Embed Size (px)
Citation preview

1st Edition August 2006
THERAPEUTIC APHERESIS
Operator Competency Based Orientation & Education Package.
Name:……………………………………………………………………….….. Date:…………………………………………………………………………….
Prepared by Tamla Tait, Austin Health, Victoria Claire Dowsing, Royal Melbourne Hospital, Victoria

1st Edition, August 2006 2
Authors Note The aim of this competency package is to provide a basic generic document for Apheresis staff, outlining common terminology and therapeutic procedures. It is also intended as a common tool for assessment of Apheresis staff across Australia & New Zealand There will be sections of this document that may not be relevant to some units depending on the type of procedures performed This document should be used in conjunction with existing hospital policy & procedures, company provided training, and machine operator manuals We have deliberately not included some items such as standard precautions, as these should be common practice. Mandatory competencies have only been referred to as these may vary from unit to unit It will be each apheresis unit’s decision to deem which components are relevant to them & instruct apheresis staff accordingly. We have also provided an assessment tool for each of the four (4) common apheresis machines in use across Australia & New Zealand. Your unit may have either one or more types so again you will be able to remove those that are not relevant. The number twenty (20) relating to procedure numbers is a “ballpark” number & again can be tailored for each individual. There may be staff that need to do more than the 20 procedures & the type of procedures will depend on those performed in each individual unit.
Regards Tamla & Claire

1st Edition, August 2006 3
Table of Contents Authors Note 2 Aim 4
Qualifications of the Preceptor/Trainer 4
Objectives 5
Pre-requisite educational requirements 6
Criteria for clinical evaluation 7
Introduction 8
Abbreviations 8
Definitions 9
Anticoagulation 9
Procedures performed at ____________________ 10 (Insert name of hospital here.)
Donor Apheresis 10
Peripheral Blood Stem Cell Collection 10
Cell development diagrams 13
Plateletpheresis – single donor platelets 15
Granulocytes 16
Dendritic cells 16
Therapeutic Apheresis 17
Therapeutic Plasma Exchange 17
Therapeutic Cytapheresis 18
Apheresis adverse events 20
Adverse events competency assessment criteria 21
References 22
Recommended reading 23
Acknowledgements 23
Core competency assessment – MCS plus 24
Core competency assessment – CS-3000+ 28
Core competency assessment – Amicus 32
Core competency assessment – COBE Spectra 36
Core competency assessment – COM.TEC 40

1st Edition, August 2006 4
Aim All apheresis operators working within the______________________________, will meet (Insert name of institution/department) the essential objectives and core competencies listed below, as applicable to ________________________________ to ensure the safe and appropriate delivery of (Insert name of institution/department) care to patients and donors, along with the appropriate and timely collection of requested blood components.
Qualifications Of The Preceptor/Trainer A preceptor is a staff member experienced in the institution’s operations and procedures who acts as a role model, teacher and resource person in orienting new employees. The preceptor individualises the orientation program in conjunction with a supervisor or other responsible educator(s) for the institution at the end of the orientation period.
Criteria for Preceptor: • Staff member, who has functioned in the unit for one year, or an exemplary employee, who meets all remaining criteria • Indicates strong interest in being a preceptor • Demonstrates expertise in knowledge and skills required for successful operation of apheresis devices • Demonstrates ability to apply teaching/learning principles • Demonstrates ability to set goals, establish priorities, and solve problems effectively • Demonstrates effective communication skills • Functions in accordance with the practices, policies, and procedures of the institution

1st Edition, August 2006 5
Objectives In order to operate without direct supervision by the end of the initial orientation and evaluation period, the apheresis trainee operator must fulfil the following criteria:
• Demonstrate basic knowledge of blood components
• Demonstrate knowledge of collected blood products, their functions, including, storage and handling, ABO and Rh typing
• Be cognisant of basic cytapheresis terminology
• Demonstrate knowledge of the types of apheresis procedures performed at
______________________ (Insert name of institutionl & department here.)
• Understand the rationale for each type of apheresis procedure performed at ____________________ and the disease processes they to treat
(Insert name of institutionl & department here.)
• Understand the nature of cell separator function and the use of anticoagulants, including common adverse events
• Have the ability to describe the adverse events associated with apheresis
procedures and appropriate corrective actions
• Demonstrate safe and appropriate operation of the apheresis machines currently in use, including knowledge of alarm conditions, troubleshooting and maintenance
• Be able to demonstrate knowledge of required documentation, and patient/donor
assessment for each apheresis procedure
• Be able to demonstrate knowledge of the relevant standard operating procedure(s) (SOP’s) for each type of apheresis procedure and the location of the Policy and Procedure Manual(s) for apheresis procedures within the ________________________.
(Insert name of department)
• Demonstrates competence in Donor Selection and Screening Responsibilities Staff are required to:
• Successfully complete this learning module and competency assessment
• Contribute towards maintaining knowledge and understanding of apheresis procedures
• Complete this competency in conjunction with material and education provided by
the relevant apheresis machine companies’ clinical support
Undertake all activities in accordance with relevant procedural guidelines

1st Edition, August 2006 6
Pre – Requisite Educational Requirements
• Successful completion of __________________Intravenous Cannulation (Insert name of institutionl here.)
self directed learning package and a minimum of six (6) successful and observed cannulations documented
• Successful completion of _____________________Blood & Blood Product (Insert name of institutionl here.) self directed competency
• Complete & pass annual cardio-pulmonary resuscitation assessment • Completes all in-house mandatory competency requirements
Apheresis Core Competency Requirements
1. Successful completion of the pre requisite educational requirements as listed above
2. Demonstrate knowledge of basic apheresis terminology, blood components and
the rationale for the different types of apheresis procedures performed by the _______________________________department
(Insert name of department) 3. Undertake twenty (20) supervised apheresis procedures. These procedures
should consist of a mix of donor apheresis procedures and patient based/therapeutic apheresis procedures or procedures relevant to each institution.
4. Demonstrate knowledge of each core competency to be assessed as listed below:
• Kit installation, set-up and priming of apheresis machine • Pre procedure preparation, completion of relevant checklists • Patient/donor preparation for apheresis procedure • Procedure commencement and monitoring • Post procedure care • Documentation • Review questions pertinent to apheresis procedure being performed
5. Undertake an initial evaluation of core competencies, once twenty (20) supervised
procedures have been completed. For successful completion of the evaluation, a minimum 90% of the assessment should be in the ‘Supervised’ assessment rating (see Criteria for Clinical Evaluation below), the remaining 10% to meet the ‘Assisted’ assessment rating
6. Successfully perform a minimum of ten (10) supervised venipunctures (using 16/ 17
gauge A-V fistula needles) as per ‘Apheresis Venipuncture’ procedure. (refer to Apheresis Manual)
7. Undertake an annual evaluation of core competencies to maintain practice.
A minimum of twenty (20) procedures to be performed per year and 90% of annual evaluation to meet the ‘Independent’ assessment rating criteria.
8. Maintain personal record/ log of procedures performed once initial evaluation
completed successfully.

1st Edition, August 2006 7
Criteria for Clinical Evaluation*
Scale Label
Standard Procedure
Quality of Performance Assistance
Independent
Safe Accurate Effect each Affect time
Proficient, coordinated, confident Occasional expenditure of excess energy Within an expedient time frame
Without supporting cues
Supervised
Safe Accurate Effect} Each Affect} time
Efficient, coordinated, confident Some expenditure of excess energy Within a reasonable time period
Occasional supportive cues
Assisted
Safe Accurate Each time Effect} most of the Affect} time
Skilful in parts of behaviour Inefficiency and uncoordination Expends excess energy Within a delayed time period
Frequent verbal and occasional physical directive cues in addition to supportive ones
Marginal
Safe, but not alone Performs at risk Accurate – not always Effect} occasionally Affect}
Unskilled, inefficient Considerable expenditure of excess energy Prolonged time period
Continuous verbal and frequent physical cues
Dependent
Unsafe Unable to demonstrate behaviour
Unable to demonstrate procedure behaviour Lacks confidence, coordination, efficiency
Continuous verbal and physical cues
X Not observed
*Bondy, K. 1983, ‘Criterion-referenced definitions for rating scales in clinical evaluation’. Journal of Nursing Education, 22, no. 9, pp. 376-382.

1st Edition, August 2006 8
Introduction Apheresis, derived from the Greek words ‘apo’ meaning ‘away’ and ‘heresis’ – ‘taking’, is the process which involves the removal of whole blood, and then separating and collecting any of the components, whilst returning remaining blood components to the patient/donor. In some situations this requires the replacement of a collected component to maintain haemodynamic status. Often the term ‘apheresis’ is prefixed by the name of the component being targeted –
• Plasmapheresis: collection of plasma • Plateletpheresis: collection of platelets • Leukapheresis: collection of white blood cells • Eythrocytapheresis: collection of red blood cells
The advent of sophisticated blood cell separators has dramatically changed the applications of apheresis with increasingly specific blood cells being targeted. Anticoagulated blood is separated either by centrifugation (cells are separated according to size and density) or filtration (cell size) or a combination of both. This technology is now used in both the donor setting for the collection of blood products (apheresis has become an integral component of transfusion medicine) and in therapeutic applications for the treatment of many disease processes - often as supportive therapy alongside conventional therapies such as chemotherapy. Apheresis can be used in adult and paediatric settings safely and effectively. Automated cell separators are machines used to collect and/or treat blood components in apheresis. The devices have an enclosed extracorporeal circuit through which whole blood travels with the aid of pumps. Whole blood is separated within these machines by centrifugation: blood components have different specific gravities. When exposed to centrifugal force blood components will separate according to their specific gravities. This method of separation is the most commonly used in apheresis procedures. Abbreviations
• FBE/FBC - Full Blood Examination/ Full Blood Count • WBC - White blood cell • MNC - Mononuclear cell. • PBPC - Peripheral Blood Progenitor Cell. • PBSC - Peripheral Blood Stem Cell. • G-CSF- Granulocyte Colony Stimulating Factor. • CFU - Colony Forming Units. • DC - Dendritic cells • PVA - Peripheral venous access • CVC - Central Venous Catheter • ACD-A - Anticoagulant Citrate Dextrose solution - A • Hct - Haematocrit • SOP - Standard operating procedure • Plt - Platelet • WCC - White cell count • ARCBS - Australian Red Cross Blood Service • PMN - Polymorphonuclear Leukocytes (neutrophils/ granulocytes) • HPC - Haematopoietic Progenitor Cells

1st Edition, August 2006 9
Definitions Haematopoiesis - Is the process by which circulating blood cells are produced in sufficient numbers, under normal conditions and in times of increased need. Times of increased need may include response to infection, bleeding, and increased oxygen demand after chemotherapy. In infants haematopoiesis occurs in almost every bone. By adulthood it occurs mainly in large bones such as the sternum, ribs, pelvis, skull and the proximal end of the long bones. Leukocytes – Are white blood cells (WBC) & there are three (3) different lineages:
• Granulocytes (neutrophils, basophils, eosinophils) • Monocytes • Lymphocytes
Erythrocytes – Are red blood cells (RBC). Their primary function is to transport haemoglobin that carries oxygen from the lungs to the tissues. Megakaryocytes – Are the precursor to platelets. Their primary function is to participate in the clotting mechanism by adhering to injured tissue & each other to form a clot. Stem Cells – Are produced in the bone marrow from which all blood cells originate. The stem cell is the most primitive cell having the ability to replicate repeatedly and differentiate into both the myeloid or lymphoid cell lines. CD34+ - Is a cell surface antigen representative of a stem cell as well as some other cell types. Currently there are no methods to directly identify or quantitate stem cells therefore CD34 is used as a surrogate marker for stem cells. Dendritic Cells - Dendritic cells (DC) are the most effective or 'professional' of the antigen-presenting cells (APC) that initiate primary immune responses. They are located at surveillance sites where they capture and process antigens. Dendritic cells not only activate lymphocytes to induce the immune response, but they also minimize autoimmune reactions by tolerizing T cells to self-antigens. There is evidence for two developmental lineages for DC: a myeloid line shared with phagocytes, and a lymphoid line shared with T cells. Autologous – A transplant or transfusion in which, the patients own blood / bone marrow / stem cells are used. Allogeneic - A graft or tissue from someone other than the patient, usually a matched sibling (a brother or sister), but may be a matched unrelated volunteer donor.
Human Leukocyte Antigens - Human leukocyte antigen (leukocyte is the name for a white blood cell, while antigen refers to a genetic marker) is a substance that is located on the surface of white blood cells. This substance plays an important role in the body's immune response. Because the HLA antigens are essential to immunity, identification aids in determination of the degree of tissue compatibility between transplant recipients and donors. Testing is done to diminish the likelihood of rejection after transplant, and to minimise graft-versus-host disease (GVHD) following major organ or bone marrow transplantation.
Anticoagulation Anticoagulation of the donor/patient blood whilst in the extracorporeal circuit is necessary to prevent blood from clotting. The anticoagulant of choice for most apheresis procedures is citrate (ACD-A). ADC-A is administered directly into the patient’s blood as it is drawn into the extracorporeal circuit, and then returned to the donor/patient indirectly where it is rapidly metabolised by the kidney, liver and muscles. ACD-A prevents coagulation by lowering the pH of the blood and also binds ionised calcium, essential in the clotting process (Rhomy, 1994). The half-life of ACD-A is 20-60 minutes where

1st Edition, August 2006 10
liver function is normal. A citrate reaction is therefore more likely to occur if the patient has abnormal liver function. Systemic anticoagulants such as heparin are not used in the donor setting. Heparin does not affect the pH or ionised calcium levels in the blood therefore platelet aggregation is not inhibited making the use of heparin as an anticoagulant not conducive for platelet storage (Rhomy, 1994). Vascular Access Good vascular access is essential for a successful apheresis procedure. At least one (1) good cubital fossa vein is required to draw whole blood from the donor/patient. A steel 16-17 gauge backeye butterfly needle is used to support rapid flow of whole blood during apheresis procedures. If good peripheral access is not available, then a large bore central venous catheter should be considered, such as a ‘Vascath’ / ‘Certofix’ (generally 11 – 12 French). Apheresis Procedures Performed at _________________________ (Insert name of institution/department) Tick procedures performed � Peripheral Blood Stem Cell Collection (PBSC) � Therapeutic plasmapheresis (TPE / Plasma exchange,) � Therapeutic Leukapheresis � Plateletpheresis � Therapeutic plateletpheresis � Granulocyte collection � Therapeutic erythrocytapheresis (Red Cell Exchange, RCE) Donor Apheresis Peripheral Blood Stem Cell Collection: Peripheral blood stem cell collection (PBSC) is the collection of haematopoietic progenitor cells (HPC’s) from the peripheral blood circulation of patients and donors. Often called stem cells, these cells have the capability to self renew and differentiate into any of the blood cell lines produced in the bone marrow and are used in bone marrow rescue after high dose chemotherapy for the treatment of leukaemia and other cancers. PBSC harvest/collection has in the main replaced the traditional bone marrow procedure. PBSC collections may be from patients donating cells for their own, future use (autologous collection) or from donors (allogeneic collection). The donor may be matched and related to the recipient, as in the case of a sibling donor, or matched and unrelated to the recipient, as in the case of an Australian Bone Marrow Donor Registry (ABMDR). If the sibling is an identical twin of the recipient the collection is referred to as syngeneic. All donors are tested & matched for six (6) key Human Leukocyte Antigens (HLA) & their associated molecules with the recipient. In either situation the patient/donor receives priming with granulocyte colony stimulating factor injections (G-CSF), a naturally occurring hormone which mobilises HPC’s into the peripheral blood stream. Patients may also receive priming with chemotherapy prior to their collection to enhance cell numbers and limit the possibility of tumour contamination within the collected product. A surface antigen called CD34+ identifies progenitor cells. This enables these cells to be counted when the blood is tested by flow cytometry. The number of collected CD34+ cells in the final product determines whether sufficient progenitor cells have been collected for transplant. Stem cell factor may also be given to patients who have not mobilised with G-CSF. For autologous collections a minimum of 2.0 x 106/kg (recipient bodyweight) CD34+ cells are required. (Referring physician will notify what the target yield will be). Prior to collection the patient will have blood taken for FBE, CD34+, U&E, virology. PBSC collection will go ahead if CD34+ ≥__________________________ plus or minus
Insert minimum CD34 required for collection) WCC ≥_______________________________.
(Insert minimum WCC count required for collection)

1st Edition, August 2006 11
For allogeneic collections, ideally, 4.0 – 6.0 x 106/kg (recipient bodyweight) CD34+ cells are required. Approximately 2-3 total blood volumes of blood are processed through the apheresis machine to ensure adequate cell numbers are collected, and the procedure may take from 3-5 hours to complete. Subsequent collections (at the discretion of the attending physician) are scheduled daily until required cell numbers have been collected. Autologous collections are processed by ____________________ scientific laboratory (Insert name of department) staff, frozen (cryo-preserved) and stored in liquid nitrogen tanks until required for transplantation. Allogeneic collections are generally transfused ‘fresh’ to the patient, either on the day of collection, or the following day if a second collection is required. Allogeneic collections may be stored up to 72 hours at 4º Celsius, allowing for transport to other areas in the country or around the world. PBSC Transplantation PBSC transplantation has been used increasingly in the treatment of malignant and non-malignant haematological disorders and solid tumours. The aim of PBSC and bone marrow transplantation is: • The administration of high dose myelosuppressive chemotherapy to destroy disease with
subsequent stem cell rescue, and • The replacement of diseased bone marrow. (Williams L.A. & McCarthy P.L.) Prior to PBSC transplantation, the collection of an adequate number of stem cells is required using apheresis. Stem Cells/Progenitor Cells The stem cell is the most primitive cell having the ability to replicate repeatedly and differentiate into both the myeloid or lymphoid cell lineages. It has the ability to reconstitute haematopoiesis following ablative treatment to the bone marrow. Currently there is no method to quantify stem cells therefore a surrogate marker, CD34, is used to distinguish stem cells from other cell types. Most stem cells are found in the bone marrow however some are also found in the peripheral circulation but in very small quantities. Approximately 0.03-0.05% of the white blood cells (WBCs) in the peripheral blood of normal healthy individuals express CD34, a marker for stem or progenitor cells. This is in contrast to marrow, in which 3-5% of cells express CD34. (McLeod, 2000). Stem cells in the peripheral circulation are termed Peripheral Blood Progenitor Cells (PBPC). Stem/progenitor cells found in the peripheral blood are in insufficient quantities to adequately collect the required dose for transplantation, therefore a method to ‘mobilise’ stem cells into the peripheral blood is required.
Mobilisation A variety of methods can be used to increase the number of circulating PBSCs/PBPCs in the peripheral blood by “mobilising” them from the bone marrow into the circulation. McLeod (2000) states:
“The rationale for mobilising stem cells is to decrease the number of apheresis procedures required to obtain as many stem and progenitor cells as needed to provide prompt and sustained haematopoietic reconstitution”.
Without mobilisation it takes many donations of lengthy duration to yield sufficient numbers for transplantation. Mobilisation methods include chemotherapy, haematopoietic growth factors and a combination of both.

1st Edition, August 2006 12
• ChemotherapyChemotherapy is used in the autologous transplant setting. A variety of chemotherapeutic regimens can mobilise stem cells into the peripheral circulation. The type of chemotherapeutic regimen used is dependent on the patient’s disease and medical condition. Chemotherapy induces a transient myelosuppression in patients with the leukocyte count dropping to below 1.0 x 109 /L 7-14 days post administration. This is then followed by a “rebound phase” increasing the leukocyte count to well above baseline levels indicating haematopoietic recovery. During this rebound phase, there can be an increase in CD34+ levels up to 20-25 fold of those at baseline. These increased levels can persist for several days during which PBSCs/PBPCs can be collected. Currently chemotherapy alone is not used for mobilisation of PBSCs in the autologous setting. All patients receive G-CSF. • Haematopoietic growth factorsHaematopoietic growth factors are glycoproteins, which act on haematopoietic cells by binding to specific cell surface receptors and stimulating proliferation, differentiation and some end-cell functional activation. Growth factors can be used alone to mobilise stem cells from the bone marrow into the peripheral circulation. G-CSF is the most common of these factors and is administered subcutaneously for 4-5 days prior to apheresis and continues until completion of all donations. Stem cell factor may also be used in cases where mobilisation did not occur using G-CSF. This type of mobilisation method is used both in the allogeneic and autologous settings.
• Chemotherapy and Growth FactorsA combination of both chemotherapy and growth factors has proven to be a very effective mobilisation method. It is currently the most common method of mobilisation in the autologous setting. The combination of the two can increase the circulating CD34+ level up to 100-160 times that of baseline.
• Factors Affecting MobilisationAt times it may be difficult to obtain sufficient amounts of PBSCs/PBPCs for transplantation. Failure to mobilise may be due to a variety of factors, which include: 1. Mobilisation technique 2. Prior treatment- chemotherapy/radiotherapy (i.e.) melphalan, carboplatin and carmustine
(BCNU) administered over long periods of time or in large doses 3. Presence of marrow disease or metastases 4. Diagnosis 5. Patient/Donor age 6. Sepsis 7. Genetic factors
Advantages • No requirement for general anaesthesia as compared with bone marrow donation • Less invasive procedure • Decreased period of neutropenia and thrombocytopenia post transplant due to PBSC/PBPC
being more mature than bone marrow cells Disadvantages • Donor exposure to apheresis related complications • Specific apheresis donor requirements • Potential and unknown adverse effects from mobilisation growth factors • Expensive • Labor intensive • Donor time commitment (may require up to two (2) consecutive donations to obtain a
sufficient yield for transplantation)

1st Edition, August 2006 13
Diagram depicting cell development

1st Edition, August 2006 14
Taken from "Understanding bone marrow and stem cell transplants" by Bacup) http://www.dsrct.demon.co.uk/sct.htm

1st Edition, August 2006 15
Plateletpheresis - Single Donor Platelets Platelets can be donated via apheresis from: 1. Donor volunteers who may be ABO or HLA (Human Leukocyte Antigen) compatible, or 2. Family members Platelets obtained using apheresis are commonly referred to as single donor platelets. One bag of single donor platelets (SDP’s) is equivalent to one bag of ‘pooled’ platelets prepared from whole blood donations. A panel of HLA-typed donors is available from the Australian Red Cross Blood Service (ARCBS). Donations can be taken every 14 - 28 days as per ARCBS guidelines. The cytapheresis unit at ARCBS liaises with the hospital unit to coordinate donation and patient requirements. Specific recipient details and blood tests (for HLA typing if required) are supplied to ARCBS by the requesting doctor. Apheresis platelets contain approximately >240 x 109/unit (or 2.4x1011/unit) of platelets and <1.0 x 106/unit of leucocytes, (as per ARCBS guidelines). Patients undergoing bone marrow transplantation who require matched apheresis platelets will need to have donor collections scheduled to support them throughout the post transplant period. Not all states universally leucodeplete their platelets so please refer to the platelet product label. Indications Indications for single donor platelets are generally for patients who have demonstrated refractoriness to random donor platelet concentrates or to prevent or limit refractoriness. Refractoriness can be defined as “the failure of two (2) consecutive transfusions to give a corrected increment of greater than 7.5 x 10 9/l one (1) hour after transfusion in the absence of fever, infection, severe haemorrhage, splenomegaly or disseminated intravascular coagulation” (Brozovic, Hows & Contreras, 1998). Patients should be tested for the presence of HLA antibodies and, if necessary, the exclusion of anti-HPA-1a. Those who meet the criteria for immunologic refractoriness to platelets should receive either ABO or HLA matched single donor platelets. Advantages:• Limited donor exposure • Leukocyte reduced at time of donation via filtration or elutriation reducing febrile non
haemolytic transfusion reactions and alloimunisation causing platelet refractoriness. • Reduces the risk of CMV transmission • Low RBC count Disadvantages: • Limited availability of group A and O at times •• Labour intensive specific apheresis donor requirements • Donor exposure to apheresis related complications • Family donors: issues of risk disclosure due to coercion and obligation.

1st Edition, August 2006 16
Granulocytes PMN concentrates, commonly referred to as granulocyte transfusions (GTx or “Buffy coats”) are used to treat bacterial, yeast and fungal infections associated with severe neutropenia (<0.5 x10 9/ PMN/L) and disorders of neutrophil function. The use of granulocyte transfusions has been controversial over the years and
“this can be explained in part by the development of more effective antimicrobial agents to treat infections and, possibly, by availability of recombinant haematopoietic growth factors and peripheral blood progenitor transfusions to hasten marrow function, many physicians hold strong negative opinions about the value of GTx – believing it holds little, if any, role in the management of infected neutropenic patients” (Strauss., 1995).
Another limiting factor to the use of granulocyte transfusions was the inadequate number of granulocytes collected to obtain a therapeutic dose and the known possibility of life-threatening pulmonary toxicity, which can occur after transfusion. Granulocytes collections from donors may be used for the treatment of severe neutropenia in patients who have a coexisting intractable infection (bacterial, yeast and fungal infections), which has failed to respond to antibiotic therapy. Daily transfusions are given until the infection has resolved or the patient’s neutrophil count is stable at >0.5 x 109/L. Donors are generally recruited from the patient’s immediate family circle and friends, and are preferably ABO compatible. Routine screening for viral serology is performed prior to the collection and all donors are assessed by the nominated Medical Officer / Consultant for eligibility to donate. The ARCBS donor declaration form may be used to screen donors but ensure you are using the current version of the form. (Available from ARCBS) Granulocytes will require irradiation prior to transfusion; this may be performed in-house if irradiation facilities are available. If not check the in-house policy on where product needs to be sent for irradiation.
In order to maximise collection efficiency (CE%), donors receive oral dexamethasone and G-CSF injections prior to donation to increase the numbers of circulating polymorphonuclear neutrophils (PMNs) in the peripheral blood. A red cell sedimenting agent (e.g., Dextran 70 or equivilant) is added to the extracorporeal circuit to sediment the donor’s red blood cells (RBC) during the collection and therefore ensures enhanced collection of granulocytes with lower RBC contamination The decision to use granulocyte donations is generally one of urgency. Granulocytes are infused daily until there is an improvement in patient’s clinical condition. Donations of granulocytes are taken from the patient’s family and friends. Generally two (2) consecutive donations/donor are required. Extensive donor screening is undertaken according to relevant apheresis service institutional policies and procedures. Although not collected by ARCBS it is advisable that an ARCBS donor declaration form or similar in house form is used in the screening process.
Issues Relating to Donation of Granulocytes • Donor exposure to apheresis related adverse events • Specific apheresis donor requirements • Adverse effects from mobilisation medication • Labour intensive donor work-up • Donor time commitment • Issues relating to donor disclosure of risks due to coercion and obligation

1st Edition, August 2006 17
Dendritic Cells Dendritic cells may be collected for clinical research trials. If your institution is affiliated with research centres you may collect these cells. All trials have their own protocols and specific requirements, refer to in-house protocols for further information. Therapeutic Apheresis The aim of apheresis in this setting is the removal of a harmful circulating factor, which is implicated in a disease process and is causing injury to a given organ. “Therapeutic apheresis is not curative, but rather, it is an adjunct to conventional therapy in which relief of symptoms and control of pathogenic process may be achieved more quickly”. (ASFA). Therapeutic apheresis only affects the intravascular compartment. The efficacy of the treatment is related to: 1. The volume of blood processed, 2. The rate of resynthesis of the offending factor, and 3. The ability of the end organ to repair itself. Therapeutic apheresis can be divided into two (2) areas: 1. Therapeutic Plasma Exchange 2. Therapeutic Cytapheresis Plasmapheresis - the collection of plasma without giving replacement fluid. Therapeutic Plasma Exchange (TPE) Unlike plasmapheresis, plasma exchange is the removal of large quantities of plasma requiring replacement by an appropriate fluid to maintain homeostasis. The goal of TPE is to remove, or reduce to a minimum, the plasma constituents implicated in a disease process. The use of TPE in the treatment of diseases has ranged from being logically sound to highly speculative. According to Urbaniak and Robinson (1998), plasma exchange
“is most successful when there is a measurable, well characterised, pathogenic substance present which causes acute tissue or organ damage that is reversible or preventable by timely intervention”.
Therapeutic plasma exchange (TPE) involves the removal and replacement of a patient’s plasma whilst returning the patient’s own cellular blood components. The intended outcome is the rapid removal of an offending toxin or pathogen thought to be responsible for, or the by-product of, a disease process. For example, in Waldenström’s Macroglobulinaemia, excess plasma proteins such as IgM, can be rapidly removed to alleviate symptoms caused by increased blood viscosity. Adjunctive therapies such as chemotherapy regimens can be given to maintain levels of plasma proteins within normal range. In order for TPE to be effective the substance thought to be causing the disease process needs to be plasma bound, for example, immunoglobulins, fibrinogen and coagulation factors, complement proteins and autoantibodies, thereby ensuring that it can be effectively removed with the patient’s plasma. Replacement fluid is usually Albumin 4%, however in certain disease processes Fresh Frozen Plasma (FFP) or Cryosupernatant Plasma is the preferred replacement. Replacement fluids are given concurrently, with the collection of patient’s plasma into waste bags. This maintains haemodynamic stability. Patients require constant monitoring for problems associated with large volume fluid shifts and reactions to replacement fluids, as well as the general adverse events associated with apheresis. Often 1-1.5 plasma volumes (usually 3-4L) are removed to ensure that the offending pathogen or toxin is removed. Calculations are performed to determine the percentage of plasma in a patient’s total blood volume using the patient’s current haematocrit as determined by full blood examination (FBE). The referring physician prescribes the volume of plasma to be removed.

1st Edition, August 2006 18
Frequency of procedures is determined by the referring physician and would depend on the speed at which the offending substance is renewed in the blood. TPE may be required daily, sometimes twice daily, alternate days or even weekly to maintain a patient’s condition. Long-term maintenance TPE has been effective in treating diseases such as Myasthenia Gravis or chronic, relapsing Thrombotic Thrombocytopenic Purpura (TTP). All referrals for plasma exchange must be reviewed and assessed by the attending physician or registrar of the apheresis service. Patients are also assessed by apheresis qualified nursing staff. TPE has been proven to be an effective therapeutic option for a wide range of medical conditions, from renal disorders such as Goodpasture’s syndrome, neurological disorders such as Myasthenia Gravis and haematological conditions such as TTP. For a comprehensive list of diseases treated and the likely benefits of TPE, refer to the Journal of Clinical Apheresis, Volume 15, Numbers 1 & 2, 2000, Special Issue: Clinical applications of Therapeutic Apheresis. In this journal each indication for TPE is listed according to it’s effectiveness in treating or alleviating the disease process listed. Categories rate from I (considered to be primary therapy) to IV (no benefit shown from controlled trials undertaken, TPE not recommended). Examples of disease processes in which TPE has shown benefit are: • Hyperviscosity Syndrome (Waldenstrom’s Macroglobulinaemia, Multiple Myeloma) • Acute Myasthenia Gravis • C.I.D.P. (Chronic Inflammatory Demyelinating Polyneuropathy) • Goodpasture’s Syndrome • Acute Guillian-Barre Syndrome • TTP (Thrombotic Thrombocytopenia Purpura) • Cryoglobulinaemia • Poisons (mushroom) • Drugs
Replacement Fluids The selection of the type of replacement fluid is an important consideration when prescribing therapeutic plasma exchange. Generally 1 to 1.5 plasma volumes are removed during a plasma exchange treatment and replaced with an equivalent volume of replacement fluid. The replacement fluid of choice is usually Albumin 4% or in combination with 0.9% Normal Saline. FFP replacement is usually not administered as replacement fluid due to the risk of associated transfusion reactions. However, FFP is the choice of replacement fluid used in TTP. NB: When FFP is used as the replacement fluid the ACD-A ratio will need to be adjusted to prevent citrate toxicity due to the citrate component of the FFP, i.e. to reduce the amount of ACD-A given Therapeutic Cytapheresis Rapid removal of cellular components implicated in a disease process Leukocyte CytapheresisIndicated in various forms of leukaemia to rapidly remove white blood cells and reduce blood viscosity thereby preventing neurologic and respiratory impairment. White blood cell (WBC) levels greater than 100 x 109/l can cause fatal problems associated with an increase in blood viscosity, vascular occlusion, and associated problems with blood flow to vital organs. Generally found in patients with myeloproliferative disorders and acute leukaemia, for example, chronic myeloid leukaemia (CML), or acute myeloid leukaemia (AML). The severity

1st Edition, August 2006 19
of the presenting symptoms varies between individual patients and the types and volume of white cell burden within the bloodstream. The role of therapeutic leukapheresis is to initially and rapidly decrease the burden of leukocytosis on the body by 50-60% whilst chemotherapy is commenced. Patients are referred by the attending physician, who will determine the frequency and number of procedures to be performed. Procedure parameters are tailored to the type of white cell being targeted to ensure the greatest collection efficiency. Large volumes of cells may be collected, therefore fluid replacement may be indicated to counter problems associated with hypovolaemia. Therapeutic leukapheresis is often performed as an acute, emergency procedure and the patient may require intensive nursing in an area such as ICU. In this situation the procedure is undertaken in ICU. Red Cell CytapheresisUsed for rapid, isovolaemic removal of large quantities of red cells, which may also be abnormal. e.g. polycythaemia rubra vera, sickle cell crisis. Platelet CytapheresisUsed to rapidly lower platelet counts in patients with myeloproliferative disorders and with platelet count >1000 x 10 9/L. The main aim is to prevent the development of thrombotic and haemorrhagic complications until conventional therapy can control platelet production. It should be noted that in disease processes, which result in thrombocythaemia, the platelets are generally atypical and function poorly and therefore platelet transfusions post apheresis may be indicated (this is rare).

1st Edition, August 2006 20
Apheresis Adverse Events Although apheresis is a relatively safe procedure it is not without potential complications. The rate of adverse events during apheresis is generally greater in therapeutic procedures as compared to donor procedures. This is due to the age and co-morbidities of patients in the therapeutic setting as opposed to healthy donors. Nursing staff must understand these complications and adverse events in order to try and prevent such incidents occurring. The ability of the nurse to detect or pre-empt adverse events and initiate prompt corrective action to minimise the impact to the patient/donor and/or procedure is essential. Many apheresis complications may develop as a result of the procedure itself or alternatively from the patients primary or secondary medical conditions. Identifying any pre existing medical conditions and determining the possible impact on the management of the patient during an apheresis procedure, aids in minimising or preventing any adverse events. (Refer to patient assessment sheet Apheresis manual) The following is a list of potential adverse events associated with apheresis. Hypocalcaemia (citrate toxicity) • Most commonly seen in the donor setting • Related to the infusion of citrate anticoagulant • May be mild, moderate or severe (warranting cessation of procedure) Vasovagal • Common in whole blood donation • Also seen with apheresis procedures but with less frequency. • Related to donor anxiety, fear, pain
Hypovolaemia/Hypervolaemia • Changes in intravascular volume as a result of fluid shifts • Removal of whole blood and retainment of components • Extracorporeal volume i.e.) >15% of donor’s/patient’s whole blood volume in circuitry at any
one time • Fluid overload in patients with cardiac/renal dysfunction • Drug related eg: ACE inhibitors should be withheld 24 hours pre-plasma exchange to prevent
hypovolaemia Vascular Access • Haematoma • Venous sclerosis • Thrombosis • Infection • Nerve, muscle, tendon injury • May be more frequent in apheresis procedures as compared with whole blood donations due
to the longer indwelling time of the catheter
Air Embolism • Malfunction with machine circuitry
Mechanical Haemolysis • Potential destruction of Red Blood Cells within machine circuitry as a result of collapsed or
kinked tubing and improper harnessing of kit
Transfusion Reactions • Therapeutic setting • Associated with blood products used as replacement fluid in plasma exchange i.e. Albumin,
FFP

1st Edition, August 2006 21
Coagulopathy • Therapeutic setting • Altered coagulation status post therapeutic plasma exchange when plasma is exchanged with
replacement fluids, which do not have coagulation factors
Pharmacological Changes • Therapeutic setting • Removal of large quantities of plasma during plasma exchange may decrease the
concentration of certain medications. The quantity of medication removed is related to its plasma binding capacity, distribution and clearance of the drug
Careful monitoring of the donor/patient before, during and after is essential in providing a safe and effective procedure. Astute nursing care and assessment are imperative in the prompt management of reactions, which may occur. Adverse Events Competency Assessment Criteria General
• List four (4) pre existing conditions that may contribute to procedure related adverse events
• State six (6) potential apheresis adverse events & corresponding definitions Haematoma Formation
• Explain two (2) contributing factors to haematoma formation at the site of intravenous cannulation
• Describe three (3) signs & symptoms associated with haematoma • Explain the nursing intervention with suspected & actual haematoma formation
Nerve Injury
• Describe two (2) signs & symptoms of nerve injury • Explain the nursing intervention with suspected or actual nerve injury
Citrate Reaction
• Describe the role of citrate in apheresis procedures • Describe the progression of signs & symptoms if mild, moderate & severe citrate reactions • List 3 factors that predispose patients to citrate reactions • Explain the nursing intervention involved with treating mild, moderate & severe citrate
reactions Vasovagal Episodes
• List three (3) factors that may precipitate a vasovagal episode • Describe the signs & symptoms of a vasovagal episode • Explain the nursing intervention involved for treating a vasovagal episode
Hypovolaemia / Hypervolaemia
• Give definitions of hypovolaemia / hypervolaemia • Describe the two (2) main signs & symptoms of hypovolaemia / hypervolaemia • Explain the nursing interventions involved with hypovolaemia / hypervolaemia
Allergic Reaction
• List two (2) causes of allergic reactions associated with apheresis • Describe four (4) general signs & symptoms of allergic reaction • Explain the nursing interventions involved with allergic reactions • Name three (3) drugs used in the treatment of allergic reactions

1st Edition, August 2006 22
Blood Component Transfusion Reactions • Describe three (3) main signs & symptoms of
o Acute haemolytic transfusion reaction o Non haemolytic transfusion reaction o Allergic reactions
• Explain the immediate nursing intervention associated with blood transfusion reaction
References ASFA. 1998, Principles of Apheresis Technology. Australian Red Cross Blood Service, Transfusion Medicine, Manual 2003. www.arcbs.redcross.org.au
Blood Transfusion Practice & Clinical use of Blood in Australia, www.arcbs.redcross.org.au
Journal of Clinical Apheresis, Volume 15, Numbers 1 & 2, 2000, Special Issue: Clinical applications of Therapeutic Apheresis Kelvy S., Kin H., Sink B., Vammvaskas E. & Weinstein R. (Eds) (1998). Principles of Apheresis Technology. 2nd edition ASFA, Tucson, Arizona. McLeod B., Price T. & Drew M. (Eds) (2000). Apheresis, Principles and Practice. AABB Press, Bethesda Maryland. Urbaniak S.J. & Robinson A. (1998). Therapeutic Apheresis. In M. Contreras (Ed.), ABC of Transfusion. (pp67-70). Rhomy J. (Ed). (1994). Apheresis Topics: Anticoagulant. Hemisphere. 7(4). COBE Laboratories. Brozovic B., Hows J. & Contreras M. (1998). Platelet and Granulocyte Transfusions. In M. Contreras (Ed.), ABC of Transfusion. (pp17-23). Williams L. & McCarthy P.L. Diseases treated with peripheral stem cell transplantation. In Stem Cell Transplantation: A Clinical Textbook.
Websites www.anzsbt.org.auwww.arcbs.redcross.org.auwww.hsanz.org.auwww7.health.gov.au/nhmrc

1st Edition, August 2006 23
Recommended Reading (To be updated & revised by individual apheresis units) ‘Apheresis manual’ – ________________________department (Insert name ofinstitution / department)
ASFA. 1998, Principles of Apheresis Technology. Lopez, J & Hausz, M. Therapeutic Apheresis, American Journal of Nursing/Oct (pp 1572-1578. McLeod, B. 1997 Apheresis Principles & Practice AABB Maryland USA (pp67 –80, 223 - 239) Price, C & McCarley, P. Technical Considerations of Therapeutic plasma exchange a Nephrology Nursing Procedure, ANNA Journal/Febuary 1993/vol20/No 1(PP41 – 46). Price, C & McCarley, P. Physical Assessment for Patients Receiving Therapeutic Plasma Exchange, ANNA Journal/June 1994/vol21/No 4. Purandare, L Therapeutic Apheresis, Professional Nurse June, 1994 (pp626 - 631) Sigmon, J. Basic Principles of the ABO and Rh blood Group Systems for Hemapheresis practitioners, 1992, Wiley-Liss, Inc. (pp208 – 213) Tortora, G, Principles of Anatomy & Physiology 5th Ed, Physiology of Circulation (pp 492 – 498. Wake, B. Blood volume calculations, apheresis update 1995 RAH. Weeks, D, Washing the blood, RN may 1991 (pp60 - 64)
Acknowledgements Melisa Darby – Peter MacCallum Institute, Victoria Slavica Curcic – Austin Health, Victoria Dr Carole Smith – Austin Health, Victoria Dr Marija Borosak – ARCBS, Victoria Dr Erica Wood – ARCBS, Victoria Apheresis Interest Group, Victoria Dawn Thorp – “Apheresis Guru”, Adelaide Angela Booth – Bone Marrow Transplant Network, New South Wales

1st Edition, August 2006 24
Insert name of Institution & Department Core competency assessment for
Haemonetics MCS plus
Date: Assessor’s Name:
TraineeNname:
Procedure Type:
Procedure No.
Rating scale: Independent (I), Supervised (S), Assisted (A), Marginal (M), Dependent (D), Not observed (X), Not applicable (N) (Bondy, K. 1983) 1. Installation Set-up and Prime:
Assessment rating Checklist I S A M D X NSelects appropriate procedure worksheet & checklist. Prior to powering machine on ensures correct protocol card is inserted
Chooses appropriate disposable set and in-date solutions. Powers on apheresis machine selects appropriate procedure. Performs disposable set up correctly as per machine manufacturer’s operator manual for Haemonetics MCS +.
Correctly follows LED prompts to auto load pumps. Correctly follows LED prompts to initiate kit prime. Attaches additional infusion lines as per appropriate SOP (TPE only). Records correct patient details, UR number, Lot nos. and expiry date on appropriate procedure worksheet.
Checks pre-procedure laboratory tests (where available). Enters Hct into patient parameters screen.
Gathers appropriate equipment for vascular access & collection of any requested blood tests. Identifies alarms and resolves problem.

1st Edition, August 2006 25
2. Patient preparation:
Assessment rating Checklist I S A M D X NGathers patient medical history from HIS. Ensures correct paperwork has been completed i.e. patient consent, IV fluid orders, medical assessment if new patient, medication order.
Verbally identifies patient/donor. Checks date of birth and patient ID label details.
Reviews: Medical assessment sheet �, Therapeutic apheresis referral �, ARCBS Cytapheresis donation record and completed Blood donation statement/medical questionnaire �, (tick appropriate box).
Measures height & weight of patient & enters into patient parameters of machine.
Ensures machine set up checklist is completed by second staff member prior to commencement of procedure.
Orientates patient/donor to environment, including accompanying significant others.
Positions patient/donor comfortably. Explains procedure including potential adverse events, or verifies knowledge of procedure – documents witnessed consent on consent form (as required).
Performs initial patient assessment, vital signs and venous access, checks patient has eaten & been to the toilet.
Uses appropriate replacement fluid for procedure/disease being treated. Verbally and visually checks fluid replacement with second staff member, verifying patient name, UR number, DOB, blood group and expiry date (as applicable).
Performs venous access as per relevant SOP for venipuncture, CVC’s and A-V fistula cannulation.
Takes required pre procedure specimens as documented in appropriate SOP or as requested by MO on pathology request form and labels specimens according to SOP.
3. Procedure commencements and monitoring:
Assessment rating Checklist I S A M D X NInitiates procedure, documents time of commencement on appropriate worksheet.
Maintains adequate draw/return flow rates, assesses patient/donor comfort and venepuncture / CVC sites during procedure.
Checks anticoagulant flow rate, adjusts according to recommended parameters as per SOP.
Records procedure parameters & patient vital signs on worksheet every 15 minutes.
Maintains fluid balance during procedure as indicated by patient’s history and status.
Attends to alarm conditions promptly and accurately. Is able to access and change parameters via LED screen during procedure to maximise procedure efficiency and patient comfort.
Adjusts whole blood endpoint as appropriate for procedure.

1st Edition, August 2006 26
Monitors patient / donor for signs & symptoms of citrate toxicity & responds appropriately to resolve as necessary.
Identifies adverse reactions promptly and responds appropriately to resolve or minimise reaction.
On completion of procedure, takes post procedure specimens as indicated in relevant SOP, or as requested by MO maintaining asepsis. Ensure patient vital signs stable.
4. Post procedure care:
Assessment rating Checklist I S A M D X NRemoves venipuncture needles and disposes of sharps in appropriate biohazard sharps container.
Applies pressure bandage to avoid haematoma and bleeding. Applies adequate pressure to A-V fistula to prevent bleeding/haematoma.
Follows ______________________ guidelines for flushing and (insert department name
heparinisation of CVC’s.)
Takes post procedure vital signs prior to patient getting up. Provides post procedure instructions to patient as per ‘Apheresis Manual’ SOP. Offers refreshments as required.
Removes collected product and labels according to relevant SOP. Ensures safe delivery or collection of product to appropriate recipient as per SOP.
Completes details on appropriate procedure worksheet, documents procedure in patient medical notes and other documents as applicable to__________________________ (insert department name)
Removes and disposes of disposable kit in biohazard receptacle. Cleans area as per ‘Machine maintenance’ SOP.
5. Review questions:
Assessment rating Checklist I S A M D X NAble to explain rationale for procedure and anticipated outcomes, including target yields of collected products.
Identifies causes and treatment for vasovagal reactions in apheresis. (Initial review)
Identifies causes and treatment for citrate reactions in apheresis. (Initial review)
Identifies causes and first line management of cardiac arrest (Initial review)
Identifies causes and treatment for venous access problems. (Initial review)

1st Edition, August 2006 27
6. Comments: …………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………
Initial / Annual Evaluation Successful: Yes ���� No ����
Review Date:
Assessor’s Signature:
Trainee Signature:

1st Edition, August 2006 28
Insert name of department/ hospital Core competency assessment for
Baxter CS-3000 plus with/without AMS
Date: Assessor’sName:
Trainee Name:
Procedure Type:
Procedure No.
Rating scale: Independent (I), Supervised (S), Assisted (A), Marginal (M), Dependent (D), Not observed (X), Not applicable (N) (Bondy, K. 1983) 1. Installation Set-up and Prime:
Assessment rating Checklist I S A M D X N
Selects appropriate procedure worksheet & checklist.
Powers on apheresis machine, selects appropriate procedure. Chooses appropriate separation and collection containers for procedure.
Chooses appropriate disposable set and in-date solutions.
Performs disposable set up correctly as per machine manufacturer’s operator manual.
Initiates prime sequence, strings AC ratio wheel at step 2 of prime (where appropriate).
Primes inlet and return lines.
Attaches additional collection bags and reinfusion lines as per appropriate SOP (RCE, TPE only).
Records correct patient ID details, UR number, Lot nos. and expiry on appropriate procedure worksheet.
Identifies alarms and resolves problems.

1st Edition, August 2006 29
2. Patient preparation:
Assessment rating Checklist I S A M D X NGathers patient medical history. Ensures correct paperwork has been completed i.e. patient consent, IV fluid orders, medical assessment if new patient, medication order.
Verbally identifies patient/donor. Checks date of birth and patient ID label details.
Reviews: PBPC prescription �, Therapeutic apheresis referral �,ARCBS Cytapheresis donation record and completed Blood donation statement/medical questionnaire �, ABMDR referral � (tick appropriate box).
Checks pre-procedure laboratory tests (where available). Gathers appropriate equipment for vascular access & collection of any requested blood tests.
Orientates patient/donor to environment, including accompanying significant others.
Positions patient/donor comfortably. Explains procedure including potential adverse events, or verifies knowledge of procedure – documents witnessed consent on consent form (as required).
Performs initial patient assessment, vital signs and venous access review. Checks patient has eaten & been to the toilet.
Uses appropriate replacement fluid for procedure/disease being treated. Verbally and visually checks fluid replacement with second staff member, verifying patient name, UR number, DOB, blood group and expiry date (as applicable).
Performs venous access as per relevant SOP for venipuncture, CVC’s and A-V fistula cannulation.
Takes required pre procedure specimens as documented in appropriate SOP or as requested by MO on pathology request form and labels specimens according to SOP.
3. Procedure commencement and monitoring:
Assessment rating Checklist I S A M D X NInitiates procedure, documents time of commencement on appropriate worksheet.
Maintains adequate draw/return flow rates, assesses patient/donor comfort and venipuncture / CVC sites during procedure.
Checks anticoagulant flow rate, adjusts according to recommended parameters as per SOP. Accurately re-strings ratio wheel (as applicable) to deliver recommended AC ratio.
Records procedure parameters & patient vital signs on worksheet every 15 minutes.
Adjusts run parameters as per relevant SOP. Maintains fluid balance during procedure as indicated by patient’s history and status.

1st Edition, August 2006 30
Attends to alarm conditions promptly and accurately. Is able to access and change parameters via operator panel/manual control panel during procedure to maximise procedure efficiency and patient comfort.
Adjusts whole blood endpoint as appropriate for procedure. Monitors patient / donor for signs & symptoms of citrate toxicity & responds appropriately to resolve as necessary.
Identifies adverse reactions promptly and responds appropriately to resolve or minimise reaction.
Performs reinfusion when procedure complete, takes post procedure specimens as indicated in relevant SOP, maintaining asepsis.
4. Post procedure care:
Assessment rating Checklist I S A M D X NRemoves venipuncture needles and disposes of sharps in appropriate biohazard sharps container.
Applies pressure bandage to avoid haematoma and bleeding. Applies adequate pressure to A-V fistula to prevent bleeding/haematoma.
Follows ______________________ guidelines for flushing and (insert department name)
heparinisation of CVC’s.
Takes post procedure vital signs prior to patient getting up. Provides post procedure instructions to patient as per ‘Apheresis Manual’ SOP. Offers refreshments as required.
Removes collected product and labels according to relevant SOP. Ensures safe delivery or collection of product to appropriate recipient as per SOP.
Completes details on appropriate procedure worksheet, documents procedure in patient medical notes and other documents as applicable to _______________________ (insert department name)
Removes and disposes of disposable kit in biohazard receptacle. Cleans area as per ‘Machine maintenance’ SOP.

1st Edition, August 2006 31
5. Review questions:
Assessment rating Checklist I S A M D X NAble to explain rationale for procedure and anticipated outcomes, including target yields of collected products.
Identifies causes and treatment for vasovagal reactions in apheresis. (Initial review).
Identifies causes and treatment for citrate reactions in apheresis. (Initial review).
Identifies causes and first line management of cardiac arrest. (Initial review).
Identifies causes and treatment for venous access problems. (Initial review).
6. Comments: …………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………
Initial / Annual Evaluation Successful: Yes ���� No ����
Review Date:
Assessor’s Signature:
Trainee Signature:

1st Edition, August 2006 32
Insert name of Institution & Department
Core competency assessment for Baxter Amicus
Date: Assessor’s Name:
Trainee Name:
Procedure Type:
Procedure No.
Rating scale: Independent (I), Supervised (S), Assisted (A), Marginal (M), Dependent (D), Not observed (X), Not applicable (N) (Bondy, K. 1983) 1. Installation Set-up and Prime:
Assessment rating Checklist I S A M D X NSelects appropriate procedure worksheet.
Powers on apheresis machine, selects appropriate procedure.
Chooses appropriate spool holder for procedure. Chooses appropriate disposable set and in-date solutions. Performs disposable set up correctly as per machine manufacturer’s operator manual.
Initiates prime sequence as per machine prompts.
Records correct patient details, UR number, Lot nos. and expiry on appropriate procedure worksheet.
Identifies alarms and resolves problems. Primes inlet and return lines.

1st Edition, August 2006 33
2. Patient preparation
Assessment rating Checklist I S A M D X NGather patient medical history. Ensure correct paperwork has been completed ie patient consent, IV fluid orders, medical assessment if new patient, medication order.
Verbally identifies patient/donor. Checks date of birth and patient ID label details.
Reviews: PBPC prescription �, Therapeutic apheresis referral �,ARCBS Cytapheresis donation record and completed Blood donation statement/medical questionnaire �, ABMDR referral � (tick appropriate box).
Checks pre procedure laboratory tests (where available). Orientates patient/donor to environment, including accompanying significant others.
Positions patient/donor comfortably. Gathers appropriate equipment for vascular access & collection of any requested blood tests. Explains procedure including potential adverse events, or verifies knowledge of procedure – documents witnessed consent on consent form (as required).
Performs initial patient assessment, vital signs and venous access. Checks patient has eaten & been to the toilet.
Enters patient/donor parameters via touch screen as relevant to procedure.
Performs venous access as per relevant SOP for venipuncture, CVC’s and A-V fistula cannulation.
Takes required pre procedure specimens as documented in appropriate SOP or as requested by MO on pathology request form and labels specimens according to SOP.
3. Procedure commencements and monitoring:
Assessment rating Checklist I S A M D X NInitiates procedure, documents time of commencement on appropriate worksheet.
Maintains adequate draw/return flow rates, assesses patient/donor comfort and venipuncture / CVC sites during procedure.
Checks citrate infusion rate, adjusts according to recommended parameters as per SOP.
Records procedure parameters & patient vital signs on worksheet every 15 minutes.
Attends to alarm conditions promptly and accurately.

1st Edition, August 2006 34
Is able to access and change parameters via touch screen during procedure to maximise procedure efficiency and patient comfort.
Adjusts whole blood endpoint as appropriate for procedure. Monitors patient / donor for signs & symptoms of citrate toxicity & responds appropriately to resolve as necessary.
Identifies adverse reactions promptly and responds appropriately to resolve or minimise reaction.
Performs reinfusion when procedure complete, takes post procedure specimens as indicated in SOP, or as requested by MO, maintaining asepsis. Labels specimens according to SOP.
4. Post procedure care:
Assessment rating Checklist I S A M D X NRemoves venipuncture needles and disposes of sharps in appropriate biohazard sharps container.
Applies pressure bandage to avoid haematoma and bleeding. Applies adequate pressure to A-V fistula to prevent bleeding/haematoma.
Follows ______________________ (insert department name) guidelines for flushing and heparinisation of CVC’s.
Takes post procedure vital signs prior to patient getting up. Provides post procedure instructions to patient as per ‘Apheresis Manual’ SOP. Offers refreshments as required.
Removes collected product and labels product according to relevant SOP. Ensures safe delivery or collection of product to appropriate recipient as per SOP.
Completes details on appropriate procedure worksheet, documents procedure in patient medical notes and other documents as applicable to ___________________________ (insert department name)
Removes and disposes of disposable kit in biohazard receptacle. Cleans area as per ‘Machine maintenance’ SOP.
5. Review questions:
Assessment rating Checklist I S A M D X NAble to explain rationale for procedure and anticipated outcomes, including target yields of collected products.
Identifies causes and treatment for vasovagal reactions in apheresis. (Initial review).
Identifies causes and treatment for citrate reactions in apheresis. (Initial review).
Identifies causes and first line management of cardiac arrest. (Initial review).
Identifies causes and treatment for venous access problems. (Initial review).

1st Edition, August 2006 35
6. Comments: …………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………
Initial / Annual Evaluation Successful: Yes ���� No ����
Review Date:
Assessor’s Signature:
Trainee Signature:

1st Edition, August 2006 36
Insert name of Institution & Department
Core competency assessment for Gambro COBE Spectra
Date: Assessor’s Name:
Trainee Name:
Procedure Type:
Procedure No.
Rating scale: Independent (I), Supervised (S), Assisted (A), Marginal (M), Dependent (D), Not observed (X), Not applicable (N) (Bondy, K. 1983) 1. Installation Set-up and Prime:
Assessment rating Checklist I S A M D X NSelects appropriate procedure worksheet.
Chooses appropriate disposable set and in-date solutions.
Powers on apheresis machine. Performs disposable set up correctly as per machine manufacturer’s operator’s manual.
Chooses appropriate procedure. Initiates prime sequence.
At the end of prime, follows menu prompts to perform Alarm tests.
Records correct patient details, UR number, Lot nos. and expiry on appropriate procedure worksheet.
Enters patient data (height, weight, haematocrit, WCC etc) accurately to relevant procedure.
Records parameters entered on appropriate procedure worksheet.
Identifies alarms and resolves problem.

1st Edition, August 2006 37
2. Patient preparation:
Assessment rating Checklist I S A M D X NGathers patient medical history. Ensures correct paperwork has been completed i.e. patient consent, IV fluid orders, medical assessment if new patient, medication order.
Verbally identifies patient/donor. Checks date of birth and patient ID label details.
Reviews: PBPC prescription �, Therapeutic apheresis referral �,ARCBS Cytapheresis donation record and completed Blood donation statement/medical questionnaire �, ABMDR referral � (tick appropriate box).
Checks pre procedure laboratory tests (where available). Gathers appropriate equipment for vascular access & collection of any requested blood tests.
Orientates patient/donor to environment, including accompanying significant others.
Positions patient/donor comfortably. Explains procedure including potential adverse events, or verifies knowledge of procedure – documents witnessed consent on consent form (as required).
Performs initial patient assessment, vital signs and venous access. Checks patient has eaten & been to the toilet.
Uses appropriate replacement fluid for procedure/disease being treated. Verbally and visually checks fluid replacement with second staff member, verifying patient name, UR number, DOB, blood group and expiry date (as applicable).
Performs venous access as per relevant SOP for venipuncture, CVC’s and A-V fistula cannulation.
Takes required pre procedure specimens as documented in appropriate SOP or as requested by MO on pathology request form and labels specimens according to SOP.
3. Procedure commencements and monitoring:
Assessment rating Checklist I S A M D X NInitiates procedure, documents time of commencement on appropriate worksheet.
Maintains adequate draw/return flow rates, assesses patient/donor comfort and venipuncture / CVC sites during procedure.
Checks anticoagulant flow rate, adjusts according to recommended parameters as per SOP.
Records procedure parameters & patient vital signs on worksheet every 15 minutes.
Maintains fluid balance during procedure as indicated by patient’s history and clinical indications / status.
Attends to alarm conditions promptly and accurately. Is able to access and change parameters via LED screen during procedure to maximise procedure efficiency and patient comfort.
Monitors patient / donor for signs & symptoms of citrate toxicity & responds appropriately to resolve as necessary.
Identifies adverse reactions promptly and responds appropriately to

1st Edition, August 2006 38
resolve or minimise reaction. Performs rinseback (not RCE procedures) when procedure complete. In RCE procedures, terminates procedure when endpoint values reached.
On completion of procedure, takes post procedure specimens as indicated in relevant SOP, or as requested by MO maintaining asepsis.
4. Post procedure care:
Assessment rating Checklist I S A M D X NRemoves venipuncture needles and disposes of sharps in appropriate biohazard sharps container.
Applies pressure bandage to avoid haematoma and bleeding. Applies adequate pressure to A-V fistula to prevent bleeding/haematoma.
Follows ______________________ (insert department name) guidelines for flushing and heparinisation of CVC’s.
Takes post procedure vital signs prior to patient getting up. Provides post procedure instructions to patient as per ‘Apheresis Manual’ SOP. Offers refreshments as required.
Removes collected product and labels product according to relevant SOP. Ensures safe delivery to/or collection of product by appropriate person/department as per SOP.
Completes details on appropriate procedure worksheet, documents procedure in patient medical notes and other documents as applicable to ___________________________ (insert department name)
Removes and disposes of disposable kit in biohazard receptacle. Cleans area as per ‘Machine maintenance’ SOP.
5. Review questions:
Assessment rating Checklist I S A M D X NAble to explain rationale for procedure and anticipated outcomes, including target yields of collected products.
Identifies causes and treatment for vasovagal reactions in apheresis. (Initial review)
Identifies causes and treatment for citrate reactions in apheresis. (Initial review)
Identifies causes and first line management of cardiac arrest. (Initial review)
Identifies causes and treatment for venous access problems. (Initial review)

1st Edition, August 2006 39
6. Comments: ……………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………
Initial / Annual Evaluation Successful: Yes ���� No ����
Review Date:
Assessor’s Signature:
Trainee Signature:

1st Edition, August 2006 40
Insert name of Institution & Department
Core Competency Assessment for the Fresenius HemoCare COM.TEC
Date: Assessor’s Name:
Trainee Name:
Procedure Type:
Procedure No.:
Rating scale: Independent (I), Supervised (S), Assisted (A), Marginal (M), Dependent (D), Not observed (X), Not applicable (N) (Bondy, K. 1983) 1. Installation Set-up and Prime:
Assessment rating Checklist I S A M D X NSelects appropriate procedure worksheet.
Powers on apheresis machine, selects appropriate procedure.
Chooses appropriate chamber holder for procedure. Chooses appropriate disposable set and in-date solutions. Performs disposable set up correctly as per instrument ‘HELP’ screen and/or manufacturer’s operator manual.
Initiates prime sequence as per machine prompts.
Records correct patient details, UR number, Lot nos. and expiry on appropriate procedure worksheet.
Identifies alarms and resolves problems. Enters patient data (height, weight, haematocrit, WCC, pre CD34 etc.) accurately to relevant procedure.

1st Edition, August 2006 41
2. Patient preparation
Assessment rating Checklist I S A M D X NGather patient medical history. Ensure correct paperwork has been completed i.e. patient consent, IV fluid orders, medical assessment if new patient, medication order.
Verbally identifies patient/donor. Checks date of birth and patient ID label details.
Reviews: PBPC prescription �, Therapeutic apheresis referral �,ARCBS Cytapheresis donation record and completed Blood donation statement/medical questionnaire �, ABMDR referral � (tick appropriate box).
Checks pre procedure laboratory tests (where available). Orientates patient/donor to environment, including accompanying significant others.
Positions patient/donor comfortably. Gathers appropriate equipment for vascular access & collection of any requested blood tests.
Explains procedure including potential adverse events, or verifies knowledge of procedure – documents witnessed consent on consent form (as required).
Performs initial patient assessment, vital signs and venous access. Checks patient has eaten & been to the toilet.
Enters patient/donor parameters via operator screen as relevant to procedure.
Performs venous access as per relevant SOP for venipuncture, CVC’s and A-V fistula cannulation.
Takes required pre procedure specimens via Pre-Sample bag and Vacuette as documented in appropriate SOP or as requested by MO on pathology request form and labels specimens according to SOP.
3. Procedure commencements and monitoring:
Assessment rating Checklist I S A M D X NInitiates procedure, documents time of commencement on appropriate worksheet.
Maintains adequate draw/return flow rates, assesses patient/donor comfort and venepuncture / CVC sites during procedure.
Checks citrate infusion rate, adjusts according to recommended parameters as per SOP.
Records patient vital signs on worksheet every 15 minutes. N.B. The COM.TEC Blood Cell Separator automatically provides a thermal ‘print-out’ of all procedural information (events and parameters entered including alarm codes and resolution action). Institution guidelines/SOP’s may include this printout in medical records for future reference.
Attends to alarm conditions promptly and accurately. Is able to access and change parameters via operator screen during procedure to maximise procedure efficiency and patient comfort.
Adjusts whole blood endpoint as appropriate for procedure. Monitors patient / donor for signs & symptoms of citrate toxicity & responds appropriately to resolve as necessary.

1st Edition, August 2006 42
Identifies adverse reactions promptly and responds appropriately to resolve or minimise reaction.
Performs reinfusion when procedure complete, takes post procedure specimens as indicated in SOP , or as requested by MO, maintaining asepsis. Labels specimens according to SOP.
4. Post procedure care:
Assessment rating Checklist I S A M D X NRemoves venepuncture needles and disposes of sharps in appropriate biohazard sharps container.
Applies pressure bandage to avoid haematoma and bleeding. Applies adequate pressure to A-V fistula to prevent bleeding/haematoma.
Follows ______________________ guidelines for flushing (insert department name) and heparinisation of CVC’s.
Takes post procedure vital signs prior to patient getting up. Provides post procedure instructions to patient as per ‘Apheresis Manual’ SOP. Offers refreshments as required.
Removes collected product and labels product according to relevant SOP. Ensures safe delivery or collection of product to appropriate recipient as per SOP.
Completes appropriate details procedure worksheet, documents procedure in patient medical notes and other documents as applicable to ___________________________ (insert department name) N.B. The COM.TEC Blood Cell Separator automatically provides a thermal ‘print-out’ of all procedural information (events and parameters entered including alarm codes and resolution action). Institution guidelines/SOP’s may include this printout in medical records for future reference.
Removes and disposes of disposable kit in biohazard receptacle. Cleans area as per ‘Machine maintenance’ SOP.
5. Review questions:
Assessment rating Checklist I S A M D X NAble to explain rationale for procedure and anticipated outcomes, including target yields of collected products.
Identifies causes and treatment for vasovagal reactions in apheresis. (Initial review).
Identifies causes and treatment for citrate reactions in apheresis. (Initial review).
Identifies causes and first line management of cardiac arrest. (Initial review).
Identifies causes and treatment for venous access problems. (Initial review).

1st Edition, August 2006 43
6. Comments: ……………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………
Initial / Annual Evaluation Successful: Yes ���� No ����
Review Date:
Assessor’s Signature:
Trainee Signature:





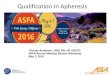






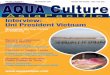





![3.3.5 Msa Kisangani Railway Ext Aug06 - En - Cleaned[1]](https://img.pdfslide.us/doc/110x75/577cdb651a28ab9e78a80ff5/335-msa-kisangani-railway-ext-aug06-en-cleaned1.jpg)









