Embed Size (px)
Citation preview

Unit 3 • Chapter 12. Assessment of the hormonal milieu 199
Un
it 3
Ch
ap
ter
12
unit 3.assessing exposure to the environment
chapter 12.
Assessment of the hormonal milieu
Susan E. Hankinson and Shelley S. Tworoger
Summary
The hormonal milieu has been hypothesized to play a role in a range of human diseases, and therefore has been a topic of much epidemiologic investigation. Hormones of particular interest include: sex steroids; growth hormones; insulin-like growth factors; stress hormones, such as cortisol; and hormones produced by the adipose tissue, termed adipokines. Depending on the hormone, levels may be measured in plasma or serum, urine, saliva, tissue, or by assessing genetic variation in the hormone or hormone metabolizing genes. Sample collection, processing, and storage requirements vary according to the type of sample collected (e.g. blood or urine) and the hormone of interest. Laboratory analysis of hormones is frequently complex, and the technology used to conduct the assays is constantly evolving.
For example, direct or indirect radioimmunoassay, bioassay or mass spectrometry can be used to measure sex steroids, each having advantages and disadvantages. Careful attention to laboratory issues, including close collaboration with laboratory colleagues and ongoing quality control assessments, is critical. Whether a single hormone measurement, as is frequently collected in epidemiologic studies, is sufficient to characterize the hormonal environment of interest (e.g. long-term adult hormone exposure) is also an important issue. While the assessment of hormones in epidemiologic studies is complex, these efforts have, and will continue to, add importantly to our knowledge of the role of hormones in human health.
Introduction
The study of hormones and their involvement in human health has been considered for many years, and their measurement has increasingly become an important part of many epidemiologic studies. Examining how various endogenous and exogenous hormones are related to disease increases our understanding of disease etiology, which may ultimately lead to improved prevention recommendations for both high-risk groups and the general population. Issues surrounding the appropriate use of hormone measures in epidemiologic studies are complex and require careful planning by study investigators. Many choices must be made, including the type of biospecimen to collect from participants, the timing and conduct of sample collection, the choice of hormones and assay modalities,

200
and ultimately how to interpret the results. While several of these issues are dealt with in previous chapters (sample collection and processing in Chapter 3 and interpretation of assay results in Chapter 8), here the focus is on examples and concerns in measuring hormones. Because of the broad range of hormones found in humans, this chapter cannot cover every aspect of hormone measurement. However, general issues are addressed that should be considered when designing epidemiologic studies of hormones, such as the importance of hormones in medical research, their measurement in human samples, and issues regarding assay development and interpretation.
Context and public health significance
Hormones are chemicals produced by living cells that act as chemical messengers or signal molecules (1). The hormonal environment is a critical regulator of many physiologic processes, including growth, energy metabolism, fertility and the stress response. A wide range of well-documented diseases are linked to changes, either increases or decreases, in the hormonal milieu (Table 12.1). The role of hypoinsulinemia and insulin resistance in diabetes, excess insulin-like growth factor (IGF I in acromegaly and deficiency in dwarfism, excessive production of thyroid hormone in Graves disease, and overproduction of cortisol in Cushing syndrome are all examples. In addition to these well-established causal relationships, the hormonal milieu has been hypothesized to play a role in a range of other diseases, which have been the focus of many epidemiologic studies. Several examples, described further below, include the association of sex steroid
hormones and breast cancer, the IGF system and cognitive function, and the role of adipokines such as adiponectin in both diabetes and heart disease.
This chapter focuses on the measurement of endogenous hormones (i.e. hormones produced by the body). The role of exogenous hormones (i.e. originating outside the body), particularly the use of oral contraceptives and postmenopausal hormones by millions of women worldwide, also has been the subject of substantial scientific study. The evaluation of exogenous hormones is not addressed here, largely because characterizing exposure to these agents is routinely accomplished via administration of questionnaires or tallying of pharmacy prescription records. However, any epidemiologic study of endogenous hormones must take into account sources of exogenous exposure that may influence endogenous hormone levels.
Examples/case studies
Sex steroids and breast cancer risk in postmenopausal women
Substantial data support a role of hormones, particularly sex steroids, in the etiology of breast cancer. There are consistent associations with reproductive factors, and increased risks associated with postmenopausal obesity and use of postmenopausal hormones (2). Further, drugs that either block estrogen binding to the estrogen receptor (selective estrogen receptor modulators, such as tamoxifen) or prevent the production of estradiol (aromatase inhibitors) are effective both in preventing breast cancer and improving survival of women with the disease (3–5). Considerable data assessing circulating sex steroids in postmenopausal women and breast cancer risk have accrued from prospective epidemiologic studies, where circulating levels of endogenous hormones are measured in study subjects before
Table 12.1. Examples of diseases potentially caused (at least in part) by hormones that have been the subject of epidemiologic study
Hormone Conditions known or hypothesized to be related
Sex steroids (e.g. estradiol and testosterone)
Infertility, osteoporosis, cancer (e.g. breast, endometrial and prostate cancers)
Vitamin D metabolites Hypertension, osteoporosis, cancer (e.g. colon and breast cancer)
Insulin Diabetes, heart disease, cancer (e.g. colon and endometrial cancers), cognitive function
Insulin-like growth factor/Growth hormone axis
Cancer (e.g. colon, prostate and breast cancers), heart disease, cognitive function, osteoporosis
Prolactin Immunologic diseases (e.g. rheumatoid arthritis and systemic lupus erythematosus), breast cancer
Adiponectin and other adipokines Diabetes, heart disease, cancer (e.g. colon and breast cancers)
Stress hormones (e.g. cortisol) Heart disease, cancer (e.g. breast cancer)
Melatonin Breast cancer, sleep disorders

Unit 3 • Chapter 12. Assessment of the hormonal milieu 201
Un
it 3
Ch
ap
ter
12
disease diagnosis (6). Overall, a strong positive association exists between breast cancer risk and circulating levels of both estrogens and androgens. Women in the top versus bottom 20% of estrogen levels have a two- to three-fold higher risk of breast cancer (7). The associations are similar for several forms of estrogen (e.g. estradiol, estrone, estrone sulfate). Although additional confirmation is required, the association appears strongest for estrogen receptor-positive breast tumours and is robust across groups of women at varying risk of breast cancer (e.g. defined by family history). Also, a single blood estrogen measure predicts subsequent breast cancer risk for at least 8–10 years. Generally, the more limited data available on urinary estrogens suggests similar predictive ability. For testosterone, a commonly measured androgen, the data are very consistent, with a significant positive association between circulating levels and postmenopausal breast cancer; the magnitude of the association is similar to that observed for estrogens (7). Most studies also noted a similar, although somewhat modest, positive association with other androgens, such as androstenedione, dehydroepiandrosterone (DHEA) and DHEA sulfate.
The insulin-like growth factor (IGF) axis and cognitive function
Insulin-like growth factor I (IGF-I) is a protein hormone that mediates many actions of growth hormone and plays a key regulatory role in cell growth and proliferation (1). Tissue bioavailability of IGF is regulated in large part by its binding to six known IGF binding proteins. Insulin-like growth factor binding protein 3 (IGFBP-3) is the most abundant of
these, and it substantially prolongs the circulating half-life of IGF-I. Most circulating IGF is produced by the liver, although it can be produced locally in other body tissues. IGF is known to play a role in brain development and function (8); it is produced in the brain and can pass through the blood-brain barrier. In animal studies, IGF improves memory and learning (8), and raising IGF levels was found to decrease formation of amyloid β (9), a major constituent of the neural plaques that are a hallmark of Alzheimer's disease. In several recent cross-sectional and prospective studies, the association between circulating levels of IGF-I, IGFBP-3, or free (unbound) IGF-I have been assessed in relation to cognitive function. Although results have not been entirely consistent, it appears that older adults with higher levels of IGF, the IGF-1:IGFBP-3 ratio, or free IGF-1 tended to have better cognitive function as assessed by several cognitive tests (10–13).
Adiponectin and risk of diabetes and heart disease
In recent years, adipose tissue has been recognized as an active endocrine organ that secretes many biologically active substances, termed adipokines. Although adipokine research is relatively new, accruing laboratory and human data on adiponectin, one of the most abundant adipokines, support a role in diabetes and possibly heart disease (14–16). Adiponectin functions as an insulin-sensitizer, and also has important anti-inflammatory and anti-atherogenic actions. For example, adiponectin increases insulin sensitivity in animal models of insulin resistance, and reverses diet-induced insulin resistance in adiponectin knockout mice. The protein is inversely associated with
body mass index (BMI) and insulin, and positively associated with serum lipids. Several cross-sectional, case–control, and prospective studies have reported either a strong significant inverse association for diabetes, or a modest inverse or no association for heart disease (17–21).
Predictors of hormone levels
In addition to the role of hormones in human health and disease, many studies have evaluated how the external environment influences the endogenous production of hormones in an effort to determine potential modes of action in causing (or preventing) disease. Examples include assessments of body size, physical activity and diet in relation to circulating hormone levels. The influence of alcohol intake on the hormonal milieu provides a good example. Both small randomized trials (22,23) and cross-sectional studies (24,25) have confirmed that alcohol intake increases estrogen levels in women, providing one potential mechanism for the positive association between alcohol intake and breast cancer risk. Further, alcohol intake has been found to increase insulin sensitivity (26) and HDL levels (27) and decrease fibrinogen levels (27), providing several mechanisms for the well-confirmed inverse association between alcohol intake and heart disease risk.
Strengths, limitations and lessons learned
Biologic samples for hormone evaluation
Many types of biologic specimens have been collected in epidemiologic studies where hormones are of interest (Table 12.2). In this section is a brief discussion of common sample types, and their advantages

202
Tabl
e 12
.2. C
olle
ctio
n an
d pr
oces
sing
requ
irem
ents
and
adv
anta
ges
and
disa
dvan
tage
s of
var
ious
bio
logi
cal s
peci
men
type
s co
llect
ed in
epi
dem
iolo
gic
stud
ies
Sam
ple
Type
Col
lect
ion,
pro
cess
ing
and
stor
age
requ
irem
ents
Adv
anta
ges
Dis
adva
ntag
es
Blo
od, v
enip
unct
ure
+Tra
ined
phl
ebot
omis
t+N
eedl
es, t
ubes
, bio
haza
rd w
aste
, tou
rniq
uet,
glov
es,
stor
age
vial
s+P
rimar
ily c
linic
-bas
ed+S
pin
and
aliq
uot p
lasm
a or
ser
um+D
elay
ed p
roce
ssin
g fo
r 48
hour
s ok
ay fo
r som
e ho
rmon
es+M
echa
nica
l or l
iqui
d ni
troge
n fre
ezer
s
+Can
mea
sure
bro
ad ra
nge
of h
orm
ones
+Col
lect
larg
e vo
lum
es fo
r fut
ure
assa
ys+F
or p
lasm
a tu
bes,
can
col
lect
whi
te b
lood
cel
ls fo
r D
NA
and
red
bloo
d ce
lls+C
an c
olle
ct m
ultip
le ty
pes
of s
ampl
es (e
.g. s
erum
, pl
asm
a) s
imul
tane
ousl
y
+Les
s fe
asib
le fo
r cos
t and
logi
stic
reas
ons
for l
arge
st
udie
s, e
spec
ially
ove
r a la
rge
geog
raph
ic a
rea
+Inv
asiv
e te
chni
que
may
low
er p
artic
ipat
ion
rate
s+R
equi
res
labo
rato
ry a
nd s
tora
ge s
pace
+Bio
haza
rd p
oten
tial
Blo
od, f
inge
r stic
k (fi
lter
pape
r)+F
inge
r lan
ce, f
ilter
pap
er, i
nstru
ctio
ns+C
linic
or h
ome-
base
d+N
o pr
oces
sing
+OK
at r
oom
tem
pera
ture
for ~
1 w
eek
for s
ome
horm
ones
+Sta
ndar
d 4°
C re
frige
rato
r or −
20°C
free
zer
+Can
mea
sure
som
e ho
rmon
es+F
easi
ble
to c
olle
ct o
n a
larg
e-sc
ale
+Allo
ws
seria
l sam
plin
g+R
elat
ivel
y no
n-in
vasi
ve+M
inim
al s
tora
ge s
pace
nee
ded
+Cor
rela
ted
with
pla
sma
leve
ls fo
r wom
en; l
ess
clea
r fo
r men
+Not
a b
ioha
zard
afte
r sam
ple
drie
s
+Low
sam
ple
volu
me
limits
num
ber o
f ass
ays
+Ind
ivid
ual h
aem
atoc
rit le
vels
can
alte
r mea
sure
d co
ncen
tratio
ns+R
equi
res
low
hum
idity
dur
ing
trans
port
and
stor
age
+Cer
tain
filte
r pap
ers
may
inhi
bit s
ome
assa
ys
Urin
e, c
up+C
olle
ctio
n cu
p, a
ntis
eptic
wip
e, in
stru
ctio
ns, s
tora
ge
vial
s+F
or in
fant
s pu
t a p
ad in
the
diap
er+C
linic
or h
ome-
base
d+M
ay re
quire
add
ition
of a
cid
+Del
ayed
pro
cess
ing/
free
zing
for 4
8 ho
urs
okay
for
som
e ho
rmon
es+M
echa
nica
l or l
iqui
d ni
troge
n fre
ezer
s
+Can
mea
sure
bro
ad ra
nge
of h
orm
one
met
abol
ites
+Fea
sibl
e to
col
lect
on
a m
odes
t sca
le+N
on-in
vasi
ve a
nd p
ainl
ess
+Allo
ws
seria
l sam
plin
g+G
ener
ally
cor
rela
ted
with
pla
sma
leve
ls+C
olle
ct la
rge
volu
mes
for f
utur
e as
says
+Ass
ays
ofte
n re
quire
larg
er v
olum
e th
an fo
r blo
od+M
ust m
easu
re c
reat
inin
e to
det
erm
ine
urin
e co
ncen
tratio
n+R
equi
res
labo
rato
ry a
nd s
tora
ge s
pace
+Has
bio
haza
rd p
oten
tial
+Can
col
lect
24-
hour
, ove
rnig
ht, f
irst-m
orni
ng, o
r spo
t ur
ine
Urin
e, fi
lter p
aper
+Col
lect
ion
cup,
ant
isep
tic w
ipe,
filte
r pap
er,
inst
ruct
ions
+Clin
ic o
r hom
e-ba
sed
+Oka
y at
room
tem
pera
ture
for ~
1 w
eek
for s
ome
horm
ones
+Sta
ndar
d −2
0°C
free
zer
+Can
mea
sure
som
e ho
rmon
e m
etab
olite
s+F
easi
ble
to c
olle
ct o
n a
larg
e sc
ale
+Non
-inva
sive
and
pai
nles
s+M
inim
al s
tora
ge s
pace
nee
ded
+Allo
ws
seria
l sam
plin
g+N
ot a
bio
haza
rd a
fter s
ampl
e dr
ies
+Has
bee
n us
ed o
nly
in a
lim
ited
num
ber o
f stu
dies
+ Lo
w s
ampl
e vo
lum
e lim
its n
umbe
r of a
ssay
s+C
erta
in fi
lter p
aper
s m
ay in
hibi
t som
e as
says
Sal
iva,
spo
t col
lect
ion
+Sev
eral
col
lect
ion
type
s: U
nstim
ulat
ed, s
aliv
ette
, co
tton
rolls
, gum
-stim
ulat
ed+N
eed
inst
ruct
ions
, sto
rage
via
ls+C
linic
or h
ome-
base
d+O
kay
at ro
om te
mpe
ratu
re fo
r ~1
wee
k fe
asib
le fo
r so
me
horm
ones
+Sta
ndar
d −2
0°C
free
zer
+Can
mea
sure
som
e ho
rmon
es+F
easi
ble
to c
olle
ct o
n a
larg
e sc
ale
+Non
-inva
sive
and
pai
nles
s+A
llow
s se
rial s
ampl
ing
+May
refle
ct ti
ssue
exp
osur
e, a
s ho
rmon
e m
ust
diffu
se a
cros
s sa
livar
y gl
and
cells
+Cor
rela
ted
with
pla
sma
leve
ls fo
r wom
en; l
ess
clea
r fo
r men
+Can
onl
y de
tect
free
(not
bou
nd) h
orm
ones
, whi
ch
ofte
n ha
ve a
low
con
cent
ratio
n+C
an b
e co
ntam
inat
ed w
ith b
lood
, whi
ch h
as h
igh
conc
entra
tions
of t
otal
hor
mon
e+M
ay n
ot re
flect
som
e ci
rcul
atin
g ho
rmon
es in
men
+Use
of s
timul
atio
n or
sal
ivet
tes
incr
ease
s so
me
horm
one
valu
es
Sal
iva,
ora
l diff
usio
n si
nk+D
iffus
ion
sink
(hor
mon
es d
iffus
e ac
ross
it),
inst
ruct
ions
, sto
rage
via
ls+C
olle
ct c
ontin
uous
ly fo
r lon
g pe
riods
+Hom
e-ba
sed
+Oka
y at
room
tem
pera
ture
for ~
1 w
eek
feas
ible
for
som
e ho
rmon
es+S
tand
ard
−20°
C fr
eeze
r
+Mea
sure
s in
tegr
ated
leve
ls o
ver t
ime
+May
refle
ct ti
ssue
exp
osur
e of
hor
mon
es u
nder
na
tura
l con
ditio
ns+S
epar
ates
bou
nd a
nd u
nbou
nd h
orm
ones
to re
duce
bl
ood
cont
amin
atio
n+P
artic
ipan
ts fi
nd it
acc
epta
ble
+Dev
ice
cost
can
be
high
+Onl
y av
aila
ble
for a
lim
ited
num
ber o
f hor
mon
es+N
ot a
s fe
asib
le in
a la
rge,
pop
ulat
ion-
base
d st
udy

Unit 3 • Chapter 12. Assessment of the hormonal milieu 203
Un
it 3
Ch
ap
ter
12
and disadvantages, with respect to measuring the hormonal milieu.
Blood
Blood specimens, collected by venipuncture, are the most common and flexible sample type collected in epidemiologic studies. Levels of many hormones can be determined in blood, primarily because assay development traditionally has focused on this sample type. Various kinds of blood samples can be collected, including serum and plasma (e.g. EDTA, sodium heparin, citrate); each has advantages and disadvantages depending on the biomarker(s) of interest (28,29). For example, sex hormone levels generally are similar when comparing serum with EDTA or heparin plasma (30–33). However, most studies suggest slightly higher levels of sex hormones in plasma versus serum; despite this, both are acceptable (30,31,33).
The primary advantages of blood collected using venipuncture include the capability to measure many hormones, as well as the ability to collect multiple blood specimens simultaneously (e.g. plasma and serum) (34). Additionally, if collecting plasma, both red and white blood cells can be saved; the latter can be used to isolate DNA. Also, relatively large sample volumes can be collected at one time, allowing for many assays to be conducted per participant.
Despite these advantages, venipuncture is expensive, as it requires a trained phlebotomist and extensive equipment (e.g. needles, appropriate collection tubes, gloves, etc.) (34). Thus, it generally is not feasible to collect specimens using this method in very large studies, or studies where the population is geographically dispersed. One exception to this rule is studies of
medical professionals who have training in phlebotomy, or are well connected to the medical care system, such as when nearly 33 000 blood samples from nurses who live across the United States were obtained in the Nurses’ Health Study (NHS) cohort (24). After pilot testing for feasibility, women were mailed a blood collection kit with instructions, and asked to have someone draw the blood and ship it back, with a chill pack, to the study laboratory via overnight mail. Mobile clinics also have been used successfully, such as in the National Health and Nutrition Examination Survey (NHANES) (35). Another disadvantage of venipuncture is low participation rates because of its invasive nature. Specifically in the NHS, it was noted that among women who had declined giving blood, 50% agreed to give a cheek cell specimen (36). Further, liquid blood specimens have biohazard potential, requiring special training and storage conditions.
To overcome difficulties with venipuncture, several recent studies have focused on collecting blood on filter paper using a finger prick (34,37–43). This method has been used for years to test for uncommon, but treatable, genetic conditions in infants (38). Recently, extraction methods have improved such that many hormones can be assayed from blood spots, including thyroid hormones, prolactin, sex hormones, gonadotropins, growth factors, leptin and stress hormones (37,39–43). The primary advantages include that the method is relatively non-invasive, can be conducted serially, presents a reduced biohazard potential when dry, and is feasible to collect on a large scale (40–43). One study reported that women found repeated blood spot sampling to be less troublesome than venipuncture or saliva collection (40).
Bre
ast m
ilk+B
reas
t pum
p, c
onta
iner
, ins
truct
ions
, sto
rage
via
l+H
ome-
base
d+L
ittle
kno
wn
abou
t pro
cess
ing
or a
ccep
tabl
e am
ount
of
tim
e un
til fr
eezi
ng
+May
refle
ct b
reas
t tis
sue
horm
one
expo
sure
+Use
for i
nfor
mat
ion
on in
fant
hor
mon
e co
nsum
ptio
n+F
ew a
ssay
s de
velo
ped
for t
his
sam
ple
type
+Onl
y ap
plie
s to
lact
atin
g w
omen
Bre
ast n
ippl
e as
pira
te fl
uid
+Tra
ined
nur
se o
r clin
icia
n+S
yrin
ge, a
pplic
ator
, sto
rage
via
ls+L
ittle
kno
wn
abou
t pro
cess
ing
or a
ccep
tabl
e am
ount
of
tim
e un
til fr
eezi
ng
+May
refle
ct b
reas
t tis
sue
horm
one
expo
sure
+May
bet
ter m
easu
re in
tracr
ine
prod
uctio
n of
ho
rmon
es
+Few
ass
ays
deve
lope
d fo
r thi
s sa
mpl
e ty
pe+O
nly
appl
ies
to w
omen
+Can
onl
y be
obt
aine
d fro
m a
bout
50%
of w
omen
+Onl
y sm
all v
olum
es c
an b
e ob
tain
ed
Oth
er ti
ssue
s+G
ener
ally
can
onl
y be
obt
aine
d vi
a su
rger
y by
a
clin
icia
n+F
resh
sam
ples
mus
t be
flash
-froz
en im
med
iate
ly+P
roce
ssin
g in
to p
araf
fin re
sults
in a
bilit
y to
sto
re
long
-term
at r
oom
tem
pera
ture
+Can
mea
sure
hor
mon
e le
vels
at t
he ti
ssue
of i
nter
est
+May
be
able
to s
tain
par
affin
-em
bedd
ed ti
ssue
to
dete
rmin
e pr
otei
n le
vels
sem
i-qua
ntita
tivel
y+C
an e
xtra
ct D
NA
or R
NA
+Few
ass
ays
curr
ently
ava
ilabl
e fo
r tis
sue
+Par
affin
em
bedd
ing
may
lim
it as
say
type
s+V
ery
inva
sive
and
diff
icul
t to
obta
in o
n a
larg
e-sc
ale

204
However, there are several disadvantages of blood collection via finger prick. The most important is that only a limited number of hormones can be assayed from one collection. In addition, differences in haematocrit between participants can introduce systemic or random measurement error in hormone levels, since the sample is whole blood (37,41). Some evidence suggests, however, that the filter paper can partially ameliorate this problem, as blood with high haematocrit tends to impregnate a smaller volume on the filter paper (37). Further, some studies have reported that while correlations for sex hormones between venipuncture and filter paper are high for women, the correlations appear lower in men (40,41); the mechanism behind this is unclear. When measuring estradiol, testosterone and progesterone in men and premenopausal women, blood spot hormone levels explained 89% of the variance of serum levels in women, but only 46% in men (41). Other issues to note are that certain filter paper types may inhibit some assays (38), clear participant instructions are important for obtaining reliable samples (34), and the filter paper must be kept at a relatively low humidity (38).
Urine
Urine specimens are another commonly collected biological specimen, particularly because their collection is non-invasive (34). It also can be easily collected in infants and toddlers by putting a pad in the child’s diaper. In general, urine contains hormone metabolites, rather than primary hormones, and reflects excretion over the period of the collection. Therefore, it can be difficult to determine over what time period to collect the urine (e.g. 24 hours, overnight, first morning
sample, or spot collection (34). The timing of urine collections depends on the hormone of interest. For example, the intraclass correlations (ICC) for a morning-spot versus 24-hour urine were 0.78 for estrone-3-glucuronide and 0.46 for pregnandiol-3-glucuronide; similar ICCs were observed for overnight versus 24-hour urines. This suggests that a morning spot urine was acceptable for the estrone metabolite, but neither the spot nor overnight urine appear to capture all the circadian variation for pregnandiol. Morning urines are acceptable for assessing nocturnal urinary melatonin production (44). Urine can be collected serially and in large volumes, allowing for multiple assays to be run. It can also be collected on filter paper to minimize storage needs and reduce the biohazard potential (34).
A primary disadvantage of urine is that its concentration varies substantially both between persons and within the same person over time (45). Creatinine is commonly used to measure urine concentration. Most studies have calculated the analyte/creatinine ratio to adjust for volume. However, it has been reported that creatinine levels should be included in the regression model as an independent variable. This adjusts for concentration while allowing one to assess the significance of other predictors in the model independently of creatinine levels (45). One other disadvantage of urine is that most hormones, or their metabolites, exist in low concentrations, often necessitating large volumes to conduct the assays.
Saliva
More recently, saliva has been used for measuring hormones. Generally, plasma and salivary hormone values
were highly correlated, including for cortisol, androgens, estrogens and progesterones (46). These hormones enter the saliva by passive diffusion, thus the levels specifically reflect the free, unbound, circulating fraction (47,48). Melatonin levels also correlate well between plasma and saliva (49). However, for several protein hormones, such as thyroid hormones, prolactin, or IGF-1, the salivary level bears little relationship to plasma levels and is unlikely to be of any research value (47).
Advantages of saliva sampling include: it is non-invasive, painless, easily performed, relatively inexpensive, has higher rates of compliance, and can provide quantitative data of biologically active hormone levels in circulation (40,46). Salivary sampling also avoids stress sometimes associated with venipuncture, which can elevate some hormones, particularly cortisol (50). Another benefit is that saliva samples can be collected at home with minimal training (40,50); further serial collections are easily conducted.
Despite these advantages, a major disadvantage of saliva is that hormone concentrations are much lower than in plasma, because salivary hormone levels reflect the free levels, which is typically 1–10% of the total plasma level (40). Therefore, saliva assays often require large sample volumes and highly sensitive (and thus expensive) assays (50). Further, blood contamination in the oral mucosa can lead to substantial measurement error by increasing measured levels. Stimulated saliva collection methods, additionally, can bias hormone assays. For example, the use of cotton-based absorbent materials, or chewing gum, to stimulate saliva flow can artificially elevate assay results (40). Therefore, it is important to

Unit 3 • Chapter 12. Assessment of the hormonal milieu 205
Un
it 3
Ch
ap
ter
12
pilot sample collection techniques to ascertain whether such procedures interfere with the assays of interest.
One lesser known method of saliva sampling is a diffusion-sink device (51). This device is a small ring that the participant places orally for some set time period. The sink has a membrane that allows diffusion of free hormones, and thus measures the average freely diffusing concentration of an analyte over time. These devices reject artefacts arising from blood plasma contamination of saliva and provide a time-averaged sample, without requiring the subject to adhere to a frequent-sampling schedule (51).
Other sample types
Other specimen types, such as breast milk, breast nipple aspirate fluid and other tissues (e.g. tumour, adipose, colon polyps) can be obtained (34,52); however, they often are difficult to collect or require invasive procedures. The greatest disadvantage, though, is that it can be hard to conduct assays on these specimen types. Despite this, measuring hormones in these specimens may reflect true exposure at the tissue level better than from other sampling types.
Collection, processing and storage
As discussed in Chapter 3, the collection, processing, and storage of samples may affect the ability to accurately measure the hormonal milieu (36,53–56). Several factors for sample collection must be considered, including the study population, timing and location of the collection. Depending on these factors, the samples may need to be processed in a non-standard manner. A common issue in epidemiologic studies is that
of delayed processing or delayed freezing. The effects of such protocols on the hormone of interest must be evaluated before assaying. Finally, storage of study specimens, particularly long-term storage in prospective studies, is an important and complex issue requiring appropriate acquisition of space and resources to maintain freezers and other related equipment.
Sample collection
Selection of the appropriate study population for any epidemiologic study is important. However, when studying hormone levels, careful consideration of the participants is often necessary to reduce bias. For example, in a study of predictors of estrogen levels, it would be inappropriate to combine men and women, premenopausal and postmenopausal women, or postmenopausal women taking hormones (PMH) versus not, as these groups have different mean estrogen levels. In this case, if gender, menopausal or PMH status was associated with the exposure, the observed association will be biased. Statistical adjustment alone generally cannot correct for this strong bias, particularly if the association varies across these subgroups.
The following example of the relationship between adiponectin and estradiol levels illustrates how combining inappropriate populations can alter study results. Experimental data suggest that adiponectin may, in part, regulate estradiol levels. But because adiponectin and estradiol are both derived primarily from adipose tissue in postmenopausal women, it is important to study this association on a population level, including adjustment for body mass index (BMI). One study observed no relationship after adjustment for
BMI in postmenopausal women not using PMH (57). This contradicted two previous studies, which reported that additional adjustment for BMI did not attenuate the relationship (58,59). However, one study (59) combined PMH users and non-users, likely biasing the results, since PMH users had higher estrogen and lower adiponectin levels than non-users. The other study combined premenopausal and postmenopausal women (58). Given that premenopausal women have higher estradiol levels, and that the primary sources of estradiol are the ovaries in premenopausal women and body fat in postmenopausal women (1), the results of this study likely were biased as well.
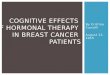
Also important is the timing of the sample collection, since some hormones can fluctuate yearly, seasonally, monthly, daily, hourly and even from minute to minute (Figure 12.1). Other factors that can influence some hormones include fasting, alcohol intake, physical activity and medications. Understanding the underlying biology of the hormone(s) of interest is important to determining the optimal timing of sample collection. Three examples of this issue are elaborated upon.
Estrogen and progesterone are known to vary widely during the menstrual cycle in premenopausal women (1). Sample collection in this population, therefore, should either standardise the day(s) in the cycle on which samples are drawn, or collect detailed information about menstrual cycle start dates before and after the collection. In the NHSII, premenopausal women were asked to collect two blood samples, one in the early follicular phase and one in the mid-luteal phase, times when sex hormones are relatively stable from day to day (60). Women also returned a postcard with the

206
date their next menstrual cycle began. This information, along with the date of their previous cycle, allowed calculation of the cycle day on which the blood samples were drawn. One disadvantage of this method is that the investigator is reliant on women to remember when to collect the blood samples. Another method is to have women use home-based ovulation kits to time sample collection for a certain number of days after ovulation (61). The major disadvantages of this method are cost and the
need to train women to use the kits appropriately. An alternative approach is to ask women to collect a sample on any day of their menstrual cycle and then provide specific dates of their cycle before (and if possible, after) collection and their average cycle length (62). This allows estimation of the cycle day. The main disadvantage of this method is that it reduces power to examine menstrual phase-specific associations. Ultimately, the collection method is dependent on the population and resources.
Several hormones have a circadian rhythm, with the most well characterized being melatonin. Levels are high at night while sleeping, and decrease during the daylight hours (44). In small, laboratory-based studies, the most common method of assessing melatonin has been to collect serial blood samples over a 24-hour period. However, this method is too labour-intensive for large epidemiologic studies. One alternative is to collect a blood sample at the same time of day for each participant. The utility
Figure 12.1. Four types of hormonal variation. Graph (a) shows how estradiol changes by day of the menstrual cycle with day 0 being the day of ovulation among 20–34 year olds ( ) and 35–46 year olds (•) cycling women (adapted from (116)). Graph (b) provides an example of how vitamin D concentrations vary over the course of one year (i.e. by season) among postmenopausal women living in New Zealand (adapted from (117)). Graph (c) demonstrates circadian variation across 3 days of a commonly measured urinary metabolite of melatonin, 6-sulphatoxymelatonin, in both young and elderly individuals (adapted from (118), copyright © 2005, Informa Healthcare. Reproduced with permission of Informa Healthcare). Graph (d) shows how IGF-1 levels vary by age in men and women, with a sharp increase early in life and a slow decline later in life (adapted from (119))

Unit 3 • Chapter 12. Assessment of the hormonal milieu 207
Un
it 3
Ch
ap
ter
12
of this method is limited, though, since the circadian pattern is not entrained to the same time of day for everyone (63). Another option is to collect urine to assay melatonin metabolites. Studies indicate that urinary levels, from either a 24-hour or first morning urine, or sequential saliva samples, are highly correlated with plasma melatonin (44,64,65).
A third example is that of plasma, or serum insulin, which is strongly affected by the number of hours since last eating (1). At minimum, time of last food consumption should be collected at the blood draw. However, if these hormones are important biomarkers, investigators should instruct participants to not consume any food or drink for at least 8 to 10 hours before the blood draw. Study staff should carefully ask participants about their food intake during that time and reschedule the collection if necessary. Of note is that for some diseases an alternative hypothesis exists: that the postprandial insulin response is most relevant to disease risk (66). If so, collecting a blood sample soon after eating would be preferred.
Sample processing
Sample collection and its processing should be conducted in a rigorous and standardized manner. In general, certain methods are preferred (e.g. immediate processing of samples); however this may not be feasible in some studies, particularly when participants are dispersed geographically. While this topic is covered in detail in Chapter 3, two issues are highlighted which are often faced when assessing hormones: delayed processing and delayed freezing.
Extensive pilot testing has shown that many hormones, including estrogens, androgens,
prolactin, IGFs and gonadotropins, are not substantially affected by blood remaining unprocessed for 24 to 48 hours, while others, such as adrenocorticotropic hormone (ACTH), arginine vasopressin and free PSA, cannot be assessed with this protocol (31–33,67–70). Interestingly, several studies reported increasing testosterone levels with delayed processing, likely due to ex vivo conversion of precursor hormones (32,68,70). However, levels across delayed processing times remained highly correlated, suggesting that this approach is acceptable. Thus, each hormone of interest should be pilot tested for stability of the analyte over increasing time of delayed processing.
A delay in freezing can occur if there is delayed processing or if samples are processed immediately and frozen at a later time. For blood specimens, most hormones are stable if kept chilled (~4 °C) for up to 3 days before freezing; however, others, such as free PSA and ACTH, should be processed and frozen immediately (31,33,67,69). Urinary catecholamine levels appear to be stable when stored for 24 hours at room temperature or chilled, provided that samples are acidified at once (71). Saliva hormones tend to be stable, and can be stored at room temperature for at least one week without degradation (47). However, these samples can mould after 4–7 days; thus they should be frozen or refrigerated if possible (34). In general, filter paper collections need to be kept refrigerated at a low humidity to maintain hormone stability (38).
Storage options
Freezing and refrigeration are the most commonly used storage modalities; the merits of these
options are enumerated in Chapter 3. In general, liquid nitrogen freezers (≤ 130 °C) are the best choice for long-term storage of samples, since temperatures in mechanical freezers can vary widely (72). Unfortunately it is difficult to directly assess the effects of long-term storage on hormone degradation. Two study designs can be used. One method is to collect samples at one time point and then measure the hormone(s) of interest several times over a period of years. Thus, baseline biomarker levels are the same for each person, but laboratory drift can make comparison of assay results over time difficult, especially if the assay changes. Interpretability strongly depends on the reliability of the assay. The second method is to collect samples from the same individuals, or population, over a period of years, storing them at each time point. Then, assay the samples together at the end of the study, reducing issues with assay variability. However, within-person changes in levels over time means that it is unclear whether the levels at each time are the same. Despite this, degradation of samples stored for long periods is an important issue.
There is some evidence that storage at −20 °C may not be acceptable for sex hormones (73,74). In particular, sex hormone binding globulin (SHBG) may dissociate from estradiol and testosterone, decreasing measurable non-bound levels of these hormones (73). However, long-term storage for blood at −70 °C or colder appears to be acceptable for estradiol, testosterone, DHEAS, prolactin, IGFs, TGF-β1 and urinary 6-sulfatoxymelatonin, among others (30,74–79). If degradation is at issue, samples should be transferred to a colder storage modality. Given that modest levels of degradation

208
can be difficult to detect, another approach is to match the samples being compared (e.g. cases and controls) on storage time. This will reduce the effect of measurement error. Statistical modeling can also adjust for storage time or freezer temperature.
Overall issues surrounding sample collection, processing and storage are vital considerations when using hormone samples in epidemiologic studies. In particular, pilot studies that test sample collection and processing procedures are needed to determine feasibility and participant acceptability. Furthermore, if any non-standard protocols are used, it is important to test the effect of this on the hormones of interest before sending study samples for assay. In studies with long-term storage of samples, it is important to be aware of possible sample degradation over time and how that may affect the study design, analysis and interpretation.
Laboratory measurement issues
Three common sources of error are introduced when using biomarkers: issues related to specimen collection, processing, and storage (discussed in the previous section) (30,53,80); laboratory error and variability (36); and within-person variability over time (81). Since Chapter 8 discusses these latter two issues in detail, this chapter focuses specifically on hormone assays. In particular, there are often multiple methods for assaying a hormone, each with advantages and disadvantages. For example, one assay may require a large volume but have a higher sensitivity, while another uses a smaller volume but has lower sensitivity. Two examples are illustrated below.
The first example relates to measurement of sex hormones such as estradiol and testosterone. Three classes of assays are available to measure these hormones: mass spectrometry (MS); indirect radioimmunoassay (RIA), including a pre-extraction step; and direct immunoassays using chemiluminescent, colorimetric or fluorescent markers (82). When choosing which assay to use in a study, several factors should be taken into account, such as the amount of sample used, cost per sample, ease of assay, comparability with previous studies, and most importantly the assay reliability, validity and sensitivity in the hormone value range of the population under study (especially of concern if the values are low). Other issues are the abundance of structurally similar hormone metabolites that can cross-react with assay antibodies, and the binding of some hormones by SHBG, which can interfere with antibody binding (83,84). Differences in assays can be observed merely by noting the very different median levels of sex hormones measured in postmenopausal women across nine studies of breast cancer risk (7).
For sex hormones, the MS method obtains the highest marks for reliability, sensitivity and cross-reactivity (83). This method can measure multiple hormone metabolites simultaneously with a moderate amount of serum, plasma, or urine (~0.5mL). While MS is thought to be the gold standard for hormone measurement, recent analysis of inter-laboratory variation suggests that further standardization across laboratories is needed (83). This assay also is not widely available due to the expensive equipment and the need for highly-trained personnel to run the assays. The indirect assay methodology employs an extraction
step before RIA to remove hormone metabolites that can cross-react with the antibody. This method has a high correlation with MS measures, although values tend to be slightly higher than those measured by MS, and uses a similar sample volume (85,86). The primary disadvantage of this method is that it cannot be easily automated and is thus labour-intensive and expensive (83). Direct assays, in general, do not have an extraction step before antibody binding. While these assays are high-throughput, easily available, inexpensive and use low volume, they may have only modest correlations with MS and indirect assays, and substantially overestimate hormone values, as well as a poor sensitivity for samples with low hormone concentrations (82–86). In general, these assays are not useful for clinical applications where precise levels must be determined, and are likely a major source of variability in epidemiologic study results (for a thorough review of this topic, see (83)).
The second example exemplifies the importance of understanding the biology of the hormone being measured, in this case prolactin. One limitation of the prolactin assay used in most epidemiologic studies to date (an immunoassay) is that it measures multiple forms of prolactin circulating in plasma (87). However, these forms likely have different biological activities (88,89). For example, glycosylated prolactin appears to have a higher metabolic clearance rate and lower biologic activity than the non-glycosylated form (89,90). Assays to specifically measure particular prolactin isoforms are difficult, time-intensive and require large amounts of plasma, and hence are not feasible in epidemiologic studies. The Nb2 lymphoma cell bioassay, however, is a sensitive measure of

Unit 3 • Chapter 12. Assessment of the hormonal milieu 209
Un
it 3
Ch
ap
ter
12
overall somatolactogenic activity in biological fluids. This assay measures the activity of both prolactin and growth hormone (91), although a modification of the assay, including anti-growth hormone antibodies, allows for specific evaluation of prolactin bioactivity. This measure and the ratio between the prolactin bioassay and immunoassay have been evaluated in several studies of systemic lupus erythematosus and found to be of importance (90,92,93). A breast cancer case–control study reported that prolactin levels measured by bioassay, but not immunoassay, were significantly higher in cases versus controls (94). The correlation between the immunoassay and bioassay is about 0.50, suggesting that the bioassay provides additional information beyond the immunoassay (94).
Another important issue arises when pooling data from multiple different studies, such as in the sex hormone-breast cancer study mentioned above (7). Since each study conducts assays at various laboratories and times, frequently the distribution of the analyte (e.g. hormone levels) differs across studies (95). Various analytic techniques are available to deal with this problem (96). One method is to use study-specific quantile cut-points to determine risk estimates comparing high versus low values for each study, which can then be pooled. The major drawbacks of this method are that it is difficult to evaluate what absolute hormone levels are related to disease, and to assess dose–response relationships. Another method used is to pool the risk estimates for a doubling (or tripling, etc.) of sex hormone concentrations within each study and then pool the risk estimates. However, the only way to assess how the absolute levels
of a hormone compare across studies is to reassess a subset of samples from each laboratory used in each of the different studies (i.e. a calibration study) using a gold-standard assay.
Another approach to evaluating hormone levels is to assess genetic variation (e.g. single nucleotide polymorphisms (SNPs)), in the gene(s) associated with the hormone. Although estimates vary by hormone, a substantial component of the between-person variation observed in circulating hormone levels is genetically determined (e.g. ~40% for IGF-I (97)). For example, to assess the role of the steroid vitamin D in osteoporosis, several studies have evaluated SNPs in the vitamin D receptor (98). Furthermore, many studies have assessed variation in the sex steroid hormone metabolizing pathway in relation to cancer risk (99–101). Advantages to this approach include: retrospective case-control designs can be used without concern of the disease altering circulating hormone levels, genetic variation may provide information on the tissue hormonal environment, and genetic assays tend to be robust and with little to no variation in measures across studies. Disadvantages include not knowing the function (if any) of the SNPs measured, and small effect sizes. Ultimately, clearer answers likely will be obtained with approaches that evaluate multiple SNPs in a gene or across multiple genes in a pathway, but this requires extremely large sample sizes and complex statistical tools that are still in development. Although promising, this approach to evaluate the hormonal milieu has yet to provide substantial insight into the hormone-disease relationship (102). Yet with increasing sample sizes and method development, the potential of this approach should be realized soon.
Within-person stability over time
A particularly important source of measurement error in hormone studies is random variation in biomarker levels within an individual over time. Thus one measurement of the biomarker, as is common in many epidemiologic studies, may not accurately reflect an individual’s long-term exposure. Measurement error correction, or inclusion of multiple samples per participant, can ameliorate the attenuating effects of biomarkers with a high intra-individual variability over time (103–105).
The intraclass correlation coefficient (ICC) can be used to measure the stability or reliability within individuals over time or across different assay platforms (103,106-108). It is the ratio of the between-person variance with the total variance (between- plus within-person variance), and ranges from 0 to 1.0 (80,109). The ICC is distinct from a Pearson or Spearman correlation coefficient in that a common mean is assumed between repeated measures. The ICC can be assessed on the natural log-transformed or untransformed scale, although if the data are skewed it is best to log-transform. An advantage of the ICC is that the impact of the within-assay variability is considered relative to the total variation. For example, a somewhat high assay coefficient of variation (CV) may not be acceptable if there is very limited between-person variation (resulting in a low ICC), as the additional laboratory variability could overshadow true differences between individuals.
Overall, most sex steroid hormones are reasonably stable within postmenopausal women over a 1–3 year period, with intraclass correlations ranging from 0.5 to 0.9

210
(103,110-112). Similarly, IGF-I and IGFBP–3 levels have correlations in the range of 0.6 to 0.8 over a 1–3 year period (106,113). Urinary melatonin levels also appear stable over several years (114). Thus, although using a single blood measure for these hormones will result in some misclassification and attenuation of relative risks, this level of reproducibility is similar to that observed for other biological variables, such as blood pressure and serum cholesterol measurements; all parameters that are considered well-measured and consistent predictors of disease in epidemiologic studies (115). In contrast, prolactin has a lower reproducibility, with correlations over time in the range of 0.45 or lower, indicating greater attenuation in the relative risk estimates when using a single blood measurement. In a setting such as this, where
measurement error is higher (since the correlation of hormone levels within woman over time is lower), statistical methods that account for this error in the calculation of relative risks should be used (see Chapter 8), or collecting multiple samples per subject considered.
Future directions and challenges
Overall, the use of hormone measurements is becoming more common in epidemiologic studies. Several factors must be considered in the study design, sample collection, assay choice, and statistical analysis. Of greatest importance is a suitable choice of study population and sample type(s) (collected at an appropriate time), as well as proper storage facilities. Any non-standard methods should be pilot-tested before conducting
the formal study. Pilot studies should also be conducted when considering the use of a new assay or laboratory. Choice of assay type can have a large impact on measurement error, and, ultimately, the interpretation of results. Although not discussed in this chapter, assessment of laboratory precision and reproducibility on an on-going basis is extremely important (36). Additionally, studies assessing hormone stability within an individual over time are important to conduct, particularly if the hormone is the exposure of interest. It is important to ultimately address all these issues to obtain results that are both reliable and valid. A better understanding of the role of hormones in human disease will benefit immensely from well-conducted epidemiologic studies.
References
1. Strauss JF, Barbieri RL. Yen and Jaffe's reproductive endocrinology. Philadelphia (PA): Elsevier Saunders; 2004.
2. Hankinson SE, Colditz GA, Willett WC (2004). Towards an integrated model for breast cancer etiology: the lifelong interplay of genes, lifestyle, and hormones. Breast Cancer Res, 6:213–218.doi:10.1186/bcr921 PMID:15318928
3. Cuzick J, Powles T, Veronesi U et al. (2003). Overview of the main outcomes in breast-cancer prevention trials. Lancet, 361:296–300.doi:10.1016/S0140-6736(03)12342-2 PMID:12559863
4. Lewis-Wambi JS, Jordan VC (2005-2006). Treatment of postmenopausal breast cancer with selective estrogen receptor modulators (SERMs). Breast Dis, 24:93–105. PMID:16917142
5. Lønning PE (2007). Adjuvant endocrine treatment of early breast cancer. Hematol Oncol Clin North Am, 21:223–2 3 8 . d o i : 1 0 .1 0 1 6 / j . h o c . 2 0 0 7. 0 3 . 0 0 2 PMID:17512446
6. Hankinson SE (2005-2006). Endogenous hormones and risk of breast cancer in postmenopausal women. Breast Dis, 24:3–15. PMID:16917136
7. Key T, Appleby P, Barnes I, Reeves G; Endogenous Hormones and Breast Cancer Collaborative Group (2002). Endogenous sex hormones and breast cancer in postmenopausal women: reanalysis of nine prospective studies. J Natl Cancer Inst, 94:606–616. PMID:11959894
8. Sonntag WE, Ramsey M, Carter CS (2005). Growth hormone and insulin-like growth factor-1 (IGF-1) and their influence on cognitive aging. Ageing Res Rev, 4:195–212.doi:10.1016/j.arr.2005.02.001 PMID:16024298
9. Carro E, Trejo JL, Gomez-Isla T et al. (2002). Serum insulin-like growth factor I regulates brain amyloid-beta levels. Nat Med, 8:1390–1397.doi:10.1038/nm793 PMID:12415260
10. Dik MG, Pluijm SM, Jonker C et al. (2003). Insulin-like growth factor I (IGF-I) and cognitive decline in older persons. Neurobiol Aging, 24:573–581.doi:10.1016/S0197-4580(02)00136-7 PMID:12714114
11. Kalmijn S, Janssen JA, Pols HA et al. (2000). A prospective study on circulating insulin-like growth factor I (IGF-I), IGF-binding proteins, and cognitive function in the elderly. J Clin Endocrinol Metab, 85:4551–4555.doi:10.1210/jc.85.12.4551 PMID:11134107
12. Okereke O, Kang JH, Ma J et al. (2007). Plasma IGF-I levels and cognitive performance in older women. Neurobiol Aging, 28:135–142.doi:10.1016/j.neurobiolaging.2005.10.012 PMID:16337715

Unit 3 • Chapter 12. Assessment of the hormonal milieu 211
Un
it 3
Ch
ap
ter
12
13. Okereke OI, Kang JH, Ma J et al. (2006). Midlife plasma insulin-like growth factor I and cognitive function in older men. J Clin Endocrinol Metab, 91:4306–4312.doi:10.1210/jc.2006-1325 PMID:16912125
14. Gable DR, Hurel SJ, Humphries SE (2006). Adiponectin and its gene variants as risk factors for insulin resistance, the metabolic syndrome and cardiovascular disease. Atherosclerosis, 188:231–244.doi:10.1016/j.atherosclerosis.2006.02.010 PMID:16581078
15. Menzaghi C, Trischitta V, Doria A (2007). Genetic influences of adiponectin on insulin resistance, type 2 diabetes, and cardiovascular disease. Diabetes, 56:1198–1209.doi:10.2337/db06-0506 PMID:17303804
16. Sattar N, Wannamethee G, Sarwar N et al. (2006). Adiponectin and coronary heart disease: a prospective study and meta-analysis. Circulation, 114:623–629.doi: 10.1161/CIRCULATIONAHA.106.618918 PMID:16894037
17. Choi KM, Lee J, Lee KW et al. (2004). Serum adiponectin concentrations predict the developments of type 2 diabetes and the metabolic syndrome in elderly Koreans. Clin Endocrinol (Oxf), 61:75–80.doi:10.1111/j.1365-2265.2004.02063.x PMID:15212647
18. Pischon T, Girman CJ, Hotamisligil GS et al. (2004). Plasma adiponectin levels and risk of myocardial infarction in men. JAMA, 291:1730–1737.doi:10.1001/jama.291.14.1730 PMID:15082700
19. Snijder MB, Heine RJ, Seidell JC et al. (2006). Associations of adiponectin levels with incident impaired glucose metabolism and type 2 diabetes in older men and women: the hoorn study. Diabetes Care, 29:2498–2503.doi:10.2337/dc06-0952 PMID:17065691
20. Vendramini MF, Ferreira SR, Gimeno SG et al.; Japanese-Brazilians Diabetes Study Group (2006). Plasma adiponectin levels and incident glucose intolerance in Japanese-Brazilians: a seven-year follow-up study. Diabetes Res Clin Pract, 73:304–309.doi:10.1016/ j .d iabres.2006.02.002 PMID:16546285
21. Wannamethee SG, Lowe GD, Rumley A et al. (2007). Adipokines and risk of type 2 diabetes in older men. Diabetes Care, 30:1200–1205.doi:10.2337/dc06-2416 PMID: 17322479
22. Dorgan JF, Baer DJ, Albert PS et al. (2001). Serum hormones and the alcohol-breast cancer association in postmenopausal women. J Natl Cancer Inst, 93:710–715.doi: 10.1093/jnci/93.9.710 PMID:11333294
23. Reichman ME, Judd JT, Longcope C et al. (1993). Effects of alcohol consumption on plasma and urinary hormone concentrations in premenopausal women. J Natl Cancer Inst, 85:722–727.doi:10.1093/jnci/85.9.722 PMID: 8478958
24. Hankinson SE, Willett WC, Manson JE et al. (1995). Alcohol, height, and adiposity in relation to estrogen and prolactin levels in postmenopausal women. J Natl Cancer Inst, 87:1297–1302.doi:10.1093/jnci/87.17.1297 PMID:7658481
25. Rinaldi S, Peeters PH, Bezemer ID et al. (2006). Relationship of alcohol intake and sex steroid concentrations in blood in pre- and post-menopausal women: the European Prospective Investigation into Cancer and Nutrition. Cancer Causes Control, 17:1033–1043.doi:10.1007/s10552-006-0041-7 PMID: 16933054
26. Davies MJ, Baer DJ, Judd JT et al. (2002). Effects of moderate alcohol intake on fasting insulin and glucose concentrations and insulin sensitivity in postmenopausal women: a randomized controlled trial. JAMA, 287:2559–2 5 6 2 . d o i :10 .10 01 / j a m a . 2 8 7.19 . 2 5 5 9 PMID:12020337
27. Rimm EB, Williams P, Fosher K et al. (1999). Moderate alcohol intake and lower risk of coronary heart disease: meta-analysis of effects on lipids and haemostatic factors. BMJ, 319:1523–1528. PMID:10591709
28. Holland NT, Smith MT, Eskenazi B, Bastaki M (2003). Biological sample collection and processing for molecular epidemiological studies. Mutat Res, 543:217–234.doi:10.1016/S1383-5742(02)00090-X PMID:12787814
29. Landi MT, Caporaso NE Sample collection, processing and storage. In: Toniolo P, Boffetta P, Shuker DEG et al., editors. Application of biomarkers in cancer epidemiology. Lyon: IARC Scientific Publication; 1997. p. 223–236.
30. Bolelli G, Muti P, Micheli A et al. (1995). Validity for epidemiological studies of long-term cryoconservation of steroid and protein hormones in serum and plasma. Cancer Epidemiol Biomarkers Prev, 4:509–513. PMID:7549807
31. Evans MJ, Livesey JH, Ellis MJ, Yandle TG (2001). Effect of anticoagulants and storage temperatures on stability of plasma and serum hormones. Clin Biochem, 34:107–112.doi:10.1016/S0009-9120(01)00196-5 PMID:11 311219
32. Key T, Oakes S, Davey G et al. (1996). Stability of vitamins A, C, and E, carotenoids, lipids, and testosterone in whole blood stored at 4 degrees C for 6 and 24 hours before separation of serum and plasma. Cancer Epidemiol Biomarkers Prev, 5:811–814. PMID: 8896892
33. Taieb J, Benattar C, Birr AS et al. (2000). Delayed assessment of serum and whole blood estradiol, progesterone, follicle-stimulating hormone, and luteinizing hormone kept at room temperature or refrigerated. Fertil Steril, 74:1053–1054.doi:10.1016/S0015-0282 (00)01546-6 PMID:11056261
34. Rockett JC, Buck GM, Lynch CD, Perreault SD (2004). The value of home-based collection of biospecimens in reproductive epidemiology. Environ Health Perspect, 112:94–104.doi:10. 1289/ehp.6264 PMID:14698937
35. National Center for Health Statistics. Plan and operation of the Third National Health and Nutrition Examination Survey, 1988–1994. Vital Health Stat 1. No. 32. US Department of Health and Human Services Publication PHS 94–1308. Hyattsville (MD): National Center for Health Statistics; 1994.
36. Tworoger SS, Hankinson SE (2006). Use of biomarkers in epidemiologic studies: minimizing the influence of measurement error in the study design and analysis. Cancer Causes Control, 17:889–899.doi:10.1007/s10552-006-0035-5 PMID:16841256
37. Diamandi A, Khosravi MJ, Mistry J et al. (1998). Filter paper blood spot assay of human insulin-like growth factor I (IGF-I) and IGF-binding protein-3 and preliminary application in the evaluation of growth hormone status. J Clin Endocrinol Metab, 83:2296–2301.doi: 10.1210/jc.83.7.2296 PMID:9661598
38. Howe CJ, Handelsman DJ (1997). Use of filter paper for sample collection and transport in steroid pharmacology. Clin Chem, 43:1408– 1415. PMID:9267321
39. Miller AA, Sharrock KC, McDade TW (2006). Measurement of leptin in dried blood spot samples. Am J Hum Biol, 18:857–860.doi:10.1002/ajhb.20566 PMID:17039473
40. Shirtcliff EA, Granger DA, Schwartz EB et al. (2000). Assessing estradiol in biobehavioral studies using saliva and blood spots: simple radioimmunoassay protocols, reliability, and comparative validity. Horm Behav, 38:137–147.doi:10.1006/hbeh.2000. 1614 PMID:10964528
41. Shirtcliff EA, Reavis R, Overman WH, Granger DA (2001). Measurement of gonadal hormones in dried blood spots versus serum: verification of menstrual cycle phase. Horm Behav, 39:258–266.doi:10.1006/hbeh.2001. 1657 PMID:11374911
42. Worthman CM, Stallings JF (1994). Measurement of gonadotropins in dried blood spots. Clin Chem, 40:448–453. PMID:8131281
43. Worthman CM, Stallings JF (1997). Hormone measures in finger-prick blood spot samples: new field methods for reproductive endocrinology. Am J Phys Anthropol, 104:1–21.doi:10.1002/(SICI)1096-8644(199709)104:1<1::AID-AJPA1 >3.0.CO;2 -V PMID:9331450
44. Cook MR, Graham C, Kavet R et al. (2000). Morning urinary assessment of nocturnal melatonin secretion in older women. J Pineal Res, 28:41–47.doi:10.1034/j.1600-079x.2000.280106.x PMID:10626600
45. Barr DB, Wilder LC, Caudill SP et al. (2005). Urinary creatinine concentrations in the U.S. population: implications for urinary biologic monitoring measurements. Environ Health Perspect, 113:192–200.doi:10.1289/ehp.7337 PMID:15687057
46. King SL, Hegadoren KM (2002). Stress hormones: how do they measure up? Biol Res Nurs, 4:92–103.doi:10.1177/1099800402 238334 PMID:12408215

212
47. Chiappin S, Antonelli G, Gatti R, De Palo EF (2007). Saliva specimen: a new laboratory tool for diagnostic and basic investigation. Clin Chim Acta, 383:30–40.doi:10.1016/j.cca. 2007.04.011 PMID:17512510
48. Lechner W, Marth C, Daxenbichler G (1985). Correlation of oestriol levels in saliva, plasma and urine of pregnant women. Acta Endocrinol (Copenh), 109:266–268. PMID:4013613
49. Voultsios A, Kennaway DJ, Dawson D (1997). Salivary melatonin as a circadian phase marker: validation and comparison to plasma melatonin. J Biol Rhythms, 12:457–466. PMID:9376644
50. Vining RF, McGinley RA, McGinley RA (1986). Hormones in saliva. Crit Rev Clin Lab Sci, 23:95–146.d o i : 1 0 . 3 1 0 9 / 1 0 4 0 8 3 6 8 6 0 9 1 6 5 7 9 7 PMID:3512171
51. Wade SE (1992). Less-invasive measurement of tissue availability of hormones and drugs: diffusion-sink sampling. Clin Chem, 38:1639–1644. PMID:1525992
52. Gann PH, Geiger AS, Helenowski IB et al. (2006). Estrogen and progesterone levels in nipple aspirate fluid of healthy premenopausal women: relationship to steroid precursors and response proteins. Cancer Epidemiol Biomarkers Prev, 15:39–44.doi:10.1158/1055-9965.EPI-05-0470 PMID:16434584
53. Tworoger SS, Hankinson SE (2006). Collection, processing, and storage of biological samples in epidemiologic studies: sex hormones, carotenoids, inflammatory markers, and proteomics as examples. Cancer Epidemiol Biomarkers Prev, 15:1578–1581.doi:10.1158/1055-9965.EPI-06-0629 PMID:16985015
54. Vaught JB (2006). Blood collection, shipment, processing, and storage. Cancer Epidemiol Biomarkers Prev, 15:1582–1584.doi:10.1158/1055-9965.EPI-06-0630 PMID: 16985016
55. Vaught JB, Caboux E, Hainaut P (2010). International efforts to develop biospecimen best practices. Cancer Epidemiol Biomarkers Prev, 19:912–915.doi:10.1158/1055-9965.EPI -10-0058 PMID:20233852
56. Betsou F, Lehmann S, Ashton G et al.; International Society for Biological and Environmental Repositories (ISBER) Working Group on Biospecimen Science (2010). Standard preanalytical coding for biospecimens: defining the sample PREanalytical code. Cancer Epidemiol Biomarkers Prev, 19:1004–1011.doi:10.1158/ 1055-9965.EPI-09-1268 PMID:20332280
57. Tworoger SS, Mantzoros CM, Hankinson SE (2007). Relationship of plasma adiponectin with sex hormone and insulin-like growth factor levels. Obesity (Silver Spring), 15:2217–2224.doi:10.1038/oby.2007.263 PMID:17890489
58. Gavrila A, Chan JL, Yiannakouris N et al. (2003). Serum adiponectin levels are inversely associated with overall and central fat distribution but are not directly regulated by acute fasting or leptin administration in humans: cross-sectional and interventional studies. J Clin Endocrinol Metab, 88:4823–4831.doi:10.1210/jc.2003-030214 PMID:14557461
59. Im JA, Lee JW, Lee HR, Lee DC (2006). Plasma adiponectin levels in postmenopausal women with or without long-term hormone therapy. Maturitas, 54:65–71.doi:10.1016/j.maturitas.2005.08.008 PMID:16198517
60. Tworoger SS, Sluss P, Hankinson SE (2006). Association between plasma prolactin concentrations and risk of breast cancer among predominately premenopausal women. Cancer Res, 66:2476–2482.do i :10 .115 8 /0 0 0 8 - 5 472 .CA N - 05 - 33 69 PMID:16489055
61. Davis S, Mirick DK, Chen C, Stanczyk FZ (2006). Effects of 60-Hz magnetic field exposure on nocturnal 6-sulfatoxymelatonin, estrogens, luteinizing hormone, and follicle-stimulating hormone in healthy reproductive-age women: results of a crossover trial. Ann Epidemiol, 16:622–631.doi:10.1016/j.annepidem.2005.11.005 PMID:16458540
62. Kaaks R, Berrino F, Key T et al. (2005). Serum sex steroids in premenopausal women and breast cancer risk within the European Prospective Investigation into Cancer and Nutrition (EPIC). J Natl Cancer Inst, 97:755–765.doi:10.1093/jnci/dji132 PMID:15900045
63. Hsing AW, Meyer TE, Niwa S et al. (2010). Measuring serum melatonin in epidemiologic studies. Cancer Epidemiol Biomarkers Prev, 19:932–937.doi:10.1158/1055-9965.EPI-10-0004 PMID:20332275
64. Nowak R, McMillen IC, Redman J, Short RV (1987). The correlation between serum and salivary melatonin concentrations and urinary 6-hydroxymelatonin sulphate excretion rates: two non-invasive techniques for monitoring human circadian rhythmicity. Clin Endocrinol (Oxf), 27:445–452.doi:10.1111/ j .1365 -2265.1987.tb01172.x PMID:3436070
65. Pääkkönen T, Mäkinen TM, Leppäluoto J et al. (2006). Urinary melatonin: a noninvasive method to follow human pineal function as studied in three experimental conditions. J Pineal Res, 40:110–115.doi:10.1111/j.1600-079X.2005.00300.x PMID:16441547
66. Michaud DS, Wolpin B, Giovannucci E et al. (2007). Prediagnostic plasma C-peptide and pancreatic cancer risk in men and women. Cancer Epidemiol Biomarkers Prev, 16:2101–2109. PMID:17905943
67. Woodrum D, French C, Shamel LB (1996). Stability of free prostate-specific antigen in serum samples under a variety of sample collection and sample storage conditions. Urology, 48 Suppl;33–39.doi:10.1016/S0090-4295(96)00607-3 PMID:8973697
68. Hankinson SE, London SJ, Chute CG et al. (1989). Effect of transport conditions on the stability of biochemical markers in blood. Clin Chem, 35:2313–2316. PMID:2591049
69. Jane Ellis M, Livesey JH, Evans MJ (2003). Hormone stability in human whole blood. Clin Biochem, 36:109–112.doi:10.1016/S0009-9120(02)00440-X PMID:12633759
70. Kristal AR, King IB, Albanes D et al. (2005). Centralized blood processing for the selenium and vitamin E cancer prevention trial: effects of delayed processing on carotenoids, tocopherols, insulin-like growth factor-I, insulin-like growth factor binding protein 3, steroid hormones, and lymphocyte viability. Cancer Epidemiol Biomarkers Prev, 14:727–730.doi:10.1158/1055-9965.EPI-04-0596 PMID:15767358
71. Elfering A, Grebner S, Semmer NK et al. (2003). Two urinary catecholamine measurement indices for applied stress research: effects of time and temperature until freezing. Hum Factors, 45:563–574.do i :10 .1518 / h fes .4 5 .4 .5 6 3 . 270 8 6 PMID:15055454
72. Su SC, Garbers S, Rieper TD, Toniolo P (1996). Temperature variations in upright mechanical freezers. Cancer Epidemiol Biomarkers Prev, 5:139–140. PMID:8850276
73. Langley MS, Hammond GL, Bardsley A et al. (1985). Serum steroid binding proteins and the bioavailability of estradiol in relation to breast diseases. J Natl Cancer Inst, 75:823–829. PMID:3863985
74. Phillips GB, Yano K, Stemmermann GN (1988). Serum sex hormone levels and myocardial infarction in the Honolulu Heart Program. Pitfalls in prospective studies on sex hormones. J Clin Epidemiol, 41:1151–1156.doi:10.1016/0895-4356(88)90018-2 PMID:3210063
75. Barba M, Cavalleri A, Schünemann HJ et al. (2006). Reliability of urinary 6-sulfatoxymelatonin as a biomarker in breast cancer. Int J Biol Markers, 21:242–245. PMID:17177163
76. Ito Y, Nakachi K, Imai K et al.; JACC Study Group (2005). Stability of frozen serum levels of insulin-like growth factor-I, insulin-like growth factor-II, insulin-like growth factor binding protein-3, transforming growth factor beta, soluble Fas, and superoxide dismutase activity for the JACC study. J Epidemiol, 15 Suppl 1;S67–S73.doi:10.2188/jea.15.S67 PMID:15881197
77. Cauley JA, Gutai JP, Kuller LH, Dai WS (1987). Usefulness of sex steroid hormone levels in predicting coronary artery disease in men. Am J Cardiol, 60:771–777.doi:10.1016/0002-9149(87)91021- 6 PMID:3661391
78. Koenig KL, Toniolo P, Bruning PF et al. (1993). Reliability of serum prolactin measurements in women. Cancer Epidemiol Biomarkers Prev, 2:411–414. PMID:8220084
79. Orentreich N, Brind JL, Rizer RL, Vogelman JH (1984). Age changes and sex differences in serum dehydroepiandrosterone sulfate concentrations throughout adulthood. J Clin Endocrinol Metab, 59:551–555.doi: 10.1210/jcem-59-3-551 PMID:6235241

Unit 3 • Chapter 12. Assessment of the hormonal milieu 213
Un
it 3
Ch
ap
ter
12
80. Armstrong BK, White E, Saracci R. Principles of exposure measurement in epidemiology. New York (NY): Oxford University Press; 1992.
81. Vineis P. Sources of variation in biomarkers. In: Toniolo P, Boffetta P, Shuker DEG et al., editors. Application of biomarkers in cancer epidemiology. Lyon: IARC Scientific Publication; 1997. p. 59–71.
82. Stanczyk FZ, Cho MM, Endres DB et al. (2003). Limitations of direct estradiol and testosterone immunoassay kits. Steroids, 68:1173–1178.doi:10.1016/j.steroids.2003. 08.012 PMID:14643879
83. Stanczyk FZ, Lee JS, Santen RJ (2007). Standardization of steroid hormone assays: why, how, and when? Cancer Epidemiol Biomarkers Prev, 16:1713–1719.d o i :10 .115 8 /10 5 5 - 9 9 6 5 . EPI - 0 6 - 076 5 PMID:17855686
84. Stanczyk FZ, Jurow J, Hsing AW (2010). Limitations of direct immunoassays for measuring circulating estradiol levels in postmenopausal women and men in epidemiologic studies. Cancer Epidemiol Biomarkers Prev, 19:903–906.doi:10.1158/ 1055-9965.EPI-10-0081 PMID:20332268
85. Hsing AW, Stanczyk FZ, Bélanger A et al. (2007). Reproducibility of serum sex steroid assays in men by RIA and mass spectrometry. Cancer Epidemiol Biomarkers Prev, 16:1004–1008.doi:10.1158/1055-9965.EPI-06-0792 PMID:17507629
86. Lee JS, Ettinger B, Stanczyk FZ et al. (2006). Comparison of methods to measure low serum estradiol levels in postmenopausal women. J Clin Endocrinol Metab, 91:3791–3797.doi:10.1210/jc.2005-2378 PMID:16882749
87. Haro LS, Lee DW, Singh RN et al. (1990). Glycosylated human prolactin: alterations in glycosylation pattern modify affinity for lactogen receptor and values in prolactin radioimmunoassay. J Clin Endocrinol Metab, 71:379 –383.doi:10.1210/ jcem-71-2-379 PMID:2380335
88. Sinha YN (1995). Structural variants of prolactin: occurrence and physiological significance. Endocr Rev, 16:354–369. PMID: 7671851
89. Hoffmann T, Penel C, Ronin C (1993). Glycosylation of human prolactin regulates hormone bioactivity and metabolic clearance. J Endocrinol Invest, 16:807–816. PMID:8144855
90. García M, Colombani-Vidal ME, Zylbersztein CC et al. (2004). Analysis of molecular heterogeneity of prolactin in human systemic lupus erythematosus. Lupus, 13:575–583.doi:10.1191/0961203304lu1068oa PMID: 15462486
91. Bernichtein S, Jeay S, Vaudry R et al. (2003). New homologous bioassays for human lactogens show that agonism or antagonism of various analogs is a function of assay sensitivity. Endocrine, 20:177–190.doi:10.1385/ENDO:20:1-2:177 PMID:12668884
92. Cruz J, Aviña-Zubieta A, Martínez de la Escalera G et al. (2001). Molecular heterogeneity of prolactin in the plasma of patients with systemic lupus erythematosus. Arthritis Rheum, 44:1331–1335.doi:10.1002/1529-0131(200106)44:6<1331::AID-ART225>3.0. CO;2-Q PMID:11407692
93. Leaños-Miranda A, Chávez-Rueda KA, Blanco-Favela F (2001). Biologic activity and plasma clearance of prolactin-IgG complex in patients with systemic lupus erythematosus. Arthritis Rheum, 44:866–875.doi:10.1002/1529-0131(200104)44:4< 866::AID-ANR143>3.0.CO;2-6 PMID:11315926
94. Maddox PR, Jones DL, Mansel RE (1992). Prolactin and total lactogenic hormone measured by microbioassay and immunoassay in breast cancer. Br J Cancer, 65:456–460.doi:10.1038/bjc.1992.92 PMID:1558804
95. Taioli E, Bonassi S (2002). Methodological issues in pooled analysis of biomarker studies. Mutat Res, 512:85–92.doi:10.1016/S1383-5742(02)00027-3 PMID:12220591
96. Key TJ, Appleby PN, Allen NE, Reeves GK (2010). Pooling biomarker data from different studies of disease risk, with a focus on endogenous hormones. Cancer Epidemiol Biomarkers Prev, 19:960–965.doi: 10.1158/1055-9965.EPI-10-0061 PMID: 20233851
97. Harrela M, Koistinen H, Kaprio J et al. (1996). Genetic and environmental components of interindividual variation in circulating levels of IGF-I, IGF-II, IGFBP-1, and IGFBP-3. J Clin Invest, 98:2612–2615.doi:10.1172/JCI119081 PMID:8958225
98. Uitterlinden AG, Ralston SH, Brandi ML et al.; APOSS Investigators; EPOS Investigators; EPOLOS Investigators; FAMOS Investigators; LASA Investigators; Rotterdam Study Investigators; GENOMOS Study (2006). The association between common vitamin D receptor gene variations and osteoporosis: a participant-level meta-analysis. Ann Intern Med, 145:255–264. PMID:16908916
99. Dunning AM, Dowsett M, Healey CS et al. (2004). Polymorphisms associated with circulating sex hormone levels in postmenopausal women. J Natl Cancer Inst, 96:936–945.doi:10.1093/jnci/djh167 PMID:15 199113
100. Hunter DJ, Riboli E, Haiman CA et al.; National Cancer Institute Breast and Prostate Cancer Cohort Consortium (2005). A candidate gene approach to searching for low-penetrance breast and prostate cancer genes. Nat Rev Cancer, 5:977–985.doi:10. 1038/nrc1754 PMID:16341085
101. Olson SH, Bandera EV, Orlow I (2007). Variants in estrogen biosynthesis genes, sex steroid hormone levels, and endometrial cancer: a HuGE review. Am J Epidemiol, 165:235–245.doi:10.1093/aje/kwk015 PMID: 17110639
102. Rebbeck TR, Martínez ME, Sellers TA et al. (2004). Genetic variation and cancer: improving the environment for publication of association studies. Cancer Epidemiol Biomarkers Prev, 13:1985–1986. PMID:1559 8750
103. Hankinson SE, Manson JE, Spiegelman D et al. (1995). Reproducibility of plasma hormone levels in postmenopausal women over a 2–3-year period. Cancer Epidemiol Biomarkers Prev, 4:649–654. PMID:8547832
104. Michaud DS, Manson JE, Spiegelman D et al. (1999). Reproducibility of plasma and urinary sex hormone levels in premenopausal women over a one-year period. Cancer Epidemiol Biomarkers Prev, 8:1059–1064. PMID:10613337
105. White E. Effects of biomarker measurement error on epidemiological studies. In: Toniolo P, Boffetta P, Shuker DEG et al., editors. Application of biomarkers in cancer epidemiology. IARC Scientific Publication; 1997. p. 73–93.
106. Missmer SA, Spiegelman D, Bertone-Johnson ER et al. (2006). Reproducibility of plasma steroid hormones, prolactin, and insulin-like growth factor levels among premenopausal women over a 2- to 3-year period. Cancer Epidemiol Biomarkers Prev, 15:972–978.doi:10.1158/1055-9965.EPI-05-0848 PMID:16702379
107. Kotsopoulos J, Tworoger SS, Campos H et al. (2010). Reproducibility of plasma and urine biomarkers among premenopausal and postmenopausal women from the Nurses’ Health Studies. Cancer Epidemiol Biomarkers Prev, 19:938–946.doi:10.1158/1055-9965.EPI-09-1318 PMID:20332276
108. Thomas CE, Sexton W, Benson K et al. (2010). Urine collection and processing for protein biomarker discovery and quantification. Cancer Epidemiol Biomarkers Prev, 19:953–959.doi:10.1158/1055-9965.EPI-10-0069 PMID:20332277
109. Rosner B. Fundamentals of biostatistics. Belmont (CA): Duxbury Press; 1995.
110. Micheli A, Muti P, Pisani P et al. (1991). Repeated serum and urinary androgen measurements in premenopausal and postmenopausal women. J Clin Epidemiol, 44:1055–1061.doi:10.1016/0895-4356(91)90 007-V PMID:1940998
111. Muti P, Trevisan M, Micheli A et al. (1996). Reliability of serum hormones in premenopausal and postmenopausal women over a one-year period. Cancer Epidemiol Biomarkers Prev, 5:917–922. PMID:8922301
112. Toniolo P, Koenig KL, Pasternack BS et al. (1994). Reliability of measurements of total, protein-bound, and unbound estradiol in serum. Cancer Epidemiol Biomarkers Prev, 3:47–50. PMID:8118385
113. Muti P, Quattrin T, Grant BJ et al. (2002). Fasting glucose is a risk factor for breast cancer: a prospective study. Cancer Epidemiol Biomarkers Prev, 11:1361–1368. PMID:12433712

214
114. Schernhammer ES, Hankinson SE (2005). Urinary melatonin levels and breast cancer risk. J Natl Cancer Inst, 97:1084–1087.doi:10.1093/jnci/dji190 PMID:16030307
115. Willett WC (1998). Nutrition and chronic disease. Public Health Rev, 26:9–10. PMID:97 75714
116. Welt CK, McNicholl DJ, Taylor AE, Hall JE (1999). Female reproductive aging is marked by decreased secretion of dimeric inhibin. J Clin Endocrinol Metab, 84:105–111.doi:10.1210/jc.84.1.105 PMID:9920069
117. Bolland MJ, Grey AB, Ames RW et al. (2007). The effects of seasonal variation of 25-hydroxyvitamin D and fat mass on a diagnosis of vitamin D sufficiency. Am J Clin Nutr, 86:959–964. PMID:17921371
118. Kripke DF, Youngstedt SD, Elliott JA et al. (2005). Circadian phase in adults of contrasting ages. Chronobiol Int, 22:695–709.doi:10.1080/07420520500180439 PMID:1614 7900
119. Yu H, Mistry J, Nicar MJ et al. (1999). Insulin-like growth factors (IGF-I, free IGF-I and IGF-II) and insulin-like growth factor binding proteins (IGFBP-2, IGFBP-3, IGFBP-6, and ALS) in blood circulation. J Clin Lab Anal, 13:166–172.doi:10.1002/(SICI)1098-2825(1999)13:4<166::AID-JCLA5 >3.0.CO;2-X PMID:10414596