Embed Size (px)
Citation preview
1
Traumatic Brain Injury
Number 1 killer of children and
young adults
Review of SCI Lecture
Statistics • MVAs cause 50% of all head injuries
• Falls = 21%
• Violence = 12%
• Sports = 10%
• Male > Female
• Ave. age at time of injury between 15 & 24
2
Prevention
• ...The only true “cure” for TBI
• Preventive measures
– Wearing seat belts & bike helmets
– responsible alcohol consumption (no drinking
and driving)
– Use of proper protective equipment in athletics
Classifications
• Head injuries classified according to the
Glasgow Coma Scale:
– mild
– moderate
– severe
can also be classified according to
• open vs. closed
• high-velocity vs. low velocity impact
• diffuse vs. focal
3 Factors Affecting Outcome
• 1. Premorbid Status
• 2. Primary Injury: the amount of immediate
damage to the brain from the impact of the
brain injury
• 3. Secondary Injury: the cumulative effect
of secondary brain damage produced by
systemic and intracranial mechanisms that
occur after the initial injury
3
3 Factors Affecting Outcome
• 1. Premorbid Status
– normal vs. altered (enchephalitis, CVA)
• 2. Primary Injury: depends on the nature,
direction, and magnitude of forces applied
to the brain, skull, and body
Factors Affecting Outcome • 3. Secondary injury: following TBI,
numerous conditions decrease the energy
supply to the brain, causing secondary
injury to the brain
– Hypoxic-ischemic injury (HII)
– Intracranial hematomas
– Intracranial infection, cerebral artery
vasospasm, tumors, obstructive hydrocephalus,
post-traumatic epilepsy
Types of Primary Injury – local brain damage: injury is localized to the
area of the brain underlying the site of impact
• produces predictable neurologic signs
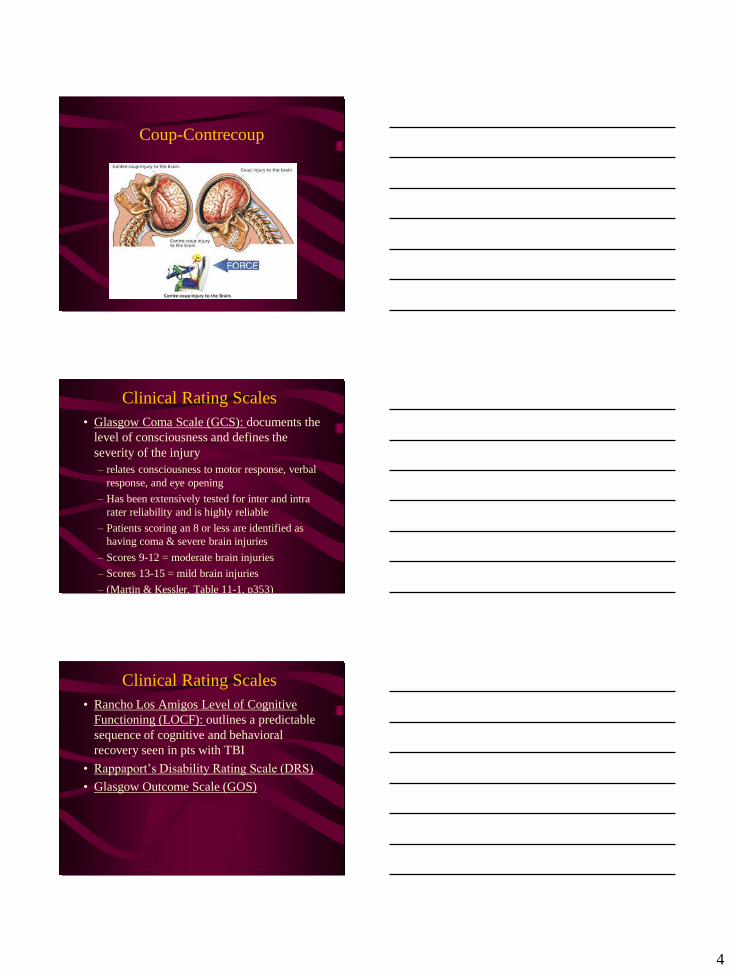
– Coup-contrecoup injuries: a severe blow to the
head damages under the site of impact and
directly opposite the site due to the brain
bouncing within the skull
– polar brain damage: occurs when the head is
accelerated and decelerated (MVA)
• brain impacts on the skull
– Diffuse axonal injury (DAI)
4
Coup-Contrecoup
Clinical Rating Scales
• Glasgow Coma Scale (GCS): documents the
level of consciousness and defines the
severity of the injury
– relates consciousness to motor response, verbal
response, and eye opening
– Has been extensively tested for inter and intra
rater reliability and is highly reliable
– Patients scoring an 8 or less are identified as
having coma & severe brain injuries
– Scores 9-12 = moderate brain injuries
– Scores 13-15 = mild brain injuries
– (Martin & Kessler, Table 11-1, p353)
Clinical Rating Scales
• Rancho Los Amigos Level of Cognitive
Functioning (LOCF): outlines a predictable
sequence of cognitive and behavioral
recovery seen in pts with TBI
• Rappaport’s Disability Rating Scale (DRS)
• Glasgow Outcome Scale (GOS)
5
Diagnostic Procedures • EEG
• CT
• MRI
• Cerebral Blood Flow Mapping
– PET
Interdisciplinary team – Patient & family
– PT, OT, SLP
– MD, rehab nurse, case manager/team
coordinator
– MSW
– neuropsychologist
Acute Management • PT is indicated in early management of the
pt with moderate or severe head injury
• Initial rx revolves around prevention of
complications:
– respiratory distress
– contracture development
– skin breakdown
– PROM; splinting; passive standing in tilt table
6
Acute Management
• Functional mobility training: begins when
the pt’s medical status is stable
– increase upright standing tolerance
– increase pt’s active movement capabilities
– sensory stimulation (reviewed later)
– **always check in with the RN because a pt’s
status can change dramatically in a short period
of time and alerts the RN that PT is beginning
which can alter the pt’s status (increased vital
signs)**
Direct Impairments
• 1. Cognitive
• 2. Neuromuscular
• 3. Visual / perceptual
• 4. Swallowing
• 5. Behavioral
• 6. Communication
Direct Impairments
• 1. Cognitive
– Altered Level of Consciousness
– Coma: defined as “not obeying commands, not
uttering words, and not opening the eyes.” &
sometimes the GCS score is used to define
coma, a score of ______ defines a coma
– Vegetative: decreased level of awareness with
intact eye opening and sleep-awake cycles, but
no ability to follow commands or speak
7
Direct Impairments
• 2. Neuromuscular
– Often present with abnormal tone
• From spasticity that affects entire body & function
to low tone of indiv muscle groups that does not
impact function
– Proprioception & kinesthesia are common
sensory deficits
– May see balance deficits, nystagmus,
hemiparesis, ataxia, vestibular loss, visual
deficits, etc
Direct Impairments
• 3. Visual/Perceptual Impairments
– Hemianopsia
– Blindness
– Spatial neglect
– Apraxia
– Somatagnosia
– Right-left discrimination
Direct Impairments
• 4. Swallowing
– Dysphagia is very common
8
Direct Impairments
• 5. Behavioral Deficits
– Are the most enduring & socially disabling of
any of the impairments commonly seen after
TBI
– Patient will have a behavioral program created
by the neuropsychologist
– Sexual disinhibition, emotional disinhibition,
apathy, aggressive disinhibition, low frustration
tolerance & depression often lead to a life of
seclusion & loneliness
Direct Impairments
• 6. Communication
– Expressive or receptive aphasia
– Reading comprehension
– Written expression
– Language skills deficits
– dysarthria
Indirect Impairments
• Contractures
• mobility
• skin breakdown
• heterotropic
ossification
• decreased endurance
• Infection
• pneumonia
• impaired speech
secondary to trach
• DVT
9
Management Based on Cognitive
Level
• Because the cognitive level of the pt
determines the extent to which s/he can
be actively involved in the treatment, the
organization of PT treatment information
is built around the pt’s cognitive level
• Treatment considerations for pts in
Rancho Los Amigos levels (LOCF)...
LOCF • 1. No response
• 2. Generalized response
• 3. Localized response
• 4. Confused - agitated
• 5. Confused - inappropriate
• 6. Confused - appropriate
• 7. Automatic - appropriate
• 8. Purposeful - appropriate
Low Level Management
• LOCF I - III
• Evaluation: PROM, spontaneous activity,
response to stimulation, muscle tone and
reflexes, and the presence of gross motor
skills (postural reactions)
10
Low Level Management
• Goals: prevent any complications
(contractures, decubiti) and increase the pt’s
level of interaction with the environment
(by encouraging active movement and
response to stimulation)
Low Level Management
(Treatment) • PROM: can be reasonably aggressive, but
must use caution
• Sensory stimulation: used for arousal and
to elicit movement. Must watch for the
response to the stimulation (can manifest as
changes in HR, RR, BP or eye movement,
facial grimacing, head turning,
vocalizations). Must note the following:
Low Level Management
(Treatment)
– latency: time delay between stimulus and
response
– consistency: how many times (within a set
number of reps) does a pt respond to the same
stimulus
– intensity: the response should be proportional
to the stimulation
– duration: brief form of stimuli should result in
brief forms of response
11
Low Level Management
(Treatment)
– visual stimulation: utilize pictures of family
and friends; systematically stimulate all areas of
the visual field (account for visual field
deficits); document visual attentiveness and
tracking
– olfactory stimulation: provided by placing
scents under a pts nose for 10 - 15 seconds
during quiet breathing (best results from the
pt’s own favorite smells)
– tactile stimulation: provided during functional
activities (turning, bathing, dressing)
Low Level Management
(Treatment)
– vestibular stimulation: provided by C/S
ROM, rolling on a mat, rocking, or pushing
the pt in a wc.
– auditory stimulus: use normal
conversational tone, discuss topics that have
meaning to the pt. Avoid background noise
(it competes with meaningful stimuli)
Low Level Management
(Treatment)
• Positioning:
12
Mid-Level Management
• LOCF IV: present very specific challenges
because these pts are in a confused and
agitated state
– Evaluation: in addition to those areas evaluated
in LOCF I - III, must assess functional tasks
(ambulation, basic transfers)
– Goals: increase or maintain ROM, prevent
deconditioning, improve response to simple
commands, prevent outbursts through a highly
structured environment
Mid-Level Management
– Special considerations:
• remember the pt is confused: the pt should be seen
by the same person at the same time, in the same
place every day; establishes a routine
• expect no carryover: teaching new skills is
UNREALISTIC
• model calm behavior
• be prepared with numerous activities
• offer options: “would you rather play ball or go for a
walk?”
• expect egocentricity: the pt will tend to only think
about him or herself.
Mid-Level Management – Treatment: ROM, gross motor activity
• **attempt to improve endurance rather than progress
to more challenging tasks (because that requires new
learning)**
• may need to employ creative techniques: “come
walk with me to get the cards” instead of “let’s take
a walk”
• attention deficits are addressed through activity
participation (pt attention can gradually improve
during activities)
13
Mid-Level Management
• LOCF V - VI: these pts are confused but no
longer agitated; can follow simple
commands but if demands increase and
structure decreases, performance
diminishes; carryover is present but best for
relearned activities; new learning very
limited
Mid-Level Management – Evaluation: usually possible to perform a
formal eval but should be concise with simple
instructions
– Goals: increase pt participation in program;
increase/maintain ROM; increase conditioning;
treatment of any motor deficit (i.e. hemiparesis,
peripheral nerve injury, etc)
Mid-Level Management – Treatment: should…
• maintain structure: pt performance still depends on it
• emphasize safety
• keep instructions to a minimum: too much can
confuse and irritate the pt
• use physical props to improve compliance: timer so pt
has concrete sense of time; videotape of performance
so pt can view that performance realistically
14
High-Level Management
• LOCF VII - VIII
• Usually during this stage that the pt is
D/C’d from inpatient facilities
• Prior to D/C, it is necessary to wean the pt
from the structure that was critical in early
rehab
– the pt has some insight now into his/her
strengths and weaknesses and should be
involved in decision making as much as
possible
High-Level Management
• Goals: assist the pt in integrating the
cognitive, physical, and emotional skills
that are necessary to function in the real
world.
– judgement, problem solving, planning are
emphasized
High-Level Management
• Treatment: focuses on community skills,
social skills, ADL
• Judgement, problem solving, and planning
are emphasized
15
High-Level Management
– these pts will require vocational and driving
services to reach their optimal functional level
– PT services at this point usually are for specific
motor disorders and do not differ significantly
from the types of therapy provided to pts
without cognitive dysfunction.
– ** overall goal is for the pt to function
optimally in society **
Issues That Cross All Levels
• ROM: decreases occur due to several reasons
– prolonged bed rest; decreased consciousness,
spasticity, lack of voluntary movement
– Treatments for spasticity include oral meds, nerve
and motor point blocks, serial casting, positioning
systems
Issues That Cross All Levels
• Mobility: must take the cognitive issues into
consideration
early rolling (low-level); supervised wc propulsion
(mid-level); assisted ambulation; power wc
16
Issues That Cross All Levels
• Documentation: must precisely record
the physical and cognitive functioning.
– For example, a pt may have a high physical
functioning level but require close
supervision due to poor safety awareness.
This should not be documented as
independent physical capacity because of the
cognitive impairment
Issues That Cross All Levels
• Adaptive equipment
– wheelchair: manual or power; variety of
controls
– advanced computer technology
• simple letter board for communication
• or complex environmental control unit
Issues That Cross All Levels
• Outcome prediction: our ability to predict
outcomes is very limited due to the extreme
complexities of the issues related to head
injury
– being able to live independently, earn an
income, manage daily activities and affairs are
the outcomes that survivors strive for
• many can reach this level
• many cannot
17
Integrating Physical and Cognitive
Components of a Task into
Treatment Interventions • Cognitive and Behavioral Impairments:
– Disorientation: calendar, memory book
– Attention deficits: stopwatch or timer
– Memory deficits: memory book, computerized
schedule books, watches and pillboxes
– Problem-solving deficits: create situations that
alert to safety; route finding tasks, obstacle
courses
Integrating Physical and Cognitive
Components of a Task into
Treatment Interventions
– Behavioral deficits: consistent schedule,
structured environment, keeping patient
occupied
– Aggressive behaviors
– Motor deficits: high level balance activities,
use of movable surfaces
Treatment Guidelines for Behavioral
Impairments
• Agitated patient
– remove all jewelry
– remove anything from around your neck -
ID tag, necklaces, ties
– see the patient regardless - if they are too
agitated to treat, then walk the halls with
them or provide some quiet supervision
18
Treatment Guidelines – Throw your goals out the window!! #1 goal is
SAFETY - for you and the patient
– call for help if you need it
– talk normally - listen to yourself. Talking in a
calm and soothing voice does not mean a sing-
song voice. Be natural - joke around if it helps,
be matter of fact if it helps, but don’t baby these
folks
Treatment Guidelines
• Don’t push it - if the patient refuses and it
seems like pushing them will agitate them,
stop and take a break
Treatment Guidelines • Verbal aggression
– remain calm and concrete
– be “with” the patient
– be aware
– empathize
– key words and verbal praise
– give space
19
Treatment Guidelines – Watch body language and voice tone; calm
non-threatening nonconfrontive
– remember the client will process information
more slowly, less accurately
– don’t attempt to teach or counsel until de-
escalated
– DO NOT argue, threaten, get angry, get
aggressive, bend or discard rules
Treatment Guidelines – DO NOT get into a power struggle or make
false promises
– DO redirect without going off the subject
– use humor where appropriate
– “listen”
– lessen stimulus: get patient to leave area or get
others to leave
Treatment Guidelines – Offer help: “what can I do to help?”; “let me
help you with…”
– provide orientation information
_ reinforce limits
– FOLLOW THE PLAN
20
Wrap up Today’s Lecture
Questions???
• O’Sullivan, S.B. & Schmitz, T.J., (2000),
Physical Rehabilitation, 4th Ed., F.A. Davis
Company: Philadelphia.