Embed Size (px)
Citation preview
1
Assessment and Diagnosis of Dementia in Individuals with Intellectual Disability: A Toolkit for Clinicians and
Caseworkers
Gregory D. Prichett, Psy.D.
8/07/2017

2
Table of Contents Introduction Alzheimer Disease: Onset, Course and Clinical Characteristics Overview Clinical Course-Early, Middle and Late Stage Features Dementia Rates in the General Population Risk Factors for Alzheimer Disease Neuropathology of Alzheimer Disease Diagnosis of Alzheimer Disease
Developmental and Intellectual Disability Overview Causes of Intellectual Disability Down Syndrome Intellectual Disability, Aging and Dementia Overview Longevity Risk Factors for Alzheimer Disease Prevalence, Onset and Progression of Alzheimer Disease Clinical Manifestations of Alzheimer Disease Neuropathology of Alzheimer Disease in Persons with ID Clinical Diagnosis of Alzheimer Disease in Individuals with Intellectual Disability Diagnostic Challenges Is There a Test for Alzheimer Disease? Diagnostic Criteria ICD-10 Criteria for Dementia and Alzheimer Disease Psychiatric Impairment and Intellectual Disability Overview Prevalence Rates of Psychiatric Disorders in Adults with ID Depression in Adults with Intellectual Disability Life Stress
Diagnosis of Psychiatric Disorders in Adults with ID Diagnostic Overshadowing Impact of Intellectual Disability on Presentation of Psychiatric Disorders Why is this important?
Diagnostic Criteria for Psychopathology in Persons with ID Assessment of Psychiatric Status in ID Individuals

3
Special Considerations for the Diagnostic Interview
Assessment: A Baseline Comparison Approach to Diagnosis of Dementia in ID Assessment Measures Observer Rated Scales Direct Neuropsychological Measures Adaptive Behavior Scales Screen Measure Measures of Adjustment, Emotional Functioning and Psychopathology Summary References and Resources

4
INTRODUCTION Individuals with intellectual disability (ID) are living longer and, as such, at increased risk for developing age-related conditions including dementia. Diagnosis of dementia is complex in adults with ID owing to their pre-existing intellectual and psychosocial deficits and atypical presentation. Traditional diagnostic approaches that rely on the use of standardized assessment measures to document declines at a single point in time in the general population are typically inappropriate for use with the ID population as they presume a “normal” level of premorbid function. Rather, the diagnosis of dementia in individuals with ID requires documentation of a change in status from a baseline level of function using longitudinal behavioral observations and individually tailored assessment techniques scaled for use with the ID population. Many physicians and healthcare professionals lack training in the needs of individuals with intellectual disability across the lifespan (U.S. Public Health Service, 2002), and more specifically, are inadequately prepared to recognize symptoms or conduct diagnostic assessment of adults with ID who may be affected by dementia (Perkins and Moran, 2010). With the rising life expectancy and growing population of individuals with ID, clinicians and case workers can expect to encounter increasing numbers of persons with intellectual disability who develop dementia. Development of specialist assessment skills in this area will be important to meet this growing demand. Incorporating these assessment strategies into an organized screening protocol will improve diagnostic accuracy and medical and care management. This tool kit was developed for clinicians and caseworkers who are concerned about the presence of dementia in their patients and clients with intellectual disability. It compares and contrasts the incidence, prevalence and clinical features of dementia of the Alzheimer type in adults with ID (with an emphasis on Down Syndrome) with that of the general population and then outlines the modifications to diagnostic approaches that are needed to improve diagnostic accuracy for those ID adults potentially affected by dementia. A number of neuropsychological assessment measures that have been developed or adapted for use with ID adults are then reviewed. It is hoped this tool kit will serve as useful clinical reference and assessment resource for dementia care professionals to enhance services to this uniquely vulnerable population.

5
ALZHEIMER DISEASE: ONSET, COURSE AND CLINICAL CHARACTERISTICS For comparative purposes a review of assessment, course and clinical characteristics of Alzheimer’s disease in the general population is provided below. Overview Alzheimer’s disease is a slowly progressive, degenerative disorder of the brain that leads to abnormal brain function, increasing functional dependence, and eventual death. While the disorder is marked by a slow gradual decline in cognitive and behavioral function, impairments can be abruptly unmasked by significant stressors or inter-current illness or injury. A small number of individuals develop the condition before the age of 60, but the disease is most common in individuals over the age of 65. While the neuropathological brain changes associated with Alzheimer disease are similar amongst affected individuals, the presentation and course of dementia may vary considerably from one individual to the next. Clinical Course The course of Alzheimer disease is typically described in terms of early, middle and late stage features. Early Stage In the early or onset stage of the disease changes may appear gradually and are often difficult to distinguish from normal aging (The Arc, 1995). There may be subjective awareness of memory lapses and word finding difficulties. Despite these subtle changes the affected individual may still function independently and continue to work, drive and engage in social activity without major difficulty. Eventually, a triad of cognitive deficits emerges characterized by memory impairment, difficulties with expressive language and visual-spatial disturbances (Strub and Black, 1989; Welsh-Bohmer and Warren, 2006). Memory impairment is often the most prominent deficit early on and frequently the presenting complaint of patients and families. The disturbance is characterized by difficulty forming new memories along with a rapid rate of forgetting of recent information over time. This disturbance in manifested by forgetfulness for names and recent events, repetitive statements and questions, and misplacement of items. Remote memory and semantic knowledge are relatively preserved in this stage. The early stage memory losses parallel the underlying neuropathology in the medial temporal lobes where input pathways from the entorhinal cortex and hippocampal regions are disrupted over the course of the disease leading to isolation from the association areas of the cortex (Welsh-Bohmer and Warren, 2006). In addition to memory loss, expressive language difficulties are common in the early stages of Alzheimer Disease and often are manifested by a vacuous speech quality that becomes increasingly devoid of substantive word content. Receptive language is better preserved and generally not affected at this stage. Visual-spatial disturbances are also present although patients may not complain about them unless these functions are a regular requirement of their job or daily activities. Problems with way-finding or geographical confusion, such as losing one’s way in a familiar environment, may signal emerging

6
problems. Visual-spatial disturbances are often easily documented on formal tasks of drawing, construction and visual perception. Accompanying the deterioration in these basic cognitive abilities, general problem solving and executive function may wane. As a consequence of these early-stage changes, the affected individual may begin to experience impairment in daily functioning, particularly when performing tasks in social or work settings or when patients attempt to solve novel problems in which the individual is unable to rely on well-established routinized skills or strategies. Subtle emotional changes can often accompany, and at times precede the memory and cognitive changes seen in the early stages of the disease. The affected individual may complain of or otherwise demonstrate a loss of interest in work, family and usual vocational interests (Strub and Black, 1989). Uncharacteristic restlessness or irritability or sudden changes in mood may occur for no apparent reason. In other cases the affected individual may become quiet or withdrawn. The emergence of hypochondriacal concerns without a physical basis, especially in a previously healthy middle aged or elderly individual, may reflect the patient’s attempt to find a physical explanation for the vague feeling that something is wrong. As awareness of losses increases the affected individual may react with symptoms of anxiety, denial and compensation. The early stage may last for a period of one to five years (The Arc, 1995; Dalton and Janicki, 2013). During this stage the neurologic exam typically remains normal (Strub and Black, 1989). Middle Stage As the disease progresses symptoms noted in the early stage become more pronounced, and the individual is less able to meet the demands of everyday life. Typically the most obvious sign of decline into moderate or progressive stage of Alzheimer disease is a more distinct problem with language abilities (The Arc, 1995; Strub and Black, 1989; Welsh-Bohmer & Warren, 2006). The affected individual may have pronounced difficulties naming objects and following a logical conversation. Where basic receptive abilities are generally preserved in the early stage, the affected individual may also start to have difficulty understanding directions or instructions, particularly if they are complex or multi-step. Language may become concrete, tangential and perseverative. While speech remains fluent at first, increasing word retrieval difficulties may lead to a halting quality to speech output with paraphasic word substitution errors becoming more evident as the disease advances, and increasing but many times unsuccessful attempts to compensate for word retrieval difficulties with circumlocution. Individuals in the middle stage of the disease become easily disoriented and confused with regard to time, place and the persons around them (The Arc, 1995). Episodic memory loss is profoundly affected now and becomes characterized by intrusion errors and recognition memory deficits suggesting that the memory loss has progressed beyond consolidation deficits to involve greater difficulties with encoding and temporal sequencing of events, both of which lead to confusion between recent and remote events from past stored experiences (Welsh-Bohmer & Warren, 2006). Affected individuals in the middle stage of Alzheimer’s disease may also begin to experience a loss of self-care skills including toileting, and problems with incontinence may result. Difficulties in initiating and organizing previously known motor tasks such as dressing or manipulation of hand tools becomes evident at this stage reflecting emergence of apraxic signs.

7
Early on in this stage, the affected individual may retain insight into their condition sufficient to develop secondary anxiety and depression. Over time significant behavioral disturbance including agitation, suspiciousness, delusions and hallucinations may develop and if left unrecognized and/or untreated, can lead to more pronounced loss of functional ability. With progression, the cognitive and functional declines that emerge in the moderate to severe stages of Alzheimer disease parallel the spread of neuropathological brain changes from the medial temporal lobes (hippocampi, entorhinal cortex) to the parietal and frontal cortices and eventually consume most of the neocortex (Schoenberg and Duff, 2011). The neuropsychological changes that take place in the progressive stage usually occur over a span of 5-15 years (Dalton and Janicki, 2013). Third Stage Along with generalized intellectual deterioration, patients in the third or terminal stage of Alzheimer’s disease move to a more distinctly aphasic, apratic and agnostic stage and substantial dysfunction ensues (Strub and Black, 1989). Basic skills such as eating or drinking are forgotten, often resulting in substantial weight loss. Difficulties executing previously learned skilled movements, such as dressing and getting in and out of bed, for example, become prominent in this stage. Dysnomia becomes marked and is made worse now by the inability to recognize common objects (object agnosia). The spontaneous speech of affected individuals decreases markedly, and comprehension is greatly reduced. Ability to recognize other persons and their environment is greatly diminished (The Arc, 1995). Both short- and long-term memories are lost. In the third or terminal stage, physical symptoms are now prominent including the emergence of primitive/infantile reflexes, abnormal eye tracking movements and resistance to passive motion. Other indications of progression in this stage include carphologia and the mirror sign. At this stage persons affected by Alzheimer disease require complete and total care and often are bed-ridden. In the advanced phase of this stage affected patients become non-communicative, completely apathetic, withdrawn and mute. They often show evidence of pseudobulbar affect and develop masked facies, seizures, myoclonus and flexion of the lower extremities. They may constantly mouth objects. Any of a number of medical complications including pneumonia, aspiration, UTI and/or sepsis commonly precede death. Changes in the terminal stage typically occur over the course of 3-5 years (The Arc, 1995). A summary of the signs, symptoms and clinical course of Alzheimer disease are provided below.

8
Signs and Symptoms of Alzheimer Disease in the General Population The Arc, 1995
EARLY STAGE MIDDLE STAGE LATE STAGE
forgetfulness – recent memory loss
Cognitive decline Subjective awareness of
cognitive changes Gradually evolving
vocational/social dysfunction
Difficult to distinguish from normal aging
No distinct physical presentation
Distinct problems with language
Pronounced loss of memory and cognitive abilities
Frequent confusion and disorientation
Loss of self-care skills Personality and behavior
change
Global disorientation and confusion
Remote memory loss Disordered and fragmented
speech Basic skills forgotten Incontinence Weight loss General physical
deterioration Parkinsonian features Immobility, rigidity and
frequent falls Totally dependent
Dementia Rates in the General Population Alzheimer’s disease is the most common form of dementia, accounting for approximately 50% of all cases (The Arc, 2001). Based on estimates in 2016, 5.4 million Americans were believed to have Alzheimer Disease. An estimated 5.2 million of those individuals are aged 65 or older while approximately 200 thousand persons are under 65 (Alzheimer’s Association-n.d.-a). By the year 2025 the number of people aged 65 or older with Alzheimer’s disease is expected to nearly triple from 5.2 million to a projected 13.8 million assuming no medical breakthrough or cure is found (Heller and Factor, 2004). The female to male ratio in Alzheimer’s disease is 2:1 at all ages (Strub and Black, 1989).
Median survival time following diagnosis of Alzheimer disease depends strongly on the patient’s age and the presence of comorbid medical conditions. Median life span ranges from 7-10 years for those diagnosed in their 60’s or 70’s while median life span was 3 or less years for individuals diagnosed when they were in their 90’s (Brookmeyer et al, 2002). The average duration between onset of symptoms and diagnosis is 2.8 years (Brookmeyer et al, 2002). Dementia rates for the general population are listed below.
Dementia Rates in the General Population, Brookmeyer et al (2011)
AGE ALL DEMENTIA ALZHEIMER’S DISEASE
71-79 4.97 2.32 80-89 24.19 18.10 90+ 37.20 29.6 Total 13.67 9.51

9
Risk Factors for Alzheimer Disease Research has identified a number of risk factors that increase the risk of Alzheimer’s disease (Alzheimer’s Association, n.d.-b).
Age – Age is the greatest known risk factor for Alzheimer’s disease. Most individuals with Alzheimer’s disease are 65 or older. The risk increases with advancing age. The likelihood of developing dementia of the Alzheimer’s type doubles every 5 years. After age 85 the risk reaches nearly 50% (Alzheimer Association, n.d.-b).
Family History – First degree relatives are at greater risk to develop the disease, and the risk increases if more than one immediate family member has the disease (Green et al, 2002; Fratiglioni et al, 1993; Mayeux et al, 1991; Lautenschlager et al., 1996; Alzheimer’s Association, n.d.-b).
Genetic Risk Factors
Susceptibility Genes – The presence of ApolipoproteinE-e4 (APOE-e4) increases the risk of, but does not directly cause, Alzheimer’s disease in 20-25% of the cases. In addition, due to increased risk, APOE-e4 may also play a role in symptom onset. Alzheimer’s disease may appear at a younger age than usual in patients with APOE-e4 gene (Alzheimer’s Association, n.d.-b ; Breitner et al., 1999; Green et al, 2002).
Deterministic Genes – Familial (autosomal dominant) AD may be caused by variances in the genes that code proteins: amyloid precursor protein (APP), presenilin-1 (PS-1) and presenilin-2 (PS-2). Familial AD usually develops before the age of 60 and may appear as early as 30-40 years of age. Familial Alzheimer’s disease accounts for less than 5% of all cases (Alzheimer’s Association, n.d.-c).
Head Trauma – A history of traumatic brain injury (TBI) places individual’s at greater risk for developing AD and other dementias across the life span (Vincent et al, 2014; Mortimer et al, 1991; Plassman et al, 2000; Lye et al, 2007; Salib and Hillier, 1997). The more severe or frequent the TBI the greater the risk (Gardner and Yaffe, 2014; Nordstrom et al, 2014) including mild TBI/post-concussive injury (Gavett et al, 2010). TBI may also reduce the time of onset of Alzheimer’s disease among persons at risk for developing the disease (Nemitz et al, 1999).
Neuropathology of Alzheimer’s Disease
Amyloid plaques and neurofibrillary tangles are the two most common markers of AD in the brain (Schonberg and Duff, 2011). The plaques and tangles are not unique to AD; rather, it is the abundance of these neuropathological changes and their distribution that distinguishes Alzheimer’s disease from other forms of dementia. These neuropathological changes begin in the medial temporal lobes (entorhinal cortex; hippocampus), and as the disease progresses expands to include association areas of the neocortex (Welsh-Bohmer and Warren, 2006). The cellular changes lead to gross morphological changes in the brain resulting in cortical atrophy, more prominent in the temporal and parietal areas, and compensatory enlargement of the ventricles (Schonberg and Duff, 2011).
Diagnosis of Alzheimer Disease
The diagnosis of Alzheimer’s disease is made by clinical history and exam and requires documentation of declines in memory and cognitive abilities sufficient to cause impairment in social and/or occupational

10
functioning (American Psychiatric Association-DSM-IV, 1994; World Health Organization-ICD-10, 1992) without disturbance of consciousness and in the absence of other systemic causes or diseases that could account for the symptoms.

11
DEVELOPMENTAL AND INTELLECTUAL DISABILITY
Overview
Developmental disability refers to mental and/or physical disabilities that occur before the age of 22, impede normal growth and development, result in significant functional limitations in three or more areas of major life activities and continue into old age (The Arc, 1995; Developmental Disabilities Act, Publication L, 106-402). Mental retardation (intellectual disability), cerebral palsy, epilepsy, developmental delay, autism/Autistic Spectrum Disorder, Fetal Alcohol Sydrome and numerous specific syndromes and neurologic conditions such as phenylketonuria, Rett syndrome and Prader-Willi syndrome are examples of various types of developmental disability.
According to the American Association on Intellectual and Developmental Disabilities (AAIDD), mental retardation or intellectual disability, which is the preferred term, is a disability characterized by significant limitations in both intellectual functioning and adaptive behavior which covers many everyday social and practical skills. The disability originates before the age of 18 (AAIDD.org, n.d.).
Intellectual disability is diagnosed through standardized tests of intelligence and adaptive behavior. Typically criteria for ID is an intellectual level (IQ) of less than or equal to two standard deviations below the mean (i.e. IQ = 70 or lower) compared to similar aged peers. Limitations in adaptive behavior may be indicated by a score of approximately 2 standard deviations below average in any one of three areas (conceptual skills, social skills, practical skills) or an overall score in all three areas of approximately two standard deviations below the mean for that age group (AAIDD.org, n.d.; Reynolds et al., 2013-a; See also Reynolds et al-b,c)
Many individuals with intellectual disability will also meet criteria for developmental disability but not all. In fact, at least half of all ID persons will not meet the functional limitations requirements of DD (The Arc-a, 2001). An estimated 4.6 million Americans have an intellectual or developmental disability (Larson, 2000).
Causes of Intellectual Disability
Intellectual disability can be caused by any condition that impairs the development of the brain. Numerous causes have been discovered but in approximately one-third of affected individuals the cause is unknown. (The Arc -b, 2011). Some common causes for ID are as follows:
Genetic—phenylketonuria, fragile X syndrome, Down syndrome
Problems during pregnancy—alcohol, tobacco or drug abuse; malnutrition; illness of the mother (toxoplasmosis, cytomegalovirus, rubella, syphilis).
Problems at birth – prematurity/low birth weight; anoxia; birth injury
Problems after birth- childhood diseases (whooping cough, chicken pox, measles, Hib disease) that may lead to meningitis and encephalitis; Traumatic brain injury, near drowning, exposure to environmental toxins.
Poverty and Cultural Deprivation-poverty is associated with higher risk of malnutrition, childhood diseases, exposure to environmental health hazards and inadequate health care increasing the risk of intellectual disability. Lack of adequate cultural, educational and environmental stimulation can contribute to intellectual disability.

12
Down Syndrome
Down syndrome (DS) is the most common genetic cause of intellectual disability accounting for 1 out of 691 live births per year (CDC, 2012). Besides intellectual disability Down syndrome is associated with more than 80 clinical traits including congenital heart disease, immune system deficiencies, risk of leukemia and dementia. Some common physical traits associated with DS are low muscle tone, small stature, upper slant of eyes and single, deep crease across the center of the palm.
Down syndrome occurs when an affected individual has a full or partial extra copy of chromosome 21 (Lejeune et al, 1959-a,b). This additional genetic material alters the course of development and causes the characteristics associated with Down syndrome (NDSS.org, n.d.). The cause of the extra genetic material is unknown.
There are three types of Down syndrome: Trisomy 21, translocation and mosaicism. Trisomy 21, or nondisjunction, results from an extra full copy of chromosome 21. This accounts for 95% of all cases of DS. Translocation is the attachment of the long arm of an extra chromosome 21 to either chromosome 14, 21 or 22. Translocation accounts for about 4% of all cases. Mosaicism occurs when some but not all cells are trisomic, and accounts for approximately 1% of all cases (NDSS.org, n.d.).
Maternal age is the only factor that has been linked to an increased risk of Down syndrome resulting from nondisjunction or mosaicism. Due to higher birth rates of younger females, 80% of children with Down syndrome are born to females under the age of 36 (NDSS.org, n.d.).

13
INTELLECTUAL DISABILITY, AGING AND DEMENTIA
Overview
As with the general population, the prevalence of dementia increases with age in the population of individuals with intellectual disability. Similar to the general population, the core symptoms of dementia in persons with ID involve progressive loss of function in multiple cognitive domains and areas of adaptive function leading to eventual death. In contrast, adults with ID are affected differently by dementia when compared to the typically developing population. Memory and cognitive changes may not be the most prominent or early signs. Instead, personality and behavior change may mark the early stages of the disease. Neurologic signs may be more pronounced early on as well.
Pre-existing intellectual and psychosocial deficits make it difficult to detect memory loss and cognitive changes when they do occur. Evidence of decline will depend on their premorbid level of function and demands of everyday life. The following section will review important factors related to aging and dementia in the ID population including life expectancy, risk factors for dementia in the ID population, prevalence rates of dementia in Down syndrome and non-Down syndrome persons with ID, and the clinical manifestations of Alzheimer disease and dementia in persons with intellectual disability.
Longevity
Life expectancy of persons with ID is increasing. In the 1930’s the mean-age at death for people with ID was about 19 years, while in the 1990’s the mean-age was 66 years, whereas for persons with Down syndrome the average age at death increased from 9 years in the 1920’s to 56 years in the 1990’s (Penrose, 1949; Janicki et al., 1999) The presence of multiple disabilities and level of ID influence life expectancy with a median life expectancy of 74.0 years, 67.6 years and 58.6 years found for mild, moderate and severe levels of ID, respectively (Bittles et al, 2002; Copus, 2013).
As of the year 2000, there were an estimated 641,161 adults with ID/DD over the age of 59 in the US. That number is predicted to nearly double in size to approximately 1.2 million by the year 2030 when the last of the baby boomers reach age 60 (Heller and Factor, 2004). While the life expectancy of people with ID is increasing it still remains lower than that of the general population. This is felt to be due to the prevalence of a number of health conditions common to individuals with DD/ID. By the time they reach middle age people with ID have greater tendency towards obesity and decreased physical fitness as well as emergence of age related health issues including dementia.
Among ID adults with Down syndrome, life span is still shorter than the overall population of people with intellectual disability (Bittles et al, 2002) and when compared to the general population (Minino et al, 2006). Increased mortality rates in Down syndrome population in early life are believed due primarily to increased incidence of congenital heart disease and leukemia. Higher mortality rates later in life are thought to be due to a number of factors, two of which are increased risk of dementia and a tendency towards premature aging (Zigman, 2013).
Risk factors for Alzheimer’s disease or dementia among people with developmental disability
Similar to the general population, individuals with intellectual disability are at increased risk of developing dementia if they have a history of severe or multiple head injuries (The Arc, 1995), or a family history of Alzheimer disease (The Arc, 1995; McCarron, 2004). Individuals with

14
intellectual disability not due to Down syndrome are at least at the same risk if not greater risk for developing dementia as they age to greater than 59 years (Strydom et al., 2013) and individuals with Down syndrome over the age of 40 are at substantially increased risk of developing Alzheimer disease.
People with Down syndrome are affected differently by dementia of the Alzheimer’s type. They have higher rates of Alzheimer’s disease when compared to the general population or to that of non-DS-ID. This is believed due to two factors: genetic links and a tendency toward premature aging. Neuropathological studies have consistently shown the characteristic brain changes associated with Alzheimer disease are present in “virtually all” adults with DS by the age of 40 (Malamud, 1972). “Over expression” of the amyloid precursor protein (APP) gene is related to amyloid plaque deposits in the brain and is critical to the development of AD. Researchers ( Goldgaber et al, 1987; Robakis et al, 1987; Tanzi et al. 1987) have established a genetic link between AD and DS: The APP gene is located on chromosome 21 in an area that must be trisomic for full expression of the DS phenotype. In addition to genetic links, because Down Syndrome persons experience precocious aging (Fraser & Mitchell, 1876; Madan et al, 2006; Dalton et al., 1993; Wisniewski & Hill, 1985; Brown, 1985; Schupf, 2006; Zigman & Lott, 2007;) they tend to experience age-related health concerns including dementia approximately 15-20 years earlier than adults in the general population. Typically Down syndrome adults are in their late 40’s or early 50’s when symptoms of Alzheimer’s disease first appear (The Arc, 2001). The symptoms of Alzheimer disease may be experienced somewhat differently in adults with Down syndrome. Memory or cognitive loss is not always prominent or first noted change. Instead, changes in personality, behavior and mood may be some of the earliest signs. Typically a general loss of interest in day-to-day activities is seen. Cognitive and executive declines may be seen indirectly by increasing dependence and a loss of ability to carry out previously mastered activities of daily living. When memory loss is present early on it tends to be manifested by forgetfulness for common day-to-day routines and places (McCarron, 2004). Importantly, not all adults with DS will develop Alzheimer’s disease. Some will show no sign of dementia well into their 70’s and die of other causes. Ball et al (2006) reported the following dementia rates for persons with Down Syndrome:
Risk Factors for Alzheimer’s disease or dementia among people with DD
over the age of 40 and has Down syndrome if the individual has some form of head injury, especially severe or multiple head injuries if the individual has a family history of Alzheimer’s disease if the individual is over the age of 59 and has an intellectual disability of another cause
15
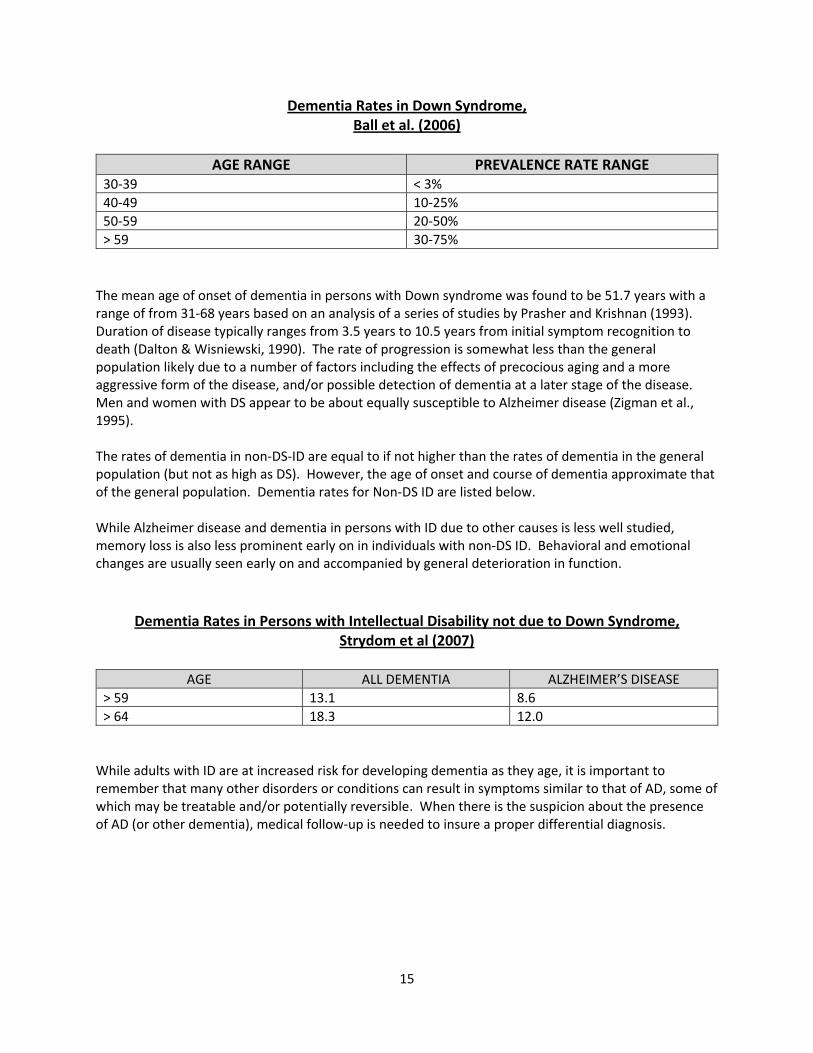
Dementia Rates in Down Syndrome, Ball et al. (2006)
AGE RANGE PREVALENCE RATE RANGE
30-39 < 3% 40-49 10-25% 50-59 20-50% > 59 30-75%
The mean age of onset of dementia in persons with Down syndrome was found to be 51.7 years with a range of from 31-68 years based on an analysis of a series of studies by Prasher and Krishnan (1993). Duration of disease typically ranges from 3.5 years to 10.5 years from initial symptom recognition to death (Dalton & Wisniewski, 1990). The rate of progression is somewhat less than the general population likely due to a number of factors including the effects of precocious aging and a more aggressive form of the disease, and/or possible detection of dementia at a later stage of the disease. Men and women with DS appear to be about equally susceptible to Alzheimer disease (Zigman et al., 1995). The rates of dementia in non-DS-ID are equal to if not higher than the rates of dementia in the general population (but not as high as DS). However, the age of onset and course of dementia approximate that of the general population. Dementia rates for Non-DS ID are listed below. While Alzheimer disease and dementia in persons with ID due to other causes is less well studied, memory loss is also less prominent early on in individuals with non-DS ID. Behavioral and emotional changes are usually seen early on and accompanied by general deterioration in function.
Dementia Rates in Persons with Intellectual Disability not due to Down Syndrome,
Strydom et al (2007)
AGE ALL DEMENTIA ALZHEIMER’S DISEASE > 59 13.1 8.6 > 64 18.3 12.0
While adults with ID are at increased risk for developing dementia as they age, it is important to remember that many other disorders or conditions can result in symptoms similar to that of AD, some of which may be treatable and/or potentially reversible. When there is the suspicion about the presence of AD (or other dementia), medical follow-up is needed to insure a proper differential diagnosis.

16
Clinical Manifestations of Alzheimer Disease Similar to the general population, the core symptoms of dementia in ID involve progressive loss of function in multiple cognitive domains. As noted, the clinical presentation of dementia in the ID population may be different as personality and behavior changes can mark the earliest signs especially in lower functioning individuals. The following section describes the major clinical manifestations of Alzheimer disease and dementia in individuals with ID (with an emphasis on Down Syndrome). Changes in Emotional Control, Motivation and Social Behavior
Changes in personality and behavior are often the first signs of an emerging dementia in persons with ID and are typically manifested by emotional lability, increased irritability, apathy/inactivity, stubbornness and coarsening of social behavior (Aylward et al., 1995). Irritability is often evident by low frustration tolerance, ease of anger or upset and general moodiness. Lability of emotions is manifested by mood swings, crying spells, becoming easily tearful, nervousness, fearfulness and shakiness suggesting a general loss of confidence, excessive worry about anything and everything, need for more prompting and encouragement, and greater dependence on others , and hypochondriasis with frequent and numerous bodily symptoms and complaints that are unfounded and out of character for the individual. Marked apathy and inactivity is demonstrated by withdrawal and social isolation, and a pervasive loss of interest and initiative in favorite foods and tv programs, past times, family activities and social gatherings coupled with a slowness affecting all aspects of functioning including walking, eating, speaking and general movements. Deb et al (2007-a) Stubbornness and coarsening of social behavior may be exhibited by oppositional/resistive behaviors and general uncooperative mood, becoming verbally and/or physically aggressive or behaviorally disturbed (or by an increase in the frequency, intensity, duration or pervasiveness of baseline maladaptive behaviors, or by a loss of previous aspects of personality/behavior, e.g. mischievousness, jolliness, independent-mindedness, need for sameness or routine, conscientiousness, meticulousness. Cognitive Loss The perception of cognitive loss will depend on the individual’s premorbid level of function and the demands of everyday life. The first suspicions of decline are often based on changes in adaptive function, as these are more concrete and generally easier to document (Aylward et al., 1995). Corresponding to the personality and behavior changes that can be seen early on in the development of dementia in ID, there may be a decline in frontal/executive functions and related adaptive abilities prior to the onset of memory impairment or full blown dementia. This has led some investigators to conclude that a frontotemporal type of dementia may represent the pre-clinical stage of dementia, particularly in adults with DS (Ball et al., 2006; Ball et al., 2008; Rowe et al., 2008). Cognitive deficits in judgement planning and organization may be observed in persons with mild ID who can no longer make weather-appropriate clothing choices or plan or carry out non-routine tasks such as

17
shopping or cooking. For those who normally only engage in routine tasks such as dressing, grooming, and toileting, etc., more fundamental cognitive deficits are observed typically with indications of apraxia, aphasia, alexia and agraphia. For those individuals with mild to moderate ID (IQ = 40-70) who have relatively well-developed verbal skills, cognitive loss can be seen with word finding difficulty, dysnomia and diminished ability to follow commands. If the individual’s premorbid verbal skills were relatively poor at baseline, decreased, use of language progressing to total loss of verbal expression is seen. Often there is a corresponding loss of previously acquired skills to read, write, count, color and draw. For those previously able to perform these skills there is a decreased ability to carry out basic ADL’s such as dressing, grooming, bathing, toileting and self-feeding. Inappropriate use of everyday objects may also be observed, e.g. using a toothbrush as a hair brush. In individuals with severe to profound ID (IQ <40) a general slowing in all areas is present with greater impairments to attention and decreased temporal and spatial orientation. Difficulties distinguishing day and night and inability to locate rooms in the home may be seen. Memory Loss As with cognition, memory loss will depend on the individual’s premorbid level of IQ and the memory demands of everyday life. In ID adults, memory may not be the first or most prominent change early on. When memory loss does occur its progression is similar to that seen in the general population accepting those tasks too complex or difficult to begin with. Memory loss in individuals with mild to moderate ID is frequently manifested as forgetfulness for names, recent conversations and events as well as the location of everyday items. Disorientation to time and the temporal sequence of events is present, as well as spatial disorientation to one’s environment as evidenced by difficulties getting around the home, neighborhood or worksite. As memory loss progresses increasing reminders and prompting are required to carry out daily activities, and the affected individual may experience difficulty remembering the steps necessary to perform previously mastered tasks or directions. The ability to assess memory loss in severe to profound ID depends upon their premorbid verbal skills and their ability to meet task demands. For individuals with profound ID (mental age of <2) their cognitive intellectual limitations may preclude detection on standardized tests. Greater reliance needs to be placed on informant report and the use of neurologic signs such as the presence of myoclonic jerks, seizure activity, abnormal posture/gait, rigidity and incontinence. Common Physical Signs
Common physical signs can accompany the onset or progression of dementia in ID adults. Approximately 50% to 80% of ID adults develop late onset seizure or a new type of seizure after being diagnosed with dementia. Approximately 20% who develop dementia also show Parkinsonian features including slowness and shuffling of gait, rigidity and posture abnormalities. Pathological reflexes, urinary incontinence and myoclonic jerks also can be present (Lai and Williams, 1989). Based on a recent comprehensive review of the literature, Strydom et al (2010) nicely summarized the sequence of dementia symptoms in ID adults, as detailed below.

18
Sequence of Dementia Symptoms in ID Adults Strydom et al., 2010
ADULTS WITH DS NON-DSID
Trigger Symptoms
Memory loss and disorientation
General deterioration in function Behavioral and emotional change
Deterioration in speech Personality and behavior change Functional deterioration Neurologic symptoms – seizures,
incontinence Frontal lobe-related symptoms
Sequence of Memory and Cognitive Changes – Early and Middle Stage Dementia (in order of typical progression)
Memory loss Deficits in executive function
Memory/cognitive decline less prominent early on
Complex cognitive functions Visual organization Verbal memory Semantic and short-term memory Dyspraxia
Sequence of Functional Decline, Personality and Behavior Change
Decline in ADLs –successive deterioration in o Personal hygiene o Housekeeping skills o Dressing o Spatial orientation o Eating
Signs of depression – o Lack of energy o Low mood o Disturbed sleep
Psychosis – persecutory delusions; auditory hallucinations
Increasing number and more severe maladaptive behaviors o Irritability o Aggression o Self-injurious behavior o General slowness o Apathy o Loss of interest o Decreased social engagement
More aggressive than DS counterparts (but higher prevalence of other behavioral change in DS)
ADULTS WITH DS NON-DSID
Neurological and Physical Changes
Epilepsy Myoclonus Pathologic reflexes Brain atrophy associated with frontal
lobe dysfunction Rigidity Postural abnormalities
Late stage symptoms – o Urinary/fecal incontinence o Difficulty walking
End-Stage Symptoms
Unresponsive to environment Loss of ability to speak Total dependence

19
Unable to walk Incontinent Parkinsonian features Almost all have seizures
Neuropathology of Alzheimer Disease in Persons with Intellectual Disability Numerous neuropathological studies (Lai and Williams, 1989; Holland and Oliver, 1995; Mann et al., 1984; Hof et al., 1995;) have found Alzheimer disease changes with prominent gyral and central atrophy, especially of the anterior temporal lobes. Neuritic plaques and tangles are abundant and distributed in the hippocampus, parahippocampal gyri, amygdal and neocortex, in both Down syndrome and non-DS cases. The neuropathological changes tended to be more severe in the DS cases than the non-DS ID cases with Alzheimer disease.

20
CLINICAL DIAGNOSIS OF DEMENTIA IN INDIVIDUALS WITH INTELLECTUAL DISABILITY Diagnostic Challenges The diagnosis of dementia relies on documentation of declines in cognitive and adaptive skills from previous levels of functioning and exclusion of other potential causes of diminished function. In the ID population the diagnosis of dementia is more complex for several reasons (Nagdee, 2011; Aylward et al, 1995):
Premorbid cognitive and psychosocial deficits – ID adults often lack the skills to perform common standardized diagnostic tests. The matter is compounded by the ID person’s limited ability to self-report. Often there may be a lack of consistent and reliable documentation of premorbid function. The combination of these factors makes it difficult to detect declines until they become pronounced
Atypical presentation – changes in adaptive skills and behavior may pre-date early impairments in memory in individuals with ID. Given the high prevalence of maladaptive emotional and behavioral problems (e.g. verbal/physical aggression, self-injurious behavior, distractibility, impulsivity) in this population, especially depression, it can be difficult to differentiate changes related to dementia from new onset or recurrent behavior or psychiatric problems.
Susceptibility to other causes of decline – differential diagnosis is made more challenging by susceptibility to other medical conditions common in individuals with ID that mimic dementia. Associated disorders, such as thyroid abnormalities, arthritis, hearing and visual loss, vitamin deficiencies, depression, susceptibilities to the effects of systemic illness, infections, pain, and adverse effects of medications, all can have effects on memory, cognition, mood and behavior that lead to deterioration in function.
It is important to systematically consider these factors in your differential diagnosis to avoid misdiagnosis and to identify areas that warrant further evaluation. Diagnosis of dementia in persons with intellectual disability can be greatly facilitated by having an established baseline of function before any problems become apparent. A working group of experts in the field (Aylward et al., 1995) have recommended assessments of baseline function be conducted at least once before the age of 36 in individuals with DS and by the age of 50 in persons with non-DS-ID, and periodically thereafter to facilitate early detection. If individuals are screened regularly, other conditions that mimic dementia can be ruled out and/or treated. Early detection is also important as it enables for care and treatment decisions to be adjusted over time to cope with increasing care needs.
Is there a test for Alzheimer’s disease?
As with the general population, there is no single diagnostic test for Alzheimer’s disease or dementia in the ID population. If suspected, a complete physical exam and more frequent medical, neurological and psychological evaluations are needed to establish the progressive nature of the symptoms and rule out other causes. All procedures involved in the assessment of dementia in the general population should be followed as closely as possible with necessary modifications to accommodate the individual with ID

21
The National Task Group on Intellectual Disabilities and Dementia Practices (Moran et al., 2013) provide the following Consensus Recommendations for the Evaluation and Management of Dementia in Adults with ID. Components of a standard diagnostic workup include a detailed medical history presented by a family member, caregiver or someone else well-acquainted with the individual. A thorough physical and neurologic exam include testing of sensorimotor systems, a psychiatric assessment to rule out the presence of a psychiatric disorder, particularly depression; neuropsychological testing to obtain in-depth measures of neurocognitive functions, including memory, orientation, language skills, intellectual abilities and perception; as well as routine laboratory tests including blood work and urinalysis. Chest x-ray, EEG and electrocardiography and other specialized tests should be done as deemed appropriate. The Task Group further recommends, at minimum, annual evaluations and rescreening be obtained to look for changes in existing skills and functioning. (Details of the NTG recommendations can be found at: doi: 10.1016/j.mayocp.2013.04024).
Diagnostic Criteria Currently there are no diagnostic criteria specific for use with the ID population. The previously referenced working group ( Aylward et al., 1995) proposed ICD-10 (WHO, 1992) criteria as the most appropriate for use with individuals with ID. While not specific to the ID population, the ICD-10 criteria place greater emphasis on non-cognitive aspects of dementia which are often the early signs of dementia in individuals with ID, especially the severely cognitively impaired. The ICD-10 diagnostic system also makes use of a two-step process to first establish a diagnosis of dementia and then subtype it. Because clinicians are well-aware of the strong associations between Down syndrome and Alzheimer’s disease, the Work Group reasoned there may be a tendency for evaluators to assume all cognitive declines represent Alzheimer’s disease. Conversely, the clinician may attribute the development of non-cognitive behavior changes to dementia without evidence of cognitive or memory decline. This two-step process helps to avoid the pitfalls of preconception and confirmatory bias which can adversely influence clinical inference, by providing a built-in mechanism to consider other possible causes of cognitive decline. Diagnostic Certainty To make a probable diagnosis of dementia of the Alzheimer’s type, a well-documented progression of symptoms needs to be established and other possible conditions or disorders ruled out. Complete evaluations must be performed periodically to establish decline. A possible diagnosis of dementia is made when the presentation or course is somewhat aberrant or is made in the presence of secondary disorders that may produce dementia but are not considered a primary cause of dementia. ICD-10 (WHO, 1992) criteria for Dementia and Alzheimer’s Disease are outlined below.

22
ICD-10 CRITERIA FOR DEMENTIA AND ALZHEIMER’S DISEASE
ICD-10 Criteria for Dementia 1. Decline in memory. Most evident in the learning of new information, although in more severe cases
the recall of previously learned information may also be affected. The impairment applies to both verbal and nonverbal material.
2. Decline in other cognitive abilities. Characterized by deterioration in judgment and thinking, such as planning and organizing, and in the general processing of information. Deterioration from a previously higher level of performance should be established.
3. Awareness of the environment. Absence of clouding of consciousness for a period of time sufficiently long to allow the unequivocal demonstration of decline in memory and other cognitive functions.
4. Decline in emotional control or motivation, or a change in social behavior. Changes are manifested in at least one of the following: (1) emotional lability, (2) irritability, (3) apathy, or (4) coarsening of social behavior.
5. Duration. Decline of memory and other cognitive functions must be present for at least six months.
IDC-10 Criteria for Alzheimer’s Disease 1. All criteria for dementia are met. 2. Exclusionary Criteria. No evidence from the history, physical examination or special investigations
for any other possible cause of dementia, a systemic disorder, or alcohol or drug abuse. 3. Onset and progression. For a diagnosis of Alzheimer’s disease, there must be evidence of gradual
onset and continuing cognitive decline.
23
PSYCHIATRIC IMPAIRMENT AND INTELLECTUAL DISABILITY
Overview
Historically, individuals with intellectual disability were assumed to be too psychologically primitive to develop psychiatric disorders (Herskovitz and Plesset, 1941). However research has shown that developmentally disabled/intellectually disabled persons experience the full range of mental illness (Sovner and DesNoyers-Hurley, 1983; Szymanski, 1977; Reid, 1972) and in fact are at increased risk for psychological problems.
The diagnosis of psychiatric impairments in individuals with intellectual disability is complex. Individuals presenting with behavioral or emotional disturbances may have significant intellectual and psychosocial deficits that influence the presentation of psychiatric symptoms and limit the use of traditional diagnostic criteria. Differential diagnosis can be enhanced when diagnostic criteria are adjusted to take into account the intellectual and psychosocial limitations of ID adults, diagnostic “behavioral equivalents” are emphasized and by paying careful attention to course.
Prevalence Rates of Psychiatric Disorders in Adults with ID
Psychiatric disorders have been found to be two to four times more common in the DD/ID population than the general population (Eaton and Menolascino, 1982; Cooper and Bailey, 2001; Clay and Thomas, 2005). Burt (1999) provides a summary of a number of studies of the prevalence rates for anxiety, depression, manic depression, schizophrenia and personality disorder for ID adults below.
Prevalence Rates for Psychiatric Diagnoses in Adults with ID Anxiety 1-25% Depression 5-67% Manic Depression Rare, 7 cases with DS reported Schizophrenia 21-24% Personality Disorder 15-35%
Depression in Adults with Intellectual Disability
Depression is by far the most prevalent of the psychiatric diagnoses in ID and more common in DS than non-DS intellectual disability. Particularly for Down syndrome persons, depression often presents as behavioral change such as withdrawal, loss of adaptive living skills and observable change in mood. In addition to mood changes, concurrent severe behavior problems and psychotic features are common manifestations of depression. In cases of major depressive disorder of mild severity, mild to moderate impairments in social relationship may be noted as well as in work and school functioning or daily living skills. Symptoms can last, on average, as long as one year (McGuire and Chicoine, 1996).
In more severe cases of depression debilitating impairments are seen in at least two functional areas of social relations, work or school activities or ADL’s. A usual pattern in severe cases includes isolation from social relationships, job loss or extended work absence and significant reduction in self-care and daily living skills. Psychotic features are commonly observed and characterized by extreme withdrawal

24
and trance-like stupor, delusions and hallucinatory-like conversations with self and imaginary others (self-talk or soliloquy). While it is common for individuals with Down syndrome to engage in self-talk, the incidence of such behavior may become more numerous, extreme and public. Their conversations with themselves or imaginary others may become more animated, angry in content and seemingly oblivious to the presence of others and a social convention. Symptoms of severe major depression can last anywhere from two to three years (McGuire & Chicoine, 1996).
Co-existing anxiety, behavioral disturbance (verbal/physical aggressiveness, self-injurious behavior, self-stimulating behavior, ritualistic behavior) and OCD are common at all levels of depression.
Life Stress
Loss and life stress are common triggers for psychological disorders, especially depression. Carers often do not believe individuals with ID understand the concept of death and minimize its effects. Typically, ID adults report distress over sadness, even if they do not understand the concept of death completely (Burt, 2008-b).
Since individuals with ID have limited ability to self-report their experience of personal loss, it is vitally important for clinicians to look for the presence of psychosocial stressors that may be correlated in time with the onset or persistence of any concerning changes in behavior that could be suggestive of a mental disorder or dementia.
One of the most common and impactful stressors is the loss or serious illness of a parent or close friend. That a life event such as this can often precipitate a major depressive episode is not surprising when one considers that an illness of a parent may pose significant stress to a dependent adult ID person living at home. The effect of a stressful life event such as this are often additive (Cooper, 2016), e.g. the death of a parent or primary care provider can lead to changes in residence, a move from familiar neighborhood and work or day service programs, loss of previous social networks, and accompanied by changes in personal cares that are being provided by a stranger, and may lead to having to share a new home with new people and a new routine.
Psychosocial stressors experienced by persons with ID might cause behavioral and emotional reactions that can be mistaken for serious mental disorders (Hurley et al. 2007). Sovner & Hurley (1986) note that adults with ID can be “exquisitely vulnerable to stress-induced intellectual and emotional decompensation producing breakdowns in reality testing that result in brief reactive psychoses in response to apparent minimal stress.” Sovner & Hurley (1993) referred to these transient psychotic states which often remit when the stress subsides, as “psychotoform” to reflect the fact the changes resemble features of psychosis but non-psychotic disorders cannot be ruled out.
It is also important for carers working with adults with ID to be cognizant of possible stressful life events to determine if stress or loss may be factors in the individuals’ mood or behavioral presentation. In addition to those cited above, common stressors to consider include: transitions from educational system to residential or vocational system; changes in work routine; disruptions at home; staff turnover at home or work; new personal relationships; changes in the frequency of family visits or the quality of

25
interactions; other non-specific but day-to-day interpersonal challenges (hearing people argue, being interrupted, not being “quick enough”); and anniversary dates of losses. Systematic use of a stress index such as that proposed by Burt (2008-c) and adapted by Lunsky and Bramston, 2006) may be of use as they are geared to people with ID. See also Health Issues for Adults with Down Syndrome (Chicoine et al., 2002) and The Groove by Dennis McGuire (Burt, 2008-d) for additional insight on the impact of lifestyle disruption on persons with ID.

26
DIAGNOSIS OF PSYCHIATRIC DISORDERS IN ADULTS WITH ID
Diagnostic Overshadowing
The diagnosis of psychiatric impairments in the DD/ID population is complex and a number of factors can influence clinical inference in the diagnostic process leading to misdiagnosis. Given that there is a high rate of maladaptive behaviors at baseline for this population a general diagnostic issue has been the tendency for clinicians unfamiliar with the population of persons with ID to attribute all behavioral problems to an individual’s intellectual handicap. Reiss et al. (1982) referred to this phenomenon as diagnostic overshadowing. Another common clinical bias in diagnosing psychiatric disorders in persons with ID is to assume that a change in behavior is due to mental health causes without considering other potential medical factors underlying the symptoms or complaints (Hurley et al 2007).
Impact of Intellectual Disability on the Presentation of Psychiatric Disorders
Sovner (1986) has identified four additional nonspecific factors associated with developmental disabilities/intellectual disabilities which influence the diagnostic process and limit the use of traditional diagnostic criteria.
Psychosocial Masking – Impoverished social skills and limited range of life experiences results in unsophisticated clinical presentation, e.g., in a manic episode an intellectually normal individual might hold a grandiose notion he is God, whereas an adult with ID might think he is not intellectually disabled.
Baseline Exaggeration – Increases in the frequency and intensity of pre-existing maladaptive behaviors (e.g. physical or verbal aggression, self-injurious behavior, self-stimulating behavior) during the course of a mental illness may be the prominent features and are often the chief presenting complaint prompting clinical attention. Signs and symptoms of psychiatric illness may thus represent a mix of new behaviors and/or an increase in the severity of pre-existing ones.
Cognitive Disintegration – This refers to the tendency for ID persons to become emotionally and cognitively disorganized when under stress, leaving them vulnerable to breakdowns in reality testing. If superimposed on a psychiatric illness such as depression the effects of the cognitive disintegration may make them susceptible to mood-congruent hallucinations and delusions and behavioral regression. Sovner & Hurley, (1993), referred to this tendency to hallucinate under stress as a psychotoform phenomenon. This seemingly bizarre presentation may be misdiagnosed as schizophrenia.
Intellectual Distortion – Traditional/standard diagnostic criteria and assessment procedures rely heavily on the ability to self-report subjective feelings, but persons with ID/DD often lack the requisite verbal and conceptual skills to communicate their psychological status due to their baseline intellectual limitations. Unless clinicians are able to rely on indirect means of evaluating psychological disorders, such as utilizing diagnostic/behavioral equivalents (Sovner and Hurley, 1982; Hurley et al 2007), they may misinterpret the ID person’s clinical presentation.

27
Why Is This Important?
The significance of a misdiagnosed or untreated psychiatric disorder cannot be understated. There is a strong association between psychiatric disorders and behavioral problems. If not carefully evaluated, hallucinatory-like self-talk and behavioral regression that can accompany a depressive disorder, for example, may be inaccurately diagnosed and treated as a psychotic disorder. Psychiatric impairments share many overlapping symptoms with Alzheimer disease and are associated with significant decline in intellectual, memory, language and adaptive function. Thus, it can be difficult to differentiate the effects of psychiatric impairments from that of a possible dementia. Finally there is some evidence to suggest that psychiatric impairments, depression in particular, may serve as prodromal syndrome for a later developing progressive dementia in Down Syndrome (Burt et al, 1992). Therefore it is critically important to consider the diagnosis of depression and other psychiatric impairments before assuming the presence of dementia of the Alzheimer’s type in persons with DD/ID.
While assessment of psychiatric impairments in DD/ID adults can be challenging, differential diagnosis can be enhanced when diagnostic criteria are adjusted to account for the adaptive and expressive limitations of ID adults; behavioral changes are emphasized as opposed to subjective feelings; other medical problems are ruled out; and by paying close attention to a clinical course (McGuire and Chicoine, 1996). With respect to the differentiation of depression versus Alzheimer’s disease, generally speaking, individuals with ID with depression will tend to show an up and down course with regard to their cognitive and functional status while individuals with dementia will eventually show progressive decline.
Diagnostic Criteria for Psychopathology in DD/ID Persons
There are no widely accepted diagnostic criteria or scales for use in the diagnosis of depression- or other psychiatric impairments for that matter- in adults with ID. A number of diagnostic schemes have been proposed. Two promising multiaxial diagnostic systems designed for use with ID/DD persons are the Diagnostic Criteria for Psychiatric Disorders for Use with Adults with Learning Disabilities (DC-LD) (Royal College of Psychiatrists, 2001); and the Diagnostic Manual-Intellectual Disability (DM-ID), (Fletcher et al., 2007) Other authors have developed psychiatric disorder specific diagnostic behavioral equivalents for depression (Sovner & Hurley, 1982; Reiss et al, 1982; Smiley and Cooper, 2003); anxiety (McGuire and Chicoine, 1996); manic depression (Sovner & Hurley, 1982); and schizophrenia ( Meyers and Pueschel, 1993); that may be helpful.
One useful set of criteria for diagnosis of depression relies on observable symptoms of depression that have been reported in the literature for adults with mental retardation and is based on a revised version of the Mood Assessment Scale for Demented Adults (Sunderland et al, 1988). The adapted diagnostic criteria for this Mood Assessment Scale-caregiver report (Burt, 1999) are as follows:

28
OBSERVABLE SYMPTOMS OF DEPRESSION IN ADULTS WITH MENTAL RETARDATION
Core symptoms suggesting depression
Looks sad, down-cast, preoccupied or tearful No longer initiates or participates in activities
previously enjoyed Gets irritable or upset easily, more than
expected for a given situation Looks restless or agitated
Additional symptoms
Looks sleepy or drowsy during the day Has trouble falling asleep, staying asleep or
waking too early Has had a decrease or increase in eating Complains about feeling bad or needing to go
to the doctor Looks anxious or concerned about something Has a low energy level Had reduced physical and facial expressiveness
to external stimuli No longer enjoys previously enjoyed activities Frequently asks for assistance regardless of
need for help Speech has changed in terms of tone, rate,
spontaneity, loudness Has noticeable difference in mood throughout
the day Repeatedly does something to hurt him/herself Sits and stares or sits stiffly Looks slowed down Physically or verbally aggressive Loss of daily living skills Looks fearful
Recommended criteria for diagnosis of depression in ID is the presence of at least one core symptom, plus 4 additional symptoms present for a minimum of 2 weeks, resulting in significant impairment in daily function, and with other causes being ruled out.
A number of global measures of psychopathology have been developed or adapted for use with the DD/ID population. These instruments are described elsewhere in this toolkit. In some complex cases, application of behavioral assessment methodologies (i.e. Applied Behavior Analysis) may be useful as an

29
aid in diagnosing psychiatric disorders, particularly affective disorders and behavior problems (Sovner & Lowry, 1990).
Assessment of Psychiatric Status
Psychiatric assessment should include all aspects of a standard psychiatric assessment used with the general population plus additional biopsychosocial and developmental considerations relevant to people with DD/ID. For a detailed discussion of these considerations see Cooper (2016); Hurley et al, 2007; Fletcher et al. 2007). Sovner and Hurley (1993) also provide an easy to use and succinct psychiatric consultation information form for use with persons with developmental disability.
Special Considerations for the Diagnostic Interview with Individuals with Intellectual Disability
Because of the limitations cited above, special care is needed when interacting with persons with ID in the diagnostic setting. The following recommendations are provided (Moran, 2013; Hurley et al,2007; Cooper, 2016) to give guidance on the matter:
Assessment Environment
Use relaxed and familiar environment
Remove physical barriers
Position self to allow communication with the person and the carer
Maintain a noise free/distraction free environment
Allow plenty of time
Nonverbal communication
Establish and maintain eye contact
Be friendly and relaxed; smile
Use a gentle tone of voice
Maintain a relaxed and open posture
Convey an easy going manner
Remain calm to provide reassurance
Be patient and supportive
Allow plenty of time

30
Verbal Communication
Use simple vocabulary
Speak slowly and clearly
Use short sentences
Ask one question at a time
Wait for an answer before proceeding
Check back with the person that the question was correctly understood; if unclear, repeat and rephrase
Avoid framing questions in a yes/no format if at all possible
If a yay-saying or nay-saying response pattern is suspected, use double dissociation questions to clarify consistency and reliability of responses.

31
Assessment-A Baseline Comparison Approach to Diagnosis of Dementia in ID The diagnosis of dementia in individuals with intellectual disability requires a change in status from baseline functioning, not a change from a normal level of functioning (as with the general population). Longitudinal assessment that documents baseline or best level of functioning in addition to changes in cognitive and behavioral functioning over time is necessary before sufficient information can be obtained to form a diagnosis of dementia. Baseline functioning in individuals with intellectual disability is significantly more heterogeneous than the general population and individuals can have wide-ranging and varying baselines of strengths and weaknesses even within the same range of intellectual disability. In addition, people with intellectual disability can have a wide range of behavior problems typical for them. Assessing the clinical significance of such behaviors requires a comparison with typical adulthood functioning. For these reasons, a working group of dementia experts (Aylward et al, 1995) recommended use of a baseline comparison approach to diagnosis of dementia in ID. ID persons are screened when healthy to obtain a “best level” of baseline performance and then followed longitudinally, with periodic re-screenings to assess for change in status. The baseline comparison approach incorporates use of a combination of direct assessment measures and caregiver reports. Direct assessments are needed to document changes in neuropsychological status as caregivers are often not reliable in reporting memory and cognitive functioning. Conversely, caregiver reports are required to document that any declines in memory and cognitive function are significant enough to affect daily functioning. A number of direct assessment measures have been developed or adapted for use with the ID population. While these instruments can provide objective evidence of current cognitive function, they are not without their limitations. Even though the measures have been developed for use with the ID population, floor effects are present to varying degrees and the instruments may be of limited use with individuals with severe intellectual disability or limited verbal ability. A number of indirect measures have also been adapted for use with the ID population. However, these measures must also be interpreted with caution as aging informants may be developing cognitive difficulties themselves, limiting accuracy, or caregivers may know the subject too well or not well enough to be objective. It is recommended that multiple informants across several different settings be utilized. In addition, while many observer-rated indirect measures include coverage of cognitive domains of function in their measures, indirect assessments do not assess cognition directly. Ultimately, a combination of direct and indirect assessment measures is likely to provide the highest sensitivity and specificity. There are a variety of different tools used for the assessment of dementia in ID, but as Zeilinger et al (2013) found a number of the measures were neither designed for assessment of dementia nor for persons with ID! It is therefore recommended that clinicians select only those instruments designed or adapted for use in detecting dementia in ID and that the measures are valid and reliable, sensitive to change early and throughout the course of dementia and measure a wide range of neuropsychological domains. See Elliott-King J. et al (2016) for a critical review of numerous instruments used in the diagnosis of dementia in adults with ID.

32
Assessment Measures Below are listed some of the more commonly used direct and indirect assessment measures for use with the ID population. Observer-rated scales observed below include:
Dementia Scale of Down Syndrome (DSDS) (Gedye, 1995) Dementia Questionnaire for Mentally Retarded Persons (DMR) (Evenhuis, 1992) Camdex-DS (Hon et al. 1999; Ball et al, 2006) Dementia Screening Questionnaire for Individuals with Intellectual Disabilities (DSQIID)(Deb et
al., 2007)
Dementia Scale for Down Syndrome (DSDS): The Dementia Scale for Down Syndrome (Gedye, 1995) is an informant-based instrument designed to aid in the diagnosis of dementia in adults with ID, especially DS. It is also used to establish a baseline for those at risk. The items are grouped into early, middle, late and very late stages of dementia. The informant is asked to classify features as not applicable, absent or present and, if present, if the feature is typical or atypical of the adult. New features are tallied for each stage along with a separate tally of cognitive signs and then compared to criteria for diagnosis and staging. The DSDS provides a differential diagnosis screening questionnaire section to address other potential causes for dementia. The DSDS has been found to have good sensitivity and specificity. It is comprehensive but contains no measure of general disability. It correlates well with other observer rated instruments. It has use restrictions limited to psychologists and psychometrists with two years of experience in dementia evaluation. Order forms for the DSDS booklets and manual can be obtained at http://www.gedye.ca/ Dementia Questionnaire for Mentally Retarded Persons (DMR): The Dementia Questionnaire for Mentally Retarded Persons (Evenhuis, 1992) is an English translation of the work of Heleen Evenhuis, an ID physician from the Netherlands. It was designed to facilitate a diagnosis of dementia in ID. It is described as a “screening instrument” for selection of persons for further specialist diagnostic assessment. The DMR is based on observation of caregivers over the previous two months. It consists of 50 items and 8 subscales divided into 2 subcategories. The cognitive subcategory covers short-term and long-term memory, as well as spatial and temporal orientation, while the social subcategory covers speech, practical skills, mood, activities, interests and behaviors. There are three response categories, 0 (no deficit) to 2 (severe deficit). It provides a usual measure of general disability. It is generally quick and easy to use (15-20 minutes) and there is a short form available. It does, however, have floor effects with advanced dementia and is not considered an appropriate instrument for single application. It is applicable for individuals with the mental ages of 2-10 but is not appropriate for individuals with profound or severe ID with other severe physical, motor or hearing impairments. The DMR does not have use restrictions nor is specialized administrative training required. To obtain test materials go to www.harcourt.nl

33
Cambridge Examination of Mental Disorders of the Elderly-Down Syndrome (CAMDEX-DS): The Camdex-DS (Hon et al.,1999; Ball et al., 2006) is a modified version of the Cambridge Exam for Mental Disorders of the Elderly used to document increasing prevalence with age. The author notes that the aims (in part) were to incorporate in a single schedule all the information necessary to enable an accurate clinical diagnosis of dementia with people with ID, but caution that it is not to be viewed as a substitute but rather an aide to the diagnostic process. The Camdex-DS is designed for use in the community by trained healthcare professionals. It is considered a test battery for comprehensive assessment that can be somewhat time-consuming. It is structured about areas of function likely to change with the onset of dementia. The measure contains informant interview and direct cognitive assessment (the CAMCOG-to be detailed later), patient interview and a standardized schedule for recording observations, physical exam and information on labs. It also collects information on cognitive and functional decline, current mental and physical health and best level of functioning. It has generally good reliability and predictive validity but is susceptible to floor effects in more significantly impaired individuals. Test materials available at Cambridge University Press. (Cambridge.org) Dementia Screening Questionnaire for Individuals with Intellectual Disability (DSQIID): The Dementia Screening Questionnaire for Individuals with Intellectual Disabilities (Deb et al. 2007) was designed as a user friendly, observer rated dementia screening developed to overcome the floor effects of existing dementia screening scales. It was derived from interviews with caregivers of adults with DS and dementia. It was then validated on a large sample. It consists of 53 items in 3 parts. Part 1 assesses “best” ability. Part 2 assesses behaviors and symptoms suggestive of dementia on a 4-point rating scale. Part 3 consists of 10 comparative questions answered on a yes/no basis. The DSQIID has very good sensitivity and specificity. It is quick and easy to score in any setting. Its single fixed cutoff may limit usefulness in adults with more advanced stages of dementia and with varying degrees of baseline intellectual disability. A copy of the test form and administrative instructions can be found in the original journal article. See reference list. Direct Neuropsychological Measures Direct neuropsychological measures commonly used for cognitive assessment and intellectual ability include the:
Test of Severe Impairment (TOSI) (Albert & Cohen, 1992) Cambridge Cognitive Examination-Down Syndrome (CAMCOG-DS) (Hon et al., 1999; Ball et al.,
2006) Institute for Behavioral Research Evaluation of Mental Status (IBREMS) (Wisniewski & Hill,
1985) Test of Severe Impairment (TOSI): The Test of Severe Impairment (Albert and Cohen, 1992) was originally designed as a downward extension of the MMSE to objectively assess patients with severe cognitive dysfunction (MMSE< 11/30), and was subsequently validated in persons with ID (Cosgrove et al, 2000). It assesses a range of skills involving motor, language, memory, conceptualization and general knowledge functions. Only eight questions require a verbal response. It is generally brief and easy to use and yields a range of scores that enables the measure to be applicable across a range of ID. Its psychometric properties are

34
generally good and have been correlated with tools that measure functional decline (DLSQ; NIH, 1989)) at baseline and diagnosis. Its degree of difficulty is appropriate for moderate to severe intellectual disability to score on unless they are in advanced stages of dementia. A copy of the test protocol is available in Prasher (2009). Cambridge Cognitive Examination-Down Syndrome (CAMCOG-DS): The CAMCOG-DS (Hon et all, 1999; Ball et al., 2006) is the self-contained neuropsychological component of the CAMDEX that was validated in subjects with DS. It is made up of seven subscales that measure orientation, language, memory, attention, praxis, abstraction and perception- functions that are known to decline in dementia. The authors state that the CAMCOG-DS enables examination of patterns and profiles of cognitive performance through subscale analysis. As a revised version it has expanded remote recall and executive function measures involving ideational fluency and visual reasoning. The authors report that it has few floor effects, and scores correlate with age. Available at Cambridge University Press. Cambridge.org. Institute for Behavioral Research Evaluation of Mental Status (IBREMS): On the IBR Evaluation of Mental Status (Wisniewski and Hill, 1985) adults respond to 37 items assessing orientation, language, short-term and long-term memory, writing, drawing and general knowledge. Recall and recognition format is provided. If an IQ is available when the individual was healthy, the IBREMS enables a cut-off score for assessment at a single point in time, but the IQ must be > 25. Caution is advised as when using this cut-off Silverman et. (2004) found a rather high rate of misclassification of non-demented subjects as demented patients(20%). The IBREMS has good sensitivity and specificity, otherwise. The test protocol and administration instructions are appended to the original journal article by Wisniewski and Hill (1985). See reference list. Adaptive Behavior Scales A number of adaptive behavior scales have been used for use in documenting declines in everyday function. Two commonly used instruments include the Adaptive Behavior Dementia Question (ABDQ) (Prasher et al., 2004) and the Daily Living Skills Questionnaire (DLSQ) (NIH, 1989). Adaptive Behavior Dementia Questionnaire (ABDQ): The ABDQ (Prasher et al., 2004) contains 15 items from the Adaptive Behavior Scales that were found to be strongly linked between declines in adaptive skills and aging and dementia in older adults with DS. Items are rated much worse, worse, the same, better, or much better than normal. Weighted scores are summed and compared to a cut-off. The ABDQ has good sensitivity and specificity. It is user friendly. It can be done on older DS adults regardless of ID or cooperation level, but it does not provide a measure of general disability. Test items and administration/scoring instructions are listed in the original journal article by Prasher et al (2004). A copy of the test materials is contained in Prasher, (2009).

35
Daily Living Skills Questionnaire (NIH, 1989): On the DLSQ (National Institute on Aging, 1989) informants provide information concerning a variety of ADL’s including dressing, grooming, eating, manual dexterity and geographical orientation. No significant floor effects were found. It has a high positive predictive value and correlates strongly with direct cognitive tests. The DLSQ can be found at NIA.NIH.gov

36
Indirect and Direct Screening Measures for Dementia O’Caoimh, et al, (2013)
CLASSIFICATION MEASURE ADVANTAGES DISADVANTAGES SENSITIVITY/SPECIFICITY FOR
AD IN DS REFERENCE
Observer-rated measures
DSDS
Comprehensive Measures change through course of dementia Includes differential diagnosis screening scale No significant floor effects Allows for staging of dementia
No measure of general disability Use restrictions Lengthy administration Reduced sensitivity with mild-moderate ID Scoring system is not simple
89% / 85% Gedye 1995
DMR
Applicable to mild, moderate and severe ID Includes a general measure of disability No restrictions on use Brief administration
Not applicable to severe ID with other severe disabilities
Requires repeat administration for valid results Ceiling/bottom effects with profound/ v. mild ID
92% / 92% Evenhuis (1992)
CAMDEX-DS
Comprehensive Includes a measure of general disability Incorporates 3-step assessment process that
facilitates formulation of differential diagnosis
Floor effects Lengthy administration
88% / 94% Ball et al. (2004)
DSQIID Validated in a large sample Brief administration Excellent IRR
Single fixed cut-off limits usefulness in more advanced stages of dementia and varying degree of baseline ID
92% / 91% Deb et al. (2007)
Neuropsychological tests
TOSI
Assess range of skills Only 8/24 items require a verbal response Brief/easy to administer Range of scores makes applicable across all levels of
ID IRR good
No measure of general disability Ceiling effect in mild ID
NA / NA Albert & Cohen (1992)
CAMCOG-DS
Assesses wide range of cognitive domains including remote recall and executive function
Subscale profile analysis Scores correlate with age Few floor effects
Limited diagnostic value at a single point in time. Not as sensitive with severe ID, severe sensory impairment or already advanced dementia
See CAMDEX-DS Ball et al. (2004)
*IBREMS Brief, easy to administer Enables cut-off score if IQ available when healthy.
Concentration subscale too difficult for many 90% / 89% Wisniewski and Hill (1985)
Measures of adaptive function
ABDQ
Can be completed on all ID adults regardless of level of ID or cooperation
User friendly Brief administration Screens for DAD in DS
No measure of general disability Cognition not assessed Utility with non-DSID unclear
89% / 94% Prasher et al. (2004)
DLSQ Correlates well with direct cognitive measures No floor effects
No assessment of cognition No measure of general disability
NA / NA National Institute
of Aging (1989)
*Test measure added to aid in comparison

37
SCREEN MEASURE
National Task Group-Early Detection Screen for Dementia (NTG-EDSD)
In addition to the above noted indirect and direct assessment measure for diagnosing dementia in ID, one additional screen measure is worth noting. The National Task Group – Early Detection Screen for Dementia (NTG-EDSD), Esralew et al (2013) offers carers and staff a resource to record changes in cognitive and adaptive function known to be associated with dementia. It is not an assessment or diagnostic instrument but rather an “administrative screen” that provides information to begin conversations with healthcare providers. It was adapted for use from the DSQIID (Deb et al, 2007). The EDSD gathers information on relevant demographics and ratings of health, mental health and life stressors. It reviews multiple domains of function and includes surveys of chronic health conditions. It also lists signal items that may reflect early signs of dementia. The EDSD can be helpful in training caregivers and staff to become good observers and reporters of information. It serves as a running record of health and function to be reviewed annually. In addition, it serves as a tool accessible to caregivers who are not trained to do assessment but who have valuable information about change in daily function. Measures of Adjustment, Emotional Functioning and Psychopathology A number of psychopathology scales have been developed for adults with ID. These instruments allow for making normative comparisons with symptoms that may fall outside the typical range and, in some cases, permit comparisons between self-report and informant ratings. These scales were not typically designed for use with individuals with possible comorbid dementia but may be used to document baseline symptoms (if screened early) and may be clinically useful to document change in status over time with serial reassessments. Psychopathology scales listed below include:
Emotional Problems Scale (Prout and Strohmer, 1991) Reiss Screen for Maladaptive Behavior (Reiss, 1988) DASH-2 (Matson, Gardner, Coe and Sovner, 1991; Sevin, Matson, Williams & Kirkpatrick-
Sanchez, 1995) Anxiety, Depression and Mood Scale (ADAMS) (Esbensen, Rohahn, Aman &Ruedrich,2003) Psychopathology Instrument for Mentally Retarded Adults (PIMRA) (Senatore, Matson & Kazdin,
1984) Emotional Problems Scale The Emotional Problems Scale (Prout and Strohmer, 1991) consists of two complimentary instruments designed for use as part of a comprehensive clinical evaluation of individuals aged 14 years and older with mild intellectual disability or borderline intelligence. The 135 item 4-point behavioral rating scale is used to indicate how often a client has exhibited specific behaviors during the previous 30 days including those reflective of thought/behavior disorder, verbal aggression, physical aggression, sexual maladjustment, distractibility, hyperactivity, somatic concerns, depression, withdrawal and low self-esteem. Broader scales assess externalizing and internalizing behavioral tendencies.

38
The 147 item self-report inventory uses a yes/no format and is written at a third grade reading level. The inventory is read to the individual and the authors claim that it can be completed by persons with very low reading levels and non-readers. The self-report inventory yields scores for positive impression, thought/behavior disorder, impulse control, anxiety, depression, low self-esteem and total pathology. Normative data were obtained on 673 and 704 individuals respectively for each of the two instruments. Results of the ratings are tallied and presented in normalized T-scores and percentile scores. Internal consistency and reliability coefficients ranged from .9 to .97 and from .77 to .96 respectively. The authors claim the EPS has been shown to be related to a variety of relative clinical variables. The EPS is available at: integratedassessments.com Reiss Screen for Maladaptive Behavior The Reiss Screen for Maladaptive Behavior (Reiss, 1988) screens for mental health problems in adolescents and adults with intellectual disabilities. Its empirically derived scales evaluate the probability that a person has an aggressive disorder, autism, avoidant disorder, dependent personality disorder, depression, paranoia and psychosis. The instrument also evaluates the probability of drug abuse, overactivity, self-injury, sexual problems, stealing and suicidal tendencies. The Reiss Screen is completed by caregivers, teachers, work supervisors or parents. Respondents rate the extent to which each of 38 symptoms is no problem, a problem or a major problem in the person’s life. Each item is defined in non-technical language and includes concrete examples. The test is normed for adolescents and adults aged 16 and up with all levels of severity of intellectual disability. The test screens for psychiatric disorder in three different ways: severity of challenging behavior, psychiatric diagnosis and rare but significant symptoms such as suicidal behavior. The author reports the total score that is generated reflects a measure of severity of disorder that is well-suited to assess progress over time. The author reports that the total scores are a valid indicator of whether or not a person with an intellectual disability also has a mental health problem. The eight scale scores also were reported to have a high degree of validity as well. Test materials may be obtained at: www.idspublishing.com. Diagnostic Assessment for the Severely Handicapped Scale -2 (DASH-2) The DASH-2 (Matson et al., 1991) was designed as a multi-dimensional instrument to assess the severity of individual symptoms as well as frequency and duration covering 13 major psychiatric disorders. It is intended to address psychiatric problems for profoundly and severely mentally retarded persons. Items comprising the DASH were derived from DSM-3-R and previously published studies and instruments and selected according to appropriateness for subjects with intellectual and adaptive abilities in the severe to profound ID levels and comprehensibility to informants without training in psychiatric assessment. A total of 83 items was included. The separate dimensions of behavior were selected for rating frequency, duration and severity and are scored on one of three levels: 0, 1 or 2. Ratings are requested based upon the subject’s behavior during the previous two weeks. Subscales included anxiety, mood disorder/depression, mood disorder/mania, pervasive developmental disorder- autism, schizophrenia, stereotypies/tics, self-injurious behavior, elimination disorders, eating disorders, sexual disorders, organic syndromes, impulse control and miscellaneous behavior problems. Data is collected on

39
symptom frequency, duration and severity in individual interviews with direct care staff. Interrater reliability was generally good. Test materials are available at: www.disabilityconsultants.org. Assessment Instrument for Anxiety, Depression and Mood Scale (ADAMS) The ADAMS (Esbensen et al, 2003) was designed as a comprehensive screening measure for anxiety and depression in persons with mental retardation. The measure consists of 55 items generated from DSM-4 criteria, previous assessment instruments and clinical experience that tap aspects of anxiety, fear, compulsiveness, appetite, communication, concentration, depression, energy level, mood, physical state, sleep disturbance and social interaction. Items are rated on a scale of 0 “not a problem” to 3 “severe problem” indicating the frequency and severity with which a particular behavior or symptom is present. Factor analysis indicated that it is generally a measure of manic/hyperactive behavior, depressed mood, social avoidance, generalized anxiety and compulsive behavior. Internal consistency of the subscales and retest reliability for both the total scale and subscales was high. Interrater reliability was satisfactory. The validity of the ADAMS was assessed with a clinical sample of 129 individuals with mental retardation who were seen in a psychiatric clinic, and this provided additional support for the subscales. The ADAMS was proposed as a psychometrically sound instrument for screening anxiety, depression and mood disorders among individuals with mental retardation. Publisher: Anna Esbensen, Ph.D. University of Wisconsin-Madison 1500 Highland Avenue Madison, WI 53705 608-263-5609 Psychopathology Instrument for Mentally Retarded Adults (PIMRA) The PIMRA (Senatore et al., 1985) was developed as a screening instrument to aid in the differential diagnosis of individuals with intellectual disability. The PIMRA includes a respondent version and an informant version. There are 56 items on the Informant version representing 7 classes of psychopathology including schizophrenia, affective disorders, psychosexual disorder, adjustment disorder, anxiety disorder, somatoform disorder and personality disorder based on DSM-III criteria. There is one additional subscale measuring inappropriate adjustment. Parents/caretakers familiar with the individual rates each item. The respondent version is adapted from the informant version and uses simpler, more concrete language. Both versions contain the same 8 scales. Test-Retest reliability was acceptable for the total scale but low to acceptable for the eight subscales. Validity was not well established for five of eight of the subscales. The PIMRA may be obtained at: www.disabilityconsultants.org.

40
PSYCHOPATHOLOGY INSTRUMENTSMEASURE P0PULATION/LEVEL OF ID INFORMANT SOURCE DOMAINS ASSESSED COMMENTS
EPS
Prout and Strohmer
(1991)
Borderline to M – Mod ID Age 14 and older
Caregiver & Self-Report Scales
Behavioral Rating Scale (BRS) o Caregiver ratings of frequency of
10 specific behavior dimensions past 30 days
o Two broader scales assessing internalizing/ externalizing behavior
Self-Report Inventory (SRI) o Yielding scales for positive
impression plus 5 areas of psychopathology plus a total pathology score
o Behavioral dimensions include thought/behavior disorder, verbal aggression, physical aggression, sexual maladjustment, distractibility, hyperactivity, somatic concerns, depression, withdrawal and low self-esteem
Yields profile of normalized T-scores allowing comparisons against a reference group
SRI can be completed by individuals with very low reading levels and non-readers
Reiss (1988) All levels of severity of ID Age 16 and older
Caregiver ratings 2 raters required
Caregivers rate the presence of 38 maladaptive behaviors during the past 3 months
Ratings then averaged and compared to norms for commonality
It produces 8 subscales: aggressive behavior, autism, psychosis, paranoia, depression--behavioral & physical signs, dependent personality disorder and avoidant personality disorder
Uses cut-off scores to determine if results positive for dual diagnoses signaling need for further mental health evaluation
No data on TRR Criteria validity established
DASH-II MATSON ET
AL (1991)
Severe to profound ID adults
Caretaker ratings Multidimensional instrument to assess severity, frequency and duration of symptoms covering 13 major psychiatric disorders—impulse control, organic problems, anxiety, mood disorder, mania, PDD/autism, schizophrenia, stereotypies/tics, self-injurious behavior, elimination disorder, eating disorder, sleep disorder, sexual disorders
Useful for identifying syndrome patterns
Provides systematic means of assessing psychopathology with severe to profound ID with good reliability
ADAMS Esbensen et
al (2003)
All ranges of ID Caregiver Comprised of 5 subscales: manic/hyperactive behavior, depressed mood, social avoidance, generalized anxiety, and compulsive behavior
28 items of the scale are rated on 0 to 3 point-scale from “not a problem” to “severe problem”
Psychometrically sound overall Narrow score limits usefulness for
anxiety, mania and depression Valid screening instrument for
bipolar disorder, depression and OCD but anxiety scale warrants further study—may not be independent construct due to overlap with other subscales
PRIMA Senatore et
al (1985)
Adults with full range of ID Respondent and informant version
Informant version contains 56 items derived from DSM-III classifications of psychopathology
Respondent version adopted from informant version using simpler concrete language
Each version consists of 8 subscales: schizophrenia, affective disorder, psychosexual disorder, adjustment disorder, anxiety disorder, somatoform disorder, personality disorder and poor mental adjustment
Test/Retest reliability acceptable for total scales but low to acceptable for 8 subscales
Further research needed to establish validity of some subscales

41
SUMMARY Individuals with intellectual disability (ID) are living longer and, as such, are at increased risk for age-related health conditions including dementia. With the rising life expectancy and growing population of persons with ID, clinicians and case workers can expect to encounter increasing numbers of persons with ID who develop dementia. Detecting dementia in intellectual disability populations is difficult due to their premorbid cognitive and psychosocial deficits, tendencies for dementia to present atypically in this population and their susceptibility to other medical problems that mimic dementia. Clinicians often lack adequate training in recognizing signs and symptoms of dementia in the ID population, and in conducting diagnostic assessments. Thus, there is a strong need for enhanced diagnostic processes and development of specialist assessment skills to meet this growing clinical demand. Personality and behavior changes often predate the onset of memory or other cognitive loss in ID dementia. Currently, there are no criteria specific to the diagnosis of dementia in ID. Criteria commonly used in the general population do not take into account the unique non-cognitive features of dementia in ID. Use of ICD-10 dementia diagnostic criteria is recommended as these criteria place greater emphasis on the non-cognitive aspects of dementia and employ a 2-step differential diagnostic process. Standard assessment measures used “at a single point in time” to document declines in function in the general population presume a normal level of premorbid functioning and are, thus, inappropriate for use with this population as many ID adults lack the skills to perform these tasks at baseline. Longitudinal assessment with measures appropriate for use with ID adults is required to document changes in status from a baseline or “personal best” level of function. Baseline screenings should ideally be done when healthy and periodically repeated. Comprehensive workups should be initiated when change is detected. The diagnosis of dementia in persons with intellectual disability is further complicated by the high prevalence of psychiatric and behavioral disorders that can mimic or compound the symptoms of dementia. Differential diagnosis can be enhanced by taking into account the adaptive and expressive limitations of adults with ID, emphasizing diagnostic behavioral equivalents, ruling out other medical causes and by paying careful attention to course. A number of neuropsychological assessment measures have been developed to aid in the clinical diagnosis of dementia in adults with ID. Combining direct assessment measures and observer-rated skills is likely to provide the highest sensitivity and specificity.

42
REFERENCES
Albert, M., & Cohen, D. (1992). The test of severe impairment: An instrument for the assessment of patients with severe cognitive dysfunction. Journal of American Geriatrics Society, 40, 449-453.
Alzheimer’s Association. (n.d.-a). Latest facts & figures report. Retrieved from
http://www.alz.org/facts/overview.asp. Alzheimer’s Association. (n.d.-b) Alzheimer's & Dementia Risk Factors. Retrieved from
http://www.alz.org/alzheimers_disease_causes_risk_factors.asp American Association on Intellectual and Developmental Disabilities (AAIDD. (n.d.). AAIDD Definition and
diagnostic criteria for Intellectual disability. Retrieved from http://aaidd.org/intellectual-disability/definition*. WRYITLIrK70.
American Psychiatric Association. (1994). Diagnostic and Statistical Manual of Mental Disorders, Fourth
Edition. Washington, DC, American Psychiatric Association. Aylward, E. H., Burt, D. B., Thorpe, L. U., Lai, F., & Dalton, A. J. (1995). Diagnosis of dementia in
individuals with intellectual disability. Washington, American Association on Mental Retardation.
Ball, S. L., Holland, A. J., Hon, J., Huppert, F. A., Treppner, P., & Watson, P. C. (2006). Personality and
behavior changes mark the early stages of alzheimer’s disease in adults with down syndrome: Findings from a prospective population-based study. International Journal of Geriatric Psychiatry, 21, 661-673. www.interscience.wiley.com, doi:101002/gps.1545.
Ball, S. L. , Holland, A. J., Treppner, P., Watson, P. C., & Huppert, F. A. (2008). Executive dysfunction and
its association with personality and behavior changes in the development of alzheimer’s disease in adults with down syndrome and mild to moderate learning disabilities. British Journal of Clinical Psychology, 47, 1-29. doi: 10.1348/014466507x230967.
Bittles, A. H., Peterson, B. A., Sullivan, S. G., Hussain, R., Glasson, E. J., & Montgomery, P. D. (2002). The
influence of intellectual disability on life expectancy. Journal of Gerontology: Medical Sciences, 57A(7), M470-M472.
Breitner, J. D. S., Wyse, B., Anthony , J., Welsh-Bohmer, K., Steffens, D., Norton, M., et al. (1999). APOE
E4 count predicts age when prevalence of AD increases, then declines. The Cache County Study. Neurology, 53, 321-331.
Brookmeyer, R., Corrada, M. M., Curriero, R. C., Kawas, C. (2002). Survival following a diagnosis of
alzheimer’s disease. Archives of Neurology, 59(11), 1764-1767.

43
Brookmeyer, R., Evans, D. A., Hebert, L., Langa, K. M., Heeringa, S. G., Plassman, B. L., & Kukull, W. A. (2011). National estimates of prevalence of alzheimer’s disease in the united states. Alzheimer’s & Dementia, 7(1), 61-73.
Brown, W. T. (1985). Genetics of aging. In M. P. Janicki & H. M. Wisniewski, H. M. (Eds.), Aging and
developmental disabilities: Issues and approaches (pp 185-194). Baltimore: Brookes. Burt, D. B., Loveland, K. A., & Lewis, K. R. (1992). Depression and the onset of dementia in adults with
mental retardation. American Journal of Mental Retardation, 96, 502-511. Burt, D. B. (2008-a). Depression. Understanding Adults with Intellectual Disability and Dementia:
Implications for Assessment. Day 1(C), 74-88. Professional Development and Applied Studies, Two-Day Conference, University of Wisconsin-Madison, Madison, WI.
Burt, D. B. (2008-b). Bereavement and Loss. Understanding Adults with Intellectual Disability and
Dementia: Implications for Assessment. Day 1(C), p87. Professional Development and Applied Studies, Two-Day Conference, University of Wisconsin-Madison, Madison, WI.
Burt, D. B. (2008-c). Stress Index. Understanding Adults with Intellectual Disability and Dementia:
Implications for Assessment. Day 2(Assessment Battery), p23. Professional Development and Applied Studies, Two-Day Conference, University of Wisconsin-Madison, Madison, WI.
Burt, D. B. (2008-d). The Groove. Understanding Adults with Intellectual Disability and Dementia:
Implications for Assessment. Day 1(A), 27-30. Professional Development and Applied Studies, Two-Day Conference, University of Wisconsin-Madison, Madison, WI.
Burt, D. B. (2013). Dementia & depression. In M. P. Janicki & A. J. Dalton (Eds), Dementia, aging and
intellectual disabilities: A handbook (pp 198-216). Routledge, New York. Center for Disease Control. (2012). World down syndrome day. Retrieved from
http://www.cdc.gov(ncbddd/birthdefects/features/down syndrome world day-2012.html Chicoine, B., McGuire, D. & Gratigny, S. (2002). Health issues for adults with DS. Research in Intellectual
Disabilities, 12, 1-10. Clay, J. & Thomas, J.C. (2005). Prevalence of Axis I psychopathology in an intellectually disabled
population: type of population and residential supports. Journal of Developmental and Physical Disabilities, 17(1), 75-84.
Cooper ,S-A, & Bailey,N.M. (2001). Psychiatric disorders amongst adults with learning disabilities-
prevalence and relationship to ability level. Irish Journal of Psychological Medicine, 18, 45-53. Cooper, S-A.(2016). Classification and assessment of psychiatric disorders in adults with intellectual
disabilities. Intellectual Disability and Health. Retrieved from http://www.intellectualdisability.info/mental-health/articles/classification-and-assessment-of-psychiatric-disorders-in-adults-with-intellectual-disabilities

44
Coppus, A. (2013, August 16). People with intellectual disability: What do we know about adulthood and life expectancy? Retrieved from http://onlinelibrary.wiley.com/doi/10.1002/ddrr.1123/abstract
Dalton, A.J., & Janicki, M.P. (2013). Aging and dementia. In M.P. Janicki & A.J. Dalton (eds) Dementia,
Aging and Intellectual Disabilities: A Handbook. (pp. 5-31). Routledge: New York. Dalton, A. J., Seltzer, G. B., Adlin, M. S., & Wisniewski, H. M. (1993). Association between alzheimer’s
disease and down syndrome: Clinical observations. In J. M. Berg, H Karlinsky, & A. J. Holland (Eds.), Alzheimer’s Disease, Down Syndrome and Their Relationship (pp 53-69). Oxford: Oxford University Press.
Dalton, A. J., & Wisniewski, H. M. (1990). Down syndrome and the dementia of alzheimer’s disease.
International Review of Psychiatry, 2, 41-50. Deb, S., Hare, M. A., Prior, L., & Bhaumik, S. (2007-a). Symptoms of dementia among adults with Down’s
Syndrome: A qualitative study. Journal of Intellectual Disability Research, 51(9), 726-739. Doi: 10.1111/j.1365-2788.2007.00956.x
Deb, S., Hare, M. A., Prior, L., & Bhaumik, S. (2007-b). Dementia screening questionnaire for individuals
with intellectual disabilities. British Journal of Psychiatry, 190, 440-444. Developmental Disabilities Assistance and Bill of Rights Act of 2000. Publication L, 106-402. From
http://www.act.hhs.gov/programs/add/DDACT2.htm Eaton, L. F., & Menolascino, F. J. (1982). Psychiatric disorders in the mentally retarded: Types, problems,
and challenges. American Journal of Psychiatry, 139, 1297-1303. Elliot-King, J., Shaw, S., Bandelow, S., Devshi, R., Kassam, S., Hogervorst, E. (2016). A critical literature
review of the effectiveness of various instruments in the diagnosis of dementia in adults with intellectual disabilities. Alzheimer’s & Dementia: Diagnosis, Assessment and Disease Monitoring. https://doi.org/10.1016/j.dadm.2016.06.002. (uncorrected proof). Accessed online 9/27/2016 at www.sciencedirect.com.
Esbensen, A. J., Rojahn, J., Aman, M. G., & Ruedrich, S. (2003). Reliability and validity of an assessment
instrument for anxiety, depression and mood among individuals with mental retardation. Journal of Autism and Developmental Disorders, 33(6), 617-629.
Esralew, L., Janicki, M. P., Disipio, M., Jokinen, N., & Keller, S. M. and Members of the National Task
Group Section on Early Detection and Screening. (2013). National Task Group Early Detection Screen for Dementia: Manual. Retrieved from www.aadmd.org/ntg/screening.
Evenhuis, H. M. (1992). Evaluation of a screening instrument for dementia in aging mentally retarded
persons. Journal of Intellectual Disability Research, 36, 337-447. Factor, A. R. (2004). Aging with a developmental disability. Listening session testimony for the 2005
White House Conference on Aging, Chicago, Illinois.

45
Fletcher, R., Loschen, E., Stavrakaki, C., First, M. (2007). Introduction. Diagnostic Manual-Intellectual Disability: A Textbook of Diagnosis of Mental Disorders in Persons with Intellectual Disability DM-ID, Kingston, NY: NADD (National Association for the Dually Diagnosed).
Fraser, J. & Mitchell, A. (1876). Kalmuc idiocy: report of a case with autopsy with notes on sixty-two
cases. Journal of Mental Science, 22, 169-179. Fratiglioni, L., Ahlbom, A., Viitanen, M., & Winblad, B. (1993). Risk factors for late- onset Alzheimer’s
disease: A population- based, case-control study. Annals of Neurology, 33(3), 258-266.
Gardner, R. C., & Yaffe, K. (2014). Traumatic brain injury may increase risk of young onset dementia. Annals of Neurology, 75(3), 339-341.
Gavett, B. E., Stern, R. A., Cantu, R. C., Nowinski, C. J., & Mckee, A. C. (2010). Mild traumatic brain injury: A risk factor for neurodegeneration. Alzheimers Research & Therapy, 2(3), 18. Retrieved from http://alzres.com/content/2/3/18.
Gedye, A. (1995). Dementia scale for down syndrome. Gedye Research and Consulting. Vancouver, British Columbia. Retrieved from http://www/gedue/ca/.
Goldgaber, D., Lerman, M. I., McBride, W. O., Saffiotti, U., & Gajdusek, D.C. (1987). Isolation,
characterization and chromosomal localization of human brain cDNA clones coding for the precursor of the amyloid of brain in alzheimer’s disease, down syndrome and aging. Journal of Neural Transmission ( Supplement), 24, 23-84.
Green, R. C., Cupples, L. A., Go, R., Benke, K., S., Edeki, T., Griffith, P. A., . . . Farrer, L. A. (2002). Risk of
dementia among White and African American relatives of patients with Alzheimer disease. Journal of the American Medical Association, 287(3), 329.
Heller, T. & Factor, A. (2004). Older adults with developmental disabilities and their aging family
caregivers. Chicago: RRTC on Aging with Developmental Disabilities, University of Chicago-Illinois.
Herskovitz, H.H. & Plesset, M.R. (1941). Psychoses in adult mental defectives. Psychiatric Quarterly, 15,
574-588. Hof, P.R., Bouras, C., Perl, D.P., Sparks, D.L., Mehta, N., Morrison, J.H. (1995). Age-related distribution of
neuropathologic changes in the cerebral cortex of patients with Down syndrome: Quantitative regional analysis and comparisons with Alzheimer’s disease. Archives of Neurology, 52, 379-391.
Holland, A.J., & Oliver, C. (1995). Down’s syndrome and the links with Alzheimer’s disease. Journal of
Neurology, Neurosurgery & Psychiatry, 59, 111-114. Hon, J., Huppert, F. A., Holland, A. J., & Watson, P. (1999). Neuropsychological assessment of older
adults with Down syndrome: An epidemiological study using the Cambridge Cognitive Examination (CAMCOG). British Journal of Clinical Psychology, 38:155-165.

46
Hurley, A. D., Levitas, A., Lecavalier, L., Pary, R. J. (2007). Assessment and Diagnostic Procedures. Diagnostic Manual-Intellectual Disability: A Textbook of Diagnosis of Mental Disorders in Persons with Intellectual Disability DM-ID, Kingston, NY: NADD.
Janicki, M.P., Dalton, A. J., Henderson, C. M., Davidson, P. W. (1999). Mortality and morbidity among
older adults with intellectual disability: Health services considerations [Abstract]. Disability and Rehabilitation, 21(5-6), 284-294.
Lai, F., & Williams, R. S. A. (1989). Prospective study of Alzheimer’s disease in down syndrome. Archives
of Neurology, 46, 849-853. Larson, S. L. et al., (2000) Prevalence of mental retardation and/or developmental disabilities: Analysis of
the 1994/1995 NHIS-D. MR/DD Data Brief. Minneapolis, MN: Institute on Community Integration, University of Minnesota.
Lautenschlager, N. T., Cupples, L. A., Rao, V. S., Auerbach, S. A., Becker, R., Burke, J., . . . Farrer, L. A.
(1996). Risk of dementia among relatives of Alzheimer’s disease patients in the MIRAGE study: What is in store for the oldest old? Neurology, 46(3), 641-650.
Lejeune, J., Gautier, M., Turpin, R., (1959-a). A study of somatic chromosomes from 9 mongoloid
children. CR Hebd Seances Acad Sci, 248, 1721-22. Lejeune, J., Gautier, M., Turpin, R. (1959-b). A study of somatic chromosomes in nine infants with
mongolism. CR Acad Sci, 240, 1026-1027. Lunsky, Y. & Bramston,P. (2006). A preliminary study of perceived stress in adults with intellectual
disabilities according to self-report and informant ratings. Journal of Intellectual and Developmental Disability, 31(1) 20-27.
Lye, T. C., Shores, E. A. (2000). Traumatic brain injury as a risk factor for Alzheimer’s disease: A review.
Neuropsychology Review, 10(2), 115-129. Madan, V., Williams, J., & Lean, J. T. (2006). Dermatological manifestations of down’s syndrome. Journal
of Clinical and Experimental Dermatology, 31, 623-629. Malamud, N. (1972). Neuropathology of organic brain syndromes associated with aging. In C. M. Gaitz
(Ed.), Aging Brain (pp. 63-87). New York, NY: Plenum. Mann, M.A., Yates, P.O., & Marcyniuk, B. (1984). Neuropathology and Applied Neurobiology, 10, 185-
207. Matson, J. L., Gardner, W. I., Coe, D. A., & Sovner, R. (1991). A scale for evaluating emotional disorder in
severely and profoundly mentally retarded persons: Development of the diagnostic assessment for the severely handicapped (DASH) scale. British Journal of Psychiatry, 159, 404-409.
Mayeux, R., Sano, M., Chen, J., Tatemichi, T., & Stern, Y. (1991). Risk of dementia in first-degree relatives
of patients with Alzheimer’s disease and related disorders. Archives of Neurology, 48(3), 269-273.

47
McCarron, M. (2004). Alzheimer’s dementia in persons with intellectual disability: Some common
questions and concerns. Dublin: NAMHI. Retrieved from http://hdl.handle.net/10147/337720. McGuire, D. E., & Chicoine, B. A. (1996) Depressive disorders in adults with down syndrome. The
Habilitative Mental Health Newsletter, 15(1). Minino, A., Heron, M. & Smith, B. (2006). Deaths: preliminary data for 2004. NCHS Health E-Stats:
Hyattsville, MD. Moran, J. A., Rafii, M.S., Keller, S. M., Singh, B. K., & Janicki, M. P. (2013). The national task group on
intellectual disabilities & dementia practices consensus recommendations for the evaluation and management of dementia in adults with intellectual disabilities. Mayo Clinic Proceedings, 88(8), 831-840. doi:10.1016/j.mayocp.2013.04.024
Mortimer, J. A., Duijn, C. M., Chandra, V., Fratiglioni, L., Graves, A. B., Heyman, A., . . . Soininen, H.
(1991). Head trauma as a risk factor for Alzheimers disease: A collaborative re-analysis of case-control studies. International Journal of Epidemiology, 20(Supplement 2), S28-S35.
Myers, B. M., & Pueschel, S. M. (1993, Nov. & Dec.). Differentiating schizophrenia from other mental
and behavioral disorders in persons with developmental disabilities. The Habilitative Mental Healthcare Newsletter, 12.
Nagdee, M. (2011). Dementia in intellectual disability: A review of diagnostic challenges. African Journal
of Psychiatry, 14, 194-199. National Down Syndrome Society (NDSS). (n.d.). Down Syndrome Facts. Retrieved from
http://www.ndss.org/down syndrome/down_syndrome_facts/. National Institute of Aging. (1989). The Daily Living Skills Questionnaire. Nemetz, P. N., Leibson, C., Naessens, J. M., Beard, M., Kokmen, E., Annegers, J. F., & Kurland, L. T.
(1999). Traumatic Brain Injury and Time to Onset of Alzheimers Disease: A Population-based Study. American Journal of Epidemiology, 149(1), 32-40.
Nordström, P., Michaëlsson, K., Gustafson, Y., & Nordström, A. (2014). Traumatic brain injury and young
onset dementia: A nationwide cohort study. Annals of Neurology, 75(3), 374-381. O’Caoimh, R., Clune, Y, & Malloy, D. M. (2013) Journal Alzheimer’s Disease and Parkinsonism, 57.
Retrieved from http://www.dx.doi.org/10.4172/2161-0460.S7-001. Penrose, L. S. (1949). The incidence of mongolism in the general population. Journal of Mental Science,
95, 685-688. Perkins, E. A., & Moran, J. A. (2010). Aging Adults With Intellectual Disabilities. Journal of the American
Medical Association, 304(1), 91. http://jama.jamanetwork.com/

48
Plassman, B. L., Havlik, R. J., Steffens, D. C., Helms, M. J., Newman, T. N., Drosdick, D., . . . Breitner, J. C. (2000). Documented head injury in early adulthood and risk of Alzheimers disease and other dementias. Neurology, 55(8), 1158-1166.
Prasher, V. P., Farooq, A., & Holder, R. (2004). The adaptive behavior dementia questionnaire (ABDQ):
Screening questionnaire for dementia in alzheimer’s disease in adults with down syndrome. Research in Developmental Disabilities, 25, 385-397.
Prasher, V. P., & Krishnan, V. H. R. (1993). Age of onset and duration of dementia in people with down
syndrome: Integration of 98 reported cases in the literature. International Journal of Geriatric Psychiatry, 8, 915-922.
Prout, H. T., & Strohmer, D. C. (1991). Emotional Problems Scale. Odessa, FL: Psychological Assessment
Resources, Inc. Reid, A. H. (1972). Psychoses in adult mental defectives: I. manic depressive psychosis. The British
Journal of Psychiatry, 120(555), 205-212.
Reiss, S., Levitan, G. W., & Szyszko, J. (1982). Emotional disturbance and mental retardation: Diagnostic overshadowing. American Journal of Mental Deficiency, 86(6), 567-574.
Reiss, S. (1988). Reiss Screen for Maladaptive Behavior Test Manual. Worthington, OH.: IDS Publishing Corporation.
Reynolds, T., Zupanick, C. E., & Dombeck, M. (2013-a). Diagnostic Criteria For Intellectual Disabilities:
DSM-5 Criteria. Retrieved July 10, 2017, from https://www.mentalhelp.net/articles/diagnostic-criteria-for-intellectual-disabilities-dsm-5-criteria/
Reynolds, T., Zupanick, E. E., Dombeck, M. (2013-b). The American Association On Intellectual And
Developmental Disabilities (AAIDD) Diagnostic Criteria For Intellectual Disability. Retrieved July 19, 2017, from http://www.mentalhelp.net/articles/the-american-association-on-intellectual-and-developmental-disabilities-aaidd-diagnostic-criteria-for-intellectual-disability/
Reynolds, T., Zupanick, E. E., Dombeck, M. (2013-c). Comparing The APA and the AAIDD Diagnostic
Criteria for Intellectual Disability. Retrieved July 10, 2017 from https://www.mentalhelp.net/articles/comparing-the-apa-and-the-aaidd-diagnostic-criteria-for-intellectual-diasability
Robakis, N. K., Wisniewski, H. M., Jenkins, E. C., Devine-Gage, E. A., Houck, G. E., . . . Brown, W. T. (1987).
Chromosome 21q21 sublocalisation of gene encoding beta-amyloid peptide in cerebral vessels and neuritic (senile) plaques of people with alzheimer’s disease and down syndrome. Lancet, 1, 384-385.
Rowe, J., Lavender, A., & Turk, V. (2006) Cognitive executive function in down syndrome. British Journal
of Clinical Psychology, 45, 5-17. doi:10.1348/014466505X29594. Royal College of Psychiatrists. (2001). DC-LD (Diagnostic Criteria for Psychiatric Disorders for Use with
Adults with Learning Disabilities/Mental Retardation). London: Gaskell.

49
Salib, E., & Hillier, V. (1997). Head injury and the risk of Alzheimer’s disease: A case control study.
International Journal of Geriatric Psychiatry, 12(3), 363-368. Schoenberg, M. R., & Duff, K. (2011). Dementia and Mild Cognitive Impairment in Adults. In M. R.
Schoenberg & J. G. Scott (eds.). The Little Black Book of Neuropsychology: A Syndrome-Based Approach. 14, 357-403. Springer Science & Business Media, LLC. . Doi 10.1007/978-0-387-76978-3_14,
Schupf, N. (2006). Genetics, alzheimer’s disease and down syndrome. In V. Prasher (Ed.), Down
Syndrome & Alzheimer’s Disease: Biologic Correlates (pp. 37-57). London, UK: Radcliffe Publishing.
Senatore, V., Matson, J. L., & Kazdin, A. E. (1985). An inventory to assess psychopathology of mentally
retarded adults. American Journal of Mental Deficiency, 89(5), 459-466. Sevin, J. A., Matson, J. L., Williams, D., & Kirkpatrick-Sanchez, S. (1995). Reliability of emotional
problems with the diagnostic assessment for the severely handicapped (DASH). British Journal of Clinical Psychology, 34(1), 93-4.
Silverman, W., Schupf, N., Zigman, W., Devenny, D., Miezejeski, C., Schubert, R., & Ryan, R. (2004).
Dementia in adults with mental retardation: Assessment at a single point in time. American Journal on Mental Retardation, 109(2).
Smiley, E., & Cooper, S. A. (2003). Intellectual disabilities, depressive episode, diagnostic criteria and
Psychiatric Disorders for Use with Adults with Learning Disabilities/Mental Retardation (DC-LD). Journal of Intellectual Disability Research, 47(Supp 1 Sept/Oct), 62-71.
Sovner, R., & Hurley, A. D. (1982). Diagnosing depression in the mentally retarded. Psychiatric Aspects of
Mental Retardation, 1, 1-3. Sovner, R., Hurley, A. D. (1982). Diagnosing Mania in the Mentally Retarded. Psychiatric Aspects of
Mental Retardation, 1, 8-11. Sovner, R., & Hurley, A.D. (1983). Do the mentally retarded suffer from affective illness? Archives of
General Psychiatry, 40, 61-67. Sovner, R., & DesNoyers-Hurley, A. (1986). Four factors affecting the diagnosis of psychiatric disorders in
mentally retarded persons. Psychiatric Aspects of Mental Retardations Reviews, 5(9). Sovner, R. (1986). Limiting factors in the use of DSM-III criteria with mentally ill/mentally retarded
persons. Psycho-Pharmacology Bulletin, 22(4), 1055-1059.
Sovner, R., & Lowry, M. A. (1990). A behavioral methodology for diagnosing affective disorders in individuals with mental retardation. The Habilitative Mental Healthcare Newsletter, 9.
Sovner, R. S. & Hurley, A., D. (1993). Psychotoform psychopathology. The Habilitative Mental Healthcare Newsletter, 112-113.

50
Sovner, R., & Hurley, A. D. (1993).The psychiatric consultation information form for persons with
developmental disabilities. The Habilitative Mental Healthcare Newsletter, 12(5).
Strub, R. L., & Black, F. W. (1989). Alzheimer’s/Senile Dementia Alzheimer’s Type. Neurobehavioral Disorders: A Clinical Approach, 6, 140-196. F. A. Davis Company: Philadelphia.
Strydom, A., Livingston, G., King, M., & Hassiotis, A. (2007). Prevalence of dementia in intellectual
disability using different diagnostic criteria. The British Journal of Psychiatry, 191(2), 150-157. Strydom, A., Shooshtari, S., Lee, L., Raykar, V., Torr, J., Tsiouris, J., . . . Maaskant, M. (June 2010).
Dementia in older adults with intellectual disabilities – Epidemiology, presentation & diagnosis. Journal of Policy & Practice in Intellectual Disabilities, 7(2), 96-110.
Strydom, A., Chan, T., King, M., Hassiotis, A., & Gill., L. (2013). Incidence of dementia in older adults with
intellectual disabilities. Research in Developmental Disabilities, 34, 1881-1885. Sunderland, T., Hill, J. L., Lawlor, B. A., & Molchan, S. E. (1988). NIMH dementia mood assessment scale
(DMAS). Psychopharmacology Bulletin, 24(4) 747-753. Szymanski, L. S. (1977). Psychiatric diagnosis evaluation of mentally retarded individuals. Journal of the
American Academy of Child Psychiatry, 16, 16-87. Tanzi, R. E., Gusella, J. F., Watkins, P. C., Bruns, G. A., St George-Hyslop, P., Van Keuren, M. L., . . . Neve,
R. L. (1987). Amyloid beta protein gene: cDNA, mRNA distribution and genetic linkage near the alzhiemer locus. Science, 235, 880-884.
The Arc. (1995). Developmental Disabilities & Alzheimer’s Disease: What You Should Know. The Arc of
the United States. Retrieved from https://www.thearc.org. The Arc. (2001). Q & A: Alzheimer’s Disease and People with Mental Retardation. Silver Spring, MD: The
Arc of the United States. Website: http//www.thearc.org. The Arc. (2011-a) Introduction to Intellectual Disability. From http://www.thearc.org/what-we-
do/resources/fact-sheet/introduction-to--intellectual-disability The Arc. (2011-b) Causes and Prevention of Intellectual Disability. From http://www.thearc.org/what-
we-do/resources/fact-sheet/causes-and-preventing US Public Health Service. (2002). Closing the Gap: A National Blueprint for Improving the Health of
Individuals with Mental Retardation: Report of the Surgeon General’s Conference on Health Disparities and Mental Retardation. Washington, DC: US Public Health Service.
Vincent, A. S., Roebuck-Spencer, T. M., & Cernich, A. (2014). Cognitive changes and dementia risk after
traumatic brain injury: Implications for aging military personnel. Alzheimers & Dementia, 10(3).

51
Welsh-Bohmer, K. A., & Warren, L. H. (2006) Neurodegenerative Dementias. In D. K. Attix & K. A. Welsh-Bohmer (eds.). Geriatric Neuropsychology: Assessment & Intervention, 3, pp. 56-88. Gilford Press: New York.
Wisniewski, K., & Hill, A. L. (1985). Clinical aspects of dementia in mental retardation & developmental
disabilities. In M.P. Janicki & H. M. Wisniewski (Eds.), Aging and developmental disabilities: Issues and approaches (pp195-206). Baltimore: Brookes.
World Health Organization (1992). ICD-10 International statistical classification of diseases & related
health problems. 10th Revision. Geneva:WHO. Zeilinger, E. L., Katharina, A. M., & Weber, G. A, (2013). A systematic review on assessment instruments
for dementia in persons with intellectual disabilities. Research in Developmental Disabilities, 34, 3962-3977.
Zigmen, W. B. (2013). Atypical aging in down syndrome. Developmental Disabilities Research Reviews,
18, 51-67. Zigman, W. B., & Lott, I. T. (2007). Alzheimer’s disease in down syndrome: Neurobiology and risk. Mental
Retardation and Developmental Disabilities Research Reviews, 13, 31-40. Zigmen, W., Schupf, N., Haveman, M., & Silverman, W. (1995). Epidemiology of alzheimer’s disease in
mental retardation: Results & recommendation from an international conference. Washington: American Association on Mental Retardation.
Other helpful resources: Janicki, M.P. & Dalton, A.J. (eds) (2013). Dementia, Aging and Intellectual Disabilities: A Handbook.
Routledge: New York. Jokinen, N., Janicki, M. P., Keller, S. M., McCallion, P., Force, L. T. and the National Task Group on
Intellectual Disabilities and Dementia Practices. (2013). Guidelines for structuring community care and supports for people with intellectual disabilities affected by dementia. Journal of Policy and Practice in Intellectual Disabilities, 10(1), 1-24.
Moran, J. A., Rafii, M. S., Keller, S. M., Singh, B. K., Janicki, M. P. (2013). The national task group on
intellectual disabilities and dementia practices consensus recommendations for the evaluation and management of dementia in adults with intellectual disabilities. Mayo Clinic Proceedings, 88(8), 831-840.
Moran, J. (2013). Aging and Down Syndrome: A Health and Well-being Guidebook. National Down
Syndrome Society. www.ndss.org. Prasher, V. P. (Ed). (2009) Neuropsychological assessments of dementia in down syndrome and
intellectual disabilities. London: Springer-Verlag.









![Multi-functionalized nanoparticles for therapy and diagnosis …...of dementia [Gotz, 2011] and affecting the middle- to old-aged individuals, approximately one in four individuals](https://img.pdfslide.us/doc/110x75/60be9eebd56c1d61c63f62cb/multi-functionalized-nanoparticles-for-therapy-and-diagnosis-of-dementia-gotz.jpg)



















