Embed Size (px)
Citation preview

http://informahealthcare.com/bijISSN: 0269-9052 (print), 1362-301X (electronic)
Brain Inj, Early Online: 1–10! 2014 Informa UK Ltd. DOI: 10.3109/02699052.2014.947619
ORIGINAL ARTICLE
Assessment practices of speech-language pathologists for cognitivecommunication disorders following traumatic brain injury in adults:An international survey
Matthew Frith1,2,3, Leanne Togher2,3, Alison Ferguson4, Wayne Levick5, & Kimberley Docking2,3
1Kaleidoscope: Children, Young People & Families, Hunter New England Local Health District, NSW, Australia, 2Speech Pathology, Faculty of Health
Sciences, University of Sydney, Sydney, Australia, 3NHMRC Centre of Research Excellence in Brain Recovery, Sydney, Australia, 4School of Humanities
& Social Sciences, and 5School of Psychology University of Newcastle, Newcastle, Australia
Abstract
Primary objective: This study’s objective was to examine the current assessment practices ofSLPs working with adults with acquired cognitive communication impairments following a TBI.Methods and procedures: Two hundred and sixty-five SLPs from the UK, the US, Canada,Australia and New Zealand responded to the online survey stating the areas of communicationfrequently assessed and the assessment tools they use.Main outcomes and results: SLPs reported that they routinely assessed functional communi-cation (78.8%), whereas domains such as discourse were routinely assessed by less than half ofthe group (44.3%). Clinicians used aphasia and cognitive communication/high level languagetools and tools assessing functional performance, discourse, pragmatic skills or informalassessments were used by less than 10% of the group. The country and setting of servicedelivery influenced choice of assessment tools used in clinical practice.Conclusions: These findings have implications for training of SLPs in a more diverse range ofassessment tools for this clinical group. The findings raise questions regarding the statisticalvalidity and reliability of assessments currently used in clinical practice. It highlights the needfor further research into how SLPs can be supported in translating current evidence about theuse of assessment tools into clinical practice.
Keywords
Assessment, cognitive, language, survey
History
Received 25 August 2013Revised 16 May 2014Accepted 20 July 2014Published online 26 August 2014
Introduction
Speech Language Pathologists (SLPs) play an integral role in
the rehabilitation of a person after a traumatic brain injury
(TBI). SLP assessment and intervention commences in the
acute setting with a focus primarily on dysphagia manage-
ment [1], observation and monitoring of communication
abilities during post-traumatic amnesia [2] and further on
in the rehabilitation process SLPs have an important contri-
bution in cognitive rehabilitation, with assessment and
management of cognitive communication disorders [3].
Rehabilitation after a TBI is a specialized field and requires
expert clinical decision-making skills where there is an
understanding of the person’s impairments in communication
and how this relates to their ability to participate in real life
activities [4].
Considering this is a complex specialized field, there is
limited consensus in the literature to assist the SLP to
make appropriate clinical decisions regarding the type of
methodology and complimentary assessment choices in this
rehabilitation setting. One approach is to use locally regulated
SLP practice guidelines, but internationally there are incon-
sistencies amongst speech language pathology associations
on practice guidelines for the assessment and management
of cognitive communication disorders. In countries such as
Australia and New Zealand there are no practice guidelines or
position papers regarding the selection of relevant assess-
ments in this specialized field of practice and in the UK,
while the Royal College of Speech & Language Therapists
(RCSLT) have produced guidelines [5] for the assessment and
management of aphasia, as yet there is no reference to
cognitive communication disorders. However, more detailed
guidelines are available through the US and Canada. The
American Speech-Language-Hearing Association [6, 7] have
produced a number of general guidelines and position papers
on the assessment of cognitive communication disorders,
while The College of Audiologists and Speech Language
Pathologists of Ontario [8] have produced detailed preferred
practice guidelines for both the assessment and management
of cognitive communication disorders. Both papers make
reference to assessment of cognitive functions such as
attention, concentration, executive function, memory/new
learning as well as linguistic components such as auditory
Correspondence: Matthew Frith, Speech Pathologist, Kaleidoscope,HNE LHD PO BOX 2563 Dangar, NSW, Australia 2309, Australia.Tel: +61(0)249 257963. Fax: +61(0)249257955. E-mail:[email protected]
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y D
okuz
Eyl
ul U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.

comprehension, oral expression, discourse, word finding,
reading rate and comprehension and written expression.
The Academy of Neurologic Communication Disorders
and Sciences (ANCDS) has similarly published guidelines on
standardized testing [9] and non-standardized testing [10].
Surprisingly, these guidelines have received very little
citation, but they do provide valuable information for the
SLP to guide clinical decision-making. The ANCDS surveyed
clinicians and test distributors about assessments that are
recommended to be used in TBI and cognitive communica-
tion disorders [9]. These were reviewed by the ANCDS
committee for reliability and validity and of 85 tests, only six
were recommended for adult patients that met the majority of
criteria for reliability and validity. The tests which were
recommended by the ANCDS committee included
the Functional Independence Measure FIM [11]; American
Speech Language Hearing Association Functional
Assessment of Communication Skills in Adults ASHA
FACS [12]; Communication Activities of Daily Living
Second Edition CADL-2 [13]; Repeatable Battery for the
Assessment of Neuropsychological Status RBANS [14]; and
the Western Aphasia Battery WAB [15]. Some of the
described [10] non-standardized assessment procedures used
by Speech Language Pathologists focused mainly on dis-
course procedures including monologic and conversational
discourse. The authors discussed some of the inherent
weaknesses with non-standardized approaches, such as lack
of normative data to distinguish impaired and normal
discourse abilities within the context of the person and the
influences context has on discourse. It was also recommended
that rating scales and checklists used in discourse and
pragmatic assessments about the person and communication
partner should be used with caution due to weak psychometric
properties and the level of training required to reliably use
them.
Not much has been documented on the influence of
assessment choices for SLPs working with people with TBI.
Surveys of SLPs working in TBI in the US have highlighted
that undergraduate training does not provide adequate training
in TBI [16, 17]. The questions that a clinician should ask
themselves when deciding on an assessment have been
described in detail [18]. These four questions consisted of:
(1) Does the test identify a cognitive communication
disorder?; (2) Does it characterize the components contribut-
ing to the performance?; (3) Are the test results appropriate
for the real life situations?; and (4) Does it assist with
decisions about intervention? The statistical aspects of test
construction and its importance in test selection has been
discussed [9], however a survey conducted in the US
suggested that, despite poor validity and reliability, the
choice of assessment by SLPs was most commonly based
on whether it identified deficits and assisted with goal-setting
and therapeutic planning [19]. The same survey demonstrated
that test choice was also more likely to be based on advice
from fellow colleagues, workshops and conferences rather
than evidence-based literature [19]. Ylvisaker et al. [4]
identified that evidence statements (for example guidelines)
can also impact on clinical decision-making. Time factors,
such as the available clinical time and the time required
to administer a test, have been described as impacting on
assessment choices [19–21]. Years of clinical experience has
also been highlighted as another factor that may impact on
clinical decision-making skills [4], as well as the benefits
of a mentor or experienced clinician to assist with decision-
making.
While some guidelines exist in some countries around the
world, with very little else to guide an SLP’s decision
regarding assessment selection, there has been some research
into the assessment practices of Speech Language
Pathologists working in TBI. The difficulties inherent with
this population include the heterogeneous nature of the TBI
population and the varying severity. SLPs have been reported
to use more standardized assessment practices in the acute
setting with the minimally conscious patient [22], such as the
Wessex Head Injury Matrix (WHIM [23]); and recent research
has also shown that, when a patient is in PTA (post-traumatic
amnesia), the SLP is more likely to monitor and observe any
changes than conduct a formal assessment [24].
More recently, there has been a stronger focus on
assessments for cognitive communication disorders after a
mild TBI in studies coming from the US and Australia [25].
SLPs in the US reported using the Ross Information
Processing Assessment [26], Boston Diagnostic Aphasia
Battery [27] and Boston Naming Test [28]. These results
were similar to the work by Frank and Barrineau [19], who
conducted a large scale study where severity of injury was not
defined. The initial data on assessment protocols for combat-
injured servicemen with a mild TBI highlighted selection of
assessments that were different again as part of clinical
practice. These included the Functional Assessment of Verbal
Reasoning Strategies (FAVRES) [29] and the Attention
Processing Test. Informal measures were included to examine
word finding and pragmatic deficits. Some Australian studies
have used case studies to highlight particular assessments
to use with TBI including sub-tests such as the inference/
listening comprehension sub-test from adolescent language
tests such as the Test of Language Competence [30] and The
Word Test 2 [31] vocabulary sub-test [32]. Test selection has
also been examined in the acute setting and it was found that
the Cognitive Linguistic Quick Test [33] was useful in
identifying deficits in an acute setting of 83 patients with
varying severity of TBI injury [34].
To the authors’ knowledge, there is no study which has
compared communication assessment practices in the field
of TBI between countries, although there has been some
comparison of aphasia assessment practice [35]. For aphasia,
there have been similarities between countries with the use of
the Western Aphasia Battery [15], Boston Diagnostic Aphasia
Examination [27] and Boston Naming Test [28] primarily
used by SLPs in Australia, Canada, the UK and the US. The
PALPA [36] and Mount Wilga [37] were reported to be
popular assessments in the UK and Australia compared with
Canada and the US. However, there was no difference in the
type of assessment tools used when comparing the practice
of speech pathologists working in acute settings compared to
community outpatient services. Assessment practices were
consistent across Australia in regard to the Mount Wilga High
Level Language assessment [37] predominately used by over
70% of clinicians in acute and community setting for CVA/
aphasia [20, 35, 38].
2 M. Frith et al. Brain Inj, Early Online: 1–10
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y D
okuz
Eyl
ul U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.

Few aphasia and TBI studies have focused on assessment
choices across settings, mainly focusing on one setting [38]
and not comparing choice of assessment tools across an
inpatient and community setting. Studies which have
reviewed assessment choice across settings have shown no
difference in the choice of tools [19, 20]. Studies have also
attempted to guide the clinician to move away from impair-
ment type tests such as aphasia assessments [39, 40] and
apply the ICF (International Classification of Functioning,
Disability and Health) model to assessment choice, with
assessments such as the FAVRES [29] and ASHA FACS [12]
for tools to assess activities and participation.
There has also been a focus on informal assessment in TBI,
primarily concentrating on discourse. Togher [41] reviewed
the theoretical approaches to discourse analysis and Coelho
[42] discussed the limitations which continue to be a barrier
to implementing this procedure. Previous research has
reported responses from clinicians who were asked about
informal assessment procedures. In literature pertaining to
both aphasia and TBI, SLPs reported using informal proced-
ures which primarily focused on observations, interviews with
the family and client and developing tools for other assess-
ments for their own use [19, 35, 38]. In the studies discussed
previously surveying SLPs about assessment practices, dis-
course analysis or discourse sampling was very rarely
reported.
Most of the research in assessment practices has focused
on the tools used and not on SLP’s perception about what they
feel are the areas of communication they assess. There is only
one paper to date which has documented this from the
perspective of SLPs [43]. This study documented SLPs
working in the US and documented that the aspects of
communication that were reported by the SLPs to be assessed
included receptive and expressive language, pragmatics,
reading, writing and cognition.
The present study was designed to identify the current
clinical assessment tools used by speech language patholo-
gists working with adults who have sustained a cognitive
communication disorder after a traumatic brain injury. The
aims of the study were to survey SLPs working in TBI and:
(1) Identify differences in the reported use of assessment
tools/protocols by SLPs in different countries.
(2) Identify whether setting of care influences the reported
use of assessment protocols/tools used by SLPs
(3) Identify whether years of experience influences the
reported use of assessment tools/protocols used by SLPs.
(4) Identify whether there was a link between all three
variables: country, setting of care and years of
experience.
Method
Participants
Speech Language Pathologists (SLPs) who reported having
specific clinical expertise in the rehabilitation of adults with
traumatic brain injury (TBI) were identified through publicly
available databases including; Speech Pathology Australia
(SPA), New Zealand Speech-Language Therapists’
Association (NZSTA), Royal College of Speech and
Language Therapists (RCSLT), Canadian Association of
Speech Language Pathologists (CASLPA) and the American
Speech-Language-Hearing Association (ASHA). These pro-
fessionals were invited to complete an online survey through
email invitation or web link using survey monkey (www.sur-
veymonkey.com). Email invitation allowed the SLPs to have
multiple opportunities to complete the survey without losing
information to which they had already responded. Three
reminders were automatically sent over a period of 8 weeks.
SLPs were also identified through Speech Pathology
Interest Groups in Brain Injury via the UK, Australia, New
Zealand, Canada and the US, as well as managers of Speech
Pathology departments throughout a number of hospitals and
community health centres. The dissemination of the survey
was modified using a general Web Link using the online
survey tool Survey Monkey (www.surveymonkey.com). This
link was not personalized to any one participant and an email
outlining the study and survey was sent to moderators of the
interest groups and managers of health services asking them
to disseminate to staff and/or colleagues. Ethics approval was
granted by the Hunter New England Human Research Ethics
Committee of Hunter New England Health reference 10/04/
21/5/10.
It was estimated that for both Australia and New Zealand
and the UK there was a greater than 50% response rate with a
lower response rate (525%) from the US/Canada group. There
was also a high rate of undeliverable emails for the US/
Canada group, which may have been an indication that the
database email addresses that were extracted were not
accurate. Overall, of those who responded, 63.4% of partici-
pants were recruited through email invitation and 36.6%
were recruited via web link. A higher number of partici-
pants were recruited through a web link in the UK
(62.3%) compared to Australia/New Zealand (13.6%) and
the US/Canada (37.2%).
Survey design
A 12 item questionnaire was developed to evaluate the
assessment practice of SLPs working in traumatic brain
injury. It formed part of a larger study, with the first seven
questions included in the analysis presented in this paper. The
seven questions asked included geographical location, clinical
setting and years of experience. A 5-point category rating
scale using fixed anchor points was used to identify SLPs’
perceptions of how often they assessed aspects of language
and communication (receptive language, expressive language,
pragmatic skills, discourse, word-finding ability, vocabulary,
high level language, problem-solving, reading decoding,
reading comprehension, written language and functional
communication). Fixed anchor points were used as they
have been recommended as more reliable when making
quantitative comparisons [44].
Descriptors were provided for each point on the rating
scale and, given the difficulties of interpreting responses
when ambiguous adverbs are used as descriptors [45], a
percentage of clinical time was provided as an additional
qualifier with the anchor points to guide the clinician in
making an accurate judgement of their assessment practices.
The quantifiers used for clinical time included; Never¼ 0%,
Infrequent 525% of clinical time, Somewhat frequent¼ 25–
DOI: 10.3109/02699052.2014.947619 Cognitive communication following TBI in adults 3
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y D
okuz
Eyl
ul U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.

550% of clinical time, Frequently450–585% of clinical time
and the Majority of the time485% of clinical time.
SLPs were also provided with four open response text
boxes and asked to list four assessments that they use
frequently and find useful in identifying the strengths and
weaknesses of a client and assists with goal-setting and
intervention practices. These descriptors were based on
general clinical questions and principles a SLP is likely to
use when using an assessment [18].
Terminology
The generic term ‘language-based communication disorders’
was used to ensure SLPs did not respond about assessment
practices relating to dysarthria, dyspraxia and dysphagia. The
term ‘cognitive communication’ was deliberately not used in
order to prevent any response-bias by SLPs, which may return
a false positive to assessing areas of cognitive communica-
tion. The chosen terminology was utilized to promote
respondents to think broadly about what aspects of language
and communication they assess in clinical practice, with areas
relating to cognitive communication derived from responses
collected.
Analysis
Responses from Survey Monkey software were downloaded
into IBM SPSS (Statistical Package for the Social Sciences
version 21). Countries were characterized into three groups
(Australia and New Zealand; UK; US and Canada). Years of
experience were characterized into 10 years and less and
greater than 10 years and setting was characterized into
Inpatient acute/rehabilitation and Community rehabilitation.
Due to the high number of assessments reported by the
respondents, a classification system was developed based on a
Simmons-Mackie et al. [21] study which categorized assess-
ments into linguistic/cognitive, functional, subjective/qualita-
tive and vague/other. In the current study, these categories
were broadened to include aphasia assessments, cognitive
communication/high level language assessments, cognitive/
neuropsychology assessments, assessment of functional per-
formance (including literacy), informal language and cogni-
tive assessments, naming and word-finding assessments,
discourse and/or pragmatic skills assessments and other.
Assessments were categorized based on expert opinion from
five SLPs working in the area of traumatic brain injury and
aphasia. Chi-Square analysis was conducted as recommended
for categorical and ordinal data [46] to make comparison
between country, years of experience and setting of care.
Results
Responses received from 265 Speech Language Pathologists
(SLPs) are reported. Of these, 2.6% did not respond to the
rating scale question which asked how often the individual
assessed different areas language and communication; 7.6%
did not provide a list of assessments commonly used in
clinical practice in the open response text box.
Demographic information
Demographic information is represented in Table I. As shown,
the majority of SLPs reported that they worked in
metropolitan centres, while the remaining group reported
working in rural and/or remote areas. The community
rehabilitation setting predominately consisted of clinicians
working in outpatient and community rehabilitation facilities
(56.5%), private practice (17.6%) and university clinics
(14.5%).
Pearson Chi-Square analysis was conducted to confirm
whether geographical location impacted on group differences
for the key variables, experience, country and setting. There
was a significant difference between geographical location
and years of experience. SLPs with greater than 10 years
of experience were less likely to work in rural and remote
areas than SLPs with less than 10 years’ experience, �2
(1, n¼ 265)¼ 7.30, p¼ 0.007.
A three-way table with Pearson Chi-Square analysis was
conducted for employment setting and clinical experience in
each country group. Results indicated a significant relation-
ship between clinical experience and employment setting �2
(1, n¼ 263)¼ 15.31, p¼ 0.00. A relative risk ratio was
obtained to determine the likelihood of country influencing
employment setting. This is described in Table II.
In all country categories there was a higher likelihood
of experienced SLPs (greater than 10 years) working in
community rehabilitation settings compared with inpatient
settings. This was only significant for the US/Canada
category.
A logistic regression was conducted to determine the
presence of significant relationships between the three
variables of clinical experience, employment setting and
country. However, this was not significant according to the
Wald test, �2 (2, n¼ 263)¼ 2.78, p¼ 0.25.
Table I. Speech language pathologists (n¼ 265) demographicinformation.
SLPs’responses (n)
Percentage ofSLPs (%)
Geographical settingMetropolitan 210 78.9Rural & Remote 56 21.1
CountryAustralia/New Zealand 81 30.6US/Canada 113 42.6
UK 69 26Unknown 2 0.8Employment setting
Inpatient acute/rehabilitation 134 50.6Community rehabilitation 131 49.4
Years of experience510 years 121 45.7410 years 144 54.3
Table II. Relative risk for country influencing years of experience andemployment setting.
Country group Relative risk Level of significance
AUS/NZ 1.37 �2 (1, n¼ 81)¼ 1.22, p¼ 0.27UK 1.31 �2 (1, n¼ 69)¼ 1.42, p¼ 0.23US/CA 2.03 �2 (1, n¼ 113)¼ 12.84, p¼ 0.00
4 M. Frith et al. Brain Inj, Early Online: 1–10
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y D
okuz
Eyl
ul U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.

Areas of communication assessed after traumaticbrain injury
SLPs reported functional communication skills (78.8%) to
be the most routinely assessed communication skill when
assessing a person after TBI. Table III highlights the
percentage of SLPs who routinely assessed each component
of communication.
Country
There were significant differences between the country where
the SLP resides and certain areas of communication. SLPs
in US/Canada (CA) reported routinely assessing problem-
solving more frequently than the UK and Australia (AUS)/
New Zealand (NZ) (�2 (8, n¼ 251)¼ 33.88, p¼ 0.00); and
frequently assessing written language (�2 (8, n¼ 243)
¼ 20.89, p¼ 0.007) and reading decoding (�2 (8, n¼ 249)
¼ 17.01, p¼ 0.030), more than SLPs in the UK and AUS/NZ.
A higher number of SLPs in the US/CA reported routinely
assessing discourse (55.7%) compared with AUS/NZ (32.0%)
and the UK (38.7%); however, this was not significant (�2
(8, n¼ 243)¼ 14.41, p¼ 0.072).
Setting of care
There were no significant differences when using a Pearson
Chi-Square between areas of communication assessed and
setting of care worldwide. In inpatient acute/rehabilitation
settings there was a higher percentage of SLPs who routinely
assessed each area of communication compared with SLPs
working in a community setting.
Years of experience
A Pearson Chi-Square revealed significant differences
between certain areas of communication assessed when
compared with years of experience of the SLP. SLPs with
more experience (410 years of experience) reported routinely
assessing more key areas of cognitive communication than
SLPs with less than 10 years of experience. These included;
pragmatic skills (�2 (4, n¼ 286)¼ 25.28, p¼ 0.00), discourse
(�2 (4, n¼ 277)¼ 25.28, p¼ 0.02), high level language (�2
(4, n¼ 287)¼ 11.99, p¼ 0.01), problem-solving (�2 (4,
n¼ 253)¼ 29.56, p¼ 0.00), word-finding (�2 (4, n¼ 288)
¼ 10.58, p¼ 0.03) and written language (�2 (4, n¼ 286)
¼ 17.17, p¼ 0.002). In addition, reading (decoding) (�2 (4,
n¼ 288)¼ 10.58, p¼ 0.003), reading comprehension (�2 (4,
n¼ 286)¼ 13.42, p¼ 0.009) and receptive language (�2 (4,
n¼ 288)¼ 10.26, p¼ 0.04) were reported as routinely
assessed more often in the more experienced clinician.
Assessment tools used in clinical practice
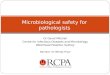
Overall, aphasia assessments (27.7% of SLPs) and cognitive
communication/high level language assessments (31.7% of
SLPs) were the most frequently used category of tools, as
depicted in Figure 1.
Cognitive Communication / High Level
Language Assessment
Assessment of Functional Performance (incl:
literacy)
Informal Language & Cognitive Assessments
(derived by clinicians &/or SP Dep’t)
Cognitive Neuropsychology Assessments
Naming & / or Word-Finding Assessment
Discourse & / or Pragmatic Skills
Assessment
Aphasia Assessment
Assessments Tools Used by SLPs by Category
Other
0 50 100
(9.2%)
(9.9%)
(5.6%)
(5.4%)
(6.2%)
(4.2%)
150 200 250
(27.7%)
(31.7%)
Number of Responses (n)
Total = 779
Figure 1. Distribution of assessment categories as reported by SLPs by all country groups.
Table III. Areas of communication routinely assessed by SLPs.
Area of communication Average %
Functional communication 78.8%Receptive language 70.7%Expressive language 70.3%Word-finding skills 62.9%High level language 62.6%Pragmatic skills 58.9%Problem-solving skills 57.5%Reading comprehension 48.4%Discourse 44.3%Written language 40%Reading (decoding) 34.8%Vocabulary 31.5%
DOI: 10.3109/02699052.2014.947619 Cognitive communication following TBI in adults 5
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y D
okuz
Eyl
ul U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.

Each assessment category contained assessment tools
which were reported to be utilized more commonly than
others. The aphasia assessment category consisted of a large
number of assessments led by the Boston Diagnostic Aphasia
Examination (BDAE) [27], which was reportedly used by
23% of SLPs, closely followed by the Western Aphasia
Battery (WAB) [15] at 21.7%. Fewer assessment tools were
reported in the cognitive communication/high level language
assessment category. The Mount Wilga High Level Language
assessment (MWHLL) [37] was used by 35.2% of clinicians,
followed by the Measure of Cognitive Linguistic Ability
(MCLA) [47] on 35.2%. In the Assessment of Functional
Performance (incl: literacy) category, The Functional
Assessment of Verbal Reasoning and Executive Strategies
(FAVRES) [29] was the most popular tool at 36.4% and in the
Cognitive/Neuropsychology Assessment category, the Ross
Information Processing Assessment (RIPA) [26] was the most
popular with 27.8%. A variety of other standardized cognitive
assessments were also included in this category. The Boston
Naming Test (BNT) [28] was the most frequently used
assessment in the Naming and/or Word Finding Assessment
category, with 66.7% of SLPs reporting their use of that
particular tool. The La Trobe Communication Questionnaire
(LCQ) [48] was the most popular tool in the Discourse/
Pragmatic Skills Assessment category, with 35.4% reporting
use of the assessment, followed by The Awareness of Social
Inference Test (TASIT) [49], with less than 20%. Various
outcome measures and paediatric language assessments
comprised the other category.
Country
A Pearson chi-square was conducted to determine if there was
a difference in assessment tools used between countries.
Results indicated a significant difference between countries
�2 (14, n¼ 779)¼ 97.31, p¼ 0.00. Table IV shows the
comparison of assessment tools by SLPs from each country.
SLPs in the US/CA reported a lower use of Cognitive
Communication/High Level Language Assessment tools
while SLPs in AUS/NZ reported significantly higher use.
In contrast, SLPs in the US/CA reported higher use of
Cognitive/Neuropsychology Assessment tools when com-
pared with SLPs in the UK and AUS/NZ. However, SLPs
in AUS/NZ reported higher use of informal language and
cognitive assessments and slightly higher use of naming/word
finding assessments and discourse and pragmatic skills
assessments. SLPs in the US/CA reported lower use of
assessment tools for discourse and pragmatic skills.
Particular assessment tools were also reported as more
popular by country. In AUS/NZ and the UK there was less
variability in assessment tools reported compared with the US
and Canada, which mostly consisted of cognitive/neuropsych-
ology assessments. AUS/NZ and the UK also had very similar
popularity with assessment tools. In AUS/NZ the most
reported assessment tools used included the MWHLL [37]
with 77.2%, MCLA [47] with 45.6%, informal assessment
practices with 32.9% and Psycholinguistic Assessment of
Language Processing in Adult Acquired Aphasia (PALPA)
[36] with 30.4%.
In the UK the most reported assessment tool was the
MCLA [47] at 55.4%, followed by CAT [50] at 46%,
MWHLL [37] at 43% and the PALPA [36] at 40%. In the
US/CA, the WAB [15] and BDAE [27] were most popular at
30.5% and the Scales of Cognitive Ability for Traumatic
Brain Injury (SCATBI) [51] at 29.5%, CLQT [33] and
informal assessment practices both at 24% and the RIPA [26]
on 23% were the most frequently used assessments. See Table
V for the popular assessment tools in each country.
Setting of care
A Pearson chi-square was conducted to determine if there was
a difference in assessments tools used within inpatient and
community settings. Results indicated a significant difference
between setting of care (�2 (14, n¼ 779)¼ 18.60, p¼ 0.01).
Table VI shows the comparison of assessment tools by setting.
Discourse was the only assessment category which was
significantly different amongst settings with discourse and
pragmatic skills assessment more likely to be completed in a
community setting. Most assessment categories were report-
edly used more often in an inpatient setting, except for
discourse (which was significant), cognitive assessments,
word-finding assessments and other assessments.
Years of experience
There were no significant differences with reported level
experience and assessment tools used by SLPs �2 (7,
n¼ 779)¼ 4.17, p¼ 0.760. There was also very little variance
Table IV. Comparison of assessment tools by country.
Country (% of use)
Assessment tool Average % AUS/NZ UK US/CA
Aphasia Assessment 27.7 25.9 32.7 25.9Cognitive Communication/High Level Language 31.7 39.9* (+) 33.2 23.6* (�)Cognitive/Neuropsychology Assessments 9.2 0.8* (�) 6.6 18.4* (+)Assessment of Functional Performance (incl: Literacy) 9.9 8.0 6.6 13.8* (+)Informal Language/Cognitive Assessment 5.6 9.5* (+) 2.4* (�) 4.6Naming and/or Word Finding Assessment 5.4 3.0* (�) 6.2 6.9Discourse and/or Pragmatic Skills Assessment 6.2 9.1* (+) 6.2 3.6* (�)Other Assessment 4.2 3.8 6.2 3.3
An adjusted standardized residuals test was carried out to determine if there were differences amongst countries on particular assessment tools.Residuals which exceeded ± 2 are presented, with a + indicating significantly higher use of assessment tool compared to average of all SLPs.A � indicates significantly less use of that assessment tool compared to average of SLPs who participated in survey. *indicates p50.001.
6 M. Frith et al. Brain Inj, Early Online: 1–10
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y D
okuz
Eyl
ul U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.

between assessments used between clinicians with greater
experience and, while it was not significant, more experi-
enced clinicians (410 years) were more likely to complete a
cognitive/neuropsychology and discourse/pragmatic skills
assessment and less likely to conduct an informal language/
cognitive assessment with a client after a traumatic brain
injury.
Discussion
This study’s primary objective was to examine the current
assessment practices of SLPs working with adults with
acquired cognitive communication impairments following a
TBI. It aimed to identify potential differences in the use of
assessment tools and protocols by SLPs across prominent
English speaking countries worldwide and whether setting of
care and years of clinical experience influenced these choices.
The results of the worldwide survey of clinicians in this field
informed each of these areas and highlighted a number of
clinical and research implications.
Overall, when assessing adults communication skills after
a TBI, SLPs reported assessing functional communication
skills the most frequently in clinical practice followed by
receptive and expressive language skills. Areas of communi-
cation considered to be sensitive to TBI [52, 53], such as
pragmatic skills, word finding skills, higher level language
abilities, discourse, literacy and problem-solving skills, were
not routinely assessed by SLPs, regardless of country, setting
or years of experience. In particular, discourse/pragmatic
skills assessment tools were used by less than 10% of the
SLPs surveyed and findings showed that discourse assess-
ments currently used included checklists such as the LCQ [48]
or the social communication assessment TASIT [52]. These
assessments have already had research conducted to evaluate
their validity and reliability which have been positive [52, 54].
These results about the assessment of discourse may contrib-
ute to a possible trend in the literature, suggesting that
perceived time taken and ease of transcription, training, the
decision process regarding the type of assessment/tool and
translating the findings into clinical practice may still be
possible deterrents for a SLP to implement discourse analysis
into clinical practice [42].
Interestingly, while Functional Communication was rated
as the most routinely assessed area of communication,
impairment-based assessments designed for aphasia and
high level language were noted to be the most prevalently
used by SLPs internationally. To date, only one assessment in
this category has been recommended for use in this popula-
tion of adults with TBI [9]: the WAB [15]. Further research
needs to evaluate why other assessments in the category of
aphasia assessments that were revealed by the survey, such as
the PALPA [36], CAT [50] and BDAE [27], are used in
clinical practice if impairment-based aphasia tools are
generally not reported in the literature to be sensitive to TBI
nor considered appropriate to the targeted function in
everyday life [39]. Most of the assessments commonly used
in studies examining cognitive communication impairments
in TBI were not identified as preferred assessment tools in
clinical practice in this study, except for the SCATBI [51],
which again has not consistently proved sensitive to milder
deficits after TBI [32, 55].
Differences were also noted between the countries repre-
sented in the survey in regards to the assessment of specific
areas of communication as well as the assessment tools used.
In the US and Canada (US/CA), SLPs more frequently
assessed areas of communication such as problem-solving,
written language and reading compared to their colleagues in
Australia/New Zealand (AUS/NZ) and the UK. As high-
lighted by past research [43], SLPs in the US are using a high
number of cognitive assessments compared to linguistic
assessments and this may be a reflection of the guidelines
distributed in the US and Canada [6–8], which highlights
cognition as an area of assessment for the SLP. Studies which
have reviewed the role of the SLP in regards to assessment of
cognition have demonstrated the overlapping role between
SLPs and Neuropsychologists [56]. A large majority of
Neuropsychologists saw the role of the SLPs was to assess
cognition as part of an assessment of communication, but
there was very little collaboration with pre-assessment
planning which had implications for integrity of psychomet-
ric assessments and the reporting of results as each discip-
line had its own interpretation and perspective view [56].
Table VI. Comparisons of assessment tools by setting.
Average(%)
Inpatient(%)
Community(%)
Aphasia Assessment 27.7 29.8 25.6Cognitive Communication/
High Level Language31.7 33.9 29.5
Cognitive/NeuropsychologyAssessments
9.2 7.9 10.6
Assessment of FunctionalPerformance (incl: Literacy)
9.9 10.5 9.3
Informal Language/CognitiveAssessments
5.6 6.4 4.9
Naming and/or Word FindingAssessments
5.4 4.8 5.9
Discourse and/or Pragmatic SkillsAssessments
6.2 3.1* (�) 9.3* (+)
Other 4.2 3.6 4.9
An adjusted standardized residuals test was carried out to determine ifthere were differences setting on particular assessment tools. Residualswhich exceeded ± 2 are presented with a +, indicating significantlyhigher use of assessment tool compared to average of all SLPs. A �indicates significantly less use of that assessment tool compared toaverage of SLPs who participated in survey. *indicates p¼ 0.01.
Table V. Popular assessment tools by country.
OverallAustralia/
New Zealand UK US/Canada
1 MWHLL MWHLL MCLA WAB/BDAE2 MCLA MCLA CAT SCATBI3 BDAE PALPA MWHLL CLQT/Informal4 WAB Informal PALPA RIPA
MWHLL, Mt Wilga High Level Language [37]; MCLA, Measure ofCognitive Linguistic Ability [47]; BDAE, Boston Diagnostic AphasiaExamination [27]; WAB, Western Aphasia Battery [15]; PALPA,Psycholinguistic Assessment of Language Processing in AdultAcquired Aphasia [36]; CAT, Comprehensive Aphasia Test [50];CLQT, Cognitive Linguistic Quick Test [33]; Informal, Informal testsmade up by the clinician; SCATBI, Scales of Cognitive Ability forTraumatic Brain Injury [51]; RIPA, Ross Information ProcessingAssessment [26].
DOI: 10.3109/02699052.2014.947619 Cognitive communication following TBI in adults 7
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y D
okuz
Eyl
ul U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.

This has implications for clinical practice about the clinical
decision-making rationale behind choosing cognitive-based
assessments over linguistic-based assessments.
Conversely, the results of the present study demonstrated
that cognitive communication and high level language
assessments (CC/HLL) were used significantly less by SLPs
in the US/CA compared to SLPs in AUS/NZ. The most
widely used CC/HL assessments in AUS/NZ and the UK
were the MWHLL [37] and the CLAMCLA [47]. The use of
the MWHLL has been documented as a preferred assessment
in Australia in adults with aphasia [35, 38], a finding which
was also evident in the current study in demonstrating
its popularity amongst clinicians for use with adult TBI
patients as well. This is an interesting finding considering
there is no known empirical research or normative data
supporting its use in clinical practice to date. The MWHLL
assessment is available online free (for example
www.Libguides.city.ac.uk) and may influence SLP choice
based on availability rather than on psychometric robustness.
However, further research is warranted to establish appropri-
ateness for individual assessments with this population in
order to guide the SLP in making the best tool selections to
assess cognitive communication abilities in adults after TBI.
It also may serve to further highlight previous research
indicating that SLPs do not place great emphasis on statistical
properties of an assessment when choosing an assessment
tool [19].
Although discourse/pragmatic assessment tools repre-
sented a smaller proportion of assessment tools reported to
be used by SLPs surveyed in this study, this category was
noted to be more prevalent in AUS/NZ settings. This may
reflect that the stated assessments of choice were more
commonly developed locally, with the potential for AUS/NZ
based SLPs to have had more exposure to these tools via
workshops or conferences; reported to be an effective method
of promoting assessment choice [19]. Similarly, use of the
FAVRES [29] in the assessment of functional performance
category was noted to be more popular in the US/CA from
where it also originated. These findings suggest that the
location where the assessment is developed may influence
SLPs local to that area in their choice of assessment tool.
Naming assessments were used significantly less in AUS/
NZ, as were cognitive assessments which may reflect role
delineation between Neuropsychologists and SLPs in those
countries. The BNT which was the most popular tool in the
naming group has also been reported as a tool used by
Neuropsychologists when examining their clinical assessment
practices [57].
Use of informal language/cognitive measures were not
considered as a preferred method of assessment by SLPs in
the UK and US/CA, with less than 3% and 5% using them,
respectively, whereas closer to 10% reported use of these
assessments in the AUS/NZ group. Of those used, tools
selected from this category focused mainly on observations of
non-specific functional activities or assessments developed by
the clinician. Observation is one form of informal assessment
that has been previously reported to be a preferred choice for
both TBI and aphasia patients [19, 21, 38]. However, further
research is required about the validity of this category of
assessment given there is no normative data and individuality
of communication styles and context-specific nature of
communication in different settings [41].
The survey conducted as part of the present investigation
highlighted that overall SLPs do not report assessing a
particular area of communication more frequently depending
on clinical setting; whether it was an inpatient or community
setting. The majority of assessments were used equally
across inpatient and community setting, similar to findings in
previous research examining clinical assessment practices in
both TBI and aphasia populations [19, 35]. However, at a
category level, discourse and pragmatic skill assessment tools
were noted to be significantly more likely to be used in a
community setting. As discourse and social skills are con-
sidered by clinicians to play a significant role in re-establishing
peer relationships and re-integrating back to work [58], it is
possible that SLPs specifically target social communication in
their assessment and rehabilitation practices in order to support
re-integration of their patients back into the community.
Methodological issues such as practice effects on repeated
measures needs to be highlighted given the lack of change in
assessment tools between inpatient and community settings.
The possible use of re-testing using the same assessment
within short time frames as the person with a TBI follows
their rehabilitation from inpatient to community and possibly
a number of different clinicians. Given previous research
highlighting that SLPs have focused less on statistical
properties [19], further investigation is warranted in deter-
mining how often assessments are re-administered in clinical
practice and whether this impacts not only on the validity and
reliability, but also regarding appropriateness for goal setting,
intervention planning and as an outcome measure.
Those areas of communication demonstrated to be more
specifically impacted or sensitive to TBI [53], such as
pragmatic skills, discourse word finding ability and literacy,
were more likely to be more frequently assessed by
experienced clinicians. However, the tools selected in the
assessment of these areas of communication were not signifi-
cantly different in regard to years of experience. Previous
research has highlighted that clinicians did not feel adequately
trained at an undergraduate level and that experience of TBI
is learnt through exposure, mentoring from experienced
staff and workshops [19]. Additionally, findings of the present
study suggest that less experienced staff in AUS/NZ are
working in regional and rural areas, often times employed as a
sole or generalist clinician, where they may not have access
to the appropriate assessment tools or support in deciding on
which appropriate tools to use. Such reports of inconsistent
use of assessments targeting areas of communication known
to be most commonly impacted by a TBI [3, 52, 59], regardless
of level of experience, further supports the importance of
further education and training. The development of prescrip-
tive guidelines worldwide may also prove useful, suggesting
what areas of communication should be assessed and the tools
that could be used as part of an assessment protocol to address
not only impairment but also tools that reflect functional
activities and participation in the community [40]. Training
programmes linking rural clinicians with metropolitan clin-
icians are also recommend and have been shown to be an
effective method in mentoring and supporting allied health
professionals in these settings [60].
8 M. Frith et al. Brain Inj, Early Online: 1–10
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y D
okuz
Eyl
ul U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.

A potential limitation of this study is the potential sample
bias, in that SLP survey participants were recruited based on
their own perception of identification using previous experi-
ence with populations/patients with TBI. SLPs were asked if
they had specialist experience working with adults with TBI.
The extent of specific TBI experience or the frequency they
may assess a client with TBI was not explicitly asked. It is,
therefore, possible that SLPs with minimal or extremely
limited experience in TBI may have participated in the survey,
although this was minimized by recruiting through special
interest groups in brain injury throughout each country. An
additional limitation is that there are also potential weaknesses
in using Likert scales due to their subjective nature of evalu-
ation and evidence that suggests that people from different
cultures and countries may answer a question on a Likert scale
more or less positively [61]. To manage this possible
weakness, the use of Likert scales was supplemented with
open-ended questions, which offered participants the oppor-
tunity to provide detail about their current clinical practice.
In addition, categorizing assessments into groups is not
always straight forward as an assessment can have multiple
sub-tests which may overlap into other categories or there
might be different perspectives of where an assessment might
be best categorized and this has been highlighted in previous
research which has attempted to map assessments to the ICF
model [40]. Nonetheless, this was addressed by obtaining
agreement from a panel of five experienced researchers in the
field of TBI on the assignment of tests to categories. Further
study is warranted to ascertain whether an assessment that is
used, is used in its entirety or parts of the assessment are used.
In conclusion, this study is the first to document
international assessment practices of SLPs working with
adults who have a cognitive communication disorder after a
TBI. Similarities between countries highlights that traditional
impairment-based aphasia tools continue to be favoured, with
less focus on specific functional assessment tools, yet
reported routinely assessing functional communication
skills. Guidelines regarding the role of SLPs’ assessment of
cognitive communication disorders were noted to have
influenced change in assessment practices in some countries,
such as the US, with cognitive assessment tools forming an
important part of a clinical assessment protocol. Countries
without guidelines such as Australia, New Zealand and the
UK focus on assessment protocols from the field of aphasia
and use aphasia and or cognitive communication/high level
language assessments. The use of discourse analysis in clinical
practice is still not used readily as part of an assessment
protocol. The study supports the need for clearer recommen-
dations and guidelines about assessment protocols for assess-
ment of cognitive communication disorders after a TBI.
Declaration of interest
The authors report no conflicts of interest. The authors alone
are responsible for the content and writing of the paper.
References
1. Morgan AT, Skeat J. Evaluating service delivery for speech andswallowing problems following paediatric brain injury: AnInternational survey. Journal of Evaluation in Clinical Practice2011;17:275–281.
2. Steel J, Ferguson A, Spencer E, Togher L. Speech pathologists’current practice with cognitive-communication assessment duringpost-traumatic amnesia: A survey. Brain Injury 2013;27:819–830.
3. Turkstra KM. Evidence-based practice for cognitive-communica-tion disorders after traumatic brain injury. Seminars in Speech &Language 2005;26:213–214.
4. Ylvisaker M, Coelho C, Kennedy M, Sohlberg MM, Turkstra L,Avery J, Yorkston K. Reflections on evidence-based practice andrational clinical decision making. Journal of Medical Speech-Language Pathology 2002;10:xxv–xxxiii.
5. Royal College of Speech & Language Therapists. RCSLT ClinicalGuidelines. Oxon, UK: Speechmark Publishing Ltd; 2005.
6. American Speech-Language Hearing Association. Evaluating andtreating communication and cognitive disorders: Approaches toreferral and collaboration for speech language pathology andclinical neuropsychology [Technical Reprt]. Rockville, MD, 2003.Available from www.asha.org/policy, accessed 30/3/2013.
7. American Speech-Language-Hearing Association. Roles ofspeech language pathologists in the identification, diagnosis, andtreatment of individuals with cognitive-communication disorders:Position statement [Position Statement]. Rockville, MD. 2005.Available online at: www.asha.org/policy2005, Accessed 24/8/2012.
8. College of Audiologists and Speech-Language Pathologists ofOntario. Preferred practice guidelines for cognitive-communicationdisorders. Ontario, Canada, 2002. Available online at: www.caslpo.com/Portals/0/ppg/ppg_ccd, accessed 1/4/2013.
9. Turkstra L, Ylvisaker M, Coelho C, Kennedy M, Sohlberg MM,Avery J, Yorkston K. Practice guidelines for standardized assess-ment for persons with traumatic brain injury. Journal of MedicalSpeech-Language Pathology 2005;13:ix–xxxviii.
10. Coelho C, Ylvisaker M, Turkstra LS. Nonstandardized assessmentapproaches for individuals with traumatic brain injuries. Seminarsin Speech & Language 2005;26:223–241.
11. Uniform Data System for Medical Rehabilitation. FunctionalIndependence Measure (FIM). Buffalo, NY: University ofBuffalo; 1996.
12. Frattali C, Thompson C, Holland A, Wohl C, Ferketic M. AmericanSpeech Language Hearing Association Functional Assessment ofCommunication Skills for Adults (ASHA FACS). Rockville, MD:American Speech Language Hearing Association; 1995.
13. Holland A, Frattali C, Fromm D. Communication Activities ofDaily Living. 2nd ed. Austin, TX: PRO-ED; 1999.
14. Randolph C. Repeatable Battery for the Assessment ofNeuropsychological Status. 1st ed. San Antonio, TX:Psychological Corporation; 2001.
15. Kertesz A. Western Aphasia Battery- Revised. HarcourtAssessment, San Antonio, TX: Inc; 2006.
16. Frank EM, Williams AR, Butler JG. Current socio-cognitivecommunication assessment protocols for children with traumaticbrain injury. Journal of Medical Speech-Language Pathology 1997;5:97–111.
17. McGrane S, Cascella P. TBI knowledge and pragmatic assessmentamong Connecticut school speech language pathologists. BrainInjury 2000;14:975–986.
18. Turkstra L, Coelho C, Ylvisaker M. The use of standardized testsfor individuals with cognitive-communication disorders. Seminarsin Speech and Language 2005;26:215–222.
19. Frank EM, Barrineau S. Current speech-language assessmentprotocols for adults with traumatic brain injury. Journal ofMedical Speech-Language Pathology 1996;4:81–101.
20. Verna A, Davidson B, Rose T. Speech-language pathology servicesfor people with aphasia: A survey of current practice in Australia.International Journal of Speech-Language Pathology 2009;11:191–205.
21. Simmons-Mackie N, Threats TT, Kagan A. Outcome assessment inaphasia: A survey. Journal of Communication Disorders 2005;38:1–27.
22. Wilson FC, Harpur J, McConnell N. Vegetative and minimallyconscious state(s) survey: Attitudes of clinical neuropsychologistsand speech and language therapists. Disability and Rehabilitation2007;29:1751–1756.
23. Shiel A, Wilson B, McLellan L. The Wessex Headn Injury Matrix(WHIM). Bury St Edmunds, UK: Thames Valley Test Company;2000.
DOI: 10.3109/02699052.2014.947619 Cognitive communication following TBI in adults 9
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y D
okuz
Eyl
ul U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.

24. Steel J, Ferguson A, Spencer E, Togher LSpeech pathologists’current practice with cognitive communication assessment duringpost-traumatic amnesia: A survey. Brain Injury 2013;27:819–830.
25. Duff MC, Proctor A, Haley K. Mild traumatic brain injury (MTBI):Assessment and treatment procedures used by speech-languagepathologists (SLPs). Brain Injury 2002;16:773–787.
26. Ross-Swain D. Ross Information Processing Assessment. 2nd ed.(RIPA-2). Austin, TX: PRO-ED; 1996.
27. Goodglass H, Kaplan E. Boston Diagnostic Aphasia Examination.3rd ed. (BDAE). Austin, TX: PRO-ED; 2000.
28. Kaplan E, Goodglass H, Weintraub S. The Boston Naming Test.2nd ed. (BNT-2). Austin, TX: Pro-Ed; 2001.
29. MacDonald S. Functional Assessment of Verbal Reasoning andExecutive Strategies. Ontario, Canada: CCD Publishing; 2003.
30. Wiig EH, Secord W. Test of Language Competence – ExpandedEdition (TLC -Expanded). San Antonio, TX: Pearson; 1989.
31. Bowers L, Huisingh R, LoGiudice C, Orman J. The Word Test 2.Austin, TX: Pro-Ed; 2005.
32. Wong MN, Murdoch B, Whelan B-M. Language disorders subse-quent to mild traumatic brain injury (MTBI): Evidence from fourcases. Aphasiology 2010;24:1155–1169.
33. Helm-Estabrooks N. Cognitive Linguistic Quick Test (CLQT). SanAntonio, TX: Pearson; 2001.
34. Blyth T, Scott A, Bond A, Paul E. A comparison of twoassessments of high level cognitive communication disorders inmild traumatic brain injury. Brain Injury 2012;26:234–240.
35. Katz RC, Hallowell B, Code C, Armstrong E, Roberts P, Pound C,Katz L. A multinational comparison of aphasia managementpractices. International Journal of Language & CommunicationDisorders 2000;35:303–314.
36. Kay J, Coltheart M, Lesser R. Pscholinguistic Assessmentsof Language Processing in Aphasia (PALPA). Oxford, UK:Psychology Press; 1992.
37. Christie J, Clark C, Mortensen L. Mount Wilga High LevelLanguage Test. Unpublished Test: Speech Pathology DepartmentMount Wilga Rehabilitation Centre; 1986.
38. Vogel AP, Maruff P, Morgan AT. Evaluation of communicationassessment practices during the acute stages post stroke. Journal ofEvaluation in Clinical Practice 2010;16:1183–1188.
39. Larkins B. The Application of the ICF in Cognitive-Communication Disorders following Traumatic Brain Injury.Seminars in Speech & Language 2007;28:334–342.
40. Hughes J, Orange JB. Mapping functional communication measure-ments for traumatic brain injury to the WHO-ICF. Canadian Journalof Speech-Language Pathology & Audiology 2007;31:134–143.
41. Togher L. Discourse sampling in the 21st century. Journal ofCommunication Disorders 2001;34:131–150.
42. Coelho CA. Management of discourse deficits following traumaticbrain injury: Progress, caveats, and needs. Seminars in Speech &Language 2007;28:122–135.
43. Ellmo W, Graser J, Calabrese D. Methods of assessment utilized byspeech-language pathologists with traumatically brain injuredadults. A national survey. Journal of New Jersey Speech andHearing Association 1997;6:17–23.
44. Hofmans J, Theuns P, van Acker F. Combining quality and quantity.A psychometric evaluation of the self-anchoring scale. Quality andQuantity 2009;43:703–716.
45. Blais JG, Grondin J. The influence of labels associated with anchorpoints of likert-type response scales in survey questionnaires.Journal of Applied Measurement 2011;12:370–386.
46. Howell D. Fundamental Statistics for the Behavioral Sciences.Belmont, CA: Duxbury Press; 1995.
47. Ellmo W, Graser J, Krchnavek B, Hauk K, Calabrese D. Measure ofCognitive Linguistic Abilities (MCLA). Norcross, GA: The SpeechBin; 1995.
48. Douglas J, Bracy C, Snow P. La Trobe CommunicationQuestionnaire. Bundoora, Victoria: Victoria School of HumanCommunication Sciences, La Trobe University; 2000.
49. McDonald S, Flanagan S, Rollins J. Awareness of Social InferenceTest, (TASIT). Sydney, Australia: Pearson; 2002.
50. Howard D, Swinburn K, Porter G. Comprehensive Aphasia Test.Routledge: Psychology Press; 2004.
51. Adamovich B, Henderson J. Scales of Cognitive Ability forTraumatic Brain Injury (SCATBI). Austin, TX: PRO-ED; 1992.
52. McDonald S, Flanagan S, Rollins J, Kinch J. TASIT: A new clinicaltool for assessing social perception after traumatic brain injury.Journal of Head Trauma Rehabilitation 2003;3:219–238.
53. King KA, Hough MS, Walker MM, Rastatter M, Holbert D. Mildtraumatic brain injury: Effects on naming in word retrieval anddiscourse. Brain Injury 2006;20:725–732.
54. Douglas JM, Bracy CA, Snow PC. Measuring perceived commu-nicative ability after traumatic brain injury: Reliability and validityof the La Trobe Communication Questionnaire. Journal of HeadTrauma Rehabilitation 2007;22:31–38.
55. Parrish C, Roth C, Roberts B, Davie G. Assessment of cognitive-communicative disorders of mild traumatic brain injury sustained incombat. Perspectives on Neurophysiology and Neurogenic Speechand Language Disorders 2009;19:47–57.
56. Wertheimer JC, Roebuck-Spencer TM, Constantinidou F,Turkstra L, Pavol M, Paul D. Collaboration between neuropsych-ologists and speech-language pathologists in rehabilitation settings.Journal of Head Trauma Rehabilitation 2008;23:273–285.
57. Rabin LA, Barr WB, Burton LA. Assessment practices of clinicalneuropsychologists in the United States and Canada: A survey ofINS, NAN, and APA Division 40 members. Archives of ClinicalNeuropsychology 2005;20:33–65.
58. Isaki E, Turkstra L. Communication abilities and work re-entryfollowing traumatic brain injury. Brain Injury 2000;14:441–453.
59. Bernicot J, Dardier V. Communication deficits: Assessment ofsubjects with frontal lobe damage in an interview setting.International Journal of Language & Communication Disorders2001;36:245–263.
60. Parkin AE, McMahon S, Upfield N, Copley J, Hollands K. Workexperience program at a metropolitan paediatric hospital: Assistingrurual and metropolitan allied health professionals exchangeclinical skills. Australian Journal of Rural Health 2001;9:297–303.
61. Lee JW, Jones PS, Mineyama Y, Zhang XE. Cultural differences inresponses to a Likert scale. Research in Nursing and Health 2002;25:295–306.
10 M. Frith et al. Brain Inj, Early Online: 1–10
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y D
okuz
Eyl
ul U
niv.
on
11/0
4/14
For
pers
onal
use
onl
y.