan on vascular injury of salt-sensitive hypertensive rats, viapleiotropic effects. Arterioscler Thromb Vasc Biol 2007;27:556–63.
24] Sukhova GK, Wang B, Libby P, et al. Cystatin C deficiency increases elastic lam-ina degradation and aortic dilatation in apolipoprotein E-null mice. Circ Res2005;96:368–75.
25] Galis ZS, Khatri JJ. Matrix metalloproteinases in vascular remodeling andatherogenesis: the good, the bad, and the ugly. Circ Res 2002;90:251–62.
26] Brassard P, Amiri F, Schiffrin EL. Combined angiotensin II type 1 and type 2receptor blockade on vascular remodeling and matrix metalloproteinases inresistance arteries. Hypertension 2005;46:598–606.
27] Dandona P, Kumar V, Aljada A, et al. Angiotensin II receptor blocker val-sartan suppresses reactive oxygen species generation in leukocytes, nuclear
factor-kappa B, in mononuclear cells of normal subjects: evidence of an anti-inflammatory action. J Clin Endocrinol Metab 2003;88:4496–501.28] McMurray J, Solomon S, Pieper K, et al. The effect of valsartan, captopril, orboth on atherosclerotic events after acute myocardial infarction: an analysis ofthe Valsartan in Acute Myocardial Infarction Trial (VALIANT). J Am Coll Cardiol2006;47:726–33.