Embed Size (px)
Citation preview
CFOMT
TlfsctrivadIafqrgwms
CPrstfdrr
S
RFmmPRCMm
©P
COLLECTIVE REVIEWS
omprehensive Endovascular Therapy foremoropopliteal Arterial Atheroscleroticcclusive Diseaseark G Davies, MD, PhD, FRCSI, FRCS, FACS, David L Waldman, MD, PhD,
homas A Pearson, MD, MPH, PhDydwowptc5fpfsst
llTeaTr
ATwbaapitufdh
reatment of the patient with symptomatic femoropop-iteal atherosclerotic disease is evolving. The superficialemoral artery is a common site for infrainguinal athero-clerotic disease, particularly the portion of the superfi-ial femoral artery that lies within the adductor canal ofhe thigh. Standard therapy is an exercise program andisk factor modification. Surgery is reserved for patientsn whom medical treatment fails. Endoluminal inter-ention coupled with aggressive proactive medical man-gement is replacing these conventional paradigms. En-ovascular therapy results in immediate symptom relief.nitial technical success rates of 90% to 95% have beenchieved for stenotic lesions, and rates of 80% to 95%or complete occlusions. Longterm patency is oftenuestioned, but modern series suggest it might be a du-able option, particularly if systemic risk factors are ag-ressively controlled. Anatomic failures do not correlateith clinical failures. This review outlines the currentanagement of superficial femoral artery atheroocclu-
ive disease.
linical problemeripheral arterial disease (PAD) of the lower extremitiesemains one of the often unrecognized manifestations ofystemic arteriosclerosis symptomatically affecting be-ween 3% and 7% of the population and up to one inive patients older than 75 years of age. It has a majoretrimental impact on quality of life1-3 and is an under-ecognized marker of multisystem vascular disease. Theisk of disease increases two- to threefold for every 10-
upported by grants HL07937, HL04161, and RR00044.
eceived January 4, 2005; Revised March 7, 2005; Accepted March 7, 2005.rom the Center for Vascular Disease, Division of Vascular Surgery, Depart-ent of Surgery (Davies); the Section of Interventional Radiology, Depart-ent of Radiology (Waldman); and the Department of Community and
reventive Medicine (Pearson); University of Rochester Medical Center,ochester, NY.orrespondence address: Mark G Davies, MD, PhD, University of Rochesteredical Center, 601 Elmwood Ave, Box 652, Rochester, NY 14642. email:
2752005 by the American College of Surgeons
ublished by Elsevier Inc.
ear increase in age after the age of 40 years,4-6 with meneveloping claudication about twice as commonly asomen. The Framingham Study estimates the incidencef PAD at 26.6 per 1,000 men and 13.3 per 1,000omen less than 65 years old, but in approximately 20er 1,000 men and women over 65 years of age.7,8 Mor-ality in claudicants is up to four times that in the non-laudicant age-adjusted population.9 Approximately5% of claudicants will die from heart disease: 10%rom a stroke and 10% from abdominal vascularathology.10-14 Less than 20% of claudicants will dierom a nonvascular cause. The strength of association iso strong that even an asymptomatic patient with alightly reduced ankle brachial index (ABI) of 0.9 has awofold relative risk of a coronary event.15
Anatomic distribution is important. Patients with iso-ated aortoiliac disease tend to be younger and have aower likelihood of preexisting coronary heart disease.hose with femoropopliteal disease, infragenicular dis-
ase, or multilevel disease tend to have the lowest ABInd the highest likelihood of coronary heart disease.9,16-21
his review will concentrate on the patient with femo-opopliteal disease.
natomyhe superficial femoral artery (SFA) is a muscular artery,hich is unique in that it is the longest artery in theody, and courses through the thigh in the musculardductor canal, exiting at a fixed point. The geometrynd elasticity of the SFA are markedly influenced by itsroximity to musculature, its continuous mobility, andts location between two joints. So it undergoes addi-ional mechanical forces not seen in other arteries. It hasnique elastic wall recoil properties that affect its con-ormability and resilience.22-24 The flow in the SFA is alsoifferent than in many vessels treated with angioplasty; itas high resistance characteristics and disturbed flow.25-27
onlaminar flow results in increased predisposition to
ISSN 1072-7515/05/$30.00doi:10.1016/j.jamcollsurg.2005.03.007

th
PAaarpsapwpntt
ebtmmfargrraoabtct
Csdm
lIcssbno
caeupiiant
wpccgAetdtrommtc
otsmwtshhf
276 Davies et al Femoropopliteal Atherosclerotic Disease J Am Coll Surg
he development of arteriosclerosis and intimalyperplasia.28,29
athophysiologylthough arteriosclerosis is a systemic disease affecting allrteries within the human body, the SFA, because of itsnatomy and physiology, is very susceptible to arterioscle-osis and can demonstrate all aspects of atheroscleroticlaque development. Arteriosclerosis may be defined as “apace occupying lesion or plaque of the inner coat of largerrteries that is focal, has a pattern of occurrence, is com-osed of an excess of fat, of an increased number of arteryall and inflammatory cells and their connective tissueroducts, and that may show calcification and ulceration,arrows the arterial lumen, may obstruct blood flowhrough the artery and may be associated with a localhrombus.”30,31
In atherogenesis, the arterial endothelium is consid-red chronically damaged by serum lipids, turbulentlood flow, and chronic inflammation. This injury leadso lipid accumulation and oxidation and the adhesion ofonocytes and platelets with time. The aggregation ofonocytes within the subendothelium constitutes the
irst stage of a “fatty streak.” These cells, in concert withdamaged or “activated” endothelium, synthesize and
elease growth factors and cytokines, leading to the mi-ration and proliferation of smooth muscle cells and theecruitment of additional blood cells, particularly mac-ophages, filled with oxidized lipids or “foam cells.”32 Ancellular core develops because of the toxic effects ofxidized lipoproteins. Oxidation of lipoproteins causesdditional tissue injury and increased accumulation oflood cells and lipids. With time, this process results inhe formation of an atheromatous plaque with a fibrousap, an acellular core, and a surrounding myoprolifera-ive and chronic inflammatory response.
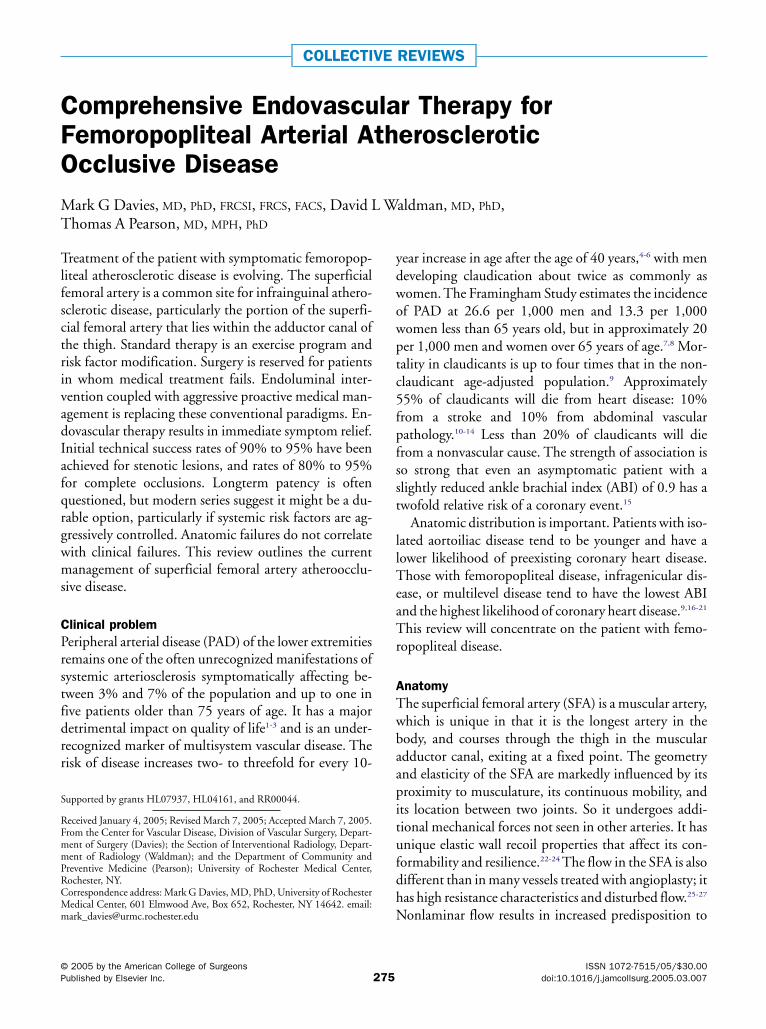
Reports by the Committee on Vascular Lesions of theouncil on Arteriosclerosis have established a new clas-
ification system for the various types of lesions (I to VI)escribed in arteriosclerosis (Fig. 1).30,31 In the older ter-
Abbreviations and Acronyms
ABI � ankle brachial indexPAD � peripheral artery diseasePTA � percutaneous transluminal angioplastySFA � superficial femoral artery
inology, the fatty streak consists of types I, II, and III o
esions; the intermediate or fibrofatty lesion, types III,V, and Va; and the fibrous plaque or advanced compli-ated lesion, types Vb, Vc, and VI.30 The SFA demon-trates all these lesions, but by the time the lesion isymptomatic (ie, manifested by claudication) the fi-rous plaque or advanced complicated lesion predomi-ates commonly with associated in situ thrombosis orcclusion.33
Fibrous plaques may be dynamic lesions that are in aontinuous state of flux or those that are not enlargingnd are considered stable or quiescent. Those that arexpanding or have thinning of the plaque cap representnstable or vulnerable lesions.30,31 The findings that thelaques are dynamic have increased the interest in med-cal therapies to induce stabilization, regression, or bothn plaque morphology. Plaque growth, whether slow orbrupt, is usually associated with surface erosion, inter-al hemorrhage, luminal thrombosis, a combination ofhese processes, or gradual vessel occlusion.30,31
The classic plaque represents a raised fibrofatty lesionith a necrotic core and a fibrous outer coat. Within thelaques are degenerating blood elements, foam cells,holesterol crystals, granulation tissue, smooth muscleells, myofibroblasts, capillaries, calcium, iron pigment,iant cells, mononuclear leukocytes, and necrotic debris.djacent to the internal elastic membrane, which oftenxhibits numerous focal disruptions and duplications,he plaque is frequently characterized by a prominenteposition of elastin and collagen in an onion skin pat-ern. The most hazardous component of the atheroscle-otic lesion is the plaque margin, where the fibrous capf the lesion is thinned and eroded by macrophages andetalloproteinases they secrete.34 Sudden death fromyocardial infarcts or acutely ischemic limbs are from
hese ruptures or fissures in the margins of the fibrousap.35
Numerous clinicopathologic investigations have dem-nstrated that surface weakness is the most common fea-ure of an unstable plaque.30,31,36 Microscopically, the ob-erved sites of injury span a broad morphologic range, frominimal surface erosions to lacerations that extend deepithin the plaque.The result of these injuries is exposure of
he luminal blood to a thrombogenic surface, setting thetage for acute thrombosis. Plaque rupture can also lead toemorrhage within the atheroma.34 Although the region ofemorrhage consists primarily of red blood cells, the sur-aces along the ruptured tract are often lined by aggregates
f platelets. Plaque hemorrhage can also develop by an en-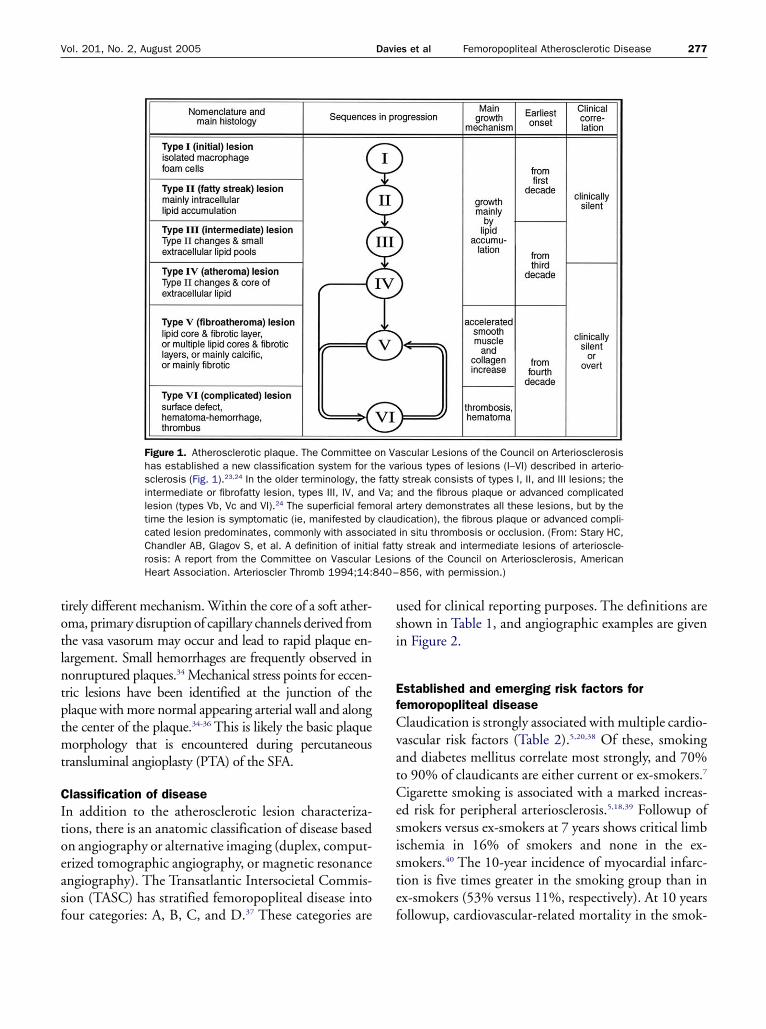
totlntptmt
CItoeasf
usi
EfCvatCesiste
840–
277Vol. 201, No. 2, August 2005 Davies et al Femoropopliteal Atherosclerotic Disease
irely different mechanism. Within the core of a soft ather-ma, primary disruption of capillary channels derived fromhe vasa vasorum may occur and lead to rapid plaque en-argement. Small hemorrhages are frequently observed inonruptured plaques.34 Mechanical stress points for eccen-ric lesions have been identified at the junction of thelaque with more normal appearing arterial wall and alonghe center of the plaque.34-36 This is likely the basic plaqueorphology that is encountered during percutaneous
ransluminal angioplasty (PTA) of the SFA.
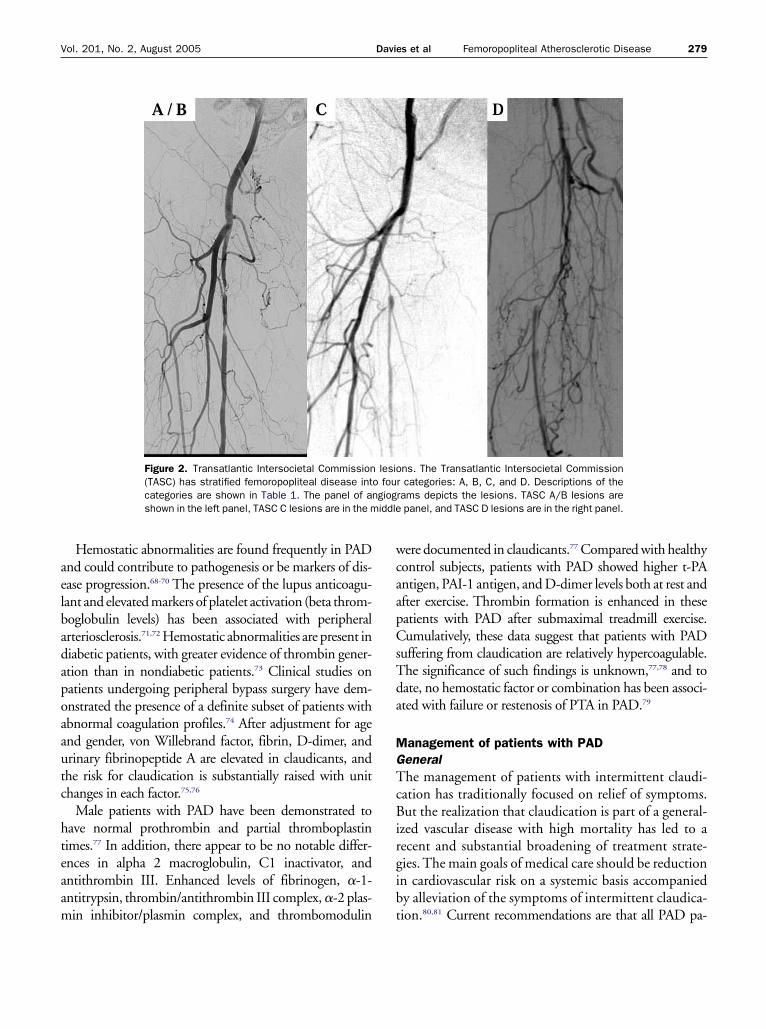
lassification of diseasen addition to the atherosclerotic lesion characteriza-ions, there is an anatomic classification of disease basedn angiography or alternative imaging (duplex, comput-rized tomographic angiography, or magnetic resonancengiography). The Transatlantic Intersocietal Commis-ion (TASC) has stratified femoropopliteal disease into
Figure 1. Atherosclerotic plaque. The Committeehas established a new classification system for tsclerosis (Fig. 1).23,24 In the older terminology, theintermediate or fibrofatty lesion, types III, IV, andlesion (types Vb, Vc and VI).24 The superficial femtime the lesion is symptomatic (ie, manifested bycated lesion predominates, commonly with assocChandler AB, Glagov S, et al. A definition of initiarosis: A report from the Committee on VascularHeart Association. Arterioscler Thromb 1994;14:
our categories: A, B, C, and D.37 These categories are f
sed for clinical reporting purposes. The definitions arehown in Table 1, and angiographic examples are givenn Figure 2.
stablished and emerging risk factors foremoropopliteal diseaselaudication is strongly associated with multiple cardio-
ascular risk factors (Table 2).5,20,38 Of these, smokingnd diabetes mellitus correlate most strongly, and 70%o 90% of claudicants are either current or ex-smokers.7
igarette smoking is associated with a marked increas-d risk for peripheral arteriosclerosis.5,18,39 Followup ofmokers versus ex-smokers at 7 years shows critical limbschemia in 16% of smokers and none in the ex-mokers.40 The 10-year incidence of myocardial infarc-ion is five times greater in the smoking group than inx-smokers (53% versus 11%, respectively). At 10 years
scular Lesions of the Council on Arteriosclerosisrious types of lesions (I–VI) described in arterio- streak consists of types I, II, and III lesions; theand the fibrous plaque or advanced complicatedrtery demonstrates all these lesions, but by the
dication), the fibrous plaque or advanced compli-in situ thrombosis or occlusion. (From: Stary HC,y streak and intermediate lesions of arterioscle-ns of the Council on Arteriosclerosis, American856, with permission.)
on Vahe va fattyVa;
oral aclau
iatedl fattLesio
ollowup, cardiovascular-related mortality in the smok-

in
hfshjthLLSem
hbanbmacptAdT
bh
wldwSfaCo
dsdctwnwmcc
rsvpahrc3darbatitdtmPT
TlT
A
B
C
D
T
278 Davies et al Femoropopliteal Atherosclerotic Disease J Am Coll Surg
ng group is more than 50%, three times that of theonsmoking group.Elevated cholesterol has been shown in the Framing-
am study to be a weak but important increased riskactor for claudication.7 Lipid profile abnormalities,uch as elevated serum triglyceride levels and reducedigh density lipoproteins, have been found in the ma-
ority of patients in studies of intermittent claudica-ion,41 and there is a strong inverse relationship betweenigh-density lipoprotein levels and claudication severity.42
ipoprotein (a) levels have been shown to correlate withDL, cholesterol, fibrinogen levels, and PAD severity.43
tudies of lipid-lowering drugs and subsequent vascularvents have focused mainly on coronary disease as aore frequent end point.It has been estimated that 50% of diabetic patients
ave evidence of PAD.44 Diabetic patients suffer fromoth micro- and macrovascular disease manifested oftens ischemia, but more frequently as motor or sensoryeuropathies.45 But a study of 100 consecutive nondia-etic patients attending a vascular clinic showed abnor-al glucose tolerance tests in 40%,46 despite the fact that
ll 40 patients had normal random or fasting blood glu-ose levels. There are three clues that might help identifyatients who have a diabetic tendency: first, a distal dis-ribution of PAD in a diabetic pattern; second, a raisedBI in the presence of symptoms of intermittent clau-ication; and third, a diabetic picture in the lipid profile.
able 1. Transatlantic Intersocietal Commission Morpho-ogic Stratification of Femoropopliteal LesionsASC classification Characteristics
Single stenosis, � 3 cm, of the superficialfemoral artery or the popliteal arterySingle stenosis, 3 to 10 cm in length, notinvolving the distal popliteal arteryHeavily calcified stenoses up to 3 cm inlengthMultiple lesions, each less than 3 cm(stenoses or occlusions)Single or multiple lesions in the absence ofcontinuous tibial runoff to improve inflowfor distal surgical bypassSingle stenosis or occlusion longer than 5 cmMultiple stenoses or occlusions each 3 to 5cm, with or without heavy calcificationComplete common femoral artery orsuperficial femoral artery occlusions orcomplete popliteal and proximal trifurcationocclusions
ASC, Transatlantic Intersocietal Commission.
he relative risk for developing PAD in the presence of t
oth smoking and diabetes mellitus is three- to fourfoldigher than with the presence of one factor alone.5,20
Markers of inflammation have been associatedith development of arteriosclerosis and cardiovascu-
ar events.47,48 In particular, C-reactive protein is in-ependently associated with PAD, even in patientsith normal lipid levels.49,50 In the Physicians Healthtudy, an elevated C-reactive protein level was a riskactor for development of symptomatic PAD and also
risk for peripheral revascularization.51 High-reactive protein levels are independent predictorsf poor PTA outcomes after revascularization.52
Elevated plasma homocysteine levels appear to be in-ependent risk factors for PAD.53-55 Although B-vitaminupplements can lower homocysteine levels, the evi-ence for benefits from supplementation in preventingardiovascular events is lacking.56,57 There are sugges-ions that elevated homocysteine levels are associatedith restenosis after percutaneous transluminal coro-ary angioplasty.58,59 One study suggests that treatmentith a combination of folate (1 mg), vitamin B12 (400cg), and pyridoxine (10 mg) may reduce the rate of
oronary restenosis and the need for revascularizationompared with placebo controls.60
Platelets and their products are known to play a keyole in arteriosclerosis. Platelet aggregability has beenhown to be 30% higher in patients with peripheralascular disease even if they are asymptomatic.61,62 Anti-latelet therapy has, not surprisingly, shown consider-ble reductions in fatal and nonfatal vascular events inigh-risk vascular patients, eg, claudicants.63-65 The riskeduction for antiplatelet therapy versus placebo in thelaudicant population was 46% for nonfatal stroke,2% for nonfatal myocardial infarction, and 20% foreath from a vascular cause. Even low risk patients onntiplatelet therapy have shown small, but considerable,isk reduction. Claudication progression, as measuredy angiography, has also been shown to be inhibited inntiplatelet-treated patients.66 A randomized, blindedrial of clopidogrel versus aspirin in patients at risk ofschemic events (CAPRIE) had a large subgroup of pa-ients with atherosclerotic vascular disease.67 Clopi-ogrel was shown to bring about a small, but substan-ially greater reduction in vascular morbidity andortality than aspirin, with a relatively greater effect in
AD patients than other vascular disease subgroups.here were no major differences in safety profiles be-
ween the two drugs.
aelbadapoaautc
hteaam
wcaapCsTda
MGTcBirgib
iddle
279Vol. 201, No. 2, August 2005 Davies et al Femoropopliteal Atherosclerotic Disease
Hemostatic abnormalities are found frequently in PADnd could contribute to pathogenesis or be markers of dis-ase progression.68-70 The presence of the lupus anticoagu-ant and elevated markers of platelet activation (beta throm-oglobulin levels) has been associated with peripheralrteriosclerosis.71,72 Hemostatic abnormalities are present iniabetic patients, with greater evidence of thrombin gener-tion than in nondiabetic patients.73 Clinical studies onatients undergoing peripheral bypass surgery have dem-nstrated the presence of a definite subset of patients withbnormal coagulation profiles.74 After adjustment for agend gender, von Willebrand factor, fibrin, D-dimer, andrinary fibrinopeptide A are elevated in claudicants, andhe risk for claudication is substantially raised with unithanges in each factor.75,76
Male patients with PAD have been demonstrated toave normal prothrombin and partial thromboplastinimes.77 In addition, there appear to be no notable differ-nces in alpha 2 macroglobulin, C1 inactivator, andntithrombin III. Enhanced levels of fibrinogen, �-1-ntitrypsin, thrombin/antithrombin III complex, �-2 plas-
Figure 2. Transatlantic Intersocietal Commission(TASC) has stratified femoropopliteal disease intcategories are shown in Table 1. The panel of anshown in the left panel, TASC C lesions are in the m
in inhibitor/plasmin complex, and thrombomodulin t
ere documented in claudicants.77 Compared with healthyontrol subjects, patients with PAD showed higher t-PAntigen, PAI-1 antigen, and D-dimer levels both at rest andfter exercise. Thrombin formation is enhanced in theseatients with PAD after submaximal treadmill exercise.umulatively, these data suggest that patients with PAD
uffering from claudication are relatively hypercoagulable.he significance of such findings is unknown,77,78 and toate, no hemostatic factor or combination has been associ-ted with failure or restenosis of PTA in PAD.79
anagement of patients with PADeneralhe management of patients with intermittent claudi-
ation has traditionally focused on relief of symptoms.ut the realization that claudication is part of a general-
zed vascular disease with high mortality has led to aecent and substantial broadening of treatment strate-ies. The main goals of medical care should be reductionn cardiovascular risk on a systemic basis accompaniedy alleviation of the symptoms of intermittent claudica-
ns. The Transatlantic Intersocietal Commissionr categories: A, B, C, and D. Descriptions of therams depicts the lesions. TASC A/B lesions are
panel, and TASC D lesions are in the right panel.
lesioo fougiog
ion.80,81 Current recommendations are that all PAD pa-

TdR
S
B
D
L
P
W
D
A
280 Davies et al Femoropopliteal Atherosclerotic Disease J Am Coll Surg
able 2. Optimal Medical Management in the Patient with Peripheral Artery Disease: Goals, Interventions, and Recommen-ationsisk intervention and goals Recommendations
mokingGoal: Complete cessation. No exposure to
environmental tobacco smoke.
Ask about tobacco use status at every visit. In a clear, strong, and personalizedmanner, advise every tobacco user to quit. Assess the tobacco user’swillingness to quit. Assist by counseling and developing a plan for quitting.Arrange followup, referral to special programs, or pharmacotherapy. Urgeavoidance of exposure to secondhand smoke at work or home.
lood pressure controlGoal: � 140/90 mmHg: � 130/85 mmHg if renal
insufficiency or heart failure is present; or � 130/80mmHg if diabetes is present.
Promote healthy lifestyle modification. Advocate weight reduction; reductionof sodium intake; consumption of fruits, vegetables, and low-fat diaryproducts; moderation of alcohol intake; and physical activity in persons withblood pressure of � 130 mmHg systolic or 80 mmHg diastolic. For personswith renal insufficiency or heart failure, initiate drug therapy if bloodpressure is � 140/90 mmHg if 6 to 12 mo of lifestyle modification is noteffective, depending on the number of risk factors present. Add bloodpressure medications, individualized to other patient requirements andcharacteristics (eg, age, race, need for drugs with specific benefits).
ietary intakeGoal: An overall healthy eating pattern.
Advocate consumption of a variety of fruits, vegetables, grains, low-fat ornonfat dairy products, fish, legumes, poultry, and lean meats. Match energyintake with energy needs and make appropriate changes to achieve weightloss when indicated. Modify food choices to reduce saturated fats (� 10% ofcalories), cholesterol (� 300 mg/d), and trans-fatty acids by substitutinggrains and unsaturated fatty acids from fish, vegetables, legumes, and nuts.Limit salt intake to � 5 g/d. Limit alcohol intake (� 2 drinks/d in men, � 1drink/d in women) among those who drink.
ipid managementPrimary goal: LDL-C � 70 mg/dL.Secondary goal: If triglycerides � 200 mg/dL,
non HDL � 30 mg/dL.Other targets: triglycerides � 150 mg/dL, HDL � 40
mg/dL in men, � 50 mg/dL in women.
Initiate lifestyle changes consisting of dietary modification, including use ofplant sterols (� 2 g/d) and increased fiber. Rule out secondary causes. Startdrugs and advance dose to bring LDL-C to goal. Usually statin orcombination of drugs with a statin. If non HDL-C elevated, consider lifestylechanges, or niacin or fibrates. If HDL-C low, consider niacin or fibrates.
hysical activityGoal: At least 30 min of moderate-intensity physical
activity on most (and preferably all) days of theweek.
If cardiovascular, respiratory, metabolic, orthopaedic, or neurologic disordersare suspected, or if patient is middle-aged or older and is sedentary, consultphysician before initiating vigorous exercise program. Moderate-intensityactivities (40% to 60% of maximum capacity) are equivalent to a brisk walk(15–20 min per mile). Additional benefits are gained from vigorous-intensityactivity (� 60% of maximum capacity) for 20–40 min on 3–5 d/wk.Recommend resistance training with 8–10 different exercises, 1–2 sets perexercise, and 10–15 repetitions at moderate intensity � 2 d/wk. Flexibilitytraining and an increase in daily lifestyle activities should complement thisregimen.
eight managementGoal: Achieve and maintain desirable weight body
mass index 18.5–24.9 kg/m2. When body massindex is � 25 kg/m2, waist circumference at iliaccrest level � 40 inches in men, � 35 inches inwomen.
Initiate weight-management program through caloric restriction andincreased caloric expenditure as appropriate. For overweight or obese persons,reduce body weight by 10% in first year of therapy.
iabetes managementGoals: Normal fasting plasma glucose (� 110 mg/dL)
and near normal HbA1c (� 7%).
Initiate appropriate hypoglycemic therapy to achieve near-normal fastingplasma glucose or as indicated by near-normal HbA1c. First step is diet andexercise. Second-step therapy is usually oral hypoglycemic drugs;sulfonylureas and/or metformin with ancillary use of acarbose andthiazolidinediones. Third-step therapy is insulin. Treat other risk factorsmore aggressively (eg, change blood pressure goal to � 130/80 mmHg andLDL-C goal to � 100 mg/dL).
spirin Patients should be on 81 mg of aspirin/d unless contraindicated. Clopedigrel
Goal: All patients on an antiplatelet agent. may also be considered at 75 mg/d.
tehd(
SScwpitcodh1aian
ichwrcspw
EEimfacgip3mT5ct
areft
ipoleatumwtigact
LPsfNoc(lAaHa(cptsapssLt
281Vol. 201, No. 2, August 2005 Davies et al Femoropopliteal Atherosclerotic Disease
ients should receive antiplatelet therapy, stop smoking,xercise, and be screened and treated for hyperlipidemia,ypertension, diabetes, and hypercoaguability in accor-ance with national guidelines and community standardsTable 2).
mokingmoking cessation is a priority in the addicted claudi-ant. More than 75% of claudicants who already smokeill have tried and failed to quit smoking. Up to 25% ofatients will try to follow clinical advice to stop smok-ng, but more than 75% of these will recommence in lesshan 3 months.82 With medical advice alone, only 5% oflaudicants will have longterm success in quitting.83 Nic-tine replacement therapy such as chewing gum, trans-ermal patches, nasal sprays, and inhalers are effective inelping patients stop. A metaanalysis of trials shows a.5- to 2-fold increase in cessation rate, with nasal spraynd inhaled nicotine showing most success.84 Combin-ng nicotine replacement therapy with treatments suchs an inhaler with a patch increases the success rate toearly 20% at 1 year.85
Amfebutamone or bupropion (Zyban, GlaxoSmithKline)s an atypical antidepressant that has recently been li-ensed as an aid to smoking cessation. It reduces theypertensive, cardiac, and other side effects of nicotineithdrawal. Trials suggest up to 30% 1-year cessation
ates, with a dose-related response.86 The goals for theare of these patients should be accessible specialistmokers’ clinics, where counseling, education, and sup-ort by specialists in tobacco cessation can be combinedith appropriate pharmacologic treatment.87
xercisexercise therapy produces considerable improvements
n the symptoms of claudicants.88-90 Physical improve-ents gained from an exercise regimen are both multi-
actorial and systemic.91 These include compensatorydaptations and redistribution of peripheral blood flow,hanges in oxidative capacity of skeletal muscle withreater use of oxygen, changes in blood composition,nhibition of additional atherosclerotic disease, and im-rovements in the cardiorespiratory system.92 A study of4 claudicants after a supervised exercise regimen over 6onths found a doubling of pain-free walking distance.1
here was also a mean drop in systolic blood pressure of.7% and a fall in mean cholesterol levels of 5.2%. Con-erns about claudicants developing an inflammatory-
ype response during walking, which may be harmful, eppear unfounded. Regular exercise training produces aeduction in the inflammatory markers associated withndothelial damage.93 So evidence suggests that patientsollowing an exercise regimen improve both claudica-ion distance and cardiovascular risk profile.
Three separate metaanalyses of exercise regimen trialsdentified similar components in the most successfulrograms.94-98 Common factors were exercise durationf greater than 30 minutes per session, frequency of ateast three sessions per week, walking as the mode ofxercise, exercising to near maximal pain tolerance, andprogram lasting 6 months or longer. In claudicants,
here appears to be equal benefit if the patient undergoespper limb exercise or lower limb exercise. Pain-free andaximum walking distance improvements were seenith both forms of exercise.97 This is likely a function of
otal body conditioning because all exercise should givemprovements in cardiovascular function; walking willive additional adaptive benefits in the muscle groupsffected by claudication. The role of supervised exerciselasses versus best exercise advice given in clinic has stillo be determined on a large trial basis.
ipid lowering therapyatients with symptomatic peripheral vascular diseasehould be considered within the high risk groups as de-ined by the Adult Treatment Panel III (ATP-III) of theational Cholesterol Education Program.99,100 The goal
f lipid lowering therapy should be set at a LDL-holesterol level of � 70 mg/dL. Hypertriglyceridemia� 200 mg/dL) is also prevalent in the peripheral vascu-ar disease population and should be treated.101 Thedult Treatment Panel III identifies the sum of LDLnd very-low density lipoprotein (VLDL), termed non-DL cholesterol, (� [cholesterol]-[HDL]) as a second-
ry target for therapy in patients with high triglycerides� 200 mg/dL). The goal for these patients is non-HDLholesterol of � 30 mg/dL.99,100 Despite the known lipidrofile abnormalities in claudicants and the proved andheoretic advantages of lipid-lowering drugs,46,99,102 fewtudies have targeted relief of claudication symptoms asn end point.103,104 A recent review by the Cochraneeripheral vascular disease group identified only sevenuitable randomized trials of lipid lowering therapy (nottatins) in patients with lower limb arteriosclerosis.104,105
ipid lowering therapy results in a marked but unimpor-ant reduction in mortality and no change in nonfatal
vents. Two of these trials did demonstrate a substantial
ra
ods3peiwo
PMcmawfwpbaswaidcc
GMttdiifb(FgdppRC
rinso
EBahtatmlp3tstoBPontcitsselb
PAtoatamptada
282 Davies et al Femoropopliteal Atherosclerotic Disease J Am Coll Surg
eduction in disease progression as quantified byngiography.105
The role of lipid lowering regimens in the treatmentf claudication has recently been readdressed. The Scan-inavian Simvastatin Survival Study (4S) had demon-trated that subjects randomized to simvastatin had a8% reduction in new or worsening claudication com-ared with subjects randomized to placebo,106 and sev-ral recent studies demonstrated improved walking abil-ty in patients treated with statin compared with patientsithout a statin, independent of cholesterol levels andther potential confounders.107-109
harmacologic therapyultiple drugs and regimens have been tested in claudi-
ation; five oral drugs have been licensed for the treat-ent of claudication. Two of these, inositol nicotinate,
nd cinnarizine, have not been established as effectivehen compared with placebo. Pentoxifylline (oxypenti-
ylline) has been shown, in a metaanalysis, to improvealking distance by 29 meters over placebo (the im-rovement was approximately 50% compared withaseline in the placebo group; pentoxifylline providedn additional 30% improvement). Naftidrofuryl hashown an increase in walking distance of up to 30%hen compared with a placebo at 6 months. Cilostazol,phosphodiesterase inhibitor, has shown a 40% increase
n walking distance at 3 months and has become therug of choice in the pharmacologic management oflaudication.98,110,111 Oral drug therapy should always beombined with exercise and risk factor modification.
ene therapyolecular therapies to induce angiogenesis are appealing in
he claudicant population because the ischemia is subacute,ime for angiogenesis to occur is available, and collateralevelopment is associated with improved symptoms and
ncreased walking distance. Molecular therapies that resultn increased levels of vascular endothelial growth factor,ibroblast growth factor, and hepatocyte growth factor haveeen used in claudication populations.112 The RAVE TrialRegional Angiogenesis with Vascular Endothelial Growthactor in Peripheral Arterial Disease) concluded that a sin-le unilateral IM administration of adenoviral vascular en-othelial growth factor121 was not associated with im-roved treadmill exercise performance or quality of life overlacebo.113 The most recentTherapeutic Angiogenesis withecombinant Fibroblast Growth Factor-2 for Intermittent
laudication (TRAFFIC) study has shown that intraarte- aial fibroblast growth factor will result in a considerablencrease in walking time at 90 days.114 These therapies areot readily available and have not been compared withtandard aggressive medical and endoluminal managementf claudication.
ndoluminal proceduresecause of the introduction of PTA in 1964 by Dotternd Judkins115 and its refinements by Gruntzig,116 PTAas grown into a viable alternative to surgical interven-ion in most arterial beds. The diseased SFA may bepproached with a repertoire of techniques. The conven-ional approach is to access the SFA in an antegradeanner and negotiate a guide wire through the target
esion before performing PTA (Fig. 3A). A similar ap-roach can be achieved in short segment occlusions (Fig.B). An antegrade transfemoral approach has initialechnical success rates of 90% to 95% for stenotic le-ions and 80% to 95% for complete occlusions. Use ofhe retrograde transpopliteal approach can increase theriginal technical success rate by an additional 6%.117
ut longer occlusions require additional techniques.ercutaneous intentional extraluminal recanalization,118
r subintimal angioplasty or Bolia angioplasty, is a tech-ique used to recannulize chronic occlusions.119 It inten-ionally achieves a dissection plane in the vessel wall toircumvent a total occlusion. Gaining luminal accessnto the distal target vessel remains the Achilles’ heel ofhis approach. Recently, the use of intravascular ultra-ound to identify and guide a needle from the false dis-ected lumen into the true lumen has been shown to beffective. Percutaneous intentional extraluminal recana-ization through the retrograde popliteal approach cane achieved in up to 80% of patients (Fig. 3C).120
athology of angioplasty and stentingngioplasty is a controlled injury to the vessel wall. Al-
hough there is no apparent loss of cells from the mediaf the vessel wall after balloon injury, studies show thatpproximately 20% of total wall DNA is lost. Some ofhis loss is of endothelial origin, but a considerablemount reflects injury to the underlying medial smoothuscle cells.121 In the immediate aftermath of angio-
lasty, programmed cell death, or apoptosis, can be iden-ified at 1 to 2 hours and disappears by 4 hours.122 Nopoptosis can be identified in the wall after injury at 3ays but by day 7, 50% of the cells again show signs ofpoptosis and by day 14, the number of apoptotic cells is
gain markedly decreased.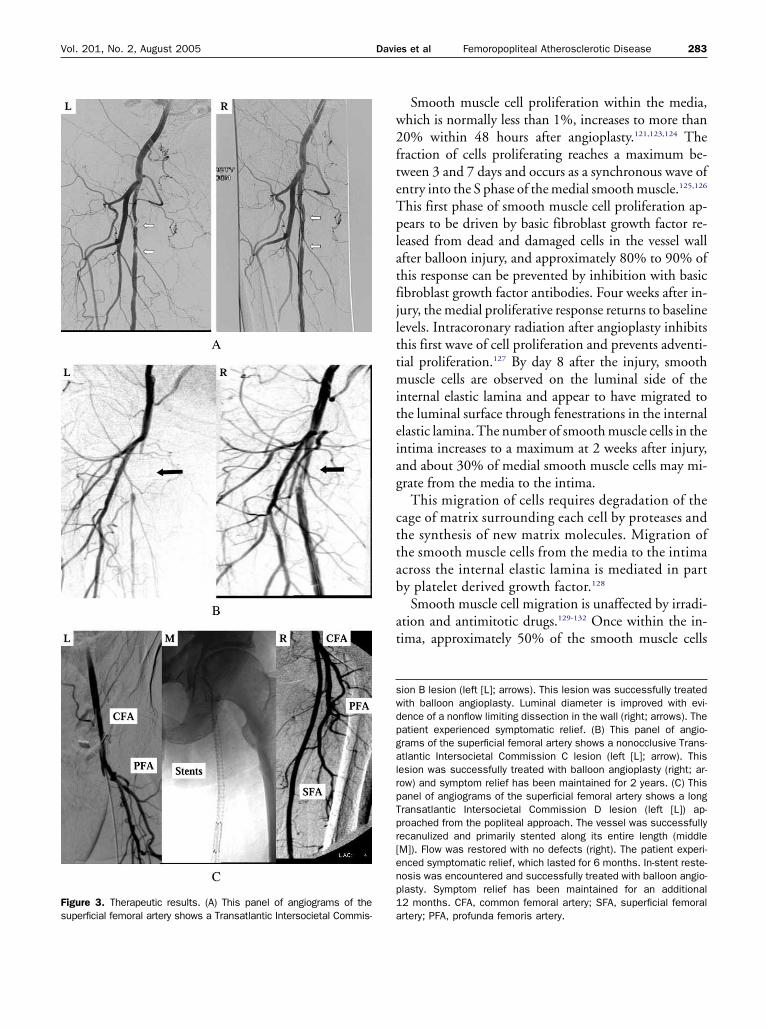
w2fteTplatfjlttmiteiag
cttab
at
swdpgalrpTpr[enp1a
Fs
283Vol. 201, No. 2, August 2005 Davies et al Femoropopliteal Atherosclerotic Disease
Smooth muscle cell proliferation within the media,hich is normally less than 1%, increases to more than0% within 48 hours after angioplasty.121,123,124 Theraction of cells proliferating reaches a maximum be-ween 3 and 7 days and occurs as a synchronous wave ofntry into the S phase of the medial smooth muscle.125,126
his first phase of smooth muscle cell proliferation ap-ears to be driven by basic fibroblast growth factor re-
eased from dead and damaged cells in the vessel wallfter balloon injury, and approximately 80% to 90% ofhis response can be prevented by inhibition with basicibroblast growth factor antibodies. Four weeks after in-ury, the medial proliferative response returns to baselineevels. Intracoronary radiation after angioplasty inhibitshis first wave of cell proliferation and prevents adventi-ial proliferation.127 By day 8 after the injury, smoothuscle cells are observed on the luminal side of the
nternal elastic lamina and appear to have migrated tohe luminal surface through fenestrations in the internallastic lamina. The number of smooth muscle cells in thentima increases to a maximum at 2 weeks after injury,nd about 30% of medial smooth muscle cells may mi-rate from the media to the intima.
This migration of cells requires degradation of theage of matrix surrounding each cell by proteases andhe synthesis of new matrix molecules. Migration ofhe smooth muscle cells from the media to the intimacross the internal elastic lamina is mediated in party platelet derived growth factor.128
Smooth muscle cell migration is unaffected by irradi-tion and antimitotic drugs.129-132 Once within the in-ima, approximately 50% of the smooth muscle cells
ion B lesion (left [L]; arrows). This lesion was successfully treatedith balloon angioplasty. Luminal diameter is improved with evi-ence of a nonflow limiting dissection in the wall (right; arrows). Theatient experienced symptomatic relief. (B) This panel of angio-rams of the superficial femoral artery shows a nonocclusive Trans-tlantic Intersocietal Commission C lesion (left [L]; arrow). Thisesion was successfully treated with balloon angioplasty (right; ar-ow) and symptom relief has been maintained for 2 years. (C) Thisanel of angiograms of the superficial femoral artery shows a longransatlantic Intersocietal Commission D lesion (left [L]) ap-roached from the popliteal approach. The vessel was successfullyecanulized and primarily stented along its entire length (middleM]). Flow was restored with no defects (right). The patient experi-nced symptomatic relief, which lasted for 6 months. In-stent reste-osis was encountered and successfully treated with balloon angio-lasty. Symptom relief has been maintained for an additional2 months. CFA, common femoral artery; SFA, superficial femoral
rtery; PFA, profunda femoris artery.igure 3. Therapeutic results. (A) This panel of angiograms of theuperficial femoral artery shows a Transatlantic Intersocietal Commis-

ps7b1lcadhot
tdsao1iiAIawtewrafst
sMuttssjpdlarc
wcmlhwmpr
ITsiitsdpoldlopdcttt
hlcimvalApmtiaas
284 Davies et al Femoropopliteal Atherosclerotic Disease J Am Coll Surg
roliferate (a second phase of mitosis). In the intima, aecond phase of cellular proliferation is first noted at dayand reaches a maximum at 14 days before returning toaseline by 28 days.126 But it may continue for up to2 weeks in areas where reendothelialization takes
onger to complete. This second phase of smooth muscleell replication in the intima appears to be mediated byutocrine and paracrine factors and remains poorly un-erstood. It also appears that the thickness of the intimalyperplasia peaks within 1 month, and its rapid devel-pment is from both cellular elements and the produc-ion of proteoglycans.
Associated with the changes in the intima and media,here are substantial changes in the adventitia, as evi-enced by increased cell proliferation and growth factorynthesis in the adventitia relative to the media afterngioplasty. In the adventitia, there is a marked infiltratef cells termed “myofibroblasts” by day 2, which by day4, can represent up to 50% of cells within thentima.133,134 The presence of myofibroblasts is commonn wound healing and leads to contraction of the wound.
similar phenomenon may occur in the healing vessel.njured vessels can undergo chronic elastic recoil or neg-tive remodeling, resulting in loss of luminal dimensionsithout an additional increase in neointimal area. Re-
rieved atherectomy material from primary and rest-notic lesions has shown that the proportion of cells,hich can be demonstrated to be proliferating in the
estenotic lesion, is low,135 but that migratory activitynd collagen synthesis of human smooth muscle cellsrom the restenotic lesions are greatly elevated, stronglyupporting the concept that remodeling is important inhe final determination of luminal diameter.136,137
The degree of intimal hyperplasia that develops in a ves-el is dependent on the length and depth of the injury.138
inimal intimal proliferation occurs when the media isninjured, but intimal hyperplasia increases in propor-ion to the depth of the medial injury, indicating thathe proliferative response reflects the direct injury to themooth muscle cells.139,140 In addition, distention ofmooth muscle cells without severe endothelial cell in-ury has been shown to result in smooth muscle cellroliferation. The length of the injury influences theuration of the reendothelialization process. Reendothe-
ialization occurs from the margins of the denuded areand possibly from the endothelial cells of the vasa vaso-um. The longer there is an incomplete endothelial cell
overing, the greater time the smooth muscle cells areithout the modulating influence of the endothelialells, and the longer the replication phases of the smoothuscle cells will be.121,123 After deep vessel wall injury,
uminal narrowing may be less dependent on intimalyperplasia formation and more dependent on vesselall remodeling.141 Medial damage is accompanied by aassive adventitial cell proliferation,142 which, in time,
rovides cells capable of contraction and negativeemodeling.
ntravascular stentshe biology of in-stent restenosis is different than that
een after balloon angioplasty.143 A stent is generally usedf the result of balloon angioplasty is technically unsat-sfactory or if there is arterial occlusion, immediate elas-ic recoil, flow-limiting dissection, or restenosis. The re-ponse of a vessel to a stent is dependent on the stentesign, length, composition, delivery system, and de-loyment technique.144 In-stent restenosis is classifiedn the basis of length of restenosis in relation to stentedength. Four categories of in-stent restenosis have beenefined: focal (� 10 mm length), diffuse (� 10 mm
ength) proliferative (� 10 mm length and extendingutside the stent), and occlusion.145 After balloon angio-lasty, there is thrombus formation, intimal hyperplasiaevelopment, elastic recoil, and negative remodeling. Inontrast, after stent placement, elastic recoil and nega-ive remodeling are eliminated146 and thrombus forma-ion followed by intimal hyperplasia development arehe main contributors to in-stent restenosis.147
Patients with diabetes and earlier restenosis have aigher rate of in-stent restenosis,148 and there is a corre-
ation with prolonged in-stent thrombus and hypergly-emia.149 Stent placement in a vessel results in general-zed injury to the length of the vessel exposed and in
ore focal injures at the areas of strut placement. Intra-ascular ultrasound has demonstrated that stents do notlways completely oppose the vessel wall along its entireength, resulting in uneven injury along its length.146
fter stent placement, the surface of the metal im-lanted into the vessel is covered by a strongly adherentonolayer of protein within 5 seconds. After 1 minute
he surface is covered by fine layers of proteins, predom-nantly fibrinogen.150 The holes between the stent wiresre filled with thrombus and the adherence of plateletsnd leukocytes is enhanced by disturbance of electro-tatic equilibrium.151,152
The basic mechanisms of smooth muscle cell prolif-
eapbompavct
ONfdat5T1tvoda
tltPrsuwtlt
tt
ffmcwiitlc
uiira
Forlp
Tnpo
T
ASAD
TVC
A
HC
S
285Vol. 201, No. 2, August 2005 Davies et al Femoropopliteal Atherosclerotic Disease
ration and migration after stent placement are the sames those after balloon injury.153 The intimal hyperplasicrocess in a stent is more prolonged and robust than in aalloon-injured artery and is proportional to the depthf injury the recipient vessel sustains154 and the inflam-atory response induced.155 It can often be much more
ronounced at the ends than in the body of the stent. Inddition, the adventitial response is prolonged, with ad-entitial giant cell body formation noted. Stents preventhronic elastic recoil and cause progressive atrophy ofhe media.156
utcomesational reporting standards for vascular procedures de-
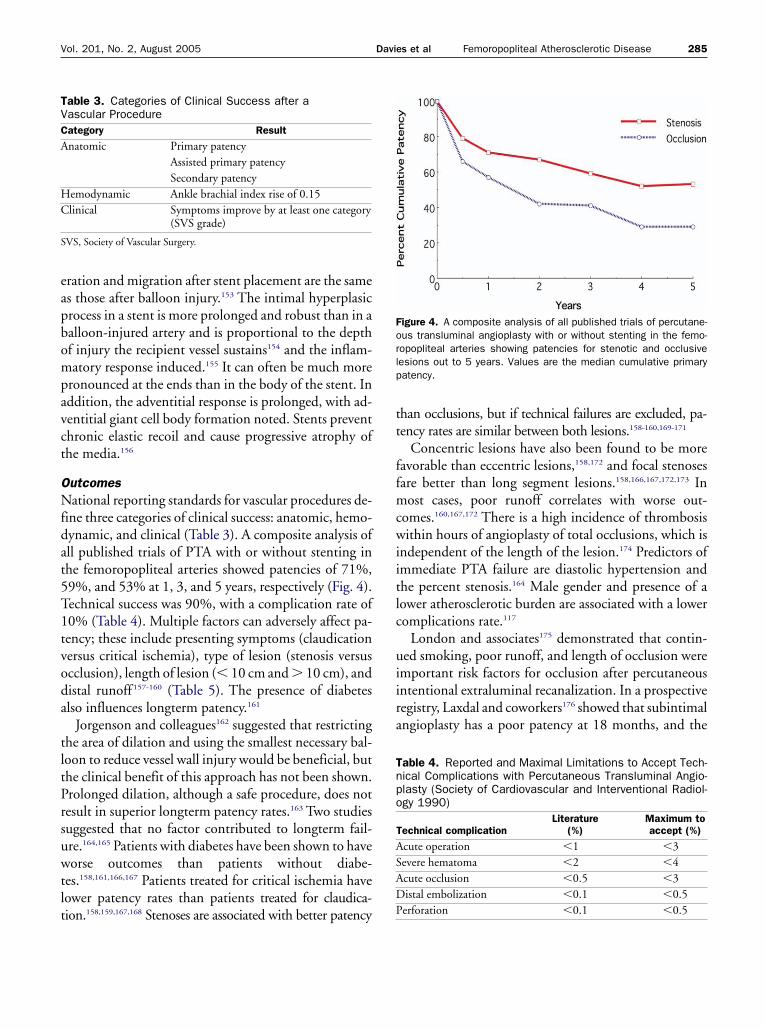
ine three categories of clinical success: anatomic, hemo-ynamic, and clinical (Table 3). A composite analysis ofll published trials of PTA with or without stenting inhe femoropopliteal arteries showed patencies of 71%,9%, and 53% at 1, 3, and 5 years, respectively (Fig. 4).echnical success was 90%, with a complication rate of0% (Table 4). Multiple factors can adversely affect pa-ency; these include presenting symptoms (claudicationersus critical ischemia), type of lesion (stenosis versuscclusion), length of lesion (� 10 cm and � 10 cm), andistal runoff157-160 (Table 5). The presence of diabeteslso influences longterm patency.161
Jorgenson and colleagues162 suggested that restrictinghe area of dilation and using the smallest necessary bal-oon to reduce vessel wall injury would be beneficial, buthe clinical benefit of this approach has not been shown.rolonged dilation, although a safe procedure, does notesult in superior longterm patency rates.163 Two studiesuggested that no factor contributed to longterm fail-re.164,165 Patients with diabetes have been shown to haveorse outcomes than patients without diabe-
es.158,161,166,167 Patients treated for critical ischemia haveower patency rates than patients treated for claudica-
able 3. Categories of Clinical Success after aascular Procedureategory Result
natomic Primary patencyAssisted primary patencySecondary patency
emodynamic Ankle brachial index rise of 0.15linical Symptoms improve by at least one category
(SVS grade)
VS, Society of Vascular Surgery.
ion.158,159,167,168 Stenoses are associated with better patency P
han occlusions, but if technical failures are excluded, pa-ency rates are similar between both lesions.158-160,169-171
Concentric lesions have also been found to be moreavorable than eccentric lesions,158,172 and focal stenosesare better than long segment lesions.158,166,167,172,173 Inost cases, poor runoff correlates with worse out-
omes.160,167,172 There is a high incidence of thrombosisithin hours of angioplasty of total occlusions, which is
ndependent of the length of the lesion.174 Predictors ofmmediate PTA failure are diastolic hypertension andhe percent stenosis.164 Male gender and presence of aower atherosclerotic burden are associated with a loweromplications rate.117
London and associates175 demonstrated that contin-ed smoking, poor runoff, and length of occlusion were
mportant risk factors for occlusion after percutaneousntentional extraluminal recanalization. In a prospectiveegistry, Laxdal and coworkers176 showed that subintimalngioplasty has a poor patency at 18 months, and the
igure 4. A composite analysis of all published trials of percutane-us transluminal angioplasty with or without stenting in the femo-opopliteal arteries showing patencies for stenotic and occlusiveesions out to 5 years. Values are the median cumulative primaryatency.
able 4. Reported and Maximal Limitations to Accept Tech-ical Complications with Percutaneous Transluminal Angio-lasty (Society of Cardiovascular and Interventional Radiol-gy 1990)
echnical complicationLiterature
(%)Maximum toaccept (%)
cute operation �1 �3evere hematoma �2 �4cute occlusion �0.5 �3istal embolization �0.1 �0.5
erforation �0.1 �0.5
mo
adittvmpsyd
ulatPasuta
o(
oikifdSfttsdidd5pf
cisogastcpsbuad1r1
PTbiaPbao
To
286 Davies et al Femoropopliteal Atherosclerotic Disease J Am Coll Surg
ajor factors contributing to occlusion are the presencef diabetes and critical ischemia.
If intravascular ultrasonography is used immediatelyfter PTA, the extent of dissection, free lumen area, andiameter are predictive factors of patency.177 Factors of
ntravascular ultrasound that favor improved patency arehe absence of calcification, dissection or plaque rup-ure, and a residual stenosis of less than 30%.178 Intra-ascular ultrasound predictor of failure at 1 and 6onths is initial residual stenosis after PTA.179 Similarly,
ronounced residual stenosis (� 30%) on duplex ultra-ound 1 day after PTA correlates with failure within 1ear; unfortunately, the converse is not true; a normaluplex at � 1 day cannot predict failure within 1 year.180
Plaque area increase and vascular remodeling contrib-te to lumen area change after PTA of the femoropop-
iteal artery on intravascular ultrasound study.181 Capeknd coauthors158 and Hunink and colleagues159 showedhat repeat PTA has similar patency as does primaryTA; in contrast, several reports showed that repeat SFAngioplasty has a low patency (� 20% at 3 years) anduggested that bypass may be more beneficial.182-185 Fail-re of PTA is not associated with worsening of the pa-ient’s clinical condition, and 19% will be recannulizedt a second sitting.186,187
Hemodynamic success is defined as an increase in ABIf 0.15. Immediate and longterm hemodynamic success
able 5. Factors Influencing the Patency of Superficial Fem-ral Artery Interventions
Factors
Positive� 2-cm lesionsNoncalcified lesions� 3.5-mm diameter vesselNo use of thrombolyticsNonsmokersLow C-reactive protein
NegativeOcclusionsSegments stented � 10 cm� 30% residual stenosisPoor tibial runoffSerum creatinine � 1.3 mg/dL
NoncontributoryAgeRaceExperience of operator
ABI � 0.15) after PTA is directly related to tibial run- o
ff.188 Most studies have shown an appropriate increasen ABI after PTA. The duration of the increase is un-nown and may or may not correlate with symptommprovement. When operation is compared with PTAor lesions appropriate for PTA, there are no notableifferences between bypass operations and PTA.182,189
tudies of patients after operation (ie, iliofemoral oremoropopliteal bypass) have shown that at 6 weeks,here is an improvement in resting ABI and improvedreadmill testing.37 Optimal results appear to be re-tricted to patients younger than 70 years, who are notiabetic, and in whom a normal ankle pressure is antic-
pated based on the lesion corrected and the anatomicistribution of PAD. But up to 20% of patients will beissatisfied with their surgical outcomes, even though0% of this dissatisfied subgroup will have a normalostoperative ABI.190 Similar data are not yet availableor PTA of the SFA.
Although anatomic patency and hemodynamic suc-ess are important, the primary reasons to perform anntervention are symptom relief and longterm clinicaluccess. Karch and colleagues191 demonstrated that 40%f patients remain symptom free 4 years after SFA an-ioplasty. Clinical failures are only partially related tonatomic patency of the treated area, and other factors,uch as progression of disease in the inflow vessels in thereated vessel and in the outflow tract, are also impli-ated. Half of these lesions are amenable to additionalercutaneous intervention. These findings that clinicaluccess appears to be higher than anatomic success haseen reported by others.192,193 Predictors of clinical fail-re in the immediate period were age, SFA occlusion,nd angioplasty rating (ie, residual stenosis, presence ofissection, occlusion); predictors in the early period (�2 months) were age, SFA occlusion, degree of arterioscle-osis, and angioplasty rating; in the late period (�2 months), only angioplasty rating was important.194
harmacotherapy after PTAhe role of pharmacotherapy after PTA in the SFA haseen driven by data derived from the coronary arterynterventional literature. Heiss and associates,195 showedmajor benefit of aspirin compared with placebo afterTA, but antiplatelet drugs have not shown a consistentenefit in preventing restenosis.196,197 Low dose aspirinppears as effective as high dose aspirin in the preventionf restenosis.198 The coronary literature supports the use
f the combination of aspirin and clopidogrel after en-
dpdtWpfcl
AFPdpdsTiast�olaspap
atowrn1wbd
sitdt4
bpal
DAtSfsivss
ADtbttaattdetgpdd
uSetdiogahsisc
287Vol. 201, No. 2, August 2005 Davies et al Femoropopliteal Atherosclerotic Disease
oluminal intervention. No data are readily available foreriphery interventions, but most centers add clopi-ogrel before and after intervention. The required dura-ion of this additional therapy has not been tested.
hether statins are beneficial after peripheral angio-lasty is unanswered by level 1 evidence, but given theact that patients with SFA disease should have theirardiovascular risk factors managed aggressively, it isikely to be a moot point.
djuvant stentingour randomized studies comparing PTA alone versusTA plus stent placement in the SFA all failed toemonstrate a benefit to stenting in terms of longtermatency and symptom relief.199-202 There is little evi-ence to support the superiority of endovasculartents over PTA alone in the femoropopliteal arteries.heir use should be confined at present to flow lim-
ting dissections or inadequate results from balloonngioplasty alone.200,203,204 Cheng and coauthors205
uggested that major factors that impede stent pa-ency were occlusions, stented segment length
10 cm, procedure in claudicants, and the usef Memotherm (Bard) stents. Liermann and col-eagues206 reported a primary patency rate of 82%fter 18 months and noted a lower patency rate fortents placed in the distal portion of the SFA com-ared with the proximal portion. Strecker and associ-tes170 reported a 2-year patency rate of 73% for stentlacement for stenosis and 32% in occlusions.Use of wall stents for short lesions and stenoses reveals
1- to 2-year primary patency of 67%; for occlusionshis dropped to 49%.171 One report suggested a high ratef early thrombosis and restenosis rate of 77% whenall stents are placed in the SFA.207 There are no peer
eviewed data in press on the longterm performance ofitinol stents in the SFA. One report noted that the2-month restenosis of nitinol stents was 46%, whichas not influenced by the cumulative length or the num-er of stents placed, but was worsened in the presence ofiabetes.208
In a bid to counteract in-stent restenosis, coveredtents have been proposed.209 There appears to be annitial gain in patency over the first 6 months.210 Al-hough this strategy did prevent in-stent restenosis, itid not prevent development of intimal hyperplasia athe ends of the device.211 Reocclusion rates of 32% to
3% in the first 12 to 18 months after implantation have (een reported.211-214 Reconstructive operations in patientsresenting with infrainguinal stent occlusion or restenosisppear to be associated with higher morbidity and majorimb amputation rates.215
rug eluting stentslthough several drug eluting stents have been used in
he coronary circulation, only one, the sirolimus elutingMART stent (Cordis Endovascular), has data availableor the periphery. The results of the SIROCCO studieshowed that despite excellent 6-month patency observedn the bare nitinol stent group, comparative analysis re-ealed a reduction in neointimal hyperplasia in theirolimus eluting stents.216,217 It did not appear that thesetents had a major clinical effect.
therectomyebulking of lesions may enhance patency. Atherec-
omy devices and endovascular endarterectomy haveeen used to achieve these aims. Directional atherec-omy appears to have a 75% patency at 24 months, buthere is a high restenosis rate.218 Endovascular SFA end-rterectomy appears to have a 65% technical success ratend a cumulative patency of 59% in patients in whomechnical success can be achieved.219 Directional atherec-omy has a patency of 57% at 2 years in patients withiabetes, complete luminal occlusion, or critical isch-mia having lower patencies.220 Studies have suggestedhat debulking segments before adjunctive balloon an-ioplasty may offer advantages in reducing acute com-lications and improving longterm patency.221,222 In ad-ition, treatment of in-stent restenosis may be helped byebulking before dilation.223
Several mechanical atherectomy devices have beensed in the treatment of peripheral vascular disease. Theimpson Atherocath is commonly used to treat focalccentric lesions in larger vessels and bypass graft anas-omoses. It is limited by its high profile and side-cuttingesign. The Silverhawk catheter (Foxhollow Inc), which
s derived from the Simpson catheter, has reduced thesebstacles to catheter placement and use. Case series sug-est that it has short-term benefits.224-226 Rotationaltherectomy (Rotablator, Boston Scientific) uses a veryigh speed rotating diamond coated burr to abrade le-ions into microparticles that are dispersed down stream;t is very useful for heavily calcified lesions, but the con-equences of distal embolization remain a considerableoncern. The transluminal endarterectomy catheter
TEC) uses aspiration to collect debris shaved by a ro-
tirlwpMwtlnSlt
LLsswTllgba
BDhpfiigtsmce
CCtaenlp
aaTadopLg1
EVPPsmdttsaewilnctgs
OWcfdbsawwmwcssc
288 Davies et al Femoropopliteal Atherosclerotic Disease J Am Coll Surg
ating cutting head and appears more effective in treat-ng soft or thrombus-containing obstructions. In aetrospective analysis of 35 SFAs treated with the trans-uminal endarterectomy catheter, the initial success rateas 100%, but the 5-year patency was 0%.227 Both theullback atherectomy catheter and Redha-Cut (Sherineed AG) catheter rely on first passing the obstructionith the entire device and then removing the material as
he catheter’s cutting blades are pulled back across theesion. In three prospective randomized trials, there waso difference between angioplasty and atherectomy forFA disease.228-230 Initial ABI, but not tibial runoff orong occlusions, appeared to be most predictive of pa-ency after atherectomy.
aser-assisted angioplastyaser-assisted angioplasty increases luminal cross-ectional area by both athero-ablation and vessel expan-ion without calcium ablation.231,232 Technical successith laser-assisted angioplasty is as high as 91%.233-235
here appears to be better initial recanalization withaser-assisted angioplasty compared with PTA, but noongterm differences between PTA and laser-assisted an-ioplasty have been appreciated.236,237 Enclosed throm-olysis associated with PTA has no advantage over PTAlone.238
rachytherapyelivery of radiation to the injured field in a vessel has
ad beneficial effects. Endovascular radiotherapy canrevent intimal hyperplasia after stent implantation inemoropopliteal arteries,239 but it partially prevents heal-ng of disrupted vessel surfaces.240 Gamma radiationnduces positive vascular remodeling after balloon an-ioplasty.241 When doses of 12 to 14 Gy (gamma radia-ion) are applied endoluminally to the femoropoplitealegment after PTA, there is a twofold increase in 12-onth patency compared with that in untreated
ontrols.242-244 Similar results were noted in the Periph-ral Artery Radiation Investigational Study trial.245
ryotherapyryoplasty is a novel therapy that combines conven-
ional balloon angioplasty with application of cryother-py. Experimental data suggest that cryotherapy inducesarly arterial wall cell loss through apoptosis, but doesot alter intimal hyperplasia development or eventual
umen area compared with conventional balloon angio-
lasty.246 The single system on the market at present uses cdouble balloon system that exerts 8 atm on the lesionnd is accompanied by cold induced injury to the wall.he hope is that cyrotherapy will allow more accurate
ngioplasty and induce apoptosis in the wall, reducingissections and vessel response to injury. The final resultsf the cryovascular safety registry have shown, in 102atients, a primary patency of 82% at 10 months.247
onger-term data are required, although case series sug-est that improved patency can be achieved up to8 months.248
xercise versus angioplastyarious trials have compared superficial femoral arteryTA to exercise therapy. They suggest that althoughTA may give a short 3- to 6-month improvement inymptoms, exercise therapy has better results at 12onths. But at 5-year followup, there appears to be no
ifference between the groups.249-252 The loss of the ini-ial advantage of PTA was attributable to restenosis ofhe dilated segment; those treated conservatively had ateadily increased benefit of exercise. The later loss of thedvantage of exercise was probably from a lack of adher-nce to the exercise program. The best effect of exerciseas found in patients with disease confined to the SFA
n contrast to PTA, which had the best effect in iliacesions.253 One study compared PTA with exercise witho treatment and suggested that PTA moderately butonsiderably improves quality of life at 1 year.254 All ofhese studies lacked sufficient power and the seminalroup of PTA with supervised exercise is missing in alltudies.
peration versus angioplastyhen examining the benefits of exercise in the claudi-
ant population, another question arises: “Is there aunctional benefit of operation in the intermittent clau-ication population?” One study compared peripheralypass operation, operation followed by 6 months ofupervised exercise training with dynamic leg exercises,nd 6 months of supervised training alone in 75 patientsith claudication. At 13 months of randomization,alking ability was improved in all three groups. Theost effective treatment for improving functional statusas exercise training plus operation. The median
hanges in maximal walking distance were 173% for theurgical group, 263% for the group that received bothupervised exercise and bypass, and 151% for the exer-ise group alone. The surgically treated patients in-
reased their walking distance more than patients who
rg
EIpaadsnqbgffs1tyc
il
ttdtshrtshpEmiat
R
Fimn
289Vol. 201, No. 2, August 2005 Davies et al Femoropopliteal Atherosclerotic Disease
eceived only exercise training did; they also had areater rate of complications than the exercise groups.255
conomicsn Sweden, the cost-effectiveness ratios (cost per month ofatency) for PTA and local open thromboendarterectomyppear equivalent.256 For a decision and cost-effectivenessnalysis of revascularization procedures for femoropoplitealisease (4,800 PTAs and 4,511 bypasses),257 six treatmenttrategies were analyzed: no treatment, initial PTA witho additional revascularization, initial PTA with subse-uent PTA, initial PTA with subsequent bypass surgery,ypass surgery followed by no therapy, and bypass sur-ery followed by graft revision. The results showed thator a 65-year-old man with disabling claudication and aemoropopliteal stenosis or occlusion, an initial PTAtrategy increased quality adjusted life years by 2 to3 months and resulted in decreased lifetime expendi-ures as compared with bypass surgery. Sensitivity anal-sis showed that when the 5-year patency of PTA ex-
igure 5. A suggested therapeutic guideline for the patient present-ng with claudication. Principal therapy must remain risk factorodification and exercise and in the recalcitrant patient, endolumi-al therapy should be considered.
eeds 30%, PTA is the preferred initial invasive strategy
n patients with disabling claudication and femoropop-iteal stenosis or occlusion.
In conclusion, aggressive proactive medical therapy inhe claudicating patient remains the most importantherapeutic step that should be initiated as soon as clau-ication is identified (Fig. 5). Exercise is important inhis initial strategy, but will also contribute to improvedymptom relief in many patients. In patients who stillave severe lifestyle-limiting claudication that does notespond to the initial medical regimen, angioplasty ofhe SFA appears to be an appropriate intervention withuccess more likely in low-grade lesions compared withigh-grade lesions. Adjuvants to a percutaneous ap-roach have not proved consistently beneficial to date.ndoluminal intervention without aggressive lifestyleodifications is not recommended because the durabil-
ty of the intervention is approximately 50% at 5 yearsnd secondary interventions are often required to main-ain patency.
EFERENCES
1. Jeremy M, Perkins T, Collin J. Do exercise programmes im-prove claudication? In: Greenhalgh RM, ed. Trials and tribu-lations of vascular surgery. London: WB Saunders; 1996:259–267.
2. Pell JP. Impact of intermittent claudication on quality of life.Eur J Vasc Endovasc 1995;9:469–472.
3. Breek JC, Hamming JF, DeVries J, et al. The impact of walkingimpairment, cardiovascular risk factors, and co-morbidity onquality of life in patients with intermittent claudication. J VascSurg 2002;36:94–99.
4. Criqui MH, Fronek A, Barrett-Conner E, et al. The prevalenceof peripheral arterial disease in a defined population. Circula-tion 1985;71:510–515.
5. Hiatt WR, Hoag S, Hamman RF. Effect of diagnostic criteriaon the prevalence of peripheral arterial disease, The San LuisValley Diabetes Study. Circulation 1995;91:1472–1479.
6. Hiatt AT, Criqui MH, Treat-Johnson D, et al. Peripheral arte-rial disease detection, awareness and the treatment in primarycare. JAMA 2001;286:1317–1324.
7. Kannel WB, McGee DL. Update on some epidemiologicalfeature of intermittent claudication: the Framingham Study.J Am Ger Soc 1995;33:13–18.
8. Kannel WB. The demographics of claudication and the agingof the American population. Vasc Med 1996;1:60–64.
9. Smith GD, Shipley MJ, Rose G. Intermittent claudication,heart disease risk factors and mortality: The Whitehall Study.Circulation 1990;82:1925–1931.
10. Leng GC, Fowkes FGR. The epidemiology of peripheral vas-cular disease. Vasc Med Rev 1993;4:5–18.
11. Imparato AM, Kim GE, Davidson T, et al. Intermittent clau-dication: its natural course. Surgery 1975;78:795–799.
12. Cronenwett JL, Warner KG, Davidson T, et al. Intermittent
290 Davies et al Femoropopliteal Atherosclerotic Disease J Am Coll Surg
claudication - current results of non-operative management.Arch Surg 1984;119:430–435.
13. Walsh DB, Gilbertson JJ, Zwolak RM, et al. The natural his-tory of superficial femoral artery stenoses. J Vasc Surg 1991;14:299–304.
14. McAllister FF. The fate of patients with intermittent claudica-tion managed non-operatively. Am J Surg 1976;132:593–595.
15. Fowkes FG, Allen PL, Tsampoulas C, et al. Validity of duplexscanning in the detection of peripheral arterial disease in thegeneral population. Eur J Vasc Surg 1992;6:31–35.
16. Criqui MH, Langer RD, Fronek A, et al. Mortality over aperiod of 10 years in patients with peripheral arterial disease.N Engl J Med 1992;325:381–386.
17. Criqui MH, Fronek A, Klauber MR, et al. The sensitivity,specificity and predictive value of traditional clinical evaluationof peripheral arterial disease: results from noninvasive testingin a defined population. Circulation 1985;71:516–522.
18. Vogt MT, McKenna M, Anderson SJ, et al. Prevalence andcorrelates of lower extremity arterial disease in elderly women.Am J Epidemiol 1993;137:559–568.
19. Newman AB, Sutton-Tyrrrell K, Vogt MT, Kuller LH. Mor-bidity and mortality in hypertensive adults with a low ankle/arm blood pressure index. JAMA 1993;270:487–489.
20. Newman AB, Siscovick DS, ManolioTA, et al. Ankle arm index asa marker of atherosclerosis in Cardiovascular Health Study(CHS) Collaborative Research Group. Circulation 1993;88:837–845.
21. Applegate WB. Ankle/arm pressure index: a useful test forclinical practice. JAMA 1993;270:497–498.
22. Wensing PJ. Arterial tortuosity in the femoropopliteal regionduring knee flexion. J Anat 1995;186:133–139.
23. Jaffe MR. The nature of SFA disease. Endovascular Today2004;3:3–5.
24. Drisko K. Characterizing the unique dynamics of the SFA.Endovascular Today 2004;7(Supplement):6–8.
25. Nesbitt E, Schmidt-Trucksass A, Il’yasov KA, et al. Assessmentof arterial blood flow characteristics in normal and atheroscle-rotic vessels with the fast Fourier flow method. MAGMA2000;10:27–34.
26. Crawford DW, Barndt RJ, Back LH. Surface characteristics ofnormal and atherosclerotic human arteries including observa-tions suggesting interaction between flow and intimal mor-phology. Lab Invest 1976;34:463–470.
27. Strandness DE. Duplex scanning in vascular disorders. 2nd ed.New York: Raven Press; 1993.
28. Nerem RM. Vascular fluid mechanics, the arterial wall, andatherosclerosis. J Biomech Eng 1992;114:274–282.
29. Davies PF, Polacek DC, Shi C, Helmke BP. The convergence ofhaemodynamics, genomics, and endothelial structure in stud-ies of the focal origin of atherosclerosis. Biorheology 2002;39:299–306.
30. Stary HC, Bleakley-Chandler A, Dinsmore RE, et al. A definitionof advanced types of atherosclerotic lesions and a histological clas-sification of atherosclerosis: A report from the Committee on Vas-cular Lesions of the Council on Arteriosclerosis, American HeartAssociation. Circulation 1995;92:1355–1374.
31. Stary HC, Chandler AB, Glagov S, et al. A definition of initialfatty streak and intermediate lesions of atherosclerosis: a reportfrom the Committeee on Vascular Lesons of the Council onAtheroslerosis, American Heart Association. Arterioscler Thromb1994;14:840–856.
32. Ross R. Rous-Whipple Award lecture: Atherosclerosis: a de-
fense mechanism gone awry. Am J Pathol1994;143:987–1002.
33. Schenk EA. Pathology of occlusive disease of the lower extrem-ities. Cardiovasc Clin 1973;5:287–310.
34. Lee RT, Libby P. The unstable atheroma. Arterioscler ThrombVasc Biol 1997;17:1859–1867.
35. Libby P. Current concepts of the pathogenesis of the acutecoronary syndromes. Circulation 2001;104:365–372.
36. Aikawa M, Libby P. The vulnerable atherosclerotic plaque:pathogenesis and therapeutic approach. Cardiovasc Pathol2004;13:125–138.
37. TASC Working Group. Management of peripheral arterial dis-ease (PAD): Transatlantic Inter-Society Consensus (TASC).Eur J Vasc Endovasc Surg 2000;19:S1–S244.
38. Graham IM, Daly LE, Refsum HM, et al. Plasma homocys-teine as a risk factor for vascular disease: The European Con-certed Action Project. JAMA 1997;277:1775–1881.
39. Kannel WB, McGee DL, Castelli WP. Latest perspectives oncigarette smoking and cardiovascular disease: the FraminghamStudy. J Cardiac Rehabil 1984;4:267–277.
40. Jonason T, Bergastrom R. Cessation of smoking in patientswith intermittent claudication. Acta Med Scand 1987;221:253–260.
41. Belch J. Medical management of intermittent claudication. In:Greenhalgh RM, ed. Vascular and endovascular opportunities.London: WB Saunders; 2000:361–388.
42. Fowkes FG, Housley E, Riemersama RA, et al. Smoking, lip-ids, glucose intolerance and blood pressure as risk factors forperipheral atherosclerosis compared with ischemic heart dis-ease in the Edinburgh Arterial Study. Am J Epidemiol 1992;135:331–340.
43. Cheng SWK, Ting ACW, Wong J. Lipoprotein(a) and its rela-tionship to risk factors and severity of atherosclerotic periph-eral vascular disease. Eur J Vasc Endovasc Surg 1997;14:17–23.
44. Brandman O, Redisch W. Incidence of peripheral vascularchanges in diabetes mellitus. Diabetes 1953;2:194–198.
45. Adler AI, Stevens RJ, Neil A, et al. UKPDS 59: hyperglycemiaand other potentially modifiable risk factors for peripheral vas-cular disease in type 2 diabetes. Diabetes Care 2002;25:894–899.
46. Ramsey L, Williams B, Johnston G, et al. Guidelines for man-agement of the British Hypertension Society: report of theworking party of the British Hypertension Society. J HumHypertens 1999;13:569–592.
47. Pearson TA, Mensah GA, Alexander RW, et al. Markers ofinflammation and cardiovascular disease: application to clini-cal and public health practice: a statement for healthcare pro-fessionals from the Centers for Disease Control and Preventionand the American Heart Association. Circulation 2003;107:499–511.
48. Wang TJ, Nam BH, Wilson PW, et al. Association ofC-reactive protein with carotid atherosclerosis in men andwomen: the Framingham Heart Study. Arterioscler ThrombVasc Biol 2002;22:1662–1667.
49. Ridker PM, Hennekens CH, Buring JE, et al. C-reactive pro-tein and other markers of inflammation in the prediction ofcardiovascular disease in women. N Engl J Med 2000;342:836–843.
50. Ridker PM, Stampfer MJ, Rifai N. Novel risk factors for sys-temic atherosclerosis: a comparison of C-reactive protein fi-
brinogen homocysteine lipoprotein(a) and standard choles-
291Vol. 201, No. 2, August 2005 Davies et al Femoropopliteal Atherosclerotic Disease
terol screening as predictors of peripheral arterial disease.JAMA 2001;285:2481–2485.
51. Ridker PM, Cushman M, Stampfer MJ, et al. Plasma concen-tration of C-reactive protein and risk of developing peripheralvascular disease. Circulation 1998;97:425–428.
52. Schillinger M, Exner M, Mlekusch W, et al. Vascular inflam-mation and PTA of the femoropopliteal artery: associationwith restenosis. Radiology 2003;225:21–26.
53. Valentine R, Kaplan HS, Green R, et al. Lipoprotein(a), ho-mocysteine and hypercoaguable states in young men with pre-mature peripheral atherosclerosis: a prospective controlledanalysis. J Vasc Surg 1996;23:53–63.
54. Hoogeveen FK, Kostense PJ, Beks PJ, et al. Hyperhomocys-teinemia is associated with an increased risk of cardiovasculardisease, especially in non-insulin dependent diabetes mellitus:a population-based study. ArteriosclerThromb Vasc Biol 1988;18:133–138.
55. Selhub J, Jacques PF, Bostom AG, et al. Association betweenplasma homocysteine concentrations and extracranial carotidartery stenosis. N Engl J Med 1995;332:286–291.
56. Jacques PF, Selhub J, Bostom AG, et al. The effect of folic acidfortification on plasma folate and total homocysteine concen-trations. N Engl J Med 1999;340:1449–1454.
57. Selhub J, Jacques PF, Bostom AG, et al. Relationship betweenplasma homocysteine and vitamin status in the Framinghamstudy population: impact of folic acid fortification. PublicHealth Rev 2000;28:117–145.
58. Mortia H, Kurihara H, Kuwaki H, et al. Homocysteine as arisk factor for restenosis after coronary angioplasty. ThrombHaemost 2000;84:7–31.
59. Hodish I, Mateetzky S, Selah BA, et al. Effect of elevated ho-mocysteine levels on clinical restenosis following coronary re-stenosis. Cardiology 2002;97:214–217.
60. Schnyder G, Roffi M, Pin R, et al. Decreased rate of coronaryrestenosis after lowering of plasma homocysteine levels. N EnglJ Med 2001;345:1593–1600.
61. Smith SB, Lowe GDO, Fowkes FGR, et al. Smoking, hemo-static facotrs and lipid peroxides in a population case con-trolled study of peripheral arterial disease. Atherosclerosis1993;102:155–162.
62. Komarov A, Panchenko E, Dobrovolsky A, et al. D-dimer andplatelet aggregability are related to thrombotic events in pa-tients with peripheral arterial occlusive disease. Eur Heart J2002;23:1309.
63. Antiplatelet Trialists’ Collaboration. Collaborative overview ofrandomized trials of antiplatelet therapy - I: Prevention ofdeath, myocardial infarction, and stroke by prolonged anti-platelet therapy in various categories of patients. BMJ 1994;308:81–106.
64. Antiplatelet Trialists’ Collaboration. Collaborative overview ofrandomized trials of antiplatelet therapy II: Maintenance ofvascular graft or arterial patency by antiplatelet therapy. BMJ1994;308:159–168.
65. Antiplatelet Trialists’ Collaboration. Collaborative meta-analysisof randomized trials of antiplatelet therapy for prevention of deathmyocardial infarction and stroke in high risk patients 1. BMJ2002;324:71–86.
66. Hess H, Mietaschk A, Deichel G. Drug-induced inhibition ofplatelet function delays progression of peripheral occlusive ar-terial disease: a prospective double blind arteriographicallycontrolled trial. Lancet 1985;I:415–419.
67. CAPRIE Steering Committee. A randomized blinded trial of
clopidogrel versus aspirin in patients at risk of ischemic events(CAPRIE). Lancet 1996;348:1329–1339.
68. Ray SA, Rowley MR, Loh A. Hypercoagulable states in pa-tients with leg ischemia. Br J Surg 1994;81:811–814.
69. Donaldson MC, Weinberg DS, Belkin M, et al. Screening forhypercoagulable states in vascular surgical practice: a pre-liminary study. J Vasc Surg 1990;11:825–831.
70. Strano A, Hoppensteadt D, Walenga J, et al. Plasma levels ofthe molecular markers of coagulation and fibrinolysis in pa-tients with peripheral arterial disease. Semin Thromb Hemost1996;22(Suppl 1):35–40.
71. Donaldson MC, Weinberg DS, Belkin M, et al. Screening forhypercoaguable states in vascular surgical practice: a prelimi-nary study. J Vasc Surg 1990;11:825–831.
72. Catalano M, Russo U, Linretti A. Plasma beta thromboglobu-lin levels and claudication states in vascular surgical practice: apreliminary study. Angiology 1986;37:339–342.
73. Gosk-Bierska I, Adamiec R, Alexewicz P, Wyokinski WE. Co-agulation in diabetic and non diabetic claudicants. Int Angiol2002;21:128–133.
74. Ray SA, Rowley MR, Bevan DH, et al. Hypercoagulable ab-normalities and postoperative failure of arterial reconstruction.Eur J Vasc Endovasc Surg 1997;13:363–370.
75. Lee AJ, Fowkes FG, Rattray A, et al. Hemostatic and rheologi-cal factors in intermittent claudication: the influence of smok-ing and extent of arterial disease. Br J Haematol 1996;92:226–230.
76. Johansson J, Egberg N, Johnsson H, Carlson LA. Serum li-poproteins and hemostatic function in intermittent claudica-tion. Arterioscler Thrombo 1993;13:1441–1448.
77. Handa K, Takao M, Nomoto J, et al. Evaluation of the coagu-lation and fibrinolytic systems in men with intermittent clau-dication. Angiology 1996;47:543–548.
78. Mustonen P, Lepantalo M, Lassila R. Physical exertion inducesthrombin formation and fibrin degradation in patients with pe-ripheral atherosclerosis. Arterioscler Thromb Vasc Biol 1998;18:244–249.
79. Price JE, Mamode N, Smith FB, et al. Haemostatic and rheo-logical factors as predictors of restenosis following PTA. Eur JVasc Endovasc 1997;14:392–398.
80. Davies AH. The practical management of claudication. BMJ2000;321:911–912.
81. Murabito JM, Evans JC, Nieto K, et al. Prevalence and clinicalcorrelates of peripheral arterial disease in the Framingham Off-spring Study. Am Heart J 2002;143:961–965.
82. Benowitz NL. Pharmacologic aspects of cigarette smoking andnicotine addiction. New Engl J Med 1988;319:1318–1330.
83. Fiore MC. Methods used to quit smoking in the United States.JAMA 1990;263:2760–2765.
84. Silagy C, Mant D, Foeler G, Lancaster T. Nicotine replacementtherapy for smoking cessation. Cochrane Databse Syst Rev2000;3:CD000146.
85. Bohadana A, Nilsson F, Rasmussen T, Martiner Y. Nicotineinhaler and nicotine patch as a combination therapy for smok-ing cessation: a randomized double-blind placebo-controlledtrial. Arch Intern Med 2000;160:3128–3134.
86. Jorenby DE, Leiscow SJ, Nides MA, et al. A controlled trial ofsustained-release bupropion, a nicotine patch or both forsmoking cessation. N Engl J Med 1999;340:685–691.
87. West R, McNeill A, Raw M. Smoking cessation guidelines for
health professionals: an update. Thorax 2000;12:987–999.
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
292 Davies et al Femoropopliteal Atherosclerotic Disease J Am Coll Surg
88. Foley WT. Treatment of gangrene of the feet and legs by walk-ing. Circulation 1957;15:689–700.
89. Larsen OA, Lassen NA. Effect of daily exercise in patients withintermittent claudication. Lancet 1966;2:1093–1096.
90. Stewart KJ, Hiatt WR, Regensteiner JG, Hirsch AT. Exercisetraining for claudication. N Engl J Med 2002;347:1941–1951.
91. Remijnse-Tamerius HC, Duprez D, deBuyzere M, et al. Whyis training effective in the treatment of patients with intermit-tent claudication. Int Angiol 1999;18:103–112.
92. Gardner AW, Katzel LI, Sorkin JD, et al. Improved functionaloutcomes following exercise rehabilitation in patients with in-termittent claudication. J Gerontol A Biol Sci Med Sci 2000;55:570–577.
93. Tisi PV, Hulse M, Chulakadabba A, et al. Exercise training forintermittent claudication: does it adversely affect biochemicalmarkers of the exercised induced inflammatory response. Eur JVasc Endovasc 1997;14:344–350.
94. Price JF, Leng GC, Fowkes FGR. Should claudicants receiveangioplasty or exercise training. Cardiovasc Surg 1997;5:463–469.
95. Gardner AW, Poehlman ET. Exercise rehabilitation programsfor the treatment of claudication pain: A meta-analysis. JAMA1995;274:975–980.
96. Cachovan M. Methods and results of controlled walking train-ing in patients with peripheral arterial occlusive disease. Z ArztlFortbild Qualitat Ssich 1999;93:626–632.
97. Walker RD, Nawaz S, Wilkinson CH, et al. Influence of upperand lower limb exercise training on cardiovascular functionand walking distances in patients with intermittent claudica-tion. J Vasc Surg 2000;31:662–669.
98. Dawson DL, Cutler BS, Meissner MH, Strandness DE Jr.Cilostazol has beneficial effects in treatment of intermittentclaudication: results from a multicenter randomized prospec-tive double blind trial. Circulation 1998;98:678–686.
99. Executive summary of the Third Report of The National Cho-lesterol Education Program (NCEP) Expert Panel on Detec-tion, Evaluation and Treatment of High Blood Cholesterol inAdults (Adult Treatment panel III). JAMA 2001;285:2486–2497.
00. Grundy SM, Cleeman JI, Merz NB, et al. Implications ofrecent clinical trials for National Cholesterol Education Pro-gram Adult Treatment Panel III Guidelines. Circulation 2004;110:227–239.
01. Selvin E, Erlinger TP. Prevalence of and risk factors for periph-eral arterial disease in the United States. Circulation 2004;110:738–743.
02. Pasternak RC, Smith SC, Bairey-Merz CN, et al. ACC/AHA/NHLBI clinical advisory on the use and safety of statins. Cir-culation 2002;106:1024–1028.
03. Leng GC, Price JF, Jepson RG. Lipid lowering therapy in thetreatment of lower limb atherosclerosis. Eur J Vasc Endovasc1998;16:5–6.
04. Laws PE, Spark JI, Cowled PA, Fitridge RA. The role of statinsin vascular disease. Eur J Vasc Endovasc 2004;27:6–16.
05. Leng GC, Price JF, Jepson RG. Lipid-lowering for lower limbatherosclerosis. Cochrane Database Syst Rev 2000;3:CD000123.
06. Pederson TR, Kjekshus J, Pyorala K, et al. Effect of simvastatinon ischemic signs and symptoms in the Scandinavian Simva-statin Survival Study (4S). Am J Cardiol 1998;81:333–335.
07. Aronow WS, Nayak D, Woodworth S, Ahn C. Effect of Sim-
vastatin versus placebo on threadmill exercise time until theonset of intermittent claudication in older patients withperipheral arterial disease at six months and at one year aftertreatment. Am J Cardiol 2003;92:711–712.
08. McDermott MM, Guralnik JM, Greenland P, et al. Statin useand leg functioning in patients with and without lower extrem-ity peripheral arterial disease. Circulation 2003;107:757–761.
09. Mohler ER, Hiatt WR, Creager MA, Study Investigators. Cho-lesterol reduction with atorvastatin improves walking distancein patients with peripheral arterial disease. Circulation 2003;108:1481–1486.
10. Money SR, Herd JA, Isaacsohn JL, et al. Effect of cilostazol onwalking distance in patients with intermittent claudicationcaused by peripheral vascular disease. J Vasc Surg 1998;27:267–274.
11. Thompson PD, Zimat R, Forbes WP, Zhang P. Meta-analysisof results from eight randomized placebo-controlled trials onthe effect of cilostazol on patients with intermittent claudica-tion. Am J Cardiol 2002;90:1314–1319.
12. Rajagopalan S, Trachtenberg J, Mohler E, et al. Phase I study ofdirect administration of a replication deficient adenovirus vec-tor containing the vascular endothelial growth factor cDNA(CI-1023) to patients with claudication. Am J Cardiol 2002;90:512–516.
13. Rajagopalan S, Mohler E, Lederman RJ, et al. Regional angio-genesis with vascular endothelial growth factor in peripheralarterial disease. Circulation 2003;108:1933–1938.
14. Lederman RJ, Mendelsohn FO, Anderson RD, et al. Ther-apeutic angiogenesis with recombinant fibroblast growthfactor-2 for intermittent claudication (the TRAFFIC study): arandomised trial. Lancet 2002;259:2053–2058.
15. Dotter CT, Judkins MP. Transluminal treatment of arterioscle-rotic obstruction. Circulation 1964;30:654–670.
16. Gruntzig AR. Percutane Rekanalization chronischer ArteriellerVerschlusse mit einem neuen Dilatationskatheter. DuetscheMedizinische Wochenschrift 1974;99:2502–2510.
17. Matsi PJ, Manninen HI, Soder HK, et al. PTA in femoralartery occlusions: primary and longterm results in 107 claudi-cant patients using femoral and popliteal catheterization tech-niques. Clin Radiol 1995;50:237–244.
18. Reekers JA, Kromhout JG, Jacobs MJ. Percutaneous inten-tional extraluminal recanalization of the femoropopliteal ar-tery. Eur J Vasc Surg 1994;8:723–728.
19. Bolia A, Miles KA, Brennan J, Bell PR. Percutaneous translu-minal angioplasty of occlusions of the femoral and poplitealarteries by subintimal dissection. Cardiovasc Intervent Radiol1990;13:357–363.
20. Yilmaz S, Sindel T, Ceken K, et al. Subintimal recanalization oflong superficial femoral artery occlusions through the retro-grade popliteal approach. Cardiovasc Intervent Radiol 2001;24:154–160.
21. Clowes AW, Reidy MA, Clowes MM. Kinetics of cellular pro-liferation after arterial injury. I: Smooth muscle cell growth inthe absence of endothelium. Lab Invest 1983;49:327–333.
22. Perlman H, Maillard L, Krasinski K, Walsh K. Evidence for therapid onset of apoptosis in medial smooth muscle cells afterballoon injury. Circulation 1997;95:981–987.
23. Clowes AW, Schwartz SM. Significance of quiescent smoothmuscle cell migration in the injured rat carotid artery. Circ Res1985;56:139–145.
24. Hanke H, Strohschneider T, Oberhoff M, et al. Time course of
smooth muscle cell proliferation in the intima and media of
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
293Vol. 201, No. 2, August 2005 Davies et al Femoropopliteal Atherosclerotic Disease
arteries following experimental angioplasty. Circ Res1990;67:651–659.
25. Majesky MW, Schwartz SM, Clowes MM, Clowes AW. Hep-arin regulates smooth muscle S phase entry in the injured ratcarotid artery. Circ Res 1987;61:296–300.
26. More RS, Rutty G, Underwood MJ, et al. Assessment of my-ointimal cellular kinetics in a model of angioplasty by means ofproliferating cell nuclear antigen expression. Am Heart J 1994;128:681–686.
27. Waksman R, Rodriquez JC, Robinson KA, et al. Effect ofintravascular irradiation on cell proliferation, apoptosis andvascular remodelling after balloon overstretch injury of porcinecoronary arteries. Circulation 1997;96:1944–1952.
28. Ferns GA, Raines EW, Sprugel KH, et al. Inhibition of neoin-timal smooth muscle accumulation after angioplasty by an an-tibody to PDGF. Science 1991;253:1129–1132.
29. Hehrlein C, Gollan C, Donges K, et al. Low-dose radioactiveendovascular stents prevent smooth muscle cell proliferationand neointimal hyperplasia in rabbits. Circulation 1995;92:1570–1575.
30. Bauriedel G, Skowasch D, Jabs A, et al. Insights into vascularpathology after intracoronary brachytherapy. Z Kardiol 2002;91(Suppl 3):1–9.
31. Schwartz SM. Smooth muscle migration in atherosclerosis andrestenosis. J Clin Invest 1997;100(11 Suppl):S87–S89.
32. Davies MG, Hagen P-O. Pathobiology of intimal hyperplasia.Br J Surg 1994;81:1254–1269.
33. Scott NA, Martin F, Simonet L, et al. Contribution of adven-titial myofibroblasts to vascular remodelling and lesion forma-tion after experimental angioplasty in pig coronaries. FASEB J1995;9:A845 (abstract).
34. Ferrer P, Valentine M, Jenkins-West T, et al. Periadventitialchanges in the balloon injured rat carotid artery. FASEB J1996;10:A618 (abstract).
35. O’Brien ER, Alpers CE, Stewart DK, et al. Proliferation inprimary and restenotic coronary atherectomy tissue: implica-tions for antiproliferative therapy. Circ Res 1993;73:223–231.
36. Bauriedel G, Windstetter U, DeMaio SJJ, et al. Migratoryactivity of human smooth muscle cells cultivated from coro-nary and peripheral primary and restenotic lesions removed bypercutaneous atherectomy. Circulation 1992;85:554–564.
37. Rekhter MD, Schwartz SM, O’Brien E, et al. Collagen I geneexpression in human coronary lesions, primary atheroscleroticversus restenosis (abstract). Circulation 1993;88(Part 2):I–228.
38. Sarembock IJ, LaVeau PJ, Sigal SL, et al. Influence of inflationpressure and balloon size on the development of intimal hyper-plasia after balloon angioplasty. A study in the atheroscleroticrabbit. Circulation 1989;80:1029–1040.
39. VanErven L, Post MJ, Velema E, Borst C. In the normal rabbitfemoral artery increasing arterial wall injury does not lead toincreased intimal hyperplasia. J Vasc Res 1994;31:153–162.
40. Sakamoto H, Nozaki S, Misumi K, et al. Smooth muscle cellproliferation in the arterial intima after stretch injury - rela-tionship between and severity of stretching and intimal hyper-plasia in the New Zealand White rabbits. Jikken Dobutsu Ex-perimental Animals 1996;45:89–93.
41. Andersen HR, Maeng M, Thorwest M, Falk E. Remodelingrather than neointimal formation explains luminal narrowingafter deep vessel wall injury - insights from a porcine coronary(re)stenosis model. Circulation 1996;93:1716–1724.
42. Moornekamp FN, Borst C, Post MJ. Endothelial cell recover- 1
age and intimal hyperplasia after endothelium removal with orwithout smooth muscle cell necrosis in the rabbit carotidartery. J Vasc Res 1996;33:146–155.
43. Cwikiel W. Restenosis after balloon angioplasty and/or stentinsertion - origin and prevention. Acta Radiologica 2002;43:442–454.
44. Lowe HC, Oesterle SN, Khachigan LM. Coronary in stentrestenosis: Current status and future strategies. J Am Coll Car-diol 2002;39:183–193.
45. Mehran R, Dangas G, Abizaid A, et al. Angiographic patternsof in stent restenosis: classification and implications for long-term outcome. Circulation 1999;100:1872–1878.
46. Hoffman R, Mintz GS, Dussaillant RG, et al. Patterns andmechanisms of in stent restenosis: a serial intravascular ultra-sound study. Circulation 1996;94:1247–1254.
47. Virmani R, Farb A. Pathology of instent restenosis. Curr OpinLipidol 1999;10:499–506.
48. Abizaid A, Kornowski R, Mintz GS, et al. The influence ofdiabetes mellitus on acute and late outcomes following coro-nary stent implantation. J Am Coll Cardiol 1998;32:584–589.
49. Carter AJ, Bailey L, Devries J, Hubbard B. The effects of un-controlled hyperglycemia on thrombosis and formation ofneoinitma after coronary stent placement in a novel diabeticporcine model of restenosis. Coron Artery Dis 2000;11:473–479.
50. Baier RE, Dutton RC. Initial events in interaction of bloodwith a foreign surface. J Biomed Mater Res 1969;3:191.
51. Emneus H, Stenram U. Metal implants in the human body.Acta Orthop Scand 1965;36:116.
52. Parsson H, Cwikiel W, Johansson K, Swartbol P, Norgren L.Deposition of platelets and neitrophils on porcine iliac arteriesand angioplasty and Wallstent placement compared with an-gioplasty alone. Cardiovasc Intervent Radiol 1994;17:190–196.
53. Bai H, Masuda J, Sawa Y, et al. Neointima formation aftervascular stent implantation: spatial and chronological distribu-tion of smooth muscle cell proliferation and phenotypic mod-ulation. Arterioscler Thromb 1994;14:1846–1853.
54. Schwartz RS, Huber KC, Murphy JG, et al. Restenosis and theporportional neointimal response to coronary artery injury:results in a porcine model. J Am Coll Cardiol 1992;19:267–274.
55. Kornowski R, Hong MK, Fermin OT, et al. In-stent restenosis:contributions of inflammatory responses and arterial injury toneointima hyperplasia. J Am Coll Cardiol 1998;31:224–230.
56. Sanada JL, Matsui O, Yoshikawa J, Matsuoka T. An experi-mental study of endovascular stenting with special reference tothe effects on the aortic vasa vasorum. Cardiovasc InterventRadiol 1998;21:45–49.
57. Becquemin J-P, Cavillon A, Haiduc F. Surgical transluminalfemoropopliteal angioplasty: multivariate analysis outcome. JVasc Surg 1994;19:495–502.
58. Capek P, McLean GK, Berkowitz HD. Femoropopliteal angio-plasty. Factors influencing long-term success. Circulation1991;83(2 suppl):170–180.
59. Hunink MG, Donaldson MC, Meyerovitz MF, et al. Risks andbenefits of femoropopliteal percutaneous balloon angioplasty.J Vasc Surg 1993;17:183–192.
60. Johnston KW. Femoral and popliteal arteries: re-analysis ofresults of balloon angioplasty. Radiology 1992;183:767–771.
61. Clark TWI, Groffsky JL, Soulen MC. Predictors of longterm
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
294 Davies et al Femoropopliteal Atherosclerotic Disease J Am Coll Surg
patency after femoropopliteal angioplasty: results from theSTAR registry. J Vasc Intervent Radiol 2001;12:923–933.
62. Jorgensen B, Tonnesen KH, Holstein P. Late hemodynamicfailure following PTA for long and multifocal femoropoplitealstenoses. Cardiovasc Interv Radiol 1991;14:290–292.
63. Soeder HK, Manninen HI, Raesaenen HT, et al. Longtermpatency of femoropopliteal artery angioplasty: results of a pro-spective trial. J Vasc Intervent Radiol 2002;13:361–369.
64. Dalsing MC, Cockerill E, Deupreee R, et al. Outcome predic-tors in selection of balloon angioplasty or surgery for peripheralarterial occlusive disease. Veterans Administration CooperativeStudy No. 199. Surgery 1991;110:636–643.
65. Bucek RA, Hudak P, Schnurer G, et al. Clinical long-termresults of PTA in patients with peripheral arterial occlusivedisease. Vasa 2002;31:36–42.
66. Hewes R, White RJ, Murray R, et al. Longterm results ofsuperficial femoral artery angioplasty. Am J Roentgenol 1986;146:1025–1029.
67. Cambria R, Faust G, Gusberg R, et al. Percutaneous angio-plasty for peripheral arterial occlusive disease: correlates of clin-ical success. Arch Surg 1987;122:283–287.
68. Parsons RE, Suggs WD, Lee JJ, et al. Percutaneous translumi-nal angioplasty for the treatment of limb threatening ischemia:do the results justify an attempt before bypass grafting. J VascSurg 1998;28:1066–1071.
69. Martin DR, Katz SG, Kohl RD, Qian D. Percutaneous trans-luminal angioplasty of infrainguinal vessels. Ann Vasc Surg1999;13:184–187.
70. Strecker EP, Boos IB, Goettmann D. Femoropoplitreal arterystent placement: evaluation of longterm success. Radiology1997;205:375–383.
71. Rousseau H, Raillat C, Joffre F, et al. Treatment of femoropop-liteal stenoses by means of self-expandable endoprosthesis: midterm results. Radiology 1989;172:961–964.
72. Matsi PJ, Manninen HI, Vanninen RL, et al. Femoropoplitealangioplasty in patients with claudication: primary and second-ary patency in 140 limbs with 1–3 year follow up. Radiology1994;191:727–733.
73. Hunink MGM, Wong JB, Donaldson MC, et al. Revascular-ization for femoropopliteal disease. JAMA 1995;274:165–171.
74. Jorgensen B, Meisner S, Holstein P, Tonnesen KH. Early re-thrombosis in femoropopliteal occlusions treated with PTA.Eur J Vasc Surg 1990;4:149–152.
75. London NJ, Srinivasan R, Naylor AR, et al. Subintimal angio-plasty of femoropopliteal artery occlusions: the long term re-sults. Eur J Vasc Surg 1994;8:148–155.
76. Laxdal E, Jenssen GL, Pedersen G, Aune S. Subintimal angio-plasty as a treatment of femoropopliteal artery occlusions. EurJ Vasc Endovasc Surg 2003;25:578–582.
77. Gussenhoven EJ, vanderLugt A, Pasterkamp G, et al. Intravas-cular ultrasound predictors of outcome after peripheral balloonangioplasty. Eur J Vasc Endovasc Surg 1995;10:279–288.
78. Vogt KC, Just S, Rasmussen JG, Schroeder TV. Prediction ofoutcome after femoropopliteal balloon angioplasty by IVUS.Eur J Vasc Endovasc Surg 1997;13:563–568.
79. vanderLugt A, Gussenhoven EJ, Pasterkamp G, et al. Intravas-cular ultrasound predictor of restenosis after balloon angio-plasty of the femoropopliteal artery. Eur J Vasc Endovasc Surg1998;16:110–119.
80. Spijkerboer AM, Nass PC, deValois JC, et al. Evaluation of
femoropopliteal arteries with duplex ultrasound after angio-plasty. Can we predict results at one year? Eur J Vasc EndovascSurg 1996;12:418–423.
81. vanLankeren W, Gussenhoven EJ, Honkoop J, et al. Plaquearea increase and vascular remodeling contribute to lumen areachange after PTA of the femoropopliteal artery: an intravascu-lar ultrasound study. J Vasc Surg 1999;29:430–431.
82. Wilson SE, Wold GL, Cross AP. Percutaneous transluminalangioplasty versus operation for peripheral atherosclerosis: re-port of a prospective randomized trial in a selected group ofpatients. J Vasc Surg 1989;9:1–9.
83. Treiman GS, Ichikawa L, Treiman RL, et al. Treatment of re-current femoral or popliteal artery stenosis after percutaneoustransluminal angioplasty. J Vasc Surg 1994;20:577–587.
84. Milford MA, Weaver FA, Lundell CJ, et al. FemoropoplitealPTA for limb salvage. J Vasc Surg 1988;8:292–299.
85. Blair JM, Gewertz BL, Moosa H, et al. PTA versus surgery forlimb threatening ischemia. J Vasc Surg 1989;9:698–703.
86. Armstrong MW, Torrie EP, Galland RB. Consequences of im-mediate failure of percutaneous transluminal angioplasty. AnnR Coll Surg Engl 1992;74:265–268.
87. Galaria II, Surowiec SM, Rhodes JM, et al. Implications ofearly failure of superficial femoral artery endoluminal interven-tions. Ann Vasc Surg 2005;41:in press.
88. Alback A, Biancari F, Schmidt S, et al. Haemodynamic resultsof femoropopliteal PTA. Eur J Vasc Endovasc Surg 1998;16:7–12.
89. Holm J, Arfvidsson B, Jivegard L, et al. Chronic limb ischemia:a prospective randomized controlled study comparing the 1year results of vascular surgery and PTA. Eur J Vasc Surg 1991;6:517–522.
90. Zannetti S, L’Italien GJ, Cambria RP. Functional outcomeafter surgical treatment for intermittent claudication. J VascSurg 1996;24:65–73.
91. Karch LA, Mattos MA, Henretta JP, McLafferty RB, et al.Clinical failure after percutaneous transluminal angioplasty ofthe SFA and popliteal arteries. J Vasc Surg 2000;31:880–887.
92. Vroegindewij D, Tielbeck AV, Buth J, et al. Recanalization offemoropopliteal occlusive lesions: a comparison of longtermclinicalcolor duplexultrasound and arteriographic follow-up.J Vasc Interv Radiol 1995;6:331–337.
93. Surowiec SM, Davies MG, Lee D, et al. Percutaneous angio-plasty and stenting of the superficial femoral artery. J Vasc Surg2005;41:269–278.
94. El-Bayar H, Roberts A, Hye R, et al. Determinants of failurein superficial femoral artery angioplasty. Angiology 1992;43:877–885.
95. Heiss HW, Just J, Middleton D, Deichsel G. Reocclusion pro-phylaxis with dipyridamole combined with acetylsalicylic acidfollowing PTA. Angiology 1990;41:263–269.
96. Heiss HW, Mathias K, Beck AH, et al. Efficacy of acetylsali-cylic acid and dipyridamole for prevention of recurrence offemoral and popliteal arterial lesions following PTA. Cor Vasa1987;1:25–34.
97. Minar E, Ehringer H, Ahmadi R, et al. Platelet deposition atangioplasty sites and its relation to restenoses in human iliacand femoropopliteal arteries. Radiology 1989;170:767–772.
98. Minar E, Ahmadi A, Koppensteiner R, et al. Comparison ofeffects of high dose and low dose aspirin on restenosis afterfemoropopliteal PTA. Circulation 1995;91:2167–2173.
99. Zdanowski Z, Albrechtsson U, Lundin A, et al. Percutaneous
transluminal angioplasty with or without stenting for femoro-
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
295Vol. 201, No. 2, August 2005 Davies et al Femoropopliteal Atherosclerotic Disease
popliteal occlusions? A randomized controlled study. IntAngiol 1999;18:251–255.
00. Vroegindeweij D, Vos LD, Buth J, Bosch HC. Balloon angio-plasty combined with primary stenting versus balloon angio-plasty alone in femoropopliteal obstructions: a comparativerandomized study. Cardiovasc Intervent Radiol 1997;20:420–425.
01. Cejna M, Schoder M, Lammer J. PTA versus stent in femoro-popliteal obstruction. Radiologie 1999;39:144–150.
02. Becquemin J-P, Favre J-P, Marzelle J, et al. Systematic versusselective stent placement after SFA balloon angioplasty: A mul-ticenter prospective randomized study. J Vasc Surg 2003;37:487–494.
03. Chatelard P, Guibort C. Longterm results with a palmez stentin the femoropopliteal arteries. J Cardiovasc Surg 1996;37(suppl 1):67–72.
04. Sapoval M, Long AL, Raynaud AC, et al. Femoropoplitealstent placement: longterm results. Radiology 1992;184:833–839.
05. Cheng SWK, Ting ACW, Wong J. Endovascular stenting ofSFA stenosis and occlusions: results and risk factor analysis.Cardiovasc Surg 2001;9:133–140.
06. Liermann D, Strecker EP, Peters J. The Strecker Stent: indica-tions and results in iliac and femoropopliteal arteries. Cardio-vasc Intervent Radiol 1992;15:298–305.
07. Zollikofer CL, Antonucci F, Pfyffer M, et al. Arterial stentplacement with use of the Wall Stent: midterm results of clin-ical experience. Radiology 1991;179:449–456.
08. Sabeti S, Mlekusch W, Amighi J, et al. Primary patency oflong-segment self-expanding nitinol stents in the femoropop-liteal arteries. J Endovasc Ther 2005;12:6–12.
09. Cragg AH, Dake MD. Percutaneous femoropopliteal graftplacement. Radiology 1993;187:643–648.
10. Saxon RR, Coffman JM, Gooding JM, et al. Longterm resultsof ePTFE stent-graft versus angioplasty in the femoropoplitealartery: single center experience from a prospective randomizedtrial. J Vasc Interv Radiol 2003;14:303–311.
11. Deutschmann HA, Schedibauer P, Berczi V, et al. Placement ofhemobahn stent-grafts in femoropopliteal arteries: early expe-rience and midterm results in 18 patients. J Vasc Interv Radiol2001;12:943–949.
12. Blum U, Fugel P, Ebert S, et al. Stent grafting for stenotic/occlusive lesions of femoropopliteal arteries. In: 38th AnnualWorld Congress of the International College of Angiology;1996; Cologne, Germany.
13. Link J, Muller-Hulsbeck S, Brossmann J, et al. Unimanteltestents bei oberschenkelarterienverschlussen: ein erfahrungs-bericht nach 2 jahrigeranwendung. ROFO 1996;164:107(ab-stract).
14. Henry M, Amor M, Cragg M, et al. Occlusive and aneurysmperipheral arterial disease: assessment of a stent graft system.Radiology 1996;201:717–724.
15. Boeckler D, Blaurock P, Mannsman U, et al. Early surgicaloutcomes after failed primary stenting for lower limb occlusivedisease. J Endovasc Ther 2005;12:13–21.
16. Duda SH, Pusich B, Richter G, et al. Sirolimus-eluting stentsfor the treatment of obstructive superficial femoral artery dis-ease, six month results. Circulation 2002;106:1505–1509.
17. Duda SH, Poerner TC, Wiesinger B, et al. Drug eluting stents:potential applications for peripheral arterial occlusive disease.J Vasc Interv Radiol 2003;14:291–301.
18. Savader SJ, Venbrux AC, Mitchell SE, et al. Percutaneous
transluminal atherectomy of the superficial and femoral andpopliteal arteries: long-term results in 48 patients. CardiovascIntervent Radiol 1994;17:312–318.
19. Nelson PR, Powell RJ, Proia RR, et al. Results of endovascularsuperficial femoral endarterectomy. J Vasc Surg 2001;34:526–531.
20. Wildenhain PM, Wholey MH, Jarmolowski CR, Hill KL. In-frainguinal directional atherectomy: long term followup andcomparison with percutaneous transluminal angioplasty. Car-diovasc Intervent Radiol 1994;17:305–311.
21. Moussa I, Moses J, DiMario C, et al. Stenting after optimallesion debulking (SOLD) registry. Angiographic and clinicaloutcome. Circulation 1998;98:1604–1609.
22. Bramucci E, Angoli L, Merlini PA, et al. Adjunctive stent im-plantation following directional coronary atherectomy in pa-tients with coronary artery disease. J Am Coll Cardiol 1998;32:1855–1860.
23. Dauerman H, Balm D, Cutlip D, et al. Mechanical debulkingversus balloon angioplasty for the treatment of diffuse in-stentrestenosis. Am J Cardiol 1998;82:277–284.
24. Dorros G, Iyer S, Lewin R, et al. Angiographic follow up andclinical outcome of 126 patients after percutaneous directionalatherectomy (Simpson Atherocath) for occlusive peripheralvascular disease. Catheter Cardiovasc Diagn 1991;22:79–84.
25. vonPolnitz A, Nerlich A, Berger H, Hofling B. Percutaneousperipheral atherectomy: angiographic and clinical follow up of60 patients. J Am Coll Cardiol 1990;15:682–688.
26. Kuffer G, Spengel FA, Hansen R, et al. Simpson’s atherectomyof the peripheral arteries: early results and follow up. Rofo1990;153:61–67.
27. Kolvenbach R, Strosche H. Longterm results after rotationangioplasty and catheter atherectomy. A retrospective analysis.J Cardiovasc Surg 1998;39:15–18.
28. Tielbeek AV, Vroegindeweij D, Buth J, Ladman GH. Compar-ison of balloon angioplasty and Simpson atherectomy for le-sions in the femoropopliteal artery: angiographic and clinicalresults of a prospective randomized trial. J Vasc Interv Radiol1996;7:837–844.
29. Nakamura S, Conroy RM, Gordon IL, et al. A randomizedtrial of transcutaneus extraction atherectomy in femoral arter-ies: intravascular ultrasound observations. J Clin Ultrasound1995;23:461–471.
30. Gordon IL, Conroy RM, Tobis JM, et al. Determinants ofpatency after percutaneous angioplasty and atherectomy of oc-cluded SFA. Am J Surg 1994;168:115–119.
31. Mintz GS, Kovach JA, Javier SP, et al. Mechanisms of lumenenlargement after excimer laser coronary angioplasty: an intra-vascular ultrasound study. Circulation 1995;92:3408–3414.
32. Topaz O, Das T, Dahm J, et al. Excimer laser revascularization:current indications, applications and techniques. Lasers MedSci 2001;16:72–77.
33. Lammer J, Pilger E, Decrinis M, et al. Pulsed excimer laserversus continuous wave Nd:YAG laser versus conventional an-gioplasty of peripheral arterial occlusions: prospective con-trolled randomized trial. Lancet 1992;340:1183–1188.
34. Belli AM, Cumberland DC, Procter AE, et al. Total peripheralartery occlusions: conventional versus laser thermal recanaliza-tion with a hybrid probe in percutaneous angioplasty - resultsof a randomized trial. Radiology 1991;181:57–60.
35. Scheinert D, Laird JR, Schroeder M, et al. Excimer laser-assisted recanalization of long chronic superficial femoral ar-
tery occlusion. J Endovasc Ther 2001;8:156–166.
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
296 Davies et al Femoropopliteal Atherosclerotic Disease J Am Coll Surg
36. Odink HF, deValois HC, Eikelboom BC. Femoropopliteal ar-tery recanalization: factors affecting clinical outcome of con-ventional and laser assisted balloon angioplasty. Cardiovasc In-tervent Radiol 1995;18:162–167.
37. Steinkamp HJ, Rademaker J, Wissgott C, et al. Percutaneoustransluminal laser angioplasty versus balloon dilation for treat-ment of popliteal artery occlusions. J Endovasc Ther 2002;9:882–888.
38. Nicholson T. Percutaneous transluminal angioplasty and en-closed thrombolysis versus PTA in the treatment of femoro-popliteal occlusion: results of a prospective randomized trial.Cardiovasc Intervent Radiol 1998;21:470–474.
39. Liermann D, Bottcher HD, Kollath J, et al. Prophylactic en-dovascular radiotherapy to prevent intimal hyperplasia afterstent implantation in femoropopliteal arteries. Cardiovasc In-tervent Radiol 1994;17:12–16.
40. Wyttenbach R, Gallino A, Alerci M, et al. Effects of percutaneoustransluminal angioplasty and endovascular brachytherapy on vas-cular remodeling of human femoropopliteal artery by noninva-sive magnetic resonance imaging. Circulation 2004;110:1156–1161.
41. Hagenaars T, Po IFLA, vanSambeek RHM, et al. Gamma ra-diation induces positive vascular remodeling after balloon an-gioplasty: a prospective randomized IVUS scan study. J VascSurg 2002;36:31–324.
42. Minar E, Pokrajac B, Maca T, et al. Endovascular brachyther-apy for prophylaxis of restenosis after femoropopliteal angio-plasty. Circulation 2000;102:2694–2699.
43. Krueger K, Landwehr P, Bendel M, et al. Endovascular gammairradiation of femoropopliteal de novo stenoses immediatelyafter PTA: interim results of prospective randomized con-trolled trial. Radiology 2002;224:519–528.
44. Wolfram RM, Pokrajac B, Ahmadi R, et al. Endovascularbrachytherapy for prophylaxis against restenosis after long seg-ment femoropopliteal placement of stents: initial results. Ra-diology 2001;220:724–729.
45. Waksman R, Laird JR, Jurkovitz CT, et al. Intravascular radiationtherapy after balloon angioplasty of narrowed femoropopliteal ar-teries to prevent restenosis: results of the PARIS feasibility clinicaltrial. J Vasc Intervent Radiol 2001;12:915–921.
46. Cheema AN, Nili N, Li CW, et al. Effects of intravascularcryotherapy on vessel wall repair in a balloon injured rabbit
iliac artery model. Cardiovasc Res 2003;59:222–233.47. Laird JR, Biamino G, Jaff MR. Femoropopliteal outcomeswith cryoplasty: final results of the cryovascular safety registry.J Vasc Interv Radiol 2004;15:S218 (abstract).
48. Fava M, Loyola S, Polydorou A, et al. Cryoplasty for femoro-popliteal arterial disease: late angiographic results of initial hu-man experience. J Vasc Interv Radiol 2004;15:1239–1243.
49. Whyman MR, Fowkes FG, Kerracher EM, et al. Is intermit-tent claudication improved by percutaneous transluminal an-gioplasty? A randomized control trial. J Vasc Surg 1997;26:551–557.
50. Whyman MR, Fowkes FGR, Kerracher EMG, et al. Random-ized controlled trial of percutaneous transluminal angioplastyfor intermmittent claudication. Eur J Vasc Endovasc Surg1996;12:167–172.
51. Perkins JM, Collin J, Creasy TS, et al. Exercise training versusangioplasty for stable claudication. Long and medium termresults of a prospective randomized study. Eur J Vasc Surg1996;11:409–413.
52. Creasy TS, McMillan PJ, Fletcher EW, et al. Is percutaneoustransluminal angioplasty better than exercise for claudication?Preliminary results from a prospective randomized study. Eur JVasc Surg 1990;4:135–140.
53. Chetter IC, Spark JI, Kent PJ, et al. Percutaneous transluminalangioplasty for intermittent claudication: Evidence on whichto base the medicine. Eur J Vasc Endovasc Surg 1998;16:477–484.
54. Taft C, Karlsson J, Gelin J, et al. Treatment of intermittentclaudication by invasive therapy, supervised physical exercisetraining compared to no treatment in unselected randomizedpatients II: one year results of health related quality of life. EurJ Vasc Endovasc Surg 2001;22:114–223.
55. Lundgren E, Dahllof A, Lundholm K, et al. Intermittent clau-dication: surgical reconstruction or physical training? A pro-spective randomized trial of treatment efficiency. Ann Surg1989;209:346–355.
56. Vroegindewij D, Idu M, Buth J, et al. The cost effectiveness oftreatment of short occlusive lesions in the femoropopliteal ar-tery: balloon angioplasty versus endarterectomy. Eur J VascEndovasc Surg 1995;10:40–50.
57. Hunink MGM, Wong JB, Donaldson MC, et al. Revascular-ization for femoropopliteal disease: a decision and cost effec-
tiveness analysis. JAMA 1995;274:165–171.