Embed Size (px)
Citation preview
h i l d i h i l d i Approach to International Adoptees in Approach to International Adoptees in the Family Practice Officethe Family Practice Office
Shawn M. Taylor, MD, FAAPShawn M. Taylor, MD, FAAPUKMD 1UKMD [email protected]@uky.edu
Grace J. Florence, RNGrace J. Florence, RN859859--323323--6426, Ext 3106426, Ext 310,,
[email protected]@uky.edu






Objectives For TodayObjectives For TodayObjectives For TodayObjectives For Today
Gain insight into health care issues of Gain insight into health care issues of internationally adopted children.internationally adopted children.y py p
Learn how to approach the medical Learn how to approach the medical Learn how to approach the medical Learn how to approach the medical evaluation of internationally adopted evaluation of internationally adopted childrenchildrenchildrenchildren

19 61319 61319,61319,613
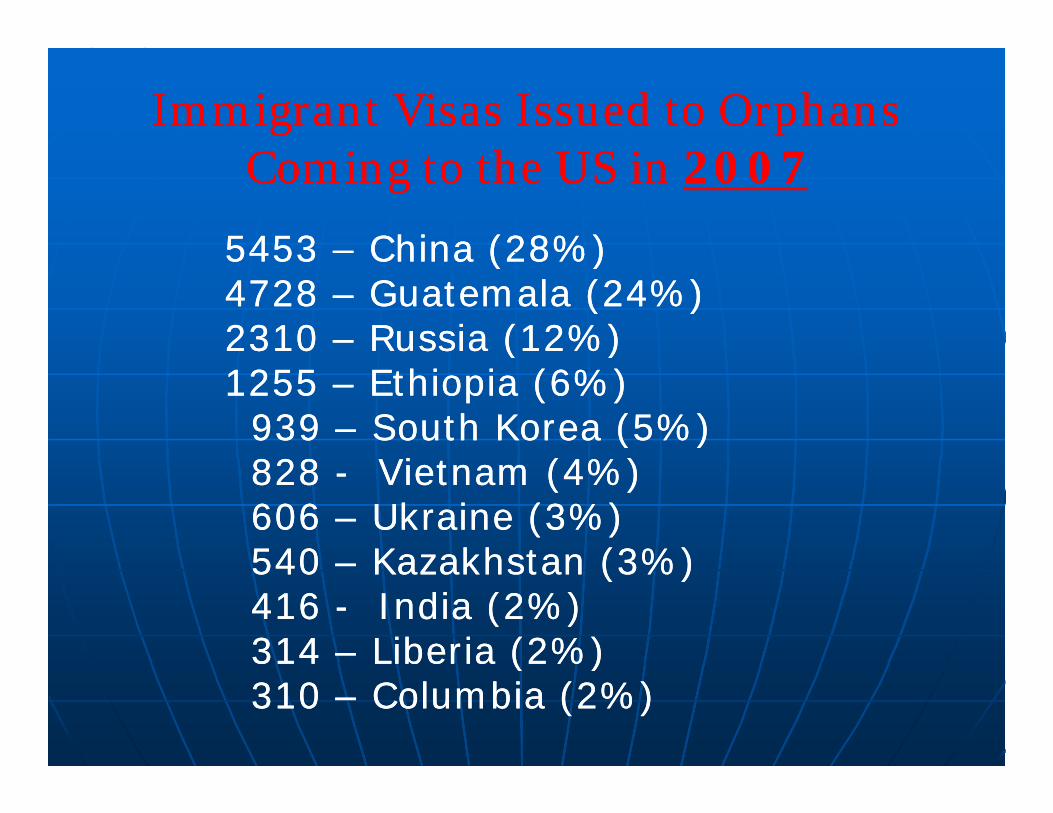
Immigrant Visas Issued to Orphans Immigrant Visas Issued to Orphans C i h US i C i h US i Coming to the US in Coming to the US in 20072007
5453 5453 –– China (28%)China (28%)5453 5453 China (28%)China (28%)4728 4728 –– Guatemala (24%)Guatemala (24%)2310 2310 –– Russia (12%)Russia (12%)( )( )1255 1255 –– Ethiopia (6%)Ethiopia (6%)939 939 –– South Korea (5%)South Korea (5%)828 828 Vi (4%)Vi (4%)828 828 -- Vietnam (4%)Vietnam (4%)606 606 –– Ukraine (3%)Ukraine (3%)540 540 Kazakhstan (3%)Kazakhstan (3%)540 540 –– Kazakhstan (3%)Kazakhstan (3%)416 416 -- India (2%)India (2%)314 314 –– Liberia (2%)Liberia (2%)314 314 Liberia (2%)Liberia (2%)310 310 –– Columbia (2%)Columbia (2%)
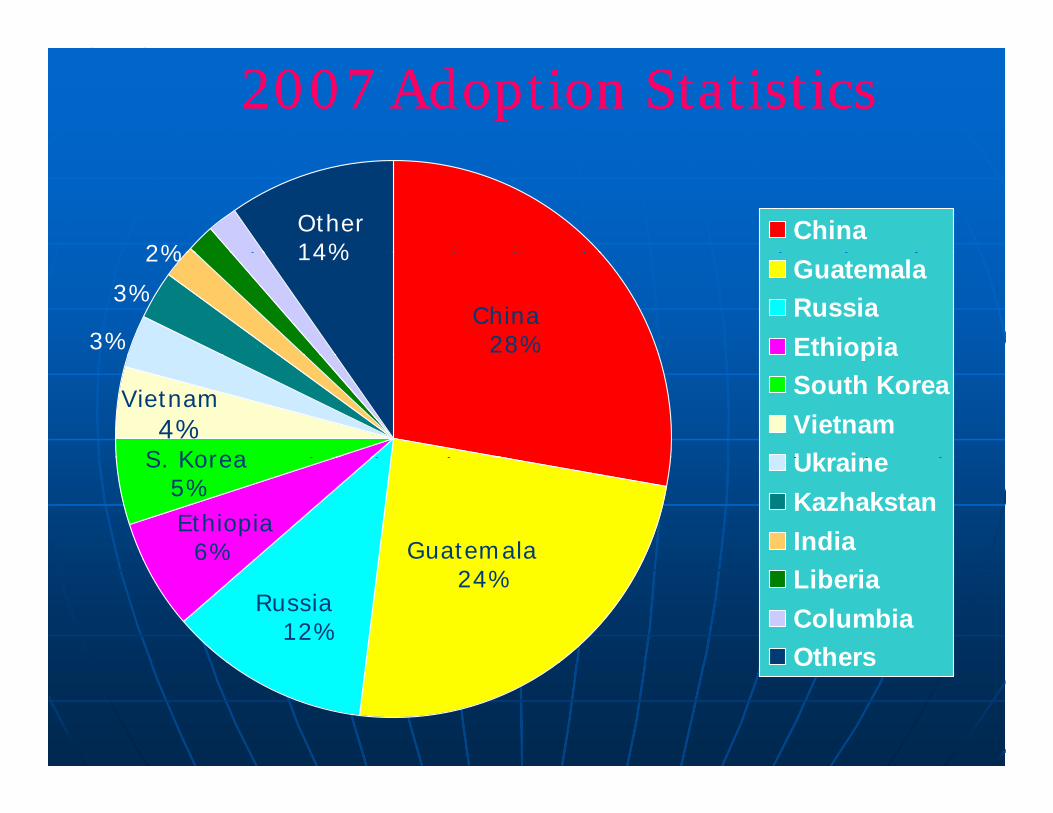
2007 Adoption Statistics2007 Adoption Statistics
China2%
Other14%
GuatemalaRussiaEthiopia
China28%3%
3%
2% 14%
EthiopiaSouth KoreaVietnamUkraineS Korea
Vietnam4%
UkraineKazhakstanIndiaGuatemala
S. Korea5%Ethiopia
6%LiberiaColumbiaOthers
24%Russia
12%Others
History of International AdoptionsHistory of International AdoptionsRooted in conflict/Humanitarian tragedies Rooted in conflict/Humanitarian tragedies
19491949 -- Helen and Carl DossHelen and Carl Doss
19551955 –– Holt FamilyHolt Family
19491949 Helen and Carl DossHelen and Carl Doss“Poster Family” for international adoptions“Poster Family” for international adoptions
19931993 –– The Hague Convention on Protection of The Hague Convention on Protection of Children and CoChildren and Co operation in Respect of operation in Respect of
19551955 Holt FamilyHolt Family
Children and CoChildren and Co--operation in Respect of operation in Respect of Intercountry AdoptionIntercountry Adoption
20072007 –– The Hague Convention fully ratified The Hague Convention fully ratified and implementedand implemented
At At leastleast 15% of all adoptions are international.15% of all adoptions are international.
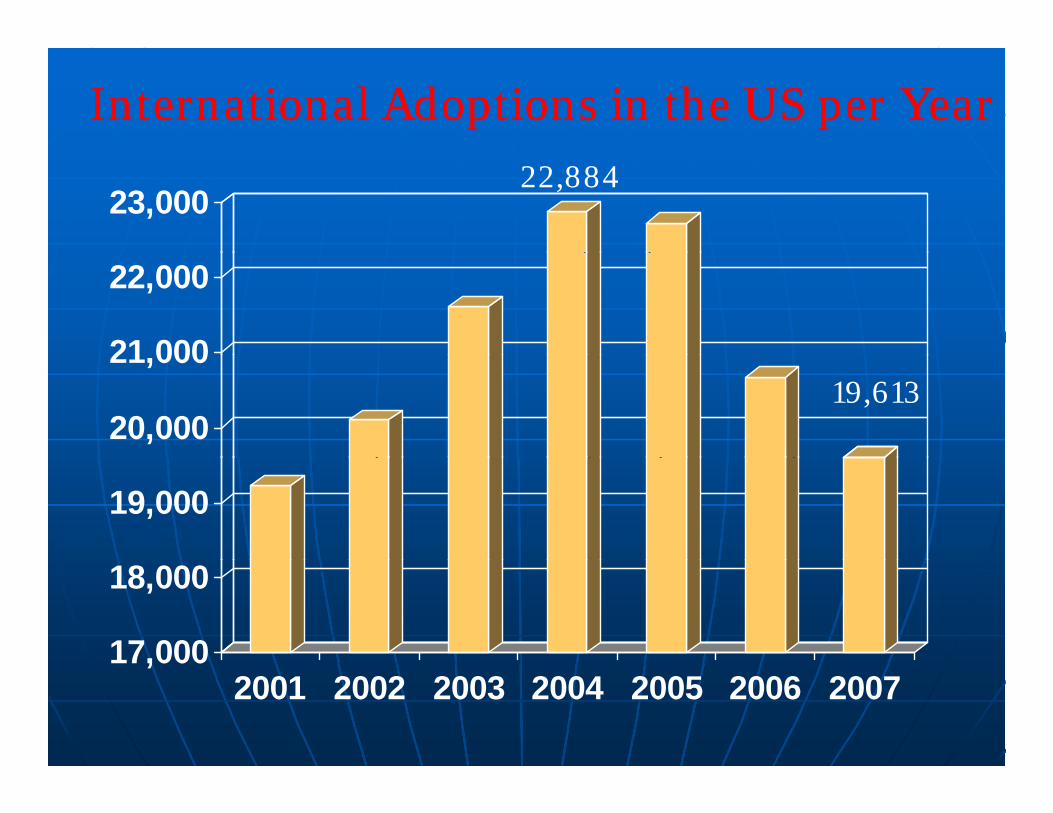
International Adoptions in the US per YearInternational Adoptions in the US per Year
23,00022,884
21 000
22,000
20,000
21,00019,613
19,000
17,000
18,000
17,0002001 2002 2003 2004 2005 2006 2007

Why People Adopt InternationallyWhy People Adopt Internationally
Desire entire spectrum of parenting experience Desire entire spectrum of parenting experience ––young a child as possible (40% vs. 3% <1yo)young a child as possible (40% vs. 3% <1yo)
Concerns about parental relationship Concerns about parental relationship Medical issues/Mental health issues (flawed)Medical issues/Mental health issues (flawed) Biologic and social drivesBiologic and social drives Biologic and social drivesBiologic and social drives
Religious beliefsReligious beliefsHumanitarian reasonsHumanitarian reasonsFamily originsFamily originsSpecial needsSpecial needsSkills ith ce tain disabilitiesSkills ith ce tain disabilitiesSkills with certain disabilitiesSkills with certain disabilities
Fundamental desire to parent


Characteristics of Internationally Characteristics of Internationally d d hildd d hildAdopted ChildrenAdopted Children
Most children now come from Most children now come from Most children now come from Most children now come from developing, resource poor countriesdeveloping, resource poor countries
Most live in orphanages as opposed to Most live in orphanages as opposed to p g ppp g ppfoster carefoster care
Infectious diseases are commonInfectious diseases are common Growth and developmental delays Growth and developmental delays
are very commonare very commonP h l i l ff f P h l i l ff f Psychological effects of Psychological effects of
institutionalizationinstitutionalization
Characteristics of Internationally Characteristics of Internationally Adopted Children (cont )Adopted Children (cont )Adopted Children (cont.)Adopted Children (cont.)
Children of all ages are available who need Children of all ages are available who need Children of all ages are available who need Children of all ages are available who need familiesfamilies
Circumstances of placement are similarCircumstances of placement are similarppImpoverishedImpoverishedUnwedUnwedRi ht t i t d f l tRi ht t i t d f l tRights terminated for neglectRights terminated for neglectAbandonmentAbandonmentChina China –– One Child PolicyOne Child PolicyChina China –– One Child PolicyOne Child Policy
Information about children is fairly Information about children is fairly incompleteincompleteco p eteco p ete
Institutions: How are Children Affected ?Institutions: How are Children Affected ?
Multiple care giversMultiple care givers Lack of stimulationLack of stimulation
Vi l ditVi l dit
Lack of consistent Lack of consistent medical caremedical care
Visual, auditoryVisual, auditory Malnutrition/poor Malnutrition/poor
nutritionnutrition
Physical and sexualPhysical and sexualabuseabuse
Mental health issuesMental health issues Propped bottlesPropped bottles Exposure to infectiousExposure to infectious
diseasesdiseases
Mental health issuesMental health issuesAbandonmentAbandonmentDeprivationDeprivationEmotional turmoilEmotional turmoil
Lead and toxinLead and toxinexposuresexposures
Chronic undiagnosedChronic undiagnosed
Emotional turmoilEmotional turmoilGrowth delaysGrowth delaysDevelopmental delaysDevelopmental delays
Chronic undiagnosedChronic undiagnosedear infectionsear infections
Institutions: Growth DelayInstitutions: Growth Delay
Children lose one month of growth for every 3Children lose one month of growth for every 3--4 months in an orphanage.4 months in an orphanage.
The longer in the orphanage the greater the The longer in the orphanage the greater the growth delays.growth delays.Reasons for the delays are multiReasons for the delays are multi factorialfactorial Reasons for the delays are multiReasons for the delays are multi--factorial.factorial.
From institutional delays From institutional delays –– 11stst weight, 2weight, 2ndnd
height 3height 3rdrd head circumferencehead circumferenceheight, 3height, 3 head circumferencehead circumference If all parameters delayed from birth think If all parameters delayed from birth think
syndrome, poor prenatal conditions or extreme syndrome, poor prenatal conditions or extreme y , p py , p pneglectneglect
Most children show rapid catchMost children show rapid catch--up growth up growth ithin 6ithin 6 12 month12 monthwithin 6within 6--12 months12 months
Growth Failure: Growth Failure: MicrocephalyMicrocephalyMicrocephalyMicrocephaly
30% of IAs 30% of IAs Poor head growth = poor brain growthPoor head growth = poor brain growth Long term cognitive difficultiesLong term cognitive difficulties Etiologies:Etiologies:
•• MalnutritionMalnutrition•• Extreme neglectExtreme neglect•• Extreme neglectExtreme neglect•• Brain abnormalityBrain abnormality•• Infection in utero (TORCH)Infection in utero (TORCH)•• Genetic syndromesGenetic syndromes•• FASFAS•• Preterm birthPreterm birth
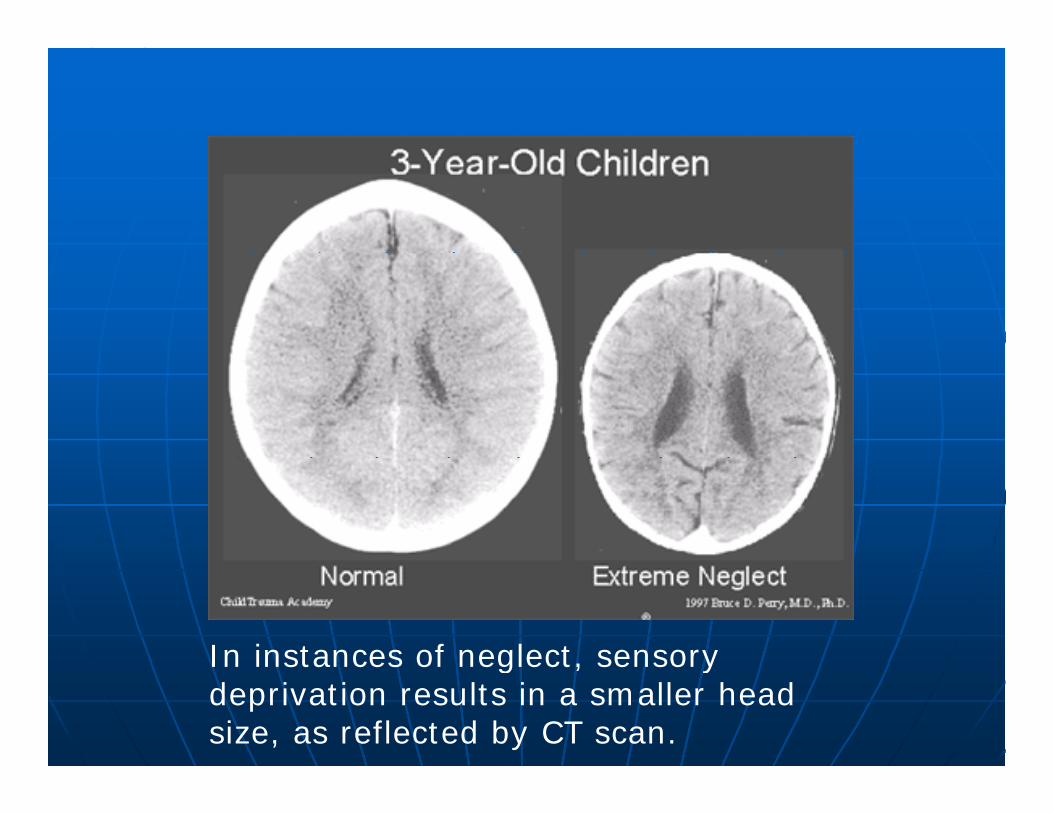
In instances of neglect, sensory In instances of neglect, sensory deprivation results in a smaller head size, as reflected by CT scan.
Institutions: Developmental DelaysInstitutions: Developmental DelaysInstitutions: Developmental DelaysInstitutions: Developmental Delays
Some form of developmental delay seen Some form of developmental delay seen 7575 80% f d t f ALL t i 80% f d t f ALL t i 7575--80% of adoptees from ALL countries, 80% of adoptees from ALL countries, even from foster care.even from foster care.
Up to 44% with global delaysUp to 44% with global delays Up to 44% with global delays.Up to 44% with global delays. The duration of institutionalization The duration of institutionalization
correlates with the correlates with the prevalence of prevalence of developmental developmental ppdelays.delays.
Gross Motor DelaysGross Motor DelaysGross Motor DelaysGross Motor Delays
Many are hypotonic and have Many are hypotonic and have Many are hypotonic and have Many are hypotonic and have decreased muscle strength.decreased muscle strength.Most obvious to parents and thus the Most obvious to parents and thus the Most obvious to parents and thus the Most obvious to parents and thus the most worrisome.most worrisome.U ll th l t i d th U ll th l t i d th Usually are the least serious and the Usually are the least serious and the shortest lasting.shortest lasting.
Fine Motor DelaysFine Motor Delays
Delayed MilestonesDelayed Milestones Orphanage PassivityOrphanage Passivity Orphanage PassivityOrphanage Passivity Lack of experienceLack of experience
•• Less desire to touch toys if Less desire to touch toys if yytouch is unpleasant or they touch is unpleasant or they are passiveare passive
•• Less ability to grab if their Less ability to grab if their y gy gtrunk is wobblytrunk is wobbly
•• Less exposure to toys Less exposure to toys VarietyVariety VarietyVariety Large and plasticLarge and plastic Not available to touchNot available to touch
St bi St bi ff ti ff ti Strabismus Strabismus –– affecting affecting eyeeye--hand coordination.hand coordination.
Language Delay SummaryLanguage Delay SummaryLanguage Delay SummaryLanguage Delay Summary
Frequently overlooked or discounted.Frequently overlooked or discounted. Frequently overlooked or discounted.Frequently overlooked or discounted. Most common delayMost common delay Often the slowest to overcomeOften the slowest to overcome Often the slowest to overcomeOften the slowest to overcome May impact overall cognitive May impact overall cognitive
development and behavior development and behavior development and behavior development and behavior regulation.regulation.
Not all language delay is because Not all language delay is because Not all language delay is because Not all language delay is because they are learning a new languagethey are learning a new language
Be sure they can hearBe sure they can hear Be sure they can hear.Be sure they can hear.
Social/Personal SkillsSocial/Personal SkillsSocial/Personal SkillsSocial/Personal Skills
A strength of adoptees.A strength of adoptees. Daily living skills are taught early.Daily living skills are taught early. Toilet training is instituted early.Toilet training is instituted early. Sharing, taking turns, cleaning up, etc. Sharing, taking turns, cleaning up, etc. Many are very social and engaging.Many are very social and engaging.

Basically…Basically…ALLALL international adoptees international adoptees
should be consideredshould be considered
Basically…Basically…
should be consideredshould be considered“special needs” “special needs”
Referral Paper WorkReferral Paper WorkReferral Paper WorkReferral Paper Work
Various forms of information: Various forms of information: Various forms of information: Various forms of information: written report, photo(s), video.written report, photo(s), video.Variable amounts of informationVariable amounts of information Variable amounts of informationVariable amounts of information
Much is subjective, not always Much is subjective, not always t l k f i f tit l k f i f tiaccurate, lack of informationaccurate, lack of information
Medical diagnoses in referral may Medical diagnoses in referral may differ from those in the USdiffer from those in the US
Objective data Objective data –– Ht, Wt, FOCHt, Wt, FOCjj , ,, ,
Referrals: Referrals: Assessing the informationAssessing the information
Review and plot growth parameters.Review and plot growth parameters.•• Growth parameters may be inaccurate or Growth parameters may be inaccurate or •• Growth parameters may be inaccurate or Growth parameters may be inaccurate or
dated.dated.•• Use of country specific growth charts.Use of country specific growth charts.
Assess pictures for Fetal Alcohol Assess pictures for Fetal Alcohol Syndrome, other genetic syndromes Syndrome, other genetic syndromes (e.g. Down syndrome).(e.g. Down syndrome).
Evaluate closely “special needs.”Evaluate closely “special needs.” Assess development, activity level, Assess development, activity level,
interaction. If concerned, request interaction. If concerned, request updatesupdatesupdates.updates.
Review blood, urine and other testing.Review blood, urine and other testing.
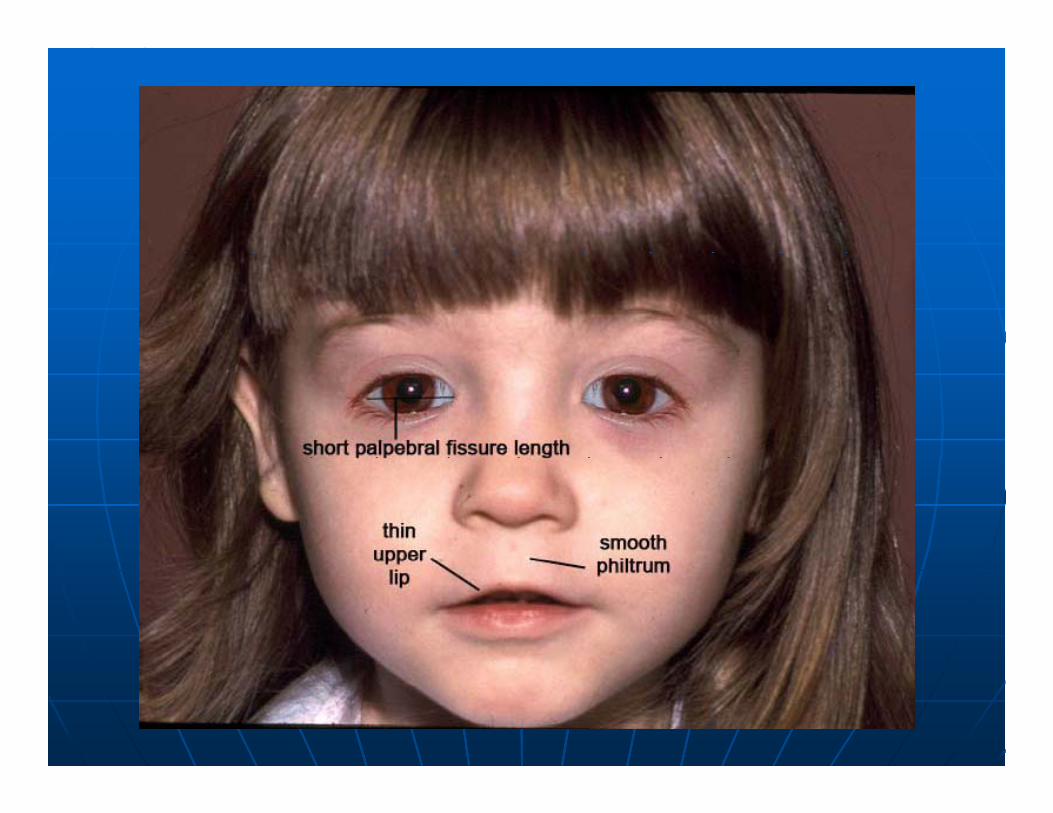
Fetal Alcohol Syndrome:Fetal Alcohol Syndrome:Typical Facial FeaturesTypical Facial Features
Small palpebral Small palpebral ff
Flattened midFlattened mid--face.face.fissuresfissures
Smooth philtrum.Smooth philtrum. Small head or chin.Small head or chin. Prominent ears.Prominent ears.
Thin upper lip.Thin upper lip. MicrocephalyMicrocephaly
Epicanthal foldsEpicanthal folds Short upturned Short upturned p yp y
nosenose
The first doctor visit :The first doctor visit : Review of past medical history, including Review of past medical history, including
all referral paperwork, labs, immunization all referral paperwork, labs, immunization records.records.
Complete Complete (means naked!)(means naked!) physical exam.physical exam. Comprehensive laboratory evaluation Comprehensive laboratory evaluation
(repeat previous tests done), screen for (repeat previous tests done), screen for TBTBTB.TB.
Developmental evaluationDevelopmental evaluation
Physicians need to remember thePhysicians need to remember thechild’s former life, not the current child’s former life, not the current
one.one.
Medical Issues: PostMedical Issues: Post--arrival Issuesarrival IssuesMedical Issues: PostMedical Issues: Post arrival Issuesarrival Issues
Skin disorders. Skin disorders. Skin disorders. Skin disorders. •• Scabies, lice, skin infections, tinea, Mongolian Scabies, lice, skin infections, tinea, Mongolian
spots.spots.
Infectious disease risks.Infectious disease risks.•• TB, Hepatitis B, Hepatitis C, HIV, syphilis, TB, Hepatitis B, Hepatitis C, HIV, syphilis,
iiparasites.parasites.
Other medical concerns.Other medical concerns.A i l d i i l th id kid A i l d i i l th id kid •• Anemia, lead poisoning, low thyroid, kidney Anemia, lead poisoning, low thyroid, kidney problems.problems.
Updating immunizationsUpdating immunizations Updating immunizations.Updating immunizations.
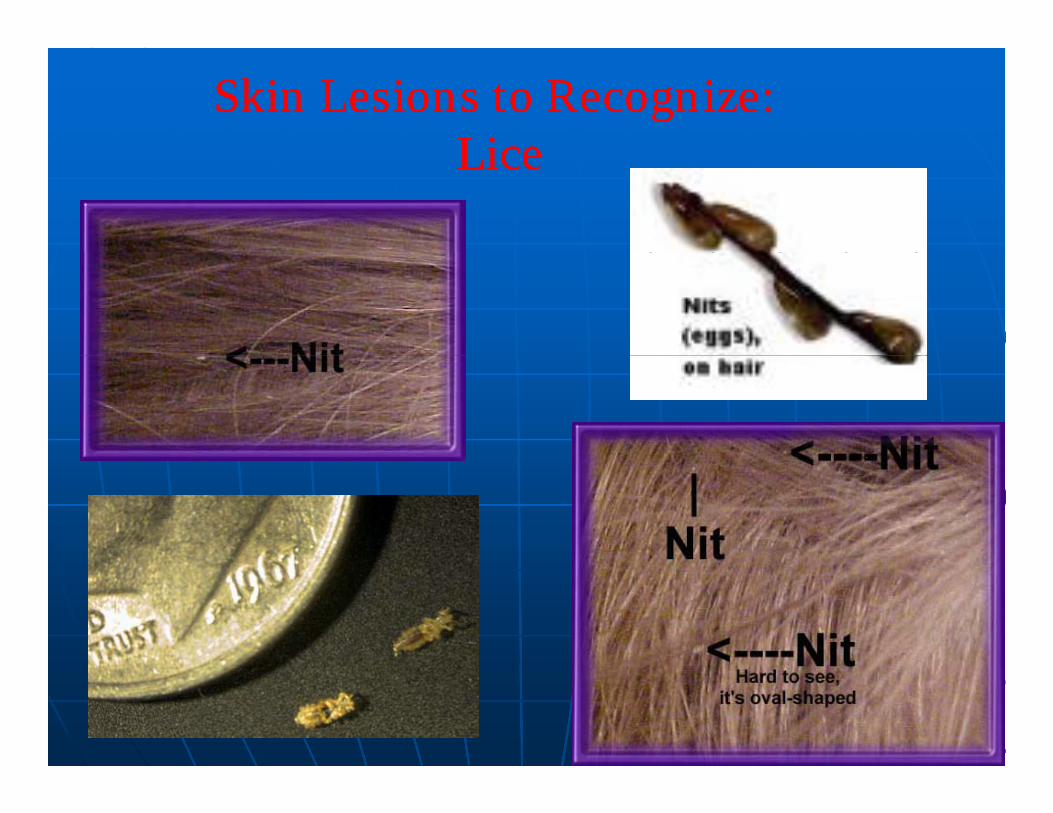
Skin Lesions to Recognize: Skin Lesions to Recognize: LiceLiceLiceLice

Skin Lesions to Recognize:Skin Lesions to Recognize:Mongolian SpotsMongolian Spots
May be on buttocks May be on buttocks May be on buttocks, May be on buttocks, back, arms, legs.back, arms, legs.Commonly seen in Commonly seen in Commonly seen in Commonly seen in dark complexioneddark complexionedchildren children X children children X
Documentation may avoid ylater misunderstandings.

Skin Lesions to Recognize: Skin Lesions to Recognize: ScabiesScabiesScabiesScabies
(www.aad.org)

Fungal InfectionsFungal InfectionsFungal InfectionsFungal Infections
Ti itiTinea capitisTinea corporis
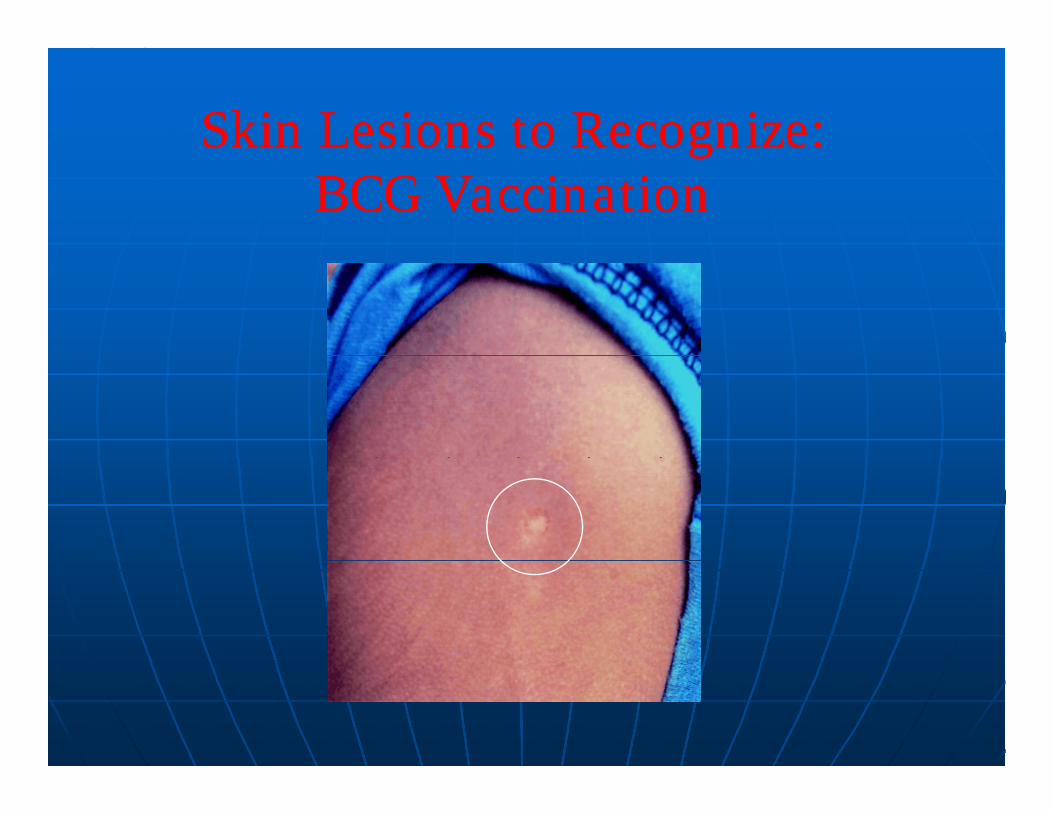
Skin Lesions to Recognize:Skin Lesions to Recognize:ggBCG VaccinationBCG Vaccination
Infectious DiseasesInfectious DiseasesInfectious DiseasesInfectious Diseases
TBTB TBTB Hepatitis BHepatitis B
H titi CH titi C Hepatitis CHepatitis C HIVHIV SyphilisSyphilis ParasitesParasites ParasitesParasites
Infectious Diseases: TBInfectious Diseases: TBInfectious Diseases: TBInfectious Diseases: TB
TB TB –– BCG (Bacilli ChalmetteBCG (Bacilli Chalmette--Guerin) Guerin) CG ( ac C a etteCG ( ac C a ette Gue )Gue )vaccine given in developing countries.vaccine given in developing countries.
A +PPD indicates likely infection with TB, A +PPD indicates likely infection with TB, dl f i BCG idl f i BCG iregardless of prior BCG vaccine.regardless of prior BCG vaccine.
Children rarely contagious Children rarely contagious –– LTBILTBIU t 30% iti f TB U t 30% iti f TB Up to 30% are positive for TB exposure or Up to 30% are positive for TB exposure or are infected. Few have the disease.are infected. Few have the disease.
ALL children should have a PPD on arrival ALL children should have a PPD on arrival ALL children should have a PPD on arrival ALL children should have a PPD on arrival andand 6 months later6 months later
If + then CXR and 9 months of INH.If + then CXR and 9 months of INH.
Infectious Disease: Blood borne pathogens:Infectious Disease: Blood borne pathogens:Hepatitis B Hepatitis C HIVHepatitis B Hepatitis C HIVHepatitis B, Hepatitis C, HIVHepatitis B, Hepatitis C, HIV
Increased incidence due to contaminatedIncreased incidence due to contaminateddl hi h di l dl hi h di l needles, higher disease prevalence needles, higher disease prevalence
(especially Russia, China).(especially Russia, China).Sp ead b blood and bod fl idsSp ead b blood and bod fl ids Spread by blood and body fluids.Spread by blood and body fluids.
Passed from mother to baby during birthPassed from mother to baby during birthHepatitis through blood/serum, wound exudates, Hepatitis through blood/serum, wound exudates, Hepatitis through blood/serum, wound exudates, Hepatitis through blood/serum, wound exudates,
sexual fluids, saliva (lowest virus concentration). sexual fluids, saliva (lowest virus concentration). HIV through blood/serum, sexual fluids, human milk, mucous HIV through blood/serum, sexual fluids, human milk, mucous
membranes membranes
Test at arrival Test at arrival andand 6 months later.6 months later. Most children do not have symptoms; risk is Most children do not have symptoms; risk is
lllong term long term Vaccinate household contacts for Hepatitis B.Vaccinate household contacts for Hepatitis B.
Infectious disease: SyphilisInfectious disease: SyphilisInfectious disease: SyphilisInfectious disease: Syphilis
Sexually transmitted diseaseSexually transmitted disease Sexually transmitted disease.Sexually transmitted disease. Test all children (RPR or VDRL), even Test all children (RPR or VDRL), even
if tested prior to adoptionif tested prior to adoptionif tested prior to adoption.if tested prior to adoption. If positive, needs further evaluation If positive, needs further evaluation
d t t td t t tand treatment.and treatment. Long term problems rare with correct Long term problems rare with correct
and early treatment.and early treatment.
Infectious Disease: Infectious Disease: i l hi l hIntestinal PathogensIntestinal Pathogens
Up to 25% + for GiardiaUp to 25% + for Giardia Up to 25% + for GiardiaUp to 25% + for Giardia May be present with/without diarrhea.May be present with/without diarrhea. Once home should collect 1Once home should collect 1--3 stools 3 stools Once home, should collect 1Once home, should collect 1 3 stools 3 stools
(minimum 48 hours spacing) to evaluate.(minimum 48 hours spacing) to evaluate. Repeat stool test after treatment; Repeat stool test after treatment; Repeat stool test after treatment; Repeat stool test after treatment;
retreatment may be necessary.retreatment may be necessary. High level of concern, but rarely serious to High level of concern, but rarely serious to High level of concern, but rarely serious to High level of concern, but rarely serious to
child/family.child/family. May show up years after arrival home.May show up years after arrival home.y p yy p y
Additional Screening TestsAdditional Screening TestsAdditional Screening TestsAdditional Screening Tests
Complete blood count Complete blood count Complete blood count Complete blood count Lead levelLead level
M t b li M t b li Metabolic screenMetabolic screen Thyroid studiesThyroid studies G6PDG6PD Vaccination titersVaccination titers Consider tests for rickets, iron Consider tests for rickets, iron
deficiency, CMP, and things peculiar to deficiency, CMP, and things peculiar to th t f i ith t f i ithe country of origin.the country of origin.
ImmunizationsImmunizationsImmunizationsImmunizations
Many are inadequate inaccurate or Many are inadequate inaccurate or Many are inadequate, inaccurate, or Many are inadequate, inaccurate, or unacceptable.unacceptable.
Accept only written documentation.Accept only written documentation.p yp y•• Assess dates given, interval between vaccine Assess dates given, interval between vaccine
doses, age at time vaccines were given.doses, age at time vaccines were given.D t i t D t i t Due to improper storage or Due to improper storage or administration, child may not be immune administration, child may not be immune despite having received vaccines.despite having received vaccines.desp te a g ece ed acc esdesp te a g ece ed acc es
When in doubt, repeat vaccines (low risk) When in doubt, repeat vaccines (low risk) or check antibody levels. or check antibody levels.

Developmental evals and referralsDevelopmental evals and referralsDevelopmental evals and referralsDevelopmental evals and referrals Early intervention services.Early intervention services.yy
•• First Steps (KY) <3yoFirst Steps (KY) <3yo
Consider other evals for more involved Consider other evals for more involved children:children:•• Speech and language therapy, physical therapy, Speech and language therapy, physical therapy,
ti l th i t ti ti l th i t ti occupational therapy, sensory integration occupational therapy, sensory integration therapy.therapy.
Older children: school involvement Older children: school involvement earlyearly Older children: school involvement Older children: school involvement early.early.
Other Recommended EvaluationsOther Recommended EvaluationsOther Recommended EvaluationsOther Recommended Evaluations
Hearing exam within 4Hearing exam within 4 6 months6 months Hearing exam within 4Hearing exam within 4--6 months.6 months.44--8% hearing loss 8% hearing loss –– URIs, URIs, chronic OM perforations congenital chronic OM perforations congenital chronic OM, perforations, congenital chronic OM, perforations, congenital infections, FMHinfections, FMH
Vision exam within 12Vision exam within 12--18 months18 months Vision exam within 12Vision exam within 12 18 months.18 months.1010--25% visual problems25% visual problems
Dental evaluation for children with Dental evaluation for children with Dental evaluation for children with Dental evaluation for children with teeth.teeth.
Mental health evaluation if needed. Mental health evaluation if needed.
Love may not be enough…Love may not be enough…
Be prepared for the challenges:Be prepared for the challenges:•• Few children escape unscathed.Few children escape unscathed.•• Help families identify community resources. Help families identify community resources.
f l d llf l d ll Be optimistic: Most families do well.Be optimistic: Most families do well. Success will be a result of a family’s Success will be a result of a family’s
it t t hildit t t hildcommitment to a child.commitment to a child. Be willing to enlist the Be willing to enlist the
h l f f lh l f f lhelp of professionals.help of professionals. Support groups.Support groups.
Resources: For Health Care Resources: For Health Care ProfessionalsProfessionalsProfessionalsProfessionals
The Handbook of International Adoption Medicine: A The Handbook of International Adoption Medicine: A Guide for Physicians Parents and ProvidersGuide for Physicians Parents and Providers by Laurie by Laurie Guide for Physicians, Parents, and ProvidersGuide for Physicians, Parents, and Providers by Laurie by Laurie C. Miller (C. Miller (PaperbackPaperback -- Dec 16, 2004)Dec 16, 2004)
Pediatric Clinics of North America Pediatric Clinics of North America Volume 52, Issue 5, Volume 52, Issue 5, , ,, ,Pages 1221Pages 1221--1532 (October 2005)International Adoption: 1532 (October 2005)International Adoption: Medical and Developmental Issues Edited by Lisa H. Medical and Developmental Issues Edited by Lisa H. Albers, Elizabeth D. Barnett, Jerri Ann Jenista, Dana E. Albers, Elizabeth D. Barnett, Jerri Ann Jenista, Dana E. Johnson Johnson
Medical Evaluation of Internationally Adopted Medical Evaluation of Internationally Adopted Children for Infectious DiseasesChildren for Infectious DiseasesRed Book 2006: 182Red Book 2006: 182--183 2007183 2007Red Book 2006: 182Red Book 2006: 182--183. 2007.183. 2007.
Julia M. Bledsoe and Brian D. JohnstonJulia M. Bledsoe and Brian D. JohnstonPreparing Families for International Adoption,Preparing Families for International Adoption,p g pp g pPediatrics in Review., Jul 2004; 25: 242 Pediatrics in Review., Jul 2004; 25: 242 -- 250. 250.

Kentucky Children’s Hospital Kentucky Children’s Hospital Kentucky Children s Hospital Kentucky Children s Hospital International Adoption ClinicInternational Adoption Clinic
Contacts:Contacts:
[email protected]@uky.eduUKMD 1UKMD 1--800800--888888--55335533
[email protected]@uky.edu859859 323323 6426 E 3106426 E 310859859--323323--6426, Ext 3106426, Ext 310