Embed Size (px)
Citation preview
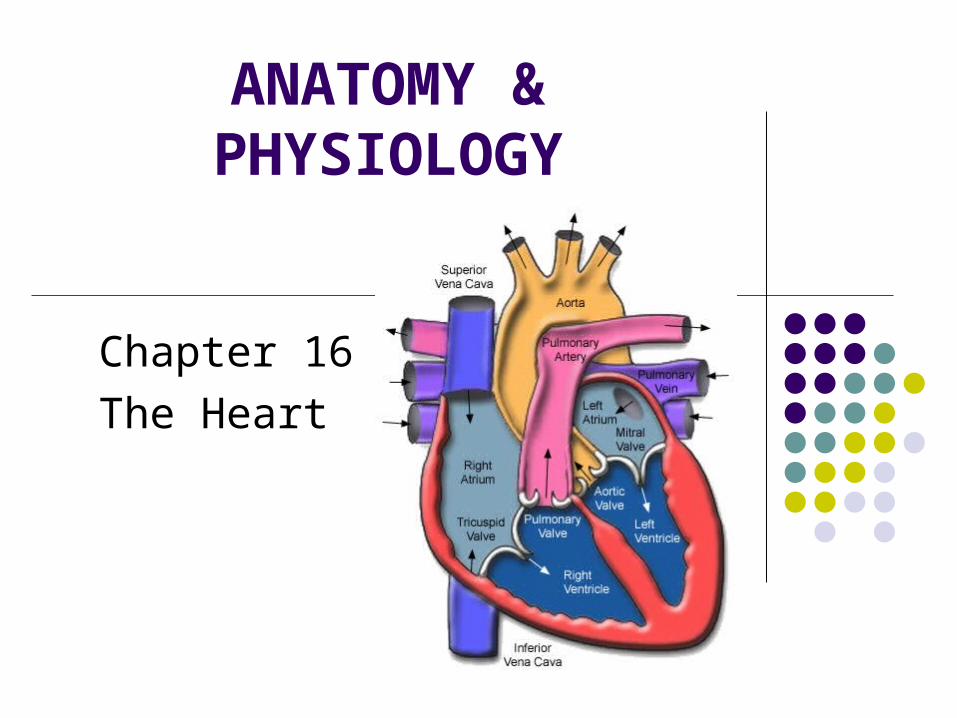
ANATOMY & PHYSIOLOGY
Chapter 16The Heart
HEART CIRCULATES THE BLOOD! It is about the size of a closed fist. Located in the thoracic cavity, within the mediastinum, between
the lungs, behind the sternum, in front of the vertebral column and above the diaphragm.
2/3 of the heart lies toward the left chest. Base of the heart: is the flat upper portion. Apex of the heart: the pointed end of the heart. Precordium: refers to the anterior chest wall overlying the heart &
great vessels Apical pulse: left mid-clavicular line @ the 5th intercostal space When an individual is at rest the heart beats approx 72-80 bpm.
STRUCTURE Hollow, muscular organ Surrounded by the pericardium Contains a lubricating fluid that prevents
friction Endocardium: smooth tissue, inner lining,
covering the valves and lines the vessels. Myocardium: makes up the major portion of
the heart—cardiac muscle tissue. It is middle layer of the heart. Epicardium: thin, outermost layer of the heart,
this layer helps form the pericardium.
Pericardium: this is the sling-like structure that supports the heart
Remember this serous membrane and its layers??? Visceral pericardium-pericardial cavity-parietal
pericardium An inflammation of the pericardium is called
pericarditis and it is characterized with a sound called friction rub.
A collection of excess fluid in this space is called pericardial effusion, this will compress the heart, making it difficult for it to relax and fill with blood, the pump will be ineffective. This is a life threatening situation called cardiac tamponade and must be relieved.
TWO HEARTS IN ONE! Right Heart & Left Heart Right heart: receives unoxygenated blood from the
superior & inferior vena cavae. The right heart pumps blood to the lungs where it is
oxygenated. It returns to…. Left heart: it is from here that blood is pumped to the
organs of the body. This circulation heart to lungs and back to heart is
called pulmonary circulation The circulation from the left heart to the organs and
back to the heart is called systemic circulation.
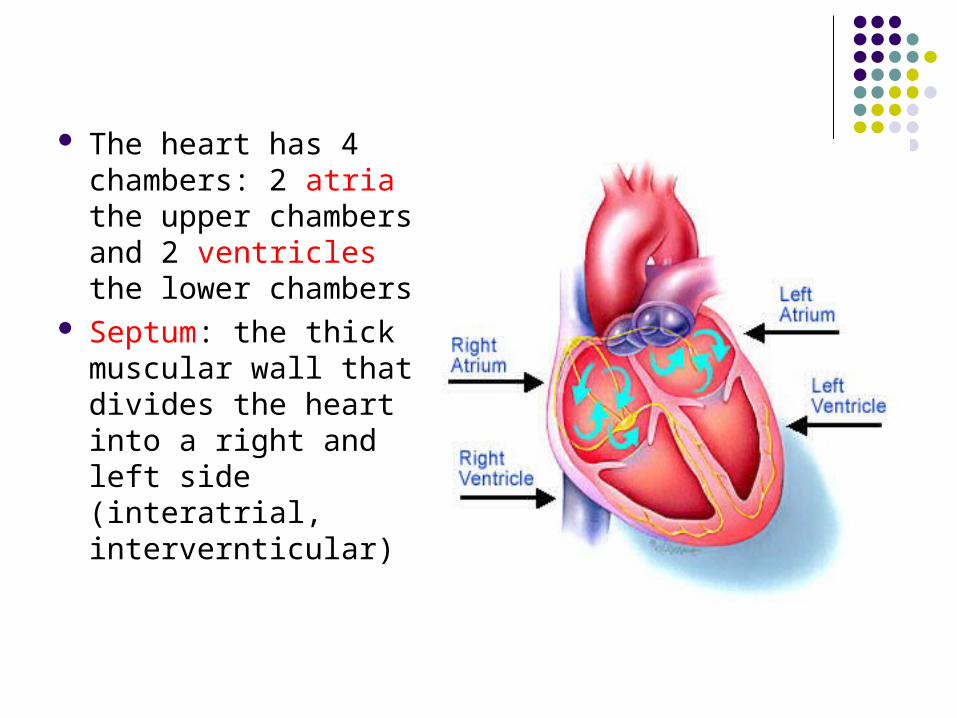
The heart has 4 chambers: 2 atria the upper chambers and 2 ventricles the lower chambers
Septum: the thick muscular wall that divides the heart into a right and left side (interatrial, intervernticular)
Right Atrium: thin-walled cavity that receives the unoxygenated blood from the vena cavae.
Right Ventricle: receives the unoxygenated blood from the right atrium—the function is to pump the blood thru the pulmonary arteries to the lungs.
Left Atrium: thin-walled cavity that receives the oxygenated blood from the lungs via the pulmonary veins.
Left Ventricle: receives the oxygenated blood from the left atrium and then pumps the blood into the systemic circulation thru the aorta (the largest artery in the body).
The left ventricle is thick compared to the atria and the right ventricle—this is important it takes great force to pump this blood throughout the body.
If the ventricles are forced to “overwork”, they will eventually enlarge, a condition called ventricular hypertrophy.
Chronic HTN can develop L ventricular hypertrophy, because the high blood pressure in the aorta makes it difficult for the (L) ventricle to pump blood into the aorta. The (L) ventricle enlarges if the BP is not lowered.
A client with pulmonary artery hypertension develops (R) ventricular hypertrophy and (R) heart failure for the same reason.
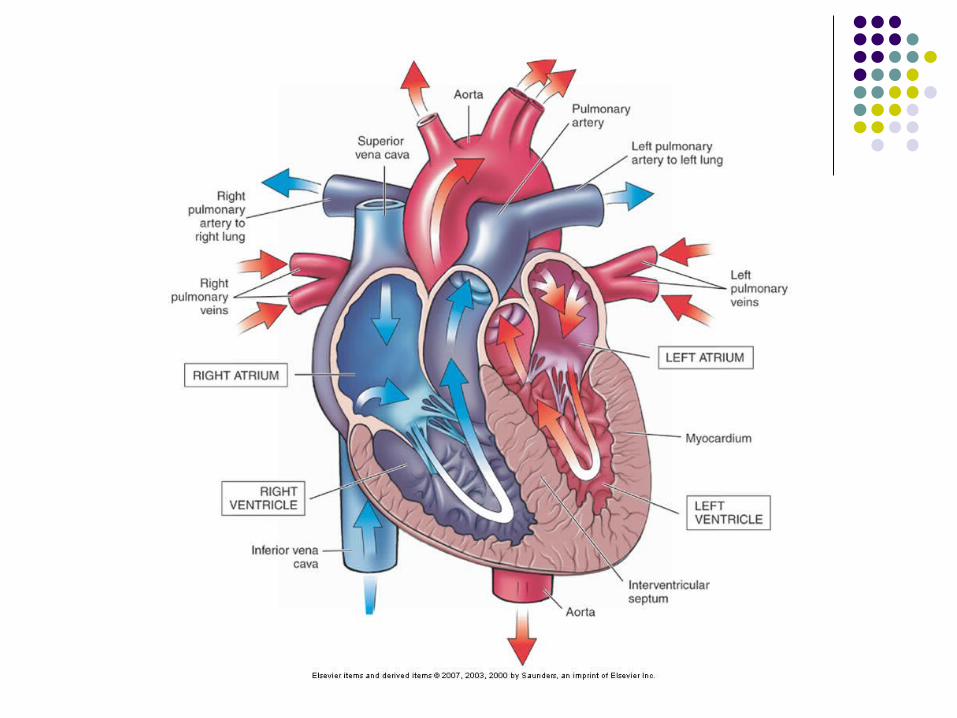
The great vessels are the large blood vessels attached to the heart.
They consist of the: Superior & Inferior Vena Cavae Pulmonary Artery Pulmonary Vein Aorta
There are four valves: atrioventricular (tricuspid, bicuspid), and semilunar (pulmonic, aortic).
The valves open & close when the heart contracts--they allow the blood to flow in one direction—prevents “backups”.
The valves lie at the entrance and exit of the ventricles.
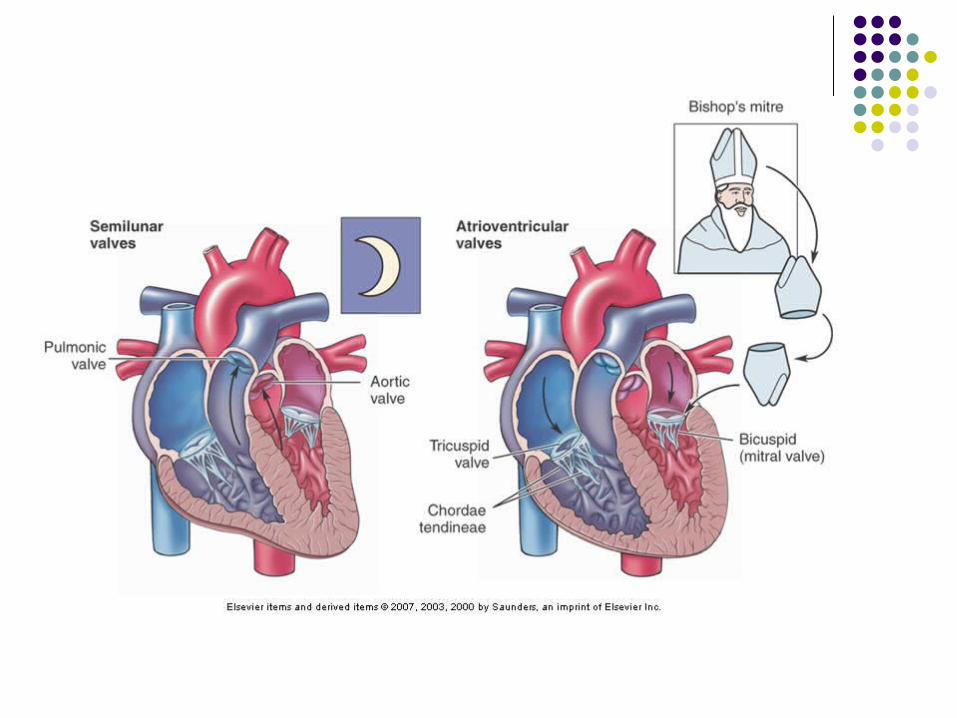
Atrioventricular Valves Between the atrium & ventricle
Tricuspid Between the Rt atrium & Rt ventricle—contains 3
“cusps” (flaps) It contains the Chordae Tendineae which are fibrous
strands that connect the tricuspid valve edges with the papillary muscles and prevents inversion of the tricuspid valve when the ventricle contracts.
**FYI it is a medical emergency if there is a rupture of Chordae Tendinae
Keeps blood flowing from the Rt atrium to Rt ventricle.
Bicuspid (Mitral) Between the L atrium & L ventricle—contains two
“cusps”. It allows the blood to flow from the Lt atrium & Lt
ventricle preventing backward flow.Semilunar Valves
Located where the blood leaves the heart, so it prevents blood from flowing back into the ventricles (from the aorta and the pulmonary arteries).
Pulmonary valve: (right semilunar valve) Between the R ventricle and the pulmonary artery
Aortic valve: (left semilunar valve) Between the L ventricle and the aorta
HEART SOUNDS Cardiac cycle = 1 complete heart beat This comes from the vibrations of the valves
as they close. Lubb-Dupp S1: Lubb: this is the closing of the tricuspid
valve and the mitral valve (loudest @ apex). S2: Dupp: this is the closing of the pulmonic
& aortic valves (loudest @ the base).
Blood Flow thru the Heart Rt heart: deoxygenated blood flows into the RA from
the superior / vena cava then thru the tricuspid valve into the RV thru the pulmonic valve to the pulmonary arteries. These carry it to the lungs where gas exchange takes place (CO2 for O2).
Lt heart: receives oxygenated blood from the lungs thru the pulmonary veins into the LA thru the bicuspid (mitral) valve to the LV then thru the aortic valve to the aorta to be carried thru the body.
Rt & Lt hearts are separated by the septa. Blood flows from a high pressure to a low
pressure Pressure is greater in the Lt heart. Blood in Lt heart=oxygenated Blood in Rt heart= unoxygenated Congenital heart defects often detour or
shunt blood so the normal circulatory path is disrupted.
A shunt is a passageway that diverts blood from a normal path
L to R shunt If a child is born with a hole in his
interventricular septum (ventricular septal defect VSD), it causes the L ventricle to pump blood into both the aorta and into the R ventricle—blood is being shunted from the left heart to the right heart.
The child would be acyanotic because the L ventricle is pumping oxygenated blood into the systemic circulation.
Rt to Lt Shunt The child presents with VSD and a stenotic
pulmonic valve--this increases the pressure within the R ventricle.
The elevated R ventricular pressure pumps blood into the L ventricle—blood is being shunted from the right heart to the left heart—the left ventricle now contains unoxygenated blood which it will pump into the systemic circulation—hence the client will present with cyanosis.
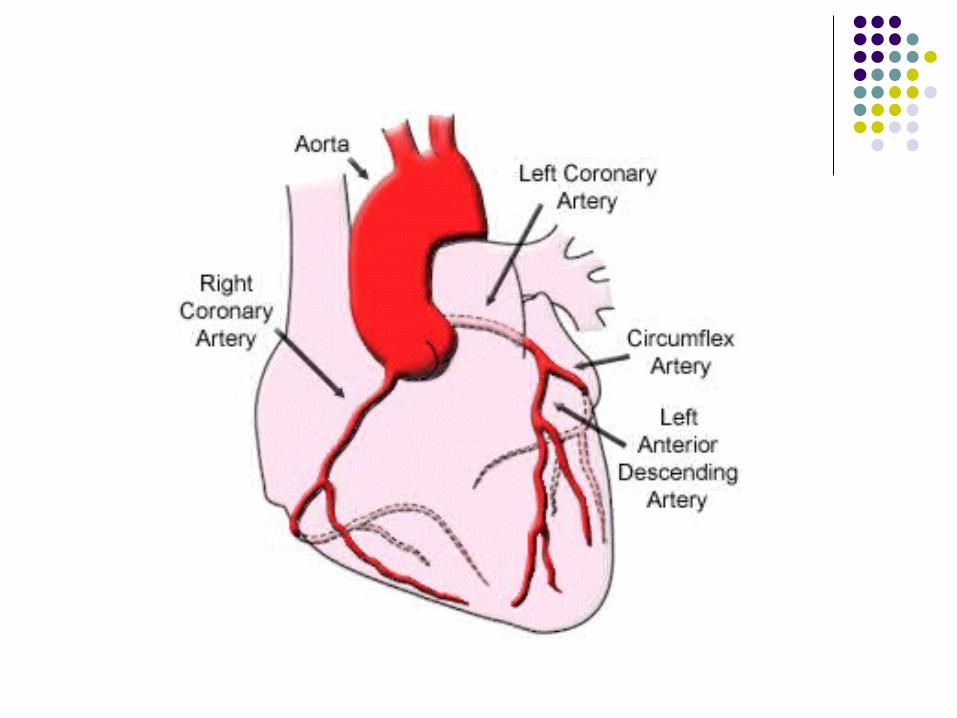
CARDIAC CIRCULATION The blood supply that nourishes the
myocardium comes from the coronary arteries.
The 2 main arteries are the L and R coronary arteries.
The RCA nourishes the right side of the heart, especially the ventricle.
The LCA branches into the Left Anterior Descending (LAD) artery and the Circumflex, they carry blood to the left side of the heart especially the ventricle.
The coronary veins collect the blood that nourishes the myocardium, it is then carried to the coronary sinus which empties the blood into the R atrium.
3 Important Characteristics of Coronary Blood Flow
1. Coronary blood flow can increase The heart must have a constant supply of
oxygenated blood, under resting conditions the heart muscle removes almost all of the O2 from the blood in the coronary arteries.
Thus if the heart need more O2, coronary blood flow must increase, this can happen with exertion (in the normal heart).
If the heart is not normal blood flow cannot increase during exertion and the myocardium is deprived of O2. This causes pain on exertion.
2. Coronary blood flow is greatest during myocardial relaxation.
Contraction of the myocardium squeezes the coronary vessels, cutting off the blood flow. When the muscle relaxes, the vessels open and restore blood flow.
When the relaxation phase is shortened (in a racing heart) coronary blood flow is decreased & the myocardial cells experience O2 deprivation—causing chest pain.
3) Coronary arteries have the capability of forming anastomoses between the arteries.
Collateral blood vessels develop in response to the diminished coronary blood flow that occurs with aging and chronic CAD. This is the reason that an older person may experience less myocardial damage from an MI than a younger person.
“Achy Breaky” Heart When blood flow diminishes, the myocardium
is deprived of O2 (ischemia)– chest pain (angina) occurs—this pain often radiates to the left shoulder, down the arm to the fingers—angina is often relieved by rest and the drugs such as nitroglycerin—this dilates the vessels and decreases the work of the heart.
Coronary artery occlusion worsens when a platelet-containing fatty plaque ruptures and completely blocks blood flow—the O2 deprived cells die causing a myocardial infarction (MI).
The adult male may present with N/V, diaphoresis and crushing chest pain
M=morphine O=oxygen A=aspirin N=nitroglycerin Use this as a way to remember emergency
treatment for an MI Elders and women present clinically different:
complaints are of fatigue, GI disturbances. Prognosis will depend on the severity and/or the
location of the infarct.
A word about enzymes…dead myocardial cells leak enzymes into the blood causing plasma elevations of cardiac enzymes: CPK (creatine phosphokinase) AST (aspartate aminotranserase), and LDH (lactic dehydrogenase), a regulator myocardial protein (troponin) also leaks out.
When there are plasma elevations of CPK, AST, LDH and troponin, it is an indication of an MI.
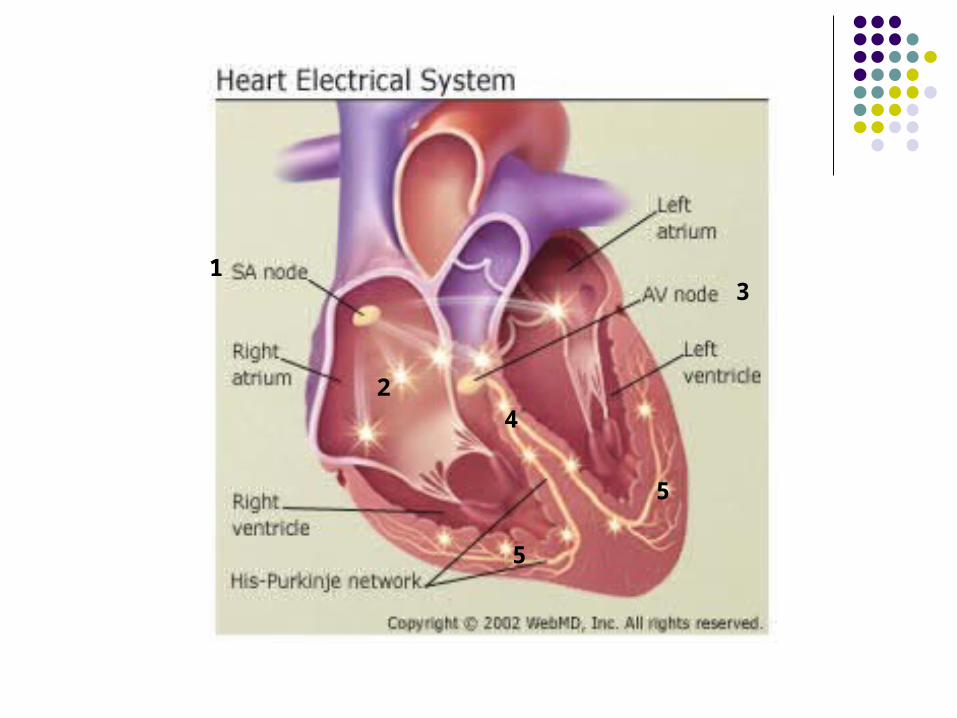
CONTROL OF HEART CONTRACTIONS The heart muscle contraction is controlled by a
group of cells located @ the opening of the superior vena cava into the RA.
SA node (sinoatrial) or the pacemaker SA node sends electrical impulses over the atria
causing them to contract (or depolarize). This causes the blood to flow downward from the
atrial chamber to the atrioventricular opening. Electrical impulses reach another group of
conducting cells: atrioventricular node (AV node). The impulses are carried to the conducting fibers in
the septum called the artioventricular bundle or the bundle of His.
This bundle divides into a fine network of branches (Perkinje network ) that spread thru the ventricles, the impulses travel to the Perkinje Fibers (***these are conduction fibers which conduct impulses thru the ventricle of the heart).
This causes the ventricles to contract (repolarize).
Cardiac cycle = 1 complete heart beat
1
2
3
4
5
5
EKG or ECG Used to record electrical activity of the heart
that causes contraction (systole) and the relaxation (diastole) of the atria and ventricles.
Systolic: heart @ work Diastolic: heart @ rest
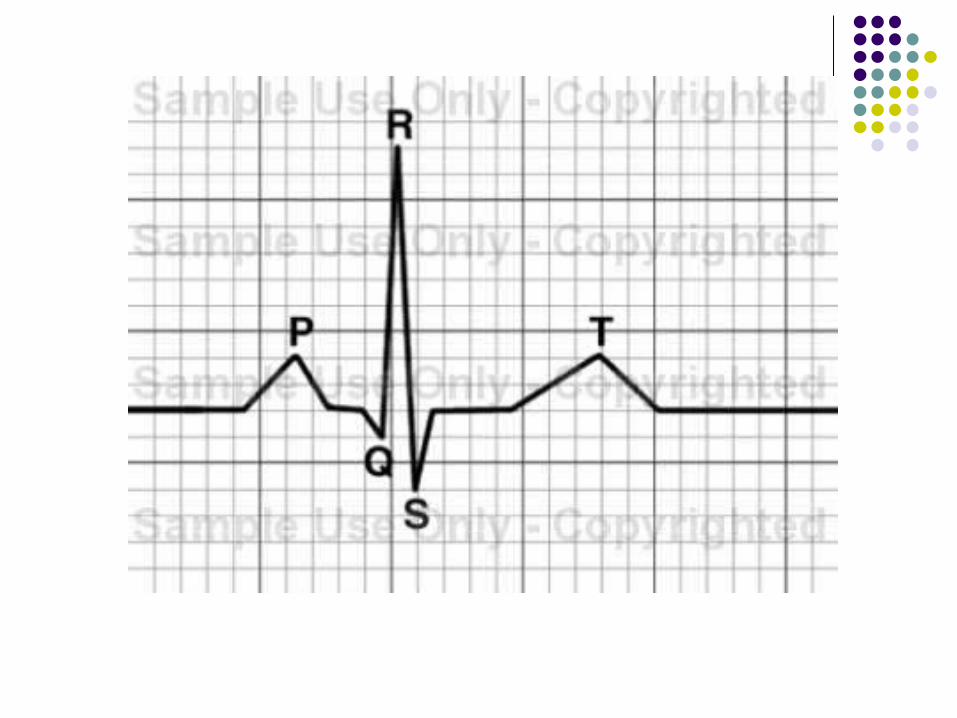
LINES or WAVES of EKG Baseline: is the isoelectric line--the flat line
separating different waves. Upward waves: positive deflections Downward waves: negative deflection
P wave: atrial depolarization (contraction)--systole QRS wave: ventricular depolarization (contraction)--
systole T wave: ventricular repolarization (relaxation)--
diastole NSR=normal sinus rhythm: the EKG appears normal
and the impulse originates in the SA node. The purpose of the EKG is to diagnose and analyze
the conduction system of the heart, to check the presence of dysrhythmia, check heart rate, and to check for an MI.