Embed Size (px)
Citation preview
Appropriate Antibiotics use in CAP and HCAP at Sisters
Hospital in 2008.Syed Faraz Masood, MBBS
Nashat H. Rabadi, MD, FCCP

Community Acquired Pneumonia
• Common : 5 to 6 million cases/year• 20% are hospitalized ( 10% in ICU)• No. 1 cause of death from infectious disease• No. 6 cause of death in adults• Mortality rates :
– Outpatients = 1-5%– Inpatients = 12% ( higher in ICU- 50%)
• Costs : 9.7 billion
: inpatient – $7,517 vs. outpatient - $264

CAPDefinition
• CXR – infiltrate
• Auscultatory findings
• Signs of RTI– Cough +/- sputum– Fever or hypothermia– WBC

CAP - Pathogenesis
• Aspiration
• Inhalation
• Hematogenous
• Direct extension
• Reactivation

RESPIRATORY PATHOGENS IN CAP
Respiratory Pathogens in CAP

Risk Factors.
• Age.
• Smoking.
• Co-morbid Conditions.
• Poor Prognosis.– Pleural Effusion.– Bacteremia.

Cultures.
• Sputum Cx– Not needed as outpatient.– May or may not be needed inpatient.
• Blood Cx
• Urinary Antigens.

CURB - 65C – Confusion
U – Urea. BUN > 20
R – Respiratory rate > 30 / min
B – Blood pressure . SBP < 90 or DBP < 60
65 – Age > 65
Number of factors Mortality Rate 0 0.7%
1 2.1% 2 9.2% 3 14.5% 4 40% 5 57%

Management.
• Site of Care:– Inpatient vs. outpatient.– Floor vs. ICU.
• PSI
• CURB 65

Empirical Treatment
• Hospitalized Patients: – 2nd or 3rd generation Cephalosporins plus a Macrolide.– Floroquinolones.
• For all critically ill patients, – 2nd or 3rd generation Cephalosporin + Macrolide or
Floroquinolones – necessary to provide coverage for Legionella Pneumophilia.
– Change antibiotics – based on culture and sensitivity.

Nosocomial Pneumonia
• Hospital Acquired Pneumonia:– > 48 hours of admission to hospital.
• Ventilator associated Pneumonia.– > 48 hours of intubation.
Health-care Associated Pneumonia.
• Antimicrobial therapy in preceding 90 days.
• Hospitalization for 2 or more days in the preceding 90 days.
• Residence in a NH or an extended care facility.
• Home infusion therapy.• Chronic Dialysis within 30 days.• Immunosuppressive state and/or therapy.
Health-care Associated Pneumonia.
• Epidemiology extrapolated from HAP/VAP
• Second most common Nosocomial Infection.
• High morbidity / mortality.
• Increase hospital stay by 7-9 days.
• Excess cost of $ 40,000 per patient.
• Early VAP/HAP (<5 days)– Similarly as CAP– No MDR pathogens.
• Late VAP/HAP (>5 days) treated similarly as HCAP:– MDR pathogens.

Microbiology
• Polymicrobial.– Methicillin-resistant Staphylococcus Aureus.– Pseudomonas Aeruginosa.– Acinetobacter– E.Coli– Klebsiella Pneumoniae (ESBL).
Increased crude and attributable mortality associated with MDR pathogens.

Pathogenesis of HCAP
• Colonization: Lower Respiratory Tract.
• Aspiration; inhalation.
• Host-related: severity of illness, prior surgery.
• Environment-related: antibiotic exposure, medications, invasive devices.
• Host’s mechanical, humoral and cellular defenses.

Diagnosis
• Lower Respiratory Tract Cultures:– Sputum Cultures.– Endotracheal aspirates.– Bronchoscopy
• Broncho-alveolar Lavage (BAL).• Protected Brushed Specimen (PBS).
Empirical Treatment
• Anti-pseudomonal cephalosporins or
• Anti-pseudomonal cabrapenems or
• Beta-lactam/beta-lactamase inhibitorsAnd
• Anti-pseudomonal floroquinolones.PLUS
• Vancomycin or Linezolid.

HAP,VAP or HCAP SuspectedObtain Blood & Lower Respiratory Tract
Cultures
Early, Appropriate, Adequate Antibiotics
Assess Clinical Response Check Microbiology
Clinical Improvement (24-48 hrs)
YESNO
• Streamline Antibiotics.
• Treat Uncomplicated patients for 7 days. • Reassess & Follow up.
Search for Complications: Abscess or Empyema
Untreated Pathogen Non-Infectious Cause
ATS Consensus Statement. AJRCCM 171: 2005

Mortality in Nosocomial Pneumonia.
• Presence of MDR pathogens.
• Initial Inappropriate antibiotics.
• Co-morbidities.

Alvarez-Lerma F, et al. Alvarez-Lerma F, et al. Intensive Care MedIntensive Care Med. 1996;22:387-394.. 1996;22:387-394.Ibrahim EH, et al. Ibrahim EH, et al. ChestChest. 2000;118L146-155.. 2000;118L146-155.Kollef MH, et al. Kollef MH, et al. Chest.Chest. 1999; 115:462-474. 1999; 115:462-474.
Initial Inadequate Therapy Increases Mortality
Kollef MH, et al.Kollef MH, et al. Chest Chest. 1998;113:412-420.. 1998;113:412-420.Luna CM, et al. Luna CM, et al. Chest.Chest. 1997;111:676-685. 1997;111:676-685.Rello J, et al. Rello J, et al. Am J Respir Crit Care MedAm J Respir Crit Care Med. 1997;156:196-200. 1997;156:196-200..
0 20 40 60 80 100
% Mortality
Initial adequatetherapy
Initial inadequatetherapy
Luna, 1997Luna, 1997
Ibrahim, 2000Ibrahim, 2000
Kollef, 1998Kollef, 1998
Kollef, 1999Kollef, 1999
Rello, 1997Rello, 1997
Alvarez-Lerma,1996Alvarez-Lerma,1996

BAL=bronchoalveolar lavage. NS=Not significant.Luna CM, et al. Chest. 1997;111:676-685.
0
10
20
30
40
50
60
70
80
90
100
Pre-BAL Post-BAL Post-result
% M
orta
lity
No Antibiotic
Adequate Antibiotic
Inadequate Antibiotic
P<.001
P=NS
P=NS
Adequate Therapy Reduces Mortality Only If Selected Prior to Identification of the Pathogen

Research Question
• Appropriateness of CAP treatment at Sister’s Hospital.
• Appropriateness of HCAP treatment at Sister’s Hospital.
• Mortality.
• Length of Stay.

Method
• IRB approval.• HIPAA Compliance.• 248 charts reviewed with diagnosis of
pneumonia.• Retrospective analysis.• Single institution (Community Hospital setting).• 1 Calendar year. (Jan 1st – Dec 31st 2008)

Classification
0
50
100
150
Patients
Patients 143 90 10 2 3
CAP HCAP HAP VAPNo
PNA
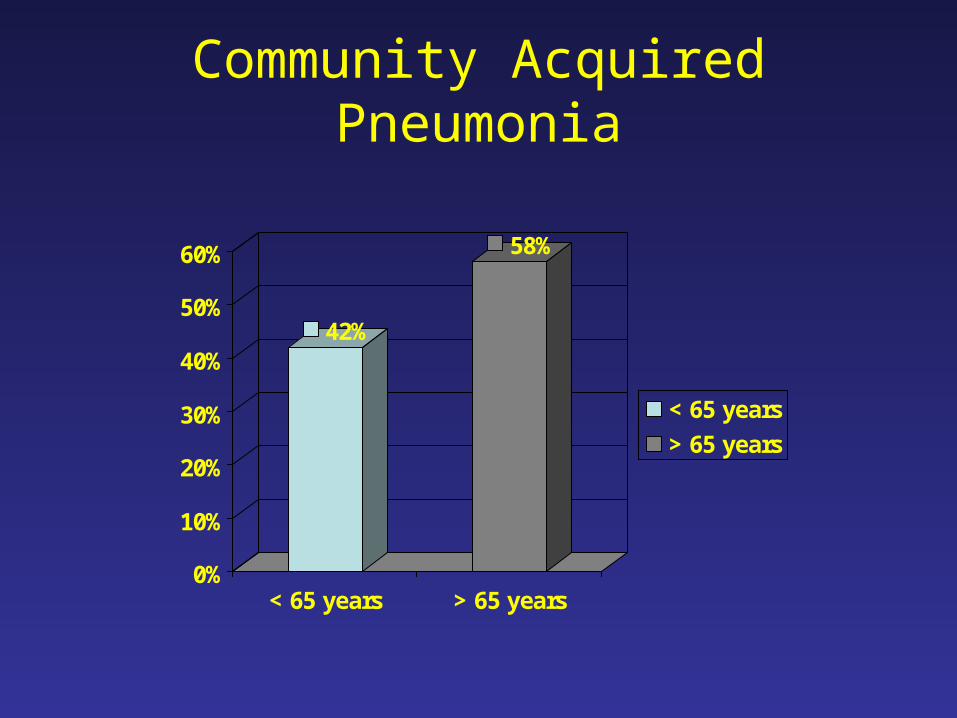
Community Acquired Pneumonia
42%
58%
0%
10%
20%
30%
40%
50%
60%
< 65 years > 65 years
< 65 years
> 65 years

Gender
54.5%
45.5%
40%
42%
44%
46%
48%
50%
52%
54%
56%
females males
females
males

Annual Frequency.
0
5
10
15
20
25
J F M A M J J A S O N D
Frequency

• Antibiotics administered in ER: 100%
• Appropriate antibiotics: 93.2%
• Cultures performed: 95.7%
• Positive Cultures: 8.1%

Coverage
101
42
0
20
40
60
80
100
120
NonHousestaff Housestaff
NonHousestaff
Housestaff

Cultures
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
Blood Cx Sputum Cx No Cultures
Blood Cx
Sputum Cx
No Cultures

Urinary Antigens for S.pneumo/Legionella
55%45% U-Ag done
U-Ag not done

Positive Cultures
0
20
40
60
80
100
120
140
Positive Cultures 11 4 2 1
Total Cultures 67 131 82
Sputum Blood U-antigens Others
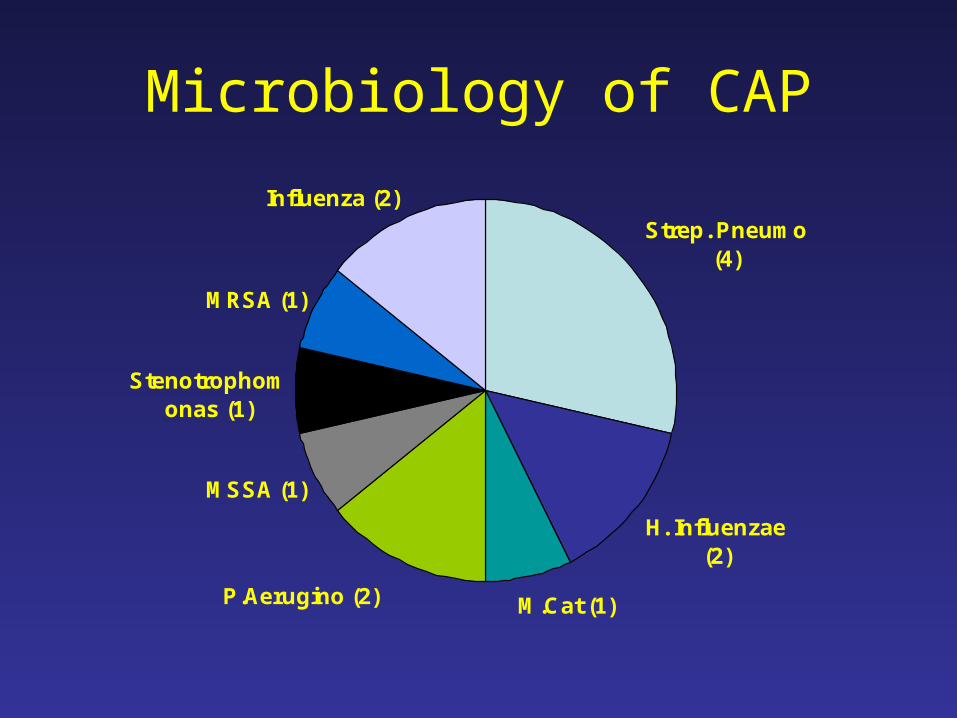
Microbiology of CAP
Stenotrophomonas (1)
MRSA (1)
Influenza (2)
MSSA (1)
P.Aerugino (2) M.Cat (1)
H. Influenzae (2)
Strep. Pneumo (4)
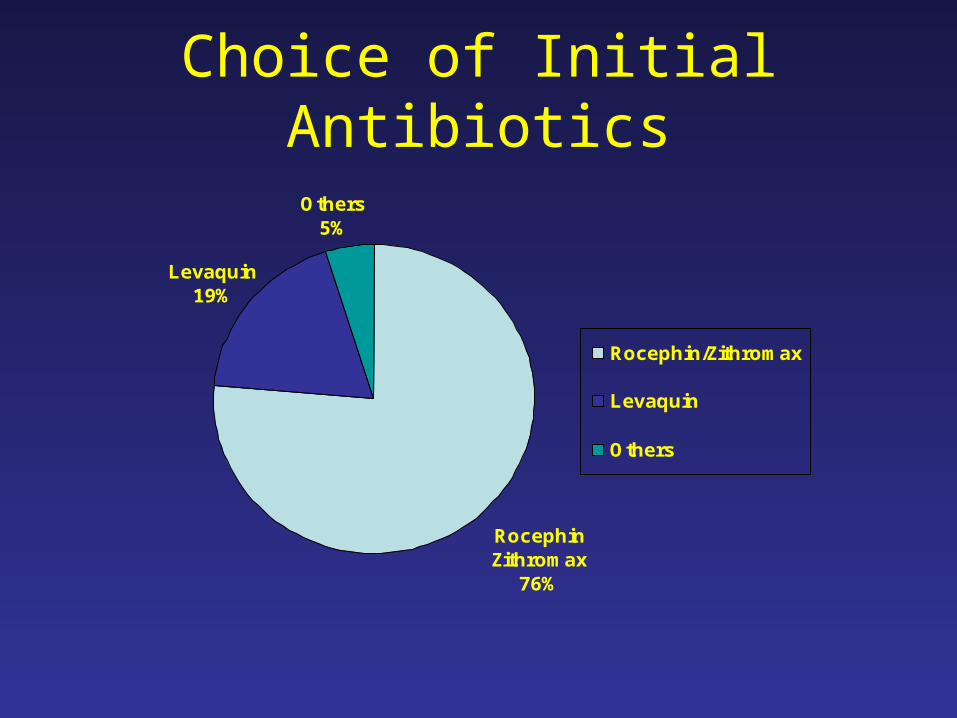
Choice of Initial Antibiotics
Others5%
Levaquin19%
RocephinZithromax
76%
Rocephin/Zithromax
Levaquin
Others

Mortality
– Number of Deaths: 6/143
– Mortality Rate: 4.2%
– Average Length of Stay: 5.8 days.
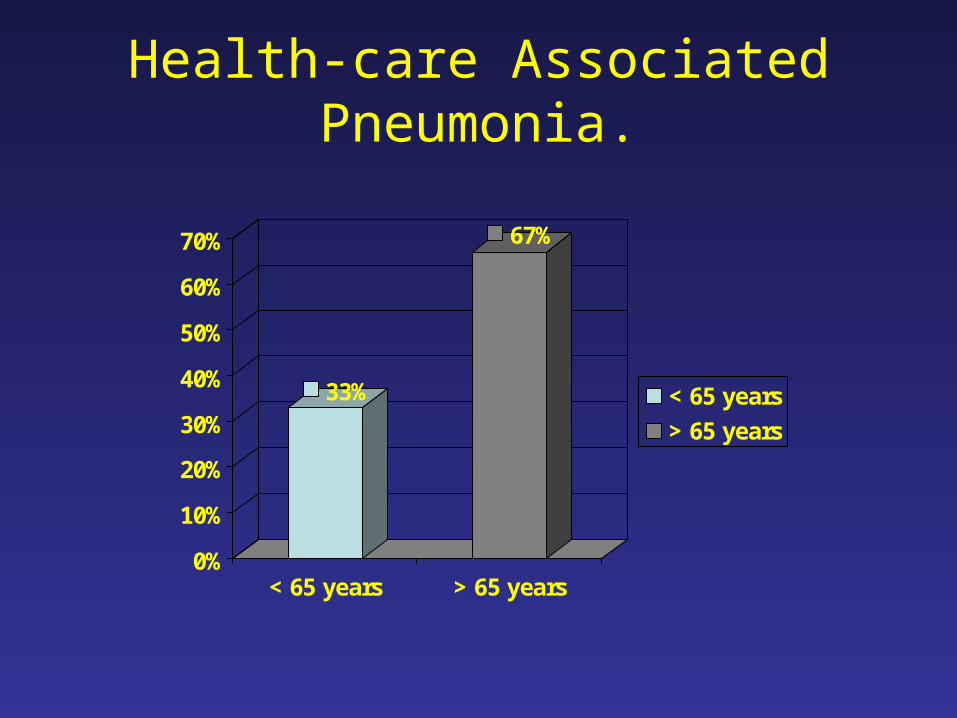
Health-care Associated Pneumonia.
33%
67%
0%
10%
20%
30%
40%
50%
60%
70%
< 65 years > 65 years
< 65 years
> 65 years

Gender
71%
29%
0%
10%
20%
30%
40%
50%
60%
70%
80%
females males
females
males

Annual Frequency
0
2
4
6
8
10
12
14
J F M A M J J A S O N D
Months.
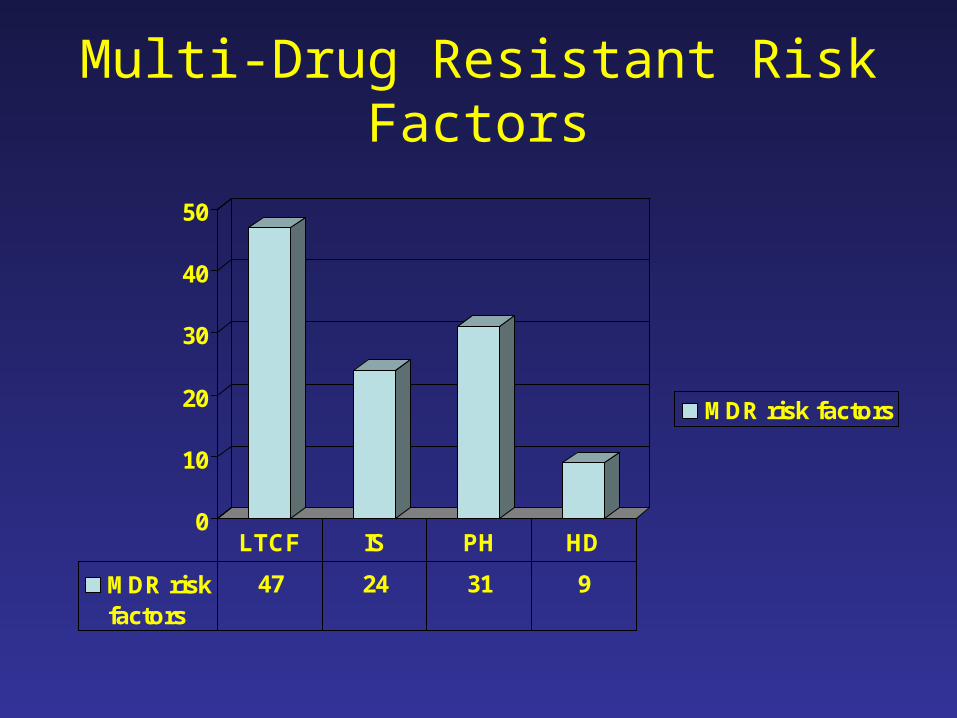
Multi-Drug Resistant Risk Factors
0
10
20
30
40
50
MDR risk factors
MDR riskfactors
47 24 31 9
LTCF IS PH HD

Initial Antibiotic Coverage in ER
0
20
40
60
80
Appropriate
'Partially'Appropriate
Inappropriate
Antibiotic 4 15 71
Appropriate'Partially'
AppropriateInappropriate

Initial Antibiotics Choice
Rocephin/Zithromax
(50)
Levaquin (14)
Vanco/Zosyn(1)
Vanco/ Zosyn/
Levaquin (1)Ceftriaxone
(4) Vanco/Imipenem (1)
Zyvox/Premaxin (1)
antibiotics

Other Combinations used…
• Vanco/Zithro• Levaquin/Genta/
Aztreonam.• Levaquin/Aztreonam• Levaquin/
Aztreonam/Clindamycin.
• Levaquin/Ceftazidime
• Aztreonam/Zithro• Levaquin/Zithro• Clindamycin• Primaxin/Zithromax• Levaquin/Clindamycin• Zosyn/Zithromax• Zosyn/Levaquin.

Coverage.
0
20
40
60
80
NonHousestaffCoverage
HousestaffCoverage
Coverage 65 25
NonHousestaff Coverage
Housestaff Coverage

Appropriately changed within 24 hours of admission
0
10
20
30
40
50
60
70
Antibiotics
Total Patients
Antibiotics 6 8
Total Patients 65 25
Non-housestaff Housestaff
9.2%
32%

Appropriate Change in Subgroups in Covered Patients.
0
2
4
6
8
10
Appropriate
Total
Appropriate 5 2 1 0
Total 10 10 2 3
LTCF IS PH HD

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Blood Cx
Sputum Cx
No cultures
Cultures. 95.50% 45.50% 2.22%
Blood Cx Sputum Cx No cultures

Urinary Antigens for S.pneumo/Legionella
51%49% U-Ag done
U-Ag not done

Positive Cultures
0
20
40
60
80
100
Positive Cultures
Total Cultures
Positive Cultures 11 4 5 1
Total Cultures 41 86 46
Sputum Blood U.Antigens Other

MicrobiologyCMV (1)Stenotropho
monas (1)Actinobacter (1)
MSSA (1)
P.Aerugino (3)
MRSA (6)
S.Pneumo (8)

• Appropriate antibiotics in ER: 4.4%
• Partially appropriate in ER: 15.5%
• Inappropriate antibiotics in ER: 78.8%
• Appropriate change in 24 hours: 16.27%

• Cultures performed: 97.7%
• Positive cultures: 18.1%
• Average Length of Stay: 9.5 days
• Average age: 71.2 years

Mortality
• Total Number of Deaths: 11/90
• Mortality Rate: 12.2%
• Deaths on Inappropriate Antibiotics: 9/11

Comparison
Variables HCAP CAPAge 71.2 years 69 years
Females 71.5% 54.5%
Sputum Cx yield 26.8% 16.2%
Blood Cx yield 4.6% 3.2%
Urinary Ag yield 10.8% 2.4%
Mortality 12.4% 4.2%
LOS 9.5 days 5.8 days
Housestaff covered
27.7% 29.3%

Where’s the problem?
Pneumonia
CAP HCAP
RECOGNIZE THE
DIFFERENCE

HAP,VAP or HCAP SuspectedObtain Blood & Lower Respiratory Tract
Cultures
Early, Appropriate, Adequate Antibiotics
Assess Clinical Response Check Microbiology
Clinical Improvement (24-48 hrs)
YESNO
• Streamline Antibiotics.
• Treat Uncomplicated patients for 7 days. • Reassess & Follow up.
Search for Complications: Abscess or Empyema
Untreated Pathogen Non-Infectious Cause
ATS Consensus Statement. AJRCCM 171: 2005

Strategies to Improve HCAP Outcomes
• Education.
• Order Sheets.
• De-escalation.
• Consultation.
• Re-evaluation.

References• National Center for Health Statistics. Health, United States, 2006, with chart book on trends in
the health of Americans. Available at: http://www.cdc.gov/nchs/data/hus/hus06.pdf. Accessed 17 January 2007.
• American Thoracic Society; Infectious Diseases Society of America. (2005). "Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia". Am. J. Respir. Crit. Care Med. 171 (4): 388–416.
• Alvarez-Lerma F, et alAlvarez-Lerma F, et al. . Modification of empiric antibiotic treatment in patients with pneumonia acquired in the intensive care unit. Intensive Care MedIntensive Care Med. 1996;22:387-394. 1996;22:387-394
• Ibrahim EH, et al.Ibrahim EH, et al. The Influence of Inadequate Antimicrobial Treatment of Bloodstream Infections on Patient Outcomes in the ICU Setting*. ChestChest. 2000;118L146-155.. 2000;118L146-155.
• Kollef MH, et al.Kollef MH, et al. Inadequate Antimicrobial Treatment of Infections: A Risk Factor for Hospital Inadequate Antimicrobial Treatment of Infections: A Risk Factor for Hospital Mortality Among Critically III Patients.Mortality Among Critically III Patients. Chest.Chest. 1999; 115:462-474. 1999; 115:462-474.
• Kollef MH, et al.Kollef MH, et al. The Influence of Mini-BAL Cultures on Patient Outcomes*: Implications for The Influence of Mini-BAL Cultures on Patient Outcomes*: Implications for the Antibiotic Management of Ventilator-Associated Pneumonia the Antibiotic Management of Ventilator-Associated Pneumonia ChestChest. 1998;113:412-420.. 1998;113:412-420.
• Luna CM, et al. Luna CM, et al. Impact of BAL Data on the Therapy and Outcome of Ventilator-Associated Impact of BAL Data on the Therapy and Outcome of Ventilator-Associated Pneumonia*.Pneumonia*. Chest.Chest. 1997;111:676-685. 1997;111:676-685.
• Rello J, et al. Rello J, et al. The Value of Routine Microbial Investigation in Ventilator-Associated The Value of Routine Microbial Investigation in Ventilator-Associated PneumoniaPneumonia Am J Respir Crit Care MedAm J Respir Crit Care Med. 1997;156:196-200.. 1997;156:196-200.

Acknowledgement
• Dr. Nashat Rabadi.
• Cliff Gadra and the Medical Records team.
• Dr. Varuna Nargunan.
• Danielle Casucci.
• Dr. Sateesh Satchidanand
• IRB team.

Thank You!