Embed Size (px)
Citation preview

50 JCN 2016, Vol 30, No 5
RESPIRATORY CARE
An individual’s respiratory rate can be simply understood as the number of breaths they
take in one minute. Respiratory rate is an important vital sign that should be measured and recorded as part of the assessment of a patient.
Abnormal respiratory rates can be used to predict potentially serious clinical events such as cardiac arrest or admission to intensive care and help get patients the prompt treatment they need (Table 1) (Cretikos et al, 2008). Research into hospital assessments indicates that patients' respiratory rates are commonly omitted from checks of their four vital signs (pulse, temperature, blood pressure and respiratory rate) (Cretikos et al, 2008).
Pulse oximetry (a non-invasive technique that indirectly monitors the oxygen saturation of a patient's blood without the need for a blood sample) is not a replacement for checking the patient's respiratory rate (Table 2) as it is not always accurate due to reduced blood perfusion in the fingers or toes (where the device is attached)and does not measure adequate ventilation (Cretikos et al, 2008).
Assessing respiratory rate and function in the community
breathing, all of which can affect the patient in different ways. Tachypnoea, for instance, is used to describe fast, shallow breathing (Hadjiliadis, 2016), with a regular rate but usually over 20 breaths per minute (Mooney, 2007). Rapid, shallow breathing is a medical emergency that may require transfer to hospital, especially with any of the following symptoms (Hadjiliadis, 2016): A blue or grey colour to the skin,
nails, gums, lips or around the eyes Chest pain, the chest is pulling
in with each breath Fever Laboured breaths Where symptoms are new and/ or
increasing in severity.
Other types of respiratory rate include: Bradypnoea: slow breathing with a
regular rate of less than 12 breaths per minute (Mooney, 2007)
Apnoea: absence of breathing, potentially leading to respiratory arrest (Mooney, 2007)
Obstructive sleep apnoea: caused by intermittent, repeated upper airways collapse during sleep. This irregular breathing typically causes poor sleep at night and excessive drowsiness during the day (Tidy and Henderson, 2014)
Dyspnoea: difficulty breathing or shortness of breath (NHS Choices, 2015)
Paroxysmal nocturnal dyspnoea: shortness of breath that causes the person to wake up during sleep and have to sit upright to get their breath back (Tidy and Henderson, 2014).It is generally caused by pulmonary oedema resulting from left ventricular failure but night time asthma attacks may present in a similar way (Tidy and Henderson, 2014)
Air hunger: a term for the acute dyspnoea that occurs in the terminal stage of a life-threatening
Jaqui Walker, general practice nurse, and freelance medical writer
Respiration is vital for life and understanding how to assess patients' respiration and the different types of respiratory rate is a vital skill for all community nurses. Respiration rate is one of the four vital signs and should not be ignored when assessing a patient. This article explains the different types of respiration; provides clear guidance on how to assess respiration, and explores some of the causes of abnormal respiratory patterns and how they can be managed.
KEYWORDS:Respiration Vital signs Breathing Pulse oximetry
Jaqui Walker
ADULT RESPIRATORY RATES
Although respiratory rates vary with age and gender, for an adult at rest the respiratory rate should be between 8–16 breaths/minute (Hadjiliadis, 2016). More than 20 breaths/minute indicates that a patient is unwell (Cretikos et al, 2008); while over 24 breaths/minute indicates a patient is critically unwell (Cretikos et al, 2008).
Respiratory rate and tidal volume (the amount of air which enters the lungs during normal inhalation at rest), change as the body tries to balance oxygen and carbon dioxide levels and correct hypoxia (lack of oxygen reaching the tissues) and/or hypercarbia (abnormally elevated carbon dioxide levels in the blood).
Various conditions including abdominal pathologies such as intenstinal or pancreatic fistulae or sepsis (infection in the body's tissues) can cause metabolic acidosis (a condition where there is too much acid in the body's fluids), which increases the hydrogen ions and Co2 production and in turn increases breathing rate and volume (Cretikos et al, 2008).
DIFFERENT TYPES OF RESPIRATORY RATE
There are different types and rates of
© 2016
Wou
nd C
are Peo
ple Lt
d

GET IN THE ZONE
Easy-to-use, module formatSearchable by product category and name Tiered approach to learning about productsLearning activity counts to your revalidation requirementsLog your learning in our free revalidation e-portfolioDesktop, tablet and mobile-friendly
http://www.jcn.co.uk/learning-zone/
97% of community nurses prefer to access product information in one independent place*.
Learn about products relevant to your work in our Products in Practice area
Entries about specific productsHow they workUnique product featuresHow to use When to use Instructional videos Clinical evidence
THE NEW JCN DIGITAL LEARNING ZONE IS THAT PLACE
*JCN survey April 2016. n=983, answers in more than one category allowed
© 2016
Wou
nd C
are Peo
ple Lt
d
RESPIRATORY CARE
52 JCN 2016, Vol 30, No 5
haemorrhage. The patient requires an immediate blood transfusion (Tidy and Henderson, 2014)Kussmaul’s respiration: a deep sighing breathing that can be present with metabolic acidosis and which may be caused by diabetic ketoacidosis or chronic kidney disease (Tidy and Henderson, 2014).
Cheyne-StokesCheyne-Stokes or periodic respiration is a term used to describe deep, then shallow and very slow laboured breathing accompanied by periods of apnoea. Dying patients often experience Cheyne-Stoke breathing (Mooney, 2007). It also affects 50% of people with moderate-to-severe congestive heart failure (Tidy and Henderson, 2014). According to Tidy and Henderson (2014), typically 'over a period of one minute, a 10-to-20-second episode of apnoea or hypopnoea occurs
followed by respirations of increasing depth and frequency. The cycle then repeats itself.'
Cheyne-Stokes breathing can be caused by brain stem lesions such as a cerebrovascular event, encephalitis, raised intracranial pressure, heart failure, chronic pulmonary oedema and altitude sickness (Tidy and Henderson, 2014). It is treated by management of the underlying heart failure, continuous positive airway pressure (CPAP) and, if required, oxygen.
Hyperventilation Hyperventilation is a term for rapid deep breaths (Hadjiliadis, 2016), which may be caused by lung disease, anxiety, panic (Hadjiliadis, 2016), and pain (Mooney, 2007). Hyperventilation reduces carbon dioxide levels in the blood and may cause dizziness, light headedness, muscle spasms in the hands and feet and tingling in the mouth and fingers (Tidy and Henderson, 2014). It is commonly caused by anxiety, but can also result from a head injury, a cerebrovascular event and stimulant drugs including too much aspirin (Tidy and Henderson, 2014).
HypoventilationHypoventilation involves shallow or slow breathing that is not enough to meet the body’s needs, resulting in an increase in carbon dioxide and a decrease in oxygen levels (Tidy and Henderson, 2014). It can be caused by obesity, obstructive sleep apnoea, severe chest wall deformities, neuromuscular diseases that cause muscle weakness (e.g. myasthenia gravis, amyotrophic lateral sclerosis, Guilliain-Barré syndrome, muscular dystrophy), and severe chronic obstructive pulmonary disease (COPD) (Tidy and Henderson, 2014).
HOW TO ASSESS RESPIRATION
Accurately assessing a patients' respiratory rate can help diagnose disease, as well as setting a clinical baseline when monitoring patients with breathing problems or who are on medication that affects their breathing (Mooney, 2007).
As well as measuring the rate of breathing, the depth and pattern of respiration should be assessed, alongside the patient’s complexion, for example, are they blue/grey in pallor (possibly signifying a lack of oxygen) or red-faced (possibly signifying over-exertion) (Mooney, 2007). The respiration rate should be regular, with equal gaps between breaths (Mooney, 2007). A blue tinge to the lips, nail bed, tip of nose or ear lobes suggests the patient has cyanosis (not receiving enough oxygen).
The patient should be observed for 'mouth breathing' or pursing of
Flu vaccination £1,000/QALY in 'at risk' population
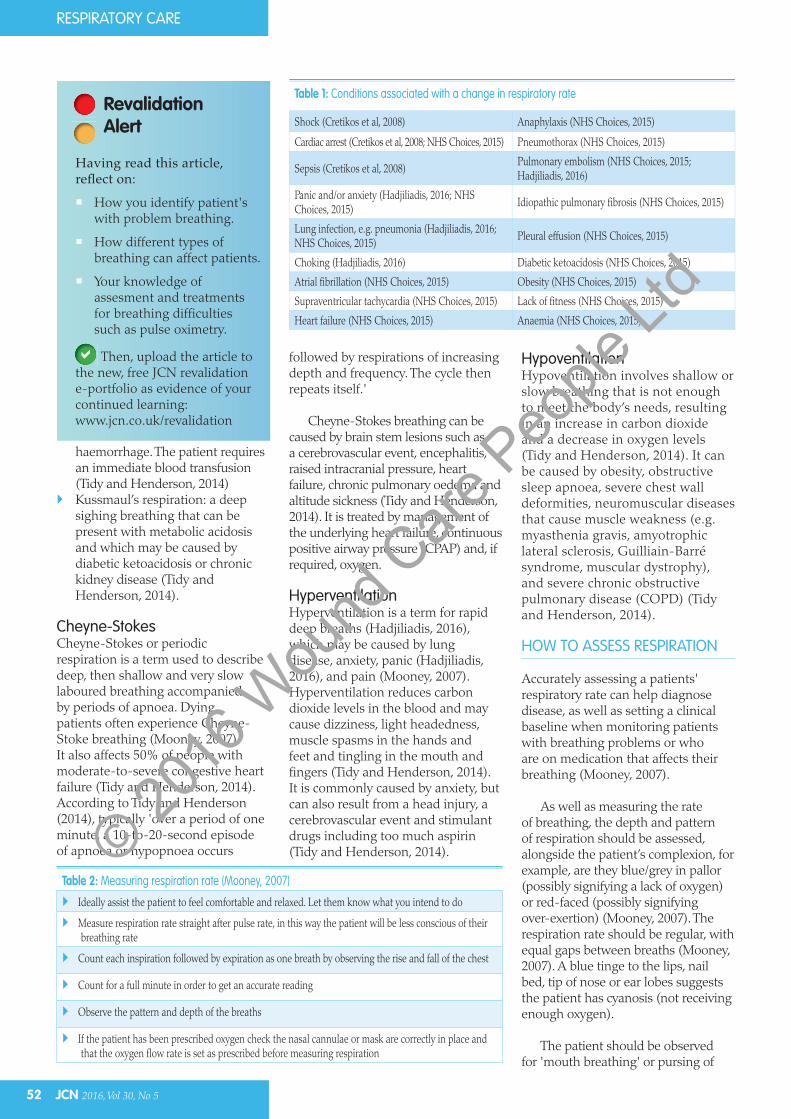
Table 2: Measuring respiration rate (Mooney, 2007)
Ideally assist the patient to feel comfortable and relaxed. Let them know what you intend to do
Measure respiration rate straight after pulse rate, in this way the patient will be less conscious of their breathing rate
Count each inspiration followed by expiration as one breath by observing the rise and fall of the chest
Count for a full minute in order to get an accurate reading
Observe the pattern and depth of the breaths
If the patient has been prescribed oxygen check the nasal cannulae or mask are correctly in place and that the oxygen flow rate is set as prescribed before measuring respiration
Table 1: Conditions associated with a change in respiratory rate
Shock (Cretikos et al, 2008) Anaphylaxis (NHS Choices, 2015)
Cardiac arrest (Cretikos et al, 2008; NHS Choices, 2015) Pneumothorax (NHS Choices, 2015)
Sepsis (Cretikos et al, 2008)Pulmonary embolism (NHS Choices, 2015; Hadjiliadis, 2016)
Panic and/or anxiety (Hadjiliadis, 2016; NHS Choices, 2015)
Idiopathic pulmonary fibrosis (NHS Choices, 2015)
Lung infection, e.g. pneumonia (Hadjiliadis, 2016; NHS Choices, 2015)
Pleural effusion (NHS Choices, 2015)
Choking (Hadjiliadis, 2016) Diabetic ketoacidosis (NHS Choices, 2015)
Atrial fibrillation (NHS Choices, 2015) Obesity (NHS Choices, 2015)
Supraventricular tachycardia (NHS Choices, 2015) Lack of fitness (NHS Choices, 2015)
Heart failure (NHS Choices, 2015) Anaemia (NHS Choices, 2015)
Having read this article,
How you identify patient's with problem breathing.
How different types of breathing can affect patients.
Your knowledge of assesment and treatments for breathing difficulties such as pulse oximetry.
Then, upload the article to the new, free JCN revalidation e-portfolio as evidence of your continued learning: www.jcn.co.uk/revalidation
RevalidationAlert
© 2016
Wou
nd C
are Peo
ple Lt
d

JCN 2016, Vol 30, No 5 53
RESPIRATORY CARE
the lips to breath out (a common sign that the airways are narrowed or collapsing, especially in COPD), use of the abdominal muscles to breath and flaring of the nostrils (Mooney, 2007).
Pulse oximetryPulse oximeters are portable and widely available at a relatively cheap cost. They can be used to measure a patient’s oxygen saturation (SaO2) and pulse, and work by measuring the oxygenation of the red blood cells in the finger tips, ear lobe or toe.
The measure can be inaccurate, for example, if the hands are cold, there is poor circulation and if
nail polish or false nails block the signal (Fahly et al, 2013). The pulse oximeter machine can also be inaccurate when oxygen saturation rates are below 80%; similarly, pulse oximetry may overestimate arterial oxyhaemoglobin saturation at low SaO2 levels in those with darker skin (Feiner et al, 2008; Fahly et al, 2013). To check the signal, count the pulse for a minute and compare this to the pulse rate on the pulse oximeter (Fahly et al, 2013).
Smoking also can result in an inaccurate reading due to the fact that smoking increases carbon monoxide blood levels and the pulse oximetry
machine cannot distinguish between oxygen and carbon monoxide in the blood leading to falsely elevated readings (Fahly et al, 2013). The SaO2 is a percentage of the amount of oxygen in the blood compared with the amount it is able to carry; a normal oxygen saturation rate is over 89% (Fahly et al, 2013).
MRC Dyspnoea scaleMeasuring the amount of breathlessness a person experiences with activity can be achieved using the Medical Research Council (MRC) dyspnoea score (www.mrc.ac.uk) (see Table 3). This score is simple to use and is often used as part of respiratory assessment by clinicians.
TREATMENT
While it does not fall within the remit of this article to cover treatment for respiratory conditions, treatment options for patients experiencing breathlesness will vary depending on the particular condition, for example, COPD, complications attached to palliative care or asthma, and may include oxygen therapy (which can be delivered in the home) or medications, such as steroids or anticholinergic drugs.
The community nurse should always perform a thorough assessment before considering any treatment and, as always, should refer to a respiratory specialist if in doubt.
Table 3: MRC Dyspnoea Scale (adapted from: Fletcher, 1952)
1: Not troubled by breathlessness except on strenuous exercise
2: Short of breath when hurrying on a level or when walking up a slight hill
3: Walks slower than most people on the level, stops after a mile or so, or stops after 15 minutes walking at own pace
4: Stops for breath after walking 100 yards, or after a few minutes on level ground
5: Too breathless to leave house, or breathless when dressing/undressing
Red Flag Symptoms
Fever
THE SCIENCE — RESPIRATORY DISEASE IN THE COMMUNITYCommunity nurses often encounter patients with chronic respiratory conditions. Any who complain of being breathless, are hypoxaemic and shows signs of peripheral cyanosis, or have a very limited exercise capacity, should have their resting oxygen saturation measured by pulse oximetry. This will help the community nurse decide whether
to refer the patient to a specialist oxygen service for assessment. Similarly, many older patients in the community will have a diagnosis of chronic lung disease and be using long-term oxygen therapy.
Patients who complain of breathlessness on exertion can be assessed with a pulse oximeter to see whether they are desaturating on exercise, which is often the first symptom described by patients with interstitial lung disease. Pulse oximetry measurement is helpful in assessing that patients' prescribed oxygen flow rates are correct, which may change over time as their condition deteriorates (here the nurse should always be prepared to request a specialist opinion, even if it is earlier than planned). Pulse oximeters are an affordable clinical assessment tool and could easily be added to the equipment that community nurses already use on an everyday basis.
Source: Murphie P (2015) Home oxygen therapy: an update for nurses. J Comm Nurs29(4): 55–9
Cre
dit:
SOC
IALi
sBET
TER
@fli
ckr.j
pg
© 2016
Wou
nd C
are Peo
ple Lt
d
RESPIRATORY CARE
KEY POINTS Respiration is vital for life and understanding how to assess patients'
respiration and the different types of respiratory rate is a vital skill for all community nurses.
Respiration rate is one of the four vital signs and should not be ignored when assessing a patient.
Many older patients in the community will have a diagnosis of chronic lung disease and be using long-term oxygen therapy.
This article explains the different types of respiration; provides clear guidance on how to assess respiration, and explores some of the causes of abnormal respiratory patterns and how they can be managed.
To receive your free copy, register at:www.journalofpracticenursing.co.uk
PRESCRIBINGPOLICY ACUTE CAREHEALTH PROMOTIONLONG-TERM CONDITIONS
Journal of General Practice Nursing
Journal of General Practice NursingPromoting practice to improve patient health and quality of life
CONCLUSION
Community nurses have an important role to play in assessing patient’s respiration rates, especially in recognising abnormal breathing patterns and understanding the causes of different types of breathing patterns. In this way abnormal breathing can be recognised and appropriate management promptly organised. JCN
REFERENCES Cretikos MA, Bellomo R, Hillman K, Chen
J, Finfer S, Flabouris A (2008) Respiratory rate: the neglected vital sign. Med J Aust 188(11): 657–9
Fahly B, Lareau S, Sockrider M (2013) Patient information series: pulse oximetry. American Thoracic Society Available at: www.thoracic.org/patients/patient-resources/resources/pulse-oximetry.pdf (accessed 5 Ocotber, 2016)
Feiner J, Severinghaus JW, Bickler PE (2008) Dark skin decreases the accuracy of pulse oximeters at low oxygen saturation: the effects of oximeter probe type and gender.
Anesthesia and Analgesia 105(6 Suppl): S18-23
Fletcher CM (1952) The clinical diagnosis of pulmonary emphysema: an experimental study. Proc R Soc Med 45: 577–84
Hadjiliadis D (2016) Rapid shallow breathing. Available at: https://medlineplus.gov/ency/article/007198.htm (accessed 5 Ocotber, 2016)
Mooney GP (2007) Respiratory assessment. How to accurately measure and record respiration rates. Nursing Times Available online: www.nursingtimes.net/clinical-
archive/respiratory-assessment/200191.fullarticle (accessed 5 Ocotber, 2016)
NHS Choices (2015) Shortness of breath. Available online: www.nhs.uk/Conditions/shortness-of-breath/Pages/introduction.aspx (accessed 5 Ocotber, 2016)
Tidy C, Henderson R (2014) Cheyne-Stokes and abnormal patterns of respiration. Available online: http://patient.info/doctor/cheyne-stokes-and-abnormal-patterns-of-respiration (accessed 5 Ocotber, 2016)
© 2016
Wou
nd C
are Peo
ple Lt
d