Assessing the Feasibility of Using Community Informant Networks
to Estimate Maternal Mortality in Pakistan Sharing Findings of a
Pilot Study March 31, 2014
Slide 2
Slide 2 of 56 Alternative Approaches to Measure Maternal
Mortality Methods: Civil registration with medical certification of
cause of deaths Sample Vital Registration with Verbal Autopsy
(SAVVY) Sisterhood method using Household surveys Direct estimation
(sibling method ) using Household surveys Census data Health
facility reporting of Maternal deaths Reproductive Age Mortality
Studies (RAMOS) Informant Listing and Follow-up Technique
(Made-in-Made-for)
Slide 3
Slide 3 of 56 Informant Listing and Follow-up Through Verbal
Autopsy Technique (Made-In Made-For) A research tool that
identifies pregnancy-related deaths in communities. Can be used as
a basis for estimating mortality at any level of sufficient size
from community to district, and national. Provides information on
the causes of mortality.
Slide 4
Slide 4 of 56 Informants listing of deaths(MADE-IN ):
Village-level informants identify deaths of women of reproductive
age (WRA) (aged 1549 years) in their communities. Follow-up with
verbal autopsies (MADE-FOR ): Follow- up interviews conducted with
family members of deceased women to confirm if deaths are maternal
or non-maternal and to explore cause of death. Two-Step
Process
Slide 5
Slide 5 of 56 Limitations of the Technique Cannot be used if
there are no suitable networks of informants Relies on the memory
of the family in describing the circumstances of a death. Deaths
early in pregnancy, and sensitive deaths (e.g. in unmarried women,
or following induced abortion) likely to be missed.
Slide 6
Slide 6 of 56 Pilot Study to Test the Feasibility of Applying
the Technique in Pakistan Primary Objective: To assess the
feasibility of applying the Community Informant Network Listing and
Follow-up with verbal autopsies (MADE-IN MADE-FOR) methodology in a
typical Pakistani district
Slide 7
Slide 7 of 56 Secondary Objectives: To identify the networks
available within rural and urban communities which can be key
informants for information on maternal deaths. To assess mechanisms
that can be employed at the community level to determine the cause
of deaths. To determine the differential characteristics and
geographical pattern of maternal deaths. Pilot Study to Test the
Feasibility of Applying the Technique in Pakistan
Slide 8
Slide 8 of 56 Timeline Activity 20132014 NovDecJanFebMarApr
Options Appraisal Field team selection & training Roll-out Data
entry and analysis Report Writing and Dissemination
Slide 9
Slide 9 of 56 Methodology Study Site: District Chakwal in
Punjab Province. Chakwal comprises four tehsils and has an
estimated population of nearly 1.4 million. 85 percent rural
population.
Slide 10
Slide 10 of 56 Map of District Chakwal
Slide 11
Slide 11 of 56 Key RH Indicators Chakwal District and Punjab
Indicator MICS 2011 PunjabChakwal Total Fertility Rate for women
age 15-19 3.582.51 Percentage of currently married women age 15-49
years who are using (or whose husband is using) a contraceptive
method 35.225.6 Percentage of currently married women aged 15-49
years with an unmet need for family planning 17.118.5 Percent
distribution of delivery by a skilled attendant (SBA) 58.574.9
Infant mortality rate 8261
Slide 14 of 56 Participation of Key Informants in Listing
Meetings: Made-In Step Type of Informant No. of Informants No. of
Listing Meetings Attendance Rate % Refusal Rate% LHW114361960 Lady
Councilors2005850 Nikah Registrars130121000 Religious
Leaders157768623
Slide 15
Slide 15 of 56 Glimpses of Network Listing Meetings to Identify
Deaths Among Women of Reproductive Ages
Slide 16
Slide 16 of 56 Glimpses of Follow-up Through Verbal Autopsy
Sessions
Slide 17
Slide 17 of 56 Number of Cases Found Cases Identified by
Village informant networks (MADE-IN) Recorded 2001 WRA deaths
(including 210 PRDs) Address not found: 94 Refused: 25 Duplicate:
74 Out of criteria Year: 135 Out of criteria Age: 249 Cases
followed up by Home visits and verbal autopsies (MADE-FOR) Total
number of WRA death cases interviewed: 1808 Final list of cases
identified Total number of WRA deaths followed up: 1424 Total
number of PRD cases: 169
Slide 18
Slide 18 of 56 Measures of Validity and Agreement Between Cases
Identified and Confirmed Through Verbal Autopsies MADE- FOR
PRDsNon- PRDs MADE- IN PRDs16618184 PPV 90% Non- PRDs 312371240 NPV
99% Total16912551424 Sensitivity 98% Specificity 99%
Slide 19
Slide 19 of 56 Ranking (%) of Major Causes of Deaths in Women
of Reproductive Age (n=1424)
Slide 20
Slide 20 of 56 Pregnancy Related Deaths by Tehsil Name of
Tehsil Number of Cases Population Case per Population
Chakwal83603,465 7270 Talagang46479,771 10429 Kallar
kahar22154,7777035 Choa Saidan Shah18133,2167400
Total1691,371,2298113
Slide 21
Slide 21 of 56 Geographical Distribution of Pregnancy Related
Deaths
Slide 22
Slide 22 of 56 Estimating Total Pregnancy Related Deaths
through the Capture and Re-capture Technique in Tehsil Chakwal and
Talagang 3428 M 10 LHW (N1= 62) RL (N2 38) RL (N2 26) LHW (N1= 37)
1918 M Chakwal Talagang T=N1xN2/M Total cases recorded in
Chakwal:72 The estimate based on CRC is 84 Total cases recorded in
Talagnag: 45 The estimate based on CRC is 53 8
Slide 23
Slide 23 of 56 Tehsil Probability of LHWs capturing deaths 95%
CI Probability of RLs capturing deaths 95% CI
Chakwal73%62-8245%34-56 Talagang70%56-8247%33-61 Probability of
LHWs vs. Religious Leaders Capturing Deaths in Chakwal and
Talagang
Slide 24
Slide 24 of 56 Probability of Capturing Deaths in Kallar Kahar
and Choa Sayeden Shah Tehsil Number of cases recorded Adjusted
number Choa Sayeden Shah1521 Kalarkahar2028
Slide 25
Slide 25 of 56 Probability of Reporting a Case by LHWs
Comparing Routine Reporting vs. Pilot Study Routine Reporting by
LHW Probability of LHWs in capturing a case in routine record 53%
95% CI: (46 60) Reporting by LHW in Pilot Study Probability of LHWs
in capturing a case in pilot study 73% 95% CI: (66 79) Added value
of reporting deaths by Religious Leaders= 18%
Slide 26
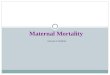
Slide 26 of 56 MMR Estimates for District Chakwal
PopulationnUnadjusted95% CI nAdjusted95% CI PRMR 58521169289 247 -
336 186318274 - 367 MMR (2 years) 58521165282 241 328 181309266 358
PMDF142416512% 10% - 13% 18113%11% - 15%
Slide 27
Slide 27 of 56 Age Specific Maternal Mortality Ratio Age
GroupPilot Study MMRPDHS 2006-7 15-19346242 20-24152210 25-29248267
30-34375246 35-39604657 40-44525855 45-49225234
Slide 28
Slide 28 of 56 Socio-Demographic Characteristics of PRDs Mean
age of respondents = 29 years
Slide 29
Slide 29 of 56 Proportion of Pregnancy Related Deaths by Socio-
Economic Status of Households with Deaths
Slide 30
Slide 30 of 56 Proportion of Pregnancy Related Deaths by Level
of Education of Women Who Died
Slide 31
Slide 31 of 56 Proportion of Pregnancy Related Deaths by
Cause
Slide 32
Slide 32 of 56 Distribution of Direct Causes of Maternal
Deaths
Slide 33
Slide 33 of 56 Care Seeking Behavior
Slide 34
Slide 34 of 56 Distribution of Antenatal Care Visits
Slide 35
Slide 35 of 56 Distribution of Type of Provider Giving
Antenatal Care
Slide 36
Slide 36 of 56 Distribution of those Who Received Antenatal
Care, by Type of Facility
Slide 37
Slide 37 of 56 Whether Certain Antenatal Care Services
Availed
Slide 38
Slide 38 of 56 Referral Advice During Antenatal Care
Slide 39
Slide 39 of 56 Distribution of Place of Referral
Slide 40
Slide 40 of 56 The Delay that Led to The Death Was it the
first, second, third or fourth delay?
Slide 41
Slide 41 of 56 Decision Making for Seeking Care
Slide 42
Slide 42 of 56 Time Taken to Make a Decision
Slide 43
Slide 43 of 56 Time Taken to Reach Health Facility
Slide 44
Slide 44 of 56 Proportion of Respondents Who Thought Treatment
Cost was Prohibitive
Slide 45
Slide 45 of 56 Perception whether Cost of Treatment was
Prohibitive by Socio-economic Status of Women
Slide 46
Slide 46 of 56 Difficulty in Arranging Funds for Treatment
Slide 47
Slide 47 of 56 Proportion of Pregnancy Related Deaths by
Location
Slide 48
Slide 48 of 56 The Tragedy Unfolding The Fourth Delay She was
first taken to the RHC from where they referred her to DHQ hospital
Chakwal. She reached the DHQ at 1.00 pm in the afternoon but
according to the family members she was not given attention by the
medical staff of the hospital till 7.00 pm. Then they were advised
to have an ultrasound from a private clinic. She was taken to the
labour room around 11.00 pm for a cesarean section. After cesarean
section she was again not cared for and she died in the
morning.
Slide 49
Slide 49 of 56 The Tragedy Unfolding The Fourth Delay She was
having her antenatal checkups done regularly from a lady doctor.
Her pregnancy was normal. She was taken to RHC for delivery. They
tried for normal delivery and then they did an Episiotomy but she
couldnt deliver. She was than referred to DHQ but without stitches
being applied and still bleeding. She died upon reaching DHQ
hospital.
Slide 50
Slide 50 of 56 The Tragedy Unfolding The Fourth Delay She was 9
months pregnant. Suddenly, she started bleeding. A local female
practitioner (nurse) was called who referred her to RHC. The staff
at RHC further referred her to DHQ after giving first aid. She was
bleeding continuously and in the same condition she was taken to
the DHQ hospital. The medical staff at DHQ referred her to
Rawalpindi. She died in transit.
Slide 51
Slide 51 of 56 The Tragedy Unfolding The Fourth Delay When
labor pains started, she was taken twice to the BHU. The LHV of the
BHU sent her back saying that there was still time for delivery.
When she was taken to the same facility a third time, she delivered
a dead baby girl and later died. According to the husband and other
people of the community, she died due to the carelessness of the
LHV.
Slide 52
Slide 52 of 56 The Tragedy Unfolding The Fourth Delay She
delivered in a private hospital. Placenta was not removed properly.
She kept on bleeding. She was referred to a tertiary care hospital
in Rawalpindi where she died.
Slide 53
Slide 53 of 56 Unfolding the Tragedy The Fourth Delay She
delivered at a private clinic. Episiotomy was in process when
load-shedding started. Generator was out of order. The torch of the
mobile phone was used for completing the surgery. She was bleeding
continuously and was taken to another facility but the bleeding did
not stop. Eventually, she died the same night.
Slide 54
Slide 54 of 56 Conclusions and Recommendations Maternal
mortality remains a major public health issue for Pakistan - the
problem may be much larger than we anticipate Reaching the
appropriate facility in the first place could have avoided the
unnecessary fourth delay LHWs are the best available source for
collecting maternal mortality data on a sustainable basis. A dual
model for collecting information on maternal deaths can enhance
accuracy, especially for areas not covered by LHWs.
Slide 55
Slide 55 of 56 Conclusions and Lessons Learnt The following can
be considered as good informant networks: -- Religious leaders
universally available need to be motivated. Nikkah Registrars a
good network but limited in numbers. Lady Councilors a good source
of information but few and not recently elected. For
sustainability, district administration should make it mandatory
for the Union Councils Secretaries to routinely collect data on
vital events including pregnancy related deaths.