Embed Size (px)
Citation preview
This article was downloaded by: [Portland State University]On: 21 November 2014, At: 12:57Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Journal of Personality AssessmentPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/hjpa20
Associations Between Symptom Validity Test Failureand Scores on the MMPI–2–RF Validity and SubstantiveScalesRoger O. Gervais a b , Dustin B. Wygant c , Martin Sellbom d & Yossef S. Ben-Porath ea Neurobehavioural Associates , Edmonton, Alberta, Canadab Department of Educational Psychology , University of Alberta , Canadac Department of Psychology , Eastern Kentucky Universityd Department of Psychology , University of Alabamae Department of Psychology , Kent State UniversityPublished online: 22 Aug 2011.
To cite this article: Roger O. Gervais , Dustin B. Wygant , Martin Sellbom & Yossef S. Ben-Porath (2011) Associations BetweenSymptom Validity Test Failure and Scores on the MMPI–2–RF Validity and Substantive Scales, Journal of Personality Assessment,93:5, 508-517, DOI: 10.1080/00223891.2011.594132
To link to this article: http://dx.doi.org/10.1080/00223891.2011.594132
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information. Taylor and Francis shall not be liable forany losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Journal of Personality Assessment, 93(5), 508–517, 2011Copyright C© Taylor & Francis Group, LLCISSN: 0022-3891 print / 1532-7752 onlineDOI: 10.1080/00223891.2011.594132
Associations Between Symptom Validity Test Failure and Scoreson the MMPI–2–RF Validity and Substantive Scales
ROGER O. GERVAIS,1,2 DUSTIN B. WYGANT,3 MARTIN SELLBOM,4 AND YOSSEF S. BEN-PORATH5
1Neurobehavioural Associates, Edmonton, Alberta, Canada2Department of Educational Psychology, University of Alberta, Canada
3Department of Psychology, Eastern Kentucky University4Department of Psychology, University of Alabama5Department of Psychology, Kent State University
This study examined the association between Symptom Validity Test (SVT) failure and the Minnesota Multiphasic Personality Inventory–2Restructured Form (MMPI–2–RF; Ben-Porath & Tellegen, 2008), in the Forensic Disability Claimant samples described in the MMPI–2–RFTechnical Manual (Tellegen & Ben-Porath, 2008a, 2008b). SVTs used included the Word Memory Test (Green, 2003), the Computerized Assessmentof Response Bias (Allen, Conder, Green, & Cox, 1997), the Medical Symptom Validity Test (Green, 2004), and the Test of Memory Malingering(Tombaugh, 1996). SVT failure was associated with significant elevations throughout the MMPI–2–RF overreporting validity scales and substantivescales. Pairwise contrasts between groups failing 0 and 3 SVTs revealed predominantly large effect sizes for the overreporting validity scales (d =0.78–1.11), and many of the substantive scales, including the Cognitive Complaints (COG) scale. Results of this study demonstrate an associationbetween SVT performance and elevated scores on the MMPI–2–RF. These results suggest that exaggeration of cognitive symptoms as demonstratedby SVT failure is also associated with overreported emotional, somatic, and neurocognitive complaints on the MMPI–2–RF.
It is well established in the neuropsychological literature thatpoor performance on cognitive symptom validity tests (SVTs) isassociated with overreporting of cognitive, emotional, and phys-ical symptoms, as well as unreliable cognitive test scores thatunderestimate actual cognitive functioning (Bianchini, Greve,& Glynn, 2005; Gervais, Rohling, Green, & Ford, 2004; Green,2007). Consequently, position statements by both the NationalAcademy of Neuropsychology (NAN; Bush et al., 2005) andthe American Academy of Clinical Neuropsychology (AACN;Heilbronner et al., 2009), as well as proposed diagnostic stan-dards for assessing malingered cognitive dysfunction (Slick,Sherman, & Iverson, 1999) and malingered pain-related disabil-ity (Bianchini et al., 2005) indicate the value of incorporatingevidence from self-report measures along with performance-based SVTs when assessing response bias.
The association between failure on SVTs and overreportingof emotional and physical symptoms suggests that responses onmultiscale self-report inventories such as the Minnesota Multi-phasic Personality Inventory–2 (MMPI–2; Butcher et al., 2001)could also share some variance with SVT performance. Indeed,some studies have demonstrated an association between cog-nitive SVT failure and elevated MMPI–2 validity and clinicalscales profiles (e.g., Boone & Lu, 1999; Larrabee, 1998, 2003;Youngjohn, Burrows, & Erdal, 1995).
Studies examining SVT failure in the context of the MMPI–2Restructured Clinical (RC) scales (Tellegen et al., 2003)have started to appear in the literature. Wygant, Gervais, andBen-Porath (2005) explored the correlation between the WordMemory Test (WMT; Green, 2003) and the MMPI–2 RC scales
Received June 25, 2010; Revised January 3, 2011.Address correspondence to Roger O. Gervais, Suite 210, 17010–103 Avenue,
Edmonton, Alberta, T5S 1K7, Canada; Email: [email protected]
in a sample of 775 disability claimants and found that WMTperformance was most strongly associated with RC1 (SomaticComplaints), RC2 (Low Positive Emotions), and RCd (Demor-alization). Examination of the RC scales across three levelsof decreasing mean WMT performance revealed significantincreases in all RC scales except RC6 (Ideas of Persecution) andRC9 (Hypomanic Activation). In a subsequent study, Wygantet al. (2007) examined the association between SVT failure andthe MMPI–2 clinical and RC scales in two samples: criminaldefendants (n = 127) and civil personal injury and disabilityclaimants (n = 141). Results of the study showed that whereasSVT failure was associated with noncredible somatic symptomreporting in both forensic samples, noncredible reporting ofpsychotic symptoms was only associated with SVT failure inthe criminal defendant sample. The authors discussed how thiswas likely due to different demand characteristics that inviteparticular types of symptom exaggeration depending on legalcontext (e.g., psychosis in an insanity defense).
Thomas and Youngjohn (2009) examined the MMPI–2 va-lidity, clinical, and RC scales in a sample of 83 traumatic braininjury (TBI) litigants and also found a significant correlationbetween SVT failure and elevations on the MMPI–2 scales, par-ticularly RC1. Estimated effect sizes (Cohen’s d) for the meandifferences between the pass and fail SVT groups revealed alarge effect size for RC1 (d = 1.10), followed by moderate ef-fect sizes for RC2 and RC8 (Aberrant Experiences; d = .67and .66, respectively). The authors noted that their study waslimited by a relatively small sample size and missing SVT data,which might have led to false negatives in the pass SVT groupand attenuated the correlations between the SVT status and theMMPI–2 scales.
The MMPI–2–Restructured Form (MMPI–2–RF; Ben-Porath& Tellegen, 2008a, 2008b) is a 338-item self-report measurelinked conceptually and empirically to contemporary theories
508
Dow
nloa
ded
by [
Port
land
Sta
te U
nive
rsity
] at
12:
57 2
1 N
ovem
ber
2014

SVT FAILURE AND MMPI–2–RF 509
and models of psychopathology and personality. The items arederived from the MMPI–2 item pool and are used to score fivesets of substantive scales, including Higher-Order (H-O), Re-structured Clinical (RC), Specific Problem (SP), Interest, andPersonality Psychopathology Five–Revised (PSY–5) scales, aswell as revised and new validity scales. The H-O, RC, SP, In-terest, and PSY–5 scales are designed to assess various aspectsand levels of psychopathology, general types of interests, andpersonality, whereas the validity scales are designed to assesstest protocol validity. A detailed description of these scales andthe rationale for the development of them is provided in theMMPI–2–RF test manuals (Ben-Porath & Tellegen, 2008a; Tel-legen & Ben-Porath, 2008).
Wygant et al. (2009) examined the MMPI–2–RF over report-ing validity scales in two analogue samples, in which medi-cal patients and individuals with a documented history of headinjury simulated disability consistent with their injuries andconditions. The authors also examined a third sample, whichconsisted of personal injury and disability claimants who wereadministered the MMPI–2 and cognitive SVTs as part of theirevaluations. The authors found that scores on the MMPI–2–RFvalidity indicators increased significantly in relation to numberof SVTs failed, with effect sizes (Cohen’s d) from the pass allSVTs group to fail two or three SVTs ranging from 1.60 (F-r) to1.21 (Fp-r). Thus, the exaggeration of cognitive deficits, as indi-cated by SVT failure, was associated with overreported somatic,emotional, and neurocognitive complaints on the MMPI–2–RF.
A number of studies have examined the incremental validityof the MMPI–2–RF validity scales in predicting overreport-ing on self-report measures or cognitive SVT failure. Gervais,Ben-Porath, Wygant, and Sellbom (2010) found that disabil-ity claimants failing any SVT obtained significantly higherscores on the MMPI–2–RF overreporting validity scales thanclaimants who passed all SVTs. The MMPI–2–RF F-r, Fp-r,and FBS-r added incrementally to their MMPI–2 counterpartsin predicting subjective memory complaints. Sellbom, Toomey,Wygant, Kucharski, and Duncan (2010) examined the utilityof the MMPI–2–RF validity scales in distinguishing betweenmalingering and nonmalingering criminal forensic groups asdefined by performance on the Structured Interview for Re-ported Symptoms (SIRS; Rogers, Bagby, & Dickens, 1992).Results of the study determined that F-r and Fp-r were themost effective scales in discriminating between the two groups,followed by Fs and FBS-r. Sellbom and Bagby (2010) usedan analogue simulation design to examine the utility of theMMPI–2–RF validity scales in discriminating between indi-viduals simulating mental health problems and patients withgenuine psychopathology. The authors found that Fp-r was su-perior to the other MMPI–2–RF validity scales in differentiatingbetween the two groups. This effect occurred even when simu-lators were coached on how the validity scales operate. Wygantand colleagues (2010) examined the incremental validity of theResponse Bias Scale (RBS; Gervais, Ben-Porath, Wygant, &Green, 2007) and the MMPI–2 and MMPI–2–RF overreport-ing validity scales in predicting SVT failure in disability andcriminal forensic samples. Results of the study demonstratedthat the RBS added incrementally to the existing MMPI–2 andMMPI–2–RF validity scales in the forensic disability sample,but not in the criminal forensic sample.
With the exception of the preceding studies examining the RCscales, and Wygant and colleagues (2009), who examined the
MMPI–2–RF overreporting scales, there are no studies to datethat examine the association between SVT performance andthe full range of MMPI–2–RF validity and substantive scales.Given the relationship between SVT performance and the over-reporting validity scales and the RC scales, it is important forthe clinician to also appreciate the extent to which SVT failuremight also be associated with overreporting across the entireMMPI–2–RF, and how this might guide clinical interpretationof the protocol. This is particularly important in forensic dis-ability practice, where judgments concerning the validity of theclinical presentation and claimed disability can influence theultimate disposition of the claim.
A unique feature of the MMPI–2–RF is the incorporation ofmultiple comparison groups in the Technical Manual (Tellegen& Ben-Porath, 2008) and option to utilize these in generatingthe MMPI–2–RF Score Report and MMPI–2–RF InterpretiveReport. Use of the comparison groups allows the clinician tocontrast an individual’s scores with those of others tested insimilar settings, thereby enhancing interpretation of the proto-col. The data set from which the Forensic Disability Claimantcomparison groups were derived contain extensive SVT data,which, in light of the association between SVT performance andoverreporting discussed previously, could also contribute to theinterpretation of the protocol. However, only preliminary exam-inations of the MMPI–2–RF validity and substantive scales inlight of these data have been undertaken (Ben-Porath, 2007).
The purpose of this study is to provide a detailed examinationof the association between SVT failure and the MMPI–2–RF va-lidity and substantive scales in the Forensic Disability Claimantcomparison groups. Research to date has documented a pos-itive association between SVT failure and elevated scores onthe MMPI–2 overreporting and clinical scales. In this study, weexpect to find similar patterns of overreporting and noncredibleresponding on the MMPI–2–RF associated with SVT failure.In keeping with the clinical characteristics of the forensic dis-ability sample, the largest effect sizes are expected to be onthe overreporting validity scales and substantive scales assess-ing emotional distress, and somatic and cognitive symptoms.We anticipate that the results of this study will provide addi-tional insight and guidance to inform clinical interpretation ofMMPI–2–RF protocols in forensic disability settings.
METHOD
Participants
The Forensic Disability Claimant comparison groups consistof 523 men and 480 women who were referred to the first au-thor’s clinical practice for a comprehensive 2-day psychologicalassessment with respect to their predominantly non-head-injurydisability claims, as described in Gervais et al. (2007). The menwere 41.0 (SD = 10.7) years of age and had 11.6 (SD = 2.4)years of education. The women were 40.1 (11.0) years of ageand had 12.5 (SD = 2.4) years of education. Ethnicity or racewas not coded in the data sets. However, as noted by Gervais andcolleagues (2010), the ethnic and racial composition of a sampleof claimants seen in the first author’s clinical practice subsequentto collection of the present data set was White (83.6%), Black(4.4%), Asian (2.7%), Aboriginal (1.1%), Hispanic (0.5%), andother (4.7%). These demographic characteristics are consistentwith the population demographics in the province of Alberta and
Dow
nloa
ded
by [
Port
land
Sta
te U
nive
rsity
] at
12:
57 2
1 N
ovem
ber
2014

510 GERVAIS, WYGANT, SELLBOM, BEN-PORATH
representative of the sample from which the Forensic DisabilityClaimant comparison groups were drawn.
Workers’ compensation (men = 75.5%, women = 43.3%)and personal injury litigation (men = 18.7%, women = 39.0%)were the predominant referral sources. Primary, but nonmu-tually exclusive diagnoses for men and women, respectively,were chronic pain (34.8% and 37.5%), depression (20.3% and22.7%), and anxiety/posttraumatic stress disorder (35.8% and34.8%). Clinical diagnoses were determined according to Di-agnostic and Statistical Manual of Mental Disorders (4th ed.[DSM–IV]; American Psychiatric Association, 1994; 4th ed.,Text revision [DSM–IV–TR]; American Psychiatric Associa-tion, 2000). All claimants in the data sets completed a core testbattery including the MMPI–2 and symptom validity testing,in addition to various tests of cognitive ability and self-reportsymptom questionnaires or inventories, followed by a detailed3-hour clinical interview. Considering that the purpose of thisstudy was to examine the association between negative responsebias, as measured by cognitive SVTs and the MMPI–2–RF va-lidity and substantive scales, we only excluded protocols withCannot Say ≥ 18, or VRIN-r/TRIN-r ≥ 80T, to avoid restrictingthe range of overreporting and response bias in the MMPI–2–RFdata.
In keeping with the NAN and AACN position statementson the necessity of assessing symptom validity (Bush et al.,2005; Heilbronner et al., 2009), the claimants in this data setcompleted at least one SVT, and in some cases, up to fourSVTs. The number of SVTs administered increased as newmeasures were developed and introduced into the test battery,as described in Gervais et al. (2007). Nearly half of the sample(48%) completed three SVTs, and 25% completed four, barringnoncompliance or other factors such as limited literacy or lin-guistic barriers. To alleviate concerns that the variable numbersof SVTs administered might skew the data and outcome of thisstudy, we randomly removed one SVT from each case in thesubgroup that had been administered four SVTs. We then con-ducted the analysis using only individuals who had completedthree SVTs (men = 415, women = 332). To simplify the anal-ysis we divided the sample into four groups: (a) fail 0 SVTs,(b) fail 1 SVT, (c) fail 2 SVTs, and (d) fail 3 SVTs, rather thanexamining each SVT individually. We then used analysis of vari-ance (ANOVA) to examine the association between the numberof SVTs failed and the MMPI–2–RF validity and substantivescales. Failure on the SVTs was determined according to theirrespective manuals. Specific cut-off scores or other failure cri-teria are not presented here in the interests of maintaining testsecurity and deterring coaching (Youngjohn, 1995). The analy-ses were conducted separately for men and women to maintainconsistency with the MMPI–2–RF Technical Manual (Tellegen& Ben-Porath, 2008), which presents the psychometric prop-erties and empirical correlates of the MMPI–2–RF scales bygender.
Measures
The MMPI–2–RF (Ben-Porath & Tellegen, 2008a, 2008b)was retrospectively scored from the MMPI–2 protocols com-pleted by all individuals in the present data set. TheMMPI–2–RF includes 338 of the original 567 items of theMMPI–2. The inventory’s 50 scales include revised validityscales and the Infrequent Somatic Responses (Fs) scale, a new
validity scale designed to identify overreporting of somaticsymptoms that are rarely endorsed by medical patients. Thesubstantive scales include the Higher Order (H-O), Restruc-tured Clinical (RC), Specific Problems (SP), and Interest scales,and revised versions of the PSY–5 scales. The Technical Manual(Tellegen & Ben-Porath, 2008) documents the development ofthe MMPI–2–RF and provides extensive data describing the re-liability and validity of the inventory in various settings. Thereis a rapidly growing body of literature on the MMPI–2–RF(see Pearson Assessments, MMPI–2–RF References by TopicBibliography at http://psychcorp.pearsonassessments.com). Inaddition, Tellegen and Ben-Porath (2008) present data indicat-ing the MMPI–2–RF scale scores derived from administrationof the 567-item MMPI–2 booklet (used in this study) are in-terchangeable with results obtained from administration of the338-item MMPI–2–RF booklet.
The WMT (Green, 2003) is a computer-administered verbalmemory test that assesses various aspects of verbal memorythrough forced-choice, multiple-choice, paired associates, andfree-recall tasks. Comparisons with established criterion groupsand expected performance patterns are used to determine thevalidity of the respondent’s test scores. Simulator studies us-ing clinical patients and highly educated sophisticated simula-tors (PhD psychologists, physicians, and insurance adjusters)asked to convincingly fake cognitive impairment without beingdetected by the WMT produced sensitivity of 96% to 100%,specificity of 100%, and a hit rate of 99% (Green, Lees-Haley,& Allen, 2003; Iverson, Green, & Gervais, 1999). Tan, Slick,Strauss, and Hultsch (2002) replicated these findings using theEnglish language WMT. Other studies using the German, Turk-ish, and Russian translations have also replicated these findings(Brockhaus & Merten, 2004; Brockhaus, Peker, & Fritze, 2003;Tydecks, Merten, & Gubbay, 2006).
The Computerized Assessment of Response Bias (CARB;Allen, Conder, Green, & Cox, 1997) is an SVT based ondigit-recognition procedures designed to detect insufficienteffort associated with exaggeration of memory problems. Thetest manual describes a validation study in which the CARBdemonstrated sensitivity of 74%, specificity of 91%, and overallhit rate of 88% in predicting WMT failure in a sample of 307compensation claimants.
The Medical Symptom Validity Test (MSVT; Green, 2004)is easier and shorter than the WMT, but otherwise conceptuallysimilar in structure and interpretation. The respondent’s scoresare interpreted with reference to various clinical comparisongroups and known profile configurations to determine thevalidity of the individual’s effort. The test has been extensivelyvalidated in various clinical and nonclinical settings withpopulations ranging from normal children; to children withserious mental, cognitive, and behavioral disorders; to elderlypatients with dementia; to those with mild to severe braininjury; and to other medical disability claimants (Blaskewitz,Merten, & Kathmann, 2008; Green, Flaro, & Courtney, 2009;Howe, Anderson, Kaufman, Sachs, & Loring, 2007; Howe &Loring, 2009; Richman et al., 2006).
The Test of Memory Malingering (TOMM; Tombaugh,1996) is a two-alternative forced-choice SVT based on picturerecognition. Validation studies using simulated malingerers anda control group described in the test manual found sensitivitybetween 82% and 89%, with specificity of 100%. Numerousstudies have demonstrated good sensitivity to insufficient effort
Dow
nloa
ded
by [
Port
land
Sta
te U
nive
rsity
] at
12:
57 2
1 N
ovem
ber
2014

SVT FAILURE AND MMPI–2–RF 511
TABLE 1.—MMPI–2–RF Validity scale T scores by number of SVTs failed: Forensic disability comparison group, men.
Number of SVTs Failed
0 1 2 3
n = 264 n = 86 n = 36 n = 29 ANOVA ES
M SD M SD M SD M SD F(3, 411) p η2 d
VRIN-r 51.3a 9.3 53.6a 9.5 53.9a 8.4 55.4a 11.4 3.015 .030 .022 0.39TRIN-r 57.0a 6.3 57.5a 7.1 58.6a 6.1 57.2a 6.5 .711 .546 .005 0.03F-r 73.9a 19.5 81.6b 22.4 90.3b 22.8 95.0b 19.6 15.376 <.001 .101 1.08Fp-r 55.2a 14.1 61.6b 17.5 61.7ab 17.7 66.8b 13.5 8.468 <.001 .058 0.84Fs 66.9a 18.5 71.4ac 22.4 79.5bc 22.4 85.3b 22.2 10.561 <.001 .072 0.90FBS-r 71.9a 13.8 77.1b 13.3 83.6bc 10.8 86.3c 12.1 17.440 <.001 .113 1.11L-r 55.5a 11.3 56.4a 11.7 57.9a 11.4 58.6a 11.1 1.009 .389 .007 0.28K-r 42.7a 9.5 41.4a 10.5 42.2a 10.7 39.8a 7.6 1.006 .390 .007 –0.34
Note. Means with different subscript are significantly different (Tukey honestly significant difference). Cohen’s d calculated for effect size between Fail 0 SVT group and Fail 3 SVTsgroup. SVT = symptom validity test; ANOVA = analysis of variance; ES = effect size; VRIN-r = Variable Response Inconsistency; TRIN-r = True Response Inconsistency; F-r =Infrequent Responses; Fp-r = Infrequent Psychopathology Responses; Fs = Infrequent Somatic Responses; FBS-r = Symptom Validity; L-r = Uncommon Virtues; K-r = AdjustmentValidity.
in various forensic and medical disability settings involvingclaims of TBI, toxic exposure, chronic pain, and psychiatricdisability (Greve et al., 2006; Haber & Fichtenberg, 2006; Iver-son, Le Page, Koehler, Shojania, & Badii, 2006; Simon, 2007).
RESULTS
MMPI–2–RF Validity Scales
ANOVA results examining the mean MMPI–2–RF validityscale T scores across four levels of SVT failure (fail 0 to fail 3SVTs) revealed that SVT failure was associated with increasingamounts of random, or variable responding (Variable ResponseInconsistency; VRIN-r) in men (p = .030, η2 = .022) but notin women (p = .932, η2 = .001). There was no significantassociation between SVT failure and fixed responding as mea-sured by True Response Inconsistency (TRIN-r; p = .546, η2
= .005 [men], .769, η2 = .003 [women]). In both men andwomen, SVT failure was associated with significant increaseson the MMPI–2–RF overreporting scales: Infrequent Responses(F-r), Infrequent Psychopathology Responses (Fp-r), InfrequentSomatic Responses (Fs), and Symptom Validity (FBS-r). Exam-ination of Table 1 reveals that the largest overall effect sizes formen were observed for FBS-r (η2 = .113) and F-r (η2 = .101).F-r also had the largest overall effect size for women (η2 = .083),followed by Fs (η2 = .060) and FBS-r (η2 = .058; see Table 2).Pairwise comparisons between the fail 0 and fail 3 SVTs groupsrevealed moderate to large effect sizes for all the overreportingindicators, led by FBS-r (men/women; d = 1.11/1.04) and F-r (men/women; d = 1.08/.99).1 Review of the underreportingindicators revealed no significant association between SVT fail-
1To address concerns about potential redundancy among the overreportingpredictors we tested a Poisson regression model in which F-r, Fp-r, Fs, andFBS-r were entered into an equation predicting number of SVT tests failed. Weused backward elimination to generate an equation in which only statisticallysignificant predictors remained in the model (robust standard errors; p > .05 wasused for removal). Overall models were significant for both men, Wald χ2(2)= 100.21, p < .001; pseudo R2 = .08; and women, Wald χ2(2) = 53.75, p <
.001; pseudo R2 = .06. The same predictors emerged as statistically significantin both models—F-r (b = .038, SE = .012, z = 3.16, p = .002 [men]; b = .046,SE = .014, z = 3.24, p = .001 [women]) and FBS-r (b = .095, SE = .017, z =5.77, p = <.001 [men]; b = .078, SE = .020, z = 3.79, p < .001 [women]).
ure and Uncommon Virtues (L-r) or Adjustment Validity (K-r)scores in men or women.
MMPI–2–RF Higher Order and RC Scales
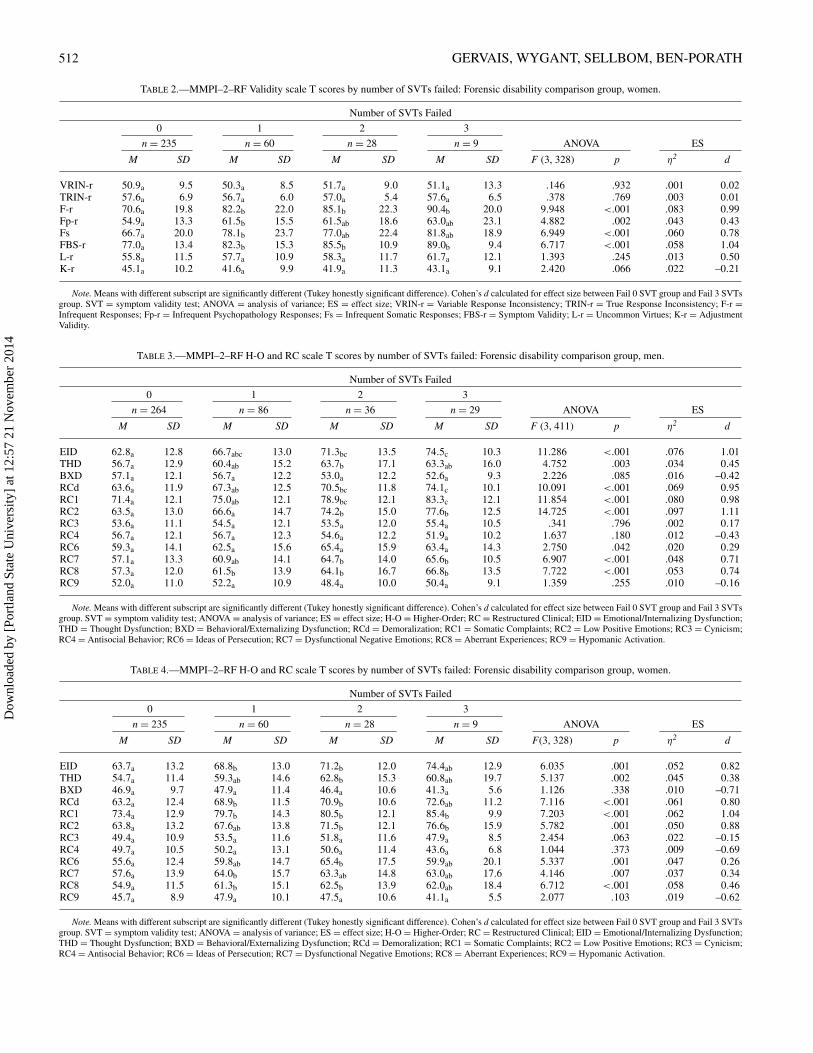
ANOVA results revealed a significant association betweenEmotional/Internalizing Dysfunction (EID) and Thought Dys-function (THD), and number of SVTs failed in both men andwomen. The largest overall effect size was observed for EID(men/women, p < .001, η2 = .076/.052) with pairwise compar-isons between the fail 0 and fail 3 SVTs groups also producinglarge effect sizes (d = 1.01/0.82). Similar results were notedfor the RC scales, with significant increases in scores across theSVT failure range on six of the nine RC scales for both men andwomen. Only RC3 (Cynicism), RC4 (Antisocial Behavior), andRC9 (Hypomanic Activation) failed to demonstrate an overallsignificant effect. Pairwise comparisons of T scores betweenthe two SVT failure ranges revealed the largest effect sizes(d; men/women) for RC2 (1.11/0.88), RC1 (0.98/1.04), andRCd (0.95/0.80). Full details of these ANOVAs are presented inTables 3 and 4.
MMPI–2–RF Somatic/Cognitive and Internalizing Scales
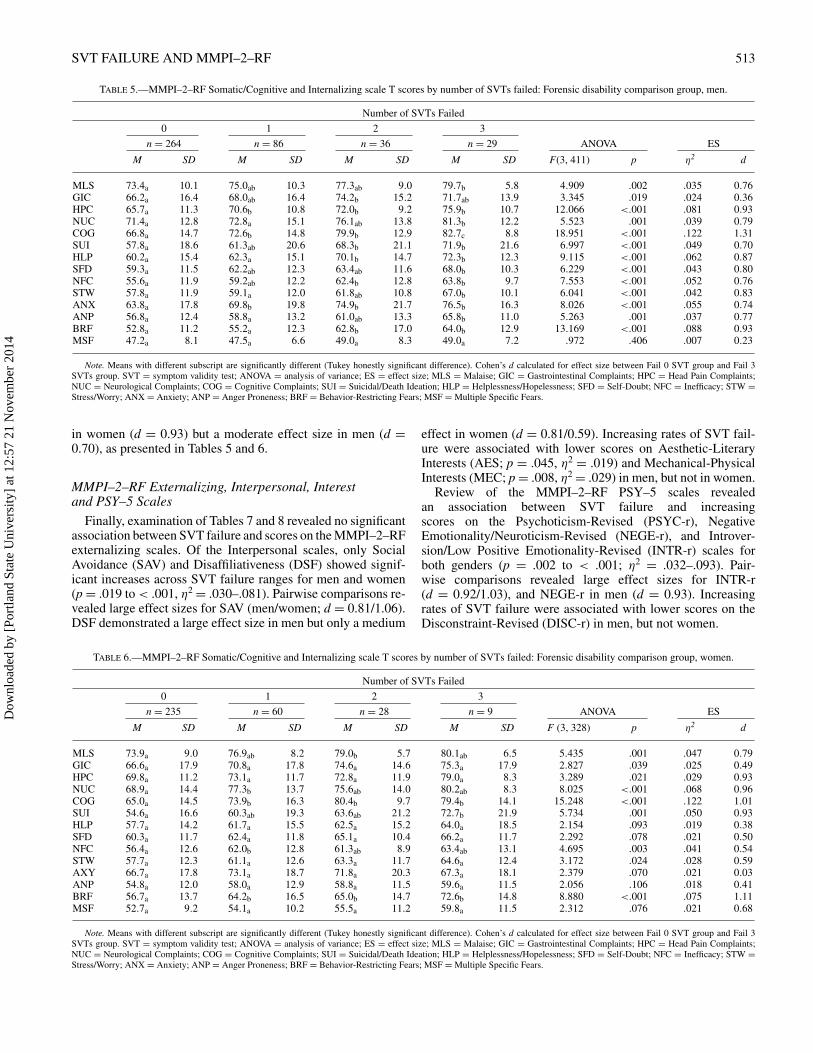
SVT failure was associated with increasing scores on allMMPI–2–RF Somatic/Cognitive scales, in both men andwomen. The largest overall effect size was obtained for theCognitive Complaints (COG) scale (men/women; p < .001,η2 = .122/.122). Pairwise comparisons of T scores of the twoSVT ranges (i.e., Fail 0 SVTs vs. Fail 3 SVTs) revealed thelargest effect size for the COG scale (d = 1.31/1.01), followedby Head Pain Complaints (HPC) and Neurological Complaints(NUC; d = .79–.96). Review of the Internalizing scales re-vealed significant associations between SVT failure and in-creased scores on all scales except Multiple Specific Fears(MSF) for men. For women, SVT failure was associated withincreasing scores only on the Suicidal/Death Ideation (SUI),Inefficacy (NFC), Stress and Worry (STW), and Behavior Re-stricting Fears (BRF) scales. The largest overall association wasobtained on BRF (men/women; p < .001, η2 = .088/.075).Examination of the pairwise comparisons revealed large effectsizes on this scale (men/women; d = 0.93/1.11). The Suici-dal/Death Ideation (SUI) scale also produced a large effect size
Dow
nloa
ded
by [
Port
land
Sta
te U
nive
rsity
] at
12:
57 2
1 N
ovem
ber
2014
512 GERVAIS, WYGANT, SELLBOM, BEN-PORATH
TABLE 2.—MMPI–2–RF Validity scale T scores by number of SVTs failed: Forensic disability comparison group, women.
Number of SVTs Failed
0 1 2 3
n = 235 n = 60 n = 28 n = 9 ANOVA ES
M SD M SD M SD M SD F (3, 328) p η2 d
VRIN-r 50.9a 9.5 50.3a 8.5 51.7a 9.0 51.1a 13.3 .146 .932 .001 0.02TRIN-r 57.6a 6.9 56.7a 6.0 57.0a 5.4 57.6a 6.5 .378 .769 .003 0.01F-r 70.6a 19.8 82.2b 22.0 85.1b 22.3 90.4b 20.0 9.948 <.001 .083 0.99Fp-r 54.9a 13.3 61.5b 15.5 61.5ab 18.6 63.0ab 23.1 4.882 .002 .043 0.43Fs 66.7a 20.0 78.1b 23.7 77.0ab 22.4 81.8ab 18.9 6.949 <.001 .060 0.78FBS-r 77.0a 13.4 82.3b 15.3 85.5b 10.9 89.0b 9.4 6.717 <.001 .058 1.04L-r 55.8a 11.5 57.7a 10.9 58.3a 11.7 61.7a 12.1 1.393 .245 .013 0.50K-r 45.1a 10.2 41.6a 9.9 41.9a 11.3 43.1a 9.1 2.420 .066 .022 –0.21
Note. Means with different subscript are significantly different (Tukey honestly significant difference). Cohen’s d calculated for effect size between Fail 0 SVT group and Fail 3 SVTsgroup. SVT = symptom validity test; ANOVA = analysis of variance; ES = effect size; VRIN-r = Variable Response Inconsistency; TRIN-r = True Response Inconsistency; F-r =Infrequent Responses; Fp-r = Infrequent Psychopathology Responses; Fs = Infrequent Somatic Responses; FBS-r = Symptom Validity; L-r = Uncommon Virtues; K-r = AdjustmentValidity.
TABLE 3.—MMPI–2–RF H-O and RC scale T scores by number of SVTs failed: Forensic disability comparison group, men.
Number of SVTs Failed
0 1 2 3
n = 264 n = 86 n = 36 n = 29 ANOVA ES
M SD M SD M SD M SD F (3, 411) p η2 d
EID 62.8a 12.8 66.7abc 13.0 71.3bc 13.5 74.5c 10.3 11.286 <.001 .076 1.01THD 56.7a 12.9 60.4ab 15.2 63.7b 17.1 63.3ab 16.0 4.752 .003 .034 0.45BXD 57.1a 12.1 56.7a 12.2 53.0a 12.2 52.6a 9.3 2.226 .085 .016 –0.42RCd 63.6a 11.9 67.3ab 12.5 70.5bc 11.8 74.1c 10.1 10.091 <.001 .069 0.95RC1 71.4a 12.1 75.0ab 12.1 78.9bc 12.1 83.3c 12.1 11.854 <.001 .080 0.98RC2 63.5a 13.0 66.6a 14.7 74.2b 15.0 77.6b 12.5 14.725 <.001 .097 1.11RC3 53.6a 11.1 54.5a 12.1 53.5a 12.0 55.4a 10.5 .341 .796 .002 0.17RC4 56.7a 12.1 56.7a 12.3 54.6a 12.2 51.9a 10.2 1.637 .180 .012 –0.43RC6 59.3a 14.1 62.5a 15.6 65.4a 15.9 63.4a 14.3 2.750 .042 .020 0.29RC7 57.1a 13.3 60.9ab 14.1 64.7b 14.0 65.6b 10.5 6.907 <.001 .048 0.71RC8 57.3a 12.0 61.5b 13.9 64.1b 16.7 66.8b 13.5 7.722 <.001 .053 0.74RC9 52.0a 11.0 52.2a 10.9 48.4a 10.0 50.4a 9.1 1.359 .255 .010 –0.16
Note. Means with different subscript are significantly different (Tukey honestly significant difference). Cohen’s d calculated for effect size between Fail 0 SVT group and Fail 3 SVTsgroup. SVT = symptom validity test; ANOVA = analysis of variance; ES = effect size; H-O = Higher-Order; RC = Restructured Clinical; EID = Emotional/Internalizing Dysfunction;THD = Thought Dysfunction; BXD = Behavioral/Externalizing Dysfunction; RCd = Demoralization; RC1 = Somatic Complaints; RC2 = Low Positive Emotions; RC3 = Cynicism;RC4 = Antisocial Behavior; RC6 = Ideas of Persecution; RC7 = Dysfunctional Negative Emotions; RC8 = Aberrant Experiences; RC9 = Hypomanic Activation.
TABLE 4.—MMPI–2–RF H-O and RC scale T scores by number of SVTs failed: Forensic disability comparison group, women.
Number of SVTs Failed
0 1 2 3
n = 235 n = 60 n = 28 n = 9 ANOVA ES
M SD M SD M SD M SD F(3, 328) p η2 d
EID 63.7a 13.2 68.8b 13.0 71.2b 12.0 74.4ab 12.9 6.035 .001 .052 0.82THD 54.7a 11.4 59.3ab 14.6 62.8b 15.3 60.8ab 19.7 5.137 .002 .045 0.38BXD 46.9a 9.7 47.9a 11.4 46.4a 10.6 41.3a 5.6 1.126 .338 .010 –0.71RCd 63.2a 12.4 68.9b 11.5 70.9b 10.6 72.6ab 11.2 7.116 <.001 .061 0.80RC1 73.4a 12.9 79.7b 14.3 80.5b 12.1 85.4b 9.9 7.203 <.001 .062 1.04RC2 63.8a 13.2 67.6ab 13.8 71.5b 12.1 76.6b 15.9 5.782 .001 .050 0.88RC3 49.4a 10.9 53.5a 11.6 51.8a 11.6 47.9a 8.5 2.454 .063 .022 –0.15RC4 49.7a 10.5 50.2a 13.1 50.6a 11.4 43.6a 6.8 1.044 .373 .009 –0.69RC6 55.6a 12.4 59.8ab 14.7 65.4b 17.5 59.9ab 20.1 5.337 .001 .047 0.26RC7 57.6a 13.9 64.0b 15.7 63.3ab 14.8 63.0ab 17.6 4.146 .007 .037 0.34RC8 54.9a 11.5 61.3b 15.1 62.5b 13.9 62.0ab 18.4 6.712 <.001 .058 0.46RC9 45.7a 8.9 47.9a 10.1 47.5a 10.6 41.1a 5.5 2.077 .103 .019 –0.62
Note. Means with different subscript are significantly different (Tukey honestly significant difference). Cohen’s d calculated for effect size between Fail 0 SVT group and Fail 3 SVTsgroup. SVT = symptom validity test; ANOVA = analysis of variance; ES = effect size; H-O = Higher-Order; RC = Restructured Clinical; EID = Emotional/Internalizing Dysfunction;THD = Thought Dysfunction; BXD = Behavioral/Externalizing Dysfunction; RCd = Demoralization; RC1 = Somatic Complaints; RC2 = Low Positive Emotions; RC3 = Cynicism;RC4 = Antisocial Behavior; RC6 = Ideas of Persecution; RC7 = Dysfunctional Negative Emotions; RC8 = Aberrant Experiences; RC9 = Hypomanic Activation.
Dow
nloa
ded
by [
Port
land
Sta
te U
nive
rsity
] at
12:
57 2
1 N
ovem
ber
2014
SVT FAILURE AND MMPI–2–RF 513
TABLE 5.—MMPI–2–RF Somatic/Cognitive and Internalizing scale T scores by number of SVTs failed: Forensic disability comparison group, men.
Number of SVTs Failed
0 1 2 3
n = 264 n = 86 n = 36 n = 29 ANOVA ES
M SD M SD M SD M SD F(3, 411) p η2 d
MLS 73.4a 10.1 75.0ab 10.3 77.3ab 9.0 79.7b 5.8 4.909 .002 .035 0.76GIC 66.2a 16.4 68.0ab 16.4 74.2b 15.2 71.7ab 13.9 3.345 .019 .024 0.36HPC 65.7a 11.3 70.6b 10.8 72.0b 9.2 75.9b 10.7 12.066 <.001 .081 0.93NUC 71.4a 12.8 72.8a 15.1 76.1ab 13.8 81.3b 12.2 5.523 .001 .039 0.79COG 66.8a 14.7 72.6b 14.8 79.9b 12.9 82.7c 8.8 18.951 <.001 .122 1.31SUI 57.8a 18.6 61.3ab 20.6 68.3b 21.1 71.9b 21.6 6.997 <.001 .049 0.70HLP 60.2a 15.4 62.3a 15.1 70.1b 14.7 72.3b 12.3 9.115 <.001 .062 0.87SFD 59.3a 11.5 62.2ab 12.3 63.4ab 11.6 68.0b 10.3 6.229 <.001 .043 0.80NFC 55.6a 11.9 59.2ab 12.2 62.4b 12.8 63.8b 9.7 7.553 <.001 .052 0.76STW 57.8a 11.9 59.1a 12.0 61.8ab 10.8 67.0b 10.1 6.041 <.001 .042 0.83ANX 63.8a 17.8 69.8b 19.8 74.9b 21.7 76.5b 16.3 8.026 <.001 .055 0.74ANP 56.8a 12.4 58.8a 13.2 61.0ab 13.3 65.8b 11.0 5.263 .001 .037 0.77BRF 52.8a 11.2 55.2a 12.3 62.8b 17.0 64.0b 12.9 13.169 <.001 .088 0.93MSF 47.2a 8.1 47.5a 6.6 49.0a 8.3 49.0a 7.2 .972 .406 .007 0.23
Note. Means with different subscript are significantly different (Tukey honestly significant difference). Cohen’s d calculated for effect size between Fail 0 SVT group and Fail 3SVTs group. SVT = symptom validity test; ANOVA = analysis of variance; ES = effect size; MLS = Malaise; GIC = Gastrointestinal Complaints; HPC = Head Pain Complaints;NUC = Neurological Complaints; COG = Cognitive Complaints; SUI = Suicidal/Death Ideation; HLP = Helplessness/Hopelessness; SFD = Self-Doubt; NFC = Inefficacy; STW =Stress/Worry; ANX = Anxiety; ANP = Anger Proneness; BRF = Behavior-Restricting Fears; MSF = Multiple Specific Fears.
in women (d = 0.93) but a moderate effect size in men (d =0.70), as presented in Tables 5 and 6.
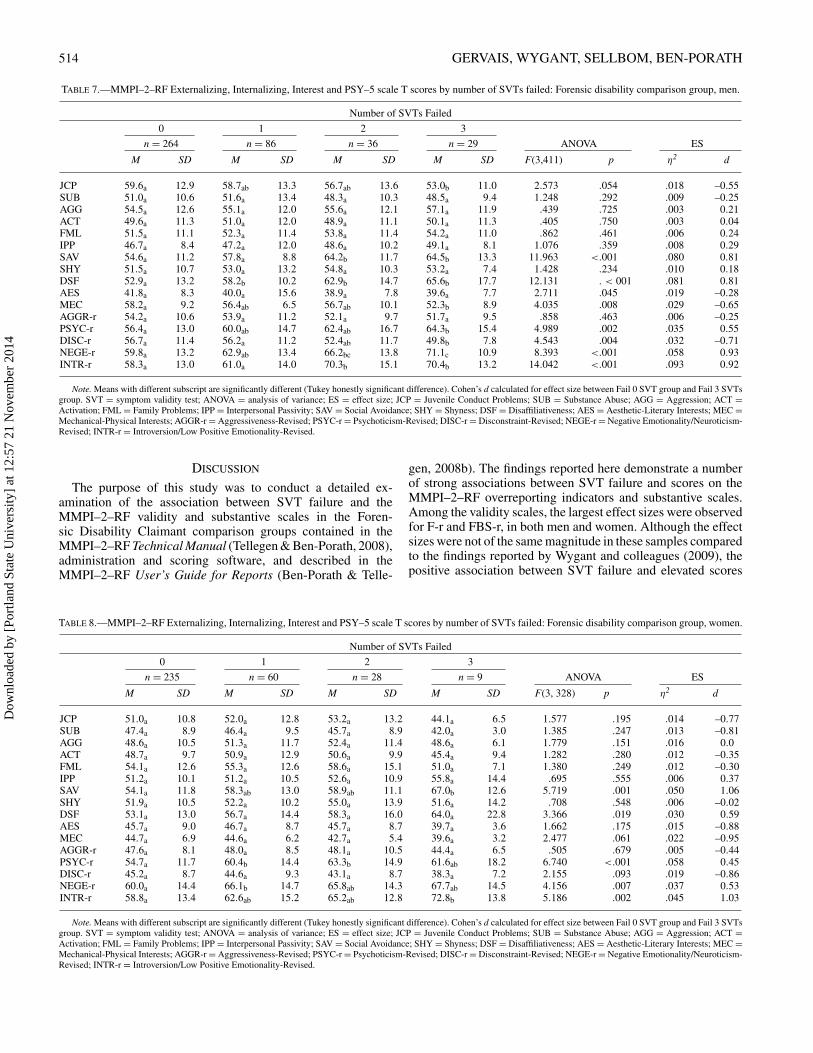
MMPI–2–RF Externalizing, Interpersonal, Interestand PSY–5 Scales
Finally, examination of Tables 7 and 8 revealed no significantassociation between SVT failure and scores on the MMPI–2–RFexternalizing scales. Of the Interpersonal scales, only SocialAvoidance (SAV) and Disaffiliativeness (DSF) showed signif-icant increases across SVT failure ranges for men and women(p = .019 to < .001, η2 = .030–.081). Pairwise comparisons re-vealed large effect sizes for SAV (men/women; d = 0.81/1.06).DSF demonstrated a large effect size in men but only a medium
effect in women (d = 0.81/0.59). Increasing rates of SVT fail-ure were associated with lower scores on Aesthetic-LiteraryInterests (AES; p = .045, η2 = .019) and Mechanical-PhysicalInterests (MEC; p = .008, η2 = .029) in men, but not in women.
Review of the MMPI–2–RF PSY–5 scales revealedan association between SVT failure and increasingscores on the Psychoticism-Revised (PSYC-r), NegativeEmotionality/Neuroticism-Revised (NEGE-r), and Introver-sion/Low Positive Emotionality-Revised (INTR-r) scales forboth genders (p = .002 to < .001; η2 = .032–.093). Pair-wise comparisons revealed large effect sizes for INTR-r(d = 0.92/1.03), and NEGE-r in men (d = 0.93). Increasingrates of SVT failure were associated with lower scores on theDisconstraint-Revised (DISC-r) in men, but not women.
TABLE 6.—MMPI–2–RF Somatic/Cognitive and Internalizing scale T scores by number of SVTs failed: Forensic disability comparison group, women.
Number of SVTs Failed
0 1 2 3
n = 235 n = 60 n = 28 n = 9 ANOVA ES
M SD M SD M SD M SD F (3, 328) p η2 d
MLS 73.9a 9.0 76.9ab 8.2 79.0b 5.7 80.1ab 6.5 5.435 .001 .047 0.79GIC 66.6a 17.9 70.8a 17.8 74.6a 14.6 75.3a 17.9 2.827 .039 .025 0.49HPC 69.8a 11.2 73.1a 11.7 72.8a 11.9 79.0a 8.3 3.289 .021 .029 0.93NUC 68.9a 14.4 77.3b 13.7 75.6ab 14.0 80.2ab 8.3 8.025 <.001 .068 0.96COG 65.0a 14.5 73.9b 16.3 80.4b 9.7 79.4b 14.1 15.248 <.001 .122 1.01SUI 54.6a 16.6 60.3ab 19.3 63.6ab 21.2 72.7b 21.9 5.734 .001 .050 0.93HLP 57.7a 14.2 61.7a 15.5 62.5a 15.2 64.0a 18.5 2.154 .093 .019 0.38SFD 60.3a 11.7 62.4a 11.8 65.1a 10.4 66.2a 11.7 2.292 .078 .021 0.50NFC 56.4a 12.6 62.0b 12.8 61.3ab 8.9 63.4ab 13.1 4.695 .003 .041 0.54STW 57.7a 12.3 61.1a 12.6 63.3a 11.7 64.6a 12.4 3.172 .024 .028 0.59AXY 66.7a 17.8 73.1a 18.7 71.8a 20.3 67.3a 18.1 2.379 .070 .021 0.03ANP 54.8a 12.0 58.0a 12.9 58.8a 11.5 59.6a 11.5 2.056 .106 .018 0.41BRF 56.7a 13.7 64.2b 16.5 65.0b 14.7 72.6b 14.8 8.880 <.001 .075 1.11MSF 52.7a 9.2 54.1a 10.2 55.5a 11.2 59.8a 11.5 2.312 .076 .021 0.68
Note. Means with different subscript are significantly different (Tukey honestly significant difference). Cohen’s d calculated for effect size between Fail 0 SVT group and Fail 3SVTs group. SVT = symptom validity test; ANOVA = analysis of variance; ES = effect size; MLS = Malaise; GIC = Gastrointestinal Complaints; HPC = Head Pain Complaints;NUC = Neurological Complaints; COG = Cognitive Complaints; SUI = Suicidal/Death Ideation; HLP = Helplessness/Hopelessness; SFD = Self-Doubt; NFC = Inefficacy; STW =Stress/Worry; ANX = Anxiety; ANP = Anger Proneness; BRF = Behavior-Restricting Fears; MSF = Multiple Specific Fears.
Dow
nloa
ded
by [
Port
land
Sta
te U
nive
rsity
] at
12:
57 2
1 N
ovem
ber
2014
514 GERVAIS, WYGANT, SELLBOM, BEN-PORATH
TABLE 7.—MMPI–2–RF Externalizing, Internalizing, Interest and PSY–5 scale T scores by number of SVTs failed: Forensic disability comparison group, men.
Number of SVTs Failed
0 1 2 3
n = 264 n = 86 n = 36 n = 29 ANOVA ES
M SD M SD M SD M SD F(3,411) p η2 d
JCP 59.6a 12.9 58.7ab 13.3 56.7ab 13.6 53.0b 11.0 2.573 .054 .018 –0.55SUB 51.0a 10.6 51.6a 13.4 48.3a 10.3 48.5a 9.4 1.248 .292 .009 –0.25AGG 54.5a 12.6 55.1a 12.0 55.6a 12.1 57.1a 11.9 .439 .725 .003 0.21ACT 49.6a 11.3 51.0a 12.0 48.9a 11.1 50.1a 11.3 .405 .750 .003 0.04FML 51.5a 11.1 52.3a 11.4 53.8a 11.4 54.2a 11.0 .862 .461 .006 0.24IPP 46.7a 8.4 47.2a 12.0 48.6a 10.2 49.1a 8.1 1.076 .359 .008 0.29SAV 54.6a 11.2 57.8a 8.8 64.2b 11.7 64.5b 13.3 11.963 <.001 .080 0.81SHY 51.5a 10.7 53.0a 13.2 54.8a 10.3 53.2a 7.4 1.428 .234 .010 0.18DSF 52.9a 13.2 58.2b 10.2 62.9b 14.7 65.6b 17.7 12.131 . < 001 .081 0.81AES 41.8a 8.3 40.0a 15.6 38.9a 7.8 39.6a 7.7 2.711 .045 .019 –0.28MEC 58.2a 9.2 56.4ab 6.5 56.7ab 10.1 52.3b 8.9 4.035 .008 .029 –0.65AGGR-r 54.2a 10.6 53.9a 11.2 52.1a 9.7 51.7a 9.5 .858 .463 .006 –0.25PSYC-r 56.4a 13.0 60.0ab 14.7 62.4ab 16.7 64.3b 15.4 4.989 .002 .035 0.55DISC-r 56.7a 11.4 56.2a 11.2 52.4ab 11.7 49.8b 7.8 4.543 .004 .032 –0.71NEGE-r 59.8a 13.2 62.9ab 13.4 66.2bc 13.8 71.1c 10.9 8.393 <.001 .058 0.93INTR-r 58.3a 13.0 61.0a 14.0 70.3b 15.1 70.4b 13.2 14.042 <.001 .093 0.92
Note. Means with different subscript are significantly different (Tukey honestly significant difference). Cohen’s d calculated for effect size between Fail 0 SVT group and Fail 3 SVTsgroup. SVT = symptom validity test; ANOVA = analysis of variance; ES = effect size; JCP = Juvenile Conduct Problems; SUB = Substance Abuse; AGG = Aggression; ACT =Activation; FML = Family Problems; IPP = Interpersonal Passivity; SAV = Social Avoidance; SHY = Shyness; DSF = Disaffiliativeness; AES = Aesthetic-Literary Interests; MEC =Mechanical-Physical Interests; AGGR-r = Aggressiveness-Revised; PSYC-r = Psychoticism-Revised; DISC-r = Disconstraint-Revised; NEGE-r = Negative Emotionality/Neuroticism-Revised; INTR-r = Introversion/Low Positive Emotionality-Revised.
DISCUSSION
The purpose of this study was to conduct a detailed ex-amination of the association between SVT failure and theMMPI–2–RF validity and substantive scales in the Foren-sic Disability Claimant comparison groups contained in theMMPI–2–RF Technical Manual (Tellegen & Ben-Porath, 2008),administration and scoring software, and described in theMMPI–2–RF User’s Guide for Reports (Ben-Porath & Telle-
gen, 2008b). The findings reported here demonstrate a numberof strong associations between SVT failure and scores on theMMPI–2–RF overreporting indicators and substantive scales.Among the validity scales, the largest effect sizes were observedfor F-r and FBS-r, in both men and women. Although the effectsizes were not of the same magnitude in these samples comparedto the findings reported by Wygant and colleagues (2009), thepositive association between SVT failure and elevated scores
TABLE 8.—MMPI–2–RF Externalizing, Internalizing, Interest and PSY–5 scale T scores by number of SVTs failed: Forensic disability comparison group, women.
Number of SVTs Failed
0 1 2 3
n = 235 n = 60 n = 28 n = 9 ANOVA ES
M SD M SD M SD M SD F(3, 328) p η2 d
JCP 51.0a 10.8 52.0a 12.8 53.2a 13.2 44.1a 6.5 1.577 .195 .014 –0.77SUB 47.4a 8.9 46.4a 9.5 45.7a 8.9 42.0a 3.0 1.385 .247 .013 –0.81AGG 48.6a 10.5 51.3a 11.7 52.4a 11.4 48.6a 6.1 1.779 .151 .016 0.0ACT 48.7a 9.7 50.9a 12.9 50.6a 9.9 45.4a 9.4 1.282 .280 .012 –0.35FML 54.1a 12.6 55.3a 12.6 58.6a 15.1 51.0a 7.1 1.380 .249 .012 –0.30IPP 51.2a 10.1 51.2a 10.5 52.6a 10.9 55.8a 14.4 .695 .555 .006 0.37SAV 54.1a 11.8 58.3ab 13.0 58.9ab 11.1 67.0b 12.6 5.719 .001 .050 1.06SHY 51.9a 10.5 52.2a 10.2 55.0a 13.9 51.6a 14.2 .708 .548 .006 –0.02DSF 53.1a 13.0 56.7a 14.4 58.3a 16.0 64.0a 22.8 3.366 .019 .030 0.59AES 45.7a 9.0 46.7a 8.7 45.7a 8.7 39.7a 3.6 1.662 .175 .015 –0.88MEC 44.7a 6.9 44.6a 6.2 42.7a 5.4 39.6a 3.2 2.477 .061 .022 –0.95AGGR-r 47.6a 8.1 48.0a 8.5 48.1a 10.5 44.4a 6.5 .505 .679 .005 –0.44PSYC-r 54.7a 11.7 60.4b 14.4 63.3b 14.9 61.6ab 18.2 6.740 <.001 .058 0.45DISC-r 45.2a 8.7 44.6a 9.3 43.1a 8.7 38.3a 7.2 2.155 .093 .019 –0.86NEGE-r 60.0a 14.4 66.1b 14.7 65.8ab 14.3 67.7ab 14.5 4.156 .007 .037 0.53INTR-r 58.8a 13.4 62.6ab 15.2 65.2ab 12.8 72.8b 13.8 5.186 .002 .045 1.03
Note. Means with different subscript are significantly different (Tukey honestly significant difference). Cohen’s d calculated for effect size between Fail 0 SVT group and Fail 3 SVTsgroup. SVT = symptom validity test; ANOVA = analysis of variance; ES = effect size; JCP = Juvenile Conduct Problems; SUB = Substance Abuse; AGG = Aggression; ACT =Activation; FML = Family Problems; IPP = Interpersonal Passivity; SAV = Social Avoidance; SHY = Shyness; DSF = Disaffiliativeness; AES = Aesthetic-Literary Interests; MEC =Mechanical-Physical Interests; AGGR-r = Aggressiveness-Revised; PSYC-r = Psychoticism-Revised; DISC-r = Disconstraint-Revised; NEGE-r = Negative Emotionality/Neuroticism-Revised; INTR-r = Introversion/Low Positive Emotionality-Revised.
Dow
nloa
ded
by [
Port
land
Sta
te U
nive
rsity
] at
12:
57 2
1 N
ovem
ber
2014

SVT FAILURE AND MMPI–2–RF 515
on the overreporting validity indicators is consistent with theintent of these scales as measures of overreported psychologi-cal dysfunction (F-r), extreme psychopathology (Fp-r), somaticcomplaints (Fs), and noncredible reports of somatic or cogni-tive symptoms (FBS-r). The association between SVT failureand the overreporting indicators provides support for the con-struct validity of these indicators. The relatively smaller effectsizes observed for Fp-r and Fs, as well as their failure to addunique predictive utility above and beyond F-r and FBS-r, are notunexpected given their specific focus on overreported extremepsychopathology and infrequent somatic complaints, symptomsthat are less directly associated with cognitive functioning andcognitive symptom validity test failure than are F-r and FBS-r(Wygant et al., 2009). Larger effects sizes on Fp-r would beexpected in settings with a greater likelihood of exaggeratedextreme psychopathology (e.g., criminal forensic settings) thanin civil disability settings (Wygant et al., 2007). Similarly, onewould expect stronger effect sizes for Fs in civil forensic ordisability settings where the demand characteristics encouragea focus on physical symptoms and disability, and the symptomvalidity measures more directly evaluate overreporting of phys-ical symptoms and disability (Sellbom et al., 2010; Wygant etal., 2009).
The Higher-Order and RC scales mirrored the pattern ob-served with the overreporting validity indicators, with the largesteffect sizes noted on EID, RCd, RC1, and RC2, reflecting in-creasing reports of emotional and somatic distress. This is notunexpected given the nature of the forensic disability samplesin which the primary diagnoses involved chronic pain, depres-sion, and anxiety/PTSD. In the context of failed SVTs, the largeeffect sizes observed on these scales suggest that reports of ex-treme emotional distress, demoralization and other depressivesymptoms, and multiple or extreme somatic complaints quitelikely involve considerable distortion and must be interpretedwith appropriate caution. There were gender differences in theeffect sizes, with men obtaining larger effect sizes for EID, RCd,and RC2. Although the reasons for this are not immediately evi-dent, one possible interpretation of this observation is the largerpercentage of men involved in workers’ compensation claims(75.5%) compared to women (43.3%) in the forensic disabilityclaimant samples. In many workers’ compensation claims, thepsychological assessment is requested as part of the adjudicationprocess to assist in determining eligibility for financial benefits.The presence of this external incentive, combined with worry orapprehension regarding the outcome of the claim, could quiterealistically influence test-taking attitude on the MMPI–2–RF,and contribute to focused overreporting of emotional distressreflected on these scales.
The effect sizes noted for the RC scales in the samples re-ported here are, with the exception of RC1, generally larger thanthe effect sizes observed by Thomas and Youngjohn (2009). Thisdiscrepancy is probably related to a number of factors includingdifferent sample characteristics, and a different complement ofSVTs in the test battery. The large association between SVTfailure and the COG scale is not unexpected and supports theconclusions of Gervais, Ben-Porath, and Wygant (2009), whodescribed elevated scores on the scale as potentially indicatingoverreporting of subjective cognitive symptoms. The large effectsizes noted for BRF in both men and women raise the question ofsymptom overreporting in traumatic stress claims, which consti-tute over one third of the Forensic Disability Claimant sample.
In such cases the elevated BRF could be tapping overreportedsymptoms of avoidance of the workplace or work-related activ-ities. The large effect sizes observed on INTR-r probably reflectthe depressive symptoms and social disengagement shared withRC2.
SVT failure is generally accepted in clinical and forensicneuropsychology as an indication of noncredible symptom re-porting and unreliable test data. Previous research suggests thatSVT scores are not significantly influenced by psychopathol-ogy, including psychosis (e.g., Duncan, 2005; Gorissen, Sanz,& Schmand, 2005) and depression (e.g., Ashendorf, Constanti-nou, & McCaffrey, 2004; Rees, Tombaugh, & Boulay, 2001).Moreover, several experimental studies suggest that physicalpathology cannot account for the level of poor performanceexhibited by individuals failing SVTs. Indeed, Etherton, Bian-chini, Greve, and Ciota (2005) and Etherton, Bianchini, Ciota,and Greve (2005) demonstrated that performance on the TOMMand the Reliable Digit Span (RDS; Greiffenstein, Baker, & Gola,1994) is unaffected by laboratory-induced pain. In a study exam-ining the effect of coaching on SVT performance in chronic painpatients, Gervais, Green, Allen, and Iverson (2001) concludedthat coaching affected performance on the target SVT but noton the SVT that was not coached. Pain and fatigue at the time ofassessment did not affect SVT performance. Additionally, Ger-vais, Russell, et al. (2001) demonstrated that individuals withfibromyalgia (which includes somatic symptoms such as pain)who were involved in disability-related evaluations had signif-icantly higher WMT failure rates than patients with the samecondition who were not involved in disability suits. Therefore,it is unlikely that genuine psychopathology and physical im-pairment in the sample reported here (as indicated by scores onthe substantive scales of the MMPI–2–RF) can account for poorperformance on SVTs.
Claimants undergoing forensic disability evaluations can uti-lize self-report instruments, such as the MMPI–2–RF, as a“voice” through which they can communicate their internal,subjective experiences. Whereas cognitive SVTs are utilizedclinically to establish whether the claimant exerted sufficienteffort to produce reliable and valid results on cognitive test-ing, claimants might perceive the SVTs as an opportunity todemonstrate their impaired neurocognitive functioning and es-tablish support for their claim. The results of this study sug-gest that, as claimants exhibit poor performance on SVTs, theyalso utilize the MMPI–2–RF to establish and demonstrate theirclaimed emotional distress and somatic problems, albeit in anoncredible manner. In effect, they utilize these two types oftests concurrently to communicate their claimed neurocognitiveimpairment, physical complaints, and emotional dysfunction,utilizing the separate modalities of the tests (i.e., performance-based SVTs and self-report items).
Claimants undergoing forensic disability evaluations can uti-lize the MMPI–2–RF as a means of genuinely describing theiradjustment in the emotional, somatic, and cognitive dimensions,but the clinician must always be aware of the possibility ofresponse bias, particularly where this is associated with over-reporting of emotional, somatic, and cognitive symptoms andclaimed disability. The association between poor performanceon cognitive SVTs and elevated scores on the MMPI–2–RF ob-served in this study suggests that the response bias tapped by thecognitive SVTs is also reflected in the symptom overreportingnoted in the test protocols. Not only was this evident for the
Dow
nloa
ded
by [
Port
land
Sta
te U
nive
rsity
] at
12:
57 2
1 N
ovem
ber
2014

516 GERVAIS, WYGANT, SELLBOM, BEN-PORATH
COG scale, as one would expect, but a similar pattern was alsoobserved for reporting of general emotional distress (EID), andcomplaints of depression, pessimism, and social introversion(RC2 and INTR-r). The greater the number of SVTs failed, thegreater the degree of overreporting noted on the MMPI–2–RFprotocols. Hence, when elevated MMPI–2–RF scores are ob-tained in the context of failed SVTs, the clinician should stronglysuspect noncredible symptom reporting and rule this out beforeconcluding that MMPI–2–RF results indicate the presence ofpsychopathology or the influence of somatic symptoms.
The findings of this study support the interpretive guidelinesspecified by Ben-Porath and Tellegen (2008a, 2008b) that el-evations on the MMPI–2–RF overreporting validity indicatorsshould alert the clinician to the possibility of an invalid protocol,or a protocol that must be interpreted cautiously due to distortionarising from exaggerated symptom reports. This study was lim-ited in that the Forensic Disability Claimant sample is composedprimarily of non-head-injury disability claimants derived fromone clinical setting. We expect that the association between SVTfailure and elevated MMPI–2–RF overreporting validity indica-tors and substantive scales observed in this study will generalizeto other forensic disability settings and samples, and potentiallyto other settings, but further research is necessary to addressthis question. Given the importance and widespread use of theMMPI–2 and growing use of the MMPI–2–RF in forensic neu-ropsychology, future studies should examine the association be-tween SVT performance and the MMPI–2–RF in patients withTBI and other neurological conditions, psychiatric conditions,and chronic pain in disability- and non-disability-seeking set-tings. This study utilized a number of well-known free-standingSVTs. Further studies using different SVT methodologies andembedded measures would also be useful to determine the ex-tent to which performance on alternative SVT procedures isassociated with overreporting on the MMPI–2–RF.
ACKNOWLEDGMENTS
Yossef Ben-Porath is a paid consultant to the MMPI–2–RFpublisher, the University of Minnesota Press, and distributor,Pearson. He receives royalties on sales of MMPI–2–RF materi-als.
Portions of this study were presented at the 44th Annual Sym-posium on Recent Research with the MMPI–2, MMPI–2–RF,& MMPI–A, May 2009, Minneapolis, MN. The authors thankAnthony Tarescavage for his assistance with the tables.
REFERENCES
Allen, L., Conder, R. L., Green, P., & Cox, D. R. (1997). CARB’ 97 manual forthe Computerized Assessment of Response Bias. Durham, NC: CogniSyst.
American Psychiatric Association. (1994). Diagnostic and statistical manual ofmental disorders (4th ed.). Washington, DC: Author.
American Psychiatric Association. (2000). Diagnostic and statistical manual ofmental disorders (4th ed., text revision). Washington, DC: Author.
Ashendorf, L., Constantinou, M., & McCaffrey, R. J. (2004). The effect ofdepression and anxiety on the TOMM in community-dwelling older adults.Archives of Clinical Neuropsychology, 19, 125–130.
Ben-Porath, Y. S. (2007, November). Introducing the MMPI–2–RF (Restruc-tured Form). Presentation at the annual meeting of the National Academy ofNeuropsychology, Scottsdale, AZ.
Ben-Porath, Y. S., & Tellegen, A. (2008a). MMPI–2–RF (Minnesota Multipha-sic Personality Inventory–2–Restructured Form) manual for administration,scoring, and interpretation. Minneapolis: University of Minnesota Press.
Ben-Porath, Y. S., & Tellegen, A. (2008b). MMPI–2–RF (Minnesota Multi-phasic Personality Inventory–2–Restructured Form) user’s guide for reports.Minneapolis: University of Minnesota Press.
Bianchini, K. J., Greve, K. W., & Glynn, G. (2005). On the diagnosis of malin-gered pain-related disability: Lessons from cognitive malingering research.The Spine Journal, 5, 404–417.
Blaskewitz, N., Merten, T., & Kathmann, N. (2008). Performance of childrenon symptom validity tests: TOMM, MSVT & FIT. Archives of Clinical Neu-ropsychology, 23, 379–391.
Boone, K. B., & Lu, P. H. (1999). Impact of somatoform symptomatology oncredibility of cognitive performance. The Clinical Neuropsychologist, 13,414–419.
Brockhaus, R., & Merten, T. (2004). Neuropsychologische Diagnostik subopti-malen Leistungsverhaltens mit dem Word Memory Test (WMT) [Neuropsy-chological assessment of suboptimal performance: The Word Memory Test].Nervenarzt, 75, 882–887.
Brockhaus, R., Peker, O., & Fritze, E. (2003, July). Testing effort in Turk-ish speaking subjects: Validation of a translation of the Word Memory Test(WMT). Poster presented at the GNP and INS conference, Berlin, Germany.
Bush, S. S., Ruff, R. M., Troster, A. I., Barth, J. T., Koffler, S. P., Pliskin, N. H.,. . . Silver, C. H. (2005). Symptom validity assessment: Practice issues andmedical necessity NAN Policy & Planning Committee. Archives of ClinicalNeuropsychology, 20, 419–426.
Butcher, J. N., Graham, J. R., Ben-Porath, Y. S., Tellegen, A., Dahlstrom, W. G.,& Kaemmer, B. (2001). MMPI–2: Manual for administration and scoring(Rev. ed.). Minneapolis: University of Minnesota Press.
Duncan, A. (2005). The impact of cognitive and psychiatric impairment of psy-chotic disorders on the Test of Memory Malingering (TOMM). Assessment,12, 123–129.
Etherton, J. L., Bianchini, K. J., Ciota, M. A., & Greve, K. W. (2005). ReliableDigit Span is unaffected by laboratory-induced pain: Implications for clinicaluse. Assessment, 12, 101–106.
Etherton, J. L., Bianchini, K. J., Greve, K. W., & Ciota, M. A. (2005). Testof Memory Malingering performance is unaffected by laboratory-inducedpain: Implications for clinical use. Archives of Clinical Neuropsychology, 20,375–384.
Gervais, R. O., Ben-Porath, Y. S., & Wygant, D. B. (2009). Empirical correlatesand interpretation of the MMPI–2–RF Cognitive Complaints (COG) scale.The Clinical Neuropsychologist, 23, 996–1015.
Gervais, R. O., Ben-Porath, Y. S., Wygant, D. B., & Green, P. (2007). Devel-opment and validation of a Response Bias Scale (RBS) for the MMPI–2.Assessment, 14, 196–208.
Gervais, R. O., Ben-Porath, Y. S., Wygant, D. B., & Sellbom, M. (2010). In-cremental validity of the MMPI–2–RF over-reporting scales and RBS inassessing the veracity of memory complaints. Archives of Clinical Neuropsy-chology, 25, 274–284.
Gervais, R., Green, P., Allen, L. M., & Iverson, G. L. (2001). Effects of coachingon symptom validity testing in chronic pain patients presenting for disabilityassessments. Journal of Forensic Neuropsychology, 2, 1–19.
Gervais, R. O., Rohling, M. L., Green, P., & Ford, W. (2004). A com-parison of WMT, CARB, and TOMM failure rates in non-head in-jury disability claimants. Archives of Clinical Neuropsychology, 19, 475–487.
Gervais, R. O., Russell, A. S., Green, P., Allen, L. M., Ferrari, R., & Pieschl, S.D. (2001). Effort testing in fibromyalgia patients with disability incentives.Journal of Rheumatology, 28, 1892–1899.
Gorissen, M., Sanz, J. C., & Schmand, B. (2005). Effort and cognition inschizophrenia patients. Schizophrenia Research, 78, 199–208.
Green, P. (2003). Green’s Word Memory Test for Windows: User’s manual.Edmonton, Alberta, Canada: Green’s Publishing.
Green, P. (2004). Green’s Medical Symptom Validity Test (MSVT): User’s man-ual. Edmonton, Alberta, Canada: Green’s Publishing.
Green, P. (2007). The pervasive influence of effort on neuropsychological tests.Physical Medicine and Rehabilitation Clinics of North America, 18, 43–68.
Green, P., Flaro, L., & Courtney, J. (2009). Examining false positives on theWord Memory Test in adults with mild traumatic brain injury. Brain Injury,23, 741–750.
Dow
nloa
ded
by [
Port
land
Sta
te U
nive
rsity
] at
12:
57 2
1 N
ovem
ber
2014

SVT FAILURE AND MMPI–2–RF 517
Green, P., Lees-Haley, P. R., & Allen, L. M. (2003). The Word Memory Testand the validity of neuropsychological test scores. In J. Hom & R. L. Denney(Eds.), Detection of response bias in forensic neuropsychology (pp. 97–124).New York, NY: Haworth Medical Press.
Greiffenstein, M. F., Baker, W. J., & Gola, T. (1994). Validation of malingeredamnesia measures with a large clinical sample. Psychological Assessment, 6,218–224.
Greve, K. W., Bianchini, K. J., Black, W., Heinly, M. T., Love, J. M., Swift,D. A., and Ciota, M. (2006). Classification accuracy of the Test of MemoryMalingering in persons reporting exposure to environmental and industrialtoxins: Results of a known-groups analysis. Archives of Clinical Neuropsy-chology, 21, 439–448.
Haber, A. H., & Fichtenberg, N. L. (2006). Replication of the Test of MemoryMalingering (TOMM) in a traumatic brain injury and head trauma sample.The Clinical Neuropsychologist, 20, 524–532.
Heilbronner, R. L., Sweet, J. J., Morgan, J. E., Larrabee, G. J., Millis, S. R., &Conference Participants. (2009). American Academy of Clinical Neuropsy-chology consensus conference statement on the neuropsychological assess-ment of effort, response bias, and malingering. The Clinical Neuropsycholo-gist, 23, 1093–1129.
Howe, L. S. L., Anderson, A. M., Kaufman, D. A. S., Sachs, B. C., & Loring,D. W. (2007). Characterization of the Medical Symptom Validity Test inevaluation of clinically referred memory disorders clinic patients. Archivesof Clinical Neuropsychology, 22, 753–761.
Howe, L. S. L., & Loring, D. W. (2009). Classification accuracy and predictiveability of the Medical Symptom Validity Test’s dementia profile and generalmemory impairment profile. The Clinical Neuropsychologist, 23, 329–342.
Iverson, G., Green, P., & Gervais, R. (1999). Using the Word Memory Test todetect biased responding in head injury litigation. The Journal of CognitiveRehabilitation, 17, 4–8.
Iverson, G. L., Le Page, J., Koehler, B. E., Shojania, K., & Badii, M. (2006).Test of Memory Malingering (TOMM) scores are not affected by chronic painor depression in patients with fibromyalgia. The Clinical Neuropsychologist,21, 532–546.
Larrabee, G. J. (1998). Somatic malingering on the MMPI and MMPI–2 inpersonal injury litigants. The Clinical Neuropsychologist, 12, 179–188.
Larrabee, G. J. (2003). Exaggerated MMPI–2 symptom report in personal in-jury litigants with malingered neurocognitive deficit. Archives of ClinicalNeuropsychology, 18, 673–686.
Rees, L. M., Tombaugh, T. N., & Boulay, L. (2001). Depression and the Test ofMemory Malingering. Archives of Clinical Neuropsychology, 16, 501–506.
Richman, J., Green, P., Gervais, R., Flaro, L., Merten, T., Brockhaus, R., &Ranks, D. (2006). Objective tests of symptom exaggeration in independentmedical examinations. Journal of Occupational and Environmental Medicine,48, 303–311.
Rogers, R., Bagby, R. M., & Dickens, S. E. (1992). Structured Interview ofReported Symptoms: Professional manual. Odessa, FL: Psychological As-sessment Resources.
Sellbom, M., & Bagby, R. M. (2010). The detection of over-reported psy-chopathology with the MMPI–2–RF (Restructured Form) validity scales.Psychological Assessment, 22, 757–767.
Sellbom, M., Toomey, J. A., Wygant, D. B., Kucharski, L. T., & Duncan, S.(2010). Utility of the MMPI–2–RF (Restructured Form) validity scales indetecting malingering in a criminal forensic setting: A known-groups design.Psychological Assessment, 22, 22–31. doi:10.1037/a0018222
Simon, M. (2007). Performance of mentally retarded forensic patients onthe test of memory malingering. Journal of Clinical Psychology, 63, 339–344.
Slick, D. J., Sherman, E., & Iverson, G. L. (1999). Diagnostic criteria for ma-lingered neurocognitive dysfunction: Proposed standards for clinical practiceand research. The Clinical Neuropsychologist, 13, 545–561.
Tan, J., Slick, D., Strauss, E., & Hultsch, D. F. (2002). Malingering strate-gies on symptom validity tests. The Clinical Neuropsychologist, 16, 495–505.
Tellegen, A., & Ben-Porath, Y. S. (2008). MMPI–2–RF (Minnesota MultiphasicPersonality Inventory–2–Restructured Form) technical manual. Minneapolis:University of Minnesota Press.
Tellegen, A., Ben-Porath, Y. S., McNulty, J. L., Arbisi, P. A., Graham, J. R., &Kaemmer, B. (2003). The MMPI–2 Restructured Clinical (RC) Scales: Devel-opment, validation, and interpretation. Minneapolis: University of MinnesotaPress.
Thomas, M. L., & Youngjohn, J. R. (2009). Let’s not get hysterical: Comparingthe MMPI–2 validity, clinical, and RC scales in TBI litigants tested for effort.The Clinical Neuropsychologist, 23, 1067–1084.
Tombaugh, T. N. (1996). Test of Memory Malingering. Toronto, Ontario,Canada: MultiHealth Systems.
Tydecks, S., Merten, T., & Gubbay, J. (2006). The Word Memory Testand the One-in-Five-Test in an analogue study with Russian speak-ing participants. International Journal of Forensic Psychology, 1, 29–37.
Wygant, D. B., Ben-Porath, Y. S., Arbisi, P. A., Berry, D. T., Freeman, D.B., & Heilbronner, R. L. (2009). Examination of the MMPI–2 RestructuredForm (MMPI–2–RF) validity scales in civil forensic settings: Findings fromsimulation and known group samples. Archives of Clinical Neuropsychology,24, 671–680.
Wygant, D. B., Gervais, R. O., & Ben-Porath, Y. S. (2005). Correlationbetween Word Memory Test (WMT) performance and the MMPI–2 Re-structured Clinical (RC) scales. Archives of Clinical Neuropsychology, 20,892.
Wygant, D. B., Sellbom, M., Ben-Porath, Y. S., Stafford, K. P., Freeman, D. B.,& Heilbronner, R. L. (2007). The relation between symptom validity testingand MMPI–2 scores as a function of forensic evaluation context. Archives ofClinical Neuropsychology, 22, 489–499.
Wygant, D. B., Sellbom, M., Gervais, R. O., Ben-Porath, Y. S., Stafford, K.P., Freeman, D. B., & Heilbronner, R. L. (2010). Further validation of theMMPI–2 and MMPI–2–RF Response Bias Scale: Findings from disabilityand criminal forensic settings. Psychological Assessment, 22, 745–756.
Youngjohn, J. R. (1995). Confirmed attorney coaching prior to neuropsycho-logical evaluation. Assessment, 2, 279–283.
Youngjohn, J. R., Burrows, L., & Erdal, K. (1995). Brain damage or compen-sation neurosis? The controversial post-concussion syndrome. The ClinicalNeuropsychologist, 9, 112–123.
Dow
nloa
ded
by [
Port
land
Sta
te U
nive
rsity
] at
12:
57 2
1 N
ovem
ber
2014