Embed Size (px)
Citation preview

A PRACTICE CHANGE TO ELIMINATE PROPHYLACTIC ANTIBIOTICS 1Appendix A: Evidence Table
Brief reference, type of study, quality rating
Methods Threats to Reliability/Validity
Study findings Conclusions
Cronan, J. J., Horn, H. L., Marcello, A., et al. (1989). Antibiotics and Nephrostomy Tube Care: preliminary observations. Part II: bacteremia. Radiology. 172: 1043–1045.
Type: RCT
Quality: Level IB
An RCT study of 104 nephrostomy tube changes in 74 patients
Patients were arbitrarily divided into groups receiving and not receiving antibiotics before nephrostomy tube exchange
assessed the occurrence of bacteriuria and pyuria
Unclear parameters regarding their definition of sepsis vs. shock, etc.
Asymptomatic bacteremia was documented in 11 of 104 tube changes (11%)
Results of five blood cultures were positive in the group receiving antibiotics, and six cases of bacteremia occurred in the group not receiving antibiotics (P = .96).
The incidence was similar in patients receiving pre-procedural antibiotics compared with those who did not.
The genitourinary tract is regarded as contaminated in the presence of the following risk factors: age, diabetes, bladder dysfunction, indwelling catheter, prior manipulation, uretero-intestinal anastomosis, or bacteriuria.
Routine nephrostomy/stent change can cause frequent, asymptomatic bacteremia in patients with colonization of bacteria in the urinary tract. Antibiotic prophylaxis was unsuccessful in preventing transient bacteremia, a factor that may have implications in patients with underlying valvular heart disease and other patients at risk for bacteremia.
Siddiq, D. M. & Dairouche,R. O. (2012). Infectious complications associated with percutaneous nephrostomy catheters: Do we know enough? International journal of artificial organs. 35 (10): 898-907.Type: Systematic Review of RCTs (13 studies)
Quality: Level IB
Systematic review of randomized control trials r/t PCNCs (percutaneous nephrostomy catheters i.e. PCN) – 13 studies total
Prevention and management of infectious complications associated with PCNCs suffer from the absence of evidence.
Relevant recommendations are based on work done in the late 1980s and early 1990s
no standardized definitions or criteria to define the various infectious complications described in this paper
Current reported rates of acute infectious complications are relatively low and there are no standard definitions for what constitutes an infection short of sepsis. The device is mostly exchanged in patients with an irreparable or terminal illness, so studying the infection statistically becomes an elaborate exercise in statistical modeling and repeated events analysis.
The current practice of preventing infectious complications associated with
Randomized, placebo-controlled, clinical trials need to be performed just as there have been multiple ones for PCNL.
Continued dependency on evidence gathered from research on bladder catheters.
Ways to decrease infection: give abx when appropriate, no PCN flushing, exchange PCN q3 months, clean site appropriately, ensure providers use PPE/handwashing prior to handling, etc.

A PRACTICE CHANGE TO ELIMINATE PROPHYLACTIC ANTIBIOTICS 2Brief reference, type of study,
quality ratingMethods Threats to
Reliability/ValidityStudy findings Conclusions
evidence r/t abx practice is poor and is extrapolated from non-randomized studies and case series
PCNCs appears to be based on data with important confounders like underlying stone disease and pre-existing urinary tract infection.
McDermott, V., Schuster, M., Smith, P. (1997). Prophylactic Antibiotic Prophylaxis in Vascular and Interventional Radiology. Journal of Roentgenology. 169.
Type: Systematic review of a combination of RCTs
Quality Rating: Level IIA
Systematic review of relevant studies to provide evidence based practice on antibiotic prophylaxis for IR procedures
Minimal studies provided to support statements, outdated studies from late 1980s.
The presence of stones, especially struvite stones, is a big risk factor for infection. The genitourinary tract is regarded as dirty if clinical infection is present
Septic shock has been reported in as many as 7% of patients undergoing nephrostomy drainage for pyonephrosis.
In the absence of infection, providing antibiotic prophylaxis for routine tube changes is not necessary once drainage is adequate and the patient is not immunosuppressed.
Since the late 80s, relatively little work was done on specific prophylactic regimes for interventional procedures, but use of surgical data has enabled the development of a practical approach that has limited infection risk. Regular review of local practice is indicated, because the field is not static and resistant bacterial strains can develop and flourish rapidly, standard regimes will be at risk of not working.
Cochran, S. T., Lee, J. J., & Kashfian, P. (1991). Nephrostomy tube placement: an outpatient procedure? Radiology. 179. 843– 847.
Type: RCT
Quality Level IIB
Patients with none of the risk factors (diabetes, obstruction, infection) were not given prophylaxis, high risk patients were given prophylaxis perioperatively.
Small sample size of low risk patients (n=24), No clear guideline supporting the high risk factors implemented by the MDs.
No statistically significant difference in low risk patients who did or did not receive antibiotics.
Considered landmark study by SIR, contributed to guideline policy issued in 2010 saying it’s not required to hang antibiotic for low risk patients undergoing routine PCN exchange
Montvilas, P. Solvig, J., & Truls, E. B. J. (2011). Single-center review of radiologically
A review of complication and success rates of the “mixed” technique (the Seldinger and
Study was related more to placement methods rather than antibiotics, but
Of 460 PCN placements, two patients did not receive prophylactic antibiotics, both
The total rate of minor complications was 14.2%

A PRACTICE CHANGE TO ELIMINATE PROPHYLACTIC ANTIBIOTICS 3Brief reference, type of study,
quality ratingMethods Threats to
Reliability/ValidityStudy findings Conclusions
guided percutaneous nephrostomy using “mixed” technique: Success and complication rates. European Journal of Radiology. 80(2). 553-558.
Type: non-experimental study
Quality Rating: IIIB
one step technique) in dilated and non-dilated systems
infection rates and abx were recorded.Retrospective data included emergent and elective PCN procedures
Many studies report sepsis as a major complication in 0.7–3.6%, but difficult to compare rates of infectious complications of PCN in different studies, this is because varying definitions are used for septicemia, post-interventional fever, sepsis and septic shock.
were recorded as positive for having mild post PCN placement sepsis, of all patients studied, 1.95% had a mild post PCN placement sepsis
Percutaneous nephrostomy considered successful in study if catheter was placed in renal pelvis and drained urine spontaneously.
None of the post PCN infections met the study’s criteria for severe sepsis or septic shock.
There was no mortality related to PCN placement.
No statistically significant difference in complications with mixed technique compared to placement methods
Matsumoto, M., Shigemura, K., Yamamichi, F., Tanaka, K. Nakano, Y., Arakawa, S. Fujisawa, M. (2012). Prevention of infectious complication and its risk factors after urological procedures of the upper urinary tract. Urologia Internationalis. 88. 43-47.Type: non-experimental study, retrospective
Quality: Level IIIB
Levofloxacin was used in 149 subjects (42.2%) and cefcapene pivoxil in 114 cases (32.3%), of single J and double J stent placements.
A febrile/ infectious complication was defined in this study as a positive infection with a fever >38°C , occurring within 30 days of follow-up.
Data did not provide which patients received what procedure (elective vs. emergent), what antibiotic they received, comorbidities, and complications, they state that these risk factors were reviewed but methodology otherwise not provided.
There were 16 febrile infectious complication cases (4.5%) after procedures, and pyuria or hydronephrosis prior to examination or treatment was an independent risk factor for infectious complication (p < 0.05) as well.
This study investigated infectious complications and risk factors, focusing on prophylactic antimicrobial administration, which they concluded may be necessary.
3.4% febrile infection rate after D-J or S-J stent insertion or exchange
Researchers concluded that prior to undergoing upper urinary tract procedures, they need to better evaluate the risk factors and that more definitive methodology is necessary, to better establish/update the guidelines. Antibiotic prophylaxis did not prevent stent colonization and it should not be given routinely.Regarding ureteral stents, antibiotics should be restricted to patients with clinical signs of infection and to high-risk patients
Venkatesan, A. M. et al. Evidence summary from SIR SIR’s guidelines on Consensus on PCN relevant PCN placement is to be considered a

A PRACTICE CHANGE TO ELIMINATE PROPHYLACTIC ANTIBIOTICS 4Brief reference, type of study,
quality ratingMethods Threats to
Reliability/ValidityStudy findings Conclusions
(2010). Practice Guideline for Adult Antibiotic Prophylaxis during Vascular and Interventional Radiology Procedures. Journal of Vascular Interventional Radiology.
Type of study: Clinical practice guidelines
Quality: Level IVA
Standards of Practice Committee members,
literature search of study methodology, results, and conclusions
qualitative weight of these articles was assembled into an evidence table
antibiotics based on percutaneous nephrostomy tube placement results from (PCN) two studies done in 1989 and 1990.
guidelines: data shows no statistical significance in infection rates when prophylactic antibiotics are hung vs not hung prior to nephrostomy tube change.
clean contaminated procedure, recommend traditional antibiotic prophylaxis unless it is a routine PCN exchange in an uninfected patient, patients with underlying renal collecting system infection and stone disease should be considered separately from the population of patients whose PCNC is placed for another indication.
Murtha, J., Kanna, V., Sasson, T., & Butani, D. (2017). Identification and Management of Sepsis in the Interventional Radiology Patient. American Journal of Interventional Radiology. 1(3). 1-7. Type: literature review
Quality: Level V
Summary of RCTs, review of current guidelines provided by the literature
Lack of recent evidence re: PCN exchanges, no recent evidence provided since the early nineties, policy created based on three landmark studies from the late 89s/early 90s
No new evidence re: PCN exchanges since early 90s
More research needed related to prophylactic antibiotic administration in IR procedures
Huang, S. Y., Asher, P., Richter, M. D., Gupta, S., Lessne, M. L. & Kim, C. Y. (2015). Prevention and management of infectious complications of percutaneous interventions. Seminars in Interventional Radiology. 32(2). 78-88.
Type: literature review
Quality rating: Level V
A review of infectious complications associated with percutaneous IR procedures, to include percutaneous nephrostomy placement.
Prophylactic antibiotics are typically given prior to PCN placement or exchange to minimize infectious episodes, authors admit they have not been well studied in the medical literature.
Evidence provided based on studies from late 80s-late 90s.
Infectious complications associated with percutaneous catheter nephrostomy (PCN) can occur during or after catheter placement.
In the immediate post-procedural period, the most common and serious systemic complication is sepsis, rate ranges from 1.3-1.8 percent., no p value given for this statement
The causative organisms are typically gram-negative bacteria, including E. coli, Proteus, and Klebsiella, though a common gram-positive pathogen is Enterococcus
Current SIR Guidelines recommend prophylactic antibiotics in all PCN placement, except for routine exchange of noninfected, non-obstructed collecting systems in immunocompetent patients.
Sutcliffe, J. A., Briggs, J. H., Summary of RCTs, to include Continues to state that the Re: PCNs, those without Reviewed the relevant study results

A PRACTICE CHANGE TO ELIMINATE PROPHYLACTIC ANTIBIOTICS 5Brief reference, type of study,
quality ratingMethods Threats to
Reliability/ValidityStudy findings Conclusions
Little, M. W., McCarthy, E., Wigham, A., Bratby, M., & Uberoi, R. (2015). Antibiotics in interventional radiology. Clinical Radiology. 70(3) 223-234.
Type: literature review
Quality: Level V
comprehensive literature search including systematic reviews, prospective and retrospective studies, and evidence obtained from expert committee reports.
field has minimal research in randomized controlled trials (RCTs) in the last 25 years to assess the need for antibiotic prophylaxis in interventional radiology, but they continue to be a standard of care for patients.
evidence of infection can be separated into those with and without risk factors. These include advanced age, diabetes, bladder dysfunction, indwelling catheter, calculi, ureterointestinal anastomosis, previous manipulation, and bacteriuria
based on quality and type of study, states that evidence is based on four articles, one rated as a B and the other three as C; B - Data derived from a single randomized controlled trial or randomized studies; C - Only consensus opinion of experts, case studies, or standard of care.
Dagli, M., Ramchanani, P. (2011). Percutaneous Nephrostomy: Technical Aspects and Indications. Seminars in Interventional Radiology. 28(4).
Type: lit review of practice and evidence
Quality: Level V
Lit review done on placement, and post-procedure management of percutaneous nephrostomy drainage are described.
No new study done related to the guidelines, redundant use of the same studies from the late 80s, very limited newer material.
The greatest risk of infectious complications is seen in patients with clinical signs of infection. In these patients, the goal of antibiotics is treatment rather than prophylaxis.
The majority of PCN exchanges are considered dirty because of the risk factors that most patients face, but antibiotics are not necessary for patients without the risk factors
Bahu, R., Chaftari, A., Hachem, R. Y., Ahrar, K., Shomali, W., Zakhem, A. E., Jiang, Y. . . Raad, I. (2013). Nephrostomy tube related pyelonephritis in patients with cancer: Epidemiology, infection rate, and risk factors. The Journal of Urology, 189(1), 130-135.
Type: non-experimental study, retrospective
Quality: IIIB
Retrospective review of 200 patients from 91/1/2009 to 9/16/2010 at MD Anderson Cancer Center, followed for 90 days after event.
Categorical variables were compared by the chi-square or Fisher exact tests
continuous variables were compared using Wilcoxon rank sum tests.
Multiple logistic regression
Risk used only categorically, not as a level of risk
Retrospective, uncontrolled variables present
Only for cancer patients
Clinical symptoms not consistently monitored
Serial urine culture results not always available
N = 200, 38 (19%) had pyelonephritis and 15 (7.5%) had asymptomatic bacteriuria.
4 undergoing exchange had episode of pyelonephritis
Pyelonephritis developed within the first month in 19 (10%) patients.
Prior urinary tract infection and neutropenia were found to be significant risk factors for pyelonephritis in patients with
Neutropenia and UTI high risk of pyelonephritis
Further investigation needed to reduce infection rate
pyelonephritis developed w/in 3 months in about 1 in 5 patients with cancer who had nephrostomy placed

A PRACTICE CHANGE TO ELIMINATE PROPHYLACTIC ANTIBIOTICS 6Brief reference, type of study,
quality ratingMethods Threats to
Reliability/ValidityStudy findings Conclusions
used to identify independent risk factors for bacteriuria and pyelonephritis.
history of cancer (p = 0.047 and 0.03

7A PRACTICE CHANGE TO ELIMINATE ANTIBIOTICS
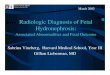
Appendix B: MUSC VIR Handbook 2016 Guidelines
Figure B1: MUSC VIR Handbook 2016 Guidelines. This figure includes 2016 guidelines regarding whether routine prophylaxis is recommended for PCN Exchange. Retrieved with permission from MUSC VIR 2016 Handbook.

8A PRACTICE CHANGE TO ELIMINATE PROPHYLACTIC ANTIBIOTICS
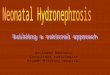
Appendix C: MUSC VIR Handbook 2017 Guidelines
Figure C1: MUSC VIR Handbook 2017 Guidelines. This figure includes 2016 guidelines regarding whether routine prophylaxis is recommended for PCN Exchange. Retrieved with permission from MUSC VIR 2017 Handbook.

9A PRACTICE CHANGE TO ELIMINATE PROPHYLACTIC ANTIBIOTICS
Figure C2. MUSC VIR Handbook 2017 Guidelines 2017 statement on antibiotic prophylaxis for non-obstructed routine PCN exchanges. Retrieved with permission from MUSC VIR Handbook 2017.

10A PRACTICE CHANGE TO ELIMINATE PROPHYLACTIC ANTIBIOTICS
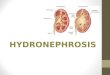
Appendix D: Map of Patients by State of Residence
State
Number of Patients
(n = 126)
SC 115 (91.3%)
GA 4 (3.2%)
NC 3 (2.4%)
VA 1 (.8%)
DC 1 (.8%)
OH 1 (.8%)
AZ 1 (.8%)
Map D1: Map of Patients by State of Residence. Map was created with Microsoft Excel Geographic Heat Map using thematic grayscale to show patient concentration by location.

11A PRACTICE CHANGE TO ELIMINATE PROPHYLACTIC ANTIBIOTICS
Appendix E: Potential Clinical Pathways for PCN Exchange Event as an Outpatient
Figure E1: Potential clinical pathways for PCN Exchange event as an outpatient
Infection Management
Post-Procedure OutcomeIntraprocedure
Determine Risk Level of Infection
Patients Undergoing
PCN Exchange
PCN Exchange Procedure
Patient has Low Risk of PCN infection No antibiotics
PCN Infection and no antibiotic
Treated as Outpatient- OR -
Admitted for Infection
No Infectionand no antibiotic
Patient has High Risk of PCN infection
Received peri-operative antibiotic
PCN Infection and received antibiotic
Treated as Outpatient- OR -
Admitted for Infection
No Infection and received antibiotic
Number of PCN exchanges (events) vary per patient
Patients undergoing regular exchanges return within 6-8 weeks for new PCN
Patients who undergo routine PCN exchange are routinely evaluated for need for PCN
Low Risk – no risk factors of infection. Antibiotic administration determined by IR team prior to procedure based on history and recent events
High Risk – one or more of the infection risk factors: obstruction, history of UTI, DM II, renal transplant, or HTN