-
Access all the past APTEI Report articles at www.aptei.com
Clinical Library
Take the APTEI Report Quiz. Evidence-based answers are revealed
inside! Pain catastrophizing is the strongest predictor of chronic
pain rT rF
The best way to prevent patient litigations is to be perceived
as caring rT rF
Myofascial work on the calf muscle can reduce plantar heel pain
rT rF
Lumbar manipulation is more effective than PA mobs in prone rT
rF The latest systematic review concludes that lumbar manips are
not superior to other interventions for acute low back pain rT
rF
Texting with head down can lead to arthritis and even neck
surgeries rT rF
Aquatic therapy is an evidence-based intervention option for
chronic pain rT rF
History of smoking is a risk factor for developing Tennis Elbow
rT rF
Cervical dysfunctions are associated with persistent lateral
elbow pain rT rF
Placebo is derived from Latin meaning I shall please Over a
decade ago, 180 patients with painful knee OA were randomly
assigned to one of three interventions, receiving arthroscopic
debridement, arthroscopic lavage or placebo surgery. The patients
in the placebo group received only the small incisions but no scope
was inserted into their knees. At 6 weeks, 1 year and 2 years, they
were all equally better with no differences in their pain and
functional scores. In fact in the short-term, the placebo group had
slightly better functional scores. This is of course not to say all
surgery (or therapy) is placebo, but there is certainly a component
of placebo in everything we do. Brain scans of pain patients who
respond to pain killers, show that the cortex activations are
almost identical irrespective if they receive real or placebo
medications. A true medical breakthrough in the future will be
learning how to consistently activate the sections of the cortex
that produce the placebo effect. Now that would be truly
revolutionary. A quote from Voltaire, a witty and highly
respectable atheist French philosopher: "L'art de la mdecine
consiste distraire le malade pendant que la nature le gurit".
Translation: "The art of medicine consists of amusing the patient
while nature cures the disease." & References: Moseley JB et al
A controlled trial of arthroscopic surgery for osteoarthritis of
the knee. N Engl J Med. 2002 Jul 11;347(2):81-8.
For More Effective Physical Therapy Direct Patient Care
APTEI REPORT Advanced Physical Therapy Education Institute
Spring2015 Number 63 A report written by: Dr. Bahram Jam, PT
Edited by: Sophia Gilevich, PT
-
Access all the past APTEI Report articles at www.aptei.com
Clinical Library
Pain Catastrophization & Reference: Sullivan MJ et al .
Catastrophizing and perceived injustice: risk factors for the
transition to chronicity after whiplash injury. Spine 2011;36(25
Suppl):S244-249. & Reference: Quartana PJ, et al Pain
catastrophizing: a critical review. Expert review of
neurotherapeutics 2009;9(5):745-758. There are now over 1000
published studies that have demonstrated the association between
pain catastrophizing and increased pain severity, longer lasting
disability, greater psychological distress, and even slower
recovery from surgery. In fact, pain catastrophizing is now
considered to be the strongest predictor of problematic pain
outcomes. So is pain catastrophizing just caused by our way of
thinking? Can it just easily be reversed by changing our thought
patterns? Some studies have revealed on brain imaging that those
who catastrophize about their pain show a pattern of brain
activation different from non-catastrophizers. It is also
hypothesized that catastrophizing may actually increase
pro-inflammatory responses to noxious stimulation. In other words,
what is now being researched is how our thoughts can contribute to
inflammation plus the augmentation and spread of pain. Clinical
application: The best way to maximize placebo is to prevent
catastrophization in the first place. Prevent them from becoming a
VOMIT (Victim of Medical Imaging Technology). Some people appear to
not like the title VOMIT, so in my next version of the poster I
will be changing it to PIT (Pitfalls of Imaging Technology) and
telling people Dont fall in the pit If you wish, I can gladly send
you the jpg versions of the poster in French, Italian, German or
Norwegian. If you are able to translate it into any other language,
please be kind and let me know!
Pain Truth Book Cost is Covered $$ For all PTs in Ontario, it is
nice to know that The Pain Truth book sold to patients for $10-$15
is accepted by the insurance companies for MVA patients. When
completing the OCF-6 Claim Form and if completing the OCF-18 form
it is under Goods. The feedback on this book has been tremendous
and even if it helps reduce catastrophization in a fraction of the
patients, it has to be worth the few dollars. You may purchase the
book for $8 from www.aptei.com
Best Advice to Preventing Litigation & Reference: Beckman HB
et al The doctor-patient relationship and malpractice. Lessons from
plaintiff depositions. Arch Intern Med. 1994 Jun
27;154(12):1365-70.
This study analyzed a number of settled malpractice law suits by
patients against their doctors in the USA. They wanted to see what
exactly prompted each patient to sue their doctor. One would assume
that poor health outcome or MD negligence would be the major
reasons for deciding to sue. However, this study concluded that the
decision to litigate was associated with: *Perceived lack of caring
*Devaluing patient views *Discounting patient concerns *Perceived
unavailability *Poor delivery of information
-
Access all the past APTEI Report articles at www.aptei.com
Clinical Library
Based on this analysis, it appears that the majority of
litigations may have been prevented if the health care provider had
better communication and had been perceived as more caring. After
all, we as health care providers are human and to err is human, but
to be perceived as not caring when you err could mean a law suit.
There are few things in life that are more stressful than dealing
with a patient complaint or litigation against you. Fortunately PTs
have relatively low litigation issues; helping to keep our
malpractice insurance premiums low!
Ways to show patients that you Care & Reference: David
Walton, PT OPA Pain Symposium 2014 Ask patients during your
assessment, What do you think is causing all your pain? By asking
this simple question you are perceived as actually caring about
what they think and not dismissing their beleifs. At the end of
your subjective exam paraphrase and say, Let me know if Ive
understood you corrcetly, ...... Those two pieces of advice sound
so simple, but can be effective in directly demonstrating to your
patients that you are listening to them and care about what they
are telling you. Not only does this reduce the chance of
litigation, it will likely improve your clinical success with your
patients. If you are perceived as caring, the patient will want to
please you ...tada ...placebo!
Heel Pain & Myofascial Work
& Reference: Renan-Ordine R1, et al Effectiveness of
myofascial trigger point manual therapy combined with a
self-stretching protocol for the management of plantar heel pain: J
Orthop Sports Phys Ther. 2011 Feb;41(2):43-50. Treating heel pain
can be frustrating especially when new shoes, heel cushions,
orthotics, and self
stretching have failed. So you try ultrasound, shock wave,
acupuncture still no relief. Here is another suggestion: try some
myofascial work on the calf muscles. This RCT allocated 60 patients
with plantar heel pain to: i) Self-stretching + soft-tissue release
(STR) techniques to the calf muscles ii) Self-stretching program
only Result: After 4 weeks, the patients in group 1 had
significantly better outcomes in tenderness, pain and function than
those in group 2. Clinical Relevance: Consider doing some kind of
soft-tissue work on the gastroc-soleus complex muscles with your
future patients with heel pain. Personal Comment: With only
anecdotal evidence to support it, I have found Tissue Distraction
Release (TDR) with movement to be very effective for helping those
with either calf cramps or heel pain.
Warn the patient that it is very painful, but the treatment
lasts only 3 minutes and I typically do it for only 2 sessions;
when it works, it works immediately. You may download my free TDR
manual and order the cups from www.aptei.com I personally rarely
use any modalities other than the cups, (...and that is when I am
desperate). If you have not yet tried TDR on tight muscles, I
strongly recommend that you get a set of cups ASAP!
-
Access all the past APTEI Report articles at www.aptei.com
Clinical Library
Slump Stretching may be Effective & Reference: Nagrale AV et
al Effect of slump stretching versus lumbar mobilization with
exercise in subjects with non-radicular low back pain: a randomized
clinical trial. J Man Manip Ther. 2012 Feb;20(1):35-42. &
Reference: Cleland JA et al Slump stretching in the management of
non-radicular low back pain: Man Ther. 2006 Nov;11(4):279-86. I
consider Slump stretching quite aggressive and have been hesitant
about doing it on patients; however my hesitation to prescribe this
exercise may be unfounded. So far there are 2 studies supporting
it. Patients in India with non-radicular low back pain (LBP) were
randomly assigned to one of 2 groups. All patients attended 2 PT
sessions for 3 weeks. Group 1: PT included lumbar mobilizations and
progressive stabilization exercises Group 2: Received the same PT
treatments but with added self Slump stretching protocol
Slump stretching is performed with the patient in long sitting
on the floor and the feet against a wall to maintain neutral ankle
dorsiflexion. The neck and the trunk are fully flexed just to the
point of mild symptom provocation (not pain). The position is held
while the PT provides a mild cervical flexion over-pressure for 30
seconds and 5 repetitions. Patients are advised on performing the
same Slump stretch at home once a day. Result: Improvements in pain
and disability scores were significantly higher for the patients in
group 2 who received the Slump stretching exercises. Clinical
Conclusion: The addition of Slump stretching to other spinal
treatments may be beneficial for patients with non-radicular
LBP.
To Manip or not to Manip? & Reference: Learnan et al No
Differences in Outcomes in People with Low Back Pain Who Met the
Clinical Prediction Rule for Lumbar Spine Manipulation When a
Pragmatic Non-thrust Manipulation Was Used as the Comparator.
Physiotherapy Canada. 2014 Fall,66(4) 359-366 In the past decade,
the lumbar manipulation Clinical Prediction Rule (CPR) has become
quite popular. However studies seem to be knocking it down, such as
the one published recently in Physiotherapy Canada. It turns out,
patients who have low back symptoms of less than 16 days duration,
with no symptoms below the knee and who have low fear avoidance
beliefs do well with either manipulation or mobilizations. Perhaps
the CPR is just a powerful prognostic influence regardless of the
type of manual therapy they get. I love research, one year you
believe in something and the next decade science proves it
differently. Although I certainly promote spinal manipulations as
one of many PT treatment options, we have yet to have a study
showing that spinal manipulations are superior to mobilization
techniques proposed by Robin McKenzie, PT and Brian Mulligan, PT
(my heroes from New Zealand!)
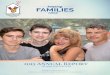
Comparing 3 Manual Therapy Techniques for LBP
& Reference: Cleland JA et al Comparison of the
effectiveness of three manual physical therapy techniques in a
subgroup of patients with low back pain who satisfy a clinical
prediction rule: a randomized clinical trial. Spine (Phila Pa
1976). 2009 Dec 1;34(25):2720-9. Patients with LBP who met the
Clinical Prediction Rule (CPR) for lumbar manipulation were
randomly allocated to receive one of three manual therapy
techniques for 2 sessions followed by 3 additional exercise
sessions.
-
Access all the past APTEI Report articles at www.aptei.com
Clinical Library
The three manual techniques were 1) General lumbar rotation
manipulation in supine
2) Specific lumbar rotation manipulation in side lying
3) Two sets of PA mobilizations over L4 and L5 spinous processes
for 60 seconds
Conclusion: The patients who received either of the manipulation
techniques had the same benefits at 1 week, 4 weeks and at 6 months
follow-up. However those who received the PA mobs had significantly
less improvements when compared to those who received the
manipulations. Personal Comments: With the greatest respect to the
father of manual therapy (G. Maitland, PT) I have yet to ever use
straight PAs on patients with LBP. I probably used them for a few
weeks after graduation 23 years ago, and then I abandoned them
after not seeing results. For the majority of my PT career I have
now mobilized only one way: mobilizations with movement (MWM) and
have abandoned any static PAs in prone.
My anecdotal experience is that I consistently get better
results with the correct MWM than I do with manipulations. I am
still awaiting a study to prove me right or wrong!
Latest Systematic Review on Manipulation and LBP
& Reference: Rubinstein SM et al Spinal manipulative therapy
for acute low back pain: an update of the cochrane review. Spine
(Phila Pa 1976). 2013 Feb 1;38(3):E158-77. Spinal manipulation
therapy (SMT) is performed on thousands of patients on a daily
basis worldwide. There are now hundreds of studies that have
investigated the efficacy of manipulation and dozens of systematic
reviews summarizing the study results. Here is a quote from the
latest systematic review. SMT is no more effective for acute low
back pain than inert interventions, sham SMT or as adjunct therapy.
SMT also seems to be no better than other recommended therapies.
(Rubinstein SM et al 2013) Clinical Relevance: If you dont practice
manipulation, its OK. There is no shortage of other potentially
effective treatment options. Aquatic Rehabis worth getting wet
for!
& Reference: Baena-Beato P et al Aquatic therapy improves
pain, disability, quality of life, body composition and fitness in
sedentary adults with chronic low back pain. Clin Rehabil. 2014
Apr;28(4):350-60. & Reference: Waller B1, et al Therapeutic
aquatic exercise in the treatment of LBP: a systematic review. Clin
Rehabil. 2009 Jan;23(1):3-14. I am impressed by the number of
studies supporting aquatic-therapy for so many conditions. It seems
like being in water can really be beneficial, its just hard getting
people into the water in the first place. This recent study
demonstrated that patients with chronic low back pain had
significant improvements in fitness levels, pain and disability
when compared to the wait list group. The patients attended 2
months of intensive aquatic therapy classes five times a week.
Group 1
Group 2
Group 3
-
Access all the past APTEI Report articles at www.aptei.com
Clinical Library
A systematic review quote, There was sufficient evidence to
suggest that therapeutic aquatic exercise is potentially beneficial
to patients suffering from chronic low back pain and
pregnancy-related low back pain. (Baena et al 2009) Clinical
Relevance: If your patients are serious about recovery and dont
mind getting into a pool, have them seriously consider aquatic
therapy. The evidence certainly supports it. Personal Comment: Two
years ago I recommended a 75 year old Scottish gentleman with
lumbar stenosis and a great sense of humour to consider
aquatherapy. He complied and went twice a week, and two years later
he is still going. I told him that I was so impressed that he was
still going to the pool as most men quit seeing that the classes
are filled with women. He responded with his thick Scottish accent,
Are you kidding me? Thats the reason I go, hahaha! A couple of
months ago I experienced various manual therapy techniques in a
warm pool done on me by Connie Jasinskas (an Exercise
Physiologist). I must admit that I was very impressed by the way I
felt after having my joint moved around in the water. Too bad a
warm pool is not feasible in every physio clinic. If you are
interested in practicing aquatic manual therapy, you can visit:
www.AquaStretchCanada.com
Beware of Texting Fear Mongering & Reference: Hansraj KK.
Assessment of stresses in the cervical spine caused by posture and
position of the head. Surg Technol Int. 2014 Nov;25:277-9. This
recent paper that regrettably got a lot of media attention (TV and
radio) simply looked at the loads placed on the cervical spine
during various angles of neck flexion simulating the typical
looking down posture while texting.
Using badly explained biomechanical calculations they published
a paper on something we intuitively knew as PTs. Basically at 0 of
neck flexion the load on the cervical spine is approximately 10lbs
which is the actual weight of the head. At 15 of neck flexion the
load increased to 27lbs. At 30 of neck flexion the load increased
to 40lbs. And finally by 60 of neck flexion (which the most typical
angle seen on people while texting and crossing the street), the
load on the cervical spine increased to 60lbs. The reason the load
is not felt immediately while texting is that the spine is
extremely adaptable and soon that posture feels normal and
comfortable. Assuming that a typical person spends at least 2 hours
a day looking down at their smart phone (a conservative estimate)
equates to over 700 hours of sustained neck flexion a year. After 5
years of texting there is now over 3000 hours of sustained stress
on the posterior neck structures. Moral of the story: Instead of
always looking down at your smart phone, once in a while lift the
phone up so it is in front of your eyes. Also do NOT text while
walking or when crossing the street. If you get hit by a car, youll
have more than just neck pain. Now the other side of the story:
Human beings have been looking down since we started eating,
cooking, reading, and playing chess. I got really annoyed when I
heard the author of the paper getting media attention by fear
mongering on the evening news. With no substantial evidence, he
boldly claimed that texting could lead to arthritis, degeneration
and even surgeries ...what nonsense!
-
Access all the past APTEI Report articles at www.aptei.com
Clinical Library
Evaluation & effective management of the cervical spine is
covered in the Advanced Cervico-thoracic program (4-day
course).
Smoking & Tennis Elbow & Reference: Titchener AG, et al
Risk factors in lateral epicondylitis (tennis elbow): a
case-control study. J Hand Surg Eur Vol. 2013 Feb;38(2):159-64. 4.
Other than repeated heavy gripping what are the other risk factors
for developing lateral epicondylalgia (LE)? This large
epidemiological study involved almost 5000 patients with LE plus
age and sex matched controls. Statistical analysis showed that the
risk factors associated with LE were (in order of risk)... 1.
Rotator cuff pathology 2. De Quervain's disease 3. Carpal tunnel
syndrome 4. Oral corticosteroid therapy 5. Previous smoking history
Interestingly risk factors NOT associated with LE were... Diabetes
mellitus, rheumatoid arthritis, alcohol intake, obesity and current
smoking. That seems odd, if you used to smoke but quit, you get
tennis elbow if you currently smoke and have not yet quit you dont
get tennis elbow. Its amazing how stats work. If death from cancer
is not enough reason, the fear of getting tennis elbow may be a
better deterrent for teenagers to never start smoking! Personal
Comment: This study failed to analyze if cervical pathology may be
a factor in the development of lateral elbow pain. Imagine if C6
nerve root is sensitized, it can mask as rotator cuff pathology,
elbow pain and De Quervains. Radial nerve may be sensitized even
when patients dont complain of any specific neck pain....read
on.
Lateral Elbow Pain Think C-Spine Dysfunction!
& Reference: Coombes BK et al Bilateral Cervical Dysfunction
in Patients With Unilateral Lateral Epicondylalgia Without
Concomitant Cervical or Upper Limb Symptoms: A Cross-Sectional
Case-Control Study. J Manipulative Physiol Ther. 2013 Dec 27. pii:
S0161-4754(13)00274-1. What is the prevalence of neck dysfunction
in patients with lateral epicondylalgia (LE)? To help answer this
important question, this study included healthy control subjects
and compared them to patients who reported of unilateral lateral
elbow pain and did NOT report of neck or any other upper limb
symptoms (e.g. numbess). The unblinded PT examiner noted that 36%
of the LE patients had some degree of paplpable neck pain and
articular dysfunctions (between C4-T2), and 41% had a positive
radial nerve neurodynamic test. Interestingly, a greater number of
tendener points and stiff segments in the c-spine was positively
associated with those with LE of longer duration. Also, a +ve
radial nerve neurodynamic test was positively associated with
greater severity of resting pain. Clinical Relevance: Every patient
with lateral elbow pain must first have their cervical spine
evaluated. If positive findings are present, address the neck and
dont waste time ultrasounding the elbow or strengthening and
stretching the wrist extensors!
Evaluation & management of lateral epicondylalgia is covered
in the Elbow & Wrist Complex course.
-
Access all the past APTEI Report articles at www.aptei.com
Clinical Library
22001155 AAPPTTEEII CCoouurrssee RReeggiissttrraattiioonn
&& VVOOMMIITT PPoosstteerr OOrrddeerr FFoorrmm Instructor:
Bahram Jam, PT
Full name (Please print clearly)
__________________________________ PT Reg.#_____ Full mailing
address_____________________________________________________
Contact Telephone Number (____)_____________E-mail:
VOMIT wall poster: ____ X $20=______ + $10 S&H + tax For
on-line registration, course objectives and exact details on
location, please visit:
www.aptei.com or
E-mail: [email protected] or Tel & Fax: 905-707-0819
Note: As these are primarily practical courses, please dress
appropriately No refunds 2 weeks or less prior to the course date
($30 is non-refundable)
CRITERIA FOR ACCEPTANCE
*Registered Physical Therapists or PT students awaiting
licensing
Total Tuition: $__________
($225 per course/day) Please mail or fax this form if paying
by credit card or send it with a cheque payable to APTEI To:
44 Sea Island Path, Thornhill, Ontario, CANADA, L3T 3A4
Tel & Fax: 905-707-0819 or Toll free: 1-866-APTEI-44
q Cheque payable to: APTEI
q Visa q M/C # ___________- ___________- ___________-
___________ exp _____/ _____
Authorization Signature: ___________________________ Date:
_________________
For automatic annual APTEI Report subscription renewal, please
visit: www.aptei.com/report
q Apr 11 q Apr 12
Foot & Ankle Complex Elbow, Wrist & Hand Complex
Edmonton, AB
q Apr 16-19 LUMBO-PELVIC CERTIFICATION PROGRAM (4-day)
(($$779955)) Moncton, NB
q Apr 24 Thoracic Spine (part I) Lethbridge, AB q Apr 25 q Apr
26
Foot & Ankle Complex Elbow, Wrist & Hand Complex
Calgary, AB
q May 1 q May 2 q May 3
Elbow, Wrist & Hand Complex Brockville, ON Montreal, QC
Ottawa, ON
q May 9 q May 10
Cervical Spine: Articular Dysfunction Cervical Spine: Neural
Tissue Jasper, AB
q May 9 FIBROMYALGIA: Debbie Patterson, PT
Calgary, AB q May 23 Edmonton, AB q May 23 q May 24
Elbow, Wrist & Hand Complex Cervical Spine: Neural Tissue
Vancouver, BC
q May 30 q May 31
Hip Complex Knee Complex North Bay, ON
q Jun 5 Lumbar Spine: Neural Tissue Niagara Falls
q Jun7 Thoracic Spine (Part II) Owen Sound q Jun 13 q Jun 14
Shoulder Complex (Part I) Shoulder Complex (Part II) Nanaimo,
BC
APTEI Acupuncture / Dry Needling (ADN) q Apr 25 q May 30 q Jun
27 q Jun 27 q Sep 19 q Oct 3 q Nov 21 q Dec 12 q Jan 16
ADN: Lower Extremity ADN: Lumbo-pelvic ADN: Examination ADN:
Introduction- Immediately Applicable Needling ADN: Introduction-
Immediately Applicable Needling ADN: Introduction- Immediately
Applicable Needling ADN: Upper Extremity ADN: Cervical &
Thoracic Spine ADN: Lower Extremity
Brampton ($295/ course) Instructor: Tom Kiroplis, Dip TCM Low
instructor to student ratio