Embed Size (px)
Citation preview

270333
1
Method or Madness?
Research and planning folder

270333
2
Contents
The Public Lunatic Asylum: ‘Bedlam’
19th Century Treatments
A History of Schizophrenia
Character Research
Characterisation
Seminar & Workshop Material
Plot & Story
Bibliography
270333
3
- The Public Lunatic Asylum-
The Birth of the Asylum
Institutions for the insane can be traced back thousands of years as early as the 5th Century. These
buildings acted as prisons to house the mentally ill, where patients would be chained, beaten or killed
to remove them from society. It wasn’t until the 18th and 19th centuries that society became more
interested in the causes of mental illness, and special buildings called madhouses were constructed to
house the mentally insane. Despite these new institutions there was little change in the treatment of
patients, who continued to be beaten and treated like animals chained to walls and used as a form of
entertainment for the wealthier social classes.
During the turn of the nineteenth century, attitudes towards the mentally ill changed drastically.
The Enlightenment provided technological advancements in society, particularly in science and
medicine, which helped people to see lunacy as a condition that could be treated, and therefore began
the reformation of madhouses across the country. The Lunacy Reform Act 1845 enforced an
improvement in the treatment of insane patients, and transformed London’s madhouses into public
lunatic asylums. These new asylums provided slightly better living conditions and advancements in
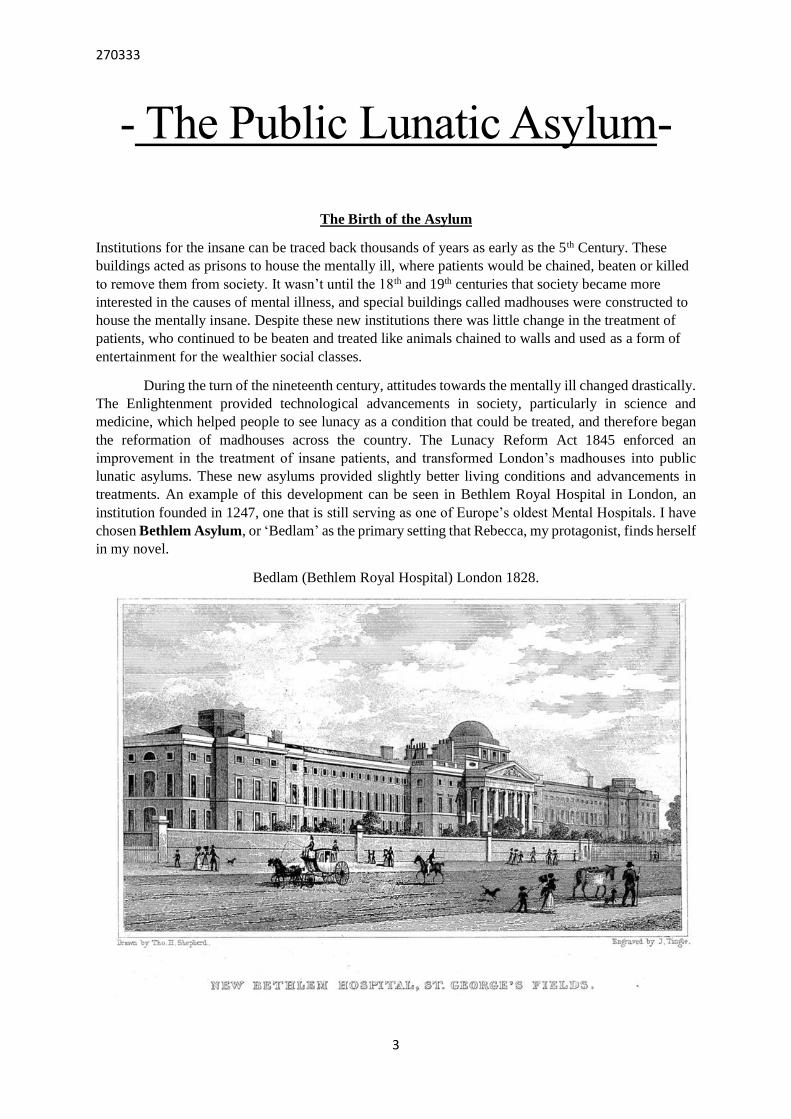
treatments. An example of this development can be seen in Bethlem Royal Hospital in London, an
institution founded in 1247, one that is still serving as one of Europe’s oldest Mental Hospitals. I have
chosen Bethlem Asylum, or ‘Bedlam’ as the primary setting that Rebecca, my protagonist, finds herself
in my novel.
Bedlam (Bethlem Royal Hospital) London 1828.

270333
4
Map of Bethlem Hospital in London now (2016)

270333
5
Bethlem Hospital circa 1850
Below is a map of Bethlem Hospital in London in 1850. It first opened as a hospital in 1330,
to house the criminally insane. In 1828, it was moved to St George’s Fields where it became a
public lunatic asylum, specialising in the treatment of the mentally ill.
This small, circular building is Bethlem Royal Hospital after it had been
moved from its original location, to St. George’s Fields.

270333
6
Diagram of Bethlem Hospital circa 1850:
‘The whole building (the House of Occupations included) covers, it is said, an area of 14
acres.’
From this diagram, we can see that the male and female patients were situated on opposite sides
of the complex, probably to avoid contact with one another. There are a number of courtyards
available for the female patients, suggesting that they were allowed outside of their cells and
could interact freely with other patients.
The female patient airing ground is where Rebecca will meet Jane, and is one of the
places where the two characters will discuss their plot to escape the asylum. The key at the
bottom of the image indicates the different rooms available to the patients for example, the day
room which indicates that patients were moved from room to room, which is where Rebecca
will write her diary entries.

270333
7
Internal Layout of Bethlem Hospital in 1816:
Although this diagram was printed forty years prior to the setting of my novel in 1854, it
displays the names of some of the staff that worked within the asylum, as well as displaying a
‘friends room’ where patients were allowed to visit their friends. I will use this in my novel as
a place that Rebeeca and Jane will spend most of their free time together when they are not
working in the Laundry room, or receiveing treatment.

270333
8
Daily Life in the Asylum
Despite the implementation of the Lunacy Reform Act in 1845, there was no noticeable change
in the treatment of the mentally ill until the late nineteenth century. Many asylums continued
to restrain their patients as a form of treatment, where they would beat them into submission if
they were uncooperative. Patients were forced to live in unsanitary conditions, in cramped cells
which only enhanced the severity of their illnesses. It wasn’t until the end of the nineteenth
century that mental illness was taken more seriously.
https://www.youtube.com/watch?v=EtgzpAbxcRI
As a part of daily life in an asylum, patients were allowed outside for fresh air and exercise.
This comment from a Lunacy Commission Inspector at Norfolk County Asylum in 1854,
shows the level of control that was enforced when they were let out of their cells. One of the
methods used to control the patients were the drills exercised by the nursing staff. These drills
were part of the patient’s daily routines and were crucial as they ensured order in an
otherwise chaotic and unpredictable environment:
"Great control is gained over the patients and the task of taking a vast number …for air and
exercise, becomes comparatively easy.”
(Female Patients Exercising in the Metropolitan Lunatic Asylum)

270333
9
Fresh air and exercise were part of a strict and organised routine for the patients in
asylums from the mid nineteenth century. In some institutions, female patients would be woken
up at a certain time where they would then be washed and have their hair brushed, before being
examined for medical purposes. There was also a specific time that the patients were put to bed
by the nursing staff. In the early 20th century, the beds were just as organised as the patients
themselves, being arranged in long lines exactly two feet and six inches apart.
Towards the end of the 19th century, patients had to work as part of their rehabilitation,
either in nearby workhouses, or if they were lucky, within the asylum itself. Domestic jobs
such as washing and drying laundry, cooking, and cleaning were all common tasks for patients,
which was believed to help with their condition.

270333
10
Extract from a report of Bethlem Hospital in 1844:
1844 Bethlem Hospital, St George's Fields, South London.
1.1.1844: 355 patients of whom 90 were criminals.
Bethlem was outside the Metropolitan Commission's investigative authority. For statistical
purposes:
"In the absence of any specific information ... we have entered the Criminal Lunatics ...
seventy Males and twenty Females, as Paupers. We have also assumed that the remainder
of the Patients ... generally, are of Private class, although we have reason to believe that
some of them are maintained, wholly or in part, at the charge of Unions or Parishes" (1844
Report p.186)"
This report indicates the number of patients
admitted to Bethlem during 1844, giving me an idea of how
many patients would have been housed within the asylum
at one time. The patients were divided up into categories to
keep the violent and dangerous patients from harming
themselves or others.
This particular report indicates that in 1844 the two
main categories of patients included Criminal Lunatics,
Paupers, and Private Class Lunatics. In my novel, both
characters, Rebecca and Jane, will be placed in the Private
Class category, the larger and less violent of the three listed
in the above report.
Harriet Jordan in her Bethlem
Royal Hospital portrait, newly
diagnosed with acute mania.
(1856)

270333
11
Payin
g fo
r Trea
tmen
t
‘The o
ne sig
nifica
nt d
evelopm
ent in
adm
issions
to B
ethlem
Hosp
ital in
the V
ictoria
n era
had
been
a m
id-cen
tury sh
ift aw
ay fro
m a
dm
itting
paupers (fo
r who
m th
e new
county lu
natic
asylu
ms w
ere thought to
cater) in
favo
ur o
f
patien
ts of th
e mid
dle a
nd skilled
labourin
g
classes’. (“
Presu
med
Cura
ble”
p.5
)
In
my
no
vel.
Reb
ecca’s w
ell ed
ucated
back
gro
und is b
ased o
n th
e assertion th
at durin
g
the 1
9th C
entu
ry, B
ethlem
Hosp
ital acted as m
ore
of a p
rivate in
stitutio
n fo
r upper class p
atients,
with
wealth
y fam
ilies. The ch
aracters of Jan
e and
Reb
ecca are exam
ples o
f patien
ts that co
me fro
m
wealth
y b
ackgro
unds an
d are w
ell educated
. This
is dem
onstrated
in th
e book P
resum
ed C
ura
ble
by
Colin
G
ale an
d
Robert
How
ard,
that
discu
ss
Beth
lem A
sylu
m d
urin
g th
e 19
th Cen
tury
.
‘Fro
m 1
882 o
nw
ard
s, patien
ts’ relatives w
ho w
ere
willin
g to
pay to
secure a
pla
ce at B
ethlem
contrib
uted
two g
uin
eas a
week to
ward
s the co
st of
care’. (“
Presu
med
Cura
ble”
p.5
)
In m
y research
I disco
vered
that a p
atient’s fam
ily
had
to p
ay fo
r care in th
e asylu
m. A
s a result,
Reb
ecca’s husb
and, Jam
es Rusw
ick, w
ill be sh
ow
n
to p
ay th
is two g
uin
ea contrib
utio
n to
keep
Reb
ecca
in th
e asylu
m after h
e reports h
er as bein
g m
entally
unstab
le. The n
ovel b
egin
s with
a signed
letter to th
e
asylu
m fro
m M
r Rusw
ick, to
confirm
the p
aym
ent
for R
ebecca’s co
ntin
ued
treatmen
t in th
e asylu
m,
illustratin
g th
at

270333
12
-Treatments-
Psychiatric treatment undertook a dramatic change during the nineteenth century. It was believed that
mental illness was a kind of state of the soul, at a time when religion had a ruling influence on the
common people. Towards the mid nineteenth century, scientists began to take a deeper interest into the
human mind, and through the technological advancements of the industrial revolution between 1820-
1840, treatment of the mentally ill became the primary focus for psychologists in the field of psychiatry.
Up until the 1870’s, treatment of the mentally ill can be described as barbaric and inhumane.
Asylum staff treated patients like animals, often confining them in cages, or animal pens where they
would be abused by staff, or viewed by visiting citizens for entertainment as seen in the picture below.
(Patients being viewed by paying citizens as a form of entertainment)

270333
13
Restraint
These pre 1850 images shows patients being chained to the walls whilst being observed by
visitors to the asylum as they suffer for profit. It was seen as a common spectacle for the wealthy
to watch the inmates as a form of entertainment.

270333
14
The primary method for maintaining control within asylums up until the 1850’s was restraint. Prior to
the Lunacy Reform act, patients were most commonly chained to the wall, or to their beds with very
little freedom to move around. Solitary confinement, straight-jackets, ice baths, and machinery such
as the restraint chair were all methods that restrained the patient to keep them calm, quiet and away
from society.
(Restraint Chair Circa 1850)
The Restraint chair was used as a ‘humane’
alternative to the straight jacket.
Chaining patients to objects was another
method of restraint used prior to 1850. In the
picture below the patient’s hands, feet and
neck are chained to the pole, restricting any
freedom of movement.

270333
15
(The Ice Bath or ‘Surprise’ Bath)
Patients would be stripped of all their clothes and told to lay in a bath, where freezing buckets of water
would be dropped onto them from above and when full, would be left to sit in it for hours. It was thought
that this would shock the patient and cause any confusion or illness to be shaken away. This of course
didn’t work, and instead caused many of the patients to die of hyperthermia.
(Straight Jacket)
Invented in 1790, the straight jacket was the
most common method of restraint within
asylums and mental institutions. These
jackets were often used on patients who
could not control themselves and were either
a danger to themselves or others. The
patient’s arms would be inserted into the
sleeves which were then crossed across the
chest. The ends of the sleeves are then tied to
the back of the wearer, ensuring that the arms
are kept close to the chest with as little
movement as possible, preventing the patient
from moving their upper body.

270333
16
(Straight Jacket)
(Restraining Belt)
(Hand mitts - used in
asylums to prevent from
patients who would tear
their clothes off, or self-
abuse)
(Neck Restraint)
(Belly Chains)
(Cuffs)
(Restraint Harness)
Below are some images of the various types of
physical restraints used in insane asylums:

270333
17
Lobotomy
"It seems possible that with additional experience and a minute study of the pathologic changes seen
in the brain, the knife may be the means of restoring to reason many cases now considered
incurable"
--Emory Lamphear (1895)
Following technological advancements of the enlightenment, the understanding of mental illness
started to improve, with a rapid growth of interest from a scientific perspective and an increase of
available treatments. These included lobotomy, which involved drilling two holes into either side of
the skull where the patients, in earlier treatments, remained conscious during the procedure.
Although the term ‘Lobotomy’ wasn’t introduced until the 20th century, surgical manipulation
of the brain was being used in asylums as early as the 1880’s. A Lobotomy was a surgical procedure
in which the nerve pathways in a lobe or lobes of the brain were severed from those in other areas.
The procedure was formerly used as a radical therapeutic measure to help grossly disturbed patients
with schizophrenia, manic depression and mania. The practice gradually fell out of favour beginning
in the mid-1950s, when medication such as antipsychotics and antidepressants came into use which,
were much more effective in treating and alleviating the distress of mentally disturbed patients.
This diagram illustrates a
frontal lobotomy. The surgeon
would drill into the skull, or
pierce the brain through the
nasal passage or from behind
the eye.

270333
18
Trepanning
As a predecessor to a Lobotomy, Trepanation was a method used before and during the 19th century.
This is an ancient procedure in which a hole is drilled or scraped into the human skull, exposing
the dura mater, to treat health problems related to intracranial diseases.
The instrument used for
trepanning was called
a trephine. It is a screw-like
device that the surgeon would
turn, rotating a sharp metal
point at the end of the device.
This action would cause the
point to pierce the skin and cut
out a round piece of skull bone,
as demonstrated in the above
diagram.
Trepanation is still used
in practises of modern day
medicine as a method of
accessing other parts of the
body that are otherwise
unreachable. However, it is no
longer used to treat mental
illness, and is a procedure that
is much more humanely
performed.

270333
19
Insulin Shock Therapy
During my research into this treatment, I discovered that the introduction of Insulin Shock
Therapy didn’t start until the 1920’s, much later than I had first anticipated when planning
my novel. As Rebecca’s Insulin treatment is a vital to the plot, I have decided to change the
date in which the novel was set from 1854 to 1884. Although this is still some years behind its
introduction, I aim to present this treatment in my novel as a one of the first private
experiments of a new, unknown drug, which would later (in the 1920’s) become known as
Insulin. As a result, the effects of the drug will be unknown to science at the time and
therefore no guideline will exist as to how it should be administered to a patient. Rebecca,
therefore, will experience a similar treatment to what we now understand to be Insulin Shock
Therapy, but with methods that differ from how it was administered in the 1940’s.
Insulin Shock Therapy, or Insulin Coma Therapy as it was more commonly known
(ICT), was a psychiatric treatment that was introduced in the 1920’s. It was used extensively
in the 1940’s as a treatment for schizophrenia and other mental illnesses. The patient would
be repeatedly injected with large doses of insulin in order to produce daily coma’s lasting up
to several weeks. This form of treatment fell out of favour in the 1960’s when neuroleptic
drugs were introduced, which calmed the patient much more effectively.
During the 1950’s, patients suffering from Schizophrenia required great physical
strength and good prognosis in order to be selected for the treatment. The procedure required
specialist staff as it was a labour intensive treatment, and there were no standard guidelines
for them to follow; different hospitals and psychiatrists developed their own protocols. In my
novel, Rebecca is the first person to be administered this treatment as a form of private
experimentation by one of the doctors in the asylum, Victor Porter. He performs the
injections himself, without any specialist unit, using the restraint chair and other restraint
devices which prevent her from moving, especially during the first few days of her treatment
where she attempts to resist. The low glucose levels that resulted from ICT made patients
extremely restless, sweaty, and liable to after-shocks. In the most severe cases, some patients
were known to suffer from brain damage, and others died from their induced comas.
Brass Ear Syringe (1880)
(Lapinlahti Psychiatric Hospital, Helsinki, 1950)
270333
20
-Schizophrenia-
In this section I will talk about the condition of Schizophrenia. Schizophrenia is a condition
that was not officially named as an illness until 1913 by German physician, Eugen Bleuler.
Early 20th century patients who were associated with abnormal social behaviour and the
failure to understand reality were diagnosed with schizophrenia.
In my novel, set in 1884, Rebecca begins to develop Paranoid Schizophrenia, a condition
which, at the time, had not yet been named as its own illness. As a result, the condition of
Schizophrenia that Rebecca develops will not be named as such at any point in the novel, and
the staff within the asylum will lack any understanding of the condition.
In my research into Schizophrenia, I found that five types of the condition were delineated in
the Diagnostics and Statistics Manual III in 1952:
• Disorganized: ‘These reactions are characterized by conspicuous motor behaviour,
exhibiting either marked generalized inhibition (stupor, mutism, negativism and waxy
flexibility) or excessive motor activity and excitement. The individual may regress to
a state of vegetation.’
• Catatonic: ‘The subject may be almost immobile or exhibit agitated, purposeless
movement.’
• Paranoid: ‘This type of reaction is characterized by autistic, unrealistic thinking, with
mental content composed chiefly of delusions of persecution, and/or of grandeur,
ideas of reference, and often hallucinations.’
• Residual: ‘This term is to be applied to those patients who, after a definite psychotic,
schizophrenic reaction, have improved sufficiently to be able to get along in the
community, but who continue to show recognizable residual disturbance of thinking.’
• Undifferentiated: ‘The chronic schizophrenic reactions exhibit a mixed
symptomatology, and when the reaction cannot be classified in any of the more
clearly defined types, it will be placed in this group. Patients presenting definite
schizophrenic thought, affect and behaviour beyond that of the schizoid personality,
but not classifiable as any other type of schizophrenic reaction, will also be placed in
this group.’
As Rebecca has vivid hallucinations, she falls into the category of Paranoid
Schizophrenia. I will use the above definition of paranoid schizophrenia as a baseline, when
trying to convey Rebecca’s hallucinations in the asylum and her deteriorating mental state.

270333
21
Below are a collection of drawings from various patients suffering with Schizophrenia:
A series of paintings of cats by Louis Wain from the early 1900's. They capture a slow descent into varying levels of schizophrenic
episodes.
Drawn by Edmund Monsiel, an artist
in the early 1900's believed to have
been a schizophrenic.
‘A depiction of the affliction’ of
Schizophrenia by Erik Baumann.

270333
22
Paranoid Schizophrenia
Paranoid Schizophrenia is the most common type of Schizophrenia, and people who are diagnosed with
this sub-type often seem more ‘normal’ than other schizophrenics. Some of the symptoms associated
with a paranoid schizophrenic are delusions and hallucinations, or an in-ability to distinguish between
fantasy and reality. Rebecca experiences visual and auditory hallucinations from her time within the
asylum which develop from her exposure from her insulin treatment. Despite the advancements in
modern day science and medicine, phycologists have yet to determine the cause of schizophrenia; it is a
completely unpreventable illness.
(This drawing was found in an old asylum; the artist was a paranoid
schizophrenic)
Here is a list of reasons for admission into an
asylum in the 19th century:
There is no classification that fits Schizophrenia,
and as a result shows that the condition didn’t
exist.
Although Rebecca develops the symptoms of a
paranoid schizophrenic, she is not diagnosed with
the condition. Instead she is experimented on with
various types of treatments that have never before
been practised by science. In my novel, Rebecca
will act as one of the first patients to be
experimented on, which will, eventually, lead to
the discovery of Schizophrenia and Insulin
Therapy as a form of treatment for the condition.

270333
23
-Character Research-
Nineteenth Century Clothing
Women:
19th Century clothing changed dramatically throughout the period. This change was
influenced by shifts in taste and by the introduction of machines used in the construction of
clothing. Sewing and weaving machines, steam power, electricity, new dye formulas, and
other inventions increased the speed and ease of clothing manufacture. These inventions were
used to add embellishments to women's clothing and allowed more illustrious styles of dress.
The pictures below demonstrate the types of clothing women used to wear during the 19th
Century, either for domestic or social purposes:
At the beginning of the century, women wore dresses that were much slimmer and more tightly
fitted. By the 1850’s it was fashionable for women to have very small waists, and so they wore
corsets to hold the shape of the dress and seem slimmer than they actually were. By this time,
dresses had become larger, and more elaborate, with several different sleeve styles for different
parts of the day. Short puffed sleeves were generally worn during the evenings, and longer
sleeves for casual wear during the day. During the late 1890’s the bulky style of dress fell out
of fashion, in favour of a more loosely cut finish. This artistic style gave more freedom of
movement, and as a result did not require corsetry to be worn.
(1850)
Mid- 19th Century dresses
included whale bone or steel
wire frames, giving the dress a
bell-like shape, defining the
waistline.
(1850)
(1885)
Late 19th Century dresses
included a bustle instead of a
frame. This caused the dress
to bulge outwards at the back.
(1825)
Early 19th Century dresses were
longer and slimmer. Corsets were
worn underneath the dress that were
tightened in order to define the
waistline, making women appear very
slim.

270333
24
Below is a timeline of diagrams that show the transformation in women’s fashion during the
19th Century:

270333
25
Men:
By the early 19th Century men's fashion had also changed. Men generally wore an undershirt
with a waistcoat, and a coat finished in long tails at the back. Throughout the period, it was
uncommon for a man to go out in public without wearing a hat. In the early 1800’s, men wore
a variety of hats to match the fanciful designs of their shirts and jackets. However, in the later
years, the low black hats that were worn at the beginning of the century would evolve into
top-hats that continued to be worn right through into the early 20th Century.
In the early 19th Century some men wore boned corsets to give them a small waist,
but in later years they wore less layers of clothing and longer jackets to give a looser fit.
Alongside their tight waistcoats and jackets, men wore breeches, although these gradually fell
out of fashion when they were all but replaced by trousers. At first, trousers were only worn
during the day and for informal dress, however, by the 1820s they were acceptable for
evening wear as well. During the second half of the century, waistcoats and jackets were still
in fashion, though men’s jackets had become longer and less styled. In the late 19th Century,
men wore plain dark jackets with high-collared shirts and vests. The colour black was
becoming increasingly fashionable, giving a smarter, cleaner look to a man’s appearance,
with less fanciful designs.
(1840)
Mid- 19th Century clothing had
changed slightly from men’s
earlier fashion. The outfit was less
fanciful and men wore trousers
rather than breeches, which were
only worn in court.
(1890)
At the end of the 19th, early 20th
Centuries, every aspect of a man’s
appearance was much plainer, with
black top-hats and longer coats. This
new suit-like appearance made men
look cleaner and smarter in
comparison to early 19th Century
clothing, with a more loosely fitted
outfit.
(1805)
Early 19th Century clothing for
men, consisted of frilly, open-
neck shirts and tight breeches.
This fancy style of clothing was
also introduced into a man’s
jacket, which was cut-off at the
front and separated at the back.

270333
26
Character Inspirations
In order to widen my understanding of the behaviourisms of patients with mental illness, and
the ways in which doctors diagnosed conditions during the 19th Century, I have based Jane
and Rebecca’s behaviours around actual patients that were admitted to Bethlem Hospital in
the late 19th Century (available from book: “Presumed Curable” by Colin Gale and Robert
Howard).
Mary Robertson
‘Mary Robertson’ was admitted to Bethlem on 28th April 1895.
(Doctor’s report for Mary Robertson)
Rebecca’s character, based on Georgina Hewett (1892). Inspired character traits:
• Hallucinations (both auditory, and visually)
• Restlessness
• Inability to sleep properly
‘Patient imagines herself to have been
hypnotised. She declares she hears
voices, and instances one as saying that
her brother has been shot and also calling
her by name. I am informed by Miss Mary
Sturge that patient describes herself as
imagining she was followed and
persecuted in the streets last autumn. Also
that she is alternately apathetic (with head
on bed or hands over her eyes) and
restless. Also that she gets out of bed
continually at night declaring that voices
are saying in the street that her brother is
dead.’
Dr Jane Harriet Walker
(p.106)
‘She confessed to hearing voices
which order her to do various acts. To
seeing forms and faces, some pleasant
and some horrible. To believing in
these voices and faces as facts. She is
greatly altered in expression of face, in
manner and in type of conversation.
Miss Mary Darby Sturge MB, house
surgeon, New Hospital for Women,
says that Mary H. Robertson is unable
to concentrate her thoughts or to read
because of the voices which constantly
haunt her. Also she declares she has
been hypnotised (which is not the
case). She says that there must be
electricity in the ward which acts in
her.’
Dr Mary Ann Dacomb Scharlieb
(p.106)

270333
27
Georgina Hewett
‘Georgina Hewett’ was another patient admitted to Bethlem Hospital on 3rd November 1892.
(Doctor’s report for Georgina Hewett)
The character of Jane Harrington, based on Georgina Hewett (1892). Inspired character traits:
• Bad language
• Incoherent rambling
• The way in which she starves herself
‘She cannot converse in a rational
manner. She will not answer questions.
She chatters continuously in an
incoherent rambling and garrulous way.
Spoke of her mother as a devil. She seems
quite unable to take care of herself. Her
mother, Mrs Jane Hewett (widow),
informs me that yesterday the patient
exposed herself at the window in a state
of nudity and that she has been for some
time unable to manage herself and her
affairs.’
Dr Francis John Roberts Russell
(p.72)
‘Her manner was excited; she keeps
talking nonsense. She made grimaces
at me and said that I had been
‘Kodaked’ by her. She also said that
she had been starved. Alice Hewett,
sister, says that she dresses up in
fantastic dresses, that she exposes
herself at the window in scanty dress,
that she uses bad language.’
Dr Edward Rosser Mansell
(p.72)

270333
28

270333
29
Novel Summary
The novel is focused around one character, Rebecca Ruswick and her experience of Bethlem
Asylum in 1884. Following a tragic accident on the family estate involving her young daughter, Eve,
Rebecca is condemned by her husband to live out her days in the asylum. It is here that Rebecca
begins treatment to cure her condition, though for much of her time in the asylum she is experimented
on and she begins to lose her mind.
She meets an anorexic, upper class woman called Jane Harrington and the pair have a lot in
common and become close very quickly. Rebecca is treated for, what is diagnosed as, Chronic Mania
and records her thoughts and experiences in a series of diary entries, which gradually become more
and more irrational. With the thought of her daughter constant on her mind, she becomes desperate to
see her daughter before she passes away and attempts to escape the asylum with Jane. Upon the day of
the escape Rebecca experiences various forms of hallucinations and it becomes almost impossible for
the reader to distinguish if what Rebecca is seeing is in fact reality; revealing symptoms of developing
schizophrenia.
With Jane’s help she manages to escape the asylum and begins her journey to the Ruswick
Estate. Once inside the house Rebecca moves upstairs and sees her husband watching over their
daughter. Determined that nothing will stop her seeing her daughter again, she sneaks up behind him
and, unware she is in the house, vengefully kills him. She enters the bedroom and is re-united with her
daughter, discovering she wasn’t too late after all.
The Accident
The accident involving Eve happened one day in February 1884. Rebecca and Eve were waking down
by the lake on the estate, as they did every morning. There was a swing that hung from one of the
ancient willow trees that loomed over the lake. On that particular morning, whilst Eve was playing on
her swing, the branch of the willow tree snapped, sending her tumbling into the icy water. Rebecca
remembers how helpless she was, trying to pull her daughter from beneath the heavy branch and
thickening mud, which was pushing her further under as she struggled to get free. Rebecca shouted
for help to free her, and eventually they carried Eve to the house. The branch had fallen on her head,
putting her in a temporary coma, but due to the freezing temperature of the water and

270333
30
- Characterisation -
Character Profiles
Name: Rebecca Jade Ruswick (Protagonist)
Age: 28 Gender: Female
Born: 4th August 1856 Marital Status: Upper-social class, Married.
Place of Birth: London, England. Date Admitted to Asylum: 17th February 1884.
Goal: To escape the asylum and get back to her daughter before she dies.
Conflict: Her doctor, Victor Porter, experiments on her throughout her time at the asylum.
His methods cause her to develop hallucinatory, and delusional symptoms that we now
associate with Paranoid Schizophrenia.
Motivation: Rebecca’s daughter, Eve, has fallen into a coma and only has a few weeks to
live. Rebecca has to race against time and the legitimacy of her own mind to escape the
asylum, and become reunited with her daughter before she dies.
-Mannerisms- (up until her delusions and hallucinations begin):
Generally quiet, unless spoken to, in which case she appears sophisticated and well-
mannered. Has all the typical values expected of a Victorian woman, well-spoken, educated,
dutiful and faithful. Lacks the confidence to express herself to her husband, whom she is
devoted to.
Excited: slight smile, attempting to conceal her feelings.

270333
31
Nervous: becomes restless, overthinks the situation and acts rashly.
Lonely: silent and reclusive in person, though likes to express her feelings on paper.
Sad: tearful, clenches her hands together.
Scared: eyes widen and begin to water, mouth closed.
Surprised: eyes widen, mouth open.
-Physical Attributes-
Hair colour: Dark Brown Body Type: Slim
Hair Style: Long/Usually in a bun Height: 5 foot 4inches
Eyes: Green Weight: 49kg (110 Pounds)
Perfectly proportioned facial features, very pretty. Usually wears her hair in a bun, though it
is cut shorter when she arrives at the asylum. There are a few light brown freckles on her
lower cheeks and she has a birthmark on her back that she is very conscious of.
Background Information:
Rebecca grew up as an only child following the death of her brother when she was very
young. Born in London in 1856, she lived with her parents until she met James Ruswick at
the age of 18. They were married a few months later, and moved to James’ father’s estate on
the outskirts of London after his unexpected death. Aged 22, Rebecca fell pregnant and some
months later gave birth to their daughter Eve. The story begins six years later, when her
husband James, condemns Rebecca to Bethlem Asylum following a tragic accident on the
estate involving their daughter Eve.

270333
32
Name: Jane Annabelle Harrington (Rebecca’s closest friend in the asylum)
Age: 34 Gender: Female
Born: 23rd October 1850 Status: Upper class, Married.
Place of Birth: Sussex, England. Date Admitted to asylum: January 2nd 1882
-Mannerisms-
Confident and outspoken. Has been well educated and is unafraid to speak her mind. Is
completely insane by the time Rebecca is admitted to the asylum, and so she is extremely
unpredictable. Is diagnosed with chronic Mania due to her frantic and aggressive behaviour.
Sympathetic towards Rebecca, and trusts no one else. Secretive. Knowledgeable of
happenings within the asylum, and uses this knowledge to help Rebecca escape.
Excited: laughs uncontrollably. .
Nervous: taps her feet together and starts humming softly to herself.
Lonely: appears very distant.
Sad: has aggressive outbursts, including the use of bad language.
Scared: likely to have violent outbursts, hitting scratching and biting.
Surprised: she interprets surprise as being scared; and responds accordingly.
-Physical Attributes-
Hair Colour: Dark Brown Body Type: Anorexic
Hair Style: Short/Curly Height: 5 foot 2inches
Eyes: Hazel Weight: 33kg (73 Pounds)
270333
33
Dangerously skinny when she first arrived. Slowly recovering some weight. Deceptively
strong for a woman who is so skinny. Fingernails were all but removed from scratching the
nursing staff in one of her outbursts. Despite its scraggily appearance, she is proud of her hair
and the similarity in colour between their hair is the reason Jane approaches her in their first
meeting.
Background Information:
Jane used to be very similar to Rebecca before being admitted to the asylum by her husband
for not eating for days at a time. Although originally admitted for being unable to take care of
herself, she was diagnosed with Chronic Mania in the first few weeks of her arrival. As an
ex-teacher, she is intelligent and from an upper class background, both of which are
similarities that help create the bond between the two characters. She is unable to have
children, despite her own desires, and is sympathetic to Rebecca’s situation regarding Eve.
She desperately wanted children, and her disbelief in realising that she can’t is the reason she
for her condition.
Name: James Ruswick (Rebecca’s Husband)
Age: 37 Gender: Male
Born: 7th December 1847 Status: Upper class, Married.
Place of Birth: London, England. Inherited his father’s Estate
Background Information:
Ill tempered, but never violent towards Rebecca. He came from a wealthy family and was
brought up to withhold gentlemen-like qualities. Loved to play the piano, and would often
play to Eve. He loved Rebecca and would often tell her so, yet Eve was the most precious
thing to him. Physically strong and not very sentimental, like most Victorian men, he believes
Rebecca’s negligence towards Eve caused the accident, and rashly condemns her to the
asylum with no intention of seeing her again.
Name: Eve Ruswick (Rebecca’s Daughter)
Age: 6
Born: 29th June 1878
Place of Birth: London, England.
Gender: Female

270333
34
Background Information:
Before falling into a coma and suffering severe injuries, Eve lived six happy years with her
parents. She was an ordinary six-year-old girl, who, like her mother, loved to experience
nature. Rebecca would take her walking around the lake on the estate regardless of the
weather. Eve’s accident happened in February, the same month her mother was condemned
to the asylum for her apparent Hysterical symptoms, following her daughter’s ill health.
Name: Victor Thomas Porter
Age: 49 Gender: Male
Born: 17th June 1835 Status: Educated Working Class
Place of Birth: Oxford, England. Employment: Doctor, Physician.
-Mannerisms-
Abrupt, deep tone of voice. Does not often express emotion, unless one of his experiments
gives him the result he wants. Doesn’t talk much, instead prefers physical contact with his
patients, for example performing surgery. Has a tendency to tap his feet when he is intrigued,
a noise that haunts Rebecca as her condition deteriorates.
Excited: grins rather than smiles.
Scared: is not intimidated easily. Used to patient outbursts.
Surprised: becomes erratic, loses all logic and becomes excited.
Confused: always refers to his notes before and after a procedure.
Intrigued: taps his feet.
-Physical Attributes-
Hair Colour: Black Body Type: Broad but not muscular
Hair Style: Short/Neat Height: 5 foot 10 inches
Eyes: Blue Weight: 69kg (154 Pounds)
Background Information:

270333
35
Victor was born in England and eventually moved to London when his parents disappeared
when he was very young. He grew up in a boarding school which taught him the discipline he
instils on his patients. Although he is a doctor, he believes himself a scientist. Very
passionate about his work. He is determined to revolutionise science with a new discovery,
and so he likes to experiment using a variety of methods. Intelligent, yet he lacks logic when
devising his experiments, which is why so many of them fail.
-Plot & Story-
Chapter 1
Chapter Summary:
Rebecca Ruswick begins the narrative, explaining how she arrived at the Asylum and how
she was put in restraints upon her arrival. She describes Dr Porter, who categorises the
patients into groups and separates the men from the women.
Chapter 2
Chapter Summary:
Rebecca is unfamiliar with the daily routine she has to follow in the asylum. She is woken
early and is confused when she is taken to various rooms to work and for treatment. She is
taken to the Airing Ground where the female patients are given exercise and allowed to roam
around as they please. This is where she meets Jane Harrington. Later, she is taken for
another stage of treatment and is given a three-hour long Ice bath.
Key Emotions:
• Anger
• Fear
• Shock
Key points in chapter:
• Arrives at asylum
• Experience of Restraint Treatment
• First meets Dr Porter

270333
36
Chapter 3
Chapter Summary:
During her treatment the following day, Rebecca continually begs to have some contact with
Eve, though Dr Porter interprets this as Hysterical behaviour and devises a new form of
treatment, never before tested on a patient. He diagnoses her with Chronic Mania and begins
Insulin Therapy. Rebecca attempts to resist but her defiance only reinforces his diagnoses that
she is insane. At this point her physical deterioration is evident and she is ill for several days.
Key Emotions:
• Anxious
• Happy
• De-moralised
Key points in chapter:
• Rebecca unfamiliar with the asylum routine
• Meets Jane
• Consultation with Dr Porter
• First Ice bath treatment
Key Emotions:
• Sad
• Desperate
• Pain
Key points in chapter:
• Rebecca continues to ask for contact with
her daughter
• Rebecca is diagnosed with Chronic
Mania
• New method of treatment is introduced:
Insulin Therapy
• Physical deterioration- becomes ill
(exhaustion/mild pneumonia from Ice
bath).

270333
37
Chapter 4
Chapter Summary:
Rebecca’s insulin therapy has continued whilst she was asleep, despite having pneumonia
and being unconscious. She wakes several days later, in a separate room restrained to the bed.
She deduces that her treatment is over. She is unstrapped and taken to the Airing Ground for
some exercise. On the way there, Rebecca believes she can hear her daughter calling to her,
but recalls how terminally ill she was before she was taken from her. She finds Jane and tells
her that she has to find a way to escape.
Chapter 5
Chapter Summary:
After her routine treatments, all the patients on the ward are taken to the ‘Friends Room’.
Twice a week, the friends room gives Rebecca and Jane another chance to meet. This is
where they begin to plot their escape, but Rebecca has no idea of the layout of the asylum and
is confused and disorientated from the drugs she’s been given. Jane takes over the
conversation and tells Rebecca what they will need for their escape and devises a plan.
Key Emotions:
• Disorientated
• Weak/Numb
• Jumpy
Key points in chapter:
• Insulin Therapy continues
• Wakes several days later from coma-
Mental deterioration
• Auditory Hallucinations begin
• Taken to Airing Ground and finds Jane
• Tells Jane of her desperation to escape
and Jane agrees to help her
Key Emotions:
• Vacant
• Distant
• Desperate
• Driven
Key points in chapter:
• Meets Jane in the ‘Friend’s Room’
• Discusses plan to escape
• Jane tells Rebecca what they will need to
do
• Jane’s plan seems illogical and irrational
to Rebecca

270333
38
Chapter 6
Chapter Summary:
Rebecca’s schedule to work in the laundry room that afternoon gives her the opportunity to
sneak out. Using Jane’s information, Rebecca makes her way down the Gallery towards one
of the treatment rooms and takes a trephine from the surgical bench. She conceals it and
returns to the laundry room without being noticed. That night she hallucinates. She believes
that Dr Porter is watching her. He tries to kill her, and believing that he knows about the
trephine, she stabs him with it and he falls to the floor. Moments later, she realises it wasn’t
real. She hides the trephine inside her pillow and returns to bed. She does not sleep.
Chapter 7
Chapter Summary:
The next day, Dr porter decides to increase the insulin dosage for Rebecca’s therapy. She is
induced in several comas for the majority of the day, but is eventually allowed to return to her
regular routine. In the airing ground, Jane finds Rebecca and asks whether she has been able
to get the item for the escape. Rebecca tells her that she has got the trephine, but they still
need an idea of the layout of the Asylum in order to plan their escape. Jane tells Rebecca of a
consultation she had with one of the other physicians. She mentions the brilliant view of the
entire complex, visible from the Physician’s room. With that Rebecca assaults one of the
guards, and is taken to see Dr Porter to try and look for a way out of the grounds but she
cannot find one. Due to her outburst a the guard Dr porter increases Rebecca’s insulin dosage
again and tells her that he is watching her closely, revealing his interest in her.
Key Emotions:
• Unstable
• Unpredictable
• Scared
Key points in chapter:
• Becoming very desperate- time is running
out
• Sneaks out of Laundry Room
• Steals a trephine from one of the
treatment rooms
• Visual Hallucinations become more
severe
Key Emotions:
• Confused
• Sad
Key points in chapter:
• Wakes from induced comas
• Meets Jane in the airing ground as usual
• Rebecca tells Jane of the trephine
• Jane reveals information about the layout
of the Asylum

270333
39
Chapter 8
Chapter Summary:
A week later. Rebecca wakes from another coma, but she has become much more mentally
fragile. She believes she can see things growing on her every time she wakes up, and hears
her daughter calling constantly. She starts to believe she might be insane, and has started to
talk to herself when she is alone. She remembers that she was running out of time to see her
daughter and becomes extremely desperate. She finds Jane in the friend’s room, and after a
conversation about the urgency of the escape, Jane has an idea which she shares with
Rebecca. Despite both character’s irrationality, Rebecca’s desperation to see her daughter
causes her to agree, and they decide to execute their plan that same evening.
Key Emotions:
• Shaky
• Irritable
• Scared
• Irrational
Key points in chapter:
• Wakes from a week-long coma
• Finds Jane in the friends room
• Speaks to her about the plan
• Discusses the details of the plan and
agree to escape that evening

270333
40
Chapter 9
Chapter Summary:
That evening, Rebecca and Jane try to escape. Rebecca begins to hallucinate compromising
the success of their plans to escape. Jane sneaks away from the other patients on the Gallery
who are being escorted to their beds. Rebecca follows her and finds herself unable to
distinguish what is and isn’t real. She sees patients staring at her who aren’t really there, and
she becomes paranoid they will alert the staff to their plan. Rebecca follows Jane into a
nearby Water Closet to hide. They continue towards the main hall, but are discovered a
passing steward. Rebecca panics and freezes, but Jane stabs him with the trephine before he
can alert the staff. Jane returns the trephine to Rebecca and opens the door. Fortunately, the
Entrance Court door remains unlocked for visitors and the pair continue out onto the front
gardens. However, Jane is captured by the pursuing guards, allowing enough time for
Rebecca to flee into the nearby woods. Jane urges her to keep going, despite Rebecca’s
reluctance to leave her friend behind.
Key Feelings:
• Scared
• Excited
• Hopeful
Key points in chapter:
• Initiates escape plan
• Jane and Rebecca hide in a Water Closet
to avoid detection
• Discovered by steward, who is then killed
by Jane
• The pair flee the Entrance Court onto the
front gardens
• Jane is re-captured, and Rebecca escapes

270333
41
Chapter 10
Chapter Summary:
The woods ran for miles and surrounded the Ruswick estate, which Rebecca often walked
with her husband James when she was younger. As she moves deeper into the woods she
begins to see oddly formed creatures, which she believes are hostile towards her. After
walking for several miles through the woodland, Rebecca collapses and falls through the
undergrowth onto her husband’s estate. She drags herself through the gardens towards the
main house. To avoid attracting attention, she opens the cellar door at the back of the house
and climbs inside. She continues to hallucinate, believing that she sees Eve run past the cellar
doorway into the Entrance Hall. Rebecca checks the hall is clear before continuing, realising
she would be too exhausted to resist capture if discovered. Upon hearing Eve’s voice calling
to her she follows her up the stairs and onto the landing, where she sees her husband standing
in the doorway of her daughter’s bedroom. She moves silently across the landing towards
him with the trephine clutched tightly in her hand.
Chapter 11
Rebecca makes a noise on the landing which causes James to turn towards her. Before he can
defend himself she sinks the trephine into his neck and, ignoring his screams, drops the
weapon and runs into the room to see her daughter lying on the bed. She holds her daughter
in her arms, and upon seeing Eve smile at her, discovers she is not too late – or so she
believes.
Key Feelings:
• Deprived
• Unpredictable
• Enthralled
Key points in chapter:
• Reaches the Ruswick Estate
• Enters the house through the cellar
• Her hallucinations are now extreme
• Rebecca follows Eve’s imagined voice
upstairs
Key Feelings:
• Vacant- unemotional
• Relieved
Key points in chapter:
• Rebecca murders her husband
• Sees her daughter lying in her bed
• Rebecca is re-united with her daughter

270333
42
-Seminar & Workshop -
Material
Setting
What is it like/how do the characters feel in these places?
The tapping of his heel was steady, luring me in like a fly to a lamp. I would have preferred
the chair for company. The wooden back of the chair was hard as he invited me to sit down
opposite him. He began to speak to me, although I wasn’t really there- distracted I suppose. A
musky smell had drifted down the hall which made me cough, interrupting me as if there
were no need for words. It seemed to come from the apothecary. I’ve seen the doctors go in
there sometimes, and when they come out they’re carrying bottles and sharp objects. One of
the bottles was glowing yellow the other day you know. I saw it.
‘Rebecca, is everything okay?’
I nodded.
‘We’re going to try something – different today’, he said.
I swallowed hard and laid on the bed.
Writing Exercise: Rebecca’s experience of a consultation with Dr Porter in the Physicians
Room in Bethlem Hospital. Focused on Rebecca’s senses.
1. Physicians Room
- Afraid of the unknown, doesn’t
know what to expect
- Feels unimportant/animalised
- Anxious/threatened/ confused
afterwards: is this her last
moment alive?
- Cure room rather than Treatment
room
- Smell of the apothecary- coughs
2. Airing Ground
- Communal
- Feels a sense of freedom, frees
her mind and body
- Excitement/able to converse with
Jane
- Smoke from the factories in the
city
270333
43
Writing Exercises
Experience of a modern day Asylum
Every week I have to sit in this damn room with nothing to look at but a desk, a pencil pot, a
box of paperclips and some paperwork with my name on it. I try not to look at the walls; too
white. Too busy. There are paintings that hang above the desk either side of the room, worn
and leaning ever so slightly to the right; which if you are a regular like me is completely
infuriating. I’d say it’s to cover the shabby white paint finish. I asked them to straighten them
once, the pictures I mean, but they just laughed and told me to focus on the questions.
There is a window behind the desk where we have our little ‘chats’; it saves me from
looking at her dull face. That is, Miss Sue Barsden- my psychiatrist. Yes, I have a
psychiatrist. They all think I’m mad, even my dear brother, Sammy; I reckon they’re totally
convinced but no one has openly admitted it to me yet.
I see all sorts of things through that window you know, like Lucy she should be here
any minute -Its usually about this time. I often wonder if I’m peering through it into another
world, silently observing from behind the thin glass panels. I’m staring now, but nothing has
happened just yet; sometimes it just takes a while but I always see her.
One sentence paragraph
They say you can cure insanity, at least they tried to, not that I was insane because I wasn’t, I
just found it a little difficult familiarising myself with my new residence, that’s what they call
it now, a residence, despite the cold hallways and damp bed sheets which are not really bed
sheets due to the fact they have been worn down, so thin in fact I could almost tear them
apart, and yes I have tried but it’s not as easy as you would think you know, tearing up a bed
sheet.
First-person narrative (Attempt 1): I tried to get across the patient’s frustration and anger
towards her doctor, and the unpredictability in the behaviour of an individual with mental
illness, like Rebecca in my novel. Written in a similar style to The Yellow Wallpaper.
First-Person Narrative (Attempt 2): This was a seminar exercise where I had to make a one-
sentence paragraph. It is about a woman who believes she is not insane and has no awareness
of her surroundings. It could be edited to become one of Jane’s utterances in a converdation
with Rebecca in the asylum as a form of her nonsensical rambling.

270333
44
Writing in Diary form
April 12th?
I’ve been here almost a month now. I think. You lose track of time in this place. Yesterday
they took me into a room and tied me down to one of the beds in the ‘patients’ room, where
Dr Porter was waiting for me as usual. I saw another patient come out just as I was going in-
he was strange though, his limbs were hanging over the arms of the two other doctors who
were carrying him out. He never even looked at me. Rude. Anyway I went in for my regular
meeting with Dr Porter who said he was going to try something new, to make me better so I
could go home! ‘It’s just a precaution’ they said. The straps felt cold around my arms and
legs as he tightened them, covering the bruising from the day before. He’s very precise! I
didn’t struggle. It’s not worth it, besides Dr Porter says it will only increase the dosage they
give me and I’ll be asleep for even longer.
Practising with Dialogue
‘Jen- Jenny did you hear me?’
‘Yes.’
‘So how are you feeling today?’
‘Fine.’
‘That’s good to hear, today we are going to move on from our normal set of
questions…’
There did you see it? I thought it was just me at first but I definitely saw her then.
‘Jen, I said I’m going to show you some photographs if that’s okay?’
‘Sure.’
‘Can you tell me what you see?’
‘A castle.’
‘Okay. Can you tell me if you see anything different about this next photo?’
‘There’s a barred gate- but the gates are shut’.
‘And what about this one?’
‘The same, only now there is a woman behind it’
‘And this one?’
‘Now there’s a girl too. She’s trying to reach for the woman but the gate won’t open.’
(Attempt 1): Rebecca’s diary entry after 3 weeks of treatment. Confused, lost track of time.
Submissive to her routine treatment.
(Attempt 1): Asylum consultation between a patient suffering from hallucinations, and her
doctor.

270333
45
‘Keep going Jenny’
‘She’s crying…’
‘It’s okay!’
‘No, the woman wants to get to her she needs to get to her. Let her through!’
‘Okay, okay thankyou Jenny. That will do for now. I just need a quick word with Sam
outside and we’ll leave it there.’
Sue’s chair scraped across the laminate floor as she stood up and walked towards the
door, but my gaze is still fixed on the girl outside the window.
‘It seems to me that the accident has affected her perception of reality. I think it would
be a good idea if she…’
Sue smiled at me before pulling the door shut, aware that I was able to hear her despite being
on the other side of the room. Lucy’s gone again. That can happen you know, if you aren’t
paying attention; she just disappears for a while but she’ll be back.
‘Jen, come on sis let’s get going’ I heard Sam say as they both re-entered the room.
‘Go where?’
‘We have to go away for a while’
‘But I can’t leave her?’
My husband John doesn’t seem to understand that. No matter how many times I say it. What
kind of mother would that make me!
‘Jenny come on’
She’ll be back soon; she always comes back.

270333
46
-Bibliography-
Websites:
https://prezi.com/r2bguokfl0u2/asylums-and-treatments-of-mental-illness-in-the-victorian-
era/
http://thetimechamber.co.uk/beta/sites/asylums/asylum-history/the-history-of-the-asylum
http://www.victorianlondon.org/health/bethlehemhospital.htm
http://studymore.org.uk/4_13_ta.htm#Bethlem1860s
https://historicengland.org.uk/research/inclusive-heritage/disability-history/1832-1914/daily-
life-in-the-asylum/
http://www.jtrforums.com/showthread.php?t=7317
http://www.britannica.com/topic/lobotomy
http://serendip.brynmawr.edu/bb/neuro/neuro01/web1/Goff.html
https://en.wikipedia.org/wiki/Trepanning
http://www.vam.ac.uk/content/articles/i/introduction-to-19th-century-fashion/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1574422/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1973489/?page=2
https://en.wikipedia.org/wiki/History_of_psychiatric_institutions#Emergence_of_public_lunatic_asyl
ums
http://www.cerebromente.org.br/n04/historia/shock_i.htm
Videos:
https://www.youtube.com/watch?v=oswUssXzFlY&nohtml5=False
https://www.youtube.com/watch?v=YA_MwaRLzm8&ebc=ANyPxKqPk0u0xMJdLq3dqRjmxTXC3
5rrkzhPi3MLdoOvCYRWk4TDnAUCGf-wGN6iesiH2JmJVcGyA-7y3NRYfLZDeiU1uiLr0Q
https://www.youtube.com/watch?v=YA_MwaRLzm8&ebc=ANyPxKqPk0u0xMJdLq3dqRjmxTXC3
5rrkzhPi3MLdoOvCYRWk4TDnAUCGf-wGN6iesiH2JmJVcGyA-7y3NRYfLZDeiU1uiLr0Q
https://www.youtube.com/watch?v=4DjQ-V2YELQ
https://www.youtube.com/watch?v=EtgzpAbxcRI

270333
47
Books:
Gale, Colin and Robert Howard Presumed Curable. Hampshire: Wrightson Biomedical Publishing
Ltd. (2003)
The Committee on Nomenclature and Statistics of the American Psychiatric Association, Diagnostic
and Statistic Manual: Mental Disorders. Washington: American Psychiatric Association Mental
Hospital Service, (1952) : p.26-27.





























