Embed Size (px)
Citation preview

Contents lists available at ScienceDirect
Biochemical Pharmacology
journal homepage: www.elsevier.com/locate/biochempharm
Appraising the “entourage effect”: Antitumor action of a pure cannabinoidversus a botanical drug preparation in preclinical models of breast cancer
Sandra Blasco-Benitoa,b,⁎,1, Marta Seijo-Vilaa,b,1, Miriam Caro-Villalobosa,b, Isabel Tundidora,b,Clara Andradasa,2, Elena García-Taboadaa, Jeff Wadec, Stewart Smithc, Manuel Guzmána,d,Eduardo Pérez-Gómeza,b, Mara Gordonc, Cristina Sáncheza,b,⁎
a Complutense University, Madrid, Spainb Instituto de Investigación Hospital 12 de Octubre, Madrid, Spainc Aunt Zelda’s, CA, United Statesd Instituto Ramón y Cajal de Investigación Sanitaria, CIBERNED and IUIN, Madrid, Spain
A R T I C L E I N F O
Keywords:CannabinoidBreast cancerTHCBotanical drug preparationChemotherapyTargeted therapy
A B S T R A C T
Breast cancer is the second leading cause of death among women. Although early diagnosis and development ofnew treatments have improved their prognosis, many patients present innate or acquired resistance to currenttherapies. New therapeutic approaches are therefore warranted for the management of this disease. Extensivepreclinical research has demonstrated that cannabinoids, the active ingredients of Cannabis sativa, trigger an-titumor responses in different models of cancer. Most of these studies have been conducted with pure com-pounds, mainly Δ9-tetrahydrocannabinol (THC). The cannabis plant, however, produces hundreds of othercompounds with their own therapeutic potential and the capability to induce synergic responses when com-bined, the so-called “entourage effect”. Here, we compared the antitumor efficacy of pure THC with that of abotanical drug preparation (BDP). The BDP was more potent than pure THC in producing antitumor responses incell culture and animal models of ER+/PR+, HER2+ and triple-negative breast cancer. This increased potencywas not due to the presence of the 5 most abundant terpenes in the preparation. While pure THC acted byactivating cannabinoid CB2 receptors and generating reactive oxygen species, the BDP modulated differenttargets and mechanisms of action. The combination of cannabinoids with estrogen receptor- or HER2-targetedtherapies (tamoxifen and lapatinib, respectively) or with cisplatin, produced additive antiproliferative responsesin cell cultures. Combinations of these treatments in vivo showed no interactions, either positive or negative.Together, our results suggest that standardized cannabis drug preparations, rather than pure cannabinoids, couldbe considered as part of the therapeutic armamentarium to manage breast cancer.
1. Introduction
It is estimated that 12% women will develop breast cancer at sometime during their lives [1]. Although the mortality rates associated tothis disease are globally decreasing due to improvement in therapiesand early diagnosis, there is an urgent need for new treatments. First,some patients show innate resistance to standard therapies, and othersacquire resistance with time despite initial responsiveness. In addition,breast cancer is a very heterogeneous disease in terms of molecularfeatures, prognosis, and treatments, and some specific subgroups pre-sent very poor outcomes and response to current therapies. Althoughsub-classification of breast cancer is a field in constant growth [2,3],
treatment decisions are presently made based on the presence of a verylimited number of predictive markers, namely estrogen and proges-terone receptors (ER and PR, respectively), and the HER2 oncogene.Thus, tumors with ER/PR expression, which represent roughly 75% ofall breast cancer cases, are treated with therapies aimed at switching offthe estrogenic signaling, either by targeting the receptors themselves[with selective estrogen receptor modulators (SERMs) as tamoxifen, apartial agonist of ER] or the endogenous synthesis of these hormones(with aromatase inhibitors) [1,3]. Tumors with overexpression ofHER2, a member of the epidermal growth factor (EGF) receptor tyr-osine kinase family, represent approximately 17% of all diagnosedbreast cancer cases, and are treated with therapies aimed at hampering
https://doi.org/10.1016/j.bcp.2018.06.025Received 30 May 2018; Accepted 21 June 2018
⁎ Corresponding authors at: Dept. Biochemistry and Molecular Biology, School of Biology, Complutense University, C/ José Antonio Nováis, 12, 28040 Madrid, Spain.
1 Contributed equally to this work.2 Present address: Telethon Kids Institute, Perth, Australia.
E-mail addresses: [email protected] (S. Blasco-Benito), [email protected] (C. Sánchez).
Biochemical Pharmacology 157 (2018) 285–293
Available online 27 June 20180006-2952/ © 2018 Elsevier Inc. All rights reserved.
T

HER2 pro-oncogenic signaling [4]. Targeted therapies include mono-clonal antibodies against different extracellular domains of HER2 (astrastuzumab and pertuzumab), and small molecule tyrosine kinase in-hibitors (as lapatinib and neratinib) that block the kinase activity of theintracellular domain of HER2, which is essential for receptor activation[4,5]. Although introduction of these treatments have greatly improvedthe outcome of these patients, most with advanced disease eventuallyrelapse after treatment, suggesting that tumors acquire or intrinsicallypossess mechanisms to escape from HER2 inhibition [6]. Finally, thereis a breast cancer subgroup of tumors that do not express either hor-mone receptors or HER2. It is therefore called triple-negative, and is theone with the worst prognosis as a whole, due to the highly aggressivefeatures of their cancer cells, their heterogeneous nature, and to thelack of targeted therapies [7]. These patients are treated with classicalchemotherapies, which indiscriminately target cells undergoing pro-liferation, either tumoral or not [7].
It is well documented that cannabinoids, the active ingredients ofthe hemp plant Cannabis sativa, produce antitumor responses in pre-clinical models of cancer, by tackling different stages of cancer pro-gression such as uncontrolled cancer cell proliferation and survival,angiogenesis and metastasis [8,9]. The vast majority of these studieshas been performed with pure compounds, mainly Δ9-tetra-hydrocannabinol (THC). The cannabis plant, however, produces hun-dreds of additional compounds (other cannabinoids, terpenoids, flavo-noids, polyphenols, etc.) that have been much less studied but showpromising therapeutic properties (anti-proliferative, anti-inflammatory,immune-stimulant, etc.), and/or the potential capability of enhancingsome THC actions [10,11], the so-called “entourage effect”. In thiscontext, we aimed at comparing the antitumor activity of pure THCversus a cannabis drug preparation, and at determining whether can-nabinoid-based therapies can improve or interfere with current stan-dard treatments in breast cancer. We addressed these questions in bothin vitro and in vivo preclinical models of the different subtypes of breastcancer.
2. Material and methods
2.1. Materials
Pure THC (≥99% HPLC) was from THC Pharm GmbH (Frankfurt,Germany). The cannabis drug preparation (CDP) was produced by AuntZelda’s (Bodega Bay, CA). Briefly, organically-grown fresh cannabisflowers were frozen at −20 °C for 48 h, and then macerated in ethanolfor 24 h at the same temperature. The plant matter was vacuum filtered,scrubbed with charcoal, and re-filtered. Alcohol was evaporated with arotary evaporator, followed by magnetic stirring on hot plate to achievecannabinoid decarboxylation. The resulting cannabinoid and terpenecomposition of the extract was determined as described below, and it isdetailed in Table 1. β-Caryophyllene, α-humulene and nerolidol 1 werepurchased from Sigma-Aldrich (St. Louis, MO), and linalool and β-pinene from True Terpenes (Portland, OR). A cocktail of terpenes wasprepared by mixing the mentioned terpenes in DMSO at the sameconcentrations present in the CDP. The CB1R-selective antagonistSR141716 (SR1) was from NIMH (Bethesda, EEUU), the CB2R-selectiveantagonist SR144528 (SR2) from Tocris Bioscience (Abingdon, UK), α-tocopherol (TOC) and tamoxifen from Sigma-Aldrich, cisplatin fromAccord (Durham, NC), and paclitaxel from MedChem Express (Sollen-tuna, Sweden). Lapatinib was kindly donated by GlaxoSmithKline(Brentford, UK) and epirubicin by Dr. Gema Moreno-Bueno (MD An-derson Cancer Center, Madrid, Spain). For experiments in cell cultures,all drugs except epirubicin and cisplatin were dissolved in DMSO.Epirubicin was dissolved in H2O, and cisplatin in PBS.
2.2. Analysis of the cannabis drug preparation
The CDP cannabinoid and terpene composition was determined by
Sonoma Labwoks (Santa Rosa, CA). The presence and concentration ofthe following cannabinoids was determined by high-pressure liquidchromatography (HPLC): Δ9-tetrahydrocannabinolic acid (THCA), Δ9-tetrahydrocannabinol (THC), Δ9-tetrahydrocannabivarin (THCV), can-nabidiol (CBD), cannabidiolic acid (CBDA), cannabigerol (CBG), can-nabinol (CBN) and cannabichromene (CBC). Separation, identificationand quantitation of terpenes and residual solvents was performed bygas chromatography with flame ionization detector (GC-FID). The fol-lowing terpenes were analyzed: α-bisabolol, camphene, 3-carene, β-caryophyllene, caryophyllene oxide, p-cymene, geraniol, guaiol, α-hu-mulene, isopulegol, D-limonene, linalool, β-myrcene, nerolidol 1, ner-olidol 2, ocimene, α-pinene, β-pinene, α-terpinene, γ-terpinene andterpinolene. The presence of microbial contaminants and pesticides wasruled out by quantitative PCR and liquid chromatography tandem massspectrometry (LC-MS/MS), respectively. Results were counter-analyzedby Canna Foundation (Valencia, Spain) and Ananda Analytics Lab(Madrid, Spain).
2.3. Cell lines and cultures
All human breast adenocarcinoma cell lines were from ATCC-LGC(Barcelona, Spain): MCF-7 and T47D (ER+, PR+, HER2−); BT474 andHCC1954 (HER2+); MDA-MB-231 and SUM 159 (ER−, PR−,HER2−). All of them were authenticated by STR profiling (Genomicscore facility at Alberto Sols Biomedical Research institute, Madrid,Spain). They were cultured in RPMI (HCC1954, BT474 and T47D),MEM (MCF7), DMEM (MDA-MB-231) or Ham’s F12 (SUM 159), sup-plemented with 10% FBS, 1% penicillin/streptomycin. T47D, MCF7,SUM 159 and BT474 cells were also supplemented with 10 μg/mL in-sulin, and SUM159 with 0.5 μg/mL hydrocortisone. All cells weremaintained at 37 °C in an atmosphere of 5% CO2.
Table 1Cannabinoid and terpene composition of the cannabis drug pre-paration.
CANNABINOID Concentration (mg/g)
THCA 3.449THC 551.308THCV NDCBD NDCBDA NDCBG 3.667CBN NDCBC NDTERPENE Concentration (mg/g)α-Bisabolol 0.177Camphene BDL3-Carene BDLβ-Caryophyllene 1.948Caryophyllene Oxide 0.032p-Cymene 0.178Geraniol NDGuaiol NDα-Humulene 0.557Isopulegol 0.023D-Limonene NDLinalool 0.620β-Myrcene 0.025Nerolidol 1 0.357Nerolidol 2 0.081Ocimene 0.049α-Pinene 0.015β-Pinene 0.317α-Terpinene 0.013γ-Terpinene 0.013Terpinolene 0.017
ND=Not detected.BDL=Below detectable limit.
S. Blasco-Benito et al. Biochemical Pharmacology 157 (2018) 285–293
286

2.4. Cell viability assays
Cells were seeded at a density of 5000 cells/cm2 in 10% FBS-con-taining medium. Twenty-four hours later, they were serum-starvedovernight, and then treated with the indicated compounds for 24 or48 h. Cells were subsequently fixed and stained with a crystal violetsolution (0.1% crystal violet, 20% methanol in H2O) for 20min. Afterintensive washing with H2O, the stained cells were solubilized in me-thanol, and absorbance measured at 570 nm. Data are expressed as thepercentage of viable cells vs. vehicle-treated cells, set at 100%, and
represented as mean ± SEM of at least 3 independent experiments.In experiments aimed at comparing the potency of pure THC vs. that
of the CDP, the same amount of THC was used. For example, if theeffect of 3 µM THC was under study, it was compared with an amount ofCDP that provided 3 µM THC. The cannabinoid receptor antagonists(1 μM) and tocopherol (10 μM) were added to the cell cultures 1 h priorto THC.
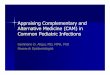
Fig. 1. Effects on preclinical models of ER+/PR+ breast cancer. (A-E) Cell viability, as determined by crystal violet staining, in response to the indicated treatmentsfor 24 h. Results are expressed as % versus vehicle-treated cells, set at 100%. (A) Viability of T47D (A) and MCF7 (B) human breast ER+/PR+ adenocarcinoma cellsin response to increasing concentrations of THC, administered either as a pure compound (THC) or as part of a cannabis drug preparation (CDP). (C-E) Viability ofT47D cells upon treatment with pure THC, a terpene cocktail containing β-caryophyllene, linalool, α-humulene, nerolidol 1 and β-pinene (TERP), or the combinationin the same proportion as in the CDP (C); in response to THC or CDP and the CB1R-selective antagonist SR141716 (SR1, 1 μM), the CB2R-selective antagonistSR144528 (SR2, 1 μM) or the antioxidant agent α-tocopherol (TOC, 10 μM) (D); or in response to tamoxifen (TAM), alone or in combination with THC or CDP. (F)Growth of ectopic tumors generated in nude mice by subcutaneous injection of T47D cells. Animals were treated with vehicle, THC (45mg/Kg), CDP (containing45mg/Kg THC), TAM (2.5 mg/Kg), or the combination of TAM and CDP. *, p < 0.05 and **, p < 0.01 vs. vehicle-treated cells/animals; ##, p < 0.01 vs. TERP (C),THC or CDP (D), TAM (E) or THC (F); $$, p < 0.01 vs. THC or CDP (E).
S. Blasco-Benito et al. Biochemical Pharmacology 157 (2018) 285–293
287

2.5. Animal studies
All procedures involving animals were performed with the approvalof Complutense University Animal Experimentation Committee andMadrid Regional Government, according to the European OfficialRegulations.
Tumors were generated in 6 week-old female nude mice (Envigo,Barcelona, Spain) by subcutaneous injection in the right flank of5× 106 HCC1954 cells or 5×106 MDA-MB-231 cells in PBS. For ER+/PR+ tumor generation, a 17β-estradiol pellet (Innovative Researchof America, Sarasota, FL) was subcutaneously inserted with a precisiontrochar (Innovative Research of America) 1 day before T47D cell in-jection (10× 106 cells). Tumor volume was routinely measured withand external caliper, and when it reached 200mm3 (for BT474 andT47D) or 100mm3 (for MDA-MB-231), animals were randomly as-signed to the different experimental groups and treatment started. PureTHC and CDP were administered at a dose of 45mg/Kg, 3 times a week,in 100 µL of sesame oil, by oral gavage (for CDP, 45mg/Kg means adose of the extract that contains 45mg/Kg of THC). Tamoxifen (2.5 mg/kg in 100 µL of sesame oil) and cisplatin (3 mg/kg in 100 µL of PBS)were administered i.p. 3 times a week; and lapatinib (100mg/Kg) dailyby oral gavage in 200 µL of 0.5% hydroxypropyl methylcellulose plus0.1% Tween 80. Control animals received the corresponding vehicleswith the same pattern and route of administration. Animals were sa-crificed after one month of treatment.
2.6. Statistical analyses
All data were analyzed using Prism 6 (GraphPad), and are presentedas mean ± SEM of at least 3 independent experiments. Unpaired 2-tailed Student’s t test was used to assess 2 independent groups. One-wayANOVA was used to test multi-group comparisons with Tukey’s post-hoc test. The groups with 2 independent variables were tested by 2-wayANOVA (in vivo experiments). Significance level was below 0.05 in allcases. IC50 values were determined with CompuSyn software.
3. Results
3.1. Effects on preclinical models of hormone-sensitive breast cancer
Although ER+/PR+ breast cancer is associated with high rates ofresponse to targeted treatments, innate and acquired resistance alsooccurs, which constitutes a clinical challenge because, like in otherbreast cancer subgroups, recurrences and disease dissemination areusually very difficult to treat (1). To analyze whether this subtype ofbreast cancer may be sensitive to cannabinoid treatment, we challengedT47D cells (a human ER+ and PR+ breast cancer cell line) with eitherpure THC or the CDP whose precise composition is detailed in Table 1.As shown in Fig. 1A, both THC and the CDP decreased the viability ofT47D cells in a concentration-dependent manner. Of interest, the bo-tanical preparation was more potent than the pure cannabinoid. Thus,the IC50 value was 2.2 μM for CDP and 2.9 μM for THC. To determinewhether this response was T47D-specific or could be extrapolated toother hormone-sensitive breast cancer cells, we conducted similar ex-periments in MCF7 cells (another human ER+ and PR+ breast cancercell line). As for T47D, both pure THC and the CDP decreased theviability of MCF7 cells, an effect that was concentration dependent(Fig. 1B). In this case, the extract tended to be more potent than thepure cannabinoid as well (IC50 THC=2.8 μM; IC50 CDP=2.4 μM).
It is important to highlight that, in these experiments, comparisonbetween effects was conducted for the same concentrations of THC,administered either as pure compound or as part of the CDP. This wouldconceivably imply that the observed differences in potency are due tothe THC-accompanying compounds present in the botanical drug pre-paration. To determine if the most abundant terpenes in the CDP wereresponsible for that effect, we generated a terpene cocktail containing
the same concentrations of β-caryophyllene, linalool, α-humulene,nerolidol 1 and β-pinene that are present in the extract (Table 1), andcombined it with THC, at the same proportion as in the PCD as well.The terpene cocktail did not produce any effect on cell viability(Fig. 1C). In addition, its combination with THC did not improve THCantiproliferative action either (Fig. 1C). These observations suggest thatother compounds (or compound combinations) present in the CDP areresponsible for its superior potency over THC.
We next studied which were the primary targets of cannabinoidantiproliferative action in ER+/PR+ breast cancer cells. As shown inFig. 1D, the effect of pure THC was not affected by pre-incubation withthe CB1R-selective antagonist SR141716 (SR1). On the contrary, THCaction was partially prevented by the CB2R-selective antagonistSR144528 (SR2), and by the antioxidant compound alpha-tocopherol(TOC) (Fig. 1D). These results indicate that the effect of THC on ER+/PR+ breast cancer cell viability is produced by activation of CB2
receptors, and the generation of reactive oxygen species (ROS). Of in-terest, neither blockade of CB2R nor preincubation with TOC preventedthe antiproliferative effect of the CDP, suggesting that, in this case,different/complementary targets and mechanisms of action are acti-vated.
Next, we aimed at analyzing how cannabinoid-based therapies mayimpact the efficacy of current standard antitumor therapies for hor-mone-sensitive breast cancer. Specifically, we combined THC or theCDP with tamoxifen. When submaximal concentrations of this SERMand pure THC were applied together to the cell cultures, the viability ofT47D cells decreased in an additive manner (Fig. 1E). Similar effectswere observed when tamoxifen and the CDP were combined (Fig. 1E).
Finally, we tested whether all the observations made in cell cultureswere also evident in a more physiological setting. Specifically, wegenerated ER+/PR+ tumors in immunedeficient mice by sub-cutaneous injection of T47D cells. At the THC doses used in this study,the pure compound did not trigger any significant antitumor response(Fig. 1F). On the contrary, and administered at the same dose of THC,the CDP produced a remarkable decrease in tumor growth (Fig. 1F),confirming the higher potency of the botanical preparation vs. the purecannabinoid as observed in vitro. Tamoxifen, on the other hand, alsoimpaired tumor growth, and in this case neither pure THC nor the CDPhad any impact (negative or positive) on its antitumoral action(Fig. 1F).
3.2. Effects on preclinical models of HER2+ breast cancer
Although with worse general prognosis than those with ER+/PR+cancer, patients with HER2-overexpressing tumors have significantlybetter clinical outcomes since the incorporation of HER2-targetedtherapies to the medical practice. However, local and distant re-currences are not unusual, and their therapeutic management is mostlypalliative [1]. Previous studies suggest that this breast cancer subtypemay be responsive to cannabinoid treatments [12]. However, as formost of the preclinical research conducted so far, those studies werecarried out with pure cannabinoids. Here, we observed that both pureTHC and the CDP decreased the viability of HCC1954 human HER2+breast cancer cells (Fig. 2A). As for hormone-sensitive cells, the bota-nical preparation was more potent than the pure compound (IC50
THC=2.7 μM; IC50 CDP=2.0 μM). Of interest, this response was notHCC1954-specific, as it was also observed in another HER2+ humanbreast cancer cell line (BT474) (Fig. 2B). The IC50 values were 3.7 μMfor pure THC and 2.7 μM for the CDP. Also in this case, neither thecocktail containing the 5 most abundant terpenes in the botanical ex-tract produced any effect on cell viability, nor the combination of thiscocktail with pure THC improved the effect of the cannabinoid on cellviability (Fig. 2C), which again points to different compounds orcombination of compounds as responsible for the increased potency ofthe CDP compared to pure THC. Regarding mechanism of action, and asin ER+/PR+ cells, THC decreased cell viability by activating CB2R and
S. Blasco-Benito et al. Biochemical Pharmacology 157 (2018) 285–293
288

generating ROS, as indicated by the observation that this effect wasprevented by SR2 and TOC, and not by SR1 (Fig. 2D). In this case,however, and unlike hormone-sensitive cells, the effect of the CDP waspartially prevented by CB2R blockade and scavenging of ROS (Fig. 2D),which suggests that additional targets and mechanisms of actions areinvolved in cannabinoid action.
For the combination therapy experiments, we used lapatinib, asmall molecule tyrosine kinase inhibitor that targets both HER2 andHER1 (EGFR) [4]. Simultaneous addition of submaximal concentrations
of lapatinib and pure THC produced an additive decrease in cancer cellviability (Fig. 2E), an effect that was also observed when combining thekinase inhibitor and a submaximal concentration of the CDP (Fig. 2E).
We then tested the effect of the cannabinoid-based therapies aloneor in combination with lapatinib in an animal model of HER2+ breastcancer. Specifically, we generated subcutaneous tumors by injection ofBT474 human HER2+ breast cancer cells into immune-compromisedmice. As in cultured cells, and using the same doses of THC in the pure-compound group as in the CDP group, the botanical extract was
Fig. 2. Effects on preclinical models of HER2+ breast cancer. (A-E) Cell viability, as determined by crystal violet staining, in response to the indicated treatments for24 h. Results are expressed as % versus vehicle-treated cells, set at 100%. (A) Viability of HCC1954 (A) and BT474 (B) human breast HER2+ adenocarcinoma cells inresponse to increasing concentrations of THC, administered either as a pure compound (THC) or as part of a cannabis drug preparation (CDP). (C-E) Viability ofHCC1954 cells upon treatment with pure THC, a terpene cocktail containing β-caryophyllene, linalool, α-humulene, nerolidol 1 and β-pinene (TERP), or thecombination in the same proportion as in the CDP (C); in response to THC or CDP and the CB1R-selective antagonist SR141716 (SR1, 1 μM), the CB2R-selectiveantagonist SR144528 (SR2, 1 μM) or the antioxidant agent α-tocopherol (TOC, 10 μM) (D); or in response to lapatinib (LAPA), alone or in combination with THC orCDP. (F) Growth of ectopic tumors generated in nude mice by subcutaneous injection of BT474 cells. Animals were treated with vehicle, THC (45mg/Kg), CDP(containing 45mg/Kg THC), LAPA (100mg/Kg), or the combination of LAPA and CDP. *, p < 0.05 and **, p < 0.01 vs. vehicle-treated cells/animals; ##,p < 0.01 vs. TERP (C), THC or CDP (D), LAPA (E) or THC (F); $, p < 0.05 vs. THC (E).
S. Blasco-Benito et al. Biochemical Pharmacology 157 (2018) 285–293
289

Fig. 3. Effects on preclinical models of triple-negative breast cancer. (A-G) Cell viability, as determined by crystal violet staining, in response to the indicatedtreatments for 24 h unless otherwise stated. Results are expressed as % versus vehicle-treated cells, set at 100%. (A) Viability of MDA-MB-231 cells (A) and SUM159(B) human breast triple-negative adenocarcinoma cells in response to increasing concentrations of THC, administered either as a pure compound (THC) or as part of acannabis drug preparation (CDP). (C-E) Viability of MDA-MB-231 cells upon treatment with pure THC, a terpene cocktail containing β-caryophyllene, linalool, α-humulene, nerolidol 1 and β-pinene (TERP), or the combination in the same proportion as in the CDP (C); in response to THC or CDP and the CB1R-selectiveantagonist SR141716 (SR1, 1 μM), the CB2R-selective antagonist SR144528 (SR2, 1 μM) or the antioxidant agent α-tocopherol (TOC, 10 μM) (D); or in response topaclitaxel (PCT) (E), epirubicin (EPI) for 48 h (F), or cisplatin (CIS) (G) for 48 h, alone or in combination with THC or CDP. (H) Growth of ectopic tumors generated innude mice by subcutaneous injection of MDA-MB-231 cells. Animals were treated with vehicle, THC (45mg/Kg), CDP (containing 45mg/Kg THC), CIS (3mg/Kg), orthe combination of CIS and CDP. *, p < 0.05 and **, p < 0.01 vs. vehicle-treated cells/animals; #, p < 0.05 and ##, p < 0.01 vs. TERP (C), THC (D), PCT (E),THC (F) or CIS (G); $, p < 0.05 and $$, p < 0.01 vs. THC or CDP.
S. Blasco-Benito et al. Biochemical Pharmacology 157 (2018) 285–293
290

significantly more potent than the pure cannabinoid in impairing tumorgrowth (Fig. 2F). As in the case of tamoxifen, lapatinib did not have anyimpact, either positive or negative, on the effect of the CDP (Fig. 2F).
3.3. Effects on preclinical models of triple-negative breast cancer
Triple-negative is the breast cancer subtype with the worst prog-nosis. These cancer cells are very aggressive in terms of proliferation,migration and invasion features. In addition, they lack specific mole-cular markers that today can be therapeutically targetable, whichmakes indiscriminate chemotherapy the only recommended treatmentfor these patients. Although a small percentage of them respond verywell to chemotherapy, the vast majority does not, and the key aim oftherapies implies increasing disease-free survival [7]. To study the ef-fect of cannabinoids on this breast cancer subtype, we used humanMDA-MB-231 cells as a model. Both pure THC and the CDP decreasedthe viability of these cells in a concentration-dependent manner(Fig. 3A). As in cells expressing ER or PR, or overexpressing HER2, theCDP was more potent than the pure cannabinoid (Fig. 3A), with IC50
values of 1.6 μM and 1.9 μM, respectively. This effect was not cell line-specific, as it was observed in another human triple-negative breastcancer cell line (SUM159) (Fig. 3B). The corresponding IC50 valueswere 2.8 μM for THC, and 2.1 μM for the CDP. Once again, the terpenecocktail did not have any significant effect on cell viability, and itscombination with pure THC did not improve cannabinoid anti-proliferative action (Fig. 3C). THC effect on the viability of MDA-MB-231 cells, when administered as a pure compound, was due, at leastpartially, to CB2R activation and ROS generation. Thus, SR2 and TOCwere able to prevent THC-induced decrease in cancer cell viability,while blockade of CB1R with SR1 was not (Fig. 3D). In contrast, theantiproliferative effect of the CDP was not prevented by any of thepharmacological tools used in this study (Fig. 3D), suggesting onceagain that different or additional mechanisms of action are activated.
The chemotherapy drugs that triple-negative patients receive in-clude, among others, taxanes (aimed at interfering with the cytoskeletalrearrangements that occur on cell replication and migration), anthra-cyclines (antineoplastic antibiotics that interfere with DNA replication)and platinum analogs (which covalently bind to the DNA, also blockingits replication) [7]. We first used a taxane (paclitaxel), and observedthat the decrease in cell viability produced by either treatment alone(paclitaxel, THC or the CDP) was not altered upon combination(Fig. 3E). Similar results were obtained when an anthracycline (epir-ubicin) was studied (Fig. 3F). We then analyzed the combination be-tween cannabinoids and the platinum-based drug cisplatin. In this case,combination with the CDP produced an increased antiproliferative re-sponse (Fig. 3G).
Finally, we tested the cannabinoid treatments, alone and in com-bination with cisplatin, in an in vivo setting. We generated triple-ne-gative tumors in immunedeficient mice by subcutaneous injection ofMDA-MB-231 cells. As in the other two subtypes of breast cancer, theCDP was significantly more potent than the pure cannabinoid when thesame dose of THC was administered (Fig. 3H). Similarly, the combi-nation of cannabinoids with cisplatin did not affect, either positively ornegatively, the antitumor action of the latter (Fig. 3H).
4. Discussion
A large body of preclinical evidence shows that cannabinoids pro-duce antitumor responses in a variety of animal models of cancer, in-cluding breast, pancreas, lung or liver adenocarcinomas, glioblastomasor melanomas, among others [8,9,12]. The solidness of these studieshas set the bases for the first controlled clinical study of the combina-tion of a cannabis-based medicine with a standard anticancer drug.Specifically, a phase 2 placebo-controlled clinical trial was performedin patients with recurrent glioblastoma multiforme, to address somesafety and efficacy endpoints of the combination of Sativex [a cannabis
extract containing equal amounts of THC and cannabidiol (CBD)] withtemozolomide (an alkylating agent that constitutes the gold-standardtreatment for this devastating type of brain tumors) (ClinicalTrials.govidentifiers NCT01812603 and NCT01812616). At the time this manu-script was submitted, the results of that study had not been publicated,but a press release of the sponsor company has partially unveiled po-sitive results (https://www.gwpharm.com/). The vast majority of thepreclinical research conducted in this field has used pure cannabinoids(mainly THC). However, the cannabis plant produces hundreds of othercompounds with potential therapeutic properties, which makes whole-plant cannabis preparations potentially better therapeutic tools. Forexample, more than 100 different phytocannabinoids have been de-scribed so far [13], and we are just beginning to study and characterizethem in terms of medical potential. In the context of cancer, and al-though research is not as exhaustive as that of THC and CBD yet, someplant-derived cannabinoids have been shown to produce anti-proliferative actions, as well as invasion/migration inhibiting effects incell cultures [14,15], which makes them potentially interesting tools toinclude in cannabinoid-based therapies. The CDP used in this study hadmeasurable amounts of CBG and THCA, for example. CBG has beenshown to display antitumor responses via TRPM8 receptors in models ofcolon cancer [16]. THCA on the other hand was recently shown to be aPPAR-γ agonist with neuroprotective activity [17], and this receptorhas been previously linked to apoptotic responses in cancer cells [18].
Aside from cannabinoids, Cannabis sativa produces other families ofchemical compounds with potential interest in the oncology field.Among them, terpenes are receiving increasing attention. These volatilecompounds are the responsible for the organoleptic properties of can-nabis, and some are starting to show potentially interesting therapeuticproperties. For example, β-myrcene is analgesic and antibacterial; α-pinene is anti-inflammatory, as well as β-caryophyllene, which is alsoanalgesic and a gastric protectant [19]. Although research in this field isin its infancy, the available information so far suggests that the pre-sence of these compounds in cannabis-based therapies may be bene-ficial. It is also important to mention that the presence of certain ter-penes [with sedative properties, like β-myrcene, for example [19]] andof CBD [with anxiolytic and antipsychotic activity [20]] in cannabispreparations may have additional advantages related with an improvedtolerability of THC.
Although current medicine is mostly based on the use of purecompounds that have single targets, it is increasingly obvious that fordiseases as complex as cancer, multi-target approaches could con-ceivably be more effective. In fact, the majority of oncologic patientsreceive several treatments simultaneously. The complex chemicalcomposition of cannabis drug preparations makes them multi-drugpreparations, which, in principle, could allow the concurrent tackling ofdifferent hallmarks of cancer, and of other symptomatology associatedto this pathology (pain, anxiety, nausea, side effects of standard an-ticancer treatments, etc.). From a pharmacological point of view, thiswould the consequence of a battery of compounds activating cannabi-noid receptor-dependent and independent signaling pathways in dif-ferent target populations (cancer cells, neuronal circuits controllingpain perception and nausea reflex, etc.). In addition, the presence ofdifferent compounds in these preparations is a source of potentialpharmacological interactions, either synergic or antagonistic. The sy-nergistic interaction between endocannabinoid compounds has beenpreviously reported. Thus, Mechoulam and coworkers described thatthe biological activity of the endocannabinoid 2-arachydonoylglicerolwas augmented by other 2-acylglycerols that, when used alone, did notproduce biological responses [21]. This was called “entourage effect”, aterm that is currently used to refer to the potential synergies betweenchemical compounds present in the cannabis plant [19]. In summary,and although the pharmacology of cannabis drug preparations extractsis obviously more complex to study, this therapeutic approach has thepotential to produce better therapeutic responses than pure cannabi-noids. Results presented herein support that idea. We have observed
S. Blasco-Benito et al. Biochemical Pharmacology 157 (2018) 285–293
291

that both in cell cultures and in animal models of breast cancer, a THC-rich CDP is more potent than pure THC in producing antitumor re-sponses. We were unable to identify the compounds or compoundcombinations responsible for this increased potency, but we ruled outthe possibility that it resided in the presence of the 5 most abundantterpenes. In addition, our results suggest that additional or differentmolecular targets and mechanisms of action are activated when theCDP is used as compared to pure THC, supporting the idea that its in-creased potency may be due to a multi-target response.
Of interest, our results show that all breast cancer subtypes respondto cannabinoids, including the highly aggressive triple-negative. Thisobservation suggests that the susceptibility of breast cancer cells tocannabinoid treatment is not related to the expression (or lack of ex-pression) or specific oncogenic signaling triggered by hormone re-ceptors or HER2. In line with this idea, many different types of cancercells, including pancreas, skin, liver or lung adenocarcinomas, glio-blastomas, hematological tumors, sarcomas, etc., have shown anti-proliferative or death-inducing effects in response to cannabinoids[8,9,12]. In fact, to the best of our knowledge, no overtly cannabis-resistant tumors have been described so far. Considering how differentcancer subtypes are, and the fact that the viability of non-transformedcells is not affected by cannabinoids at the concentrations they killtumor cells [8,9,12], it is tempting to speculate that these compoundstackle essential, as yet unidentified, cellular functions that all cancercells share, and that are absent in their non-cancerous counterparts.
Here, we also analyzed whether there was any kind of interaction,either positive or negative, between cannabinoids and some of the mostcommon treatments for breast cancer patients. Targeted therapies forER+/PR+ and HER2+ tumors showed an improved antiproliferativeactivity in cell cultures when combined with THC or the CDP. Thiseffect was not that evident when cannabinoids were combined with twoof the chemotherapeutic agents used in this study (paclitaxel andepirubicin). Previous work, however, showed a clear additive responsewhen combining paclitaxel with the endocannabinoid anandamide ingastric cancer cell lines [22]. Additional studies should be carried out toclarify whether this discrepancy is related to these precise cancer sub-types, the specific cannabinoid used, or other additional factors. Sy-nergistic responses between cannabinoids and other chemotherapeuticagents have been previously reported. For example, a positive inter-action between the antimetabolite 5-fluorouracil and the syntheticcannabinoid HU-210 was found in colorectal cancer cell cultures [23],and between the alkylating agent temozolomide and THC in glio-blastoma, both in vitro and in vivo [24]. Intriguingly, the additive effectswe observed between tamoxifen or lapatinib and cannabinoids in cellcultures was not evident in vivo. As shown in the corresponding figures,the doses we chose for tamoxifen, lapatinib, cisplatin and the CDPproduced very prominent antitumor responses. It would be interestingto determine whether combination of lower doses of all of them (pro-ducing submaximal responses by themselves) would trigger the additiveeffects we observed in vitro. In addition, it is important to highlight thatcombination with the CDP did not, in any case, diminished the anti-tumor efficacy of any of the standard treatments, which suggest thatcannabis-based therapies would not interfere with the usual therapiesthese patients receive. On the contrary, cannabinoids have been shownto protect tissues from damage produced by certain chemotherapydrugs. Thus, these compounds prevent cisplatin- and doxorubicin-in-duced neuropathic pain [25], a very distressing and common side effectthat frequently leads to treatment discontinuation. Of interest, thisprotective effect is also produced by β-caryophyllene [26], one of themost common terpenes in cannabis, and one of the constituents of thecannabis drug preparation used in this study. Cannabinoids also preventdoxorubicin-induced cardiomyopathy [27–29]. In summary, and evenif no synergistic interactions with other chemotherapy drugs (in termsof antitumor efficacy) were to occur in patients, the combination ofcurrent standard treatments and cannabis-based therapies, containingnot only THC but other plant-derived accompanying compounds, would
have a positive impact in preventing the highly toxic effects of theirtreatments and consequently on their quality of life.
Acknowledgements
This work was supported by grants from Spanish Ministry ofEconomy and Competitiveness (PI14/01101 and PI17/00041, sup-ported with European Regional Development (FEDER) funds, to CS andEP-G); Scientific Foundation of Asociación Española Contra el Cáncer(to EP-G); and Zelda Therapeutics (to CS and MG).
SB-B and IT are recipients of Formación de ProfesoradoUniversitario (FPU) and pFIS fellowships (from the Spanish Ministry ofEconomy and Competitiveness), respectively. We are indebted to EvaResel for administrative support.
Declarations of interest
Cristina Sánchez and Manuel Guzmán declare that they are mem-bers of Zelda Therapeutics Medical Advisory Board. Mara Gordon is aDirector of the same company.
References
[1] N. Harbeck, M. Gnant, Breast cancer, Lancet 389 (10074) (2017) 1134–1150.[2] C. Curtis, S.P. Shah, S.F. Chin, G. Turashvili, O.M. Rueda, M.J. Dunning, D. Speed,
A.G. Lynch, S. Samarajiwa, Y. Yuan, et al., The genomic and transcriptomic ar-chitecture of 2,000 breast tumours reveals novel subgroups, Nature 486 (7403)(2012) 346–352.
[3] H.G. Russnes, O.C. Lingjaerde, A.L. Borresen-Dale, C. Caldas, Breast cancer mole-cular stratification: from intrinsic subtypes to integrative clusters, Am. J. Pathol.187 (10) (2017) 2152–2162.
[4] J. Baselga, R.E. Coleman, J. Cortes, W. Janni, Advances in the management ofHER2-positive early breast cancer, Crit. Rev. Oncol. Hematol. 119 (2017) 113–122.
[5] S. Loibl, L. Gianni, HER2-positive breast cancer, Lancet 389 (10087) (2017)2415–2429.
[6] B.N. Rexer, C.L. Arteaga, Intrinsic and acquired resistance to HER2-targetedtherapies in HER2 gene-amplified breast cancer: mechanisms and clinical implica-tions, Crit. Rev. Oncog. 17 (1) (2012) 1–16.
[7] A. Lee, M.B.A. Djamgoz, Triple negative breast cancer: emerging therapeuticmodalities and novel combination therapies, Cancer Treat. Rev. 62 (2018) 110–122.
[8] R. Schwarz, R. Ramer, B. Hinz, Targeting the endocannabinoid system as a potentialanticancer approach, Drug Metab. Rev. 50 (1) (2018) 26–53.
[9] G. Velasco, C. Sanchez, M. Guzman, Towards the use of cannabinoids as antitumouragents, Nat. Rev. Cancer 12 (6) (2012) 436–444.
[10] J.M. McPartland, E.B. Russo, Handbook of Cannabis, Oxford University Press,Oxford, United Kingdom, 2014, pp. 280–295.
[11] E.B. Russo, Beyond Cannabis: plants and the endocannabinoid system, TrendsPharmacol. Sci. 37 (7) (2016) 594–605.
[12] M.M. Caffarel, C. Andradas, E. Perez-Gomez, M. Guzman, C. Sanchez,Cannabinoids: a new hope for breast cancer therapy? Cancer Treat. Rev. 38 (7)(2012) 911–918.
[13] M. ElSohly, G. Waseeem, Handbook of Cannabis, Oxford University Press, Oxford,United Kingdom, 2014, pp. 3–22.
[14] A. Ligresti, L. De Petrocellis, V. Di Marzo, From phytocannabinoids to cannabinoidreceptors and endocannabinoids: pleiotropic physiological and pathological rolesthrough complex pharmacology, Physiol. Rev. 96 (4) (2016) 1593–1659.
[15] A. Ligresti, A.S. Moriello, K. Starowicz, I. Matias, S. Pisanti, L. De Petrocellis,C. Laezza, G. Portella, M. Bifulco, V. Di Marzo, Antitumor activity of plant canna-binoids with emphasis on the effect of cannabidiol on human breast carcinoma, J.Pharmacol. Exp. Ther. 318 (3) (2006) 1375–1387.
[16] F. Borrelli, E. Pagano, B. Romano, S. Panzera, F. Maiello, D. Coppola, L. DePetrocellis, L. Buono, P. Orlando, A.A. Izzo, Colon carcinogenesis is inhibited by theTRPM8 antagonist cannabigerol, a Cannabis-derived non-psychotropic cannabi-noid, Carcinogenesis 35 (12) (2014) 2787–2797.
[17] X. Nadal, C. Del Rio, S. Casano, B. Palomares, C. Ferreiro-Vera, C. Navarrete,C. Sanchez-Carnerero, I. Cantarero, M.L. Bellido, S. Meyer, et al.,Tetrahydrocannabinolic acid is a potent PPARgamma agonist with neuroprotectiveactivity, Br. J. Pharmacol. 174 (23) (2017) 4263–4276.
[18] H.A. Elrod, S.Y. Sun, PPARgamma and apoptosis in cancer, PPAR Res. 2008 (2008)704165.
[19] E.B. Russo, Taming THC: potential cannabis synergy and phytocannabinoid-terpe-noid entourage effects, Br. J. Pharmacol. 163 (7) (2011) 1344–1364.
[20] A.C. Campos, M.V. Fogaca, F.F. Scarante, S.R.L. Joca, A.J. Sales, F.V. Gomes,A.B. Sonego, N.S. Rodrigues, I. Galve-Roperh, F.S. Guimaraes, Plastic and neuro-protective mechanisms involved in the therapeutic effects of cannabidiol in psy-chiatric disorders, Front. Pharmacol. 8 (2017) 269.
[21] S. Ben-Shabat, E. Fride, T. Sheskin, T. Tamiri, M.H. Rhee, Z. Vogel, T. Bisogno, L. DePetrocellis, V. Di Marzo, R. Mechoulam, An entourage effect: inactive endogenousfatty acid glycerol esters enhance 2-arachidonoyl-glycerol cannabinoid activity,
S. Blasco-Benito et al. Biochemical Pharmacology 157 (2018) 285–293
292

Eur. J. Pharmacol. 353 (1) (1998) 23–31.[22] H. Miyato, J. Kitayama, H. Yamashita, D. Souma, M. Asakage, J. Yamada,
H. Nagawa, Pharmacological synergism between cannabinoids and paclitaxel ingastric cancer cell lines, J. Surg. Res. 155 (1) (2009) 40–47.
[23] S.B. Gustafsson, T. Lindgren, M. Jonsson, S.O. Jacobsson, Cannabinoid receptor-independent cytotoxic effects of cannabinoids in human colorectal carcinoma cells:synergism with 5-fluorouracil, Cancer Chemother. Pharmacol. 63 (4) (2009)691–701.
[24] S. Torres, M. Lorente, F. Rodriguez-Fornes, S. Hernandez-Tiedra, M. Salazar,E. Garcia-Taboada, J. Barcia, M. Guzman, G. Velasco, A combined preclinicaltherapy of cannabinoids and temozolomide against glioma, Mol. Cancer Ther. 10(1) (2011) 90–103.
[25] S. O'Hearn, P. Diaz, B.A. Wan, C. DeAngelis, N. Lao, L. Malek, E. Chow, A. Blake,Modulating the endocannabinoid pathway as treatment for peripheral neuropathicpain: a selected review of preclinical studies, Ann. Palliat. Med. 6 (Suppl. 2) (2017)
S209–S214.[26] G.C. Segat, M.N. Manjavachi, D.O. Matias, G.F. Passos, C.S. Freitas, R. Costa,
J.B. Calixto, Antiallodynic effect of beta-caryophyllene on paclitaxel-induced per-ipheral neuropathy in mice, Neuropharmacology 125 (2017) 207–219.
[27] E. Hao, P. Mukhopadhyay, Z. Cao, K. Erdelyi, E. Holovac, L. Liaudet, W.S. Lee,G. Hasko, R. Mechoulam, P. Pacher, Cannabidiol protects against doxorubicin-in-duced cardiomyopathy by modulating mitochondrial function and biogenesis, Mol.Med. 21 (2015) 38–45.
[28] A.A. Fouad, W.H. Albuali, A.S. Al-Mulhim, I. Jresat, Cardioprotective effect ofcannabidiol in rats exposed to doxorubicin toxicity, Environ. Toxicol. Pharmacol.36 (2) (2013) 347–357.
[29] D.S. Hydock, C.Y. Lien, R. Hayward, Anandamide preserves cardiac function andgeometry in an acute doxorubicin cardiotoxicity rat model, J. Cardiovasc.Pharmacol. Ther. 14 (1) (2009) 59–67.
S. Blasco-Benito et al. Biochemical Pharmacology 157 (2018) 285–293
293