Embed Size (px)
Citation preview
AMERICAN SOCIETY FOR MICROBIOLOGY: EDUCATION DEPARTMENT
This handbook has been prepared to ease your transition into this unique relationship with ASM and NCID.
Handbook and Important Forms
ASM/NCID Research Fellowship Program
Application Deadline: January 15, 2006
CDC/NCID CENTERS FOR DISEASE CONTROL AND PREVENTION NATIONAL CENTER FOR INFECTIOUS DISEASES

ASM/NCID POSTDOCTORAL RESEARCH FELLOWSHIP PROGRAM
TABLE OF CONTENTS
*All forms must be typed*
Program Administrators………………………………………………………………..…3
ASM/NCID Research Fellowship Program……………………………………….....…..4-5
Operational Procedures……………………………………………………………….6-11
Conditions for Starting the Program Expectations of the Two Year Tenure with ASM and NCID The Award Package
Checklist for Fellows…………………………………………………………...……..12-14
Overview of Forms………………………………………………………………………15
Individual Forms………………………………..…………………………………16-28
Approval to Revise Research Plan Starting the Post-doctoral Research Fellowship Program Direct Deposit Authorization Form Healthcare Reimbursement Form Travel Authorization and Cash Advance Request for Relocation Allowances
Travel Expense Report Leave of Absent Form
Return from Leave of Absence Form Resignation Form Completing the Post-Doctoral Research Fellowship Program
Assessment Overview……………………………………………………………...….…29
Assessment of the ASM/NCID Program………………………………………………...30
Individual Forms……………………………………………………………….….31-38
Fellows Assessment of ASM/NCID Program Preceptor’s Assessment of ASM/NCID
2
Program Administrators
Names and Terms Used in the Handbook. The following names and terms are used throughout the handbook. Please refer to this list when you are contacting ASM or NCID.
Preceptor: Major advisor for research and professional training.
CDC Program Contact: Janet Nicholson at 404-639-3945 Email [email protected]; fax 404-639-3039 (mailing address) to ASM/NCID Fellowship Program, National Center for Infectious Diseases, Mail Stop C12, 1600 Clifton Rd, Atlanta, GA 30333
ASM Program Manager (programmatic inquiries and reimbursements): Irene Hulede at 202-942-9295, Email [email protected], fax 202-942-9329, (mailing address) to Education Department, American Society for Microbiology, 1752 N Street, NW, Washington, DC 20036
ASM Program Coordinator (professional development and insurance reimbursement): Tiffani Fonseca at 202-942-9283, Email [email protected], Fax 202-942-9329, (mailing address) to Education Department, American Society for Microbiology, 1752 N Street, NW, Washington, DC 20036
ASM Administration Contact (stipend payments): Brenda Reid at 202-942-9205, Email [email protected], fax 202-942-9341, (mailing address)-Human Resources Office, American Society for Microbiology, 1752 N Street, NW, Washington, DC 20036
3

ASM/NCID Postdoctoral Research Fellowship Program in Infectious Disease and Public Health Microbiology
Overview The American Society for Microbiology and National Center for Infectious Diseases (ASM/NCID) Postdoctoral Research Fellowship Program is a comprehensive training program which provides opportunities to participate in interdisciplinary training on global public health issues. As a fellow, you will have many opportunities to conduct novel research with the overall objective of developing practical applications in microbiology, immunology, and epidemiology for the diagnosis and prevention of infectious diseases. Exploring new ideas, techniques, and approaches will both enhance your professional experience and contribute significantly to the national effort to combat infectious diseases worldwide. Program The program is sponsored by the American Society for Microbiology (ASM) and the National Center for Infectious Diseases (NCID). The goal of ASM/NCID Fellowship is to support the development of new approaches, methodologies and knowledge in infectious disease prevention and control in areas within the public health mission of the CDC. The fellowship allows one to perform research in residence at the NCID which is headquartered at the Centers for Disease Control and Prevention (CDC) in Atlanta, GA.
Eligible fields of study include:
Bacterial and Mycotic Diseases Viral and Rickettsial Infections Nosocomial Infections HIV/AIDS Vector-borne Infectious Diseases Sexually Transmitted Diseases Parasitic Diseases
Funding The Fellowship provides an annual stipend (up to $38,225), health benefits (up to $3000 annually) for a maximum of 2 years, relocation benefits (up to $500), and (up to $2000 annually) for professional development for a maximum of 2 years. Eligibility The program is intended for individuals who either earned their doctorate degree or completed a primary residency within three years of their proposed start date. Applicants may not have a faculty position or be enrolled in a graduate degree program during the fellowship. Considerations will be given to individuals with more experience if there are compelling reasons. Qualified applicants will receive consideration without regard to race, creed, color, age, sex, or national origin.
4
Criteria for Selection Applications are reviewed for (i) scientific merit and training potential of the research proposal, (ii) training resources and environment from the identified preceptor, and (iii) congruence with the Centers for Diseases public health mission. The 2006 application system is currently available. Please visit our website http://www.asm.org/Education/index.asp?bid=15497 and click on the "Apply Online" link on the left, to access the system. Deadline: January 15, 2006 Contact ASM/NCID Postdoctoral Research Fellowship Program Education Department American Society for Microbiology 1752 N Street, N.W. Washington, D.C. 20036 (202) 942-9283 or (202) 942-9295 E-mail: [email protected]
5
Conditions for Starting the Program
Completion of Doctoral Degree. You must complete your doctoral degree and send an official transcript or letter from the graduate dean verifying completion of your graduate training to the ASM Office before starting your two-year tenure or before October 31, whichever is first. Letters and transcripts prepared in a foreign language must be translated into English.
Visa. If you are not a US citizen or permanent resident, you must provide evidence of a valid visa that permits permanent residence in the US. This evidence must be submitted to the ASM Program Contact and your NCID preceptor. The program only supports a J-1 visa. Neither the ASM nor NCID are designated sponsors of foreign visitor exchanges and cannot issue the I-20 Forms of the US Immigration and Naturalization Services or the IAP66 Forms of the US Information Agency. An official award letter that describes your responsibilities in the ASM/NCID Program is available from the ASM Office.
Security Clearance. In order to perform work on the premises of the NCID laboratories or in any CDC owned or leased facility, you must meet all security requirements and receive a favorable security clearance prior to your start date. There are no exceptions.
A two-step process has been implemented for attaining security clearance. The first step results in a temporary security clearance while the second step results in permanent security clearance. This permanent status is required for you to remain in the Program. To begin the process, you will need to contact your preceptor at CDC for the following forms:
• (Federal) Standard Form 85, "Questionnaire for Non-Sensitive Positions" (appendix) • (Federal) "Declaration for Enrollment" (appendix) • (Federal) Optional Form 612 "Optional Application for Federal Employment" (appendix) • (Federal) "FBI Fingerprint Charts" available from a local law enforcement facility (police
station). There may be a nominal charge to get fingerprinted and to have the Form returned to you.
• (Optional) Federal Standard Form 86A "Continuation Sheet for Questionnaires SF 86, SF 85 P and SF 85"
A document called, "Instructions for National Agency Check and Inquiry (NACI)" is enclosed with the federal forms to ensure that they are completed accurately. Please read this document carefully. Incomplete forms will be returned to you for further consideration and may delay your starting date. Fellows may not begin their tenure with ASM and NCID until a favorable temporary clearance has been achieved.
Favorable permanent clearance is attained after your records have been reviewed by the US Office of Personnel Management as well as the US Federal Bureau of Investigation and you have received a favorable response. Failure to attain this status will deem you ineligible to continue in the ASM/NCID Program. Final acceptance into the Program is subject to a favorable permanent clearance and your cooperation to complete and return the forms in a timely manner. Please note security clearance is a requirement for anyone (e.g. CDC employees, visiting guests, and contractors and consultants) working on the premises of a CDC owned or leased facility.
6
Expectations during the Two-Year Tenure with ASM and NCID
NCID Preceptor and Research Program. Each fellow has an NCID preceptor for day-to-day supervision. Your preceptor will provide support in all aspects of your research project and serve as your mentor. The CDC Program Contact and ASM must approve certain actions, such as major changes to your research plan and travel to professional meeting. They are also available to consult with you regarding general matters relating to your program activities.
Professional Expectations. During your participation in the program, you are required to commit all of your working time and intellectual effort to your research plan. This plan must be approved by your preceptor. In addition, the ASM and CDC Program Contacts should have a copy of this plan. You are expected to commit your full effort to:
• Conducting research, • Publishing in scientific and professional journals, • Presenting at scientific meeting, and • Participating in training workshops and meetings in your preceptor's laboratory, at
CDC or in your community.
In addition to these expectations, you will be required to:
• Meet with CDC Program Contact during your first week at CDC. If you are starting your tenure at a facility other than the one in Atlanta, you should call the CDC Program Contact in Atlanta during your first week.
• Read the laboratory's safety manual during your first week at CDC. Ask your preceptor about this manual if it is not available to you immediately.
• Attend CDC Employee Orientation in the first month. This orientation is held on the first Monday of each pay period. Contact Dawn George-Martin at 770-488-1799 in the Human Resources Management Office at CDC in Atlanta (HRMO) for details. For individuals at another facility, you should contact the same office and request written materials.
• Attend a workshop on laboratory safety in the first month. The Office of Health and Safety (OHS) at CDC in Atlanta can provide dates. You should attend other workshops on laboratory safety (e.g. radiation safety, bloodborne pathogens) if they are relevant to your research. For more information about the OHS programs, go to the World Wide Web site at http://www.cdc.gov/od/ohs/htm
• Attend Fellows Research in Progress Sessions as scheduled by the CDC Program Contact.
• Attend the annual Epidemic Intelligence Service (EIS) Conference if applicable to your area of research.
• Attend ASM sponsored Fellows Retreat as scheduled. • Attend workshops in ethics and preparation of research grants (either at CDC,
Emory University, or another comparable organization). You are encouraged to
7
seek additional training in communications, management, marketing, and team building skills.
Other Awards or Employment. As a recipient of the ASM/NCID fellowship, you may not accept any other similar fellowship or award either before your start date or during your tenure. During your tenure, you may not accept additional compensation for services from another position, including part-time research, consulting, or outside work.
Employment Status. As an ASM/NCID fellow, you are classified as a fellow and not as an employee of the Centers for Disease Control (CDC) of the American Society for Microbiology (ASM).
Leave Policy. As an ASM/NCID fellow, you are not expected to be away from your assignment for extended periods of time. By participating in this program, you have agreed to report to the worksite in accordance with the regular workweek, holiday schedules and inclement weather policies as established by the Host Laboratory. During the term of this agreement, ASM agrees to provide up to 10 days (per year) for use by the Fellow as personal vacation or sick days. Absences from the worksite in excess of 10 workdays must be preapproved by the CDC Program Contact and your preceptor and will be allowed only under extreme (exceptional) circumstances. Fellows must complete a Leave of Absence form (included in this handbook) and leave must be approved by the CDC Contact and your preceptor before leave will be granted. A copy of the signed form must be forwarded to the ASM Program Manager at least 30 days prior to your departure. Please know that any leave that is granted over and above the two-week a year period will be without pay. If leave without pay is granted, your stipend payment will be adjusted appropriately. Failure to notify the ASM Contacts in a timely manner could result in delayed stipend payments.
CDC Policies and Procedures. You are expected to adhere to all established policies and procedures of the CDC as they apply to guest researchers and to follow established guidelines for the safety and health of individuals working the laboratory. For example, in the first week, review the laboratory's safety manual. It will also be necessary for you to provide a baseline serum sample and to receive any relevant immunizations at CDC's Employee Health Clinic. Check with your preceptor about both items.
Research Proposal. If you choose to revise your research proposal, prepare another two-year research proposal in conjunction with your preceptor and submit it to both the ASM and CDC Program Contacts. If you elect to make a major change in your approved research plan, you must complete the form Approval to Revise Research Plan and return it to the ASM Office. This form asks for a written statement describing your changes and must be approved and signed by your preceptor and CDC contact.
Starting Your Tenure. Before you start, contact both your preceptor at NCIC and CDC Program Contact and inform them of your exact start date. Complete the form Starting the ASM/NCID Postdoctoral Fellowship Program and return it to the ASM
8
Office. Fellows must start their tenure before October 31. Failure to start before this date without special arrangements and approvals may jeopardize your award.
Completing Your Tenure. One month prior to completing your tenure at NCID, notify both your preceptor at NCID and the CDC Program Contact. Complete the form Completing the Post-Doctoral Research Fellowship Position and return it to the ASM Office. If you decide to resign from your award position before the official end date, you must notify your preceptor as well as the CDC and ASM Program Contacts in writing as far in advance as possible. You must also complete the Resignation Form and submit it with appropriate authorization to the ASM Office.
Important Web Sites. For further information about CDC or ASM refer to the following URL sites on the World Wide Web:
http://www.cdc.gov/ Centers for Disease Control and Prevention
http://www.cdc.gov/ncidod/ncid.htm National Center for Infectious Diseases
http://www.cdc.gov/od/ohs/ Office of Health and Safety at CDC
http://www.asmgap.org ASM Graduate and Postdoctoral Opportunities
http://www.asm.org/Education/index.asp?bid=15497 ASM/NCID Post Doctoral Research fellowship Program information for prospective applicants
http://www.asm.org/Education/index.asp?bid=369 ASM Education Homepage
http://www.asm.org/ ASM Homepage
http://www.ssa.gov/ Social Security
http://www.irs.gov/ Internal Revenue Service
http://www.irs.gov/formspubs/index.htm IRS Publication 520 (Scholarships and Fellowships), Search for Form 520
9

The Award Package
The ASM/NCID award includes three items:
• Stipends paid monthly, • Reimbursement for health care provider premiums for a single or
family subscriber paid upon request, • Reimbursement for professional development expenses paid upon
request.
Stipends. Compensation that accompanies this award is allotted up to $38,225 annually. In order to receive your stipend, it is your responsibility to complete and return to the ASM Program Contact the form Starting the Post-Doctoral Research Fellowship Position, and if you desire direct deposit service, the form Direct Deposit Authorization. These forms should be sent to the ASM Program Contact 30 days prior to your start date. Failure to do so will result in delays in your first stipend payment. Payment is available on the 15th of each month and can be deposited electronically to your bank or mailed to the address which you provide on the form Starting the Post-Doctorate Research Fellowship Position. Please know that direct deposit service is available only after the first check has been issued.
Health Benefits. The ASM/NCID award includes health benefits to you and your family. Up to $3,5000 annually is available to you for premium expenses with a health care provider. This amount may not be used to out-of-pocket medical expenses, co-payments, and deductibles. Please read information on reimbursement of Medical and Dental Insurance included in the appendices.
It is your responsibility having received this award to arrange for your own health care. Local health care and/or insurance providers in the Atlanta area include among others, Blue Cross Blue Shield of Georgia (404-842-8109) and Kaiser Permanents (404-261-2580). Please contact these providers directly or check the Yellow Pages of the telephone book for other providers. The ASM is not authorized to provide advice or to procure health and medical insurance for fellows. Please do not contact the ASM for advice. Additionally, neither ASM nor NCID endorses any health plan provider or insurance plans.
Professional Development. The ASM/NCID award includes up to $2,000 annually during the two-year tenure for professional development expenses. Eligible expenses include travel, lodging and per diem expenses to meetings, membership in professional societies, subscriptions to journals, and fees to register with the placement service of professional societies. Professional development expenses does not include travel for field work to conduct your research, computer equipment or software. All professional development expenses must be approved by both your preceptor and NCID Program Contact. A completed and signed Travel Authorization and Cash Advance
10

form, along with the ASM Travel Expense Report, must be submitted to the ASM Office before any reimbursements are made (see below).
Relocation Benefits. The ASM/NCID award allots up to $500 for relocation expenditures. A completed and signed Request for Relocation Allowances form must be submitted to the ASM Office before any reimbursements are made.
Acceptable Forms and Schedule of Reimbursable Expenses. ASM reimburses fellows for expenses incurred in two categories, health benefits and professional development. Receipts are required for all expenses. Travel expenses should be recorded on the ASM Travel Expense Report. Requests for reimbursements, such as meeting registrations, subscriptions, premiums for health care providers, can be made in writing, accompanied by proper documentation.
To be included in the reimbursement cycle, authorized requests must be received by the ASM Program Contact one week in advance, excluding holidays, prior to the reimbursement date.
Reporting and Taxability of Stipends and Other Income. As a fellow in the Program, you are receiving a fellowship grant and, therefore are classified as a fellow. You are not an ASM or NCID employee. You are awarded (1) annual stipend, (2) payments of premiums for health care provider, and (3) payment of expenses for professional development. The gross amount of the annual stipend and any funds for health care and professional development will be reported by ASM to the Internal Revenue Service as miscellaneous income. You will be responsible for sending quarterly advance payments to the Internal Revenue Service for taxes. Please consult the Internal Revenue Service or your tax advisor concerning your own income tax circumstance and the necessity to make quarterly estimated tax payments. You may also be responsible for payment of state and/or local taxes in certain locations. Foreign nationals must follow their own country's practices for reporting income. Neither the ASM nor the NCID is authorized to provide tax advice. ASM will provide 1099 tax forms in January of each year.
For information on the Internal Revenue Service's definition of Fellowship, visit http://www.irs.gov/formspubs/index.htm Search for Form 520
11

Checklist for Fellows
Upon receipt of your award letter:
_____Send confirmation of acceptance of the ASM/NCID Postdoctoral Research Fellowship Position via e-mail to ASM Program Contact (this step is required before receiving this Handbook)
Within two weeks of receipt of Handbook (to start process for security clearance):
_____Contact your CDC preceptor to obtain current information required for security clearance
_____Read instructions for National Agency Check and Inquiry (NACI)
_____Seek out local law enforcement facility and complete Federal Form 258 Fingerprinting Table
_____Complete three and if necessary, four federal forms:
1) Standard Form 85 Questionnaire for Non-Sensitive Positions and if necessary, Form 86A Continuation Sheet for Questionnaires SF86, SF 85P and SF85
2) Federal Form Declaration for Enrollment
3) Optional Form 612 Optional Application for Federal Employment or an updated resume which includes all information required on Form 612
_____Send in one packet Forms 85, FBI Fingerprint Charts, 612 and if necessary, Form 86A to the CDC preceptor
Before you start your two-year tenure:
_____Send final papers documenting completion of doctoral degree (if applicable) to ASM Program Contact
____Complete and return to ASM Program Contact from Starting the ASM/NCID Postdoctoral Research Fellowship Position
_____Notify NCID preceptor and CDC Program Contact of official start date
12

_____Complete the Direct Deposit Authorization Form and send to Human Resources Specialist at ASM at least 30 working days prior to your start date
_____For non-US citizens, obtain immigration papers for the US Immigration and Naturalization Services visa permitting permanent residence in the US and send to ASM and CDC Program Contacts
(Foreign Fellows): As soon as you arrive in the U.S., apply for a social security number at the social security office. You will not receive a stipend payment unless ASM receives a valid social security number.
During your two-year tenure:
_____Meet with CDC Program Contact in the first week
_____Read the laboratory's safety manual in the first week
_____Attend CDC Employee Orientation in the first month
_____Attend workshop on laboratory safety in the first month
_____Submit your research plan to ASM and CDC Program Contacts in the first month if you have revised your research proposal
_____Attend Research in Progress Sessions and other CDC seminar series as identified by your Preceptor and CDC Program Contact
_____Attend ASM-sponsored Fellowship Retreat each fall
_____Attend workshops on ethics and grantmanship whenever possible
_____Submit abstracts and attend professional, scientific meeting in your discipline
_____Submit manuscripts for publications
_____Get forms from and make quarterly estimated payments for income taxes to the US Internal Revenue Service
_____Complete and return ASM Form Assessment of the ASM/NCID Program twelve months after you start, or before December 1 whichever is first
_____Sign up with placement services of professional organizations
_____Complete and return the Resignation Form if you do not complete the full two years
13

At the end of your two-year tenure:
_____Two months before your last day of tenure, notify your preceptor as well as the ASM and CDC Program Contacts
_____Complete and return to the ASM Program Contact one month before your last day three items:
• Fellows Assessment of ASM/NCID Program • Longitudinal Study: Fellows Exit Survey • Completing your ASM/NCID Postdoctoral Fellowship Position Form
After your two-year tenure:
_____Notify ASM Program Contact about any address, telephone, or E-mail changes. This is most important for following through with tax information and the Longitudinal Studies.
_____Complete and return in timely manner the Longitudinal Study: Fellowship Follow-Up Survey disseminated annually in the spring (Forms are currently being updated).
14
FORMS
All Forms MUST Be Typed
Approval to Revise Research Plan Starting the Post-Doctoral Research Fellowship Position Direct Deposit Authorization Reimbursement of Medical/Dental Insurance Relocation Form Travel Authorization & Cash Advance Expense Report Leave of Absence Form Return from Leave of Absence Form Resignation Form Completing the Post-Doctoral Research Fellowship Position
15
Approval to Revise Research Plan Name_________________________ Email Address _______________________ Preceptor ______________________ NCID Division _______________________ Preceptor’s Email Address __________________________________________________ I, _________________________________________, an ASM/NCID fellow who
(your name) started on __________________________________, am requesting permission to
(start date of two year tenure) change my original research plan and direction. I understand that this change may require extra effort on my part to complete the work within the two year tenure. I have reviewed this work with my preceptor and he/she has agreed to this new plan and direction. Additionally, this plan continues to support the public health mission and goals of the organization.
In the space below, please describe your new research plan. Please limit your response to one additional typewritten page.
______________________ ___________ Fellow’s Signature Date
______________________ ___________ Preceptor’s Signature Date
______________________ ___________ CDC Program Contact’s Signature Date
Please return form to: ASM/NCID Fellowship Program
American Society for Microbiology Education Department
1752 N Street, NW Washington, DC 20036
Tel: 202.942.9283 Fax: 202.942.9329
16
Starting the Post-Doctoral Research Fellowship Position Please type and complete the following information:
Fellow’s Name _________________________________________________________________ Social security number _______________________ Official start date___________________ Preceptor’s name____________________________ NCID division________________________ Temporary address during your two-year tenure with ASM and NCID __________________________________________ __________________________________________ __________________________________________ Mailing address where you would like your stipend payment to be mailed. If this is the same address as above, leave this space blank. __________________________________________ __________________________________________ __________________________________________ In case of an emergency, please provide the name, address and telephone number of someone to contact.
Contact Person 1: Contact Person 2: ______________________________________________ ______________________________________________ ______________________________________________ ______________________________________________ ______________________________________________ ______________________________________________ ______________________________________________ ______________________________________________
All ASM/NCID fellows are required to attain favorable security clearance before starting their tenure at NCID, a federal laboratory. It is mandatory that all federal forms are completed and returned to the CDC office six weeks prior to your start date. Fellows who fail to attain favorable security clearances will not be permitted into the Program. Please remember that as an ASM fellow, you are not an employee of the Centers for Disease Control (CDC) or the American Society for Microbiology (ASM). Your total award, which includes stipend payments and payment for professional development and health care benefits expenses, is subject to income tax.
Please return form to Irene Hulede ASM/NCID Fellowship Program
American Society for Microbiology Education Department
1752 N Street, NW Washington, DC 20036 or by fax 202-942-9329
17
Direct Deposit Authorization
I, ______________________________________, on ____________________________ (Name of Fellow) (Date)
am requesting that my stipend payment be transmitted via direct deposit to the following financial institution: Name of Financial Institution _______________________________________________ Address of Financial Institution ______________________________________________ ______________________________________________ Telephone Number ______-_______-_________ Checking Account Number _________________ Savings Account Number ___________________ Transit Number ___________________________ While this service is being provided to me during my tenure at NCID, I understand:
It is my responsibility to complete and return form to the ASM Office at least 30 days prior to my start date.
That my first payment will be in the form of a live check. Direct deposit requires one pay period to take effect.
Fellow’s Signature ________________________________________________________ One voided check or savings account deposit slip is required in order to start this service. Please attach to this form. The paystubs will be mailed to the mailing address you have provided. Please be informed that all stipend payments are made on the 15th of each month.
Please return form and voided check/deposit slip to: ASM/NCID Fellowship Program
American Society for Microbiology Human Resource/Administration Office
1752 N Street, NW Washington, DC 20036
Tel: 202.942.9205 Fax: 202.942.9341
18
Reimbursement of Medical/Dental Insurance
The ASM/NCID award includes health benefits to you as a single or family subscriber. Up to $3,000 annually is available for premium expenses with a health care provider. This amount may not be used for out of pocket medical expenses, co-payments and/or deductibles. DOCUMENTATION OF INSURANCE EXPENSES Submit the following as documentation for insurance expenses:
Proof of insurance such as Policy Statement or receipt of payment from insurance company indicating breakdown of premium, if policy covers more than one individual; or
Cancelled check indicating payment of insurance and/or documentation to show proof of prepayment of insurance coverage.
ASM will only reimburse the cost for your insurance coverage as a single and family subscriber and with the appropriate documentations (i.e. photocopies of canceled checks, insurance receipts, or credit card statement, etc). Insurance expenses may be submitted for monthly, bi-monthly, semi-annual or annual basis depending upon coverage period of individual’s payment to insurance company. Please specify the date that your expenses are covered during that period. PAYMENT SCHEDULE Payment for insurance expenses will be made according to the payment plan option that you select with your insurance carrier. For example, an individual who selects a monthly insurance plan option will receive payment each month after submission of proper documentation and an individual who selects a six-month insurance plan, will receive payment twice a year. Please know that the insurance payment checks will be mailed separately from the stipend payments. ASM CONTACT FOR HEALTH BENEFITS RELATED ISSUES Tiffani Fonseca is the staff person responsible for all insurance related issues. If you have any questions regarding health benefits, please contact Tiffani at 202-942-9283 or e-mail at [email protected].
Please mail all receipts and/or documentation to: Tiffani Fonseca, Coordinator, Student Fellowship Programs
American Society for Microbiology Education Department
1752 N Street, NW Washington, D.C. 20036 or fax to 202-942-9329
Tel: 202.942.9283
19

ASM/NCID POSTDOCTORAL RESEARCH FELLOWSHIP PROGRAM HEALTHCARE EXPENSE PAYMENT FORM
This form must be typed.
Name: ______________________________________________________ Mailing Address: ______________________________________________________
______________________________________________________ ______________________________________________________
Telephone: _____________________ E-mail: _____________________________ Program start date: ____________________ Program end date: _____________________ Indicate the insurance coverage: Individual ___________ Family ___________ Indicate the type of insurance: Health ___________ Dental ___________ (Note that the maximum allowable expense per fellowship year is up to $3,000.00) Indicate the duration of premium and specify the month of insurance coverage: Monthly: ______ Amount: __________ Quarterly: ______ Amount: __________ Half yearly: ______ Amount: __________ Yearly: ______ Amount: __________ Specify Month of Insurance Coverage: _______________________ Please complete this form and return it along with the necessary receipts to: Tiffani Fonseca Coordinator - Student Fellowship Programs American Society for Microbiology 1752 N Street, NW Washington, DC 20036
Fax: 202-942-9329
20
Travel Authorization & Cash Advance Please type and complete this form, make two copies, and return all copies to the CDC Program
Contact for authorization. Send one copy to the ASM Office. Name _____________________________________________________________________ E-mail Address __________________________ Telephone Number ___________________ Destination _________________________________________________________________ Purpose for travel ____________________________________________________________ ___________________________________________________________________________ ___________________________________________________________________________ Date of Departure ____________________ Date of Return _____________________
CASH ADVANCE REQUEST Estimated cost: __________________ Meeting Registration $______ Transportation $______ Hotels/Meals $ ______ Miscellaneous $______ TOTAL: $ _______ Cash advance amount: _______________________ (maximum amount $500) I understand that if I do not reimburse ASM for any unused portion of the cash advance, IRS regulations require that the unreimbursed amount is added to my gross income and is taxable as other income. I hearby authorize a stipend deduction of all outstanding cash advances as of the date of my award termination. ____________________________________ _________________________ Signature Date Please mail check to: Name: ___________________________________ Address: ___________________________________
___________________________________
___________________________________
APPROVAL (three signatures required)
____________________________________ ________________________ Preceptor’s Signature Date _____________________________________ _________________________ CDC Program Contact’s Signature Date _____________________________________ _________________________ ASM Program Contact’s Signature Date Please return one form to ASM/NCID Fellowship Program, Education Departme t, American Society for nMicrobiology, 1752 N St., NW, Washington, DC 20036 or by fax 202-942-9329
21
22
Request for Relocation Allowances This form must be typed.
Name _______________________________________________________________________ E-mail Address __________________________ Telephone Number ___________________ Social Security Number _______________________________ Current Residence ___________________________________________________
___________________________________________________ ___________________________________________________
Date of Travel: ______________________________ Address for Check Mailing ________________________________________________
________________________________________________
________________________________________________ Amount Requested: $___________ (maximum amount $500) * Please list expenses claimed for the amount requested above.
_______________________ _____ ________________ Fellow’s Signature Date
Payment will not be made until this form is completed, signed and submitted to the ASM Office.
Please return form to:
ASM/NCID Fellowship Program American Society for Microbiology
Education Department 1752 N Street, NW
Washington, DC 20036 Tel: 202.942.9283 Fax: 202.942.9329
NAME _____________________________________ ADDRESS _________________________________
American Society for Microbiology 1752 N Street, N.W.,
Washington, DC 20036-2804
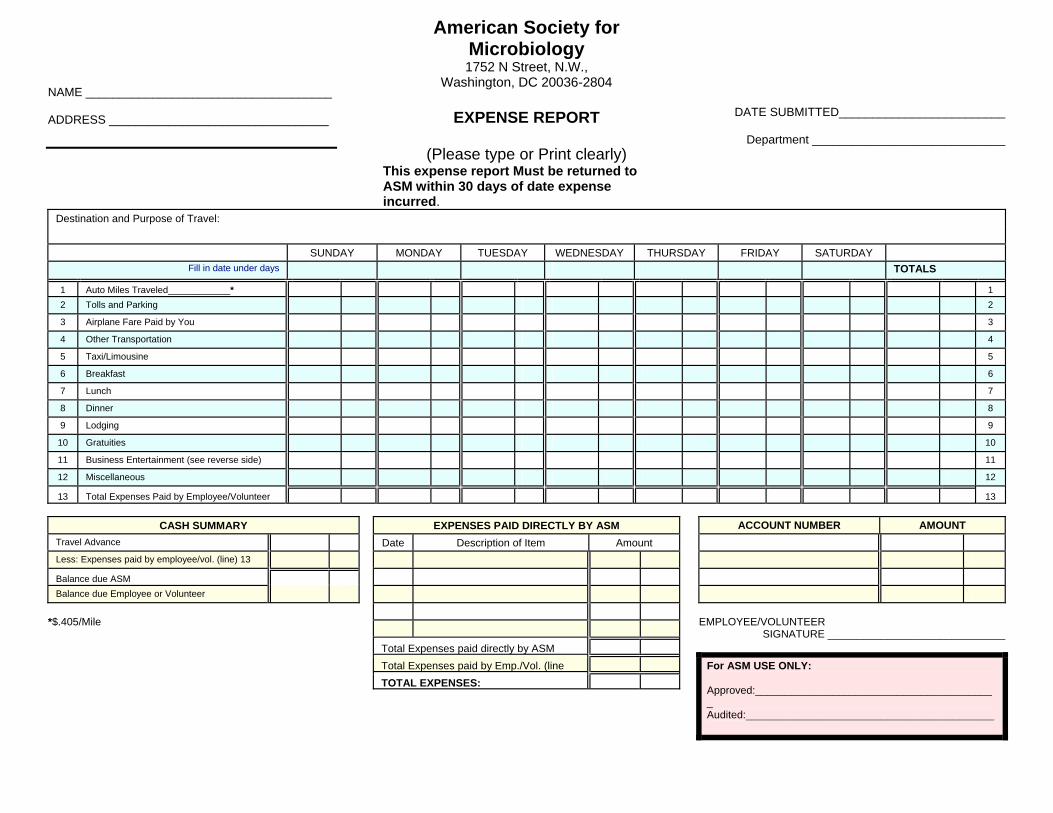
EXPENSE REPORT
(Please type or Print clearly) This expense report Must be returned to ASM within 30 days of date expense incurred.
DATE SUBMITTED_________________________
Department _____________________________
Destination and Purpose of Travel:
SUNDAY MONDAY TUESDAY WEDNESDAY
THURSDAY FRIDAY SATURDAY
Fill in date under days TOTALS
1
Auto Miles Traveled____________*
1
2 Tolls and Parking
2
3
Airplane Fare Paid by You
3
4
Other Transportation
4
5
Taxi/Limousine
5
6
Breakfast
6
7
Lunch
7
8
Dinner
8
9
Lodging
9
10
Gratuities
10
11
Business Entertainment (see reverse side)
11
12
Miscellaneous
12
13
Total Expenses Paid by Employee/Volunteer
13
CASH SUMMARY
Travel Advance
Less: Expenses paid by employee/vol. (line) 13
Balance due ASM
Balance due Employee or Volunteer
*$.405/Mile
EXPENSES PAID DIRECTLY BY ASM Date Description of Item Amount
Total Expenses paid directly by ASM
Total Expenses paid by Emp./Vol. (line
TOTAL EXPENSES:
ACCOUNT NUMBER
AMOUNT
EMPLOYEE/VOLUNTEER
SIGNATURE ______________________________
For ASM USE ONLY: Approved:_________________________________________ Audited:__________________________________________

INSTRUCTIONS FOR EXPENSE REPORT FORM This form is to be used by employees or volunteers for reporting business related expenses reimbursable by ASM. The report is to be filed whenever expenses are incurred. Please keep a copy of this submission for your own personal records.
LOCATIONS VISITED List each of the locations you visited together with the date in this section.
REIMBURSABLE EXPENSES PAID BY EMPLOYEE OR VOLUNTEER Receipts, paid bills or other documentary evidence for expenditures of $25.00 or more, MUST accompany this report although ASM encourages submissions of receipts for all expenses regardless of amount. Accompanying documents MUST clearly indicate amount, date, and place of expenditure. A completed credit card copy is acceptable. Receipt stubs without identifying marks are NOT acceptable. Line 1 - Mileage - Multiply the “Auto Miles Traveled” each day by the current mileage allowance rate. Indicate the per mile rate used. Line 2 - Tolls and Parking - Fees paid in connection with the use of personal, company, or pre-approved rental automobiles are to be included on this line. Line 3 - Airline Fares Paid by You - Do NOT include on this line any tickets purchased with ASM issued credit cards or furnished by ASM's travel agent. For airline tickets submit either an original receipt, an original invoice from a travel agent, or a copy of the ticket or invoice from the volunteer's employer. Line 4 - Other Transportation - This line is to be used for rail, bus and subway fares and pre-approved auto rental paid by you. (Attach receipts.) Rental cars will be reimbursed with prior authorization from the appropriate board chair or ASM officer when the cost is the same or less than other available transportation
Line 5: Taxi and Limousine - List out of pocket expenses. Line 6, 7 and 8: Breakfast, Lunch and Dinner - Meal cost expenses are to be included on the appropriate line. Meal costs purchased for customers or business associates should be entered on Line 11 and details must be supplied in the section “DETAILS OF ENTERTAINMENT EXPENSES..." shown below on this report. Line 9: Lodging - While traveling away from home, receipts for all lodging expenditures must be attached regardless of amount. A breakdown of this bill is required; consequently, include on this line lodging amounts and charges not applicable to other line categories of this report. Line 10: Gratuities - All reimbursable tips and gratuities are to be included on this line. Excessive tipping (more than 10 -20%) will NOT be reimbursed. Line 11: Business Entertainment - Entertainment will be reimbursed only if all required information concerning each expenditure is clearly indicated in the section “DETAILS OF ENTERTAINMENT EXPENSES..." shown below on this report. Amounts charged on this line without adequate explanation of business purpose will NOT be reimbursed. These costs must be pre-approved and directly related to the meeting or activity, and the relationship to the meeting or activity or to ASM business MUST be explained. Line 12: Miscellaneous - All reimbursable expenses such as telephone, laundry, etc., and amount not provided for on lines 1 - 11 are includable here. Expenses are to be described in the section “...EXPLANATION OF MISCELLANEOUS EXPENSES” shown below on this report.
EXPENSES PAID DIRECTLY BY ASM Ticket stubs or receipts for all credit card purchases and travel agent furnished transportation MUST be attached to this report. CREDIT CARD PURCHASES - Such as air fare which are charged to ASM using ASM issued credit cards MUST be described in detail in the �Expenses Paid Directly by ASM’s section of this report.
DETAILS OF ENTERTAINMENT EXPENSES AND EXPLANATION OF MISCELLANEOUS EXPENSES
DATE
PERSONS ENTERTAINED COMPANY PLACE OF ENTERTAINMENT BUSINESS PURPOSE AMOUNT
25
Leave of Absence Form This form must be typed, completed, and returned to ASM office at least 30 days prior to
effective date of leave of absence.
Fellow’s Name ___________________________________________________________ Email Address____________________________________________________________ Telephone Number________________________________________________________ Preceptor’s Name ________________________ NCID Division ____________________ Effective Date of Leave ___________________ Anticipated Date of Return ___________________ I am taking a leave of absence for the following reason(s): My forwarding address will be: ________________________________________ ________________________________________ ________________________________________ As an ASM/NCID fellow, I understand that it is my responsibility to complete a Return from Leave of Absence Form at least one month before I return in order for my file to be reactivated in the program. ____________________________ ___________________ Fellow’s signature Date ____________________________ ___________________ Preceptor’s signature Date ____________________________ ___________________ CDC Program Contact’s signature Date
Please return form to: ASM/NCID Fellowship Program
American Society for Microbiology Education Department
1752 N St., N.W. Washington, DC 20036
Tel: 202.942.9283 Fax: 202.942.9329
Return from Leave of Absence Form This form must be typed, completed, and returned to the ASM office at least 30 days
prior to your effective return date after your leave of absence.
Fellow’s name ______________________________________________________ Current Address ______________________________________________________
______________________________________________________ ______________________________________________________
Email address _______________________ Telephone number _______________________ Preceptor’s Name ___________________________ NCID Division_________________ Effective Date of Leave of Absence___________________________________________ Effective Date of return from Leave of Absence_________________________________ I plan to complete the ASM/NCID Postdoctoral Training Program by________________ My address during the remainder of my tenure in the program will be:
______________________________________________ ______________________________________________ ______________________________________________
_____________________________ ______________________________ Fellow’s signature Date _____________________________ ______________________________ Preceptor’s signature Date _____________________________ ______________________________ CDC Program Contact’s signature Date
Please return form to: ASM/NCID Fellowship Program
American Society for Microbiology Education Department
1752 N St., NW Washington, DC 20036
Tel: 202.942.9283 Fax: 202.942.9329
26
Resignation Form This form must be typed, completed, and returned to the ASM office at least 30 days prior
to the effective date of resignation. Fellow’s Name ___________________________________________________________ Preceptor’s Name _____________________ NCID Division ______________________ Effective date of resignation ___________________ Start date________________________ I am resigning this two-year tenure for the following reason(s): My Forwarding Address will be: ______________________________________________ ______________________________________________ ______________________________________________ Forwarding E-mail Address will be: __________________________________________ ______________________________ ______________________________ Fellow’s signature Date ______________________________ ______________________________ Preceptor’s signature Date ______________________________ ______________________________ CDC Program Contact’s signature Date Please remember that as an ASM/NCID fellow, you are required to keep the Office informed about your professional progress over the next ten years. Annual questionnaires will be sent during the spring. The results of this study will provide the necessary information to assess the success of this program. Thank you for your cooperation.
Please return form to: ASM/NCID Fellowship Program
Education Department American Society for Microbiology
1752 N Street NW Washington, DC 20036
Tel: 202.942.9295 or by fax 202-942-9329
27
Completing the Post-Doctoral Research Fellowship Position This form must be typed and completed
at least two months prior to your last day in the program.
Please complete the following information: First Name ______________________ Last Name ____________________ Current Address ______________________________________
______________________________________ ______________________________________
Current Telephone Number _____-_____-______ E-mail Address _________________ Social Security Number _____-_____-______ _____________________________ ______________________________ Preceptor’s Name NCID Division
_____________________________ Last working date
Forwarding address (This address is important for tax purposes as well as the ASM/NCID longitudinal studies of your professional progress):
______________________________________ ______________________________________ ______________________________________
Forwarding e-mail address (if available) _______________________________________ Please remember that as an ASM/NCID fellow, you are required to keep the Office informed about your professional progress over the next ten years. Annual questionnaires will be sent during the spring. The results of this study will provide the necessary information to assess the success of this program. Thank you for your cooperation.
Please return form to: ASM/NCID Fellowship Program
American Society for Microbiology Education Department
1752 N Street, NW Washington, DC 20036
or send it by fax to 202.942.9329 at least two months prior to your last day
Tel: 202.942.9295
28
ASSESSMENT Please print legibly in blue
or black ink.
Explanation of the Assessment of the ASM/NCID Program Fellows Assessment of ASM/NCID Postdoctoral Research
Fellowship Program Preceptors Assessment of ASM/NCID Postdoctoral
Research Fellowship Program
29

Assessment of the ASM/NCID Program
Fellows Assessment of the ASM/NCID Program. All ASM/NCID fellows are required to assess the overall program twice during their tenure (see schedule below). A questionnaire for collecting this information is included in the appendix and is called Fellows Assessments of the ASM/NCID Program.
Part I of the survey documents your professional development through a self-assessment and asks for current and continued plans to conduct research, publish and present research findings, and attend workshops and other related short courses. Part II seeks information about the training environment at NCID and asks questions about accessibility to resources and expertise, scientific guidance and networking opportunities. Part III asks about the ASM's administrative responsibilities.
Preceptor's Assessment of the ASM/NCID Program. All ASM/NCID preceptors are required to complete and return an assessment of the overall program twice during your tenure (see schedule below). Preceptors evaluate your professional growth in six areas, including (1) research knowledge and skills, (2) judgment, (3) communications, (4) initiatives, (5) adaptability, and (6) technical and scientific maturity. Part II asks for information about the training environment and is a self-assessment. Part III asks about ASM's administrative responsibilities. A copy of this assessment is included in the appendix for your information and is called the Preceptors Assessment of the ASM/NCID Program.
Schedule for Completing Assessments. You must first complete the same assessment twice during your 2-year tenure. The first time to complete the assessment is 12 months after your start date or before September 1, whichever is first. Indicate on the form in the boxes provides that the information is completed during the interim period. Continuation with the ASM/NCID Program into a second year is contingent upon satisfactory completion of the first year as documented through the assessment. The second time to complete the assessment is one month before completion of the program and before the final stipend payment is made. Please indicate on the form in the boxes provided that the information is completed during the final period. Failure to submit these final reports in a timely manner may delay final stipend payments. Fellows who finish early should complete and send the assessment along with the Completing the Postdoctoral Research Fellowship Position Form. Send all form to the ASM Program Contact.
Long Term Assessment of Fellows Professional Development. In an effort to assess the effectiveness of this program and to provide necessary information for continued support of the Program to the U.S. Congress, you will be required to participate in surveys conducted annually for ten years post-tenure; you should complete and return the Longitudinal Study/ Fellowship Follow-up Exit Survey to the ASM Office. Follow-Up Surveys requesting similar information will be disseminated in the spring for a maximum of 10 years.
30
Fellows Assessment of ASM/NCID Postdoctoral Research Fellowship Program
Please print legibly in black or blue ink.
Fellow’s Name ___________________________________________________________ Preceptor Name __________________________________________________________ Start Date (month and year) _______________ Check one: Which time period are you completing this questionnaire? ____ Interim (10-12 months after start) ____ Final (22-24 months after start) ____ Neither (resigning early from program) If you are leaving early, please explain the nature of your resignation and your last working date.
31
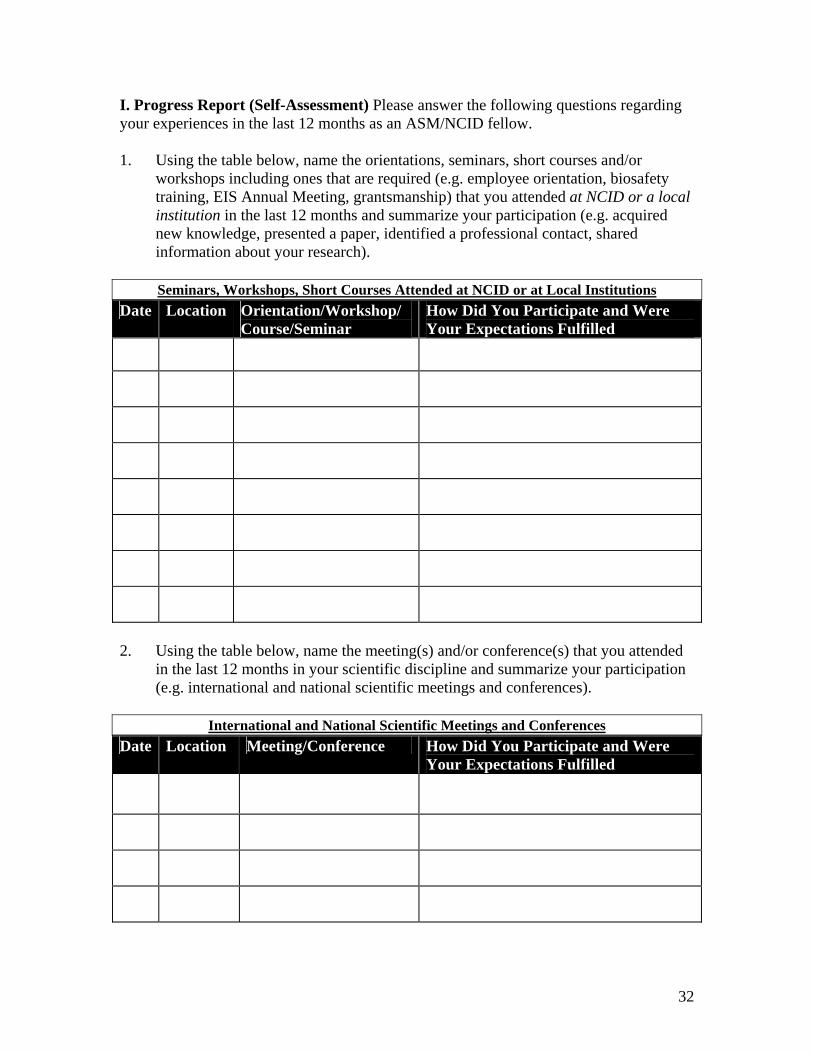
I. Progress Report (Self-Assessment) Please answer the following questions regarding your experiences in the last 12 months as an ASM/NCID fellow. 1. Using the table below, name the orientations, seminars, short courses and/or
workshops including ones that are required (e.g. employee orientation, biosafety training, EIS Annual Meeting, grantsmanship) that you attended at NCID or a local institution in the last 12 months and summarize your participation (e.g. acquired new knowledge, presented a paper, identified a professional contact, shared information about your research).
Seminars, Workshops, Short Courses Attended at NCID or at Local Institutions
Date Location Orientation/Workshop/Course/Seminar
How Did You Participate and Were Your Expectations Fulfilled
2. Using the table below, name the meeting(s) and/or conference(s) that you attended
in the last 12 months in your scientific discipline and summarize your participation (e.g. international and national scientific meetings and conferences).
International and National Scientific Meetings and Conferences
Date Location Meeting/Conference How Did You Participate and Were Your Expectations Fulfilled
32
3. In the space below, print legibly and summarize your research goals and objectives and describe what you have done to achieve these goals and objectives. In your concluding paragraph, please describe what you hope to achieve before the end of your tenure. Begin here and limit your response to one additional page. Be sure to put the date, your name and your preceptor’s name on the report.
33
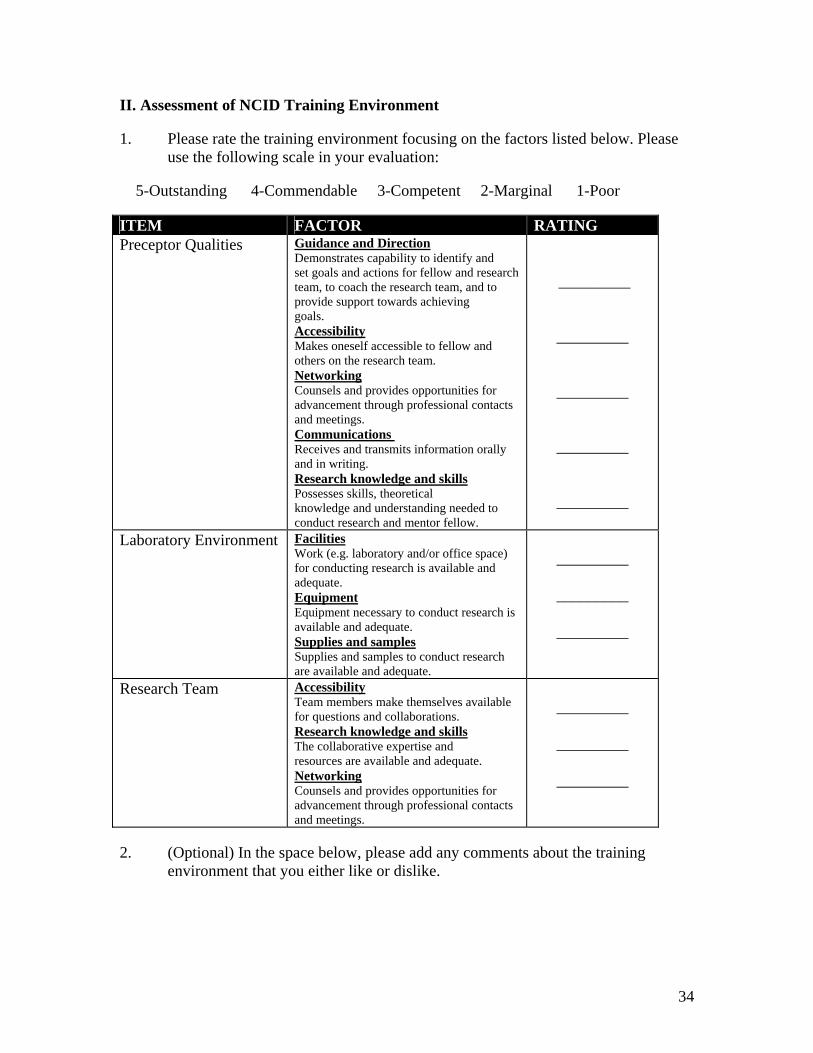
II. Assessment of NCID Training Environment 1. Please rate the training environment focusing on the factors listed below. Please
use the following scale in your evaluation: 5-Outstanding 4-Commendable 3-Competent 2-Marginal 1-Poor ITEM FACTOR RATING Preceptor Qualities Guidance and Direction
Demonstrates capability to identify and set goals and actions for fellow and research team, to coach the research team, and to provide support towards achieving goals. Accessibility Makes oneself accessible to fellow and others on the research team. Networking Counsels and provides opportunities for advancement through professional contacts and meetings. Communications Receives and transmits information orally and in writing. Research knowledge and skills Possesses skills, theoretical knowledge and understanding needed to conduct research and mentor fellow.
_________
_________
_________
_________
_________
Laboratory Environment Facilities Work (e.g. laboratory and/or office space) for conducting research is available and adequate. Equipment Equipment necessary to conduct research is available and adequate. Supplies and samples Supplies and samples to conduct research are available and adequate.
_________
_________
_________
Research Team Accessibility Team members make themselves available for questions and collaborations. Research knowledge and skills The collaborative expertise and resources are available and adequate. Networking Counsels and provides opportunities for advancement through professional contacts and meetings.
_________
_________
_________
2. (Optional) In the space below, please add any comments about the training
environment that you either like or dislike.
34
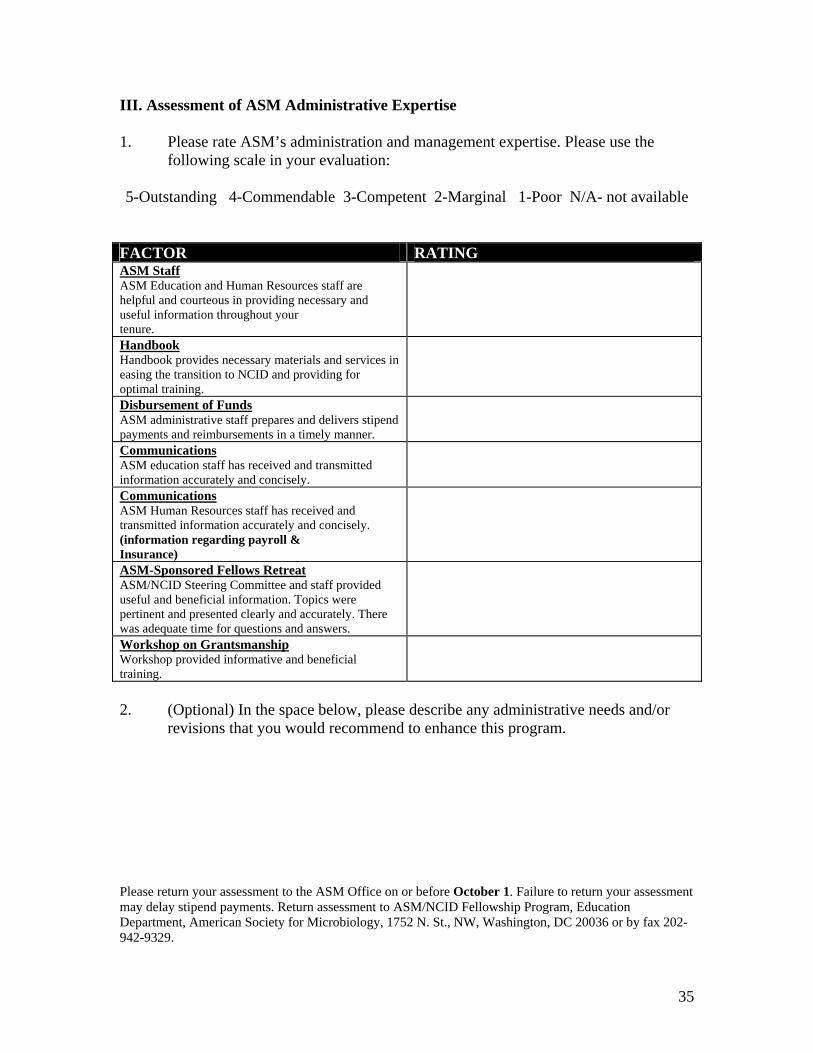
III. Assessment of ASM Administrative Expertise 1. Please rate ASM’s administration and management expertise. Please use the
following scale in your evaluation: 5-Outstanding 4-Commendable 3-Competent 2-Marginal 1-Poor N/A- not available
FACTOR RATING ASM Staff ASM Education and Human Resources staff are helpful and courteous in providing necessary and useful information throughout your tenure.
Handbook Handbook provides necessary materials and services in easing the transition to NCID and providing for optimal training.
Disbursement of Funds ASM administrative staff prepares and delivers stipend payments and reimbursements in a timely manner.
Communications ASM education staff has received and transmitted information accurately and concisely.
Communications ASM Human Resources staff has received and transmitted information accurately and concisely. (information regarding payroll & Insurance)
ASM-Sponsored Fellows Retreat ASM/NCID Steering Committee and staff provided useful and beneficial information. Topics were pertinent and presented clearly and accurately. There was adequate time for questions and answers.
Workshop on Grantsmanship Workshop provided informative and beneficial
training. 2. (Optional) In the space below, please describe any administrative needs and/or
revisions that you would recommend to enhance this program. Please return your assessment to the ASM Office on or before October 1. Failure to return your assessment may delay stipend payments. Return assessment to ASM/NCID Fellowship Program, Education Department, American Society for Microbiology, 1752 N. St., NW, Washington, DC 20036 or by fax 202-942-9329.
35
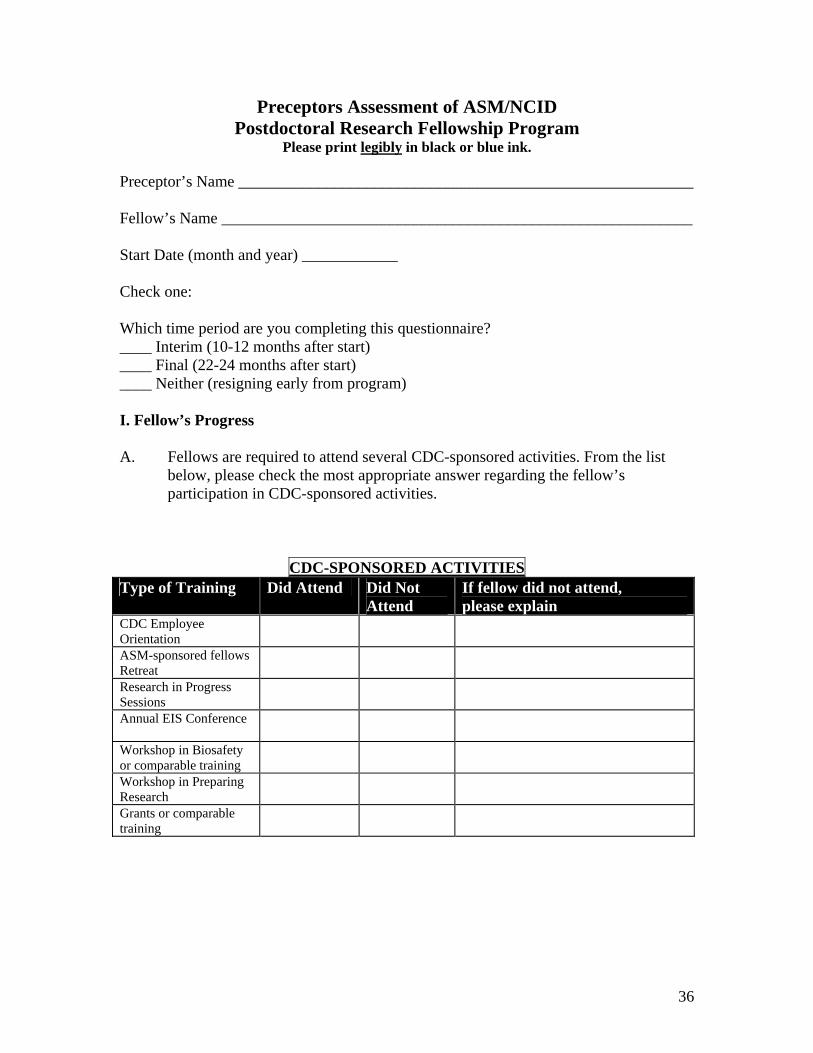
Preceptors Assessment of ASM/NCID Postdoctoral Research Fellowship Program
Please print legibly in black or blue ink.
Preceptor’s Name _________________________________________________________ Fellow’s Name ___________________________________________________________ Start Date (month and year) ____________ Check one: Which time period are you completing this questionnaire? ____ Interim (10-12 months after start) ____ Final (22-24 months after start) ____ Neither (resigning early from program) I. Fellow’s Progress A. Fellows are required to attend several CDC-sponsored activities. From the list
below, please check the most appropriate answer regarding the fellow’s participation in CDC-sponsored activities.
CDC-SPONSORED ACTIVITIES Type of Training Did Attend Did Not
Attend If fellow did not attend, please explain
CDC Employee Orientation
ASM-sponsored fellows Retreat
Research in Progress Sessions
Annual EIS Conference
Workshop in Biosafety or comparable training
Workshop in Preparing Research
Grants or comparable training
36
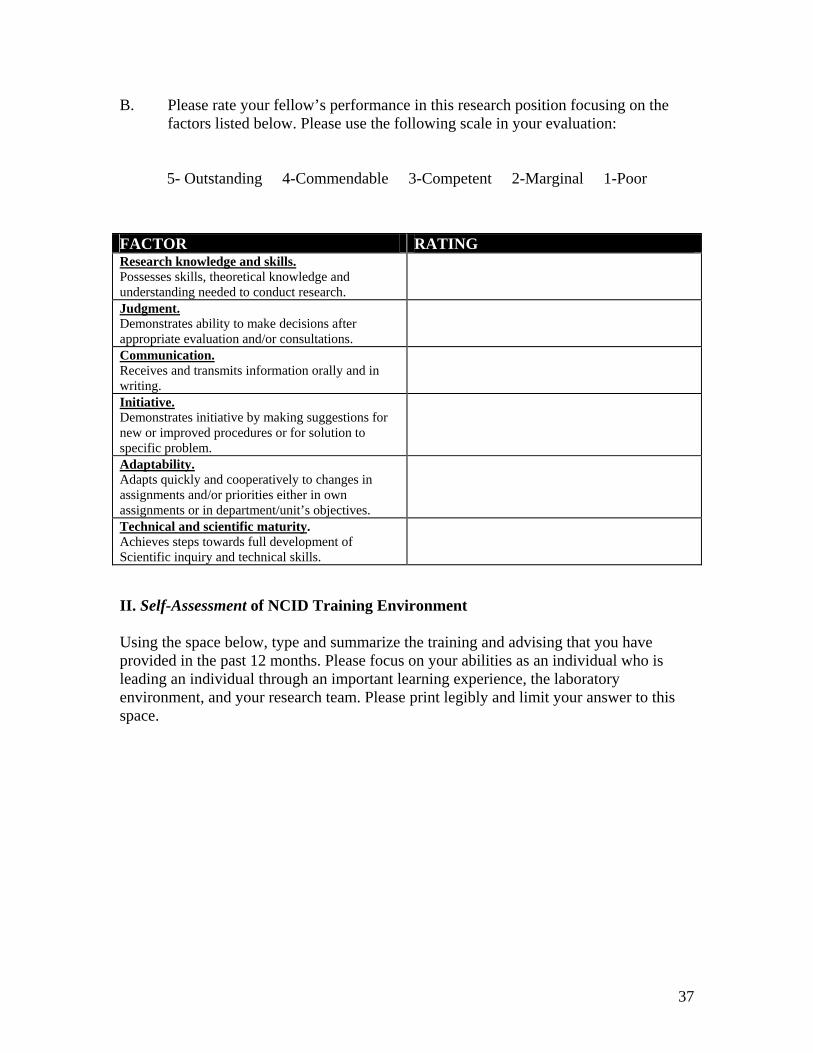
B. Please rate your fellow’s performance in this research position focusing on the factors listed below. Please use the following scale in your evaluation:
5- Outstanding 4-Commendable 3-Competent 2-Marginal 1-Poor FACTOR RATING Research knowledge and skills. Possesses skills, theoretical knowledge and understanding needed to conduct research.
Judgment. Demonstrates ability to make decisions after appropriate evaluation and/or consultations.
Communication. Receives and transmits information orally and in writing.
Initiative. Demonstrates initiative by making suggestions for new or improved procedures or for solution to specific problem.
Adaptability. Adapts quickly and cooperatively to changes in assignments and/or priorities either in own assignments or in department/unit’s objectives.
Technical and scientific maturity. Achieves steps towards full development of Scientific inquiry and technical skills. II. Self-Assessment of NCID Training Environment Using the space below, type and summarize the training and advising that you have provided in the past 12 months. Please focus on your abilities as an individual who is leading an individual through an important learning experience, the laboratory environment, and your research team. Please print legibly and limit your answer to this space.
37
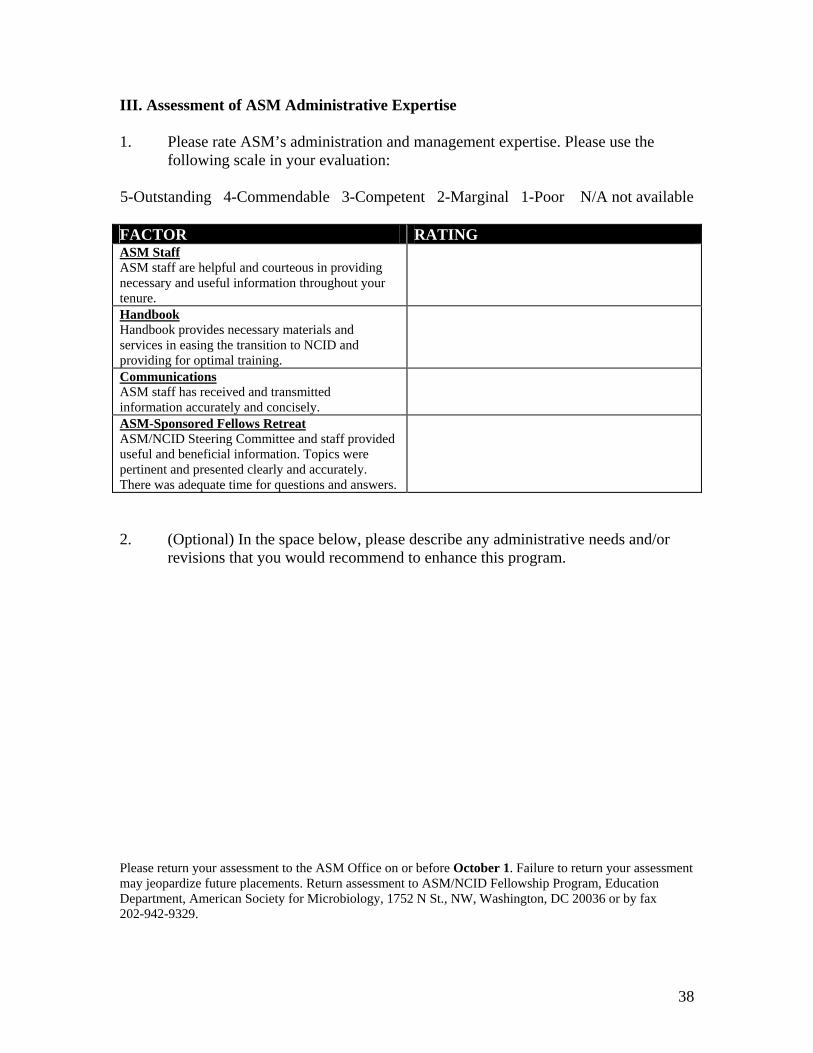
III. Assessment of ASM Administrative Expertise 1. Please rate ASM’s administration and management expertise. Please use the
following scale in your evaluation: 5-Outstanding 4-Commendable 3-Competent 2-Marginal 1-Poor N/A not available FACTOR RATING ASM Staff ASM staff are helpful and courteous in providing necessary and useful information throughout your tenure.
Handbook Handbook provides necessary materials and services in easing the transition to NCID and providing for optimal training.
Communications ASM staff has received and transmitted information accurately and concisely.
ASM-Sponsored Fellows Retreat ASM/NCID Steering Committee and staff provided useful and beneficial information. Topics were pertinent and presented clearly and accurately. There was adequate time for questions and answers. 2. (Optional) In the space below, please describe any administrative needs and/or
revisions that you would recommend to enhance this program. Please return your assessment to the ASM Office on or before October 1. Failure to return your assessment may jeopardize future placements. Return assessment to ASM/NCID Fellowship Program, Education Department, American Society for Microbiology, 1752 N St., NW, Washington, DC 20036 or by fax 202-942-9329.
38





























