Embed Size (px)
Citation preview
794
CURRENT COMMENT
ARE WE LOSING FOCUS ON THE INTERNAL ELASTIC LAMINA IN
GIANT CELL ARTERITIS?
JOHN P. O’BRIEN and WILLIAM REGAN
“ I t thus seems likely that elastin evolved us an adaptive response to the stresses imposed on arteries by the eficient high pressure circulatory system achieved etirly in vertebrate evolution. ’’
Sage and Gray ( I )
Approaches to the etiology of giant cell (temporal) arteritis
In researching the etiology and pathogenesis of a disease, it is often helpful to start by defining its locus or site. Until recently, it has been almost univer- sally agreed that the locus of giant cell arteritis (GCA) is the supporting internal elastic lamina of the temporal and other superficial arteries. This was first clearly demonstrated by Kimmelstiel and coworkers in 1952 (2). Those authors also emphasized that a peculiar degeneration, with rigid changes, swelling, and frag- mentation of the lamina, elicited the granulomatous giant cell reaction. Many studies and accounts of the disease accept this view of the initiating role of the lamina. Thus, after likewise noting the “peculiar de- structive alterations in the internal elastic lamina,” and the possibility of “some insult,” Healey and Wilske (3) conclude their chapter on the etiology of GCA by saying:
. _ _ From the Pathology Laboratory, Wales Medical Center,
and the Department of Dermatology, Repatriation General Hospital, Sydney, Australia.
John P. O’Brien, MD, FRCPA: Pathology Laboratory, Wales Medical Center; William Regan, DDM. FACD: Department of Dermatology, Repatriation General Hospital.
Address reprint requests and correspondence to John P. O’Brien, MD, FRCPA, Pathology Laboratory, Wales Medical Cen- ter, 66 High Street, Randwick 2031, Sydney, Australia.
Submitted for publication October 24, 1991; accepted in revised form February 26, 1992.
“In summary, one hypothesis that would explain many of the observed phenomena of giant cell arteritis is as follows: in some geneti- cally predisposed individuals, the elastic tissue in the arterial wall becomes altered and antigenic. This may be the result of normal aging change in which there is disruption of elastin or, alterna- tively, it may be in response to some unidentified external stimulus. This altered elastic tissue then serves as an antigen to provoke a cell-mediated immune response, which produces inflammation within the vessel wall.”
However, we believe that an apparent trend away from this approach has recently occurred. For instance, in their 1991 paper entitled “Analysis of Adhesion Molecules in the Immunopathogenesis of Giant Cell Arteritis,” Wawryk et al (4) cited only a single reference to the lamina. That reference was an article published in 1972, more recent work on the lamina having been omitted. More notably, 2 papers in Arthritis and Rheumatism, both authored by multiple senior investigators and both seeming to express the official (or, perhaps, semi-official) view of the Ameri- can College of Rheumatology (ACR), also exemplify this shift in focus.
The 2 articles are part of the ACR criteria for the classification of 7 selected vasculitis syndromes, which were authored by the vasculitis committee. One of the two articles, with Dr. Gene G. Hunder of the Mayo Clinic as the primary author, is a detailed summary of the clinicopathologic features of GCA (5 ) . Having stated at the outset that “The etiology of GCA is unknown,” the closest they get to mentioning a role for the lamina is when they state: “Histologically, a granulomatous inflammatory process is seen that is
Arthritis and Rheumatism, Vol. 35, No. 7 (July 1992)
ELASTIC TISSUE AND GCA 795
usually focused along the internal elastic lamina.” The second paper, with Dr. J. T. Lie, also of the Mayo Clinic, as the primary author, deals with the pathology of GCA, along with that of the other 6 vascular disorders (6). The sole comment about the lamina comes at the very end of the section on GCA: “Frag- mentation of the internal elastic lamella of the arterial wall occurs commonly in temporal arteritis, but this feature alone is not the sine qua non of temporal arteritis. It occurs with regularity in all temporal arteries of the aged (>60 years), and it persists long after the active phase of the disease.”
Granting that these papers are primarily con- cerned with diagnosis, it is nevertheless difficult to avoid concluding that in the diagnosis and etiology of GCA, the ACR gives little importance to laminal elastic tissue. This is a substantial change in emphasis from the classic, lamina-based approach taken by Kimmelstiel and colleagues, who stress its importance by including it in the title of their paper (2). However, those authors made no comment on the nature of the obscure laminal defect.
The actinic (radiation) hypothesis of GCA The actinic hypothesis (7) proposes that the
primary causative lesion of GCA is an in situ actinic elastotic degeneration of the lamina and not “normal aging.” Using a sensitive, or “controlled,” hematoxy- lin and eosin stain (as used in the original study of 330 subjects at autopsy), the degeneration of the internal elastic lamina of aged subjects was found to be mor- phologically identical to, or at least indistinguishable from, the degeneration found in actinically damaged dermal elastic (elastotic) fibers (7-9). Since the time of Unna (lo), this moderate, transparent, blue hematoxy- lin change in the dermis has been universally accepted as diagnostic of actinic damage, thus the common name, actinic (or solar) basophilic elastosis ( I 1) (see Figure 1A and Figure 2 in ref. 9).
A further, and probably highly significant con- currence of equivalent changes in artery and skin was observed (9). As in the dermis, the apparently actinic, blue-staining, elastotic change in arterial laminae of nearly half (46%) of the specimens was found to be conspicuously more advanced superficially, that is, in the outer, or “weather,” wall of the artery, as befits an extraneous and penetrating radiant cause (see Figure 1B in ref. 9). Electron microscopy revealed an accen- tuation of apparent actinic degeneration in the form of “dense zones” within the weather-side lamina (see ref. 9).
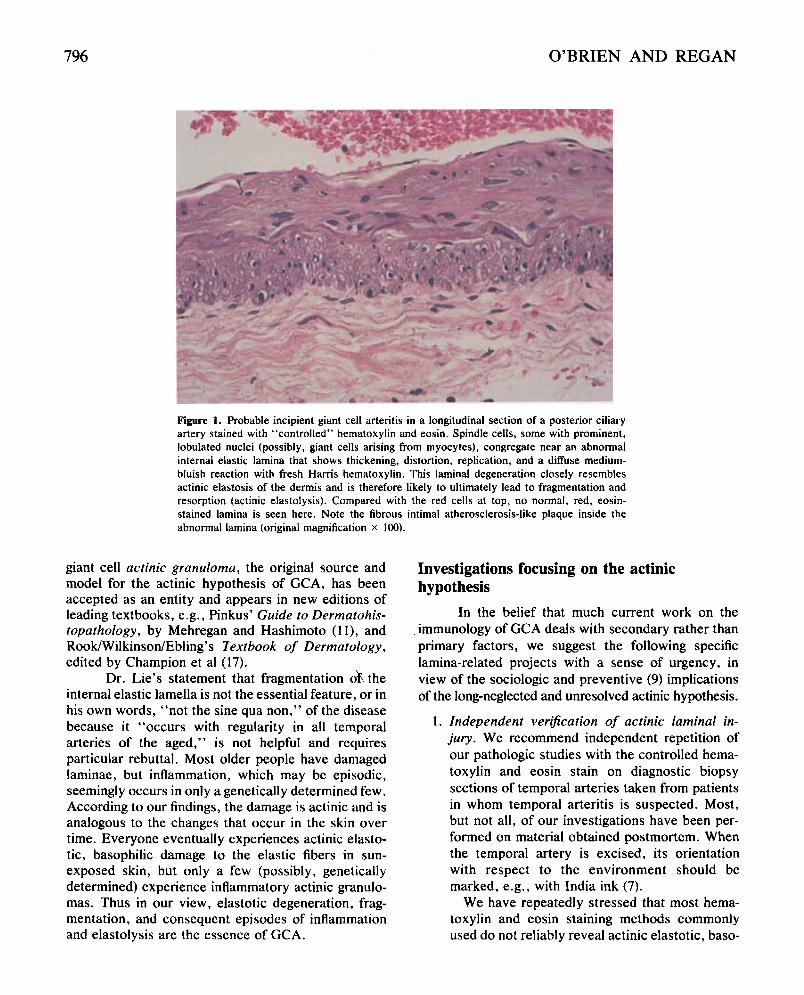
We have found that in early GCA, nascent giant cells first appear on damaged lamina (Figure I) . When frank arteritis supervenes, the granulomatous re- sponse is histologically identical to the specific giant cell reactions of sun-damaged elastotic skin that are now generally known as actinic granulomas ( I 1-17). Any differences in the pathologic reactions in the arteries as compared with the skin may reasonably be ascribed to the vastly different anatomy and function of arteries.
The need for scientific debate Being thus committed to the actinic hypothesis
of GCA, we regard the ACR’s apparent down-grading of the importance of the lamina as unfortunate. One immediate effect of this view would be to discourage new investigations into the subject; moreover, a trend toward dismissing the role of the lamina may influence evaluations of previous investigations as well. For it must be considered significant that in the ACR’s vasculitis committee reports, there is no mention of the now substantial body of published evidence in support of the actinic (electromagnetic) elastotid elastolytic nature of the laminal defect-the only ex- plicit hypothesis known to us that, in a single expres- sion, meets both of the etiologic criteria described by Healey and Wilske: “aging” (albeit, actinic aging) and “some unidentified external stimulus.” The actinic hypothesis, first proposed more than 14 years ago and subsequently greatly expanded (7-9,18-22), is long overdue for open and critical appraisal, as well as independent evaluation, in accordance with the hon- ored tradition of science and medicine.
We believe our work on the “peculiar” degen- eration of the elastic lamina in GCA is relevant and valid. Our findings of typical actinic elastotic, baso- philic degeneration of the temporal lamina are neither accidental nor contrived, and we have published full- color micrographs which demonstrate the findings (7-9). We therefore respectfully invite the members of the ACR vasculitis criteria committee to contribute to the debate by disclosing the basis of their decision to omit all mention of the actinic component in their reports.
Not all investigators currently studying GCA ignore the potential contribution(s) of the elastic lam- ina; Cid et a1 (23) and Bengtsson (24) have given it notice. Recent epidemiologic studies of the GCA syn- drome by Machado et al(25), Cimmono et al(26), and Galetta et a1 (27) allude to the actinic factor as a possible explanation of their findings. The cutaneous
796 O’BRIEN AND REGAN
Figure 1. Probable incipient giant cell arteritis in a longitudinal section of a posterior ciliary artery stained with “controlled” hematoxylin and eosin. Spindle cells, some with prominent, lobulated nuclei (possibly, giant cells arising from myocytes), congregate near an abnormal internal elastic lamina that shows thickening, distortion, replication, and a diffuse medium- bluish reaction with fresh Hams hematoxylin. This laminal degeneration closely resembles actinic elastosis of the dermis and is therefore likely to ultimately lead to fragmentation and resorption (actinic elastolysis). Compared with the red cells at top, no normal, red, eosin- stained lamina is seen here. Note the fibrous intimal atherosclerosis-like plaque inside the abnormal lamina (original magnification x 100).
giant cell actinic granuloma, the original source and model for the actinic hypothesis of GCA, has been accepted as an entity and appears in new editions of leading textbooks, e.g., Pinkus’ Guide to Dermatohis- topathology, by Mehregan and Hashimoto ( I 11, and Rook/Wilkinson/Ebling’s Textbook of Dermatology, edited by Champion et al (17).
Dr. Lie’s statement that fragmentation oh the internal elastic lamella is not the essential feature, or in his own words, “not the sine qua non,” of the disease because it “occurs with regularity in all temporal arteries of the aged,” is not helpful and requires particular rebuttal. Most older people have damaged laminae, but inflammation, which may be episodic, seemingly occurs in only a genetically determined few. According to our findings, the damage is actinic and is analogous to the changes that occur in the skin over time. Everyone eventually experiences actinic elasto- tic, basophilic damage to the elastic fibers in sun- exposed skin, but only a few (possibly, genetically determined) experience inflammatory actinic granulo- mas. Thus in our view, elastotic degeneration, frag- mentation, and consequent episodes of inflammation and elastolysis are the essence of GCA.
Investigations focusing on the actinic hypothesis
In the belief that much current work on the immunology of GCA deals with secondary rather than primary factors, we suggest the following specific lamina-related projects with a sense of urgency, in view of the sociologic and preventive (9) implications of the long-neglected and unresolved actinic hypothesis.
I. Independent verijication of actinic laminal in- jury. We recommend independent repetition of our pathologic studies with the controlled hema- toxylin and eosin stain on diagnostic biopsy sections of temporal arteries taken from patients in whom temporal arteritis is suspected. Most, but not all, of our investigations have been per- formed on material obtained postmortem. When the temporal artery is excised, its orientation with respect to the environment should be marked, e.g., with India ink (7).
We have repeatedly stressed that most hema- toxylin and eosin staining methods commonly used do not reliably reveal actinic elastotic, baso-

ELASTIC TISSUE AND GCA 797
2.
3.
4.
philic (blue-staining) degeneration of the lamina or display unaltered red-staining (normal) lamina for meaningful comparison. (Summaries of the controlled method are given in references 7, 8, and 13, and a more detailed account can be obtained from the authors.) We are aware that some laboratories have had difficulty with the stain. The most important points for its success- ful performance are to use a quality-checked Harris hematoxylin that has not been previously used for other staining. The stain should be decolorized but left a little darker blue than usual, and the buffered eosin solution must be made up with eosin Y of color index 45380. We now use it at a concentration of 3%; to ensure that any remaining normal elastic tissue retains the red eosin color, the slides need to be differ- entiated only briefly (-15 seconds) in absolute ethyl alcohol (no weaker). Extraction of eosin ceases when the slides are transferred into a second absolute alcohol. The presence of lysozyme. Lysozyme is a new marker for actinic elastotic damage in the skin (28) and eye (29). It seems certain to prove useful for the display of the same damage in “exposed” arteries. Electron microscopy. As illustrated in our recent paper (9), it has been found that abnormal elastic laminae show fairly characteristic actinic changes in electron micrographs. Further work on this aspect, including immunoelectron micros- copy (29), would be helpful. A histochemical technique for demonstrating ac- tinically damaged elastin and elastotic tissue. Harris hematoxylin appears to be remarkably specific for actinic elastotic damage, if one care- fully excludes the much darker, granular appear- ance of calcified elastic tissue. Nevertheless, a sensitive immunohistochemical procedure spe- cific for elastotic degeneration would be invalu- able for diagnostic interpretation and further re- search.
The blue-staining reaction of abnormal elastin and elastic tissue probably reflects a biochemical abnormality (9) which may well be of antigenic degree and specificity. It is relevant here to mention that the same abnormal elastic tissue appears to stimulate autoimmune reactions in actinic granuloma and GCA.
We therefore suggest that immunologists may be able to develop a specific actinic elastotic antibody in animals and to adapt it for diagnostic
5 .
6.
use. To our knowledge, such a development has not been reported. Data for preparing antibodies against a variety of elastin-related antigens are given by Jacob et al (30). An actinic elastotic antigen would need to be prepared from samples of exposed dermis (e.g., from the neck or the back of the hands) that had been demonstrated to display advanced elastotic degeneration by the Harris hematoxylin stain. A diagnostic serum prepared from this antigen would doubtless con- tain antibodies to other dermal components, and these would most likely include antibodies to normal elastin. Removal of unwanted antibodies by absorption with normal human elastin antigen (from aorta or ligamentum nuchae) and with other antigens (possibly including whole, normal dermis) would likely be required. The serum would need to be tested on both normal and elastotic dermis, using a sensitive 2-stage (“sand- wich”) technique. Elastin-related serologic studies. In regard to the serologic manifestations of the GCA syndrome, we follow the French school (31), believing that there are opportunities for studies of anti-elastin antibodies, elastin peptides, elastases, elastase- inhibitors, and haptoglobin (19) in plasma, as well as desmosine (31) in urine. Basic research on the identity of damaging wave bands. Still more basic are research projects related to the identification of the electromag- netic wave band or bands that induce actinic elastotic degeneration in the elastic tissue of the skin and superficial arteries. We have already pointed out the probable suitability of the rodent tail for this investigation (9). Recently, we have found what may be a still more suitable test subject: the wing of the Australian “flying fox,” or “fruit bat,” Pteropus poliocephalus. In this animal, elastic tissue occurs in broad, solid bands within the thin wings. The arteries in the middle of the wing contain sharply defined internal elas- tic laminae. Other large bats are likely to have a similar anatomy and may be equally useful for exploring the pathogenesis of actinic damage in elastic tissues and its role in provoking the GCA syndrome.
Conclusion Evidence is presented that actinic (radiation)
damage to the radiation-sensitive internal elastic lam- ina of the temporal artery is the basis of giant cell
O’BRIEN AND REGAN
(temporal) arteritis. Suggestions for future work on this pathogenesis are made.
REFERENCES 1. Sage EH, Gray WR: Evolution of elastin structure,
Elastin and Elastic Tissue. Edited by LB Sandberg, WR Gray, C Franzblau. New York, Plenum Press, 1977
2. Kimmelstiel P, Gilmour MT, Hodges HH: Degeneration of elastic fibers in granulomatous giant cell arteritis (temporal arteritis). Arch Pathol 54: 157-168, 1952
3. Healey LA, Wilske KR: The Systemic Manifestations of Temporal Arteritis. New York, Grune & Stratton, 1978
4. Wawryk SO, Ayberk H, Boyd AW, Rode J: Analysis of adhesion molecules in the immunopathogenesis of giant cell arteritis. J Clin Pathol 44:497-501, 1991
5 . Hunder GG, Bloch DA, Michel BA, Stevens MB, Arend WP, Calabrese LH, Edworthy SM, Fauci AS, Leavitt RY, Lie JT, Lightfoot RW Jr, Masi AT, McShane DJ, Mills JA, Wallace SL, Zvaifler NJ: The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum 33: 1122-1 128, 1990
6. Lie JT and Members and Consultants of the American College of Rheumatology Subcommittee on Classifica- tion of Vasculitis: Illustrated histopathologic classifica- tion criteria for selected vasculitis syndromes. Arthritis Rheum 33: 1074-1087, 1990
7. O’Brien JP: A concept of diffuse actinic arteritis: the role of actinic damage to elastin in “age change” and arteritis of the temporal artery and in polymyalgia rheu- matica. Br J Dermatol98:1-13, 1978
8. O’Brien JP: Destruction of elastic tissue (elastolysis) as a link between atherosclerosis and the temporal arteritisl polymyalgia rheumatica syndrome: observations on an actinic factor in vascular disease. Pathol Biol (Paris)
9. O’Brien JP, Regan W: A study of elastic tissue and actinic radiation in “aging,” temporal arteritis, polymy- algia rheumatica, and atherosclerosis: the actinic storm in the modem world. J Am Acad Dermatol24:765-776, 1991
10. Unna PG: The Histopathology of the Diseases of the Skin. New York, MacMillan, 1896
11. Mehregan AH, Hashimoto K: Pinkus’ Guide to Derma- tohistopathology. Fifth edition. East Norwalk, CT, Ap- pleton & Lange, 1991
12. O’Brien JP: Actinic granuloma: an annular connective tissue disorder affecting sun- and heat-damaged (elasto- tic) skin. Arch Dermatol 111:460-466, 1975
13. O’Brien JP: Actinic granuloma: the expanding signifi- cance: an analysis of its origin in elastotic (“aging”) skin and a definition of necrobiotic (vascular), histiocytic, and sarcoid variants. Int J Dermatol 24:473-490, 1985
14. McGrae JD Jr: Actinic granuloma: a clinical, histopatho- logic and immunocytochemical study. Arch Dermatol 122:4347, 1986
15. Moulin G: Le granulome actinique. Ann Dermatol Ve- nereol 114:269-271, 1987
32:123-138, 1984
16. Steffen c : Actinic granuloma (O’Brien). J Cutan Pdthol 15:66-74, 1988
17. Burton JL: Disorders of connective tissue: actinic gran- uloma (syn. O’Brien’s granuloma), Rook/Wilkinson/ Ebling’s Textbook of Dermatology. Fifth edition. Edited by RH Champion, JL Burton, FJG Ebling. Oxford, Blackwell Scientific Publications, 1992
18. O’Brien JP: Solar and radiant damage to elastic tissue as a cause of internal vascular disease: protective aspects relating to the skin, temporal artery and eye. Australas J Dermatol 21:l-9, 1980
19. O’Brien JP, Argyle JC: The role of actinically provoked systemic elastolysis in polymyalgic vascular disease: a study based on serum fluorescence and haptoglobin. Am J Dermatopathol 3:273-286, 1981
20. O’Brien JP: A new risk factor in vascular disease: exces- sive solar and other actinic radiation in giant-cell arteritis and atherosclerosis. Int J Dermatol26:345-348, 1987
21. O’Brien JP: Vascular accidents after actinic (solar) expo- sure: an aspect of the temporal arteritis/polymyalgia rheu- matica syndrome. Int J Dermatol26:366-370, 1987
22. O’Brien JP: The temporal arteritis/polymyalgia rheumatica syndrome, Elastin and Elastases. Vol. 11. Edited by L Robert, W Homebeck. Boca Raton, FL, CRC Press, 1989
23. Cid MA, Campo E, Ercilla G, Palacin A, Vilaseca J, Villalta J, Ingelmo M: Immunohistochemical analysis of lymphoid and macrophage subsets and their immuno- logic activation markers in temporal arteritis: influence of corticosteroid treatment. Arthritis Rheum 32:884- 893, 1989
24. Bengtsson B-A: Giant cell arteritis. Curr Opin Rheuma- to1 2:6&65, 1990
25. Machado EBV, Gabriel SE, Beard CM, Michet CJ, O’Fallon WM, BaLlard DJ: A population-based case- control study of temporal arteritis: evidence for an association between temporal arteritis and degenerative vascular disease? Int J Epidemiol 18:836-841, 1989
26. Cimmino MA, Caporali R, Montecucco CM, Rovida S , Baratelli E, Broggini M: A seasonal pattern in the onset of polymyalgia rheumatica. Ann Rheum Dis 49521-523,1990
27. Galetta SL, Raps EC, Wulc AE, Farber MG, Plock GL, Nichols CW, Friedman HM: Conjugal temporal arteri- tis. Neurology 40:1839-1842, 1990
28. Albrecht S , From L, Kahn HJ: Lysozyme in abnormal dermal elastic fibers of cutaneous aging, solar elastosis and pseudoxanthoma elasticum. J Cutan Pathol 18:75- 80, 1991
29. Li Z-Y, Wallace RN, Streeten BW, Kuntz BL, Dark M: Elastic fiber components and protease inhibitors in pinguecula. Invest Ophthalmol Vis Sci 32: 15734585, 1991
30. Jacob MP, Fulop T. Robert L: Immunological properties of elastin, Elastin and Elastases. Vol. I. Edited by L Robert, W Homebeck. Boca Raton, FL, CRC Press, 1989
31. Robert L , Hornebeck W, editors: Elastin and Elastases. Vols. I and 11. Boca Raton, CRC Press, 1989