Embed Size (px)
Citation preview

JOURNAL OF PATHOLOGY, VOL. 178: 182-189 (1996)
ASSESSMENT OF THE DISTRIBUTION OF MITOCHONDRIAL RIBOSOMAL RNA IN MELAS AND IN THROMBOTIC CEREBRAL INFARCTS BY IN SITU
HYBRIDIZATION SETH LOVE AND DAVID A. HILTON
Depurtment of Neuropathology, Frenchay Hospital, Bristol BS16 ILE, U. K.
SUMMARY
In situ hybridization to mitochondrial ribosomal RNA (rRNA) has been used to study the distribution of mitochondria in paraffin-embedded autopsy brain tissue from two patients with MELAS (mitochondrial myopathy , encephalopathy, lactic acidosis, and stroke-like episodes) and other organs from one of the patients. Comparison of in situ hybridization and electron microscopic findings in an antemortem biopsy specimen of pylorus from the latter patient showed a close correspondence between the distribution of hybridization signal on light microscopy and of mitochondria in ultrathin sections. Strong hybridization signal was present over smooth muscle fibres of the muscularis externa, which contained abnormal accumulations of mitochondria on electron microscopy. Hybridization to sections of skeletal muscle confirmed previous reports of ‘ragged-red’ fibres in this disorder and of mitochondrial accumulations in the walls of intramuscular blood vessels. To try to elucidate the role of vessel wall accumulation of mitochondria in the genesis of the stroke-like lesions, the distribution of mitochondrial rRNA was assessed in sections of brain from both of the cases of MELAS and several cases of atherothrombotic cerebrovascular disease. Blood vessels in and adjacent to the cerebral lesions of MELAS showed strong hybridization signal with the mitochondrial probes, as was also seen in infarcts of various ages in the control brains. Only weak signal was present in the walls of blood vessels distant from the lesions, in both MELAS and control brains. These findings suggest that mitochondria accumulate in vascular endothelium and tunica media as a normal response to cerebral infarction or ischaemia. The accumulation of mitochondria in the cerebral lesions of MELAS may, a t least in part, be a reaction to the destructive effects of the underlying metabolic dysfunction.
KEY WORDS-MELAS; in situ hybridization; mitochondrial rRNA; blood vessels; pylorus; skeletal muscle; pancreatic islets; cerebral infarcts
INTRODUCTION
MELAS (mitochondrial myopathy, lactic acidosis, and stroke-like episodes) is an uncommon disorder of children and young adults. Clinical features include sudden onset of headaches, vomiting, convulsions, cortical blindness, and hemiplegia or hemianopia. Although there is usually some recovery between epi- sodes, the natural history is of increasing clinical impair- ment and, eventually, death. In most cases, there is a single point mutation in mitochondrial DNA (mtDNA), usually at nucleotide 3243, in the tRNAL“U(URR’ gene,2 although mutations at other positions, particularly nucleotide 3271, have been detected in some MELAS patients.’ The same nucleotide 3243 mutation has been found in a subgroup of patients with maternally- inherited diabetes mellit~s,~-’ usually in association with sensorineural deafness, and we have also detected the nucleotide 3243 mutation in association with chronic intestinal pseudo-obstruction,8 known by the acronym CIP0,9 although other acronyms have been applied to this disorder including POLIP-polyneuropathy, ophthalmoplegia, leukoencephalopathy and intestinal pseudo-obstruction,” and MNGIE-mitochondria1 neurogastrointestinal encephalomyopathy . ’ ’
Addressee for correspondence: S. Love, Department of Neuro- pathology, Frenchay Hospital, Bristol BS16 ILE, U.K.
CCC 0022-34 17/96/020 182-08 0 1996 by John Wiley & Sons, Ltd.
The pathogenesis of the stroke-like episodes and other manifestations of MELAS and these allied mitochon- drial disorders remains unclear. A higher proportion of mtDNA is mutated in clinically affected than in asymptomatic members of families with MELAS12 and in some families, the age of onset seems to be inversely related to the ratio of mutant to wild-type mtDNA.” However, although some studies have found a correla- tion between the relative amount of mtDNA in different tissues and the clinical presentati~n,’~’’ in other studies no such correlation has been demonstrable.83’ ‘-18 Sev- era1 authors have raised the possibility that the lesions in MELAS are essentially ischaemic in nature, due to a ‘mitochondrial angiopathy’.’’ 2’ Pathological studies of the central nervous system have shown infdrct-like lesions of varying ages, particularly in the cerebral hemispheres, within which the occipital lobes are often worst affected. There is evidence of increased activity of the mitochondrial enzyme succinate dehydrogenase in the intramuscular blood vessels of MELAS patients2* and an increase in the amount of mtDNA was detected by in situ hybr id i~a t ion .~~ Some, 1 y 3 2 0 , 2 4 3 2 5 although not
studies have reported abnormal accumulation of mitochondria within the endothelial cells and tunica media of blood vessels in the brain in MELAS. These observations have prompted speculation that the mito- chondrial accumulations may narrow the lumina of arterioles sufficiently to cause ischaemia.
Received 8 February 1995 Accepted 26 June 1995

ISH TO MITOCHONDRIA IN MELAS AND CEREBRAL INFARCTS 183
To investigate the distribution of mitochondria within the brains and other tissues of MELAS cases, we have used in situ hybridization (ISH) with digoxigenin- labelled probes to mitochondrial ribosomal RNA (rRNA). We have previously shown this technique to provide a good indication of the distribution of mito- chondria, even in paraffin sections.27 To evaluate the significance of the findings in the central nervous system, we have also assessed the distribution of mitochondria in cases of cerebral infarction due to atherothrombotic cerebrovascular disease.
MATERIALS AND METHODS
Two patients with MELAS were studied. The clinical and pathological findings in both patients have been reported in detail previously26 and the nucleotide 3243 mutation in mtDNA was demonstrated in autopsy material from one of these patients by the olymerase chain reaction (PCR) and Pan digestion.' ISH was performed on paraffin sections of brain from both patients and on the following additional material from the patient with the nucleotide 3243 mutation: sections of a pyloric biopsy that had been taken during life and sections of skeletal muscle, pancreas, liver, heart, and kidney obtained at autopsy.
ISH was also performed on paraffin sections of several thrombotic cerebral infarcts. The infarcts ranged in age from a few days to months or longer. The sections were obtained from a range of autopsy brain specimens and, in three cases, cerebral biopsies, from patients without any clinical or biochemical features to suggest mitochondrial disease.
Fig. l-Section of a pyloric biopsy from a MELAS patient, showing normal-looking antral mucosa, submucosa, and part of the muscularis externa. Haematoxylin and eosin
Fig. 2-Strong ISH signal for mitochondrial rRNA in smooth muscle fibres of the muscularis externa, blood vessels (arrows), and myenteric ganglia (inset) in a biopsy from a MELAS patient
Sections of appropriate normal control tissues- brain, pylorus, skeletal muscle, pancreas, liver, heart, or kidney-were included in each batch of ISHs.
Probes Synthetic oligonucleotides, complementary to the 16s
subunit of mitochondrial rRNA and labelled at the 3' end with poly-dUTP- 1 1 -digoxigenin, were used as described p r e v i ~ u s l y . ~ ~ - ~ ~
In situ hybridization
Paraffin sections, 5 pm in thickness, were collected onto aminopropyltriethoxysilane-coated glass slides. The sections were dewaxed in xylene and alcohol, washed in 2 x SSC at 70°C for 10 min, digested in 15 puglml proteinase K for 60 min at 37"C, and refixed in 0.4 per cent paraformaldehyde in 0.1 M phosphate buffer for 20 min at 4°C. Hybridization was overnight at 37°C in 5Opl of buffer containing 0.1 ndpl probe, 30 per cent formamide, 600 mM NaC1, 0.1 M phosphate buffer, 10 per cent dextran sulphate, and 150pglml sheared salmon sperm DNA. The sections were washed in 2 x SSCl30 per cent formamide at 37T, incubated for 10 min in Tris-HC1 (pH 7.5)/0.5 M NaC1/3 per cent bovine serum albumin, and then for 30 min with anti-digoxigenin antibody conjugated to alkaline phosphatase (Boehringer Mannheim). Bound anti- body was visualized by reaction with nitroblue tetrazo- lium salt and 5-bromo-4-chloro-3-indolyl phosphate solution.

184 S. LOVE AND D. A. HILTON
Fig. .?-Electron micrograph showing smooth muscle fibres in the pyloric biopsy from the MELAS patient. The fibres contain abnormal accumulations of mitochondria, including several that are of abnormal size and shape (large arrows) and a few with osmiophilic inclusions (small arrow)
RESULTS Pylovus
In sections stained with haematoxylin and eosin, the biopsies appeared entirely normal (Fig. 1). On ISH, strong signal was present in the mucosal epithelium, in the walls of blood vessels, in submucosal and myenteric ganglia, and in the smooth muscle of the muscularis externa (Fig. 2). Hybridization to control sections of normal pylorus showed strong signal in the mucosa, blood vessels, and ganglia, but only weak signal in the muscularis externa.
The distribution of signal on ISH was compared with that of mitochondria in ultrathin sections of
glutaraldehyde-fixed tissue from the same biopsy. This confirmed the presence of numerous mitochondria in smooth muscle fibres of the muscularis externa (Fig. 3), also in ganglion cells, Schwann cells, and, to a lesser extent, endothelial cells and cells in the tunica media of intramuscular and submucosal blood vessels. Many of the mitochondria were abnormally large or excessively elongated and a few contained dense, osmiophilic bodies. No paracrystalline inclusions were noted.
Skeletal muscle There was no discernible hybridization to muscle
fibres in control sections and only scanty, variable

1SH TO MITOCHONDRIA IN MELAS AND CEREBRAL INFARCTS 185
Fig. &Section of skeletal muscle from the MELAS patient hybridized with probes to mitochondrial rRNA. The fascicle towards the top left of the figure includes several fibres with abnormally strong hybridiza- tion signal, including some in which the signal is predominantly subsarcolemmal (small arrows). Note the strong hybridization to interfascicular blood vessels (large arrows)
hybridization to blood vessels, Sections from the MELAS patient included many fibres with excessive hybridization signal (Fig. 4). In several of these, the signal was strongest in the subsarcolemmal region, as would be expected in mitochondrial myopathy. Most interfascicular arterioles and venules, and some endo- mysial capillaries, also showed strong hybridization for mitochondrial rRNA. In arterioles, the hybridization was to the tunica media as well as to the endothelium.
Pancreas
The pattern of hybridization to exocrine pancreatic tissue in the MELAS patient was similar to that in control sections, with moderate but quite variable signal over acinar cells and ductular epithelium. Control tissue included many pancreatic islets, which hybridized rela- tively strongly with the mitochondrial probes. In the MELAS patient, only two islets were identified in a cross-section of pancreatic tail and these showed only weak hybridization signal (Fig. 5).
Liver, heart, and kidney
No obvious abnormalities were noted in the pattern of hybridization in the MELAS patient but tissue preser- vation was suboptimal and the sections were unsuitable for detailed assessment.
Brain
Blood vessels in and adjacent to the cerebral infarct- like lesions of MELAS showed strong hybridization
Fig. 5-Sections of pancreas from the MELAS patient (a) and control (b). Although the strength and pattern of mitochondrial ISH to exocrine pancreatic tissue is similar in both sections, there is weaker signal over the islet in the MELAS patient (arrow) than over the islets in the normal control (arrows)
signal with the mitochondrial probes (Figs 6, 7, and 8). This was a consistent finding in all the lesions examined in both cases. The hybridization was to vascular endothelium and tunica media and, in the more recent lesions, to scattered macrophages. There was only weak signal in the walls of blood vessels away from the infarct-like lesions, although moderately intense hybridi- zation signal was noted in scattered neurons, in the larger blood vessels in the leptomeninges, and in choroid plexus epithelium.
Thrombotic infarcts of all ages showed strong hybridization to the walls of blood vessels (Figs 9 and 10) and, in recent lesions, to macrophages as well. As in the cases of MELAS, there was also hybridization to scattered neurons, to the larger blood vessels in the leptomeninges, and to choroid plexus epithelium; there was only weak hybridization to blood vessels at a distance from the infarcts.
DISCUSSION
Our findings provide further evidence of the accumu- lation of mitochondria in the walls of blood vessels in some of the tissues affected by MELAS. The strong hybridization to mitochondrial rRNA in the walls of blood vessels in skeletal muscle is in keeping with the observation by Hasegawa et of increased succinate dehydrogenase activity and the detection of excessive amounts of mtDNA by ISH.23 ISH also provided clear evidence of the accumulation of mitochondria in the

186 S. LOVE AND D. A. HILTON
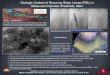
Fig 6-Pdrdkl sections of Lerebrdl cortex from d MELAS patient, stained with haematoxylin and eosin (top) and hybridized for mito- chondrid~ rRNA (bottom) The cortex includes several old infarct-like lesions. within which blood vessels show strong mitochondrial hybridi- zation signal (arrous to corresponding lesions in haematoxylin and eosiii-stnined section and ISH prepdrdtion)
endothelium and tunica media of blood vessels within the cerebral lesions of MELAS.
The role and pathogenetic significance of the mito- chondria] accumulations in the walls of blood vessels is, however, debatable. Several observations argue against the simple hypothesis that the mitochondrial aggre- gates narrow the vascular lumina so much as to cause
Fig 7-Section through an old MELAS lesion, viewed at higher magnification, showing much stronger hybridization for mitochondrid in the walls of blood vessels within the lesion (towards the bottom of the figure) than in those outside (top of figure, Arrows to some)
ischaemic damage. No angiographic abnormalities have been noted in these patients.2’’26 Studies of cerebral blood flow have shown flow to be increased rather than decreased, both within the lesions and in the preserved parts of the Our present observations suggest that the accumulation of mitochondria in the walls of blood vessels may in part be a reactive phenomenon, the pattern closely resembling that in cerebral infarcts. In both MELAS and thrombotic infarcts, the ISH signal with the mitochondrial probes was much weaker away from the lesions than within or adjacent to them.
The precise stimuli for mitochondrial proliferation are not known but may include ischaemia, tissue acidosis, and a variety of chemical mediators released during tissue necrosis. Heffner and Barrod2 recorded striking proliferation of intramuscular mitochondria in tibialis anterior in the rat within 24 h of application of a rubber band tourniquet to the thigh. The resulting accumula- tions included many mitochondria that were abnormally large or contained paracrystalline inclusion bodies. Other reports of abnormalities in the distribution or appearance of mitochondria in ischaemic skeletal muscle include those of Reznik3’ and Karpati et In tissue culture, mtDNA with the MELAS-associated mutation has a marked replicative advantage over wild-type mtDNA.35 One might therefore expect that proliferation of mitochondria in vivo would cause an increase in the ratio of mutant to wild-type mtDNA but, a t least in skeletal muscle fibres, this does not seem to be the case: the relative proportions of mutant and wild-type mtDNA as assessed by PCR seem to be the same in ‘ragged-red’ as in ‘non-ragged-red’ fibres.’6

ISH TO MITOCHONDRIA IN MELAS AND CEREBRAL INFARCTS 187
Fig. &Parallel sections through the edge of a recent infarct-like lesion in a MELAS patient. One section has been stained with haematoxylin and eosin (top); the other has been hybridized for mitochondrial rRNA (bottom). Blood vessels within and immediately adjacent to the lesion (towards the bottom of the figures) show strong hybridization signal
It is possible that the pathogenesis of the lesions in MELAS differs in different tissues, as does the under- lying metabolic defect. MullerHocker et nl.37 found reduced levels of cytochrome c oxidase activity and immunohistochemically-detectable protein in heart and skeletal muscle, but not brain. Conversely, NADH dehydrogenase (complex I) activity was markedly
Fig. 9-Parallel sections through the edge of a recent infarct in a control brain. One section has been stained with haematoxylin and eosin (top); the other has been hybridized for mitochondria1 rRNA (bottom). As in Fig. 8, there is stronger hybridization signal over blood vessels within and adjacent to the lesion (which is towards the bottom of the figures) than over those further away (arrows to some)
reduced in brain (to 20 per cent) but only moderately reduced (to 50 per cent) in skeletal muscle.
Little has previously been reported on the pathologi- cal basis of the gastrointestinal abnormalities in MELAS. Magnetic resonance imaging in patients with the syndrome of polyneuropathy, ophthalmoplegia,

188 S. LOVE AND D. A. HlLTON
the technique can be used to analyse the distribution of mitochondria in a wide range of archival paraffin- embedded tissues.
Fig. 10-Section through an old, atherothrombotic infarct it1 the cerebral cortex of a control brain. Blood vessels within the infarct show strong hybridization signal for mitochondrial rRNA, whereas those further away are relatively weakly labelled (arrows to some)
leucoencephalopathy, and chronic intestinal pseudo- obstruction was reported by Simon et a1." to show 'endoneurial fibrosis and demyelination' in the periph- eral nervous system. These authors attributed the gastrointestinal dysmotility to visceral neuropathy. However, apart from our own brief previous descrip- tion,26 there are, to our knowledge, no reports of the pathology of the gastrointestinal tract itself. The pres- ence of large accumulations of mitochondria in the smooth muscle fibres of the muscularis externa are similar to the findings in skeletal muscle and suggest that the gastrointestinal dysmotility may be myogenic rather than neurogenic in origin.
The association of the mtDNA nucleotide 3243 mutation with a subtype of diabetes mellitus is well do~umen ted .~ Most patients do not have other features of MELAS, but Kadowaki et ~ 1 . ~ found bio- chemical evidence of diabetes mellitus in 8 of 39 patients with MELAS due to the nucleotide 3243 mutation. Only limited conclusions can be drawn from our observations on the pathology of the pancreas in a single case of MELAS, particularly as a diagnosis of diabetes mellitus was never suggested during life in this patient. The paucity of islets and the reduced mitochondrial hybridi- zation signal are, however, consistent with observations of decreased secretion of insulin in diabetes due to the nucleotide 3243 rnutation5x6 and it will be of interest to see whether or not these observations hold true in other patients with this mutation.
Finally, the close correlation between the findings on ISH and on electron microscopy of the pyloric biopsy confirm the validity of using ISH for histological detec- tion of mitochondria. The present study illustrates how
REFERENCES
1. Pavlakis SG, Phillips PC, DiMauro S, De Vivo DC, Rowland LP. Mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes: a distinctive clinical syndrome. Ann Neural 1984, 16: 481 488.
2. Goto Y, Nonaka I, Horai S. A mutation in the tRNALe"(UUR' gene associated with the MELAS subgroup of mitochondrial encephalopathies. Nature 1990; 348: 651-653.
3. Goto Y, Nonaka 1, Horai S. A new mtDNA mutation associated with mitochondria] myopathy, encephalopathy, lactic acidosis. and stroke-like episodes (MELAS). Biochim Biophys Acta 1991; 1097: 238-240
4. Alcolado JC, Majid A, Brockington M, el al. Mitochondrial gene defects in patients with NIDDM. Diabetologia 1994: 37: 372-376.
5. Kadowaki T, Kadowaki H, Yasumichi M, rt a/. A subtype of diabetes mellitus associated with a mutation of mitochondria1 DNA. N Eng[ J Med 1994; 330 962-968.
6. Suzuki S, Hinokio Y, Hirai S, ef a/. Pancreatic p-cell secretory defect associated with mitochondrial point mutation of the tRNAL'"(lJ"R' gene: a study in seven families with mitochondrial encephalomyopathy, lactic acidosis and stroke-like episodes (MELAS). Diohetologia 1994; 37: 818-825.
7. Van den Ouweland JMW, Lemkes HHPJ, Trembath RC, et a1 Maternally inherited diabetes and deafness is a distinct subtype of diabetes and associated with a single point mutation in the mitochondrial tRNALen(UL'R) gene. Diabetes 1994; 43 746-751.
8. Love S, Nicoll JAR, Kinrade E. Sequencing and quantitative assessmeiit of mutant and wild-type mitochondrial DNA in paraffin sections from cases of MELAS. .I Pafhnl 1993; 170 9-14.
9. Li V, Hostein J, Romero NB, ef 01. Chronic intestinal pseudoobstruction with myopathy and ophthalmoplegia. A muscular biochemical study of a niitochondrial disorder. Dig Dis Sci 1992; 37: 456463.
10. Simon LT, Horoupian DS, Dorfman LJ, Herrick MK, Wassei-stein P, Smith ME. Polyneuropathy, ophthalmoplegia, leukoencephalopathy, and intesti- nal pseudo-obstruction: POLIP syndrome. Ann Nrurol 1990, 2 8 349-360.
1 I . Hirano M, Silvestri G, Blake DM, et a/. Mitochondrial neurogastrointesti- nal encephalopathy (MNGIE): clinical, biochemical, and genetic features of an autosomal recessive mitochondrial disorder. Neurology 1994; 4 4 721- 127.
12. Liou CW, Huang CC, Chee ECY, et a/. MELAS syndrome: correlation between clinical features and molecular genetic analysis. Acta Neurol S a n d 1994; 9 0 354-359.
13. Macmillan C, Lach B, Shoubridge EA. Variable distribution of mutant mitochondrial DNAs (tRNALc"'324") in tissues of symptomatic relatives with MELAS. the role of mitotic segregation. Neuralugy 1993; 43 1586- 1590.
14. De Vries D, De Wijs I, Ruitenbeek W, et a/. Extreme variability of clinical symptoms among sibs in a MELAS family correlated with heteroplasmy for the mitochondrial A3243G mutation. J Neuroi Sci 1994: 124 77-82.
15. Matthews PM, Hopkin J, Brown RM. Stephenson JBP, HiltonJones D, Brown GK. Comparison of the relative levels of the 3243 (A-G) mtDNA mutation in heteroplasmic adult and fetal tissues. J Mrd Gene! 1994; 31: 4 1 4 4 .
16. Hamazaki S, Koshiba M, Sugiyama T. Organ distribution of mutant mitochondrial tRNAL'"'"UR' gene in a MELAS patient. Acra Pothol Jpn 1993; 4 3 187-191.
17. Martinuzzi A, Bartolomei L, Carrozzo R, et al. Correlation between clinical and molecular features in two MELAS families. J Neurd Sci 1992; 113 222-229.
IS . Shoji Y, Sato W, Hayasaka K, Takada G. Tissue distribution of mutant mitochondrial DNA in mitochondrial myopathy. encephalopdthy, lactic acidosis and stroke-like episodes (MELAS). J lnher M w i h Di.s 1993; 16: 27-30.
19. Miaukami K, Sasaki M, Suzuki T, et al. Central nervous system changes in mitochondria1 encephalomyopathy: light and electron microscopic study. Acta Neurriparhol 1992; 83: 449452.
20. Ohama E, Ohara S, Ikuta F, Tanaka K, Nishizawa M, Miyatake T. Mitochondrial angiopathy in cerebral blood vessels of mitochondrial encephalomyopathy. Acta Neuroputhol 1987; 7 4 226--233.
21. Sat0 W, Tanaka M, Sugiyama S, r f a/ . Cardiomyopathy and angiopathy in patients with mitochondrial myopathy, encephalopathy, lactic acidosis, and strokelike episodes. Am H a r t J 1994; 128: 733-741
22. Hasegawa H, Matsuoka T, Goto YI, Nonaka I . Strong succinate dehydrogenase-reactive blood vessels in muscles from patients with mito- chondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes. Ann Neurol 1991; 2 9 601-605.
23. Tokunaga M, Mita S, Sakuta R, Nonaka I , Araki S. Increased mitochon- drial DNA in blood vessels and ragged-red fibers in mitochondrial myop- athy, encephalopathy, lactic acidosis, and stroke-like episodes (MELAS). Ann Nrurol 1993; 33: 275-280.

ISH T O MITOCHONDRIA IN MELAS AND CEREBRAL INFARCTS 189
24. Kishi M, Yoshinori Y, Kutihard T , er r r l . An autopsy case of mitochondrial encephalomyopathy: biochemical and electron microscopic studies of the brain. J Neurol Sci 1988; 86 3 1 4 0
25. Foster C, Hubner G, MullerHocker J, el crl. Mitochondria1 angiopathy in a family with MELAS. .Ywropediorrics 1992; 2 3 165-168.
26. Nicoll JAR, Moss TH, Love S , Campbell MJ, Schutt W H . Clinical and autopsy findings in two cases of MELAS presenting with stroke-like episodes but without clinical myopathy. Clin Ncuruputhol 1993; 1 2 38--43.
27. Hilton DA, Love S, Goodwin T. Pringle JH. Demonstration ofmitochoii- drial ribosomal RNA in frozen and parafin-embedded sections of skeletal muscle by in ,siiu hybridization. Neciroiiiiilir~l Appl Nmrohiol 1994; 2 0 573 -576.
28. Hilton DA, Variend S. Pringle JH. Demonstration of Coxsackie virus RNA in formalin-tixed tissue sections from cases of childhood myocarditis by in riru hybridisation and the polymerase chain reaction. J Pulhol 1993; 170 45-5 I .
29. Hiltoii DA, Love S, Fletcher A, Pringle JH Absence of Epstein-Barr virus RNA in multiple sclerosis as assessed by iu ritu hybridisation. J Nmrol Neurosurg P.syr,hirrtrj 1994; 57: 975-976.
30. Ooiwa Y, Uematsu Y, Terada T, et ul. Cerebral blood flow in mitochondrial myopathy, encephalopathy, lactic acidosis, and strokelike episodes. Stmkr I 993; 2 4 30&309.
31. Gropen TI, Prohovnik 1, Tatemichi TK, Hirano M . Cerebral hyperemia in MELAS. Stroke 1994; 2 5 1873-1876.
32. Heffner RR, Barron SA. The early effects of ischemia upon skeletal muscle mitochondria. J Neurol Sci 1978; 3 8 295-31 5.
33. Rernik M. Aspect ultrastructural de la degenerescence du muscle strik ischkmie. Ann Anut Pathol 1967; I2 209-222.
34. Karpati G, Carpenter S, Melmed C , Eisen AA. Experimental ischemic myopathy. J NeurulSci 1974; 23: 129-161.
35. Yoneda M, Chomyn A, Martinuzzi A. Hurko 0. Attardi G. Marked replicative advantage of human mtDNA carrying a point mutation that causes the MELAS encephalopathy. Pro< Nrril Arm/ Sci USA 1992; 89: 1 1164-1 1 168.
36. Tokunaga M. Mita S, Murakami T, e l al. Single muscle tiber analysis of mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes (MELAS). Ann Neural 1994; 35: 413-419.
37. MullerHocker J, Hubner G, Bise K , rt ul. Generalized mitochondrial microangiopathy and vascular cytochi-ome c oxidase deficiency: occurrence in a ca5e of MELAS sviidroine with mitochondrial cardiomvonathv-
, 1 i
myopathy and combined complex I l l V deficiency Arth Pnthol Lah Med 1993; 117: 202-210