Embed Size (px)
Citation preview

128
URETERIC CALCULI *Diagnosis, Behaviour and Appearances, wraith Seven Case Histories
By VALENTINE A. J. SWAIN, F.R.C.S.
The symptoms which are produced by thepresence of a calculus in the ureter are well known.The pain is situated in a linz from the loin downto the groin and may be referred to the testicle orupper part of the thigh, its location depending onthe site of impaction in the ureter. If the stone islodged in the upper part of the ureter, the in-creased tension in the pelvis of the kidney due toblockage causes pain and tenderness in the pos-terior renal angle. If the impaction is lower downin the ureter, the pain and maximum tendernessare situated in the anterior abdominal wall in theupper or lower quadrants, in the region of thelateral border of the rectus abdominis muscle. Ifthe obstruction is in the distal end of the ureter,the pain is referred to the groin, perineal or rectalregion, though in most instances renal pain andtenderness are also present. By the alteration ofthe site of the pain, the patient will appreciate thedescent of the stone down the ureter.The pain is usually colicky in nature and varies
in intensity, lasting a few minutes, causing sweat-ing, pallor and vomiting in severe cases. Ab-dominal distension may also occur. In addition,urinary symptoms of haematuria, increased fre-quency and dysuria may be present. In somecases a stone or ' gravel ' may be passed perurethram a few days after an attack of colic.The presence of an excess of oxalate crystals in
the urine, or infection of the urinary tract, maysimulate pain of calculous origin. In cases ofhaematuria from the kidney, the passage of bloodclots along the ureter may produce colicky symp-toms similar to that described above. Sometimesa mistaken diagnosis of cholecystitis, appendicitisor diverticulitis is made, depending on the localiza-tion of the pain. Abdominal distension, accom-panied by intermittent colic and tenderness, willsimulate intestinal obstruction, but the presence ofposterior renal discomfort and tenderness, andperhaps urinary symptoms, will lead to a correctdiagnosis.
Occasionally a ureteric stone may be silent andbe discovered accidentally by a routine radiograph
* Based on a Postgraduate Lecture delivered at theRoyal Northern Hospital.
of the urinary tract (Fig. i). In the majority ofsuch cases an antecedent history of past urinarysymptoms or infection can be obtained. Duringthe initial attack, a small stone originally from thekidney becomes lodged in the ureter, usually in thelower third, where it will nestle and become em-bedded in the ureteric wall, ultimately blockingthe ureter by further incrustation. Infection andback pressure will eventually cause irreparabledamage to the kidney.As a rule, in most cases the signs and symptoms
of ureteric calculi are characteristic and can bediagnosed with confidence, but sometimes evenafter full investigation the presence of a stonecannot be demonstrated; its detection radio-logically depends on the size and chemical com-po3ition of the calculus and whether it is obscuredby extraneous bowel shadows in the radiograph.
In some instances an opacity in the course of theureter will require further elucidation by means ofintravenous and retrograde pyelography. Theformer will show the relation of the line of theureter to the opacity and indicate the function ofthe kidneys; in the latter, ureteric catheterizationmay encounter an obstruction, or at the cystoscopicexamination a stone may be seen lodged in theureteric orifice. The intravenous injection ofindigo carmine (io cc. of 0.4 per cent. solution) willdemonstrate whether the outflow of the urine isobstructed, by the absence of its excretion, after afew minutes, into the bladder. It will also indicatethe function of the kidney on the healthy side.The dye should normally become visible in goodconcentration at five minutes after the injection.If a ureteric catheter can be manipulated beyondthe stone, temporary relief of pain can be obtained,for drainage of the urine above the obstruction willlessen the tension in the renal pelvis. A specimenof urine should be collected via the uretericcatheter, examination of which will show thedegree of infection of the kidney and the causalorganism. If the stone prevents the passage ofthis catheter, the slow introduction of an opaquefluid up the catheter will outline the calculus anddistend the ureter below. This method wasadopted in Case 2; thereby the outline of a trans-lucent ureteric stone became visible, and the
copyright. on O
ctober 18, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.305.128 on 1 M
arch 1951. Dow
nloaded from

Alarch I SVAIN: Ujeteric Calc5li 129
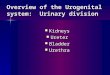
FIG. I.-A large ureteric stone on the left sideof the pelvis (Case 6).
....Q.; s
FIG. 2.-The passage of a ureteric catheteris hindered by an obstruction at 6 cm.from the distal end of the ureter (Case2).
.... ....
-,xXj ~~~~............. FIG. 3.-The introduction of a few ccs.of uroselectan via the catheter out-lines the lower end of a ureteric cal-culus. This urate stone is translucentto X-rays.
copyright. on O
ctober 18, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.305.128 on 1 M
arch 1951. Dow
nloaded from

130 POSTGRADUATE MEDICAL JOURNAL .March I951
....
:.:..: .... .e..:
.....o..
. },,j;.
..;....
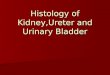
FIG. 4.-This shows that the catheter inthe left ureter and an oval opacity onthe left side of the pelvis are inalignment in the antero-posteriorview (Case i).
.:': ..:i ..:
| : . .. ...
..... E
FIG. 5.-Likewise in the oblique view, theureteric catheter and the opacitv are inline. Is this opacity a ureteric cal-culus? (Case i).
Fic. 6.-A small stone lying in the middle of the penileurethra (Case 4).
copyright. on O
ctober 18, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.305.128 on 1 M
arch 1951. Dow
nloaded from

SWAIN: Ureteric Calculi
introduction of the catheter. The fluid aided thedescent of the stone into the bladder (Figs. 2and 3).On the other hand, if a catheter can be passed
up the ureter without difficulty, the opacity isprobably not a stone. Two radiographs should betaken of the area, and if they show that the roundedshadow and the line of the catheter are approxi-mate in both antero-posterior and oblique views, theopacity is probably in the ureter, but if they areremote in either view it is most likely to be extra-ureteric-probably a phlebolith. Difficulty ariseswhen a shadow, such as a phlebolith, is adjacentto the ureter, as in Case i, and in these circum-stances stereoscopic views may be used withadvantage.
Case I. Mr. F. F. Aged 63.September I946. Onset of intermittent pain in
the left loin. No micturition symptoms. Intra-venous pyelogram showed a shadow in the lineof the ureter without obstructing its excretion.This was assumed to be a stone and was treatedexpectantly with retrograde catheterization anddilatation of the ureter. Antero-posterior andoblique views on two occasions showed the' stone '
to be in juxtaposition to the catheter (Figs. 4 and5)-
In view of the continued symptoms and failureof- the calculus to descend, operation was per-formed in April 1949. A ureteric catheter waspassed as a preliminary measure and the lower endof the ureter was exposed by an extra-peritonealapproach, and the ' stone ' was seen to be adjacentto the ureter. It was, in fact, a phlebolith lyingin a small vein; this vessel was divided afterligation above and below the phlebolith; the veinwall was incised and the phlebolith was removedwithout difficulty. In appearance it was a smooth,oval, calcified mass about 6 mm. x 4 mm. (Fig.IOC).The patient made a good recovery and for-
tunately his loin pain was relieved. He wassymptom-free when seen a year later after thissurgical interference.
Case 2. Mrs. G. D. Aged 38.June 21, 1949. Onset of pain in the left iliac
fossa radiating to back; constant ache and oc-casional colic which caused her to double up,associated with occasional increased frequency ofmicturition.July I2, 1949. Cystoscopy. Bladder normal.
Left ureteric catheter was held up at 6 cm. fromthe ureteric orifice.
September 13, I949. The ascending pyelo-graphy was repeated and the catheter was held upat the same site. An opaque dve was injected
along the catheter and showed a cup-shapedfilling defect at its upper limit as if outlining astone (Figs. 2 and 3).
September 27, I949. Exploration of ureteradvised.November I2, I949. The stone was passed per
urethram whilst patient was awaiting admissionto hospital. It was a urate stone (Fig. 6a).
December 6, I949. Intravenous pyelogramshowed return of function to the right kidney withgood excretion after five minutes.June I950. No further symptoms.As urate stones are usually translucent to
X-rays, their presence is liable to be overlookedunless a complete investigation is carried out.Fortunately this type of stone is uncommon.
Case 3. Mr. R. S. Aged 36.Past History. 1944 discharged from the Army
on account of small right renal calculi associatedwith colic. He had haematuria on one occasionand intermittent symptoms since that time.
February I, I948. Blood in the urine, pain inthe right loin and urgency of micturition.
February I7, 1948. Passed elongated stone perurethram (Fig. 6b).
Case 4. Mr. J. F. Aged 54.August 2I, 1949. Difficulty of micturition;
intermittent flow; tenderness in penile urethra.No previous history of renal pain or colic.August 28, 1950. X-ray showed stone in urethra
(Fig. 6). On passage of a sound a stricture wasencountered about 3 in. from the external meatus.After dilatation under an anaesthetic the calculuswas manipulated past this stricture and extracted.
Past History. Gonorrhoea 32 years ago.Further investigation showed that he had a few
small calculi in the left kidney, which were prob-ably secondary to the obstruction in the urethra.
Case 5. Mr. C. S. Aged 68.October 17, 1949. Admitted as an emergency
with a diagnosis of subacute obstruction with ahistory of ten days' pain in the left iliac fossa,associated with nausea, but no urinary symptoms.There had been no bowel action for five days priorto admission. Examination showed a distendedabdomen with tenderness in the left lower quad-rant. This attack was relieved by an enema.Signoidoscopy was normal and a barium enemashowed a few diverticula in the pelvic colon.Blood urea was 38 mgm. per cent., and the urinewas sterile. He was discharged a week after ad-mission with a tentative diagnosis of diverticulitis.
September io, 1950. Re-admitted with a similarhistory of constipation, pain in the left side andvomiting. The pain did not radiate and there were
March I 951I I 3 t
copyright. on O
ctober 18, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.305.128 on 1 M
arch 1951. Dow
nloaded from

132 POSTGRADUATE MEDICAI, JOURNAL March IQ5I
......t. '...^gt
... ... ..
* ....
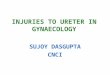
FIGS. 7 and 8.-Two opacities in the pelvis, the uppzr one of which is le3s distinct than the rounded one below (Case 5).
no abnormal physical signs apart from slighttenderness in the left iliac fossa. There were nourinary symptoms and relief was again obtainedafter an enema had been administered.
September 21, I950. An intravenous pyelogramshowed that both kidneys were excreting normallyafter five minutes, and in the line of the left ureterthere was an opacity (Figs. 7 and 8). It did notappear to obstruct the flow of dye and there wasalso a phlebolith below this ureteric stone on thesame side; I4 days later the patient passed asmall stone per urethram.
Past history,. In I943 he had a similar attack ofpain and passed a small stone.
Case 6. Mrs. V. D. Aged 30.September I947. She reported to hospital for
examination on account of amenorrhoea, whichwas, in fact, early pregnancy. She suffered fromoccasional frequency of micturition but had norecent kidney or bladder pain.
Past history. For the past i8 years she hadsuffered from intermittent attacks of pyelitis, thelast attack of renal pain being about three yearsago. Seven years ago she developed pulmonarytuberculosis for which she received treatment, thelutng condition now being quiescent.
Investigations. Intravenous pyelogram showednon-functioning of the left kidney due to a largestone at the lower end of the ureter, whichprobably originated a few years ago (Fig. i).There was also a small stone in the right kidney,which was functioning normally. Urine showed agrowth of coliform bacilli.
Case 7. Mr. J.R. Aged 57.October 25, I949. Two years' history of ur-
gency of micturition and increased frequency dayand night. Moderate enlargement of the prostate.Examination showed that he had a narrow externalmeatus whicn required dilatation before a cysto-scope could be passed. Apart from trabectulationof the bladder the cystoscopic appearances werenormal. Straight X-ray showed a linear shadowin the region of the left ureter (Fig. 9). Anintravenous pyelogram indicated that this wasoutside the line of the ureter and was probablycalcification in one of the iliac vessels. Thisopacity was an incidental finding whicn could havebeen mistaken for a ureteric stone.
The cases quoted above illustrate a few of theproblems of the diagnosis of ureteric calculi andtheir manifestations.
copyright. on O
ctober 18, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.305.128 on 1 M
arch 1951. Dow
nloaded from

Alarchii 9 i SWAIN: (treteru( Calcull I 33
....
FIG. 9.-Excretory urogram showing a line of calci-fication lying outside the line of the ureter-probably calcification in a vessel. Case 7.
The specimens obtained in Cases I, 2 and 3respectively are illustrated in Fig,. io, namely, anoxalate stone, a urate stone and a phlebolith. Thesurface of the oxalate calculus is spiculated (Fig.iob) and this irregularity renders the passage ofthis type of calculus down the ureter more difficultthan a stone with a more even surface.The urate stone is smoother (Fig. ioa), and on
its surface a longitudinal groove can be seenwnich will enable a fine stream of urine to passalong the ureter, thereby preventing completeblockage from above. Should this channel be-come blocked the tension in the pelvis and ureterabove will increase, thereby causing renal andureteric pain. Contraction of the musculatureabove the stone may clear this obstruction andrelieve the pain. This process is usuallv inter-mittent, which would account for the exacerbationof symptoms. Descent of the stone into a morecapacious part of the ureter, or into the bladder,Nvould produce alJeviation. This phenomenon ofcanalization of ureteric calculi occurs morecommonly than is generally appreciated, and nodoubt acccunts for the surprisinglv long survival ofkidnev function in some cases after the impaction
s Ag
-3-
-
--
--i,-
-----
-s
-B
5 rs-
- 3FIC. Io.-Specimen A-a urate stone (Case 2).
Specimen B-an oxalate (Case 3). SpecimenC-a phlebolith (Case i).
of a stone in its ureter. This, however, does notjustify a complacent attitude and delay in treat-ment of the obstruction.The phlebolith has a regular surface and is
oval in shape (Fig. ioc). Phleboliths are usuallymultiple and lie in a line on either side of thepelvis, and if single mav often be difficult todistinguish from a ureteric calcuilus, thoughcbaracteristically they give a laminated shadow onradiography. In Case i it was perhaps excusablethat a wrong diagnosis was mide, but operativeremoval of phleboliths is to be deprecated as theyoccur commonly in adult life and are symptomless.Also, this needless operation may be a hazardousprocedure.A calcified tuberculous gland, if situated in the
line of the ureter, mav be difficult to distinguishfrom a stone, but usually in the former the cal-cification is irregularly distributed and the glandmargins are not circumscribed; further they areoften multiple, and if situated in the mesenterv canbe moved with change of posture.
copyright. on O
ctober 18, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.305.128 on 1 M
arch 1951. Dow
nloaded from

134 POSTGRADUATE MEDICAL JOURNAL March I951
Occasionally calcification of the iliac arteriesmay simulate a stone, as in Fig. IO, but the lineardistribution of the calcification will signify that it isin the vessel walls. If, however, it only affects ashort portion it may be confused with a uretericstone. An intravenous pyelogram in this caseshows that it is remote fiom the line of the ureter.The radiograph depicting a small stone im-
pacting the urethra is of interest, as it is not oftenthat one has the opportunity to demonstrate radio-logically a calculus in that position. This stoneoriginated in the kidney and descended down the
urinary tract to become heli up by the urethralstricture (Fig. 6).The above remarks deal with a few aspects of
ureteric calculi, namely, their diagnosis and ap-pearances. In conclusion, a stone in the uretershould not be considered as a separate entity, butas a manifestaiton of calculous disease affecting thewhole urinary tract. In some patients the passageof a ureteric stone is but an incident; in others itmay preface a chapter of further urinarv disorderswhich, it is to be hoped, will have a happyending.
VALE ATQUE AVEA By-way of Domestic Education in the 18th Century
By DR. A. MEIKLEJOHN
In the Potteries district of North StaffordshireBurslem has always been regarded as the motherof the five towns, and the first free school therewas erected in I749. Early in October 1950,almost exactly 200 years later, a university collegewas instituted at Keele, just a few miles distantfrom the original school.The subscribers to the original free school
probably had no vision of a university or even auniversity college for the sons and daughters ofpoor workmen, but Josiah Wedgwood has leftus some record of his views on the education ofchildren of the middle classes. His concern was,as it must always be for most of us, the educationof his family.
Josiah Wedgwood was born at Burslem in I730,where as a very young child he attended the dameschool to which the local children were sent' moreto be out of the way of mischief than for thelearning to be obtained there.' When seven yearsold and he could walk the distance of seven milesdaily, he accompanied a group of children to Mr.Blunt's private school at Newcastle-under-Lyme.Here the master instructed his pupils in reading,writing and arithmetic, while his wife taught thegirls knitting and sewing. On the death of hisfather in 1739 young Joss was taken from schooland apprenticed to his brother Thomas in thefamily potworks. So his formal education endedat the age of nine years. Forty-four years later,in 1783, in recognition of his profound contribu-tions to ceramic science, he was elected, at thesame time as his friend Joseph Priestley, a Fellowof the Royal Society. His monument in the
Parish Church, Stoke-on-Trent, bears the inscrip-tion:
Sacred to the Memory ofJosiah Wedgwood, F.R.S. and S.A.
of Etriuria in this county.Born, August I730. Died January 3rd, I795.Who converted a rude and inconsiderableManufacturing into an elegant Art and An
important part of National Commerce.In 1764 he married his cousin Sarah Wedgwood
and between I765 and I778 a family of four sonsand four daughters was born to them. It is in re-lation to the four eldest surviving children (Richarddied in infancy), Susan or Sukey (the mother ofCharles Darwin), Jack, Joss and Tom that Wedg-wood has recorded for us a father's thoughts on theeducation of his family.As was the custom of the times, all about the
age of six or seven years were sent off to boardingschool; Sukey went to Manchester while herbrothers attended a school at Bolton conductedby the Revd Mr. Holland. This school seems tohave been much in demand and vacancies notalways available, for on November 8, 1776, Wedg-wood writes:
' You were so obliging to tell us some timesince that you could take our Son Joss underyour care the next summer, which offer we shallthankfully acept, and shall be glad if you can atthe same time make room for our youngest (Tomborn 177I), who wishes to accompany hisBrothers, and will be a pretty little sort of aScholar by midsummer.'
copyright. on O
ctober 18, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.305.128 on 1 M
arch 1951. Dow
nloaded from