Embed Size (px)
Citation preview
TB Nurse Case Management Arlington, Texas July 14 - 16, 2009
Pediatric Tuberculosis Theresa Barton, MD
July 15, 2009
Pediatric Tuberculosis
Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern Medical Center
July 15, 2009
Disclosures
• Research Support: – Tibotec Pharmaceuticals
– Pfizer, Inc.
(no relation to topic)
No off-label drug usages will be discussed
Objectives
• Diagnostic process
• Progression from TB infection to TB disease
• Treatment of LTBI in children
• Management of TB disease in children
• Case studies
Pediatric TB—Background
• Definition of pediatric tuberculosis (TB): TB disease in a person <15 years old
• In 2006, • 13,779 TB cases were reported among all age
groups
– 807 (5.9%) were pediatric
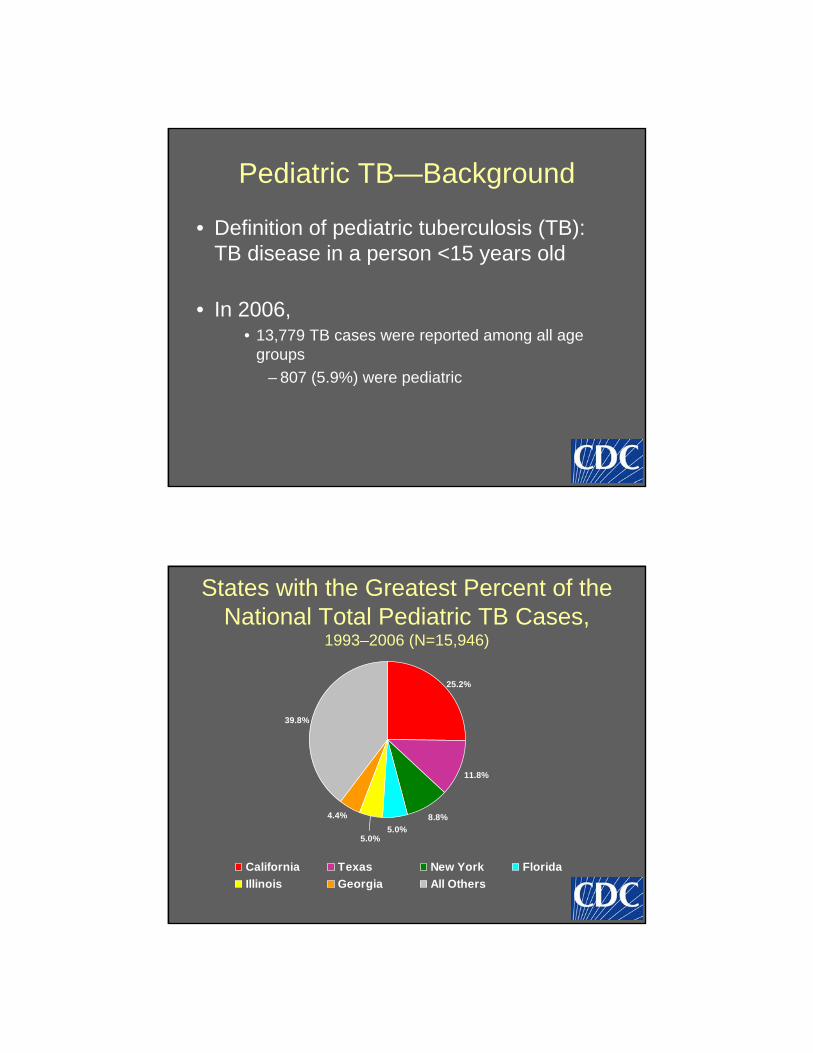
States with the Greatest Percent of the National Total Pediatric TB Cases,
1993–2006 (N=15,946)
4.4%
5.0% 5.0%
8.8%
11.8%
25.2%
39.8%
California Texas New York Florida
Illinois Georgia All Others
States with Greatest Numbers of Pediatric TB Cases, 1993–2006
*Average percent of total state cases that are pediatric, for all years **Time-averaged annual rate per 100,000
California 4,025 7.7 3.7
Texas 1,874 7.3 2.7
New York 1,399 4.8 2.6
Florida 794 4.4 1.9
Illinois 791 6.9 2.1
Georgia 700 7.8 2.8
All Others 6,363 5.9 1.3
State Number Percent* Rate**
Pediatric TB Cases
Overall U.S. 15,946 6.3 1.9
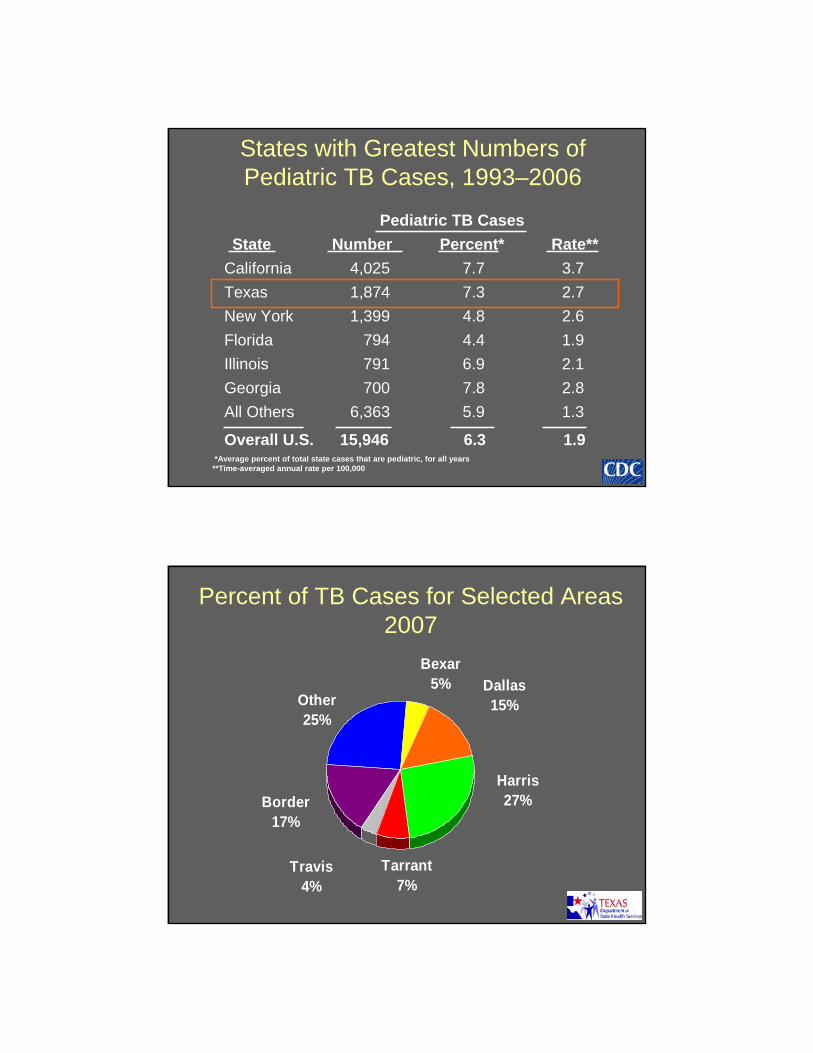
Percent of TB Cases for Selected Areas 2007
Bexar 5% Dallas
Other 15% 25%
Harris
Border 27%
17%
Travis 4%
Tarrant 7%
- -
- -
White Black Hispanic Asian
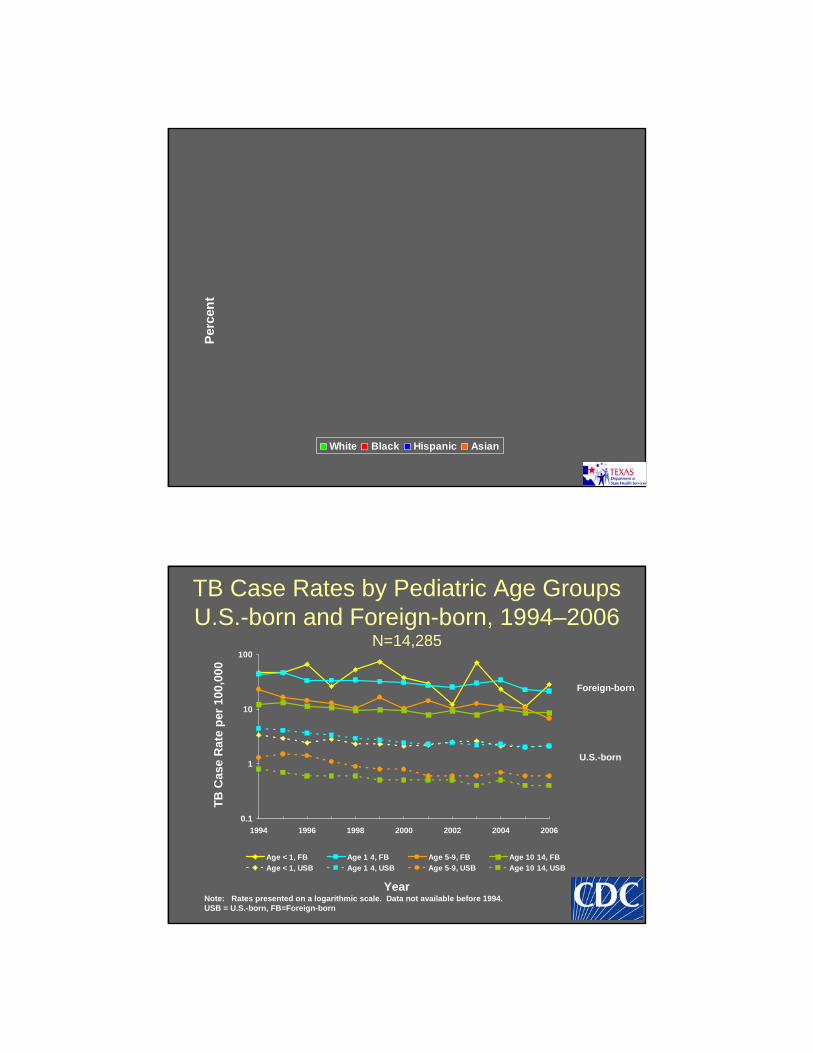
TB Case Rates by Pediatric Age Groups U.S.-born and Foreign-born, 1994–2006
N=14,285
0.1
1
10
100
1994 1996 1998 2000 2002 2004 2006
Age < 1, FB Age 1 4, FB Age 5-9, FB Age 10 14, FB
Age < 1, USB Age 1 4, USB Age 5-9, USB Age 10 14, USB
Year
TB
Cas
e R
ate
per
100
,00
0
Note: Rates presented on a logarithmic scale. Data not available before 1994. USB = U.S.-born, FB=Foreign-born
Foreign-born
U.S.-born
Per
cen
t
Foreign-born Pediatric TB Cases by Birth Country* and 4-Year Interval, 1995–
2006 (N=3,231)
1995–1998 (n) 1999–2002 (n) 2003–2006 (n)
Mexico (467) Mexico (375) Mexico (323)
Philippines (118) Somalia (79) Somalia (65)
Viet Nam (73) Philippines (67) Philippines (63)
Somalia (43) Haiti (38) Haiti (45)
Haiti (39) Viet Nam (36) Viet Nam (37)
Russia (38) Sudan (26) India (36)
Other (422) Other (417) Other (424) *Ranked by counts
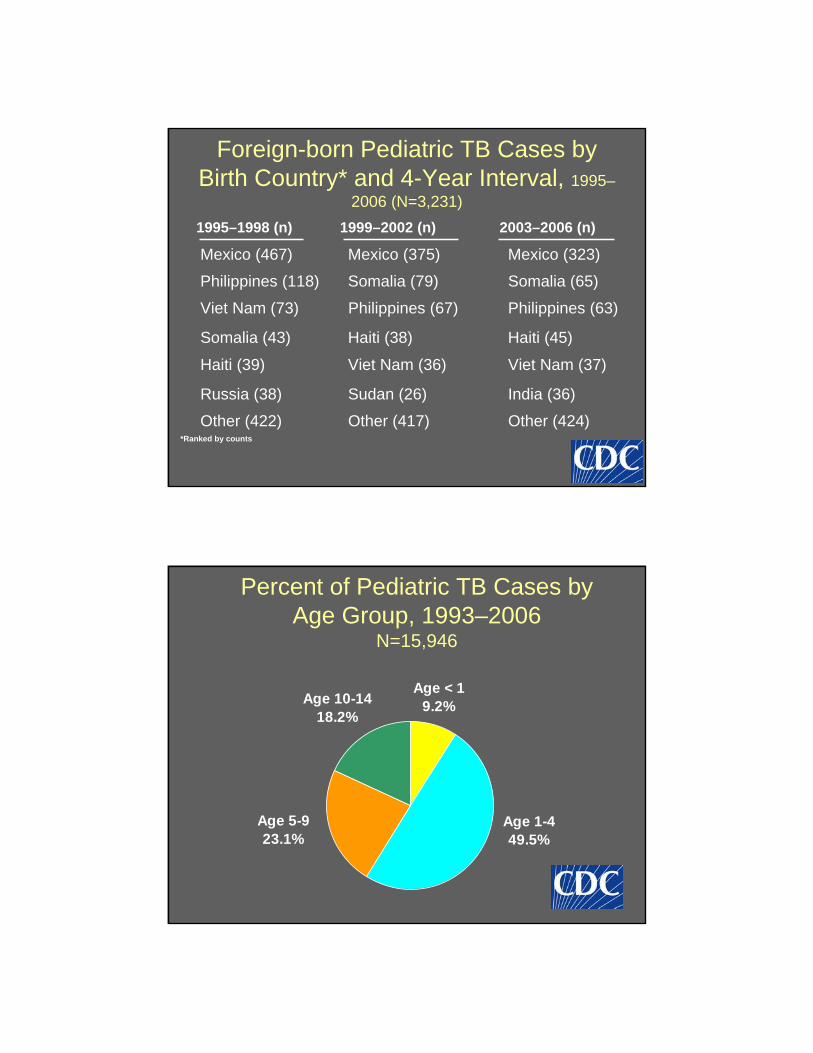
Percent of Pediatric TB Cases by Age Group, 1993–2006
N=15,946
Age < 1 Age 10-14 9.2%
18.2%
Age 1-4 49.5%
Age 5-9 23.1%
Epidemiology
• Most TB cases in children occur in urban, low-income areas and in non-white racial/ethnic groups
• Foreign-born children account for cases in children <14 years
• High risk groups: – Immigrants – International adoptees – Refugees from endemic areas – Travelers to endemic areas – Homeless – Correctional facilities
Clinical Manifestations
• Most infections in children and adolescents are asymptomatic
• Symptoms of active pulmonary disease: – Fever – Weight loss or growth delay (failure-to-thrive) – Cough – Night sweats – Lymphadenopathy
• Extrapulmonary manifestations: – Meningitis, lymphadenitis (cervical or mesenteric),
Osteomyelitis – Chronic otitis media
Progression to TB Disease
• Risk factors for progression from LTBI to active TB: – Infants (<12 months) – Post-pubertal adolescents – Recent infection (< 2 years) – Immune deficiency, especially HIV – Immunosuppressive drugs – corticosteroids,
chemotherapy, TNF-agonists – IVDU – Diabetes mellitus – Chronic renal failure – Malnutrition
Latent Tuberculosis Infection
–
––
–
––
––
Determining LTBI Risk
• Has a family member or contact had tuberculosis disease?
• Has a family member had a positive tuberculin skin test?
• Was your child born in a high-risk country?
• Has your child traveled to (or had contact with residents from) a high-risk country for more than 1 week?
Indications for Testing in Children
• Immediate TST: Contact with confirmed or suspected contagious TB case (contact investigation) Radiographic or clinical suspicion for TB Children immigrating from endemic areas, including adoptees (age > 3 months) Children with travel histories to endemic areas
• Wait 10 weeks to test, if child is well
• Routine annual TST HIV+ children Incarcerated adolescents
• Periodic or risk-based testing Certain chronic medical conditions, possible exposure Initial test should be done before starting immunosuppressive agents
– ––
–
–
–
–
Timing of Positive Skin Testing
• Incubation 2-12 weeks
• Risk of developing TB disease is highest in the first 6 months after infection, up to 2 years
• Many years may elapse between exposure and disease
Defining (+) Skin Test Results in Children
• Induration ≥5 mm Close contact with known or suspected person with TB disease Chest x-ray consistent with active or old TB Clinical evidence other TB disease (meningitis, lymphadenitis, etc) Immunosuppressive therapy or immune deficient, HIV
• Induration ≥10 mm Increased risk for dissemination
• Age < 4 years • Underlying medical condition (lymphoma, DM, chronic renal failure,
etc) Increased risk of exposure
• Born in high prevalence area • Frequent exposure to high-risk adults (HIV, homeless, nursing
home residents, incarcerated adults, migrant farm workers) • Travelers to high prevalence areas in the world
• Induration ≥15 mm Age >4years, without other risk factors
Interferon Gamma Release Assays (IGRA) in Children
• Immune competent children >= 5 years, IGRA can be used in place of TST
• Positive IGRA should be considered indicative of M. tubeculosis infection; negative IGRA may not rule out TB
• IGRA may be useful to determine whether BCG-immunized child has LTBI or false-positive TST from BCG
• NOT RECOMMENDED for children <5 years, or immunocompromised children
Therapy for LTBI
• Efficacy close to 100% in children, when adherent
• ALL infants, children and adolescents who have a positive TST but no evidence of disease should receive therapy
• Duration: 9 months
• Twice a week DOT can be considered if daily therapy not possible
–
–
–
–
–
–
–
Therapy for LTBI
• INH-Susceptible (>90% of US cases) – Isoniazid 10-15 mg/kg once daily x 9 months (max
300 mg/day) • 100mg, 300mg tablets, 10mg/mL syrup
• INH-Resistant – Rifampin 10-20 mg/kg once daily or divided BID (max
600 mg/day • 150mg, 300mg capsules, can be made into syrup by
pharmacy
• INH-RIF Resistant – Consult Specialist: PZA, fluoroquinolone, ETH are
typical choices, depending on source case susceptibilities
Maternal TB + Infant Exposure
• Mother with LTBI Household + infant evaluation
No therapy unless household contact with active TB
• Mother with active TB All household members should be evaluated within 7 days
Evaluation for congenital tuberculosis
Infant separated from mother until (1) mother receiving therapy, (2) infant receiving INH, (3) mother wears mask and is adherent to treatment
MDR TB – consider infant BCG vaccination
Women may breastfeed who have been on treatment for 2 or more weeks
Maternal TB + Breastfeeding
• Breastfeeding is OK for women being treated with the first-line anti-TB drugs – Concentrations of these drugs in breast milk
are too small to produce toxicity in the nursing newborn
• Breastfeeding women taking INH should also take pyridoxine (vitamin B6) supplementation.
TB Exposure in Children -Summary
• LTBI or active TB disease in a child almost always indicates recent infection with a contagious adult
• Foreign-born young children are at the highest risk for TB exposure
• TB screening questions should be incorporated into routine pediatric care,and should prompt TST or IGRA testing ifrisk factors idenitfied
TB Exposure in Children -Summary
• All children & adolescents exposed to a person with active TB disease should be evaluated – TST, physical exam, CXR – Newborn infants should have full evaluation for
congenital tuberculosis (confinement from mother until the mother is receiving therapy)
• Exposed children with impaired immunity or age <4 years – Initiate INH therapy even if TST negative – Repeat TST in 12 weeks to determine if continued
INH needed
–––
–
–––––––
TB Diseases in Children
• Intrathoracic Pulmonary TB Pleural disease Cardiac disease
• Extrathoracic Lymphohematogenous disease (disseminated) – includes miliary TB Lymphatic disease Central nervous system Osteoarticular Abdominal/GI Genitourinary (renal disease) Cutaneous Congenital
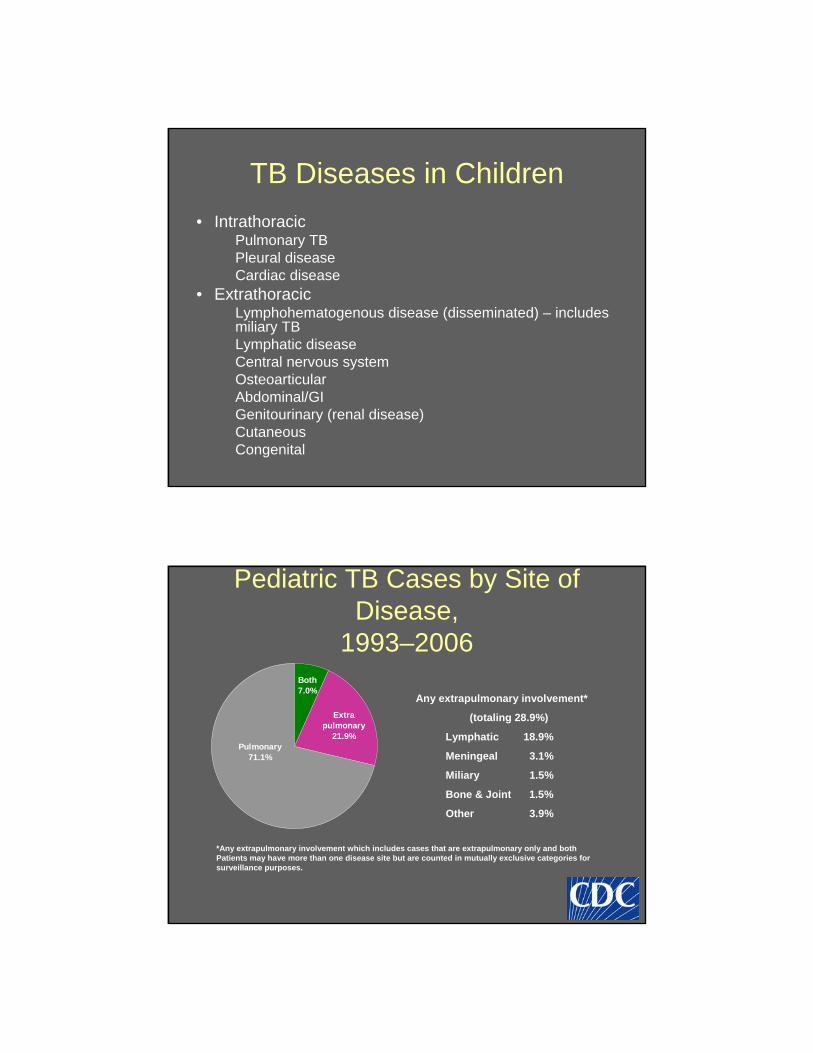
Pediatric TB Cases by Site of Disease,
1993–2006
Any extrapulmonary involvement*
(totaling 28.9%)
Lymphatic 18.9%
Meningeal 3.1%
Miliary 1.5%
Bone & Joint 1.5%
Other 3.9%
*Any extrapulmonary involvement which includes cases that are extrapulmonary only and both Patients may have more than one disease site but are counted in mutually exclusive categories for surveillance purposes.
Extra pulmonary
21.9%
Both 7.0%
Pulmonary 71.1%
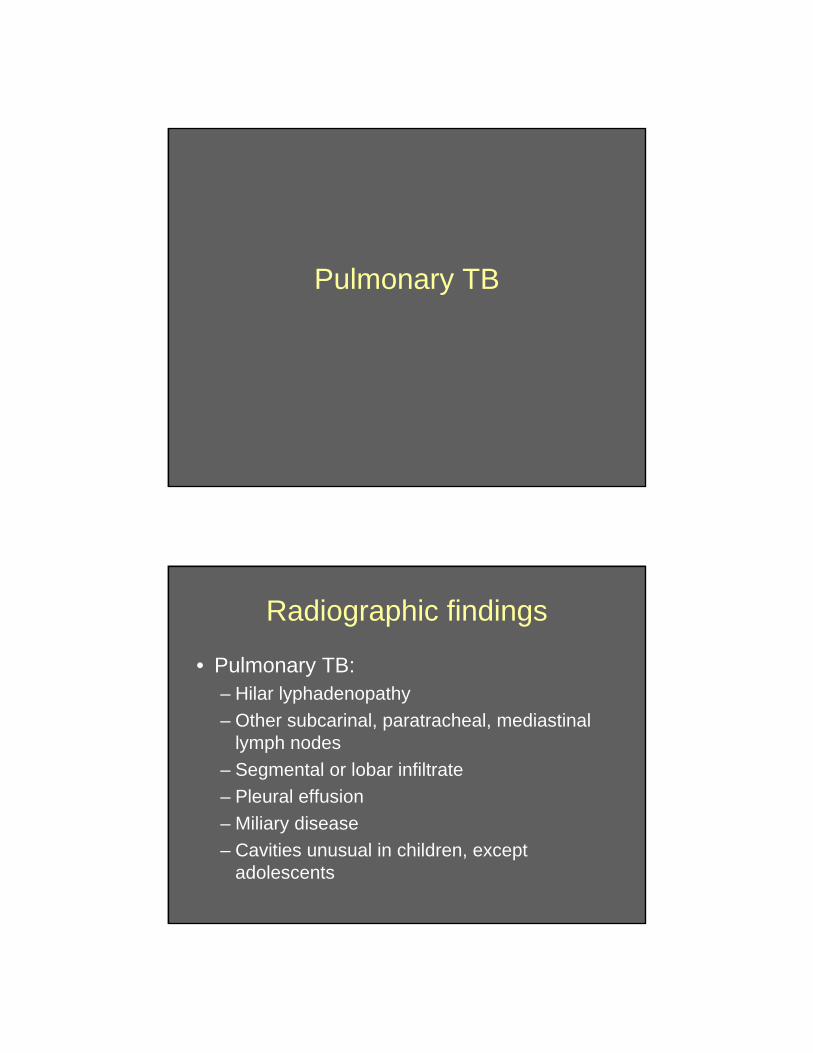
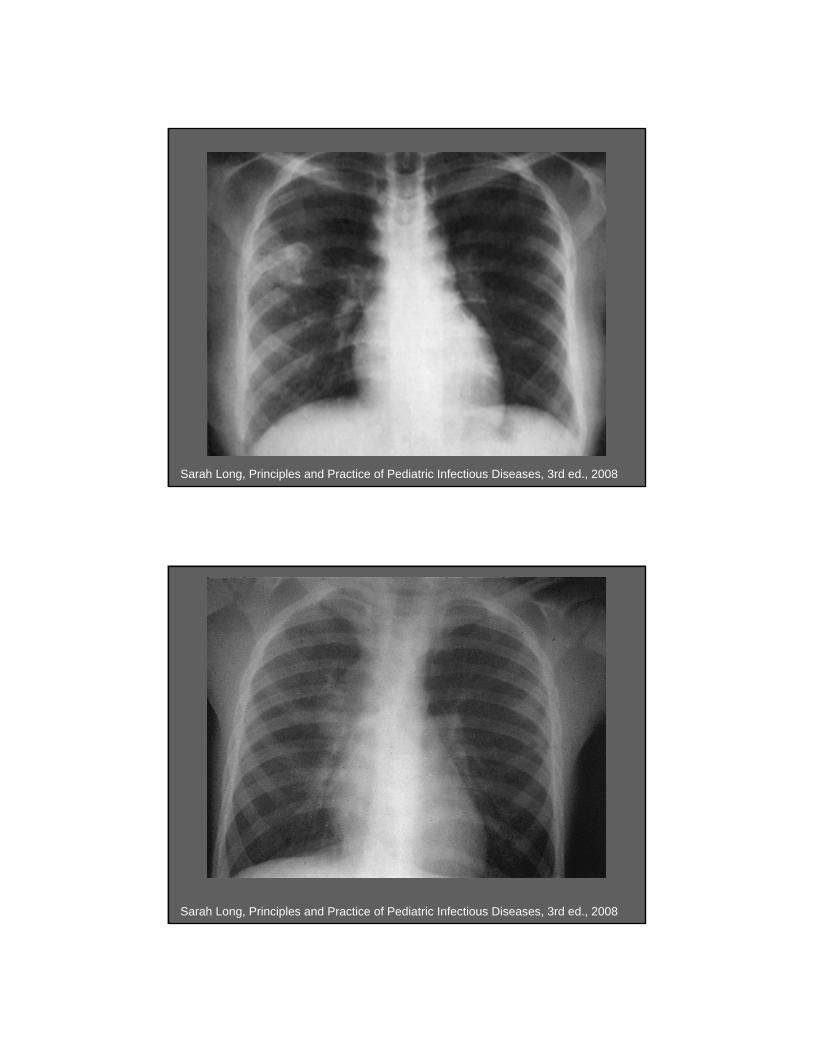
Pulmonary TB
Radiographic findings
• Pulmonary TB: – Hilar lyphadenopathy
– Other subcarinal, paratracheal, mediastinal lymph nodes
– Segmental or lobar infiltrate
– Pleural effusion
– Miliary disease
– Cavities unusual in children, except adolescents
Sarah Long, Principles and Practice of Pediatric Infectious Diseases, 3rd ed., 2008
Sarah Long, Principles and Practice of Pediatric Infectious Diseases, 3rd ed., 2008
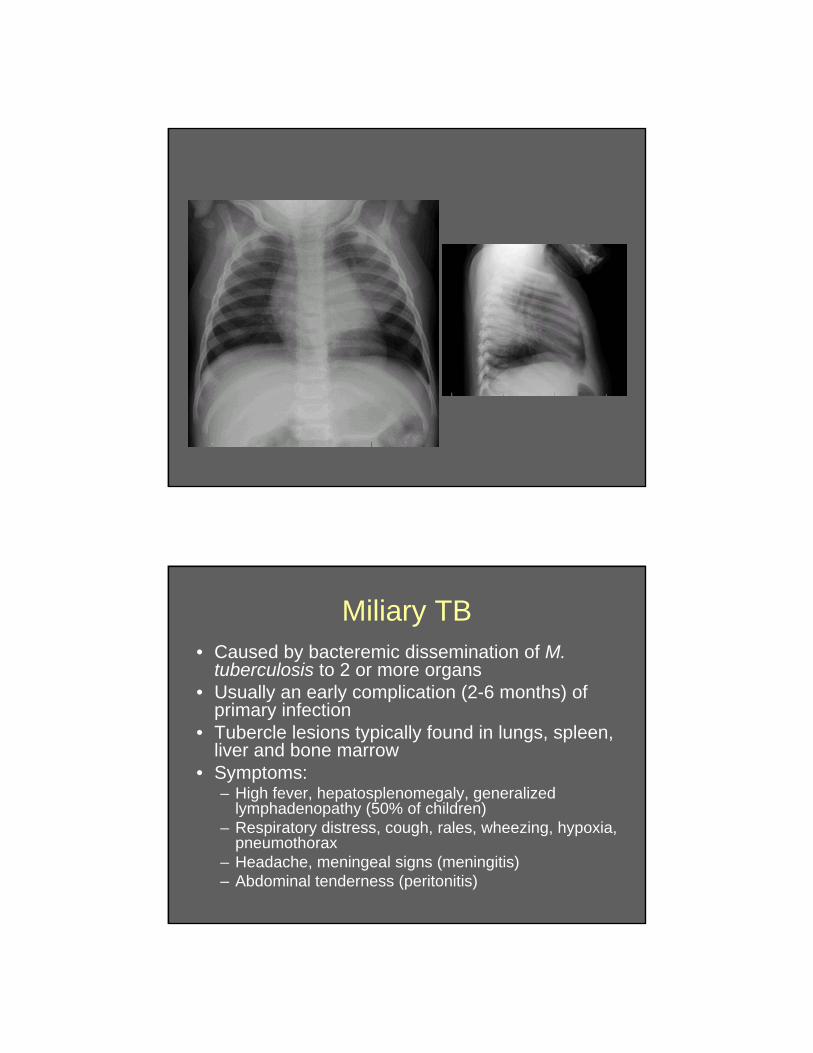
Miliary TB • Caused by bacteremic dissemination of M.
tuberculosis to 2 or more organs • Usually an early complication (2-6 months) of
primary infection • Tubercle lesions typically found in lungs, spleen,
liver and bone marrow • Symptoms:
– High fever, hepatosplenomegaly, generalizedlymphadenopathy (50% of children)
– Respiratory distress, cough, rales, wheezing, hypoxia, pneumothorax
– Headache, meningeal signs (meningitis) – Abdominal tenderness (peritonitis)
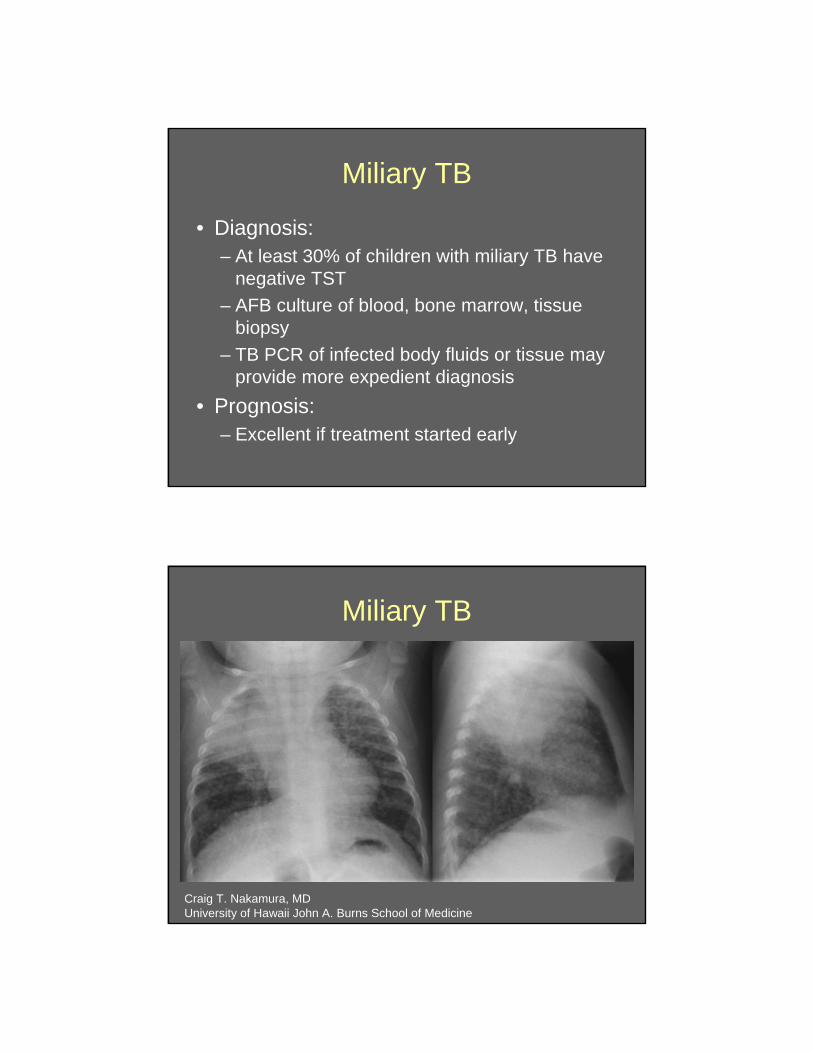
Miliary TB
• Diagnosis: – At least 30% of children with miliary TB have
negative TST
– AFB culture of blood, bone marrow, tissue biopsy
– TB PCR of infected body fluids or tissue may provide more expedient diagnosis
• Prognosis: – Excellent if treatment started early
Miliary TB
Craig T. Nakamura, MD University of Hawaii John A. Burns School of Medicine
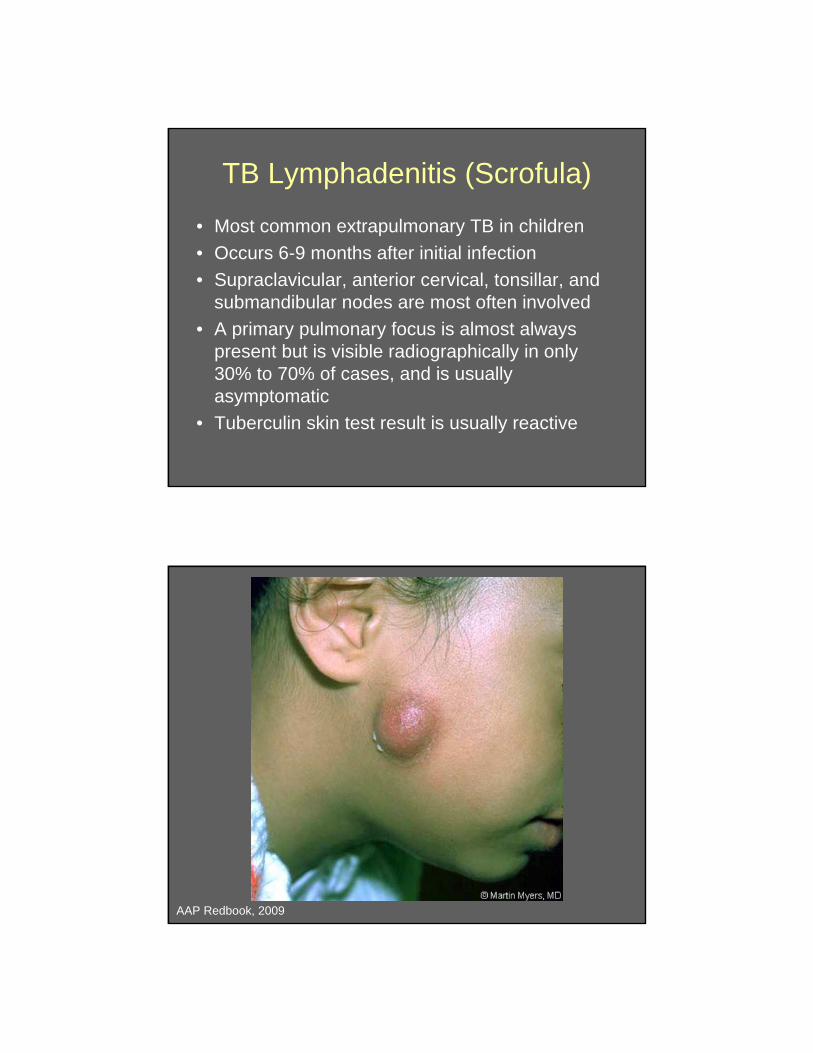
TB Lymphadenitis (Scrofula)
• Most common extrapulmonary TB in children
• Occurs 6-9 months after initial infection
• Supraclavicular, anterior cervical, tonsillar, and submandibular nodes are most often involved
• A primary pulmonary focus is almost always present but is visible radiographically in only 30% to 70% of cases, and is usually asymptomatic
• Tuberculin skin test result is usually reactive
AAP Redbook, 2009
TB Meningitis
• Occurs in 0.5% of primary infections in children
• Age: 6 months – 4 years • Onset within 2-6 months of infection • May occur with primary disease
(dissemination, miliary TB), or with reactivation
• Onset can be rapid or gradual (often more rapid in younger children)
TB Meningitis • Stage 1:
– Lasts 1 to 2 weeks – Fever, headache, irritability, and drowsiness, loss of
developmental milestones
• Stage 2: – lethargy, nuchal rigidity, seizures, hypertonia,
vomiting, cranial nerve abnormalities, and other focal neurologic signs
– Encephalitis – Communicating hydrocephalus
• Stage 3: – coma, hemiplegia or paraplegia, hypertension,
decerebrate or decorticate posturing

TB Meningitis • Diagnosis
– TST non-reactive in up to 40% – CXR normal in up to 50% – CSF findings
• Markedly elevated protein (>400 mg/dL) • Elevated WBC (10-500 cells/mm3), lymphocytic
predominance
– Head CT (with contrast) • Basilar cisternal enhancement • Communicating hydrocephalus • Cerebral edema, focal ischemia
– AFB culture of CSF, TB PCR
Sarah Long, Principles and Practice of Pediatric Infectious Diseases, 3rd ed., 2008
Congenital Tuberculosis
• Extremely rare (fewer than 300 cases reported in literature)
• Presentation: – Respiratory distress, fever, hepatosplenomegaly,
poor feeding, lethargy or irritability, lymphadenopathy, abdominal distention, ear drainage, and skin lesions
– May be present at birth – usually @ 2-3 weeks of life
• Occurrence and intensity of hematogenous dissemination during pregnancy determine congenital infection
Diagnosing TB in Children
• More difficult to diagnose than in adults –must have a higher degree of suspicion
• M. tuberculosis detected in up to 50% of gastric aspirates in non-HIV-infectedchildren
• About 10% of culture-positive children have negative TST
• Diagnosis usually made by linking child to TB contact + radiograph + skin test
Other Diagnostic Methods
• Culture for AFB – Gold standard for diagnosis, allows susceptibility
testing
– High culture positivity with cavitary disease
– Low culture positivity in absence of cavity (i.e. most children)
• Expectorated sputum
• Gastric aspirate fluid
• Pleural fluid
• Bronchoalveolar lavage fluid has low yield
– Good yield from lymph node tissue
Other Diagnostic Methods
• TB PCR
• IFN-gamma Release Assays (IGRA)

Case #1
• 6-month female infant • Brought to Emergency Dept for cough +
fever x few days • Exam notable for tachypnea, wheezing,
but otherwise looked well – exam suggestive of bronchiolitis
• CXR done because of tachypnea + fever to r/o pneumonia
• RSV testing done (negative)
http://www.mevis-research.de
Case #1
• CXR concerning for miliary TB • Further hx + exam done:
– Family originally from Honduras, infant born in US and no travel to Honduras
– Lives with parents, grandparents, paternal aunt – all reported as healthy
• Exam: normal growth parameters, no meningeal signs, no lymphadenopathy, no hepatosplenomegaly
Evaluation of infant with suspected TB
• PPD skin testing • Chest x-ray • PPD placement for household members and
close contacts +/- CXR for parents regardless of PPD result
• Gastric aspirate AFB cx • Lumbar puncture with AFB cx and TB PCR • Brain MRI for abnormal CSF • Liver function testing • Abdominal imaging if other findings suggest
miliary or disseminated disease
Case #1
• Challenges of this case: – Initial exam and history suggestive of
common pediatric disease
– Was a CXR really indicated?
– Careful history revealed family risk factors
– Immigrant family should have been screened in their own health care – how often do healthy young adult immigrants enter the health care system?
Case #2
• 11 month-old Caucasian female from Plano
• 1 week history fever + cough, not responding to oral antibiotics
• Exam: – mild respiratory distress
– diminished breath sounds on right chest
• CXR: miliary pattern, right infiltrate with pleural effusion
Case #2
• Lumbar puncture done: – NUC 65 (elevated)
– RBC 130
– Glucose 70
– Protein 244 (elevated)
• CSF culture negative
• CSF TB PCR: positive
Case #2
• No known TB risk factors – No travel
– No high-risk family members
– Parents TST negative
• Family housekeeper from Honduras TST positive – Aunt of child in Case #1
~ AN ° BEAUTY
. CUTICURA REMEDIES C URE
SKIN ANO BLOOD DISEASES
Treatment for TB Disease
• AAP Redbook: 3 drug regimen
• TX: 4 drug regimen – Risk of drug-resistant TB in TX
• Pulmonary TB: – INH, RIF, PZA, ETH
• TB Meningitis: – INH, RIF, Amikacin, ETH?
Pediatric Dosing
• ISONIAZID – 10-15 mg/kg once daily
• RIFAMPIN – 10-20 mg/kg once daily
• PYRAZINAMIDE – 20-40 mg/kg once daily
• ETHAMBUTOL – 15-25 mg/kg once daily
• AMIKACIN – 10 mg/kg IV every 8 hours
• Use of fluoroquinolones or streptomycin should be in consultation with Pediatric Infectious Disease specialist
=
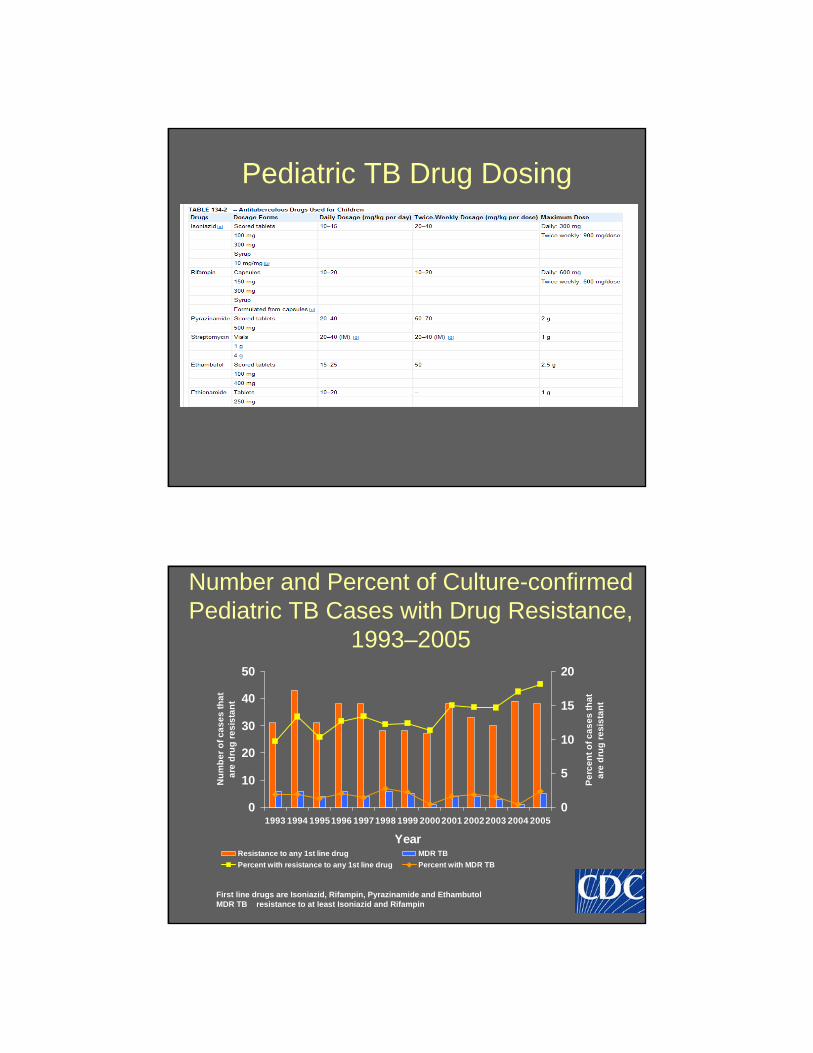
Pediatric TB Drug Dosing
Number and Percent of Culture-confirmed Pediatric TB Cases with Drug Resistance,
1993–2005
0
10
20
30
40
50
1993 1994 19951996 19971998 1999 20002001 20022003 2004 2005
Year
Nu
mb
er
of
ca
se
s t
ha
ta
re d
rug
re
sis
tan
t
0
5
10
15
20
Pe
rce
nt
of
ca
se
s t
ha
ta
re d
rug
re
sis
tan
t
Resistance to any 1st line drug MDR TB
Percent with resistance to any 1st line drug Percent with MDR TB
First line drugs are Isoniazid, Rifampin, Pyrazinamide and Ethambutol MDR TB resistance to at least Isoniazid and Rifampin
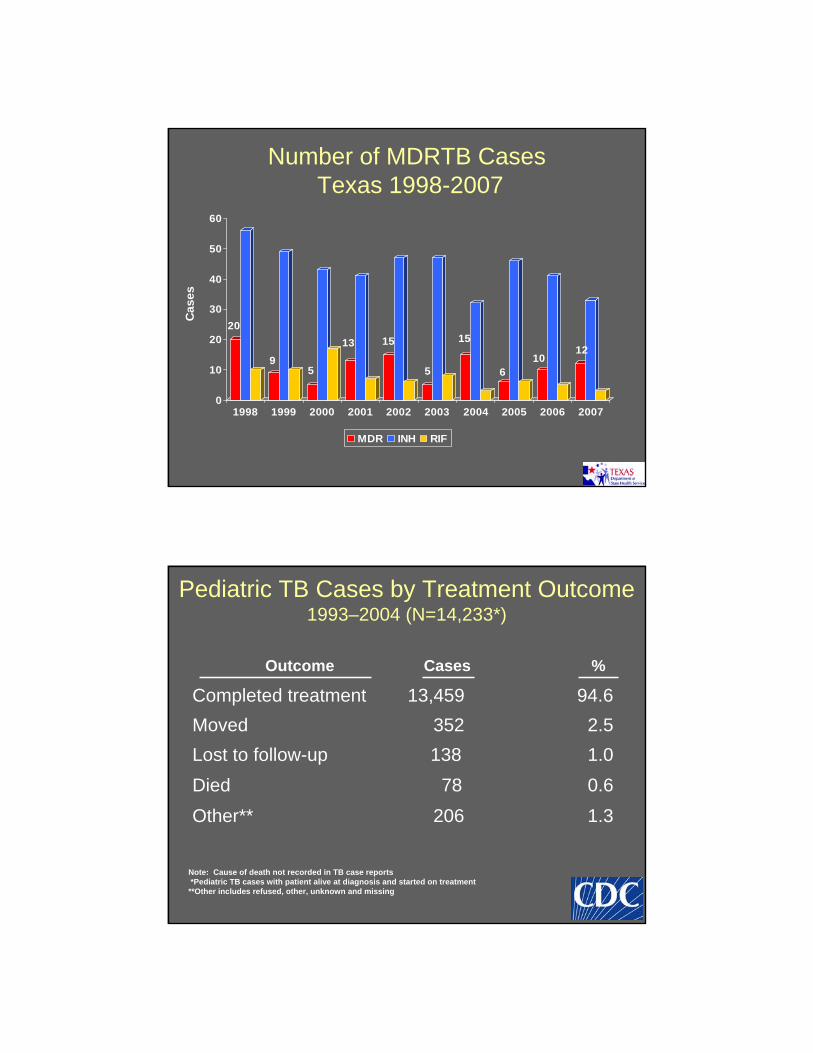
Number of MDRTB Cases Texas 1998-2007
20
9 5
13 15
5
15
6 10
12
0
10
20
30
40
50
60
Case
s
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MDR INH RIF
Pediatric TB Cases by Treatment Outcome 1993–2004 (N=14,233*)
Outcome Cases %
Completed treatment 13,459 94.6
Moved 352 2.5
Lost to follow-up 138 1.0
Died 78 0.6
Other** 206 1.3
Note: Cause of death not recorded in TB case reports *Pediatric TB cases with patient alive at diagnosis and started on treatment
**Other includes refused, other, unknown and missing
TB Diseases in Children -Summary
• Risk of disseminated or extrapulmonarydisease is increased in children – Infants <12 months of age should be
evaluated for dissemination regardless ofclinical findings
• Cavitary pulmonary TB is NOT the typical presentation – Hilar adenopathy, non-specific infiltrates
• PPD testing may not be accurate in infants <6 months
Gardner Association for the Prevention and Relief of Tuberculosis, c. 1900