Embed Size (px)
Citation preview

December I949 WYERS: Asbestosis 631
nevertheless that a considerable number of menwho develop complicated pneumoconiosis whenaged 30 to 40 are a very bad risk. Tuberculosiswas present in 36 per cent. of all pneumoconioticdeaths, in i6 per cent. of all deaths due to simplepneumoconiosis, and in 39 per cent. of all deathsdue to complicated pneumoconiosis. The figure(36 per cent.) of the extent of complicating tuber-culosis in coal miners' pneumoconiosis is higher
than the figure given by Gooding and others,but it is considerably lower than the figure forother industries, especially for slate mining inNorth Wales where tuberculosis is present in 75per cent. of pneumoconiotic deaths.
Finally, one is impressed by the apparently in-creased susceptibility of coal miners with simplepneumoconiosis to pneumonia and acute respira-tory infection.
BIBLIOGRAPHY
BALGAIRIES, E., DECLERCQ, G., JARY, J., and NADIRAS, P.( 948), Revue Medicale Miniere, 2, 12.
CUMMINS, S. LYLE, and SLADDEN, A. F. (1930), J. of Path.and Bact., 33.
CAMAZIAN (FILS), PIERRE (1947), 'Recherches Sur LesPneumokonioses Dans Les Charbonnages.'
DAVIES, I., and MANN, K. (1948), 'Proceedings of the NinthInternational Congress on Industrial Medicine.' (In thepress.)
FLETCHER, C. M. (I948), Brit. Med. J., I, 1015, 1005.GOODING, C. G. (I946), Lancet, 2, 89I.SMITH, GORDON, Personal communication.GOUGH, J., JAMES, W. R. L., and WENTWORTH, J. E.
(1949), 'A Comparison of the Radiological and PathologicalChanges in Coai Workers' Pneumoconiosis,' 3'ournal of theFacuilty of Radiologists, I, I.
GREGORY, J. C. (I83I), Fdin. Med. and Surg. Journal, 36, 389.GRENFELL, D. R., Personal communication.
HART, P. D'ARCY, and ASLETT, E. A. (I942), Special ReportSeries, M.R.C. No. 243 (B).
JENKINS, T. H. (1948), 'Medico-Mining Aspects of Pneumo-coniosis in South Wales.' Paper read before the South WalesInstitute of Engineers.
KEATING, N., Personal communication.LECLERCQ, J., BALGAIRIES, E., BONTE, G., and
DECLERCQ, G. (1948), Revue Medicale Miniere, 4, 23.McCANN, HURTADO, KALTREIDER and FRAY (I937),
journ. Clin. Invest., I6, 23.NIEIKLEJOHN, A. (I949), Lancet, 2, 360, 'Contribution of the
Employment History to Clinical Diagnosis.'ROGERS, ENID (1944), Paper read before the Tuberculosis
Association.RUBIN, ELI H. (1947), 'Diseases of the Chest,' W. B. Saunders
and Co.TATTERSALL, N. (1926), j. of Indus. Hygiene, 8, 466.'I'HOMAS, R. W., Personal communication.
ASBESTOSISBy H. WYERS, M.A., M.D., D.I.H.
Although certain difficulties remain to be ex-plained, the theory that silica is a causative agentin pulmonary fibrosis is widely accepted. When,however, the fibrogenic potentialities of silicatesare considered, these difficulties are very greatlyincreased. Olivine, for example, has been shownto provoke only a foreign body reaction and hasbeen suggested for foundry work, whereasasbestos is notorious. Studievs in mineralogicalcomposition of atmospheric dusts and ashed lungtissue are progressing and to the data foundtheories of solubility and crystal form are beingapplied. If the solubility is high, as in the case ofsilicic acid gels and sols, the material is eliminatedtoo fast to produce fibrosis. A low solubility, suchas in mixtures of quartz and aluminium, equallyretards fibrosis (King, I938). There appears alsoto be an optimum size of particle with a surfacearea which will release silica in sufficient quantityfor a stufficient length of time.
In animal experiments this was found to beabout o.i micron (Tebbens et al., I945). In thecase of asbestos fibres, it has been shown' that
whereas there is an excess of chrysotile over horn-blende varieties in dusts, ashed lung tissues con-tain only hornblende (Sundius, 1938;. Kuhn,194I). It is concluded that it is the chrysotile insolution which is the fibrosing agent. Gardner(I938) demonstrated by animal experiments thatlonger fibres produced a fibrotic reaction whichdid not occur with shorter fibres and concludedthat asbestosis is, at any rate in part, a mechanic-ally conditioned complex of lung changes. Insupport of this mechanical theory, Johnstone(I948) records the clinical observation that workersat the Thetford Mills, exposed to high concentra-tions of extremely fine asbestos dust, did not sufferfrom asbestosis.
Structurally silica shows continuous three-dimensional arrangements of SiO4 tetrahedra andto these may be related such a surface as to pro-duce the characteristic biological effects. Thosesilicates, therefore, which most nearly resemblequartz in having a three-dimensional network ofsilicon-oxygen tetrahedra are likely, theoretically,to produce similar biological phenomena, T'hese
Protected by copyright.
on April 27, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.631 on 1 D
ecember 1949. D
ownloaded from

632 POSTGRADUATE MEDICAL JOURNAL December I949
are grouped in diminishing order of similarity byNagoelschmidt (I949) as alkali feldspars, sheetstructures such as micas and kaolin, double andsingle chain structures like amphiboles andpyroxenes and, finally, the orthosilicates such asolivine. Animal experiments tend to confirm this,but it is pointed out that the type of binding of thesilicon-oxygen tetrahedra is of biological im-portance and aluminium silicates, such as sericiteand kaolin, are not likely to present a majorsilicosis hazard.The diagnosis of pathological states of the lungs,
due to dusts, also presents many clinical andradiological difficulties. A high incidence of pul-monary disease among those exposed to puresilica is presumptive evidence of an etiological re-lationship, but the rare case of talc pneumo-coniosis is difficult to establish. High atomicweights and consequent radio-opacity produceshadows on the X-ray film from inhaled dustswhich are not necessarily pathological, as, forexample, in the siderosis of arc welders (Doig andMcLaughlin, 1936).
Asbestos, its History, Uses and MineralogyWhatever doubts there may be as to the fibro-
genic potentialities of many silicates, the pro-cessing of asbestos unquestionably exposes theworker to the risk of lung disease. It has beenused on a small scale since very early times, beingknown to the Greeks as o a6£c-,or, signifying un-quenchable. Used as a substantive, - earos wasunslaked lime, whilst the masculine gender,o da a-crog was used to denote asbestos. Theword da6'apETda which in modern Englishspeech signifies the disease asbestosis, was to theGreeks a plastering or stuccoing. This last wordwas originally suggested by Cooke (I924) when healso drew attention to a passage in Herodotusdescribing a cremation cloth made of asbestos.The Romans knew it under the name of amianthus,a word of Greek origin signifying absence ofmiasma or pollution. They obtained it from theItalian Alps and the Ural. It seemed appropriatethat the Vestal Virgins, guardians of the SacredFire, symbol of the deepest emotions and instinctsin Roman family life, the last rite of paganism tobe extinguished, should have used asbestos lampwicks. Another fibrous mineral resemblingItalian amianthus was spun and woven into acloth in Siberia during the i3th century. Afactory for the manufacture of asbestos articleswas opened in Russia in 1760. The re-discoveryof asbestos in I876 contributed greatly to modernindustrial expansion.Today asbestos is used for a wide variety of
purposes. Textiles enter into the manufacture offire-fighting suits, safety curtains and boiler
mattresses. Asbestos enters into the- com-position of lagging material for steam pipes,jointing for steam pipes, panelling of rooms, tiles,the lining of chemical pans, the coating of bulk-heads of ships and marine piers and perhaps mostsignificantly into the brake linings and clutch ringsof motor cars.The properties which commend asbestos to
modern industrialists are its resistance to heat,acids, electricity and sea water and its fibrousstructure which enables it to be spun. Unlikevegetable fibre, it can be split in a longitudinaldirection to microscopic size without discoveringan ultimate elementand without loss of identity.The shortest fibre recorded is Grand Canonchrysotile and is of the order of 0.00075 mm. inlength, whilst the longest is exhibited in theMaritzburg Museum and is 43 in. in length. This'latter fibre came from Umsinga, Natal, and is alsoprobably chrysotile. The best length of fibre forspinning is i4 in. (3.75 cm.).The asbestiform minerals form a group of
silicates which differ widely in chemical com-position, but resemble each other in being fibrousand in their resistance to heat, acids and seawater. Legally ' asbestos means any fibroussilicate mineral, and any admixture containing anysuch mineral, whether crude, crushed or opened '
(Asbestos Industry Regulations, 1931). Min-eralogists classify them as follows:
i. Serpentine Group, 2H20, 3MgO, 2SiO2.Characterized by a high percentage of magnesiaand water, generally white in colour, naturallylubricant and therefore suitable for stuffing boxesand glands. Examples, chrysotile, picrolite.
2. Rhombic Amphiboles, (MgFe)O, SiO2. Sodaconfers a brown colour when present. Like thethird group the members of this division containhigh percentages of ferric oxide and have a lowwater content. The texture is harsh and elastic,enclosing a maximum amount of air in a minimumof incombustible matter. They are particularlyefficient as heat insulators. Examples, antho-phyllite, amosite.
3. Monoclinic Amphibbles. Tremolite, CaO,3MgO,4 4SiO2. Actinolite, CaO, 3(MgFe)O,4SiO2. Crocidolite, NaFe, (Si03)2, Fe SiO3.The presence of soda in this group confers a
lavender blue colour (Hall, I9I8). The ferricoxide content of crocidolite encourages slag forma-tion when it is employed as a wrapping for elec-trodes. The countries of origin are chieflyCanada (white chrysotile), South Africa (bluecrocidolite and the brown amosite), Australia andthe U.S.S.R. It is found in the banded iron-stones, the deposits being classed as cross fibre,slip fibre and mass fibre according to the directionof cleavage relative to the orientation of the vein.
Protected by copyright.
on April 27, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.631 on 1 D
ecember 1949. D
ownloaded from

Dececniber 1949 WYERS: Asbestosis 633
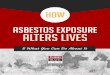
FIG. I. Asbestosis bodies in a section of fibrotic lung. From the case shown in Fig. 4.Photomicrograph x 400.
C(hemical analysis explains some of the varyingproperties of the three groups.
Canadian BlueChr- sotile Crocidolite Amosite
Per cent. Per cent. Per cent.Silica 41 50 47Alumina .. 3 I 6FXerric Oxide.. 2 35 37Magnesia .. 40 2 6Alkalis .. - 8Water 14 4 3
100 100 100
Manufacture'T'he mineral is obtained by open mining, akin
to quarrying. Outside the mine adit the crudeasbestos is reduced in size and pieces of iron aredetached manually (' cobbing') or by mechanicalmeans. It is then transported to the factory inpaper-lined sacks where it is crushed in a largeedge runner or a small pan mill, foreign matterremoved and the fibres opened in a Crightonmachine. The ancient process of carding follows,
by which the fibres are made to lie parallel in acontinuous' sliver.' Essentially this machine con-sists of toothed drums and condenser rollers. Thederivation of the word ' card' from the Latincarduus, a teasel or thistle, doubtless indicates themeans by which this operation was carried out onother fibres in primitive times. Slivers are twistedtogether to form strong yarn on spinning frames,by ring or flyer, as in other textiles. The materialis then plaited into rope or it may be woven intocloth on the conventional power loom. To themedical observer, perhaps, the loom as a specialsignificance for the weaver's beam has given itsname to living tissues. Occupying a horizontalposition in modern looms, its historical positionwas vertical. The Greeks called it 'arTOs, as theydid a ship's mast or indeed anything which wasset upright. The word came to be applied to thecloth itself and eventually to the histologicalstructure of living organisms.
History of AsbestosisIn I906 the Departmental Committee on Com-
pensation for Industrial Diseases (1907) heardevidence from various authorities arising out of
G1
Protected by copyright.
on April 27, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.631 on 1 D
ecember 1949. D
ownloaded from

634 POSTGRADUATE MEDICAL JOURNAL DJ)cember I 949
..
FIG. 2.-L.E.S., female, aet. 35. Spinning dept., fiveyears. P.M. section of lung showNing blue-blackpolygonal areas of asbestosis and thickened pleura.At the low%er pole a squamous carcinoma surroundsan aibscess cavity.
the inclusion of certain industrial diseases in theThird Schedule of the WVorkmen's CompensationAct, I906. At that enquiry Montague Murrayreported the case of an asbestos worker who haddied in the Charing Cross Hospital in I900 of' typical fibroid phthisis.' This man, a card roomworker aged 34, had stated that nine of his work-mates had died round about the age of 30. Whilstagreeing that fibroid phthisis was a clinical entityand specific to certain occupations, the Committeefelt they could not recommend its inclusion in thelist of diseases under the Third Schedule owing todifficulties chiefly of certification. Cases ofasbestosis continued to be reported, notably byFahr (I914) and by Cook (I924). It was Seiler'scase (1928), however, which seemed to establishan unequivocal relationship between asbestosand pulmonary fibrosis and which precipitated
the inquiry leading to the Report of Merewetherand Price (1930). In the following year appearedthe Silicosis atid Asbestosis (Medical Arrange-ments) Scheme (I93I), the Asbestos Industry(Asbestosis) Scheme (I93I) and the AsbestosIndustry Regulations (193I). The first dealt withthe constitution and functions of a MedicalBoard, the second with the award of compensationand the third with the control of dust. Legislationhas been generally effective in controlling thedisease.
Since I93I all entrants to dusty departmentshave been medically examined initially and againannually by panels of experts. Use has been madeof radiology and much pathological materialexamined. Dust exhaustion has received specialattention; in onie factory spinning frames are beingtotally enclosed in perspex with an ingenious
Protected by copyright.
on April 27, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.631 on 1 D
ecember 1949. D
ownloaded from

Decenmber I949 WYERS: Asbestosis 635
device which permits easy access to bobbins.Handling has been reduced to a minimum andgood housekeeping kept on a high standard. Withvery few exceptions, cases certified by the Boardas asbestosis have industrial histories extending toperiods prior to 1931.
PathologyWhereas the heavier and smaller particles of
silica find their way to the alveoli and thence to thelymphatic channels, the lighter and larger particlesof asbestos block up the finer bronchioles. Chainsof silicate tetrahedra with intervening cationsdetermine the fibrous structure of asbestos andthese chains in frayed bundles interlock and arearrested. Hence silicosis is a fibrosis of the lymphnodes and asbestosis a fibrous cuffing of thebronchioles. Dangerous fibres measure about 20microns and a noxious concentration is said tooccur when the dust count exceeds five millionparticles per cubic foot of air (Page, I937).There is no local necrosis or leucocytic reaction
to the trapped fibre such as would occur if aprotoplasmic poison like colloidal silica hydroxidewere liberated. It seems significant that if thefibrous character of chrysotile asbestos is absent,as in its chemical equivalent serpentine, the dustis inert. Instead, the lining epithelial cells aredesquammated as a result of friction and makeattempts to engulf fibres which proving too long,are sometimes observed projecting from these' dust ' cells. Asbestosis giant cells are also seen,due to small aggregations of dust cells. They arepigmented, stippled and multinuclear. Fibro-blasts appear around bronchioles and alveoli, ininterlobular septa and in the subpleural connectivetissue. Asbestosis bodies and pigment are alsopresent. Finally there is an invasion by collagenousfibres to form the characteristic reticular .patternaround the distal arborizations of the bronchialtree. The alveoli, capillaries and venules arecrushed by the fibrosis.
Asbestosis bodies can be demonstrated in thelungs, pleura and sputum. The length of timetaken for them to develop is unknown. Theycannot be found in the mineral itself. It has beenshown by staining reactions with sodium nitro-prusside and ammonium sulphide and by dis-solving the outer portion with concentrated sul-phuric acid that they consist of a central fibre ofasbestos (Fig. i) with an iron-containing, seg-mented covering which is thought to have beendeposited by a colloidal reaction between the fibreand the blood proteins (Gloyne, I929). Theirpresence is held to be evidence of exposure toasbestos and not of the disease itself.
Dense, sessile adhesions of the pleura arecommon and the interlobar fissure obliterated.
The pleura has a ground glass appearance withyellow, horn-like plaques 2 or 3 in. in diameterbesides patches of recent pleurisy. The cut surfaceof the lung exhibits the typical blue-black poly-gonal areas, roughly lobular in distribution, -1 in.to 4 in. (3 mm. to 6 mm.) in diameter on a redbackground of bronchopneumonia. The areastend to confluence at the bases and exhibit the' pleural drift' common to the pneumoconioses.Confluence is becoming rarer as the dust cloudbecomes less concentrated (Fig. 2). Compensa-tory emphysema, on the other hand, seems to beoccurring more frequently as cases live longer. Itoccurs chiefly along the margins of the lungs,sometimes giving rise to bullae but not socommonly as in silicosis. One case in the presentseries of i i5 fatal cases died of a spontaneouspneumothorax consequent on rupture of such abulla. The right heart is generally enlarged andthere are the usual signs of back pressure in theliver.
Clinical SyndromeIn the writer's series the average exposure for
males was I6.2 years, for females 7.3 years and forall cases IO.4 years. The duration of the diseasewas 6.4 years for both sexes. The mean age atdeath was 46.5 years in the case of men, 37.5years in the case of women and 40.8 years for all
G. 3a. ... S d .
X-ray of lung showing fine mottling. Fingers showgross clubbing. Advanced asbestosis.
Protected by copyright.
on April 27, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.631 on 1 D
ecember 1949. D
ownloaded from

636 POSTGRADUATE MIEDICAL JOURNAL December 1949
cases. Dyspnoea is a universal complaint:Burton Wood regarded asbestosis as a mono-symptomatic disease. Dry cough is noticeable onrising in the morning and during changes oftemperature. A paroxysm usually terminates withthe production of some thick mucoid sputum, veryrarely flecked with blood and in the later stagescontaining nummules of pus. An increase in thequantity of sputum indicates a complicating factor.Anorexia, loss of weight, fatigue and chest painsare occasional symptoms.The cardiovascular signs of the disease are im-
portant, because once established they are per-manent, whereas adventitious sounds in the chesttend to be evanescent. An earthy cyanosis hasbeen described. Of 53 consecutive cases ofasbestosis examined by the writer, 29 showedclubbing of the fingers, the toes being similarlyaffected in eight of the cases, an incidence of54.7 per cent. In the same series the secondpulmonic sound was found to be accentuated in33 patients, that is to say 62.2 per cent. of thecases. These signs appeared separately, togetherand quite often not at all even in advanced disease.The liver was never palpable in an ambulatorypatient nor was there oedema of the dependentparts.The chest is flattened bilaterally. The respira-
tory excursion rarely exceeds i in. (2.5 cm.).Percussion often reveals a sensation of resistanceto the finger (' felting ') which may be general orlocalized. Probably this is a reflection of thedense character of the fibrotic lung or of thepleural plaques which are often seen post mortem.Hyper-resonance is occasionally noted. Dry,crackling sounds can generally be heard along theemphysematous margins but often become gen-eralized or disappear altogether in the sameindividual. An odd sonorous rhonchus may beheard. There is deficient air entry at the basesand expiration over the anterior aspect of the chestis harsh.
Radiological Appearances'Whereas the roentgenogram may show con-
siderable involvement in silicosis with few, if any,symptoms, the reverse is apt to be found inasbestosis' (Sayers, 1938). This is the opinion ofall with experience of the disease. The typicalappearance of the lung fields is a diffuse haze orpin-point mottling in the lower halves or two-thirds (Fig. 3). Emphysema may be seen in theupper zones and, of later years, a granular patternin the lower zones somewhat resembling cottonwool which has been teased out (Fig. 4). Thedomes of the diaphragm are flattened and mayshow coarse striae running up into the lower lungfields. The ver-tical diameter of the chest is
FIG. 4.-T.McK., aet. 45. Sectional dept., i8 vears.Asbestosis bodies shown in Fig. I. X-ray of lungshows coarse fibrosis and emphysema. Grrossclubbing of fingers. Eventually died with ttuber-culous infection.
diminished. Thl e costo-phrenic sulcus is fre-quently blunted. A shaggy left cardiac border isoften seen in aevanced cases and sometimes theentire silhouette and diaphragmatic cupolac areblurred.
ComplicationsBronchiectasis has been stated to occur fre-
quently. Only three undoubted cases occurred inthe present series and one of these was a con-genital condition affecting the apex.
Pregnancy was associated with the deaths oftwo women suffering from asbestosis. The diseasedoes not seem to be adversely affected by preg-nancy, but the strain of labour may tip the balancein favour of right heart failure.
Bronchopneumonia is almost invariably foundpost mortem. The next commonest complicationis tuberculosis with a much lower incidence thanin silicosis and affecting a lower age group. InII5 fatal cases, I5 men and 2I women, 3I.3 percent. in all, showed also pulmonary tuberculosis.The mean age at death was 34.9 years after anaverage exposure to asbestos of 7.6 years. Takingthe remaining cases alone, the age at death was43.6 years, after an exposure of 11.5 years.
Protected by copyright.
on April 27, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.631 on 1 D
ecember 1949. D
ownloaded from

December I1949 WYERS: Asbestosis 637
An excess mortality from cancer of the lung incases of asbestosis was recorded by Merewether(I947). Of 6,884 cases of silicosis I.32 per cent.were found to be complicated by pulmonary cancerwhereas the incidence was I3.2 per cent. in 235cases of asbestosis. Wedler (I943) collected 92post-mortem reports of asbestosis cases fromdifferent parts of the world and found an in-cidence of i6 per cent. pulmonary cancers. Thedevelopment of the lesion corresponded with thelengths and intensity of the exposure (I2 to 42years). Boemke (I947) called attention to theassociation of asbestosis with pulmonary cancer,the latter almost always taking the form of car-cinoma of the pavement epithelium. He thoughtit possible that, in addition to chemical processes,the purely mechanical effects of the asbestosneedles may also be responsible for the develop-ment of carcinoma.
In the present series of II5 deaths fromasbestosis iI males and six females had pulmonarycancer whilst cancer of other organs was presentin three males and four females (pancreas, colon,stomach, ovary). The proportion of pulmonarycancers in the series was therefore I4.8 per cent.Squamous cancers were present in nine cases, oatcell in five, columnar cell in one, endothelioma ofthe pleura in one and the histology unknown inone. Two of the cases were brothers. The meanage at death was 52 years, the mean exposure toasbestos dust I7.3 years and they died a meanperiod of 6.6 years after leaving the industry(Fig. 2).
Socio-Medical Aspects of AsbestosisIt is difficult to assess the effects of such
factors as personal habits and the preference offamilies and those of defective physique for certainoccupations. Meiklejohn (I929) has pointed outthe possible effects in the past on the spread oftuberculosis among Sheffield knife grinders by thehabit of spitting into the water trough throughwhich the abrasive wheel passed. Stewart (I929)has indicated that the high incidence of tubercu-losis among boot operatives is due to the attractionof disabled persons and their families to a lightoccupation. Similarly the family histories of thosedying of asbestosis and tubercle frequently dis-close the presence of tuberculosis in those of thesame household who have never been exposed toasbestos.
Post-employment survival showed a sexdifferentiation; the mean period for men in thisseries was 2.3 years and for women 9.8 years. Nodoubt many women ceased work to marry andsymptoms of asbestosis did not appear until sometime later.Of the II5 deaths only two had commenced
work subsequent to the I93I Regulations, a manafter ten years' exposure and a woman who alsohad tuberculosis after two years' exposure. Threeother men have also developed the disease afterexposures of five, four and four years respectively,the last one having been certified in I946.The writer has 28 cases under observation at
present. The men are occupied as follows:business executive, storekeeper, painter andwindow cleaner, lagger (in other employ), cleaningbrasses, ventilation engin2er, in charge of sportsand social sections, laboratory handyman, retired,small printing press operator, foreman in chargeof stores, foreman in charge of rubber department,light carpenter, tally clerk (w2ek-end relief),handyman in canteen, at home recovering fromtuberculosis and one relief gateman. The womenare occupied as follows: light housework, incharge of works solarium, canteen work, repairingoveralls in works laundry, three doing light house-work and two doing sewing duties and mendingduties at home.The reduction in the intensity of the dust cloud
seems to be producing a more chronic type ofdisease. Merewether's investigation of 1929 in-dicated a period of seven years' exposure for thedisease to develop, whereas this series, whichcommenced in I93I, indicates that an exposure often years is necessary.Through the kindness of Dr. Roodhouse
Gloyne, the writer had access to the late Dr.Burton Wood's notes on 89 cases of asbestosiswhich he had collected up to I93 I. Of these casesI7 showed clubbing of the fingers, i.e. I9.I percent., a much lower figure than the incidence of54.7 per cent. in this series. Radiologically, thefine mottling is giving place to a coarser shadowingwhich seems to be due to compensatoryemphysema. At post mortem, confluence of thecharacteristic lesion is becoming rarer and cancerincidence is rising.
Other SilicatesOf the other silicates, talc is the only one con-
cerning which there is definite evidence of aharmful effect on the lungs, although there is someclinical and radiological evidence of pulmonaryfibrosis due to mica. McLaughlin et al. (I949)reported the first case of talc pneumoconiosis,confirmed at post mortem, to have occurred inthis country. The radiographs showed nodularshadows which, on the left side were fluffy.Histologically the lung showed greyish nodules ofloosely woven fibrous tissue in association withbronchioles. There were also 'curious bodies'closely resembling asbestosis bodies. Mineralogicalinvestigation proved that the condition was not,in fact, asbestosis but due to talc, a hydrated
Protected by copyright.
on April 27, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.631 on 1 D
ecember 1949. D
ownloaded from

638 POSTGRADUATE MEDICAL JOURNAL December 1949
magnesium silicate Mg,Si4,0,(OH2). Talc mayin certain instances arise as an alteration productof tremolite and it may replace anthophyllite, inboth cases inheriting an imperfectly fibrous form.Norwegian and Canadian talcs are platy butcontain a proportion of fibres. The respiratory
passages appeared to have acted as a filter allowingthe fibres to get into the lungs whilst rejecting theplates. The authors concluded that talc pneumo-coniosis may be ascribed primarily to the physicalform (acicular crystals) of the mineral, but thatasbestos is more actively fibrogenic.
BIBLIOGRAPHY
ASBESTOS INDUSTRY (ASBESTOSIS) SCHEME (193I),H.M. Stationery Office.
ASBESTOS INDUSTRY REGULATIONS (193I), H.M.Stationery Office.
BOEMKE, F. (I947), Med. Monatsschr., I, 2-6.BOEMKE, F. (I947), Chem. Zentr., I, 835.COOKE, W. E. (I924), Brit. Med. J., 2, I47.DEPARTMENTAL COMMITTEE ON COMPENSATION
FOR INDUSTRIAL DISEASES (o907), Minutes of Evidence,Cd. 3496, p. 127, H.M. Stationery Office.
DOIG, A. T., and McLAUGHLIN, A. I. G. (I936), Lancet, I,771.
FAHR, T. (9194), 'Asbestosis-Pneumoconiosis,' Munch. Med.Woch., 6I, 625.
GARDNER, L. U. (I938), J7. Amer. Med. Ass., xII, I.GLOYNE, S. R. (I929), Tubercle, I0, 404.HALL, A. L 'Asbestos in the Union of S. Africa,' Geological
Survey, Aiemoir No. 12, I9I8.JOHNSTONE, R. T. (I948), Occupational Medicine and Industrial
Hygiene, p. 369.KING, E. J., and ROMAN, W. (I938), Biochem. -7., 32, 2283.KUHN, J. (1941), Arch f. Gewerbepath. und Geverbehyg, I0, 473.
McLAUGHLIN, A. I. G., ROGERS, E., and DUNHAM, K. C.(I949), 'Talc Pneumoconiosis,' Brit. Y. Industr. Med., 6, 184.
MEIKLEJOHN, A. (1929), M.D. Thesis, Glasgow.MEREWETHER, E. R. A. (I947), Annual Report of the Chief
Inspector of Factories, H.M. Stationery Office.MEREWETHER, E. R. A., and PRICE, C. W. (1930), Report on
Effects of Asbestos Dust on the Lungs, H.M. Stationery Office.NAGOELSCHMIDT, G. (I949), Research, 2, 170.PAGE, R. T., and BLOOMFIELD, J. J. (I937), U.S. Pub. Health
Repts., 52, 1713.SAYERS, R. R., and LANZA, A. J. (I938), Silicosis and Asbestosis,
p. 6o.SEILER (1928), Brit. Med. Y., II, 982.SILICOSIS AND ASBESTOSIS (MEDICAL ARRANGE-
MENTS) SCHEME (I93I), H.M. Stationery Office.STEWART, A., et al. (1929), Brit. Med. Y., I, 926.SUNDIUS, N., and BYGDEN, A. (1938), . Id. Hyg. Tox., 20,
351.TEBBENS, D. D., SCHULZ, R. Z., and DRINKER, P. (1945),
Y. Ind. Hyg. Tox., 27, 199.WEDLER, H. W. (1943), 'Asbestose und Lungenkrebs,' Dent.
Med. Woch.Aug. 6, 69, No. 31/32, 575-6.
THE ROYAL MEDICAL FOUlNDATIONof Epsom College
We appeal to all members of the medical profession who do not already do so, to subscribe to the above Royal Medical Foundation.In every profession some must fall by the wayside; others must inevitably fall upon evil days.Our object is to help the families of those less fortunate brethren. To that end the Foundation in 1948 has provided
(a) 50 ordinary pensions to medical men or their widows .... ... ... ... .... ... ..... ... ... ... ..1,500(b) 45 Foundation Scholarships for boys-educated, clothed and maintained entirely free of cost ... ... ... ... 8,702(c) 13 Scholarships for girls .... ... ... ... ... ... ... ... ... ... ..... .... ... ... 570(d) Education of 28 boys at reduced fees ... ... ... ... ... ... ... ... ... ... ... .... 1,968(e) 140 pensions and annuities of varying amounts ... ... ... ... ... ... ... ... ... ... ... .3,023(f) Grants towards education of 56 boys and girls ... ... ... ... ... ... ... ... ... ... ... 1,843(g) Grants to medical men, widows and spinsters ... ... ... ... ... ... ... ... ... ... ... 497
This is an expenditure of £18,103 in the year.In order to maintain this assistance we have to rely upon the generosity of our subscribers and donors for over £14,500 per annum.Without sufficient help from them even our existing benefactions would have to be curtailed. Owing to lack of funds, many deserv-
ing applicants-medical men, widows and children of school age-remain unassisted. The Sherman Bigg Fund enables the Foun-dation to make educational grants for those who cannot obtain Scholarships. Donations to augment the income of this Fund will bemost welcome.
We therefore beg you earnestly to send either a subscription or a donation to this Foundation during 1949. When doing so youmay, if you wish, stipulate the particular form of benefaction on which it is to be expended.
Subscriptions and donations may be sent to any of us, or preferably to the Secretary, the Secretary's Office, Epsom College, Surrey,by whom full information will gladly be sent on request.
JOHN SELL COTMAN, TreasurerHAROLD SPITTA, ChairmanERNEST GOODHART, Vice-Chairman
Protected by copyright.
on April 27, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.290.631 on 1 D
ecember 1949. D
ownloaded from















![Notes on Some Remedies XXVIII. Drugs in Helminthic ... · PDF fileApril, i949] DRUGS IN HELMINTHIC DISEASES ; CHAUDHURI 155 (3) Trichuriasis (whipworm infection) Like threadworms,](https://img.pdfslide.us/doc/110x75/5a78f6fe7f8b9a00168b8bf8/notes-on-some-remedies-xxviii-drugs-in-helminthic-i949-drugs-in-helminthic.jpg)