-
Atherectomy with thrombectomy offemoropopliteal occlusions
withRotarex S®:TheLeipzigexperience
Dr.BrunoFreitas,Prof.,MDDepartmentof Interventional
Angiology,UniversitätLeipzig,Germany
SantaCasadeMaceió,Alagoas,BrazilDivisionof Vascular
Surgery,FederalUniversityof Alagoas,Brazil
Biotechnologicaland BiomedicalCenter-
Biocity,UniversitätLeipzig,GermanyFaculty of
Medicine,StateUniversityof Alagoas,Maceió,Brazil
-
LowerExtremityArterialCTOs
•
40-50%ofpatientswithsymptomaticperipheralarterialdisease(PAD)havecompleteocclusionandhalfofallpatientswithCLIwillundergosomerevascularization1.
• CTOsaremostcommonintheinfra-inguinallocation2.
•
Nearly50%ofsuperficialfemoralartery(SFA)lesionspresentasCTO3.
• CTOismuchmorecommonincriticallimbischemia(CLI).
1.Norgren,etal.JVascSurg.2007;45(supp.S):S5–67.2.Banerjee,etal.CardiovascRevascMed.2011;12(2):134.3.Banerjee,etal.JACC.
2012;60(15):1352–359.
-
Artery with circumferential medial calcification
recanalization
Artery withatheromatous thromboemboli
neovascularization
fragmentationof elastin layer
Ca
Ca
CTOwithfibrocalcic tissueandatherothrombotic softtissue
CTOsHistologic Sections fromPatients with CLI
• Recent(<3months)• Thrombus/embolus•
Acutelimbischemia(<2weeks)
• Chronictotalocclusion(≥3months)• Organizedthrombus•
Fibrotictissue• Calcification• Microchannels
-
Nodular calcification
Ca 2+
Ca 2+
Ca 2+Ca 2+
Plaque rupture with sheetcalcification and
propagatedthrombus
Ca 2+
Chronic organization
CTOsHistologic Sections fromPatients with CLI
-
UNDERSTANDING CALCIUM:Prevalence of Calcium in Atherosclerotic
Lesions
-
SoftCoreTasc C/DFemPop CTOs
-
SoftCoreTasc C/DFemPop CTOs
-
TASCC/DFemPop ”SoftCore”CTOs
After1
Passage
After3
Passages
DEB
DEB
-
SoftCoreTasc C/DFemPop CTOs
Fina
lAngiogram
Fina
lAngiogram
-
Rotarex mechanical debulking:TheLeipzigexperience
in1.200+patients
- Singlecenter registry:- Use of Thrombectomy device
inOPADpatients- Safety and efficacy
- Consecutive patient enrollment- Realworld scenario-
1.809patients treated (from 1/2005– 11/2013)- 1.572patients were
analyzable (86,9%)
-
Intervention Feature- Native „virgin“ arteries- Surgical
bypasses- Redo procedures- In-stent procedures
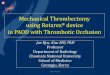
Rotarex mechanical debulking in acute/subacute thrombotic
lesions:
The Leipzig experience in 525 patients
525 Acute/Subacute
Patients
-
InterventionFeature- Native„virgin“arteries- Surgical bypasses-
Redo procedures- In-stent procedures
Rotarex mechanical debulking:TheLeipzigexperience
in1.200+patients
1203Procedures
-
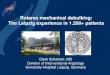
Rotarex-Catheter (Straub-Medical)
Removal – Suction –Fragmentation - Transport
40 000 -60 000 rpm
ROTAREX ROTAREXSMultilayer braided
-
InterventionFeature- Native„virgin“FemPop arteries treated
with
Rotarex S- Surgical bypasses- Redo procedures- In-stent
procedures
Rotarex S®Atherothrombectomy innativeFemPop
arteries:TheLeipzigexperience
658Procedures
From January 2011to November2013
-
Age, Mean ± SD (n) 67.4± 11.6 (658)Male gender, n(%)
428(65.1)Medical History, n(%)
Obesity 188 (29.6)Smoking 294(44.7)
Dyslipidemia 437(66.4)Diabetes 244 (37.1)
Insulin-dependent DM 37 (15.2*)Hypertension 512(77.8)
Coronary Artery Disease 208(31.6)Cerebrovascular disease
71(10.8)
Renal Impairment 75(11.4)Dialysis 8(1.2)
Previousanticoagulation 43(6.5)
Table1.Clinicalcharacteristicsof658patientstreatedwithMechanicalAtherothrombectomy
for“plain”FemPop nativearteries.*amongdiabeticpatients
Rotarex S®Atherothrombectomy innativeFemPop arteries:
Demographic characteristics (n=658)
-
Acute ( 3 months) 373 (56.7)
Rotarex S®Atherothrombectomy innativeFemPop arteries:
Onset of symptoms (n=658)
-
Rutherford Score Patient with events, n(%)
0 0
1 8 (1.2)
2 88 (13.4)
3 165 (25.1)
4 258 (39.2)
5 110 (16.7)
6 29 (4.4)
Total 658 (100)
Table2.BaselineRutherfordscoresamongpatientsatenrollmentAtherothrombectomy
DevicesinnativeFemPop arteries
Rotarex S®Atherothrombectomy innativeFemPop arteries:
Clinicalstatus – Rutherfordclass onadmission
60.3%CLI
-
Table3.OverallAngiographicandproceduralcharacteristicsamong568patientstreatedwithMechanicalatherothrombectomy
devicesfor“plain”nativearteries.
Total Vascular access sites 658
Antegrade 373 (56.7%)
Crossover 285 (43.3%)
Sheath diameter device (French)6 445 (67.6)8 213 (32.4)
Mean lesion lenght (cm) 14.8 (2-27.4)Intervention area
SFA 419 (63.7%)Popliteal 85 (12.9%)
SFA + Popliteal 154 (23.4%)
Rotarex S®Atherothrombectomy innativeFemPop arteries:
Angiographic and procedural characteristics
-
Type of lesion (complain symptoms) n(%)
Calcification 658
No/mild 321 (48.8)
Moderate 224 (34.0)
Severe 113 (17.2)
Intervention Feature 658
De-novo lesions 449 (68.2)
Previous Balloon Angioplasty 209 (31.8)
Lesion Type
Rotarex S®Atherothrombectomy innativeFemPop arteries:
Angiographic and procedural characteristics
82.8%
-
• Procedural success rate: 631 (95.9%)
• Main performed procedure• Rotational Atherothrombectomy alone:
139 (21.1%)• Rotational Atherothrombectomy + PTA: 354 (53.8%)•
Additional Stenting: 165 (25.1%)• Additional Thrombolysis: 59
(9.0%)
• Mean time follow-up: 12 ± 2.4 months • Filter usage
percentage: 41 patients (6.2%)
Rotarex S®Atherothrombectomy innativeFemPop arteries:
Acute results
-
Stenting-rate: 165(25.1%)
Full lesion stenting: 44(6.8%)
Focal stenting: 121(18.3%)
Rotarex S®Atherothrombectomy innativeFemPop arteries:
Acute results
-
Spot Stenting vs. Long Stenting afterSubintimal Approach in FP
Artery CTOs
77%
47%
J Am Coll Cardiol Intv 2015;8:472
-
Table 6. Major Adverse Events (MAE) to 12-months
post-intervention
MAEAll events
n (%)
Perforation 9 (1.4)
Bleeding 18 (2.7)
Dissection 49 (7.4)
Acute closure 19 (2.9)
Emboli 21 (3.2)
Infection 12 (1.8)
Rotarex S®Atherothrombectomy innativeFemPop arteries:
Acute results - Complications
-
Major Adverse Events (MAE) to 30 postoperative day
MAE Events (%)
Death 9 1.4
MI * 11 1.7
TLR ** 11 1.7
TVR *** 4 0.6
Major Amputation 8 1.2
Total 43 6.5
Table 4. Major Adverse Events (MAE) to 30 postoperative day.
Valuesareratenumbers(%)ofobservations• Myocardialinfarction
**Target-lesionrevascularization***Target-vesselrevascularization
Rotarex S®Atherothrombectomy innativeFemPop arteries:
ClinicalFollow-up:30-dayresults
-
Major Adverse Events (MAE) up to12 month
MAE Events (%)
Death 59 9.0
MI * 17 2.6
TLR ** 65 9.9
TVR *** 21 3.2
Major Amputation 24 3.7
Rotarex S®Atherothrombectomy innativeFemPop arteries:
ClinicalFollow-up:12months results
-
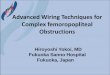
0
50
100
150
200
250
300
RF 0 RF 1 RF 2 RF 3 RF 4 RF 5 RF 6
Number of patients
Rutherford classes (RF)
BaselineFollow up
78.7% of patients withimprovement in Rutherford class
Rotarex S®Atherothrombectomy innativeFemPop arteries:
ClinicalFollow-up:12months results
-
Popliteal”SoftCore”OcclusionCLI
-
Popliteal”SoftCore”OcclusionCLI
-
Popliteal”SoftCore”Occlusion- CLI–Unmaskingculpritlesion
5X80mm POBA 5X120mm DEB
-
Popliteal”SoftCore”Occlusion- CLI–FINALRESULT
-
•
TheuseoftheRotarex-catheterinnativeperipheralarterieswithacute,subacuteandchroniclesionsresultedinahighproceduralsuccessrateof95.9%
•
Thelowrateofproceduralcomplicationsand30dayclinicaleventssupportsthesafetyofthedeviceinabroadrangeoflesions
•
The12-monthsTLRrateof9.9%togetherwithamarkedimprovementoftheclinicalstatusdemonstratestheclinicaleffectivenessat1year.
•
Despiteofareasonablenumberofcases,it’saSingleCenterexperience,retrospectiveanalysis.
• Effectivetoolforremovingsoftatherothrombotic
lesionsandhighlightigundercovered “guilty”lesions– lessstenting
Rotarex S®Atherothrombectomy innativeFemPop arteries:
TheLeipzigexperience in568patientsSummary
-
Thanks alot !!!!!
-
Atherectomy with thrombectomy offemoropopliteal occlusions
withRotarex S®:TheLeipzigexperience
Dr.BrunoFreitas,Prof.,MDDepartmentof Interventional
Angiology,UniversitätLeipzig,Germany
SantaCasadeMaceió,Alagoas,BrazilDivisionof Vascular
Surgery,FederalUniversityof Alagoas,Brazil
Biotechnologicaland BiomedicalCenter-
Biocity,UniversitätLeipzig,GermanyFaculty of
Medicine,StateUniversityof Alagoas,Maceió,Brazil