Embed Size (px)
Citation preview

Articles
www.thelancet.com Published online May 17, 2012 DOI:10.1016/S0140-6736(12)60312-2 1
Plasma HDL cholesterol and risk of myocardial infarction: a mendelian randomisation studyBenjamin F Voight*, Gina M Peloso*, Marju Orho-Melander, Ruth Frikke-Schmidt, Maja Barbalic, Majken K Jensen, George Hindy, Hilma Hólm, Eric L Ding, Toby Johnson, Heribert Schunkert, Nilesh J Samani, Robert Clarke, Jemma C Hopewell, John F Thompson, Mingyao Li, Gudmar Thorleifsson, Christopher Newton-Cheh, Kiran Musunuru, James P Pirruccello, Danish Saleheen, Li Chen, Alexandre F R Stewart, Arne Schillert, Unnur Thorsteinsdottir, Gudmundur Thorgeirsson, Sonia Anand, James C Engert, Thomas Morgan, John Spertus, Monika Stoll, Klaus Berger, Nicola Martinelli, Domenico Girelli, Pascal P McKeown, Christopher C Patterson, Stephen E Epstein, Joseph Devaney, Mary-Susan Burnett, Vincent Mooser, Samuli Ripatti, Ida Surakka, Markku S Nieminen, Juha Sinisalo, Marja-Liisa Lokki, Markus Perola, Aki Havulinna, Ulf de Faire, Bruna Gigante, Erik Ingelsson, Tanja Zeller, Philipp Wild, Paul I W de Bakker, Olaf H Klungel, Anke-Hilse Maitland-van der Zee, Bas J M Peters, Anthonius de Boer, Diederick E Grobbee, Pieter W Kamphuisen, Vera H M Deneer, Clara C Elbers, N Charlotte Onland-Moret, Marten H Hofk er, Cisca Wijmenga, W M Monique Verschuren, Jolanda M A Boer, Yvonne T van der Schouw, Asif Rasheed, Philippe Frossard, Serkalem Demissie, Cristen Willer, Ron Do, Jose M Ordovas, Gonçalo R Abecasis, Michael Boehnke, Karen L Mohlke, Mark J Daly, Candace Guiducci, Noël P Burtt, Aarti Surti, Elena Gonzalez, Shaun Purcell, Stacey Gabriel, Jaume Marrugat, John Peden, Jeanette Erdmann, Patrick Diemert, Christina Willenborg, Inke R König, Marcus Fischer, Christian Hengstenberg, Andreas Ziegler, Ian Buysschaert, Diether Lambrechts, Frans Van de Werf, Keith A Fox, Nour Eddine El Mokhtari, Diana Rubin, Jürgen Schrezenmeir, Stefan Schreiber, Arne Schäfer, John Danesh, Stefan Blankenberg, Robert Roberts, Ruth McPherson, Hugh Watkins, Alistair S Hall, Kim Overvad, Eric Rimm, Eric Boerwinkle, Anne Tybjaerg-Hansen, L Adrienne Cupples, Muredach P Reilly, Olle Melander, Pier M Mannucci, Diego Ardissino, David Siscovick, Roberto Elosua, Kari Stefansson, Christopher J O’Donnell, Veikko Salomaa, Daniel J Rader, Leena Peltonen, Stephen M Schwartz, David Altshuler, Sekar Kathiresan
SummaryBackground High plasma HDL cholesterol is associated with reduced risk of myocardial infarction, but whether this association is causal is unclear. Exploiting the fact that genotypes are randomly assigned at meiosis, are independent of non-genetic confounding, and are unmodifi ed by disease processes, mendelian random isation can be used to test the hypothesis that the association of a plasma biomarker with disease is causal.
Methods We performed two mendelian randomisation analyses. First, we used as an instrument a single nucleotide polymorphism (SNP) in the endothelial lipase gene (LIPG Asn396Ser) and tested this SNP in 20 studies (20 913 myocardial infarction cases, 95 407 controls). Second, we used as an instrument a genetic score consisting of 14 common SNPs that exclusively associate with HDL cholesterol and tested this score in up to 12 482 cases of myocardial infarction and 41 331 controls. As a positive control, we also tested a genetic score of 13 common SNPs exclusively associated with LDL cholesterol.
Findings Carriers of the LIPG 396Ser allele (2·6% frequency) had higher HDL cholesterol (0·14 mmol/L higher, p=8×10–¹³) but similar levels of other lipid and non-lipid risk factors for myocardial infarction compared with non-carriers. This diff erence in HDL cholesterol is expected to decrease risk of myocardial infarction by 13% (odds ratio [OR] 0·87, 95% CI 0·84–0·91). However, we noted that the 396Ser allele was not associated with risk of myocardial infarction (OR 0·99, 95% CI 0·88–1·11, p=0·85). From observational epidemiology, an increase of 1 SD in HDL cholesterol was associated with reduced risk of myocardial infarction (OR 0·62, 95% CI 0·58–0·66). However, a 1 SD increase in HDL cholesterol due to genetic score was not associated with risk of myocardial infarction (OR 0·93, 95% CI 0·68–1·26, p=0·63). For LDL cholesterol, the estimate from observational epidemiology (a 1 SD increase in LDL cholesterol associated with OR 1·54, 95% CI 1·45–1·63) was concordant with that from genetic score (OR 2·13, 95% CI 1·69–2·69, p=2×10–¹⁰).
Interpretation Some genetic mechanisms that raise plasma HDL cholesterol do not seem to lower risk of myocardial infarction. These data challenge the concept that raising of plasma HDL cholesterol will uniformly translate into reductions in risk of myocardial infarction.
Funding US National Institutes of Health, The Wellcome Trust, European Union, British Heart Foundation, and the German Federal Ministry of Education and Research.
IntroductionCholesterol fractions such as LDL and HDL cholesterol are among the most commonly measured biomarkers in clinical medicine.1 Observational studies have shown that LDL and HDL cholesterol have opposing associations
with risk of myocardial infarction, with LDL cholesterol being positively associated and HDL cholesterol being inversely associated.2,3 However, observational studies cannot distinguish between a causal role in the pathological process and a marker of the underlying
Published OnlineMay 17, 2012DOI:10.1016/S0140-6736(12)60312-2
This online publication has been corrected. The corrected version fi rst appeared at thelancet.com on June 1, 2012
See Online/CommentDOI:10.1016/S0140-6736(12)60481-4
*These authors contributed equally to this work
Affi liations listed at end of paper
Correspondence to:Dr Sekar Kathiresan, Center for Human Genetic Research and Cardiovascular Research Center, Massachusetts General Hospital, Harvard Medical School, Boston, MA 02114, [email protected]

Articles
2 www.thelancet.com Published online May 17, 2012 DOI:10.1016/S0140-6736(12)60312-2
patho physiology. These two possibilities can be distin-guished in human beings by changes of the cholesterol fractions in large-scale randomised trials or by studies of inherited DNA variation. For LDL cholesterol, the results of both randomised trials of LDL-cholesterol-lowering treatments4 and from human mendelian diseases5,6 are concordant and suggest that plasma LDL cholesterol is causally related to risk of myocardial infarction. However, the available evidence for the causal relevance of HDL cholesterol from randomised trials or mendelian diseases is scarce and inconsistent.7,8
If a particular plasma biomarker is directly involved in an underlying pathological process, then inherited variation changing plasma concentrations of this bio-marker should aff ect risk of disease in the direction and magnitude predicted by the plasma concentrations. Referred to as mendelian randomisation,9–11 this ana-lytical approach has been previously applied to plasma HDL cholesterol, albeit with restricted sample sizes, a small number of single nucleotide polymorphisms (SNPs) at a few genes, and with SNPs that aff ect multiple lipid fractions.8,12–15 Hence, these studies have not been able to resolve fully the possible causal relevance of HDL cholesterol concentrations for risk of myocardial infarction.
Recently, we have used the genome-wide association approach to identify SNPs that aff ect blood lipid con-centrations.16,17 Additionally, through resequencing, we identifi ed a loss-of-function coding SNP at the endothelial lipase gene (LIPG Asn396Ser) that aff ects plasma HDL cholesterol in isolation.18,19 Here, we use these SNPs in case-control studies and prospective cohort studies to test the hypothesis that genetically raised plasma HDL cholesterol might be protective for myocardial infarction.
MethodsStudy designThe study design consisted of two components. First, using a case-control design, we tested lipid-associated SNPs individually for association with risk of myocardial infarction. Second, using a mendelian randomisation design, we tested two instruments: (1) a single SNP that related exclusively to plasma HDL cholesterol (a loss-of-function coding polymorphism at the endothelial lipase gene, LIPG Asn396Ser, rs61755018); and (2) a genetic score consisting of 14 common SNPs that exclusively associate with HDL cholesterol.
Study participantsCharacteristics of cases of myocardial infarction and controls are shown in appendix p 19. Data for up to 19 139 cases of myocardial infarction and 50 812 myo-cardial-infarction-free controls were available from 30 studies. Characteristics of the participants in six prospective cohort studies are shown in the appendix p 20. 50 763 participants from six cohort studies were studied and, of these, 4228 developed an incident fatal or
non-fatal myocardial infarction. All participants were of self-reported European or South Asian ancestry.
Statistical analysisIn myocardial infarction cases and controls, we tested each of 25 SNPs for association with myocardial infarction in up to 30 studies. These 25 SNPs repre-sented the initial polymorphisms mapped for plasma HDL or LDL cholesterol concentrations with a genome-wide association approach.16 Each selected SNP has been associated with either HDL or LDL cholesterol at p<5×10–⁸. Genotyping details are provided in the appendix p 2. We undertook logistic regression with the outcome variable of myocardial infarction status, predictor variable of individual SNP genotype, and covariates of age, sex, and principal components of ancestry. We assumed a log-additive genetic model. Overall association for each SNP was evaluated with a fi xed-eff ects inverse-variance-weighted meta-analysis.
Fatal or non-fatal myocardial infarction outcomes were ascertained in each of six prospective cohort studies as described in the appendix p 10. We constructed logistic regression models to examine the association of LIPG Asn396Ser genotype with myocardial infarction status, excluding participants who had had a previous myocardial infarc tion or ischaemic stroke. The predictor variable of LIPG Asn396Ser genotype was modelled in an additive model (ie, 0, 1, 2 copies of the 396Ser allele). Covariates in the model included age and sex. Overall association for each SNP was evaluated across the six studies with fi xed-eff ects inverse-variance-weighted meta-analysis.
We estimated a predicted risk for LIPG Asn396Ser on the basis of the association of this SNP with plasma HDL cholesterol (appendix p 21) and the association of plasma HDL cholesterol with myocardial infarction (appendix p 22) in the population. Details are provided in the appendix p 2.
We undertook instrumental variable analysis using LIPG Asn396Ser in six prospective cohort studies as listed in the appendix p 23. We additionally did an instrumental variable analysis using multiple genetic variants as instruments.20 Details of the instrumental variable analysis methods are provided in the appendix p 4. We regarded a two-tailed p<0·05 as nominally signifi cant. Heterogeneity statistics were calculated as described.21 SAS version 9.1, the R package, STATA, or PLINK software were used for all statistical analyses.22
Role of the funding sourceThe sponsors had no role in the conduct or interpretation of the study. The corresponding author had full access to all data in the study and had fi nal responsibility for the decision to submit for publication.
ResultsTo validate the statistical framework and clinical samples, we fi rst tested SNPs related to plasma LDL cholesterol in
See Online for appendix

Articles
www.thelancet.com Published online May 17, 2012 DOI:10.1016/S0140-6736(12)60312-2 3
case-control studies (table 1). For nine of ten SNPs associated with LDL cholesterol, the allele correlated with increased LDL cholesterol was also associated with increased risk of myocardial infarction (p<0·05; table 1).
Having established that SNPs related to plasma LDL cholesterol consistently aff ected risk of myocardial
infarction, we applied the same methodological frame-work in the same samples to test the hypothesis that genetic modulation of HDL cholesterol would aff ect risk of myocardial infarction. Of 15 loci related to plasma HDL cholesterol, at six loci (LPL, TRIB1, APOA1-APOC3-APOA4-APOA5 cluster, CETP, ANGPTL4, and GALNT2)
Chromosome Gene(s) of interest within or near associated interval
Major allele, minor allele (minor allele frequency)*
Modelled allele
Eff ect of modelled allele on plasma LDL cholesterol (mmol/L)*
Eff ect of modelled allele on plasma HDL cholesterol (mmol/L)*
Eff ect of modelled allele on plasma triglycerides (mmol/L)*
Sample size (MI cases/MI-free controls)
For modelled allele, observed change in MI risk (%; 95% CI)
For modelled allele, p value for association with MI
rs646776 1p13 CELSR2, PSRC1, SORT1† T, C (0·21) T 0·20 –0·03 ·· 19 139/50 812 16% (12–19) 4×10�¹⁶†
rs6511720 19p13 LDLR† G, T (0·10) G 0·23 ·· 0·09 16 503/46 576 23% (17–30) 4×10�¹²†
rs11206510 1p32 PCSK9† T, C (0·17) T 0·05 ·· ·· 18 455/23 075 13% (9–16) 1×10�⁹†
rs3798220 6q25 LPA† T, C (0·02) C 0·36‡ ·· ·· 6658/5823 72% (39–211) 4×10�⁷†
rs562338 2p24 APOB† G, A (0·20) G 0·14 ·· ·· 19 139/50 812 8% (4–12) 5×10�⁵†
rs6544713 2p21 ABCG8† C, T (0·32) T 0·13 ·· ·· 14 818/45 454 8% (4–11) 5×10�⁵†
rs7953249 12q24 HNF1A† A, G (0·44) G 0·07 ·· ·· 19 139/50 812 5% (3–9) 2×10�⁴†
rs10402271 19q13 APOE-APOC1-APOC4-APOC2† T, G (0·33) G 0·12 ·· ·· 19 139/50 812 4% (1–7) 0·007†
rs3846663 5q13 HMGCR† C, T (0·38) T 0·06 ·· ·· 19 139/50 812 4% (1–7) 0·01†
rs1501908 5q23 TIMD4-HAVCR1 C, G (0·37) C 0·06 ·· ·· 18 310/49 897 3% (0–6) 0·08
*Data presented from a meta-analysis of seven cohorts (n up to 19 840) as presented in reference 16; the eff ect of each SNP on a lipid trait was modelled if the association of the SNP with a plasma lipid trait exceeded nominal signifi cance (p<0·05). †Loci and SNPs that exceeded nominal signifi cance (p<0·05) for association of modelled allele with MI; all modelled alleles increased LDL cholesterol. ‡The C allele at this LPA variant is related to increased plasma lipoprotein(a) as presented in reference 16.
Table 1: Association of myocardial infarction (MI) with single nucleotide polymorphisms (SNPs) previously found to relate to plasma LDL cholesterol
Chromosome Gene(s) of interest within or near associated interval
Major allele, minor allele (minor allele frequency)*
Modelled allele
Eff ect of modelled allele on plasma HDL cholesterol (mmol/L)*
Eff ect of modelled allele on plasma triglycerides (mmol/L)*
Eff ect of modelled allele on plasma LDL cholesterol (mmol/L)*
Sample size (MI cases/MI-free controls)
For modelled allele, observed change in MI risk (%; 95% CI)
For modelled allele, p value for association with MI
rs17482753 8p21 LPL† G, T (0·10) T 0·08 –0·24 ·· 19 139/50 812 –12% (–16 to –7) 4×10�⁷†
rs17321515 8q24 TRIB1† A, G (0·45) G 0·02 –0·11 –0·05 19 139/50 812 –7% (–9 to –4) 2×10�⁶†
rs6589566 11q23 APOA1-APOC3-APOA4-APOA5† A, G (0·07) A 0·05 –0·27 –0·09 18 310/49 897 –10% (–15 to –5) 8×10�⁵†
rs4846914 1q42 GALNT2† A, G (0·40) A 0·02 –0·03 ·· 19 139/50 812 –3% (–6 to –1) 0·02†
rs2967605 19p13 ANGPTL4† C, T (0·16) C 0·05 –0·07 ·· 13 595/16 423 –5% (–10 to –1) 0·03†
rs3764261 16q13 CETP† C, A (0·32) A 0·10 ·· –0·03 16 503/46 576 –4% (–7 to 0) 0·04†
rs61755018 (Asn396Ser)
18q21 LIPG A, G (0·015) G 0·14‡ ·· ·· 17 165/49 077 –6% (–18 to 9) 0·41
rs17145738 7q11 MLXIPL C, T (0·11) T 0·03 –0·15 ·· 19 139/50 812 –1% (–4 to 3) 0·61
rs3890182 9q31 ABCA1 G, A (0·14) G 0·03 ·· 0·05 19 139/50 812 –1% (–5 to 4) 0·76
rs2338104 12q24 MMAB, MVK G, C (0·46) G 0·03 ·· ·· 19 139/50 812 0% (–3 to 3) 0·85
rs471364 9p22 TTC39B T, C (0·12) T 0·03 ·· ·· 15 693/47 098 0% (–5 to 5) 0·97
rs2271293 16q22 LCAT G, A (0·11) A 0·03 ·· ·· 19 139/50 812 4% (–1 to 8) 0·10
rs174547 11q12 FADS1-FADS2-FADS3 T, C (0·33) T 0·03 –0·06 ·· 19 139/50 812 3% (–1 to 6) 0·11
rs1800588 15q22 LIPC C, T (0·22) T 0·05 0·07 ·· 17 917/49 514 4% (0 to 7) 0·04
rs16988929 20q13 HNF4A C, T (0·01) T 0·01 ·· ·· 17 041/20 137 31% (12 to 54) 9×10�⁴
*Data presented from a meta-analysis of seven cohorts (n up to 19 840) as presented in reference 16; the eff ect of each SNP on a lipid trait was modelled if the association of the SNP with a plasma lipid trait exceeded nominal signifi cance (p<0·05). †Loci and SNPs that exceeded nominal signifi cance (p<0·05) for association of modelled allele with MI; all modelled alleles increased HDL cholesterol. ‡Eff ect size presented is from the Atherosclerosis Risk in Communities Study.
Table 2: Association of myocardial infarction (MI) with single nucleotide polymorphisms (SNPs) previously found to relate to plasma HDL cholesterol

Articles
4 www.thelancet.com Published online May 17, 2012 DOI:10.1016/S0140-6736(12)60312-2
the allele correlated with raised HDL cholesterol was also associated with decreased risk of myocardial infarction (p<0·05; table 2). Of note, at the HNF4A locus, the HDL-cholesterol-raising allele was surprisingly associated with increased risk of myocardial infarction (p=0·0009).
All six SNPs associated with both HDL cholesterol and myocardial infarction had additional eff ects on plasma LDL cholesterol or triglycerides, or both (p<5×10–⁸ for the additional eff ects on LDL cholesterol or triglycer ides). For example, at APOA1-APOC3-APOA4-APOA5 rs6589566, the allele associated with increased HDL
cholesterol also relates to reduced LDL cholesterol and reduced triglycerides. The pleiotropic eff ects of such SNPs undermine the ability to defi ne a causal role for HDL cholesterol, independent of eff ects on LDL cholesterol or triglycerides.
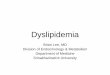
To evaluate plasma HDL cholesterol specifi cally, we undertook mendelian randomisation, a form of instrumental variable analysis.23 We identifi ed a variant that aff ected only plasma HDL cholesterol without changing other lipid or non-lipid cardiovascular risk factors. In the LIPG gene, roughly 2·6% of individuals carry a serine substitution at aminoacid 396 (substituted for wild-type asparagine). Carrier status for 396Ser was associated with signifi cant increases in HDL cholesterol in each of four prospective cohort studies, with the eff ect size ranging from 0·08 mmol/L to 0·28 mmol/L per copy of the Ser allele (fi gure 1, appendix p 21; p=0·002 in FHS, p=0·02 in CCHS, p=5×10–⁶ in MDC, and p=7×10–⁷ in ARIC).
In a meta-analysis including all four studies, carrier status for 396Ser was associated with an increase of roughly 0·29 SD units in HDL cholesterol (p=8×10–¹³). There was no evidence of heterogeneity across the four studies (I²=0·58; Cochran’s heterogeneity p=0·07). LIPG Asn396Ser was not signifi cantly associated with other risk factors for myocardial infarction including plasma LDL cholesterol, triglycerides, systolic blood pressure, body-mass index, risk of type 2 diabetes, fasting glucose, plasma C-reactive protein, waist-to-hip ratio, fi brinogen, and small LDL particle concentration (p>0·05 for each; appendix pp 24–26). Therefore, LIPG Asn396Ser satisfi ed the three main criteria for mendelian randomisation analysis—ie, that the genotype should be associated with an intermediate biomarker (fi gure 1), should not be associated with confounding factors (appendix pp 24–46), and should exert its eff ect on the clinical outcome only through the specifi c intermediate biomarker (appendix p 22).24
Under the model that plasma HDL cholesterol causally relates to risk of myocardial infarction, individuals with an inherited increase in HDL cholesterol (eg, those carrying the LIPG 396Ser allele) are expected to have reduced risk of myocardial infarction. On the basis of the associations between SNPs and HDL cholesterol, and HDL cholesterol and myocardial infarction, we estimated that carriage of LIPG 396Ser should decrease risk of myocardial infarction by 13% (odds ratio [OR] 0·87, 95% CI 0·84–0·91).
To establish whether LIPG 396Ser carriers are indeed protected from risk of myocardial infarction, we studied the association of LIPG Asn396Ser with incident myocardial infarction in 50 763 participants from six prospective cohort studies, the gold standard with respect to epidemiological study design. Of these participants, 4228 developed a fi rst myocardial infarction event. LIPG Asn396Ser was not associated with myocardial infarction in any of the six studies (fi gure 2). Combining these
Asn/AsnSer carriers
1·25FHS CCHS MDC ARIC
Cohort
HDL
chol
este
rol (
mm
ol/L
)
1·35
1·45
1·55
1·65
Figure 1: Plasma HDL cholesterol concentrations in carriers versus non-carriers of the Ser allele at the LIPG Asn396Ser polymorphismError bars show standard error. FHS=Framingham Heart Study. CCHS=Copenhagen City Heart Study. MDC=Malmo Diet and Cancer Study. ARIC=Atherosclerosis Risk in Communities Study.
AngioGOCARD/KORAIFS
deCODEEPIC-NL
GerMIFS-IIGRACEMAHA
PennCATH UCP
POPGENPROCARDIS
PROMISSHEEP
WTCCCAll case-control studies
ARICCCHSDCHFHS
HPFSMDC
All cohort studiesOverall
0·76 (0·46–1·24)1·25 (0·51–3·08)0·97 (0·60–1·58)0·64 (0·27–1·53)1·36 (0·82–2·24)2·48 (1·10–5·56)1·08 (0·68–1·72)0·82 (0·37–1·83)0·87 (0·44–1·72)0·69 (0·42–1·14)0·66 (0·45–0·98)1·27 (0·74–2·16)1·35 (0·85–2·14)0·74 (0·49–1·12)0·94 (0·82–1·09)0·80 (0·45–1·40)1·33 (0·73–2·43)1·12 (0·66–1·90)2·35 (0·69–8·00)1·97 (0·86–4·51)1·01 (0·74–1·38)1·10 (0·89–1·37)0·99 (0·88–1·11)
1953577729334
1127683785485830
24332183185411511561
16 685558655933
50426
16064228
20 913
1482719
29 21818271874
656615489
113916873347189714962426
48 8728214896415881462
86925 43846 53595 407
Cases
OR (95% CI)
Controls
Number of individuals
0 0·5 1·5 2·51 2
Figure 2: Association of LIPG Asn396Ser with myocardial infarction in 116 320 participants from 20 studiesIn each study, the HDL-cholesterol-raising serine allele was modelled.

Articles
www.thelancet.com Published online May 17, 2012 DOI:10.1016/S0140-6736(12)60312-2 5
studies in a meta-analysis, LIPG Asn396Ser allele was not associated with myocardial infarction (OR 1·10, 95% CI 0·89–1·37, p=0·37; fi gure 2). There was no evidence for heterogeneity across the six cohorts (I²=0·17; Cochran’s heterogeneity p=0·31).
We also studied LIPG Asn396Ser in case-control studies involving an additional 16 685 cases of myocardial infarction and 48 872 controls and noted that this SNP was not associated with myocardial infarction (OR 0·94, 95% CI 0·82–1·09, p=0·41; table 2, fi gure 2), with no evidence of heterogeneity across the 14 case-control studies (I²=0·34; Cochran’s heterogeneity p=0·11). Finally, we used meta-analysis to combine the evidence from both the prospective studies and case-control studies (116 320 participants; 20 913 cases and 95 407 con-trols). In all available samples, LIPG Asn396Ser remained not associated with risk of myocardial infarction (OR 0·99, 95% CI 0·88–1·11, p=0·85; fi gure 2). There was no evidence for heterogeneity across all 20 studies (I²=0·30; Cochran’s heterogeneity p=0·10).
We formally estimated the magnitude of an association of genetically raised HDL cholesterol with myocardial infarction, using LIPG Asn396Ser as the instrument. The mendelian randomisation estimate was computed from the ratio of the coeffi cient of the association between genotype and disease to that of the association between genotype and plasma HDL cholesterol; this instrumental variable estimate refl ects the potential causal eff ect of plasma HDL cholesterol on the risk of myocardial infarction.
Table 3 presents the instrumental variable estimate for the association of plasma HDL cholesterol with risk of myocardial infarction in each of six prospective cohort studies. In each study, genetically raised plasma HDL cholesterol was not associated with risk of myocardial infarction. In meta-analysis, genetically raised plasma HDL cholesterol was also not associated with risk of myocardial infarction (OR 1·02 per 0·03 mmol/L [1 mg/dL] increase in HDL cholesterol, 95% CI
0·95–1·09, p=0·64; OR 1·28 per 0·39 mmol/L [15 mg/dL] increase in HDL cholesterol, 95% CI 0·46–3·61, p=0·64).
Statistical power for instrumental variable analysis could be increased if multiple genetic variants in combination are used as instruments, according to a recent proposal.20 From our genome-wide association study of plasma lipid traits involving more than 100 000 individuals,17 we noted that 13 common SNPs had statistical evidence at genome-wide levels of signifi cance (p<5×10–⁸) for plasma LDL cholesterol and no evidence for association with triglycerides (p>0·01) or HDL cholesterol (p>0·01). We constructed a genetic score for LDL cholesterol combining the LDL-cholesterol-raising alleles at each of these 13 SNPs (appendix p 27).25 We also noted that 14 common SNPs had statistical evidence at genome-wide levels of signifi cance (p<5×10–⁸) for plasma HDL cholesterol and no evidence for association with triglycerides (p>0·01) or LDL cholesterol (p>0·01). We constructed a genetic score for HDL cholesterol combining the HDL-cholesterol-raising alleles at each of these 14 SNPs (appendix p 28). Each SNP was given a weight based on the degree of change in LDL or HDL cholesterol as estimated in roughly 100 000 individuals.17
We tested the association of genetic scores for LDL and HDL cholesterol separately for association with myocardial infarction in up to 53 146 cases and controls from the CARDIoGRAM study.26 From observational epidemiology, an increase of 1 SD in usual LDL cholesterol was associated with raised risk of myocardial infarction (OR 1·54, 95% CI 1·45–1·63; appendix p 22). In a mendelian randomisation analysis, a 1 SD increase in LDL cholesterol due to genetic score was also associated with risk of myocardial infarction (OR 2·13, 95% CI 1·69–2·69, p=2×10–¹⁰; table 4). From observational epidemiology, a 1 SD rise in usual HDL cholesterol was associated with lowered risk of myocardial infarction (OR 0·62, 95% CI 0·58–0·66; appendix p 22). However, in mendelian randomisation analysis, a 1 SD increase in
Observational epidemiology Genetically raised
Odds ratio (95% CI) per 0·03 mmol/L (1 mg/dL) increase in plasma HDL cholesterol
p value Odds ratio (95% CI) per 0·03 mmol/L (1 mg/dL) increase in plasma HDL cholesterol
p value
Cohort
Atherosclerosis Risk in Communities Study 0·97 (0·96–0·98) 7×10�¹⁸ 0·96 (0·86–1·07) 0·44
Copenhagen City Heart Study 0·98 (0·98–0·99) 6×10�¹³ 1·09 (0·95–1·26) 0·21
Malmo Diet and Cancer Study, Cardiovascular Cohort 0·97 (0·96–0·98) 1×10�⁶ 0·82 (0·66–1·01) 0·06
Framingham Heart Study 0·96 (0·94–0·98) 4×10�⁶ 1·17 (1·00–1·37) 0·06
Health Professionals Follow-up Study ·· ·· 1·84 (0·39–8·62) 0·16
Danish Diet, Cancer, and Health Study ·· ·· 1·05 (0·79–1·41) 0·71
Meta-analysis of cohort studies
Per 0·03 mmol/L (1 mg/dL) increase in plasma HDL cholesterol 0·98 (0·97–0·98) 4×10�³⁶ 1·02 (0·95–1·09) 0·64
Per 0·39 mmol/L (15 mg/dL) increase in plasma HDL cholesterol 0·70 (0·66–0·74) 4×10�³⁶ 1·28 (0·46–3·61) 0·64
Table 3: Instrumental variable analysis estimate of the association of genetically raised HDL cholesterol and risk of myocardial infarction using LIPG Asn396Ser as an instrument

Articles
6 www.thelancet.com Published online May 17, 2012 DOI:10.1016/S0140-6736(12)60312-2
HDL cholesterol due to genetic score was not associated with risk of myocardial infarction (OR 0·93, 95% CI 0·68–1·26, p=0·63; table 4).
DiscussionFor a biomarker directly involved in disease patho genesis, we expect a genetic variant that modulates the biomarker to likewise confer risk of disease. We tested this hypothesis for two plasma biomarkers: LDL and HDL cholesterol. SNPs aff ecting LDL cholesterol were consistently related to risk of myocardial infarction. However, we unexpectedly found that LIPG Asn396Ser, a genetic variant that specifi cally and substantially increases plasma HDL cholesterol, did not reduce risk of myocardial infarction. A genetic score combining 14 variants exclusively related to HDL cholesterol also showed no association with risk of myocardial infarction (panel).
These results challenge several established views about plasma HDL cholesterol. First, these data question the concept that raising of plasma HDL cholesterol should uniformly translate into reductions in risk of myocardial infarction. We raise the strong possibility that a specifi c means of raising of HDL cholesterol in human beings—namely, inhibition of endothelial lipase—will not reduce risk of myocardial infarction. In animal models, inhib ition or deletion of the endothelial lipase gene increases HDL cholesterol concentrations,27 but there has been debate as to the consequent eff ect on atherosclerosis. One report suggested that mice deleted for Lipg on an Apoe knockout genetic background have decreased aortic atherosclerosis,28 but a subsequent study showed no eff ect of Lipg deletion on aortic atherosclerosis.29
Second, these fi ndings emphasise the potential limi-tation of plasma HDL cholesterol as a surrogate measure for risk of myocardial infarction in intervention trials. The data presented here using mendelian randomisation are consistent with results from completed randomised controlled trials focused on raising plasma HDL cholesterol. Hormone replacement therapy raised plasma HDL cholesterol but did not lower risk of myocardial infarction.30 In the Atherothrombosis
Inter vention in Metabolic Syndrome with Low HDL Cholesterol/High Triglyceride and Impact on Global Health Outcomes (AIM-HIGH) trial,31 the addition of long-acting niacin to background simvastatin increased HDL cholesterol and lowered triglycerides but did not lower risk of cardio vascular events.
Of note, at the cholesterol ester transfer protein (CETP) gene, we did fi nd that common genetic variation reduces risk of myocardial infarction by 4%, a result in line with an earlier meta-analysis.32 However, the CETP variant both increases HDL cholesterol and lowers LDL cholesterol17 in a manner similar to pharmacological inhibitors of CETP.33 As such, whether the protection aff orded by the CETP variant is due to the change in HDL or LDL cholesterol is diffi cult to distinguish.
Third, biomarkers that assay HDL function might overcome some limitations of standard HDL cholesterol assays. However, a challenge will remain—namely, to prove that new functional HDL biomarkers refl ect a causal association with myocardial infarction rather than an indirect one, as seems to be the case with plasma HDL cholesterol. For example, using a new in-vitro measure involving mouse macrophages and human serum, Khera and colleagues34 showed an inverse correlation between a specifi c functional property of HDL, cholesterol effl ux capacity, and coronary artery disease status. The present study suggests that a fruitful approach to the causal evaluation of such functional measures in human beings might be large-scale study of relevant inherited DNA variation of HDL function.
There are inherent limitations to the mendelian ran-domisation study design. Naturally occurring genetic
Odds ratio (95% CI) per SD increase in plasma lipid based on observational epidemiology*
Odds ratio (95% CI) per SD increase in plasma lipid conferred by genetic score†
LDL cholesterol 1·54 (1·45–1·63) 2·13 (1·69–2·69), p=2×10�¹⁰
HDL cholesterol 0·62 (0·58–0·66) 0·93 (0·68–1·26), p=0·63
*Observational epidemiology estimates derived from more than 25 000 individuals from prospective cohort studies as shown in the appendix p 22. †LDL genetic score consisting of 13 single nucleotide polymorphisms (SNPs) as shown in the appendix p 27; HDL genetic score consisting of 14 SNPs as shown in the appendix p 28.
Table 4: Estimate of the association of genetically raised LDL cholesterol or HDL cholesterol and risk of myocardial infarction using multiple genetic variants as instruments
Panel: Research in context
Systematic reviewElectronic searches of Medline and PubMed, supplemented by hand searches of reference lists of other review articles, identifi ed reports from three large mendelian randomisation studies for plasma HDL cholesterol.7,12,15 In each of these previous reports, genetically increased plasma HDL cholesterol was not associated with risk of ischaemic heart disease.
InterpretationThe present study tested a naturally occurring loss-of-function variant in the endothelial lipase gene and, with this new instrument, we confi rm that genetically raised plasma HDL cholesterol is not associated with risk of myocardial infarction. The study further extends previous work by testing an instrument consisting of 14 common variants exclusively associated with plasma HDL cholesterol. A genetic score consisting of these 14 variants was not associated with risk of myocardial infarction. These results show that some ways of raising HDL cholesterol might not reduce risk of myocardial infarction in human beings. Therefore, if an intervention such as a drug raises HDL cholesterol, we cannot automatically assume that risk of myocardial infarction will be reduced.

Articles
www.thelancet.com Published online May 17, 2012 DOI:10.1016/S0140-6736(12)60312-2 7
variation could be a useful instrument to assess causality provided that several requirements have been satisfi ed.35,36 First, one needs suitable genetic variants for the study of the modifi able exposure of interest (in our case, plasma HDL cholesterol). Although many loci are associated with plasma HDL cholesterol, we found LIPG Asn396Ser to be particularly informative because it is specifi cally associated with substantial increases in HDL cholesterol. Additionally, we evaluated a set of 14 common genetic variants that also exclusively aff ected HDL cholesterol. Both instruments, LIPG Asn396Ser and the genetic score, produced similar results.
Second, reliable genotype-to-intermediate-phenotype and intermediate-phenotype-to-disease eff ect estimates are needed. To obtain as precise estimates as possible, we derived SNP-to-lipid eff ect estimates from analysis of a large sample involving more than 24 000 participants. Estimates of plasma lipid to myocardial infarction were derived from meta-analysis of four large cohort studies involving more than 25 000 participants.
Third, there must not be pleiotropic eff ects of the genetic variants of interest. We cannot exclude all potential pleiotropic eff ects of the LIPG Asn396Ser SNP; however, we have assessed but did not detect pleiotropic eff ects on other cardiovascular risk factors including LDL cholesterol, small LDL particle concentration, tri-glycerides, body-mass index, systolic blood pressure, plasma C-reactive protein, and type 2 diabetes status.
Finally, the absence of association of individual SNPs with myocardial infarction could be due to low statistical power. However, for the crucial SNP in the mendelian randomisation study for plasma HDL cholesterol, we had suffi cient power. In this study, LIPG Asn396Ser has been tested in 20 913 myocardial infarction cases and 95 407 myocardial-infarction-free participants. We had 90% power to detect the expected 13% reduction in risk of myocardial infarction for the LIPG Asn396Ser variant (at a two-sided α of 0·05).
In summary, our results showed that polymorphisms related to plasma LDL cholesterol were consistently associated with risk of myocardial infarction, whereas this was not the case for variants related to plasma HDL cholesterol. A polymorphism in the endothelial lipase gene and a genetic score of 14 common SNPs that specifi cally raised HDL cholesterol were not associated with myocardial infarction, suggesting that some genetic mechanisms that raise HDL cholesterol do not lower risk of myocardial infarction. Hence, interventions (lifestyle or pharmacological) that raise plasma HDL cholesterol cannot be assumed ipso facto to lead to a corresponding benefi t with respect to risk of myocardial infarction.Affi liationsDepartment of Pharmacology and Department of Genetics (B F Voight PhD), University of Pennsylvania, Philadelphia, PA, USA; Center for Human Genetic Research (B F Voight PhD, C Newton-Cheh MD, K Musunuru MD, J Pirruccello BS, R Do PhD, M J Daly PhD, S Purcell PhD, Prof D Altshuler PhD, S Kathiresan MD), Department of Molecular Biology (Prof D Altshuler MD), Cardiovascular
Research Center (C Newton-Cheh MD, K Musunuru MD, J Pirruccello BS, R Do PhD, S Kathiresan MD), Cardiology Division (C Newton-Cheh MD, C J O’Donnell MD, S Kathiresan MD), Massachusetts General Hospital, Boston, MA, USA; Program in Medical and Population Genetics, Broad Institute, Cambridge, MA, USA (B F Voight PhD, C Newton-Cheh MD, K Musunuru MD, J Pirruccello BS, Prof P I W de Bakker PhD, M J Daly PhD, C Guiducci BS, N P Burtt BS, A Surti BS, E Gonzalez BS, S Purcell PhD, S Gabriel PhD, Prof D Altshuler PhD, S Kathiresan MD); Department of Biostatistics, Boston University School of Public Health, Boston, MA, USA (G M Peloso PhD, S Demissie PhD, Prof L A Cupples PhD); Framingham Heart Study of the National, Heart, Lung, and Blood Institute, Framingham, MA, USA (G M Peloso PhD, S Demissie PhD, Prof L A Cupples PhD, C J O’Donnell MD); Diabetes and Cardiovascular Disease Genetic Epidemiology (M Orho-Melander PhD, G Hindy MD), and Department of Clinical Sciences, Hypertension and Cardiovascular Diseases (Prof O Melander MD), Skania University Hospital, Lund University, Malmö, Sweden; Department of Clinical Biochemistry, Section for Molecular Genetics, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark (R Frikke-Schmidt DMSc, Prof A Tybjaerg-Hansen DMSc); Human Genetics Center, University of Texas Health Science Center at Houston, Houston, TX, USA (M Barbalic PhD, E Boerwinkle PhD); Department of Nutrition and Epidemiology (M K Jensen PhD, E B Rimm ScD), and Department of Nutrition (E L Ding ScD), Harvard School of Public Health, Boston, MA, USA; Channing Laboratory, Department of Medicine, Brigham and Women’s Hospital, Boston, MA, USA (E B Rimm ScD, E L Ding ScD); deCODE Genetics, Reykjavik, Iceland (H Holm MD, G Thorleifsson PhD, K Stefannson MD, U Thorsteinsdottir PhD); Clinical Pharmacology and The Genome Centre, William Harvey Research Institute, Barts and The London School of Medicine and Dentistry, Queen Mary University of London, London, UK (T Johnson PhD); Medizinische Klinik II (Prof H Schunkert MD, J Erdmann PhD, P Diemert MD), and Institut für Medizinische Biometrie und Statistik (A Schillert PhD, C Willenborg MSc, I R Koenig PhD, A Ziegler PhD), Universität zu Lübeck, Lübeck, Germany; Department of Cardiovascular Sciences (Prof N J Samani MD), and Department of Health Sciences (Prof J F Thompson PhD), University of Leicester, Leicester, UK; Leicester National Institute of Health Research Biomedical Research Unit in Cardiovascular Disease, Glenfi eld Hospital, Leicester, UK (Prof N J Samani MD); Biostatistics and Epidemiology (M Li PhD), and The Institute for Translational Medicine and Therapeutics and The Cardiovascular Institute (M Reilly MD, Prof D Rader MD), University of Pennsylvania, Philadelphia, PA, USA; Department of Public Health and Primary Care, University of Cambridge, Cambridge, UK (D Saleheen MBBS, Prof J Danesh FRCP); The John & Jennifer Ruddy Canadian Cardiovascular Genetics Centre, University of Ottawa Heart Institute, Ottawa, ON, Canada (L Chen MSc, A F R Stewart PhD, Prof R McPherson MD, Prof R Roberts MD); The Clinical Trial Service Unit and Epidemiological Studies Unit (R Clarke MD, J C Hopewell PhD), and Department of Cardiovascular Medicine (J Peden PhD, Prof H Watkins MD), University of Oxford, Oxford, UK, on behalf of the PROCARDIS Consortium; University of Iceland Faculty of Medicine, Reykjavik, Iceland (K Stefannson MD, U Thorsteinsdottir PhD, G Thorgeirsson MD); Department of Internal Medicine, Division of Cardiology, Landspitali University Hospital, Reykjavik, Iceland (G Thorgeirsson); Population Health Research Institute, Hamilton Health Sciences and Department of Medicine and Department of Clinical Epidemiology and Biostatistics, McMaster University, Hamilton, ON, Canada (Prof S Anand PhD); Department of Medicine and Department of Human Genetics, McGill University, Montréal, QC, Canada (J Engert PhD); Department of Pediatrics, Vanderbilt University School of Medicine, Nashville, TN, USA (T Morgan MD); Mid-America Heart Institute and University of Missouri-Kansas City, Kansas City, MO, USA (Prof J Spertus MD); Leibniz-Institute for Arteriosclerosis Research (Prof M Stoll PhD), and Institute of Epidemiology and Social Medicine (Prof K Berger MD), University of Münster, Münster, Germany; Department of Medicine, University of Verona, Verona, Italy (N Martinelli MD, Prof D Girelli MD); Centre for Public Health, Queen’s University

Articles
8 www.thelancet.com Published online May 17, 2012 DOI:10.1016/S0140-6736(12)60312-2
Belfast, Institute of Clinical Science, Belfast, UK (Prof P P McKeown MD, C C Patterson PhD); Cardiovascular Research Institute, MedStar Research Institute, Washington Hospital Center, Washington, DC, USA (S E Epstein MD, J Devaney PhD, M-S Burnett PhD); Genetics Division and Drug Discovery, GlaxoSmithKline, King of Prussia, Pennsylvania, PA, USA (V Mooser MD); Institute for Molecular Medicine Finland FIMM, University of Helsinki, Finland (S Ripatti PhD, I Surakka BSci, Prof M S Nieminen PhD, L Peltonen PhD); Division of Cardiology Department of Medicine, Helsinki University Central Hospital, Helsinki, Finland (Prof M S Nieminen PhD, J Sinisalo MD); Transplantation Laboratory, Haartman Institute, University of Helsinki, Helsinki, Finland (M-L Lokki PhD); Chronic Disease Epidemiology and Prevention Unit, Department of Chronic Disease Prevention, National Institute for Health and Welfare, Helsinki, Finland (A S Havulinna PhD, Prof M Perola PhD, Prof V Salomaa MD); Division of Cardiovascular Epidemiology and Institute of Environmental Medicine (Prof U de Faire MD, B Gigante MD), and Department of Medical Epidemiology and Biostatistics (E Ingelsson PhD), Karolinska Institutet, Stockholm, Sweden; der Johannes Gutenberg-Universität Mainz II, Medizinische Klinik und Poliklinik, Mainz, Germany (T Zeller PhD, P Wild MD, Prof S Blankenberg MD); Division of Genetics, Department of Medicine, Brigham and Women’s Hospital, and Harvard Medical School, Boston, MA, USA (Prof P I W de Bakker PhD); Division of Pharmaco epidemiology and Clinical Pharmacology, Utrecht Institute for Pharmaceutical Sciences, Utrecht University, Netherlands (O H Klungel PhD, A H Maitland-van der Zee PhD, B J M Peters PhD, Prof A de Boer PhD); Julius Center for Health Sciences and Primary Care (Prof D E Grobbee PhD, C C Elbers PhD, N C Onland-Moret PhD, Prof Y T van der Schouw PhD, Prof P I W de Bakker PhD), and Department of Medical Genetics (C C Elbers PhD, N C Onland-Moret PhD, Prof P I W de Bakker PhD), University Medical Center Utrecht, Utrecht, Netherlands; Department of Vascular Medicine (P W Kamphuisen PhD), Department of Pathology and Medical Biology (Prof M H Hofker PhD), and Department of Genetics (Prof C Wijmenga PhD), University Medical Center Groningen, Groningen, Netherlands; Department of Clinical Pharmacy, St Antonius Hospital, Nieuwegein, Netherlands (V H M Deneer PhD); Center for Prevention and Health Services Research (W M M Verschuren PhD), and Center for Nutrition and Health (J M A Boer PhD), National Institute for Public Health and the Environment, Bilthoven, Netherlands; Center for Non-Communicable Diseases, Karachi, Pakistan (A Rasheed, P Frossard); Center for Statistical Genetics, Department of Biostatistics, University of Michigan, Ann Arbor, MI, USA (C Willer PhD, Prof G R Abecasis PhD, Prof M Boehnke PhD); Nutrition and Genomics Laboratory, Jean Mayer United States Department of Agriculture Human Nutrition Research Center on Aging at Tufts University, Boston, MA, USA (Prof J M Ordovas PhD); Department of Cardiovascular Epidemiology and Population Genetics, Centro Nacional de Investigaciones Cardiovasculares, Madrid, Spain (Prof J M Ordovas PhD); Department of Genetics, University of North Carolina, Chapel Hill, NC, USA (K Mohlke PhD); Cardiovascular Epidemiology and Genetics, IMIM, Barcelona, Spain (J Marrugat PhD, R Elosua PhD); CIBER Epidemiología y Salud Pública, Barcelona, Spain (R Elosua PhD); Klinik und Poliklinik für Innere Medizin II, Universitätsklinikum Regensburg, Regensburg, Germany (M Fischer MD, C Hengstenberg MD); Vesalius Research Center, VIB-KU Leuven (I Buysschaert MD, D Lambrechts PhD), and Department of Cardiology, University Hospital Gasthuisberg (I Buysschaert MD, D Lambrechts PhD, Prof F van de Werf MD), Leuven, Belgium; Cardiovascular Research, Division of Medical and Radiological Sciences, The University of Edinburgh, Edinburgh, UK (Prof K A Fox MBChB); Institut für Klinische Molekularbiologie, Christian-Albrechts Universität, Kiel, Germany (N E El Mokhtari MD, Prof S Schreiber MD, A Schäfer PhD); Medizinische Klinik I, Universitätsklinikum Schleswig Holstein, Campus Kiel, Kiel, Germany (D Rubin MD); Max-Rubner-Institut, Institut für Physiologie und Biochemie der Ernährung, Kiel, Germany (J Schrezenmeir PhD); LIGHT and LIMM Research Institutes, Faculty of Medicine and Health, University of Leeds, Leeds, UK (Prof A Hall MD); Department of Epidemiology, School of Public Health, Aarhus University, Aarhus,
Denmark (Prof K Overvad MD); The Copenhagen City Heart Study Bispebjerg University Hospital, Copenhagen, Denmark (Prof A Tybjaerg-Hansen MD); Department of Internal Medicine and Medical Specialities, IRCCS Fondazione Cà Granda Ospedale Maggiore Policlinico, Milan, Italy (Prof P M Mannucci MD); Division of Cardiology, Azienda Ospedaliero-Universitaria di Parma, Parma, Italy (Prof D Ardissino MD); Cardiovascular Health Research Unit, Department of Medicine and Department of Epidemiology, University of Washington, Seattle, WA, USA (Prof D Siscovick MD, Prof S Schwartz PhD); Wellcome Trust Sanger Institute Cambridge, UK (Prof L Peltonen PhD); and Department of Genetics, Harvard Medical School, Boston, MA, USA (Prof D Altshuler MD)
ContributorsBFV, DAltshuler, and SK contributed to study design. BFV, GMP, MO-M, RF-S, MB, MKJ, GH, HH, ELD, TJ, HS, NJS, RClarke, JCH, JFT, ML, GThorleifsson, CN-C, KM, JP, DS, LC, AFRS, SA, JCE, TM, JS, MS, KB, NM, DG, PPM, CCP, UT, GThorgeirsson, BG, PIWdeB, SR, CWiller, JE, PD, JD, SB, RR, RM, HW, ASH, KO, ER, EB, AT-H, LAC, MPR, OM, PMM, DAltshuler, DS, RE, KS, CJO, VS, DJR, LP, SMS, DArdissino, SK, and all collaborators contributed to data collection and did research. BFV, GMP, MO-M, RF-S, MB, MJK, GH, ELD, JCH, JFT, ML, GThorleifsson, KM, JP, DS, LD, ASurti, JCE, TM, MS, NM, CCP, BG, PIWdeB, SR, CWijmenga, SMS, DArdissino, and SK contributed to data analysis and interpreted results. BFV, GMP, DAltshuler, and SK wrote the report. HS, NJS, RClarke, CN-C, KM, JP, JCE, TM, JS, DG, PPM, EB, MPR, OM, DS, RE, CJO, VS, DJR, SMS, DAltshuler, and SK revised and reviewed the fi nal report.
Confl icts of interestKS, UT, HH, GThorleifsson, and GThorgeirsson are employees of or own stock options in deCODE Genetics, or both. SK serves on a scientifi c advisory board for Merck and has received research grants from Pfi zer, Shire Therapeutics, and Alnylam Pharmaceuticals. HS serves on scientifi c advisory boards for Merck, Servier, and AstraZeneca and received lecture fees from Pfi zer, Novartis, and Boehringer Ingelheim. The collection of clinical and sociodemographic data in the Dortmund Health Study was supported by the German Migraine & Headache Society (DMKG) and by unrestricted grants of equal share from AstraZeneca, Berlin Chemie, Boots Healthcare, GlaxoSmithKline, McNeil Pharma (formerly Woelm Pharma), MSD Sharp & Dohme, and Pfi zer to the University of Muenster. VM, DW, CK, and MW are full-time employees of GlaxoSmithKline. All other authors declare that they have no confl icts of interest.
AcknowledgmentsThis Article is dedicated to Leena Peltonen, who passed away on March 11, 2010. A full listing of the acknowledgments is provided in the appendix p 12.
References1 Expert Panel on Detection, Evaluation, and Treatment of High
Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001; 285: 2486–97.
2 Prospective Studies Collaboration. Blood cholesterol and vascular mortality by age, sex, and blood pressure: a meta-analysis of individual data from 61 prospective studies with 55 000 vascular deaths. Lancet 2007; 370: 1829–39.
3 Di Angelantonio E, Sarwar N, Perry P, et al. Major lipids, apolipoproteins, and risk of vascular disease. JAMA 2009; 302: 1993–2000.
4 Cholesterol Treatment Trialists’ (CTT) Collaborators. Effi cacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90 056 participants in 14 randomised trials of statins. Lancet 2005; 366: 1267–78.
5 Rader DJ, Cohen J, Hobbs HH. Monogenic hypercholesterolemia: new insights in pathogenesis and treatment. J Clin Invest 2003; 111: 1795–803.
6 Cohen JC, Boerwinkle E, Mosley TH Jr, Hobbs HH. Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N Engl J Med 2006; 354: 1264–72.

Articles
www.thelancet.com Published online May 17, 2012 DOI:10.1016/S0140-6736(12)60312-2 9
7 Barter PJ, Caulfi eld M, Eriksson M, et al. Eff ects of torcetrapib in patients at high risk for coronary events. N Engl J Med 2007; 357: 2109–22.
8 Frikke-Schmidt R, Nordestgaard BG, Stene MC, et al. Association of loss-of-function mutations in the ABCA1 gene with high-density lipoprotein cholesterol levels and risk of ischemic heart disease. JAMA 2008; 299: 2524–32.
9 Gray R, Wheatley K. How to avoid bias when comparing bone marrow transplantation with chemotherapy. Bone Marrow Transplant 1991; 7 (suppl 3): 9–12.
10 Katan MB. Apolipoprotein E isoforms, serum cholesterol, and cancer. Lancet 1986; 327: 507–08.
11 Davey Smith G, Ebrahim S. ‘Mendelian randomization’: can genetic epidemiology contribute to understanding environmental determinants of disease? Int J Epidemiol 2003; 32: 1–22.
12 Johannsen TH, Kamstrup PR, Andersen RV, et al. Hepatic lipase, genetically elevated high-density lipoprotein, and risk of ischemic cardiovascular disease. J Clin Endocrinol Metab 2009; 94: 1264–73.
13 Kathiresan S, Melander O, Anevski D, et al. Polymorphisms associated with cholesterol and risk of cardiovascular events. N Engl J Med 2008; 358: 1240–49.
14 Willer CJ, Sanna S, Jackson AU, et al. Newly identifi ed loci that infl uence lipid concentrations and risk of coronary artery disease. Nat Genet 2008; 40: 161–69.
15 Haase CL, Tybjaerg-Hansen A, Ali Qayyum A, Schou J, Nordestgaard BG, Frikke-Schmidt R. LCAT, HDL cholesterol and ischemic cardiovascular disease: a mendelian randomization study of HDL cholesterol in 54,500 individuals. J Clin Endocrinol Metab 2012; 97: E248–56.
16 Kathiresan S, Willer CJ, Peloso GM, et al. Common variants at 30 loci contribute to polygenic dyslipidemia. Nat Genet 2009; 41: 56–65.
17 Teslovich TM, Musunuru K, Smith AV, et al. Biological, clinical and population relevance of 95 loci for blood lipids. Nature 2010; 466: 707–13.
18 deLemos AS, Wolfe ML, Long CJ, Sivapackianathan R, Rader DJ. Identifi cation of genetic variants in endothelial lipase in persons with elevated high-density lipoprotein cholesterol. Circulation 2002; 106: 1321–26.
19 Edmondson AC, Brown RJ, Kathiresan S, et al. Loss-of-function variants in endothelial lipase are a cause of elevated HDL cholesterol in humans. J Clin Invest 2009; 119: 1042–50.
20 Palmer TM, Lawlor DA, Harbord RM, et al. Using multiple genetic variants as instrumental variables for modifi able risk factors. Stat Methods Med Res 2011; published online Jan 7. DOI:10.1177/0962280210394459.
21 Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002; 21: 1539–58.
22 Purcell S, Neale B, Todd-Brown K, et al. PLINK: a tool set for whole-genome association and population-based linkage analysis. Am J Hum Genet 2007; 81: 3.
23 Lawlor DA, Harbord RM, Sterne JA, Timpson N, Davey Smith G. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med 2008; 27: 1133–63.
24 Ding EL, Song Y, Manson JE, et al. Sex hormone-binding globulin and risk of type 2 diabetes in women and men. N Engl J Med 2009; 361: 1152–63.
25 Ehret GB, Munroe PB, Rice KM, et al. Genetic variants in novel pathways infl uence blood pressure and cardiovascular disease risk. Nature 2011; 478: 103–09.
26 Schunkert H, Konig IR, Kathiresan S, et al. Large-scale association analysis identifi es 13 new susceptibility loci for coronary artery disease. Nat Genet 2011; 43: 333–38.
27 Ishida T, Choi S, Kundu RK, et al. Endothelial lipase is a major determinant of HDL level. J Clin Invest 2003; 111: 347–55.
28 Ishida T, Choi SY, Kundu RK, et al. Endothelial lipase modulates susceptibility to atherosclerosis in apolipoprotein-E-defi cient mice. J Biol Chem 2004; 279: 45085–92.
29 Ko KW, Paul A, Ma K, Li L, Chan L. Endothelial lipase modulates HDL but has no eff ect on atherosclerosis development in apoE-/- and LDLR-/- mice. J Lipid Res 2005; 46: 2586–94.
30 Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women. Heart and Estrogen/progestin Replacement Study (HERS) Research Group. JAMA 1998; 280: 605–13.
31 Boden WE, Probstfi eld JL, Anderson T, et al. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med 2011; 365: 2255–67.
32 Thompson A, Di Angelantonio E, Sarwar N, et al. Association of cholesteryl ester transfer protein genotypes with CETP mass and activity, lipid levels, and coronary risk. JAMA 2008; 299: 2777–88.
33 Cannon CP, Shah S, Dansky HM, et al. Safety of anacetrapib in patients with or at high risk for coronary heart disease. N Engl J Med 2010; 363: 2406–15.
34 Khera AV, Cuchel M, de la Llera-Moya M, et al. Cholesterol effl ux capacity, high-density lipoprotein function, and atherosclerosis. N Engl J Med 2011; 364: 127–35.
35 Smith GD, Ebrahim S. Mendelian randomization: prospects, potentials, and limitations. Int J Epidemiol 2004; 33: 30–42.
36 Nitsch D, Molokhia M, Smeeth L, DeStavola BL, Whittaker JC, Leon DA. Limits to causal inference based on Mendelian randomization: a comparison with randomized controlled trials. Am J Epidemiol 2006; 163: 397–403.

Supplementary appendixThis appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors.
Supplement to: Voight BF, Peloso GM, Orho-Melander M, et al. Plasma HDL cholesterol and risk of myocardial infarction: a mendelian randomisation study. Lancet 2012; published online May 17. DOI:10.1016/S0140-6736(12)60312-2.

Appendix

SNP Selection and Genotyping
We selected the initial 25 SNPs mapped for plasma HDL-C or LDL-C concentrations using a
genome-wide association approach.1 Each selected SNP has been associated with either HDL-C
or LDL-C at a P<5 x 10-8.
In case-control studies, genotypes were extracted from 16 genome-wide association
studies (GWAS) and directly genotyped in an additional 14 studies. Array-based genotyping was
conducted using Affymetrix 500K, Affymetrix 5.0, Affymetrix 6.0, Illumina Human Hap300,
Illumina HumanHap370, Illumina HumanHap610 chips as previously described.2 Imputation for
un-genotyped SNPs and quality control were conducted as previously described.2 Direct
genotyping was attempted in 13 studies using the Sequenom iPLEX MassARRAY platform or
the Illumina HumanCVDBeadChip Infinium II assay.3 Direct genotyping at deCODE was done
using the Centaurus (Nanogen) platform. We only considered SNPs that exceeded stringent
quality control criteria including genotyping call rate > 95% and Hardy-Weinberg equilibrium
filters (P > 10-6 for SNPs from GWAS or P > 0.001 for all other SNPs).
In each of six prospective cohort studies, LIPG Asn396Ser was directly genotyped as
described in Supplementary Table 2.
Predicted MI Risk for LIPG Asn396Ser Based on Plasma HDL-C Difference
We estimated a predicted risk for LIPG Asn396Ser based on the relationship of this SNP with
plasma HDL-C and the relationship of plasma HDL-C with MI in the population. For LIPG
Asn396Ser, we estimated the SNP-to-HDL-C parameter estimate from four prospective cohort
studies involving >25,000 participants (Supplementary Table 3).
2

We obtained the HDL-C-to-MI parameter estimates from four prospective cohort studies.
In the Atherosclerosis Risk in Communities Study (ARIC), Copenhagen City Heart Study
(CCHS), Framingham Heart Study (FHS) 2nd Generation participants, and Malmo Diet and
Cancer Study-Cardiovascular Cohort (MDCS-CC), we constructed logistic regression models to
examine the association of incident MI status with plasma LDL-C, HDL-C, or triglycerides
(TG), excluding subjects who had had a prevalent MI or ischemic stroke. The predictor variable
of plasma lipid fraction was modeled in standard deviation units. Covariates in the model
included age and gender. As a single time point measurement of a plasma lipid fraction can
underestimate the relationship between lipids and MI,4 we adjusted the hazard ratios for
regression dilution bias 5 in a manner consistent with other recent studies.6 The overall effect of
each plasma lipid fraction across the four studies was summarized using fixed-effects inverse-
variance-weighted meta-analysis (Supplementary Table 4).
Using the SNP-to-biomarker and the biomarker-to-MI relationships as inputs, we derived
predicted MI risk for LIPG Asn396Ser. For LIPG Asn396Ser, we first calculated the change in
plasma HDL-C in SD units. This degree of change in plasma HDL-C was algebraically
converted to an odds ratio for MI by multiplying the plasma HDL-C change (in SD units) by the
beta-coefficient (representing log odds ratios) from the HDL-C-to-MI modeling described
above.6
Instrumental Variable Analysis Using LIPG Asn396Ser
We performed instrumental variable analysis in the six prospective cohort studies listed in
Supplementary Table 5. In four of the six studies (ARIC, CCHS, HPFS, and MDCS-CC), we
used the qvf command, with Murphy–Topel variance, to fit the data to logistic-regression models
3

for MI using LIPG Asn396Ser as a randomized instrument.7 For two studies, an alternate two-
stage regression approach was used because of the presence of related individuals (FHS) or case-
cohort design (DCH). For these two studies, in the first stage, generalized estimating equations
(FHS) or a generalized linear model (DCH) was fitted with the outcome variable of plasma
HDL-C and predictor variables of LIPG Asn396Ser genotype, age, and gender. In the second
stage, a generalized linear model was used to test the association of MI status with the fitted
HDL-C from the first stage. A summary instrumental variable estimate for the association of
plasma HDL-C with MI risk across the six studies was generated with fixed-effects variance-
weighted meta-analysis.
Mendelian randomization using multiple genetic variants as instrumental
variables
It has recently been proposed that statistical power for instrumental variable analysis could be
increased if multiple genetic variants in combination were used as instruments.8 From our
recently published genome-wide association study of plasma lipids traits involving >100,000
individuals,9 we observed that 13 SNPs had statistical evidence at genome-wide levels of
significance (P < 5 x 10-8) for plasma LDL-C and no evidence for association with triglycerides
(P>0.01) or HDL-C (P>0.01). We constructed a “LDL-C genetic score” combining the LDL-C
raising alleles at each of these 13 SNPs (Supplementary Table 9). We also observed that 14
SNPs had statistical evidence at genome-wide levels of significance (P < 5 x 10-8) for plasma
HDL-C and no evidence for association with triglycerides (P>0.01) or LDL-C (P>0.01). We
constructed a “HDL-C genetic score” combining the HDL-C raising alleles at each of these 14
4

SNPs (Supplementary Table 10). Each SNP was given a weight based on the degree of LDL-C
change or HDL-C change as estimated in ~100,000 individuals.9
We defined genetic risk scores in the following way10: Using a set of m SNPs, for the i-th
SNP in the j-th individual denote xij as the 0/1/2 coded genotype (for directly genotyped SNPs)
or expected allele dosage (which takes real values between 0.0 and 2.0 for imputed SNPs). Using
results from Teslovich et al.,9 define the set of regression coefficients to be w1, w2, ..., wm. Then
the risk score for subject j is defined to be
(1) sj = s0 + w1 x1j + w2 x2j + ... + wm xmj,
where s0 is the intercept. In all our analyses, we specify the coefficients w1, w2, ..., wm to be the
effect sizes, in standard deviation units per coded allele, estimated in single SNP analyses of
LDL-C or HDL-C.
We also note that, when considering multiple SNPs that are in linkage equilibrium with
each other, and small effect sizes per SNP, effect sizes estimated jointly for all SNPs using a
multiple regression model are effectively identical to those estimated in a series of single SNP
regression models. Thus regression on the risk score can be reconstructed from regressions on
each of the m SNPs in turn, without further access to individual-level data.
The calculations involved are of the same type as for meta-analysis; the coefficient of the
risk score is a weighted mean of the per-SNP regression coefficients, where each is weighted by
its corresponding wi. The estimated variance of the risk score is given by similarly weighting the
estimated variances (squared standard errors) of each per-SNP regression coefficient. The
assumption of zero LD between SNPs ensures that these contributions are independent.
Importantly, as with inverse-variance weighted meta-analysis, in large samples this procedure
gives valid p-values under the null, i.e. when there is no relationship between the “lookup”
5

phenotype and any variants at the SNPs contributing to the risk score.
Using SNP-specific results in this way, we estimated and tested the coefficient of the risk
score in independent “lookup” results using logistic regression for myocardial infarction
phenotype from the published Coronary ARtery DIsease Genome-wide Replication And Meta-
analysis (CARDIoGRAM) consortium GWAS study.11,12 These estimates and tests inherit the
covariate adjustment performed in the original SNP-specific analysis.
The CARDIoGRAM consortium combines data from 14 GWAS in individuals with
European ancestry including 22,233 cases with coronary artery disease and/or MI and 64,762
controls.11 For all of the participating studies, genome-wide scans were performed in the years
2006-2009 using either Affymetrix or Illumina platforms followed by imputation of genotypes in
most studies. Statistical methods have been standardized across the studies, and an analysis
platform has been created to allow summarized analyses on coronary artery disease, MI, and
related phenotypes. We restricted our analysis to the subgroup of up to 12,482 MI cases and
41,331 MI-free controls.
Descriptions of Case-Control Studies Italian ATVB Study, Heart Attack Risk in Puget Sound, REGICOR, MGH Premature Coronary Artery Disease Study, FINRISK, Malmo Diet and Cancer Study Early-Onset MI, PennCATH, deCODE, MedSTAR, Verona Heart Study, Mid-America Heart Institute, Irish Family Study, INTERHEART, and AMI Gene Study/Dortmund Health Study: Details for the recruitment of participants for these studies have been described in detail in a recent publication.2 WTCCC MI and German MI Family Study I: Details for the recruitment of the WTCCC CAD and German MI Family Study I are as recently described.13 For the present report, we limited the analysis to cases that met clinical criterion for MI. SHEEP: Details for the recruitment of SHEEP subjects are as recently described.14,15
6

Malmo Diet and Cancer Study Later-Onset MI: The Malmö Diet and Cancer (MDCS) study is a community-based prospective epidemiologic cohort of 28,449 persons recruited for a baseline examination between 1991 and 1996.16 All participants underwent a medical history, a physical examination, and a laboratory assessment for cardiovascular risk factors as described previously.17 From this cohort, 1,059 persons with MI at older age (age at MI for men >50 or women >60) were studied. Fatal or non-fatal MI status was determined as described previously.18 For each case, a random control was selected. COROGENE: Initially a sample was collected including all consecutive Finnish patients assigned to coronary angiogram within a 20-month period (June 2006–March 2008, n=5,330) in the Helsinki University Central Hospital. Data collection included a questionnaire, information on previous medical conditions and cardiovascular risk factors, hospital records for patients’ history, various laboratory measurements, ECG, echocardiography, and medication. Approximately 22% of the patients were angiographically free of coronary artery disease (CAD). Different stages of atherosclerosis were found in 75% of patients, of which 53% had acute coronary syndrome (ACS; n=2,172). These ACS patients were selected as the complete set of COROGENE cases. The controls for COROGENE cases were selected from the FINRISK 1997, 2002 and 2007, participants from the Helsinki-Vantaa region using risk set sampling.19 For each case independently (= with replacement), two controls (if possible) were sampled from all controls who fulfilled the following criteria. The controls had to be 1) of the same sex, 2) of the same birth cohort (within ±5 years) to reduce the effect of secular trends and 3) free of cardiovascular disease (CVD) at least until the case’s age of having ACS. The CADomics Study: CADomics (Coronary Artery Disease and genomics) is a German-based case-control study of CAD. It is a pooled study from the population-based Gutenberg-Heart Study (GHS) and the hospital (cath-lab)-based Atherogene Registry.20-22
The GHS is a population-based, prospective, observational single-center cohort study in the Rhein-Main-Region in western mid-Germany. The primary aim of GHS is to evaluate and improve cardiovascular risk stratification. The sample was drawn randomly from the governmental local registry offices that contain all citizens in the city of Mainz and the district of Mainz-Bingen. Individuals between ages 35 and 74 were enrolled and enrollment was stratified for gender, residence (urban and rural) and decade of age. Exclusion criteria were insufficient knowledge of the German language, and physical or psychological inability to participate. Cardiovascular risk factors were assessed by a computer-assisted personal interview, from laboratory analyses of a venous blood sample in a fasting state, blood pressure and anthropometric measurements.
The Atherogene Registry has been described elsewhere.20 Briefly, between June 1999 and February 2004, patients with documented CAD referred to the Department of Medicine II of the Johannes Gutenberg-University in Mainz, Germany and the Department of Medicine of the German Federal Armed Forces Central Hospital, Koblenz, were enrolled in the AtheroGene study registry. All participants had coronary angiography. Information on cardiovascular risk factors and coronary angiography were extracted from medical records. The angiograms were scored at the time of procedure by an interventional cardiologist.
For the current analysis, 1,212 had a diagnosis of MI and were included as cases in this report. A total of 2,952 did not have a history of MI and were included as controls.
7

Ottawa Heart Genomics Study I and I: Details for the recruitment of subjects are as recently described.23,24 GRACE GENETICS: The GRACE Genetics study prospectively enrolled 683 patients with an ACS between January 2001 and December 2007 in two hospitals in Belgium (University Hospital Gasthuisberg, Leuven and Onze-Lieve-Vrouw Clinic, Aalst). To ensure enrollment of an unselected ACS population, sites recruited the first 10-20 consecutive eligible patients each month.25 Controls comprised 656 healthy blood donors from the Red Cross Belgium recruited from January to March 2008.26 PROCARDIS: The PROCARDIS study is a multi-centre case-control study in which CAD cases and controls were recruited from four European countries (United Kingdom, Italy, Sweden and Germany) according to pre-specified criteria.27 All participants provided written informed consent to a protocol that was approved by the Ethics Committees of the participating institutions. All cases had a diagnosis of CAD before age 66 years and also had a sibling with CAD before age 66 years. Among the 3146 CAD cases, 2183 had a diagnosis of MI (91% confirmed by hospital discharge or general practice records) and were included as cases in this report. Controls with no personal or sibling history of CAD before age 66 years were contemporaneously recruited using the same infrastructure. Utrecht Cardiovascular Pharmacogenetics (UCP) Studies: Participants were enrolled from the population-based Pharmaco-Morbidity Record Linkage System (PHARMO, www.pharmo.nl). PHARMO links drug dispensing histories from a representative sample of Dutch community pharmacies to the national registration of hospital discharges (Landelijke Medische Registratie, LMR) since 1985 on a continuous basis. Currently, the base population of PHARMO covers approximately 2,000,000 community-dwelling inhabitants of several population-defined areas in the Netherlands. Approval for this study was obtained from the Medical Ethics Committee of the University Medical Center Utrecht, The Netherlands.
Briefly, patients with a high cardiovascular risk defined as those who received a prescription for an antihypertensive drug, or a glucose lowering drug, or who had hypercholesterolemia (prescription for a cholesterol-lowering drug or total cholesterol > 5.0 mmol/l), were selected from the PHARMO database. From this cohort, patients hospitalized for acute coronary syndrome (ACS) were included as cases (acute myocardial infarction (AMI, International Classification of Diseases (ICD)-9 code 410)) or (sub)acute forms of ischemic heart disease (ICD-9 codes 411.1 and 411.8)) if they were registered in PHARMO for at least one year and were older than 18 years. The index date was defined as the date of hospitalization for the first ACS. Controls met the same eligibility criteria as the cases, but had not developed ACS.
Participants were recruited through community pharmacies, where they received a letter in which the purpose of the study was explained. They were asked to return an informed consent form and a filled-out questionnaire. After the participant had consented to participate in the study, (s)he was sent an Oragene collection kit (hypercholesterolemic and diabetic cohort), or three cotton swabs and tubes containing buffer (hypertensive cohort) to collect saliva. All participants were explicitly asked to consent for the collection, storage and genotyping of the DNA material.
8

EPIC-NL: The EPIC-NL cohort is the Dutch contribution to the European Prospective Investigation into Cancer and Nutrition, and consists of the Prospect cohort, a prospective population based cohort of 17,357 women between 49-70 years at recruitment participating in breast cancer screening between 1993 and 1997, and the Monitoring Project on Risk Factors for Chronic Diseases (MORGEN) cohort, consisting of 22,654 men and women between 20-59 years at recruitment in three Dutch towns (Amsterdam, Maastricht and Doetinchem). At baseline, a general questionnaire containing questions on demographic characteristics, smoking, presence of chronic diseases and other potential risk factors was filled out by all participants. Body weight, height, waist, and hip circumference were also measured, and a n on-fasting blood sample was taken. Information on incident coronary heart disease occurrence during follow-up was obtained through linkage with the database of hospital discharge diagnoses from the Dutch National Medical Registry. For this study, 334 MI cases and 1,827 randomly-selected MI-free controls were genotyped. AngioGOKARD/KORA: The Lübeck and Regensburg angiographic study (Angio/GOKARD) includes 1,953 patients with angiographically proven CAD who underwent cardiac catheterization at the University Hospital Schleswig-Holstein, Campus Lübeck and University Hospital Regensburg between 2005 and 2010. Patients were not selected for particular risk factors or phenotypes.28 Controls comprise individuals from the population-based MONICA/KORA Augsburg survey F3 (n=1,564).29 PopGen: The PopGen CAD sample (n=2,433) comprised unrelated German MI patients with early onset of disease who were recruited in Schleswig-Holstein, through regional catheterisation laboratories in the northernmost region in Germany (University Hospital Schleswig-Holstein, Campus Kiel, local hospitals Rendsburg, Schleswig, Flensburg, Heide), that have been contacted by the population-based PopGen biobank (www.PopGen.de). 1,687 PopGen-controls of the Max-Rubner-Institute were part of the Metabolic Intervention Cohort Kiel (MICK) and selected by age from the general population via the registration register of the same region.30 PROMIS: Details for the recruitment of the PROMIS subjects are as recently described.31
9

Descriptions of Cohort Studies Atherosclerosis Risk in Communities Study (ARIC): The ARIC study is a prospective population-based study in 15,792 men and women, including 11,478 non-Hispanic whites and 4,314 African-Americans, drawn from 4 U.S. communities (suburban Minneapolis, Minnesota; Washington County, Maryland; Forsyth County, North Carolina, and Jackson, Mississippi). The baseline examination for this report extended from 1987 – 1989 and for this study, we included only non-Hispanic whites and excluded those with prevalent CVD. Among the remaining individuals, we analyzed the association of LIPG Asn396Ser genotype with incident fatal or non-fatal MI. The follow-up data in this study include events up to January 1, 2003. The incidence of MI was determined by contacting participants annually, by identifying hospitalizations and deaths during the previous year, and by surveying discharge lists from local hospitals and death certificates from state vital-statistics offices for potential cardiovascular events. The incidence of MI and plasma lipid measurements was determined as previously described.32 Copenhagen City Heart Study (CCHS): The Copenhagen City Heart Study is a prospective study of a cohort of >10,000 persons randomly selected from the population of the city of Copenhagen.6 The baseline examination for this report extended from 1991-1994 and we excluded all individuals all individuals with prevalent CVD at the baseline exam. Among the remaining individuals, we analyzed the association of LIPG Asn396Ser genotype with incident fatal or non-fatal MI. The follow-up data in this study include events up to January 1, 2009. The incidence of MI and plasma lipid measurements was determined as previously described.6 Danish Diet, Cancer, and Health Study (DCH): The Diet, Cancer and Health (DCH) study was initiated in 1993 when a total of 160,725 inhabitants of the greater Copenhagen or Aarhus areas who were born in Denmark and aged 50 to 64 years, were invited to participate. Eligible participants were without a record of cancer in the Danish Cancer Registry at the time of invitation. In total, 27,178 men and 29,875 women participated. Participants received a detailed FFQ by mail prior to the visit to the study clinic, where they also filled in a lifestyle questionnaire, and were asked to provide a blood sample. A detailed description of the cohort has been published previously.33 A case-cohort study was designed using incident acute coronary syndrome (ACS), including unstable angina pectoris, MI, and sudden cardiac death as the outcome.
Information on the disease endpoint was obtained by linkage with central Danish registries via the unique identification number assigned to all Danish citizens. Hospital records of potential cases were retrieved from hospitals for participants who were registered with a first-time discharge diagnosis of ACS (ICD-8 codes 410-410.99, 427.27 and ICD-10 codes I20.0, I21.x, I46.x) in The Danish National Register of Patients, which covers all hospital discharge diagnoses since 1977 and from 1995 all discharge diagnosis from out-patient clinics (until Jan 1, 2004). Cases were classified by three reviewers according to symptoms, signs, coronary biomarkers, ECGs and/or autopsy findings in accordance with the current recommendations of the American Heart Association and the European Society of Cardiology (AHA/ECS).34 Further, linkage to the Cause of Death Register allowed for identification of participants with ACS coded as a primary or secondary cause of death (to Jan 1, 2004). In total, for this report, 933 cases of MI were identified, however some of these were later excluded because of lacking questionnaire
10

data. For the creation of the cohort sample, 1588 participants were selected from the entire DCH study at random. Framingham Heart Study (FHS): Design and recruitment strategies for the Offspring cohort of the Framingham Heart Study have been described elsewhere.35 Since the initiation of the study in 1971, participants are seen in the FHS clinic every 4 to 8 years on average. Participants included in the current study (n=1,512) are from a subset of unrelated individuals from the Framingham offspring cohort who provided blood samples for DNA extraction at the sixth examination cycle. All participants underwent continuous surveillance for incident CVD events and death. A team of 3 physicians reviews all available information, hospitalization records and physician charts to adjudicate outcome events.36 We excluded all individuals with prevalent CVD at the sixth examination cycle. Follow-up for incident MI or fatal CHD (n=52) extended from the sixth examination cycle (considered baseline for this study) until December 31, 2007. Health Professionals Follow-up Study (HPFS): The HPFS was initiated in 1986 when 51,529 male health professionals between 40 and 75 years of age completed a food frequency questionnaire (FFQ) and a medical history questionnaire. The participants have been followed with repeated questionnaires on lifestyle and health every 2 years and FFQ's every 4 years. Blood samples were requested between 1993 and 1996 and obtained from 18,225 participants.37
For a nested case-control study, 426 incident nonfatal MI or fatal CHD cases that occurred between blood draw and January 31, 2004 were collected and ascertained. Cases of MI and fatal CHD were identified primarily through review of medical records. Participants who had reported an incident CHD on the follow-up questionnaire were contacted for confirmation and permission to review medical records was requested. Medical records for deceased participants were also sought for deaths that were identified by families and postal officials and through the National Death Index. Physicians blinded to the participant’s questionnaire reports reviewed all medical records. Malmo-Diet and Cancer Study (MDC): MDC is a community-based prospective epidemiologic cohort of 28,449 persons recruited for a baseline examination between 1991 and 1996.38 All participants underwent a medical history, a physical examination, and a laboratory assessment for cardiovascular risk factors. The final data with LIPG Asn396Ser genotype was available from 27,041 subjects. All participants gave written informed consent.
Cardiovascular events were ascertained through linkage of the 10-digit personal identification number of each Swedish citizen with three registries: the Swedish Hospital Discharge Register, the Swedish Cause of Death Register, and the Stroke Register of Malmö. The prespecified composite end point was defined as MI infarction and death from CHD. MI was defined on the basis of codes 410 and I21 in the International Classification of Diseases, 9th Revision and 10th Revision (ICD-9 and ICD-10), respectively. Death from CHD was defined on the basis of codes 412 and 414 (ICD-9) or I22–I23 and I25 (ICD-10) in the Swedish Cause of Death Register. Follow-up extended to December 31, 2003.
11

ACKNOWLEDGEMENTS
This manuscript is dedicated to Leena Peltonen, who passed away on March 11, 2010.
REGICOR. The REGICOR study was partially funded by the Ministerio de Ciencia y Tecnología, Instituto de Salud Carlos III / FEDER (Red Heracles RD06/0009; FIS PI09/90506, CIBERESP), Fundació Marató TV3 and AGAUR de Catalunya. Massachusetts General Hospital. The MIGen study was funded by the U.S. National Institutes of Health (NIH) and National Heart, Lung, and Blood Institute's STAMPEED genomics research program through a grant to D.A. S.K. was supported by a Doris Duke Charitable Foundation Clinical Scientist Development Award, a charitable gift from the Fannie E. Rippel Foundation, the Donovan Family Foundation, a career development award from the NIH, and institutional support from the Department of Medicine and Cardiovascular Research Center at Massachusetts General Hospital. C.N.-C. is supported by a Doris Duke Charitable Foundation Clinical Scientist Development Award, Burroughs Wellcome Fund and the NIH (HL080025 and HL098283). Broad Institute. Genotyping was partially funded by The Broad Institute Center for Genotyping and Analysis, which is supported by grant U54 RR020278 from the National Center for Research Resources. Heart Attack Risk in Puget Sound. The Heart Attack Risk in Puget Sound study was supported by the grants (R01HL056931, P30ES007033) and a contract (N01HD013107) from US National Institutes of Health. FINRISK. V.S. was supported by the Sigrid Juselius Foundation and by the Finnish Academy (grant number 129494). L.P. was supported by the Center of Excellence in Complex Disease Genetics of the Academy of Finland, the Nordic Center of Excellence in Disease Genetics and the Finnish Foundation for Cardiovascular Research. Italian Atherosclerosis, Thrombosis, and Vascular Biology Study. PMM was partially funded by grants from the Italian Ministry of Health (Progetto Finalizzato) and the Italian Ministry of Education and Research. WTCCC Study. The study was funded by the Wellcome Trust. Recruitment of cases for the WTCCC Study was carried out by the British Heart Foundation (BHF) Family Heart Study Research Group and supported by the BHF and the UK Medical Research Council. N.J.S. and S.G.B. hold Chairs funded by the BHF. N.J.S. is supported by the Leicester NIHR Biomedical Research Unit in Cardiovascular Diseases. PennCATH/MedStar. Recruitment of the PennCATH cohort was supported by the Cardiovascular Institute of the University of Pennsylvania. Recruitment of the MedStar cohort was supported by a research grant from GlaxoSmithKline and from the MedStar Research Institute. Genotyping was performed at the Center for Applied Genomics at the Children’s Hospital of Philadelphia and supported by GlaxoSmithKline through an Alternate Drug Discovery Initiative research alliance award (to M.P.R. and D.J.R.) with the University of
12

Pennsylvania School of Medicine. D.J.R. was supported by a Doris Duke Charitable Foundation Distinguished Clinical Scientist Award. Verona Heart Study. The study was supported by a grant from the Italian Ministry of University and Research and grants from the Veneto Region and the Cariverona Foundation, Verona, Italy. Mid-America Heart Institute. T.M. is supported by a career development grant from the NIH. Irish Family Study. We thank the clinical staff members for their valuable contribution to the collection of families for this study. The research was supported by the Northern Ireland Research and Development Office, a Royal Victoria Hospital Research Fellowship, the Northern Ireland Chest, Heart and Stroke Association, and the Heart Trust Fund (Royal Victoria Hospital). German MI Family Study I and II. The German Study was supported by the Deutsche Forschungsgemeinschaft and the German Federal Ministry of Education and Research in the context of the German National Genome Research Network and the EU funded integrated project LSHM-CT-2006-037593. University of Michigan. Support was provided in part by research grants HG005581, MH084698, and DK062370. Cardiogenics. Cardiogenics is an EU funded integrated project (LSHM-CT-2006-037593). INTERHEART. The INTERHEART genetics study was funded by multiple sources including a grant from the Heart and Stroke Foundation of Ontario NA 6336, the Population Health Research Institute, and the McGill University Genome Centre. Dr. Yusuf initiated and supervised the conduct of the main INTERHEART study, and obtained funding for the main study. We acknowledge the contributions of all INTERHEART investigators who worked tirelessly to maximize recruitment and ensure high quality data. We specifically thank members of the Project Office: S. Rangarajan (Study coordinator), Changchun Xie (Biostatistics) and K. Hall (Laboratory manager) for their assistance in coordinating the genetics component of the INTERHEART project. R.D. is a recipient of a Canada Graduate Scholarship Doctoral Award from the Canadian Institutes for Health Research. S.A. holds the Michael G. DeGroote and Heart and Stroke Foundation of Ontario Chair in Population Health and the May Cohen Eli Lilly Endowed Chair in Women's Health Research, McMaster University. Stockholm Heart Epidemiology Program (SHEEP). The current project from the SHEEP study was supported by the Swedish Research Council (09533), the Swedish Heart and Lung Foundation, and the Stockholm County Council (ALF). deCODE. The deCODE CAD/MI Study was sponsored by NIH grant, National Heart, Lung and Blood Institute R01HL089650-02. Atherosclerosis Risk in Communities Study. The Atherosclerosis Risk in Communities Study is carried out as a collaborative study supported by National Heart, Lung, and Blood Institute
13

contracts N01-HC-55015, N01-HC-55016, N01-HC-55018, N01-HC-55019, N01-HC-55020, N01-HC-55021, and N01-HC-55022. The genotyping of the endothelial lipase SNP was funded by the NHLBI Candidate Gene Association Resource (CARe) project. The authors thank the staff and participants of the ARIC study for their important contributions. Danish Diet, Cancer, and Health Study. The Diet, Cancer and Health (DCH) study was funded by the Danish Cancer Society. Research activities related to cardiovascular disease have been supported by the Danish Council for Independent Research (Medical Sciences). The Health Professionals Follow-Up Study (HPFS). HPFS was supported by AA11181, HL35464, and CA55075 from the National Institutes of Health, Bethesda, MD. Framingham Heart Study (FHS). This research was conducted in part using data and resources from the FHS of the National Heart Lung and Blood Institute of the National Institutes of Health and Boston University School of Medicine. The FHS is supported by a contract from the National Heart, Lung and Blood Institute (NHLBI; contract no. N01-HC-25195). J.M.O. is supported by NHLBI grant HL-54776 and by contracts 53-K06-5-10 and 58-1950-9-001 from the US Department of Agriculture Research Service. Utrecht Cardiovascular Pharmacogenetics (UCP) Studies. The UCP studies were funded by multiple sources including a grant from the Netherlands Heart Foundation 2001.064, NWO VENI grant nr. 916.66.029, Utrecht Institute for Pharmaceutical Sciences (UIPS), TI Pharma grant T6.101 Mondriaan, St Antonius Hospital Nieuwegein. EPIC-NL. The EPIC-NL study was funded by ‘Europe against Cancer’ Programme of the European Commission (SANCO), Dutch Ministry of Public Health, Welfare and Sports (VWS), Netherlands Cancer Registry (NKR), LK Research Funds, Dutch Prevention Funds, Dutch Cancer Society; ZonMW the Netherlands Organisation for Health Research and Development, World Cancer Research Fund (WCRF) (The Netherlands). Genotyping was funded by IOP Genomics grant IGE05012 from Agentschap NL. PROCARDIS. PROCARDIS is supported by the British Heart Foundation, the European Community Sixth Framework Program (LSHM-CT-2007-0372373), Astra Zeneca, The Wellcome Trust, the United Kingdom Medical Research Council, the Swedish Heart Lung Foundation, the Swedish Medial Research Council, the Knut and Alice Wallenberg Foundation, and the Karolinska Initutet. We also specifically thank Mark Lathrop, Rory Collins, Anders Hamsten, Udo Seedorf and Maria Grazia Franzosi as co-principal investigators in the PROCARDIS study; and Martin Farrall who is the chief statistician for their support in the study.
14

REFERENCES 1. Kathiresan S, Willer CJ, Peloso GM, et al. Common variants at 30 loci contribute to polygenic dyslipidemia. Nat Genet 2009;41:56-65. 2. Kathiresan S, Voight BF, Purcell S, et al. Genome-wide association of early-onset myocardial infarction with single nucleotide polymorphisms and copy number variants. Nat Genet 2009;41:334-41. 3. Keating BJ, Tischfield S, Murray SS, et al. Concept, design and implementation of a cardiovascular gene-centric 50 k SNP array for large-scale genomic association studies. PLoS One 2008;3:e3583. 4. Davis CE, Rifkind BM, Brenner H, Gordon DJ. A single cholesterol measurement underestimates the risk of coronary heart disease. An empirical example from the Lipid Research Clinics Mortality Follow-up Study. JAMA 1990;264:3044-6. 5. Clarke R, Shipley M, Lewington S, et al. Underestimation of risk associations due to regression dilution in long-term follow-up of prospective studies. Am J Epidemiol 1999;150:341-53. 6. Zacho J, Tybjaerg-Hansen A, Jensen JS, Grande P, Sillesen H, Nordestgaard BG. Genetically elevated C-reactive protein and ischemic vascular disease. N Engl J Med 2008;359:1897-908. 7. Ding EL, Song Y, Manson JE, et al. Sex hormone-binding globulin and risk of type 2 diabetes in women and men. N Engl J Med 2009;361:1152-63. 8. Palmer TM, Lawlor DA, Harbord RM, et al. Using multiple genetic variants as instrumental variables for modifiable risk factors. Stat Methods Med Res 2011 epub 1/11/11. 9. Teslovich TM, Musunuru K, Smith AV, et al. Biological, clinical and population relevance of 95 loci for blood lipids. Nature 2010;466:707-13. 10. Ehret GB, Munroe PB, Rice KM, et al. Genetic variants in novel pathways influence blood pressure and cardiovascular disease risk. Nature 2011; published online Sep 11. doi: 10.1038/nature10405. 11. Preuss M, Konig IR, Thompson JR, et al. Design of the Coronary ARtery DIsease Genome-Wide Replication And Meta-Analysis (CARDIoGRAM) Study: A Genome-wide association meta-analysis involving more than 22 000 cases and 60 000 controls. Circ Cardiovasc Genet 2010;3:475-83. 12. Schunkert H, Konig IR, Kathiresan S, et al. Large-scale association analysis identifies 13 new susceptibility loci for coronary artery disease. Nat Genet 2011;43:333-8. 13. Samani NJ, Erdmann J, Hall AS, et al. Genomewide association analysis of coronary artery disease. N Engl J Med 2007;357:443-53. 14. Reuterwall C, Hallqvist J, Ahlbom A, et al. Higher relative, but lower absolute risks of myocardial infarction in women than in men: analysis of some major risk factors in the SHEEP study. The SHEEP Study Group. J Intern Med 1999;246:161-74. 15. Samnegard A, Silveira A, Lundman P, et al. Serum matrix metalloproteinase-3 concentration is influenced by MMP-3 -1612 5A/6A promoter genotype and associated with myocardial infarction. J Intern Med 2005;258:411-9. 16. Berglund G, Elmstähl S, Janzon L, Larsson SA. The Malmo Diet and Cancer Study. Design and feasibility. J Intern Med 1993;233:45-51.
15

17. Persson M, Hedblad B, Nelson JJ, Berglund G. Elevated Lp-PLA2 levels add prognostic information to the metabolic syndrome on incidence of cardiovascular events among middle-aged nondiabetic subjects. Arterioscler Thromb Vasc Biol 2007;27:1411-6. 18. Kathiresan S, Melander O, Anevski D, et al. Polymorphisms associated with cholesterol and risk of cardiovascular events. N Engl J Med 2008;358:1240-9. 19. Langholz B, Goldstein L. Risk set sampling in epidemiologic cohort studies. Statist Sci 1996;11:35-53. 20. Rupprecht HJ, Blankenberg S, Bickel C, et al. Impact of viral and bacterial infectious burden on long-term prognosis in patients with coronary artery disease. Circulation 2001;104:25-31. 21. Tiret L, Godefroy T, Lubos E, et al. Genetic analysis of the interleukin-18 system highlights the role of the interleukin-18 gene in cardiovascular disease. Circulation 2005;112:643-50. 22. Erdmann J, Grosshennig A, Braund PS, et al. New susceptibility locus for coronary artery disease on chromosome 3q22.3. Nat Genet 2009;41:280-2. 23. Stewart AF, Dandona S, Chen L, et al. Kinesin family member 6 variant Trp719Arg does not associate with angiographically defined coronary artery disease in the Ottawa Heart Genomics Study. J Am Coll Cardiol 2009;53:1471-2. 24. Dandona S, Chen L, Fan M, et al. The transcription factor GATA-2 does not associate with angiographic coronary artery disease in the Ottawa Heart Genomics and Cleveland Clinic GeneBank Studies. Hum Genet;127:101-5. 25. Buysschaert I, Carruthers KF, Dunbar DR, et al. A variant at chromosome 9p21 is associated with recurrent myocardial infarction and cardiac death after acute coronary syndrome: The GRACE Genetics Study. Eur Heart J 2010;31: 1132-1341. 26. Buysschaert ID, Grulois V, Eloy P, et al. Genetic evidence for a role of IL33 in nasal polyposis. Allergy 2010;65: 616-22. 27. Clarke R, Peden JF, Hopewell JC, et al. Genetic variants associated with Lp(a) lipoprotein level and coronary disease. N Engl J Med 2009;361:2518-28. 28. Linsel-Nitschke P, Jansen H, Aherrarhou Z, et al. Macrophage cholesterol efflux correlates with lipoprotein subclass distribution and risk of obstructive coronary artery disease in patients undergoing coronary angiography. Lipids Health Dis 2009;8:14. 29. Wichmann HE, Gieger C, Illig T. KORA-gen--resource for population genetics, controls and a broad spectrum of disease phenotypes. Gesundheitswesen (Bundesverband der Arzte des Offentlichen Gesundheitsdienstes (Germany)) 2005;67 Suppl 1:S26-30. 30. Krawczak M, Nikolaus S, von Eberstein H, Croucher PJ, El Mokhtari NE, Schreiber S. PopGen: population-based recruitment of patients and controls for the analysis of complex genotype-phenotype relationships. Community Genet 2006;9:55-61. 31. Saleheen D, Alexander M, Rasheed A, et al. Association of the 9p21.3 locus with risk of first-ever myocardial infarction in Pakistanis: case-control study in South Asia and updated meta-analysis of Europeans. Arterioscler Thromb Vasc Biol 2010;30:1467-73. 32. Chambless LE, Folsom AR, Sharrett AR, et al. Coronary heart disease risk prediction in the Atherosclerosis Risk in Communities (ARIC) study. J Clin Epidemiol 2003;56:880-90. 33. Tjonneland A, Olsen A, Boll K, et al. Study design, exposure variables, and socioeconomic determinants of participation in Diet, Cancer and Health: a population-based prospective cohort study of 57,053 men and women in Denmark. Scand J Public Health 2007;35:432-41.
16

34. Luepker RV, Apple FS, Christenson RH, et al. Case definitions for acute coronary heart disease in epidemiology and clinical research studies: a statement from the AHA Council on Epidemiology and Prevention; AHA Statistics Committee; World Heart Federation Council on Epidemiology and Prevention; the European Society of Cardiology Working Group on Epidemiology and Prevention; Centers for Disease Control and Prevention; and the National Heart, Lung, and Blood Institute. Circulation 2003;108:2543-9. 35. Kannel WB, Feinleib M, McNamara PM, Garrison RJ, Castelli WP. An investigation of coronary heart disease in families. The Framingham offspring study. Am J Epidemiol 1979;110:281-90. 36. Wang TJ, Gona P, Larson MG, et al. Multiple biomarkers for the prediction of first major cardiovascular events and death. N Engl J Med 2006;355:2631-9. 37. Chu NF, Spiegelman D, Yu J, Rifai N, Hotamisligil GS, Rimm EB. Plasma leptin concentrations and four-year weight gain among US men. Int J Obes Relat Metab Disord 2001;25:346-53. 38. Berglund G, Elmstahl S, Janzon L, Larsson SA. The Malmo Diet and Cancer Study. Design and feasibility. J Intern Med 1993;233:45-51.
17

Supplementary Table 1. Characteristics of Cases with Myocardial Infarction and Controls Free of Myocardial Infarction*
Study Italian ATVB Study Heart Attack Risk in Puget Sound REGICOR MGH Premature Coronary
Artery Disease Study FINRISK Malmö Diet and
Cancer Study Early-Onset MI
cases Controls cases controls cases controls cases controls Cases controls cases controls N 1,693 1,668 505 559 312 317 204 260 167 172 86 99
MI age criterion men or women ≤ 45 -- men ≤50 or
women ≤ 60 -- men ≤50 or women ≤ 60 -- men ≤50 or
women ≤ 60 -- men ≤50 or women ≤ 60 -- men ≤50 or
women ≤ 60 --
Genotyping platform Affymetrix 6.0
Affymetrix 6.0
Affymetrix 6.0
Affymetrix 6.0
Affymetrix 6.0
Affymetrix 6.0
Affymetrix 6.0
Affymetrix 6.0
Affymetrix 6.0
Affymetrix 6.0
Affymetrix 6.0
Affymetrix 6.0
Country of origin Italy Italy U.S. U.S. Spain Spain U.S. U.S. Finland Finland Sweden Sweden
Mean age (y) † 39.4 ± 4.9 39.3 ± 5.0 46.0 ± 6.9 45.2 ± 7.3 45.9 ± 5.8 46.0 ± 5.6 47.0 ± 6.1 53.8 ± 11.1 47.1 ± 6.2 47.1 ± 6.0 48.5 ± 4.4 48.7 ± 4.6
Female gender (%) 11.4 11.6 51.1 55.5 20.2 21.5 29.9 33.5 33.5 31.4 41.9 42.4
Study WTCCC MI German MI Family Study I
German MI Family Study II PennCATH deCODE MedSTAR
cases controls cases controls cases controls cases controls Cases controls cases controls N 1,561 2,938 875 1,644 1,222 1,874 415 468 729 29,218 420 447
MI age criterion <66 years -- men ≤60 or women ≤ 65
-- men ≤60 or women ≤ 65
-- <66 years -- men<50 or women <60 -- <66 years --
Genotyping platform Affymetrix 500K
Affymetrix 500K
Affymetrix 500K
Affymetrix 500K
Affymetrix 6.0
Affymetrix 6.0
Affymetrix 6.0
Affymetrix 6.0
Illumina 300/370K
Illumina 300/370K
Affymetrix 6.0
Affymetrix 6.0
Country of origin U.K. U.K. Germany Germany Germany Germany U.S. U.S. Iceland Iceland U.S. U.S.
Mean age (y) † 49.3±7.9 44.7±9.3 50.2±7.9 62.5±10.1 51.3 ± 7.6 51.2±11.9 50.2±7.5 61.7 ± 9.6 56.7 ± 10.6 48.9 ± 21.6 46.8±6.8 59.7 ± 8.9
Female gender (%) 20.2 49.2 32.5 50.5 20.3 47.9 17.6 51.7 40.8 61.3 23.8 48.8
Study Verona Heart Study Mid-America Heart Institute Irish Family Study INTERHEART European Ancestry
AMI Gene Study / Dortmund Health Study SHEEP
cases controls cases controls cases controls cases controls Cases controls cases controls N 510 388 811 650 577 719 1,886 2,231 809 1,132 1,155 1,502
MI age criterion men ≤65 or women ≤ 65
-- no age criterion -- men ≤55 or
women ≤ 65 -- no age
criterion -- men <65 -- men and women 46-70 --
Genotyping platform Sequenom Sequenom Sequenom Sequenom Sequenom Sequenom Sequenom Sequenom Sequenom Sequenom Sequenom Sequenom
Country of origin Italy Italy U.S. U.S. Northern Ireland
Northern Ireland
U.S. and multiple in
Europe
U.S. and multiple in
Europe Germany Germany Sweden Sweden
Mean age (y) † 57.0±9.1 58.9±12.1 61.5±12.7 60.7±12.4 45.9±6.7 55.7±8.0 61.2±12.1 60.5±12.0 52.2±8.2 52.6±13.7 59.2±7.2 59.8±7.1
Female gender (%) 10.6 34.8 32.1 39.0 20.1 55.2 28.9 31.3 0 53.1 29.4 32.2
Study Malmö Diet and
Cancer Study Later-Onset MI
COROGENE CADomics Ottawa Heart Genomics Study I
Ottawa Heart Genomics Study II GRACE Genetics
cases controls cases controls cases controls cases controls Cases controls cases controls N 1,059 1,056 2,172 1,579 1,212 2,952 950 1,455 1,090 933 683 656
MI age criterion Men >50 or women >60 -- no age
criterion no age criterion -- men ≤55 or
women ≤ 65 --- men ≤55 or
women ≤ 65 --- no age
criterion
Genotyping platform Sequenom Sequenom Illumina Illumina Affymetrix 6.0
Affymetrix 6.0
Affymetrix 500K&6.0
Affymetrix 500K&6.0
Affymetrix 6.0
Affymetrix 6.0 Sequenom Sequenom
Country of origin Sweden Sweden Finland Finland Germany Germany Canada Canada Canada / U.S
Canada / U.S Belgium Belgium
Mean age (y) † 63.7 ± 5.9 63.7 ± 5.9 66.1 ± 12.0 55.7 ± 12.2 59.3 ± 10.8 55.3 ± 10.8 47.7±7.3 75.0±5.0 47.8±7.1 74.3±5.8 65.2±11.8 41.0±13.2
18

Female gender (%) 21.4 42.6 30.8 45.5 20.5 50.5 20.8 48.0 20.9 50.3 24.4 43.3
Study PROCARDIS UCP EPIC-NL AngioGOCARD/KORA PopGen PROMIS cases controls cases controls cases controls cases controls Cases controls cases controls N 2,183 3,347 830 1,139 334 1,827 1,953 1,482 2,433 1,687 1854 1897 MI age criterion <66 years <66 years None None None None 30-65 35-84 34-88 20-68 None None
Genotyping platform Illumina CVD chip
Illumina CVD chip
Illumina CVD chip
Illumina CVD chip
Illumina CVD chip
Illumina CVD chip Sequenom Sequenom Sequenom Sequenom Illumina CVD
chip Illumina
CVD chip Country of origin Europe Europe Netherlands Netherlands Netherlands Netherlands Germany Germany Germany Germany Pakistan Pakistan
Mean age (y) † 52.9 ± 7.7 59.4 ± 9.9 63.7 ± 10.3 62.7 ± 10.7 54.9 ± 9.2 49.0 ± 12.1 55.1 ± 6.9 52.2 ± 13.3 61.2 ± 8.2 51.2 ± 14.4 54.5 ± 10.9 52.1 ± 10.3
Female gender (%) 25.3 50.9 26.4 32.5 58.8 72.2 19.1 52.1 18.9 0.0 16.0 19.0 Values with ‘±’ are means ± s.d. *Summary characteristics are provided for maximal number of available subjects. For any given genotype, a subset may have been studied. †Mean age at MI for cases and age at recruitment for controls.
19

Supplementary Table 2. Characteristics of Participants from Prospective Cohort Studies by Myocardial Infarction Status
Prospective cohort ARIC CCHS DCH FHS HPFS MDCS*
MI status No event MI No event MI No event MI No event MI No event MI No event MI No. of individuals (%)
8,214 (93%)
558 (7%)
8,964 (93%)
655 (7%)
1,588 (63%)
933 (37%)
1,462 (97%)
50 (3%)
869 (67%)
426 (33%)
25,438 (94%)
1,606 (6%)
Women, % 56 38 58 45 38 62 53 42 0 0 63 35 Age, years 54 ± 0.1 56 ± 0.2 55 ± 0.2 66 ± 0.4 56 ± 0.1 58 ± 0.1 58 ± 0.2 63 ± 1.2 64 ± 0.3 64 ± 0.4 58 ± 0.1 62 ± 0.2 Total cholesterol, mmol/L
5.5 ± 0.01 5.8 ± 0.04 6.0 ± 0.01 6.6 ± 0.05 6.0 ± 0.03 6.4 ± 0.04 5.4 ± 0.03 5.6 ± 0.15 5.3 ± 0.03 5.5 ± 0.05 6.2 ± 0.02 6.3 ± 0.06
LDL-C, mmol/L 3.5 ± 0.01 3.9 ± 0.04 3.6 ± 0.01 4.2 ± 0.05 3.6 ± 0.02 3.9 ± 0.04 3.3 ± 0.02 3.5 ± 0.13 3.3 ± 0.03 3.5 ± 0.04 4.2 ± 0.01 4.4 ± 0.06
HDL-C, mmol/L 1.3 ± 0.01 1.1 ± 0.01 1.6 ± 0.01 1.4 ± 0.02 1.6 ± 0.01 1.4 ± 0.01 1.3 ± 0.01 1.1 ± 0.04 1.9 ± 0.01 1.1 ± 0.01 1.4 ± 0.01 1.2 ± 0.02
TG, mmol/L 1.5 ± 0.01 1.9 ± 0.06 1.8 ± 0.01 2.2 ± 0.06 1.8 ± 0.03 2.3 ± 0.04 1.7 ± 0.03 2.1 ± 0.22 1.6 ± 0.04 1.9 ± 0.05 1.4 ± 0.01 1.6 ± 0.06
Body mass index, kg/m2 27 ± 0.05 28 ± 0.2 25 ±0.05 27 ± 0.2 26 ± 0.13 27 ± 0.13 28 ± 0.13 28 ± 0.75 26 ± 0.1 26 ± 0.2 26 ± 0.03 27 ± 0.1
Genotyping method for LIPG Asn396Ser
Illumina CVD Chip Taqman Taqman Taqman Taqman Taqman
ARIC, Atherosclerosis Risk in Communities Study; CCHS, Copenhagen City Heart Study; DCH, Danish Diet, Cancer, and Health Study; FHS, Framingham Heart Study; HPFS, Health Professionals Follow-up Study; MDCS, Malmö Diet and Cancer Study All continuous traits are given as means ± SEM. All categorical variables are shown in percentages. *Lipid traits were available for 5,042-5,173 MDCS study participants.
20

Supplementary Table 3. Association of LIPG Asn396Ser with Plasma High-Density Lipoprotein Cholesterol in Four Prospective Cohort Studies
ARIC CCHS FHS MDCS-CC Meta-analysis across 4 studies N total 8,735 9,618 1,589 5,127 25,069 Number of 396Ser mutation carriers
225 232 43 133 633
Beta* 0.33 0.15 0.49 0.39 0.29 SE 0.07 0.07 0.16 0.09 0.04 P 7 x 10-7 0.02 0.002 1 x 10-5 8 x 10-13
ARIC, Atherosclerosis Risk in Communities Study; CCHS, Copenhagen City Heart Study; FHS, Framingham Heart Study; MDCS-CC, Malmö Diet and Cancer Study-Cardiovascular Cohort In each study, association results are from a linear regression model with a predictor variable of the LIPG 396Ser allele. The outcome variable was plasma high-density lipoprotein cholesterol residual after adjustment for age and gender and standardized to a mean of 0 and SD of 1. *Beta represents increment change in standard deviation units for each copy of the LIPG 396Ser allele.
21

Supplementary Table 4. Association of Plasma Lipid Level and Incident Myocardial Infarction in Four Prospective Cohort Studies
Predictor Covariate OR per
SD increase in plasma lipid level
95% CI
Atherosclerosis Risk in Communities Study
LDL cholesterol Age, gender, HDL-C, TG 1.65 1.48 - 1.85 HDL cholesterol Age, gender, LDL-C, TG 0.56 0.51 – 0.62 Triglycerides Age, gender, HDL-C, LDL-C 1.40 1.20 - 1.62
Copenhagen City Heart Study
LDL cholesterol Age, gender, HDL-C, TG 1.61 1.40 - 1.85 HDL cholesterol Age, gender, LDL-C, TG 0.74 0.64 – 0.85 Triglycerides Age, gender, HDL-C, LDL-C 1.31 1.11 - 1.55
Framingham Heart Study
LDL cholesterol Age, gender, HDL-C, TG 1.64 1.48 - 1.82 HDL cholesterol Age, gender, LDL-C, TG 0.71 0.61 – 0.82 Triglycerides Age, gender, HDL-C, LDL-C 1.88 1.65 – 2.13
Malmo Diet and Cancer Study – Cardiovascular Cohort
LDL cholesterol Age, gender, HDL-C, TG 1.23 1.11 - 1.35 HDL cholesterol Age, gender, LDL-C, TG 0.55 0.46 – 0.66 Triglycerides Age, gender, HDL-C, LDL-C 1.01 0.86 - 1.18
Meta-analysis of Four Cohort Studies
LDL cholesterol Age, gender, HDL-C, TG 1.54 1.45 - 1.63 HDL cholesterol Age, gender, LDL-C, TG 0.62 0.58 – 0.66 Triglycerides Age, gender, HDL-C, LDL-C 1.42 1.31 - 1.52
The four prospective cohort studies were: 1) ARIC, Atherosclerosis Risk in Communities Study; 2) CCHS, Copenhagen City Heart Study; 3) FHS, Framingham Heart Study; and 4) MDCS-CC, Malmö Diet and Cancer Study-Cardiovascular Cohort. In each study for each trait, the odds ratio estimates were adjusted for regression dilution bias using a parametric approach. The test-retest correlations for LDL-C, HDL-C, and TG were the following: ARIC (0.55, 0.72, and 0.56); CCHS (0.60, 0.73, and 0.58); and Framingham Heart Study (0.72, 0.72, and 0.56).
22

Supplementary Table 5. Characteristics of Participants from Prospective Cohort Studies by LIPG 396Ser Carrier Status
Prospective cohort ARIC CCHS DCH FHS HPFS MDCS-CC
LIPG 396Ser carrier status No Yes No Yes No Yes No Yes No Yes No Yes
No. of individuals (%)
8,510 (97.4)
225 (2.6)
9,387 (97.6)
232 (2.4)
2,458 (97.5)
63 (2.5)
6128 (97.4)
161 (2.6)
1255 (98.2)
23 (1.8)
5568 (97.4)
148 (2.6)
Women, % 55 55 57 53 38 37 55 56 0 0 58 58 Age, years 54.2 ± 0.1 54.3 ± 0.4 55.4 ± 0.2 58.0 ± 1.0 57.1 ± 0.1 56.2 ± 0.5 46.9 ± 0.2 47.6 ± 1.0 64.2 ± 0.2 64.0 ± 1.9 57.4 ± 0.1 57.8 ± 0.5 Total cholesterol, mmol/L
5.54 ± 0.01 5.76 ± 0.07 6.02 ± 0.01 6.27 ± 0.08 6.15 ± 0.02 6.11 ± 0.13 5.13 ± 0.01 5.41 ± 0.08 5.32 ± 0.03 5.32 ± 0.18 6.17 ± 0.02 6.39 ± 0.10
LDL-C, mmol/L 3.54 ± 0.01 3.62 ± 0.06 3.67 ± 0.01 3.74 ± 0.07 3.71 ± 0.02 3.59 ± 0.12 2.92 ± 0.01 3.04 ± 0.10 3.34 ± 0.02 3.41 ± 0.14 4.17 ± 0.01 4.22 ± 0.09
HDL-C, mmol/L 1.32 ± 0.01 1.46 ± 0.03 1.57 ± 0.01 1.65 ± 0.04 1.54 ± 0.01 1.58 ± 0.05 1.38 ± 0.01 1.52 ± 0.04 1.16 ± 0.01 1.19 ± 0.09 1.38 ± 0.005 1.52 ± 0.04
TG, mmol/L 1.53 ± 0.01 1.51 ± 0.06 1.79 ± 0.01 1.93 ± 0.08 1.98 ± 0.02 2.06 ± 0.13 3.41 ± 0.03 3.38 ± 0.20 1.70 ± 0.03 1.60 ± 0.19 1.37 ± 0.01 1.37 ± 0.06
Body mass index, kg/m2 27.29 ± 0.33 26.95 ± 0.05 25 ± 0.04 26 ± 0.3 27 ± 0.1 26 ± 0.5 27 ± 0.07 27 ± 0.5 26 ± 0.1 26 ± 0.6 26 ± 0.1 25 ± 0.3
Systolic blood pressure, mm/Hg
118.26 ± 0.18 118.69 ± 1.12 137 ± 0.2 141 ± 2 143 ± 0.4 143 ± 2 123 ± 0.3 126 ± 1.8 NA NA 141 ± 0.3 141 ± 2
Fasting glucose, mg/dl 103.69 ± 0.29 102.22 ± 1.52 104 ± 0.4 105 ± 2 NA NA 98 ± 0.5 99 ± 3 NA NA 93 ± 0.3 93 ± 2
Active cigarette smoking, % 24 19 47 53 45 52 15 19 9 9 28 26
Type 2 diabetes, % 6 7 7 8 3 0 4 3 5 3 3 2
ARIC, Atherosclerosis Risk in Communities Study; CCHS, Copenhagen City Heart Study; DCH, Danish Diet, Cancer, and Health Study; FHS, Framingham Heart Study; HPFS, Health Professionals Follow-up Study; MDCS, Malmö Diet and Cancer Study All continuous traits are given as means ± SEM. All categorical variables are shown in percentages.
23

Supplementary Table 6. Association of LIPG Asn396Ser with Plasma Low-Density Lipoprotein Cholesterol or Triglycerides in Four Prospective Cohort Studies N Beta SE P Low-density lipoprotein cholesterol ARIC 8,588 0.024 0.019 0.21 CCHS 9,618 0.006 0.021 0.77 FHS 1,589 0.013 0.041 0.75 MDCS-CC 5,045 0.031 0.089 0.73 Meta-analysis 24,840 0.016 0.013 0.23 Triglycerides ARIC 8,720 -0.018 0.033 0.60 CCHS 9,618 0.062 0.035 0.07 FHS 1,589 -0.016 0.091 0.86 MDCS-CC 5,175 0.001 0.088 0.99 Meta-analysis 25,012 0.016 0.02 0.47
The four prospective cohort studies were: 1) ARIC, Atherosclerosis Risk in Communities Study; 2) CCHS, Copenhagen City Heart Study; 3) FHS, Framingham Heart Study; and 4) MDCS-CC, Malmö Diet and Cancer Study-Cardiovascular Cohort
24

Supplementary Table 7. Association of LIPG Asn396Ser with Cardiovascular Risk Factors in the Malmo Diet and Cancer Study. Risk factor N Beta SE P Systolic blood pressure
27,868 -0.80 0.69 0.24
Body mass index 27,863 -0.19 0.15 0.20 Type 2 diabetes 2,452 cases, 23,326
non-cases -0.05 0.13 0.70
C-reactive protein 5,110 -0.55 0.40 0.17 Small LDL particle concentration
4,466 -0.07 0.09 0.47
Linear regression modeling was utilized to test the association of LIPG Asn396Ser with systolic blood pressure, body mass index, C-reactive protein or small LDL particle concentration. In these models, the predictor variable was the quantitative risk factor, the predictor variable was number of copies of the LIPG 396Ser allele, and covariates of age and gender. For type 2 diabetes, logistic regression modeling was utilized. *Small LDL particle concentration measured by airborne ion mobility assay.
25

1
Supplementary Table 8. Association of LIPG Asn396Ser with a range of cardiovascular phenotypes in the Atherosclerosis Risk in Communities (ARIC) Study
Phenotype Beta SE N P HDL cholesterol 5.41 1.01 8,720 9.6 x 10-8
apo-AI 8.63 1.93 8,720 7.9 x 10-6 LDL cholesterol 2.98 2.53 8,588 0.24
apoB 1.00 1.86 8,719 0.59 Lp(a) -4.18 6.27 8,576 0.50
Log triglycerides -0.02 0.03 8,720 0.53 Systolic blood pressure 0.28 1.09 8,734 0.26 Diastolic blood pressure 0.75 0.66 8,734 0.26
Fasting glucose -1.57 1.78 8,731 0.38 Type 2 diabetes 0.003 0.02 8,731 0.89
Cigarette smoking -0.055 0.03 8,731 0.06 Waist/hip ratio -0.0003 0.005 8,727 0.95
Fibrinogen 0.91 4.06 8,704 0.82 Log C-reactive protein -0.05 0.08 7,032 0.51
Genotypes were coded as Serine allele carrier or non-carrier. Linear or logistic regression was performed with outcome variable being phenotype in column 1, predictor variable of Serine allele carrier status, and covariates of age and gender. Betas are unstandardized and in original units for phenotype except for triglycerides and C-reactive protein where these phenotypes were log-transformed.
26

Supplementary Table 9. Evaluation of an LDL genetic score for association with myocardial infarction Data from Global Lipid Genetic
Consortium GWAS for Lipids Data from CARDIOGRAM
GWAS for MI
Marker Effect Allele
Other Allele Effect* SD P Effect SD P
rs11136341 G A 0.041 0.006 6.20E-11 -0.032 0.030 0.310 rs11220462 A G 0.057 0.008 1.88E-14 0.040 0.029 0.555 rs1169288 C A 0.042 0.005 2.21E-14 0.084 0.019 7.55E-05 rs12027135 T A 0.032 0.005 5.61E-10 -0.001 0.018 0.869
rs12916 C T 0.072 0.005 2.46E-41 0.0238 0.019 0.225 rs1800562 G A 0.065 0.011 1.39E-08 0.016 0.037 0.674 rs217386 G A 0.034 0.005 2.86E-10 0.029 0.019 0.125 rs2332328 T C 0.034 0.006 6.75E-10 0.001 0.027 0.933 rs3757354 C T 0.042 0.006 2.34E-11 0.025 0.026 0.339 rs514230 T A 0.033 0.005 5.99E-10 0.009 0.018 0.894 rs649129 T C 0.060 0.006 1.03E-21 0.119 0.024 6.17E-05 rs6511720 G T 0.206 0.009 1.03E-117 0.176 0.046 2.37E-04 rs7225700 C T 0.026 0.005 1.53E-06 0.030 0.019 0.194
The beta coefficient for association of LDL genetic score with MI was 0.756, SE of 0.119 and P= 1.8 x 10-10
*Effect is in standard deviation units
27

Supplementary Table 10. Evaluation of an HDL genetic score for association with myocardial infarction Data from Global Lipid Genetic
Consortium GWAS for Lipids Data from CARDIOGRAM
GWAS for MI
Marker Effect Allele
Other Allele Effect* SD P Effect SD P
rs13107325 C T 0.056 0.011 2.22E-07 0.004 0.053 0.912 rs1689800 A G 0.031 0.005 1.43E-09 -0.020 0.019 0.334 rs16942887 A G 0.085 0.007 8.62E-29 -0.038 0.028 0.125 rs181362 C T 0.031 0.006 7.10E-07 -0.004 0.022 0.846 rs2293889 G T 0.029 0.005 1.18E-08 0.038 0.018 0.040 rs2923084 A G 0.027 0.006 3.21E-05 0.015 0.023 0.382 rs386000 C G 0.055 0.007 2.92E-13 0.007 0.028 0.760 rs4082919 T G 0.027 0.005 2.57E-07 0.005 0.019 0.667 rs4759375 T C 0.057 0.011 6.30E-08 -0.013 0.038 0.548 rs7134594 T C 0.030 0.005 1.26E-09 0.005 0.018 0.844 rs7255436 A C 0.030 0.005 2.70E-08 -0.024 0.022 0.322 rs737337 T C 0.043 0.009 3.48E-06 -0.036 0.035 0.358 rs838880 C T 0.040 0.006 1.18E-11 0.008 0.023 0.825 rs881844 G C 0.034 0.005 2.87E-11 0.001 0.019 0.772
The beta coefficient for association of HDL genetic score with MI was -0.077, SE of 0.159 and P= 0.63 *Effect is in standard deviation units
28