Embed Size (px)
Citation preview

Postgraduate Medical Journal (May 1980) 56, 322-329
Aplastic anaemia: an analysis of 174 patientsM. A. MIR* C. G. GEARY
MB., M.R.C.P., D.C.H. M.C.Path., F.R.C.P. (Ed.)
University Department of Clinical Haematology, Manchester Royal Infirmary,Manchester M13 9WL
SummaryThe authors summarize their experience with 174patients with aplastic anaemia (AA) with particularreference to course, prognostic factors, conversion toother blood disorders, treatment and outcome.Aplastic anaemia was defined as pancytopenia and ahypocellular marrow at some time during the illness.Seven patients terminated with acute leukaemia, 8developed haematological features of sideroblasticanaemia and 5 showed a red cell membrane defectcommonly found in paroxysmal noctural haemo-globinuria.
Complete recovery occurred in only 4 patients; 70others showed a partial remission with some residualhaematological abnormality in peripheral blood.Eighteen of these had spontaneous remission. Remis-sion was brief in 27 patients who died; only 32 patientsremained in partial remission. Twenty-five per cent.of the patients with AA run an acute course and diewithin 6 months of the time of diagnosis. The re-mainder run a subacute or chronic course, punctuatedin some cases by a transient remission, but in others bya conversion to other related haematological disorders.An acute course is suggested by a rapid onset ofsymptoms, a falling neutrophil count, a haemoglobinlevel less than 5 g/dl and a very low platelet count.A chronic course is likely in those patients who have aslow onset of symptoms, a stable neutrophil count anda Hb level in excess of 5 g/dl. The authors' experienceshows that the disease runs either of the 2 coursesirrespective of the supportive therapy.
IntroductionSince Ehrlich's (1888) description of a case of
aplastic anaemia (AA) with a fulminating course, thenatural history of this disease and its haematologicalfeatures have become recognized as being extremelydiverse. Its relationship to paroxysmal nocturnalhaemoglobinuria and leukaemia (Dameshek, 1967),the occurrence of chromosomal abnormalities in
* Present address: Department of Medicine, UniversityHospital of Wales, Heath Park, Cardiff CF4 4XW.
Fanconi's anaemia (Dosik et al., 1970), and theclinical remission which follows bone marrow trans-plantation all support the concept of a defectivehaemopoietic stem cell arising after an episode ofmarrow damage. It is difficult to understand howdrugs can influence a disorder in which the basicdefect is stem cell damage.The introduction of androgen therapy by Shahidi
and Diamond (1959) stimulated a great deal ofenthusiasm but widely different results have beenreported by various workers (Sanchez-Medal et al.,1964; Mir and Delamore, 1974; Williams, Lynchand Cartwright, 1973; Davis and Rubin, 1972).Variations in diagnostic criteria may account forsome of these differences. The purpose of this paperis to review the authors' experience with 174 patientswith AA with particular regard to course, prognosticfactors and the success of therapy.
PatientsAll of the patients in this study were seen at the
Department of Clinical Haematology, ManchesterRoyal Infirmary, between the years 1940 and 1973.All had pancytopenia (i.e. Hb <11.7 g/dl; neutro-phil count <1 8x 103/\l) and a hypocellular bonemarrow some time during the course of the illness.Patients with myelophthisic anaemia, those withFanconi's anaemia and patients with AA secondaryto radiation or cytotoxic therapy were excluded.Haematological investigations were performed bystandard methods (Dacie and Lewis, 1968). Usingthese criteria the clinical and laboratory details of174 patients (76 male, 98 female) were analysed.Other workers have also noted a female over malepredominance (Vincent and De Gruchy, 1967;Bomford and Rhoads, 1941).A definite history of exposure to a drug considered
to be related to marrow aplasia was obtained in 38patients. Eleven patients had exposure to a variety ofdrugs not usually associated with AA (i.e. chlor-diazepoxide, diazepam, amitriptyline and variousphenothiazine derivatives).
0032-5473/80/0500-0322 $02.00 © 1980 The Fellowship of Postgraduate Medicine
copyright. on O
ctober 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.56.655.322 on 1 M
ay 1980. Dow
nloaded from

Aplastic anaemia 323
Haematological studiesAll but 7 of the patients had a low Hb level (< 11-7
g/dl) when they were first seen. On first examinationthe leucocyte count was more than 10 000/uLI in 3patients and between 5000 and 10 000/1 in 20 butthese values subsequently fell to below 5000/1l in all
TABLE 1. Initial and the lowest neu-trophil count
No of patientsCells/JIl Initial Lowest
0- 499 52 91500- 999 31 561000-1499 18 241500-1999 34 32000-2499 272500+ 12
patients. Table 1 shows the distribution of the initialand the lowest neutrophil counts in all patients. In91 patients the neutrophil count fell below 5000/,1during the course of their illness.The platelet count was less than 15 000 /[l in all
but 9 patients on presentation. During the course oftheir illness the count fell further and 98 patients hadvalues below 10 000/1l (Table 2).
TABLE 2. Initial and the lowest plate-let count
No. of patientsCells x 103/4tl Initial Lowest
0- 10 64 9810- 50 51 5850-100 30 14100-150 20 4>150 9
Bone marrowThe trephine marrow biopsy was not a routine
procedure in the Manchester Royal Infirmarylaboratory before the year 1963. All trephinebiopsies performed since 1964 were examined andthe patients with hypocellular marrow were includedin this group. A decision regarding the marrowcellularity of patients seen before 1963 was estab-lished by a careful survey of the aspiration reportsand of marrow sections taken at post-mortem. Onlythose patients known to have had unequivocalhypocellularity were included.
OutcomeOf the 174 patients, 44 were alive at the time of
writing this report (1979); 27 patients were lost to
follow-up; 19 of these had not achieved remission,6 had partially remitted and did not require bloodtransfusions and 2 others were still in need offortnightly blood transfusions.
DeathsOne hundred and three patients died and post-
mortem was performed on 64 of these. Infection,haemorrhage or a combination of the two was theusual terminal event. At post-mortem, infection wasconsidered to be the main cause of death in 16patients; 7 of these had septicaemia, 2 infectiveendocarditis and one had fibrocaseous pulmonarytuberculosis. Haemorrhage was the sole cause ofdeath in 26 of the 64 patients. Seven of these hadcerebral haemorrhage: one patient died withasphyxia due to sudden pharyngeal haemorrhage,while 18 others had generalized haemorrhage.Septicaemia and infection both contributed to deathin 8 patients; 6 of these had developed acute leu-kaemia as the terminal event (see below). The causeof death in these 64 patients is given in Table 3.
TABLE 3. Cause of death at post-mortemInfection
Septicaemia 7Endocarditis 2Lobar pneumonia 2Pulmonary tuberculosis 1
Others (e.g. urinary tract, upperrespiratory tract) 4
HaemorrhageGeneralized 18In the central nervous system 7In the epiglottis 1
MixedSepticaemia and haemorrhage 8
Other causesHaemosiderosis 5Carcinomatosis 2Myocardial infarction 1Cardiac failure 1Cardiac aneurysm 1Necrosis of the liver 1Alveolar proteinosisHaemochromatosis 2
Total 64
RemissionFour patients (2%) achieved complete remission
as judged by a normal bone marrow and peripheralblood picture. A fifth patient (case 75) was in fullclinical remission for 5 years during which all herhaematological data were normal. The appearanceof ring sideroblasts in her bone marrow precededthe recurrence of the anaemia 7 years after the initialdiagnosis. She died 3 years later.
copyright. on O
ctober 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.56.655.322 on 1 M
ay 1980. Dow
nloaded from

324 M. A. Mir and C. G. Geary
Partial remissionSome improvement in haematological picture
occurred in 70 patients: their haemoglobin levelimproved and they did not require blood trans-fusions but their Hb, white cell and platelet countsdid not reach normal levels. Twenty-seven of thesepatients died. The reasons for relapse were notobvious in every patient: 4 patients terminated withleukaemia, 6 had a massive cerebral haemorrhage, 2terminated with sideroblastic anaemia, one diedwith acute myocardial infarction, 2 died withhaemosiderosis and, in 5, infection was the terminalevent. In 7 patients the cause of death could not beascertained. Eleven patients were lost to follow-up.
Continuing aplasiaEight patients showed a stabilization of the haemo-
globin level, albeit at a low level, and they stillrequired periodic transfusions.
Surviving patientsFour of the 44 surviving patients have achieved
complete clinical and haematological remission;their peripheral blood picture is normal and the bonemarrow examined in 3 patients showed adequatecellularity with no features of dyshaemopoiesis. Atoxic agent was implicated in 2 of these (cases 42and 106). Of the remaining 40 surviving patients, 32showed a partial haematological recovery with someabnormality in their peripheral blood picture. A lowplatelet count was the commonest haematologicalabnormality in patients with partial remission andwas present in all these and in the other 8 who weremaintained by periodic blood transfusion. Bonemarrow was hypocellular in 22 of the 32 patients inpartial remission, and in all the 8 patients with con-tinuing aplasia who required transfusions. A com-pletely normal peripheral blood and marrow picturewas found in only 2 of the 44 surviving patients;others showed some evidence of marrow damage(hypocellularity neutropenia, thrombocytopenia) andstressed haemopoiesis (i.e. high mean corpuscularvolume (MCV), raised Hb F) after 2 to 18 years ofclinical remission. It seems that after the initialepisode of aplasia some abnormality remains eventhough it may be masked by clinical remission. Forexample, cases 75 and 112 enjoyed 5 and 20 yearsof clinical remission before they developed sidero-blastic anaemia.
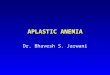
Survival curveA survival graph was constructed to show the fate
of 147 patients on whom all the follow-up data wereavailable. Twenty-nine per cent. ofthese patients diedwithin the first 6 months and 60% died within thefirst 3 years; thereafter the death rate was slow andonly 8% more died within the next 3 years (Fig. 1).
147
-
- n96
, 70IL 61 56> 51
(I 047
I I2 4 6
Time in years from diagnosisFIG. 1. Six-year survival curve of the entire series.
A further 8% died within the next 10 years but thedata on long-term survival are incomplete becausesome patients were lost to follow-up.
Prognostic factorsVarious clinical and haematological factors were
examined to explore their prognostic significance inrelation to survival of patients.
Duration of symptoms before diagnosis. Theshorter the duration of symptoms before diagnosis,the higher was the 5-year death rate. Thus, of the 22patients who had symptoms for one month or less,only 7 (32%) were alive at the end of 5 years. On theother hand, the 5-year survival rate was 47% in 40patients who had symptoms for longer than 6months before the diagnosis.Age and sex. The outcome did not relate to the age
of patients at diagnosis. Females had a better out-look with a 45% 5-year survival rate as comparedwith 32% in males.
Haematological factorsA low Hb level was associated with a bad prog-
nosis since 40% of the patients with a haemoglobinlevel of <5 g/dl at diagnosis died during the firstyear. The long-term outlook was still poorer in thesepatients, as only 18% of those who presented withan Hb level below 5 g/dl were alive after 12 years.Similarly, a platelet count of <10 000/1l wasominous as regards survival. The absolute neutro-phil count on presentation did not appear to besignificant as regards the death rate. There was a38% 5-year survival in patients with <500 neutro-phils/t1l. However, a falling neutrophil countemerged as an important factor. Of the 18 patientswith a neutrophil count of <500/Jil, in whom thecount fell further, 16 died during the first month.The degree of marrow hypoplasia and the initial
copyright. on O
ctober 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.56.655.322 on 1 M
ay 1980. Dow
nloaded from

Aplastic anaemia 325
reticulocyte count were also considered becausepatients with mild marrow hypoplasia and reticulo-cytosis responded better to oxymetholone than thosewith severe hypoplasia (Mir and Delamore, 1974).However, the overall significance of these 2 factorssignificance of these 2 factors in the entire series wasnegligible. The mean corpuscular volume (MCV)data on admission were available on 31 patients. Ofthese, 18 had a MCV of >100 fl, and 9 died. Of the13 patients with normal MCV, 9 died. Finally, the6-year survival curve (Fig. 1) showed a steeperdecline during the first year than the subsequentyears. Any patient alive 3 years after diagnosis had a70% chance of survival as compared with 25%during the first year.
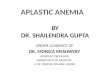
It thus seems that the duration of symptoms beforediagnosis, the platelet count and the Hb level atdiagnosis have prognostic significance. As AA caneither manifest as an acute disease with a rapidlydownhill course, or as a chronic smouldering dis-order, the authors considered whether these 3 factorswould help one decide the likely course in a patient.For this purpose, one mark was allotted for each ofthe 3 favourable factors; one if the speed of onsetwas longer than 6 months, and one each for thepresenting Hb level of more than 5 g/dl and for theplatelet count of >100000/,l. The survival curveshown in Fig. 1 was replotted for the 2 populations;one curve represented the patients who had 2 ormore marks (92 patients) and the other curverepresented those (55 patients) who had one or less(Fig. 2). The death rate was significantly (P<0 001)faster in the patients who scored one or less marks;only 7% of the 55 patients were alive at the end of
100
- 60 p60 P<000I
20-
I2 4 6Time (years)
FIG. 2. Six-year survival curve of 2 groups. Patientswere allocated in the 2 groups on the basis of the speedof onset of illness and the initial haemoglobin andplatelet values. Patients in the smaller group of 55 had arapid onset, lower haemoglobin and platelet values atdiagnosis and an acute course (see text). 0-* 55patients; 0-0 92 patients.
6 years. On the other hand, patients with 2 or moremarks as a group had a much slower death rate, andmost of these patients had probably a more chronicform of aplastic anaemia.
TherapySupportive therapy was given to all patients. This
consisted of blood transfusion, antibiotics and, inrecent years, included platelet and white cell trans-fusions. Various therapeutic agents have enjoyed ashort lived popularity but it seems clear that, withthe exception of immunosuppressants in pure redcell aplasia (Krantz and Kao, 1969) and the possiblevalue of antilymphocytic serum in some cases ofAAthere are no drugs at present which could reversemarrow aplasia in AA. The drugs used in this seriesare listed in Table 4.
TABLE 4. Summary of therapyNo. of
Treatment patients
Supportive therapy alone 43Corticosteroids alone 76Androgens and corticosteroids:Oxymetholone 25Fluoxymesterone 10Testosterone 8
Androgens alone:Oxymetholone 11Testosterone 2
Supportive therapy alone. Forty-three patientswere sustained with supportive therapy; 2 of these(patients 90 and 106), were given dimercaprolbecause heavy metals (gold, arsenic and bismuth)were implicated as the causative factors in these 2patients. One patient (case 50) was given phytohaem-agglutinin which enjoyed a short vogue in the treat-ment of AA (Humble, 1963). All these 3 patientsachieved haematological remission. Sixteen otherpatients achieved partial remission and the totalremission rate was 46% in this group.
Corticosteroids. Seventy-six patients were treatedwith corticosteroids alone and 26 (34%) of theseachieved haematological remission. In 3 patients thehaematological picture returned completely tonormal.
Oxymetholone with or without steroids. Thirty-sixpatients received oxymetholone either in combina-tion with steroids or alone and 18 patients (50%)showed some haematological improvement.
Other androgens with steroids. Eighteen patientswere treated with various androgenic hormones(fluoxymesterone and testosterone) in combinationwith steroids. Eleven patients (61%) showed somehaematological remission.
copyright. on O
ctober 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.56.655.322 on 1 M
ay 1980. Dow
nloaded from

326 M. A. Mir and C. G. Geary
A haematological remission proved to be brief insome cases and did not influence the outcome. Thus,9 patients in the Supportive Therapy group, 4 in theSteroids group, 7 in the Oxymetholone group, and 7in the Other Androgens group died after a briefhaematological remission. When survival figures arecompared, there is no significant difference betweenthe various groups (Figs 3 and 4).
100
0
- 60*S
2020 _
2 4 6Time (years)
FIG. 3. Survival curves showing comparison betweentreatment with corticosteroids (--O), all androgens(0-0) and with supportive therapy alone (A-A).
100
0-(^60
'F>~ ~ ~ 0-- o(35)c
20K (17)
I l2 4 6Time (years)
FIG. 4. Survival curves showing comparison betweentreatment with oxymetholone (0-0) and otherandrogens (A--A). The number of patients is given inparentheses.
Conversion to other haematological disordersConversion to acute leukaemia. Aleukaemic leu-
kaemia with a peripheral pancytopenic picture andaplastic anaemia are difficult to differentiate duringtheir initial stages. When one disease is diagnosedand subsequently transforms to another it is difficult
to agree on the significance of conversion particu-larly when fundamental differences exist on diag-nostic criteria. If the criteria for AA are accepted asbeing pancytopenia with hypocellular marrow atsome stage, and the transition to acute leukaemia isaccepted when there are sheets of blast cells in themarrow and there is organ infiltration by abnormalcells, various reports in the literature show that sucha transition does occur. In this series, 7 patients withfeatures of AA eventually developed acute leu-kaemia; 6 terminated with acute myeloid leukaemia,and one with smouldering leukaemia. The length oftime between the diagnosis of AA and the develop-ment of acute myeloid leukaemia was 10 months in2 patients, 18 months in one, 22 months in one, 29months in one and 46 months in the sixth patient.Case 112 developed smouldering leukaemia withfeatures of sideroblastic anaemia 20 years after theinitial diagnosis. The diagnosis was established byappropriate staining reactions. The previously hypo-plastic marrow was replaced by sheets of blast cellsin all but case 112, whose marrow showed features ofsideroblastic anaemia and smouldering leukaemia.Except this patient, post-mortem was obtained in alland the diagnosis was confirmed by marrow sectionsand by visceral infiltration. In 4 of these, the changeoccurred after the administration of oxymetholone(Delamore and Geary, 1971). Whether this was acoincidence or due to the myelostimulatory effect ofoxymetholone is difficult to say. It is worth pointingout that whereas 4 patients developed acute leu-kaemia in a group of 36 patients treated withoxymetholone, 3 others who developed acuteleukaemia came from a group of 138 patients whodid not receive oxymetholone.
Conversion to sideroblastic anaemia. AA has beenincluded in the list of conditions associated withring sideroblasts in the marrow (MacGibbon andMollin, 1965). Eight patients (cases 9, 15, 57, 75, 102,112, 149 and 153) developed haematological featurescharacteristic of sideroblastic anaemia during thecourse of their illness. Sideroblastosis is, in thiscontext, a morphological hall-mark of the dysery-thropoiesis which is found in many cases of AA.The clinical and haematological details of 3 of thesepatients (cases 9, 112 and 153) have been reported byGeary et al. (1974). In 6 of these, the diagnosis ofsideroblastic anaemia was made during a phase ofpartial recovery. In the other 2 (cases 75 and 112),periods of 5 and 20 years respectively separated the2 diagnoses; case 75 has shown a complete haemato-logical remission but in case 112 there was persistentthrombocytopenia with incomplete marrow re-covery. The final marrow picture of this last patientwas interesting because not only did it show ringsideroblasts, erythroid hyperplasia with megalo-blastoid abnormalities, it also showed some features
copyright. on O
ctober 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.56.655.322 on 1 M
ay 1980. Dow
nloaded from

Aplastic anaemia 327
of smouldering leukaemia with maturation arrestin granulopoiesis and 7% blast cells. This patientdied at home and no post-mortem was performed.His clinical details have been published elsewhere(Geary et al., 1974).
Conversion to paroxysmal nocturnal haemoglobin-uria (PNH). PNH is a recognized complication ofAA and may devejop a long time after the initialmarrow damage (Lewis and Dacie, 1967). Therehave been conflicting reports of the incidence ofPNH in AA (Najean and Bernard, 1965; Heimpel,Rehbock and Von Eimeren, 1975). In the presentseries, 5 patients showed a PNH defect in their redcells.
DiscussionDifficulties will continue in comparison between
various series as long as diagnostic criteria remainvague. The term aplastic anaemia was applied byChauffard (1904) to a syndrome of pancytopeniawith acellular marrow first described by Ehrlich(1888). In 1905 Blumer pointed out that hypoplasiaof the marrow was not a constant feature. Bomfordand Rhoads' series (1941) had some patients withhypercellular marrow, and a recent study shows thatmost patients with aplastic anaemia do show residualislands of haemopoietic tissue (Kansu and Erslev,1976). In this series, only those patients were in-cluded who had pancytopenia with hypoplasticmarrow at some stage. These criteria would providesome basis for comparison between various series.Recently, there has been renewed support in favourof hypoplasia and pancytopenia as criteria foraplastic anaemia (Williams et al., 1973; Heimpel etal., 1975). The overall incidence of drug-induced AAin this series (28%) is much lower than 86% reportedby Williams et al. (1973). However, Bottiger andWesterholm (1972) found that only 20% of theirpatients had antecedent drug or chemical exposure.The reasons for these discrepancies are not clear.
Prognostic factorsSince AA may terminate rapidly or may behave as
a chronic smouldering disorder for many years, it isimportant to look for some clinical and haemato-logical clues which might suggest the course of thedisease in a particular patient (Williams, Lynch andCartwright, 1978). Various authors have attemptedto predict the likely course of the disease; some havefound an increased reticulocyte count of favourableprognostic significance (Durate et al., 1972;Sanchez-Medal et al., 1969; Lewis, 1965).Bloom and Diamond (1968) regarded a raisedalkali-resistant haemoglobin level as a hopefulprognostic sign. In this series, reticulocyte count andmacrocytosis were not of any prognostic significancebut the patients who responded to oxymetholone
tended to have an increased reticulocyte count (Mirand Delamore, 1974). The reticulocyte count in-creased in these patients as the remission progressed.Macrocytosis would appear to reflect the presenceof a greater number of reticulocytes, which in itselfsuggests an increased erythropoietic activity (Senoet al., 1964). In fact, macrocytosis with MCV ofmore than 110/fl persisted in most patients whosurvived long enough to achieve a stable Hb level.Similarly, alkali-resistant Hb appeared to be a signof stressful erythropoiesis and reflected a responseof the erythron to the insult causing hypoplasia. Allthe features considered to be of hopeful prognosticimportance (i.e. raised MCV, reticulocytosis, fetalHb) reflect dyserythropoiesis and indicate an in-creased and stressful erythropoiesis. A continuingincrease in some of these indices would appear toshow that the erythron is less damaged and moreresponsive. In that respect these features can beregarded as being of good prognostic importance.On the other hand a falling neutrophil count, fallingHb level and platelet count reflect the stem cellfailure. In agreement with Vincent and De Gruchy(1967) it was found that all the 3 cell lines weredepressed during infection. However, in 18 patients,the prognostic value of a falling neutrophil count(<500/ld) was well revealed since 16 of these diedduring the first 6 months. Of the 8 patients who hada neutrophil count of less than 100/txl on presen-tation, 6 died during the first 4 weeks.
Conversion to other diseasesVarious authors have observed a remarkable
relationship ofAA to PNH (Lewis and Dacie, 1967),to sideroblastic anaemia (MacGibbon and Mollin,1965; Geary et al., 1974) and to leukaemia (Adams,1951; Block, Jacobson and Bethard, 1953; Cohenand Creger, 1967; Delamore and Geary, 1971).Lewis and Dacie (1967) have suggested that PNHmay represent a somatic mutation in a haemopoieticstem cell already damaged during the aplasticepisode. Similarly, progressive changes in a damagedcell may lead to sideroblastic anaemia, at times manyyears after the original episode. It is of interest tonote that sideroblastic anaemia developed 20 yearsafter AA was diagnosed in case 112 and the finalbone marrow picture showed dysmyelopoiesisassociated with ring sideroblastosis. Such evolutionmight represent a clonal degeneration in an 'un-stable' marrow. This problem is complicated by thefact that sideroblastic anaemia may develop soonafter the aplastic episode, as happened in some of thepatients in the present study. Both AA and acuteleukaemia may occur in the same populationexposed to a single toxic agent (Vigliani and Saita,1964; Hamilton, 1931). Dameshek (1967) suggestedthat these might be different manifestations of the
copyright. on O
ctober 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.56.655.322 on 1 M
ay 1980. Dow
nloaded from

328 M. A. Mir and C. G. Gear),
same fundamental injury to the pluripotent stem cell,and the actual outcome may depend on the extent ofthe damage and the constitution of the patient. Ifthis were the case one would expect a change fromAA to acute leukaemia more frequently than hasbeen reported.The limitation in the way a cell can respond to
trauma must be taken into consideration. The inter-relationship of PNH, AA and acute leukaemia maybe explained by the fact that the haemopoietic stemcell can respond to injury by these known mani-festations and the actual end result depends on thetype and the extent of the injury. At present it isreasonable to say that all 4 conditions (AA, PNH,primary sideroblastic anaemia and acute leukaemia)are irreversible disorders with grave prognosis, andthese may all be 'clonal' diseases where after theinitial damage the subsequent haematological pic-ture may result from clonal evolution, degenerationor from a loss of genetic material required for pro-duction of enzymes concerned in haem synthesis assuggested by Catovsky and his colleagues (1971).A 4% incidence of acute myeloid leukaemia in this
series is higher than most other series. Although longfollow-up and haematological surveillance are theprobable reasons for the high incidence, 2 patientswere diagnosed in 1956 when the diagnostic methodswere less well developed. It is impossible to becertain that these patients had pure AA at the timeof diagnosis. The incidence of PNH, on the otherhand, is lower than reported by Lewis and Dacie(1967) but the figures for the present series arecomparable with those published by other workers(Najean and Bernard, 1965; Heimpel et al., 1975).
Therapy and outcomeSince the prognosis of AA is poor, various thera-
peutic agents have been tried with the hope thatthese might influence the course of the disorder.Corticosteroids and androgenic steroids have beenthe commonest drugs used. This series dates back tothe times when neither of these 2 therapies wasavailable, and the authors have therefore attemptedto compare the effects of these drugs on survival ratewith the patients who received no drugs but werewholly sustained with supportive therapy. The sur-vival rate is no different in the corticosteroid groupfrom that of the 'supportive therapy' group; it isslightly better, but not significantly so, in the groupof patients treated with oxymetholone with or with-out corticosteroids. Remission as found in this seriesmay be brief and terminate in fatal relapse, acuteleukaemia or in sideroblastic anaemia. The trueefficacy of any therapeutic agent can be judged onlyafter many years. An examination of a 30-yearexperience in this series shows that none of the drugsused influences significantly the 10-year survival rate.
It has been shown that no drug has any specialadvantage over the other. Disappointing results havealso been reported after bone marrow transplan-tation (Davis and Rubin, 1972). There appear to be2 different populations of patients with AA, oneseverely affected who have an acute course anddeteriorate irrespective of any therapy. The othergroup runs a more chronic course; patients continuefor many years with or without supportive therapy.Some of these patients live for many years with somehaematological stigmata; some relapse and die withAA, while some develop one of the other haemato-logical disorders (e.g. acute leukaemia, sideroblasticanaemia) and only very few show a complete clinicaland haematological remission. It would seem thatAA is the result of a permanent damage to thehaemopoietic stem cell and the outcome is governedby the extent and the further progression of thisdamage. These findings nevertheless, support thethesis put forward by Williams et al., (1978) thatthere is a sub-population of patients with AA whosedisease tends to lead a more indolent course, and inwhom supportive measures are more likely to beeffective.
ReferencesADAMS, E.B. (1951) Aplastic anaemia. Review of 27 cases.
Lancet, i, 657.BLOCK, M., JACOBSON, L.O. & BETHARD, W.F. (1953) Pre-
leukemic human leukemia. Journal ofthe American MedicalAssociation, 152, 1018.
BLOOM, G.E. & DIAMOND, L.K. (1968) Prognostic value offetal hemoglobin levels in acquired aplastic anemia. NewEngland Journal of Medicine, 278, 304.
BLUMER, G. (1905) Aplastic anemia associated with lymphoidhyperplasia of the bone marrow. Bulletin of the JohnsHopkins Hospital, 16, 127.
BOMFORD, R.R. & RHOADS, C.P. (1941) Refractory anaemia.Quarterly Journal of Medicine, 10, 175.
BOTTIGER, L.E. & WESTERHOLM, B. (1972) Aplastic anaemia.Incidence and aetiology. Acta medica scandinavica, 192,315.
CATOVSKY, D., SHAW, M.T., HOFFBRAND, A.V. & DACIE,J.V. (1971) Sideroblastic anaemia and its association withleukaemia and myelomatosis: A report of five cases.British Journal of Haematology, 20, 385.
CHAUFFARD, M. (1904) Un cas d'an6mie pernicieuse aplas-tique. Bulletin de la Societe medicale des hOpitaux de Lyon,21, 313.
COHEN, T. & CREGER, W.P. (1967) Acute myeloid leukemiafollowing seven years of aplastic anemia induced by chlor-amphenicol. American Journal of Medicine, 43, 762.
DACIE, J.V. & LEWIS, S.M. (1968) Practical Haematology 4thedn. Churchill, London.
DAMESHEK, W. (1967) What do aplastic anemia, paroxysmalnocturnal hemoglobinuria (PNH) and hypoplastic anemiahave in common? Blood, 30, 251.
DAVIS, S. & RUBIN, A.D. (1972) Treatment and prognosis inaplastic anaemia. Lancet, i, 871.
DELAMORE, I.W. & GEARY, C.G. (1971) Aplastic anaemia,acute myeloblastic leukaemia and oxymetholone. BritishMedical Journal, 2, 743.
DOSIK, H., Hsu, L.Y., TODARO, G.J., LEE, S.L., HIRSCHHORN,K., SELIRIO, E.S. & ALTER, A.A.C. (1970) Leukemia in
copyright. on O
ctober 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.56.655.322 on 1 M
ay 1980. Dow
nloaded from

Aplastic anaemia 329
Fanconi's anemia: Cytogenic and tumor virus suscepti-bility studies. Blood, 36, 341.
DURATE, L., SANDOVAL, L., ESQUIVEL, F. & SANCHEZ-MEDAL,L. (1972) Androstane therapy of aplasic anaemia. Actahaematologica, 47, 140.
EHRLICH, P. (1888) Ober einen Fall von Anamie, mitBemerkungen iiber regenerative Veranderungen desKnochenmarks. Charite-Annalen, 13, 300.
GEARY, C.G., DAWSON, D.W., SITLANI, P.K., ALLISON, H.A.& LEYLAND, M.J. (1974) An association between aplasticanaemia and sideroblastic anaemia. British Journal ofHaematology, 27, 337.
HAMILTON, A. (1931) Benzine (benzol) poisoning. Archives ofPathology, 11, 434.
HEIMPEL, H., REHBOCK, C. & VON EIMEREN, A. (1975)Verlauf und Prognose der Panmyelopathie und der iso-lierten aplastichen Anamie, eine retrospektive Studie an 70Patienten. Blut, 30, 235.
HUMBLE, J.G. (1963) In vivo action of phytohaemagglutininin severe human aplastic anaemia. Nature. London, 198,1313.
KANSU, E. & ERSLEV, A.J. (1976) Aplastic anaemia with 'hotpockets'. Scandinavian Journal of Haematology, 17, 326.
KRANTZ, S.B. & KAO, V. (1969) Studies on red cell aplasia.II. Report of a second patient with an antibody to erythro-blast nuclei and a remission after immunosuppressivetherapy. Blood, 34, 1.
LEWIS, S.M. (1965) Course and prognosis in aplastic anaemia.British Medical Journal, 1, 1027.
LEWIS, S.M. & DACIE, J.V. (1965) Neutrophil (leucocyte)alkaline phosphatase in paroxysmal nocturnal haemo-globinuria. British Journal of Haematology, 11, 549.
LEWIS, S.M. (1969) Aplastic anaemia: problems of diagnosisand treatment. Journal of the Royal College of Physiciansof London, 3, 253.
LEWIS, S.M. & DACIE, J.V. (1967) The aplastic anaemia-paroxysmal nocturnal haemoglobinuria syndrome. BritishJournal of Haematology, 13, 236.
MACGIBBON, B.H. & MOLLIN, D.L. (1965) Sideroblasticanaemia in man: Observations on seventy cases. BritishJournal of Haematology, 11, 59.
MIR, M.A. & DELAMORE, I.W. (1974) Oxymetholone inaplastic anaemia. Postgraduate Medical Journal, 50, 166.
NAJEAN, Y. & BERNARD, J. (1965) Prognosis and evolutionof the idiopathic pancytopenias. Series Haematologica, 5, 1.
SANCHEZ-MEDAL, L., PIZZUTO, J., TORRE-LOPEZ, E. &DERBEZ, R. (1964) Effect of oxymetholone in refractoryanemia. Archives of Internal Medicine, 113, 721.
SANCHEZ-MEDAL, L., GOMEZ-LEAL, A., DUARTE, L. & RICO,M.G. (1969) Anabolic androgenic steroids in the treatmentof acquired aplastic anemia. Blood, 34, 283.
SENO, S., MIYAHARA, M., ASAKURA, H., OHCI, O.,MATSUODA, K. and TOYAMA, T. (1964) Macrocytosisresulting from early denucleation of erythroid precursors.Blood, 24, 582.
SHAHIDI, N.T. & DIAMOND, L.K. (1959) Testosterone-induced remission in aplastic anemia. American Journal ofDiseases of Children, 98, 293.
VIGLIANI, E.C. & SAITA, G. (1964) Benzene and leukemia.New England Journal of Medicine, 271, 872.
VINCENT, P.C. & DE GRUCHY, G.C. (1967) Complicationsand treatment of acquired aplastic anaemia. BritishJournal of Haematology, 13, 977.
WILLIAMS, D.M., LYNCH, R.E. & CARTWRIGHT, G.E. (1973)Drug-induced aplastic anaemia. Seminars in Haematology,10,195.
WILLIAMS, D.M., LYNCH, R.E. & CARTWRIGHT, G.E. (1978)Prognostic factors in aplastic anaemia. Clinics in Haema-tology, 7, 467.
copyright. on O
ctober 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.56.655.322 on 1 M
ay 1980. Dow
nloaded from