Embed Size (px)
Citation preview

0
Palestine Polytechnic University
Biomedical Engineering
"Apheresis"
Prepared by:
Nabhan Ebia
Presented to:
Dr. Ramzi Al-Qwasmih
4\1\2011

1
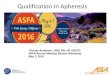
Blood Components
Blood is a complex mixture of plasma (the liquid component),
white blood cells, red blood cells, and platelets as shown in figure 1.
Plasma is 90 percent water and constitutes about 55 percent of blood
volume. Plasma can be fractionated or separated into
derivatives/products. These include albumin (the chief protein
constituent), fibrinogen (responsible in part, for the clotting of blood),
globulins (including antibodies), and other clotting factors.
Red cells contain hemoglobin, an iron-containing protein that
carries oxygen throughout the body and gives blood its red color. Donors
must have a hemoglobin level of 13.3 gm/dl to donate automated double
red cells. The percentage of blood volume composed of red cells is called
hematocrit.
Figure 1 Blood Components
Platelets are vital to life because they help prevent massive blood
loss by helping your blood to clot. Because they are sticky cells, they need
to be in constant motion after they are donated or they will clump and
cannot be transfused.
Plasma is the liquid portion of the blood that carries platelets, red
cells and proteins throughout the body. Plasma is made up of 90 percent
water and is more than 55 percent of your total blood volume.

2
Introduction to Apheresis
Apheresis is a medical technology in which the blood of a donor &
patient is passed through an Apheresis Machine that separates out one
particular constituent and returns the remainder to the circulation, so the
apheresis is a device in which the whole blood from a patient or donor is
removed. The components of whole blood are separated within the cell
separator. One or more of the separated portions are then withdrawn and
the remaining components are retransfused into the patient or the donor.
The Apheresis Machine should have facility for all blood component
collection including peripheral blood stem cells with both single &
double access platelet pheresis & also therapeutic plasmapheresis red cell
pheresis.
Figure 2 Apheresis

3
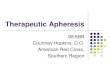
Principle of Operation
The overall operation of the device (as shown in figure 3) is the
blood is removed from a vein and mixed with a substance called citrate to
stop it clotting while in the blood collection set. It is then processed in the
collection set to separate the red blood cells from the plasma and
platelets. The components that are required are kept in the collection set
and the red blood cells are returned to the donor. This process allows 2-3
times the usual volume of plasma and up to 12 times the usual number of
platelets to be removed at a single donation, without making the donor
anaemic.
Figure 3 Principle of Apheresis
Types of Apheresis
There are two types of apheresis:
1- Donor apheresis:
In this type of ahresis the erythrocytes, platelets, and plasma are
collected .
The basic steps in apheresis are:
1) the separation f blood components
2) the removal of the desired component(s) using an online automated
system.

4
The ability of various techniques and equipment to carry out these
basic steps determines collection efficiency and product purity.
Separation can be accomplished by filtration, centrifugation, or a
combination of both. Filtration takes advantage of differences in particle
size to separate blood plasma from the cellular elements. Centrifugation
uses differences in specific gravity to separate and isolate blood
components.
Centrifugation
In a tube of blood that has reached equilibrium after the application
of centrifugal force, mature red cells (the most dense component) would
be located at the bottom, and plasma (the least dense component) would
have risen to the top. In between, in order of decreasing density, would be
neocytes (young red cells), granulocytes, mononuclear cells, and
platelets. The granulocyte fraction contains neutrophils, basophils, and
eosinophils. The mononuclear cell fraction contains lymphocytes,
monocytes, peripheral blood progenitor cells, and, in some leukemic
patients, blast cells. Unfortunately, a perfectly clean separation of these
components is not usually achieved in apheresis instruments. Instead,
there is some mixing; for example, small amounts of platelets and red
cells may be mixed in with the white blood cells (WBCs).
In the apheresis field, centrifugal separators are classified as
intermittent flow or continuous flow. In intermittent flow devices (also
called discontinuous or semicontinuous flow), blood is processed in
discrete batches. Separation can occur until the separation container is
filled with the most dense component; then the container must be emptied
before the next batch is processed. This is in contrast to continuous flow
devices, in which low-, high-, and intermediate- density fractions can all
be removed in an ongoing manner so that the separation container need
not be emptied until the end of the procedure.( see figure4)
Figure 4 Centrifuging

5
Filtration
Filtration or the use of membrane separators isolates blood
components on the basis of differences in particle size. Usually, plasma is
separated from the cellular elements. For example, the effective filter
pore size may be 0.6 micron, whereas the diameter of the platelet, the
smallest cellular element, is 2 to 3 microns. As whole blood flows by the
membrane surface under pressure, plasma passes through the pores and is
collected while the cellular elements are retained for return to the donor
or patient.
Most membrane separators used in apheresis today are composed
of a bundle of parallel, single, hollow fiber filters confined in a plastic
cylinder. Each fiber resembles a straw with many holes in its walls.
Whole blood under pressure enters at one end; as it flows through the
hollow fibers, plasma is squeezed out the walls and a more concentrated
cell suspension exits at the other end. In the most common layout, blood
enters through a bottom port, cells exit from a top port, and plasma is
withdrawn from a side port. An additional side port is usually provided to
monitor pressure.
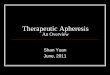
2- Therapeutic apheresis:
Blood is removed via a compatible blood pump capable of
monitoring pressures and detecting air and sent through the Plasmaflo
filter fibers, which separates whole blood from plasma. The holes in the
wall of the filter fibers are too small to allow blood cells to pass through,
so the plasma is 'sieved out' and removed by the PlasmaPro dual track
pump for discard. Simultaneously, replacement fluid is infused into the
blood circuit by the PlasmaPro and the whole blood is returned to the
patient. A typical set-up for membrane TPE is shown to the right.( see
figure5)

6
Figure 5 Theraputic Apheresis
In this type of ahresis the the basic functions are: Plasma exchange
(TPE), Selective apheresis
Cytaphersis, Erythrocytapheresis, Leucapheresis
Thrombocytapheresis, and Extracorporeal photopheresis.
It is the process of withdrawing blood from a patient, removing a
specific component and subsequently rein fusing the remaining
components to treat or palliate a disease. Therapeutic Apheresis consists
of the following procedures:
1. Plasma Exchange – The removal of plasma (the liquid portion of
the blood) from a patient and replacement with a solution mixed into the
cellular portion of the blood. The replacement solution may be plasma,
5% albumin, normal saline or lactated Ringer’s solution.
2. Red Cell Exchange – The removal of a predetermined volume of
red blood cells and transfusion of allergenic red blood cells with
reinfusion of the patient’s other blood components.
3. Cytapheresis – The removal of platelets and/or white blood cells
for therapeutic reasons.
Depending on the patient’s disease, Therapeutic Apheresis may be
performed as often as daily when prescribed by the ordering physician.

7
Apheresis techniques:
Depending on the substance that is being removed, different
processes are employed in apheresis. If separation by Density is required,
centrifugation is the most common method. Other methods involve
absorption onto beads coated with an absorbent material and filtration.
The centrifugation method can be divided into two basic
categories:
1- Intermittent-flow centrifugation (IFC):
The centrifugation process itself has four variables that can be controlled
to selectively remove desired components. The first is spin speed and
bowl diameter, the second is "sit time" in centrifuge, the third is solutes
added, and the fourth is not as easily controllable: plasma volume and
cellular content of the donor. The end product in most cases is the classic
sedimented blood sample with the RBC's at the bottom, the "buffy coat"
of platelets and WBC's (lymphocytes/granulocytes (PMN's, basophils,
eosinophils/monocytes) in the middle and the plasma on top
The machine is a tripod filter progam-control auto centrifugal
machine that unloads from the bottom with scrapers. It operates
intermittently. The program can be set according to the demands. The
machine can finish automatically feeding, separating, dewatering,
unloading and other process with hydraulic system, electric control
system. It can carry out close or distance operation. The machine adopts
unloading at low speed with narrow scrapers. It iswidely used in
separating suspension whose grain size is 0.05-0.15mm, it is also suitable
for separating materials whose heat sensitivity is strong. its crystal is not
broken and the operator may not be near. The machine has advantages,
such as high automation, large treatment volume, good separating result,
steady running, xonvenient operation and others, (see figure6).
The governor motor drives the tumbler to rotate at middle speed.
The feeding valve opens and the materials enter the tumbler through the
feeding pipes. The materials are spread even on the tumbler wall. When
the materials reach the preset volume, the feeding stops. The tumbler
rises to high speed. The liquid passes through the filter cloth and
discharges from thd tumbler wall holes under the function of the
centrifugal force. The solid remains in the tumbler. When the rotational
speed reduces to low speed, the scrapers rotate over and over again to

8
scrape the solid down from the tumbler wall and discharge it from the
bottom of the machine.
Figure 6 IFC
2- Continuous-flow centrifugation (CFC):
Continuous flow centrifugation (CFC) historically required two
venipunctures as the "continuous" means the blood is collected, spun, and
returned simultaneously. Newer systems can use a single venipuncture.
The main advantage of this system is the low extracorporeal volume
(calculated by volume of the apheresis chamber, the donor's hematocrit,
and total blood volume of the donor) used in the procedure, which may be
advantageous in the elderly and for children.
It is uniquely designed for processing very large sample volumes.-
typically, from bioreactors and fermentors-in just a single run. With its
high speed, autoclavable continuous flow rotor, the Centrifuge Stratus is
ideal for harvesting bacterial cultures, yeast, algae, human and animal
cell. With a sediment capacity of up to 400 ml and a flow rate of 36L per
hour, the Centrifuge Stratus can easily accommodate up to 50L
bioreactors or fermentors. As a result, compared with batch processing,
time savings of up to 80% can be achieved (see figure 7).
It is designed for quick filterless separation of filler from binder
solution or other mixtures containing sediments (cement, soil, clay), in
suspension. As no filter is required, there is no dispersion of material so

9
that the highest accuracy is assured. The solution is poured into the top
funnel and falls into the rotating test container dia. 70x200 mm. Because
of the centrifugal effect, the liquid rises vertically leaving the filler and
mineral particles inside the beaker. The centrifuge is supplied complete
with aluminum beaker, two sieves 0,149 mm. and 0,074 mm. mesh
respectively. The rotation speed is 11500 rpm, with automatic ramp and
preset speed control.
Figure 7 CFC
The Possible Problems Or Risks Of Apheresis Donation:
Some of the minor problems seen occasionally in normal donations
may also occur from time to time with apheresis donations. Many of
these relate to the use of a needle to puncture the vein of the donor and
include pain, bruising, infection or minor damage to the nerves in the
skin. Dizziness and fainting can also occur occasionally. These potential
problems are no more common, and some may be less common with
apheresis donations, than with ordinary whole blood donations.

10
• Apheresis donations take longer than normal donations and usually
require:
• 1-2 hours for platelet apheresis
• 35-45 minutes for plasmapheresis.
• Tingling in the fingers and around the mouth can occur when the red
blood cells are returned to the donor. This is due to the infusion of citrate
(which is mixed with the blood in the collection set to prevent clotting)
with the red blood cells. Citrate is used as a fuel by the body and is
rapidly removed from the blood stream, making this a very brief
phenomenon. It can generally be overcome by slowing the rate of return
of the red blood cells or by having a drink containing calcium.
• Despite the use of citrate, it is possible that the blood may clot while out
of the body, preventing its return. However, this is very uncommon and
the volume of blood that can be lost in this way is no more than that of a
normal whole blood donation.
• Rare theoretical risks include the possibility that air might be introduced
into the donor’s blood stream but modern apheresis machines include
alarms to prevent this and donors are monitored very closely during the
procedure.
• All the tubing, needles, and bowls used in this process are sterile and
disposable. A new blood collection set is used for each donation,
avoiding any problems of contamination.

11
References
1- Peter Flanagan "APHERESIS DONOR."
2- Frank Corbin; Herbert M. Cullis; "Development of Apheresis
Instrumentation".
3- http://www3.interscience.wiley.com/journal/113467388/abstract
last visit on 1\1\2011.
4- http://en.wikipedia.org/wiki/Apheresis. last visit on 1\1\2011.