Embed Size (px)
Citation preview
DOI: 10.1111/j.1741-6612.2008.00308.x
134
Australasian Journal on Ageing, Vol 27 No 3 September 2008, 134 –142© 2008 The Authors
Journal compilation © 2008 ACOTA
Blackwell Publishing Asia
Research
Antipsychotic use in the elderly: What doctors say they do, and what they do
John Tiller
Albert Road Clinic, The University of Melbourne, Melbourne, Victoria, Australia
David Ames
National Ageing Research Institute, The University of Melbourne, Melbourne, Victoria, Australia
Henry Brodaty
Primary Dementia Collaborative Research Centre, School of Psychiatry, University of New South Wales, Sydney, New South Wales, Australia
Gerard Byrne
Royal Brisbane and Women’s Hospital, The University of Queensland, Brisbane, Queensland, Australia
Sudarshan Chawla
Fremantle Hospital, Fremantle, Western Australia, Australia
Graeme Halliday and John Snowdon
Rozelle Hospital, Sydney, New South Wales, Australia
Graham Hepworth
Statistical Consulting Centre, The University of Melbourne, Melbourne, Victoria, Australia
Peter McArdle
Albert Road Clinic, Melbourne, Victoria, Australia
Isaac Schweitzer
The Melbourne Clinic, The University of Melbourne, Melbourne, Victoria, Australia
Objective:
To review psychiatrists’ attitudes and actual practice on the use of typical and atypical antipsychotics in the elderly.
Methods:
Audit data were collected from 18-old-age psychiatry units across Australia. The attitudes of old age psychiatrists and their perceptions of the efficacy, tolerability and clinical usefulness of antipsychotics were examined.
Results:
The medications used for 321 patients were audited, and the attitudes of the 57 prescribing doctors were assessed. All available atypicals were prescribed and reported as more efficacious and clinically useful than typicals. Adverse events perceived by doctors as an obstacle to prescribing were more frequent than reported adverse event rates in product information. All diagnostic groups improved. Off-label use comprised almost 22% in this sample.
Conclusions:
Adverse events are impediments to prescribing, more so with typical than atypical antipsychotics. All available atypicals were used and appeared effective in this elderly population.
Key words:
adverse events, antipsychotic dosage, audit, therapy.
Introduction
The use of the typical antipsychotic medicines (typicals) in theelderly for psychosis and for behavioural disorders associatedwith dementia [1,2] has been questioned, with increasingawareness of their toxicity [3]. The typicals have increased riskof tardive dyskinesia (TD) and cardiovascular risks withwidening of the QTc interval, increasing the risk of potentiallyfatal arrhythmias [4].
Atypical antipsychotic agents (atypicals) provide therapeuticoptions with a lesser risk of extrapyramidal syndromes (EPS)[5,6], generally a lower cardiovascular risk, and fewer anti-muscarinic effects [7]. The atypicals have restricted approvedand subsidised indications [8].
The recent Clinical Antipsychotic Trials of InterventionEffectiveness (CATIE) seemed to challenge the benefits ofatypicals over typicals [9,10]. The study design, however, hadbiased allocation of patients with EPS to atypicals, whichobscured their value in causing less EPS [9]. The Alzheimer’sdisease study [10] concluded that adverse events offset advant-ages in the efficacy of these drugs.
TD is an organic brain disorder, potentially permanent andirreversible, related to age, duration of treatment with anti-psychotics, treatment with anticholinergics, the presence ofacute EPS and akathisia and substance abuse [11]. The risk forthe elderly is less with atypicals than typicals [12], with a loweranticholinergic burden and less risk of falls [13].
Antipsychotic agents may induce a syndrome of inappropriateantidiuretic hormone excretion (SIADH) [14], appetitestimulation and weight gain leading to the metabolic syndrome[15]. For some elderly patients an improvement in appetite andweight can be beneficial.
The risk of diabetes and stroke has been said to increase withatypicals [2,16], particularly stroke with olanzapine andrisperidone [17,18]. This is disputed. In a retrospective study,there was no difference in the risk of ischaemic stroke betweenatypicals or typicals [19]. There was no increased overall
Correspondence to: Professor John W.G. Tiller, Department of Psychiatry, The University of Melbourne, Albert Road Clinic. Email: [email protected]
aja(05)_308.fm Page 134 Saturday, July 26, 2008 9:22 AM

A n t i p s y c h o t i c s i n t h e e l d e r l y
Australasian Journal on Ageing, Vol 27 No 3 September 2008, 134 –142
135
© 2008 The AuthorsJournal compilation © 2008 ACOTA
risk of cerebrovascular events with atypical or conventionalantipsychotics in a case controlled study [20]. Herrmann et al.[21] showed that olanzapine and risperidone were not signifi-cantly associated with increased risk of stroke compared withtypical antipsychotic use.
Increased mortality has been reported with antipsychoticagents especially typicals [22]. The US Food and DrugAdministration (FDA) warned that treatment with atypicalantipsychotics may cause almost a twofold increase in the rateof death in this population [23]. The risk of death in the elderlytreated with typicals is comparable to or greater than the riskwith atypicals [24].
Treatment in the elderly has moved to the atypicals includingfor aggression and psychosis in dementia [25,26].
Atypicals are more costly than typicals despite the tendencyto use lower doses in the elderly [2,27]. The cost of atypicalscan be a particular problem for those on fixed incomes orpensions. Despite concerns about cost, the increased use ofatypicals has little impact on total health-care costs andoutcome [28].
Doctors’ attitudes may be more influential than scientificevidence in determining patterns of medication use [29]. Weevaluated old age psychiatrists’ attitudes to these agents andtheir reported use of these agents.
Methods
Sample selection
The principal investigator contacted a convenience sample ofold age psychiatrists in each State in Australia who all agreedto participate in this project. The study sites represented arange of health systems and the doctors were those actuallyengaged in treating the elderly. Patient files of all inpatientsbeing treated with antipsychotics by these doctors werereviewed, reducing the risk of a sampling bias if only somerecords had been selected.
Questionnaires
De-identified doctor and patient data were collected in aconsistent questionnaire format (Appendix 1). Doctorquestionnaires covered their demographics, reported pre-scribing use of each atypical antipsychotic (both oral anddepot), and a pooled response for typical antipsychotic use.Respondents were also asked for their view of the overall efficacyand clinical usefulness of each agent or class. Comments onnew medicines were sought only when the contributingdoctors reported having used them at least five times.
Patient audit questionnaires included data on age, gender,primary diagnosis for antipsychotic medicine use, dose, effective-ness of agents and adverse events. Efficacy was evaluated bydetermining the change in the Clinical Global Impression(CGI) scale from the clinical estimation of the severity of illness
when starting antipsychotics to the estimation of CGI severityat the time of questionnaire completion.
Data entry and analysis
Data entry and analysis were undertaken by the StatisticalConsulting Centre of the University of Melbourne as anindependent resource. Summary statistics were calculated foreach continuous variable, and table of frequencies and percent-ages for each categorical variable. Cross-tables of frequenciesbetween pairs of variables were constructed to examinerelationships of interest. For missing data, equal weight wasgiven to each questionnaire in calculations and analysis.Missing data were treated as if they were similar to the rest ofthe data from this sample, a standard approach for managingmissing data and reasonable here as in all areas there were nomajor differences between sites.
Results
Doctors and units
Questionnaires were returned from 57 medical practitioners(mean age 46 years, 75% men), from 18 units (Appendix 2).Ninety four per cent identified themselves as old age psychia-trists, 6% psychiatry trainees, 79% had old age psychiatrytraining in Australia and 21% trained overseas, predominantlyin the UK. Fifty-two per cent were members of the Faculty ofOld Age Psychiatry of the Royal Australian and New ZealandCollege of Psychiatry and an additional 10% reported member-ships of other gerontology or old age psychiatry organisations.Forty-one per cent of all doctors spent
>
50% of their pro-fessional time in old age psychiatry. Of those participating inthis study, 59% had spent up to 9 years in old age psychiatry,17% 10–19 years, 17% 20–29 years and 7% 30 years and more.
Patients
The 321 current inpatients evaluated had a mean age of 76years (standard deviation (SD)
=
7.6), and 51% were women;166 had a dementia diagnosis, 23 had other psychiatric diag-noses, including depression in 15% of all patients.
In addition to psychiatric disorder(s), all patients had at leastone medical diagnosis, most commonly cardiovascular disease(29%). Almost all patients (316 of 321) were taking medicationsfor other illnesses.
Patients were continuing antipsychotics or had changed anti-psychotics because of lack of efficacy of previous treatment(
n
=
98; 31%) or prior adverse events (
n
=
37; 12%). Of theadverse events, EPS was the most frequent (
n
=
17; 5.3%). Inthis sample (
n
=
321), 78 (24%) were taking typicals (of whomfour were on depots) and 243 (76%) were taking atypicals (ofwhom two were on depots).
The doctors utilised the range of available antipsychotics.Reported responses were unchanged or worse in 23%, andmildly improved or better in 77%, with 35% of all patientsmoderately improved or better. There were few reported drug
aja(05)_308.fm Page 135 Saturday, July 26, 2008 9:22 AM
136
Australasian Journal on Ageing, Vol 27 No 3 September 2008, 134 –142© 2008 The Authors
Journal compilation © 2008 ACOTA
T i l l e r J , A m e s D , B r o d a t y H
e t a l .
interactions (3%) despite the number of medicines thesepatients were taking (see below).
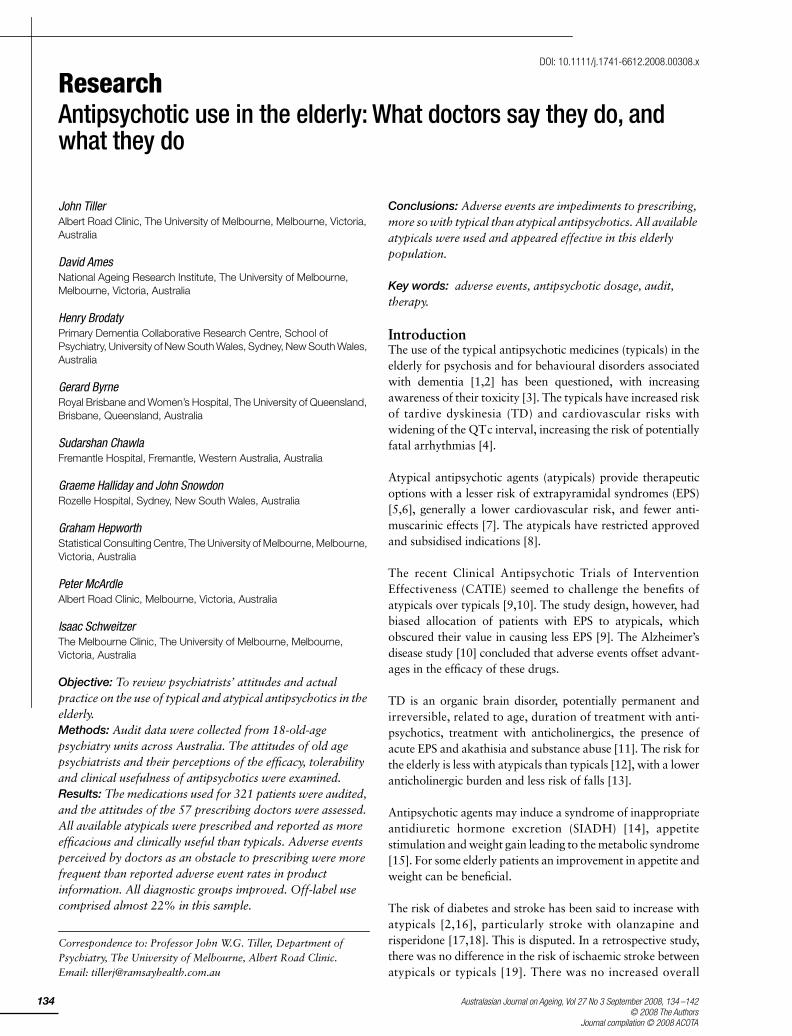
Figure 1 indicates that these patients generally improved withtreatment. We reviewed the proportion of patients with eachdiagnosis who changed in severity from moderately ill or moreso to mildly ill or less following treatment (some patients hadmore than one diagnosis). The proportion changing frommoderately ill or more to mildly ill or less was for: schizophreniapatients (101 patients; 33% responded), behavioural distur-bance with dementia (118; 18%), unipolar depression withpsychosis (40; 27%), unipolar depression without psychosis(20; 50%), bipolar disorder (30; 46%), behavioural disturbancewithout dementia (12; 42%) and other psychiatric diagnoses(42; 49%).
Medicines
Doctors reported what they believed were their most fre-quently prescribed medicines, doses, adverse events, efficacyand usefulness.
Typical antipsychotics
When this study was undertaken (2004–2005), doctors inapproximately 50% of units had to use typical agents first in
this population, with hospital cost containment the reportedreason in 96.5% of cases. This restriction no longer applies.The next influence on choice of medication was medicalsubsidy restriction (9.1%). When old age psychiatrists werefree to choose any antipsychotic agent, they generally chosean atypical.
The most commonly reported typical oral medicine chosenwas haloperidol (69% of doctors), the reported usual doserange was 1–6 mg/day with a mean target dose of 3 mg/day,followed by chlorpromazine (15% of doctors) with dose rangeof 20–400 mg/day and a target dose of approximately 150 mg;and pericyazine (10% of doctors) with dose range of 2.5–12.5 mg/day and a target dose of 5 mg/day.
Flupenthixol (32% of doctors in a range of 10–40 mg and atarget dose of 20 mg weekly) and zuclopenthixol (32% ofdoctors, range of 50–150 mg and a target dose of approximately100 mg weekly) were the most commonly reported typicaldepot medications. Haloperidol decanoate was less used(12% of doctors, dose range of 25–50 mg and a target doseof 20 mg weekly), as was fluphenazine decanoate (9% of doctors,dose range of approximately 10–25 mg and a target dose of15 mg weekly).
Over 96% of doctors reported that adverse events were obstaclesto prescribing. The most common concerns with typicalsrelated to acute EPS (86%), TD (80%), sedation (35%), hyper-prolactinaemia (18%) and weight gain (18%); with 20%reporting a variety of other adverse events as prescribingobstacles. There were no differences between oral and depotmedications regarding concerns over weight gain, but concernover sedation was more common with depots (47%) thanwith oral medication (35%). Doctors’ reported adverse eventsbeing obstacles to prescribing more frequently than reportedrates of adverse events listed in product information (PI)(Table 1).
These medicines were moderately effective or better reportedby 98% of doctors and 77% reported them clinically useful.
Figure 1: Reported severity of patients’ illness before and after treatment with the most recent antipsychotic medicine.
Table 1: Doctors’ (n ==== 57) frequency (%) of reports of selected adverse events sufficient to be an obstacle to prescribing and adverse event rates (%) as listed in product information (PI) for typical antipsychotics
Adverse event Typical oral Typical depot
Frequency of report (all orals)
PI adverse event rates (haloperidol)
Frequency of report
(all depots)
PI adverse event rates
(haloperidol depot)§
Acute EPS 86 ≥ 1 to < 10 89 ¶TD 80 † 77 ††Hyperprolactinaemia 18 ‡ 11 ‡Sedation 35 ‡ 47 ‡Weight gain 18 ‡ 19 ‡‡
†Reported as ‘uncommon’ (frequency ≥ 0.1% to < 1%).‡Reported but frequency not stated.§For both haloperidol and haloperidol decanoate.¶Reported as ‘occur frequently’.††Reported as ‘may appear in some patients’ on long-term therapy, or may appear after drug therapy has been discontinued.‡‡Reported as ‘weight changes may occur’.EPS, extrapyramidal syndromes; TD, tardive dyskinesia.
aja(05)_308.fm Page 136 Saturday, July 26, 2008 9:22 AM
A n t i p s y c h o t i c s i n t h e e l d e r l y
Australasian Journal on Ageing, Vol 27 No 3 September 2008, 134 –142
137
© 2008 The AuthorsJournal compilation © 2008 ACOTA
Atypical antipsychotics
The common obstacles to accessing atypical antipsychoticsand ascribed reasons are in Table 2.
Doctors reported prescribing the following at least five times ayear: amisulpride (by 67% of doctors), aripiprazole (53%),clozapine (64%), olanzapine (98%), quetiapine (93%) andrisperidone (98%). One in three doctors reported havingprescribed risperidone depot.
The approved indication for these medications was schizo-phrenia, and for risperidone in addition, behavioural disorderwith dementia. In practice, these agents were used for 101patients with schizophrenia, 118 patients for behaviouraldisturbance with dementia, 40 patients for unipolar depressionwith psychosis, 20 patients for unipolar depression withoutpsychosis, 30 patients for bipolar disorder and 12 for behavi-oural disturbance without dementia.
Though most patients (287) received a single antipsychotic, 34patients received two antipsychotics, and two patients receivedthree antipsychotics.
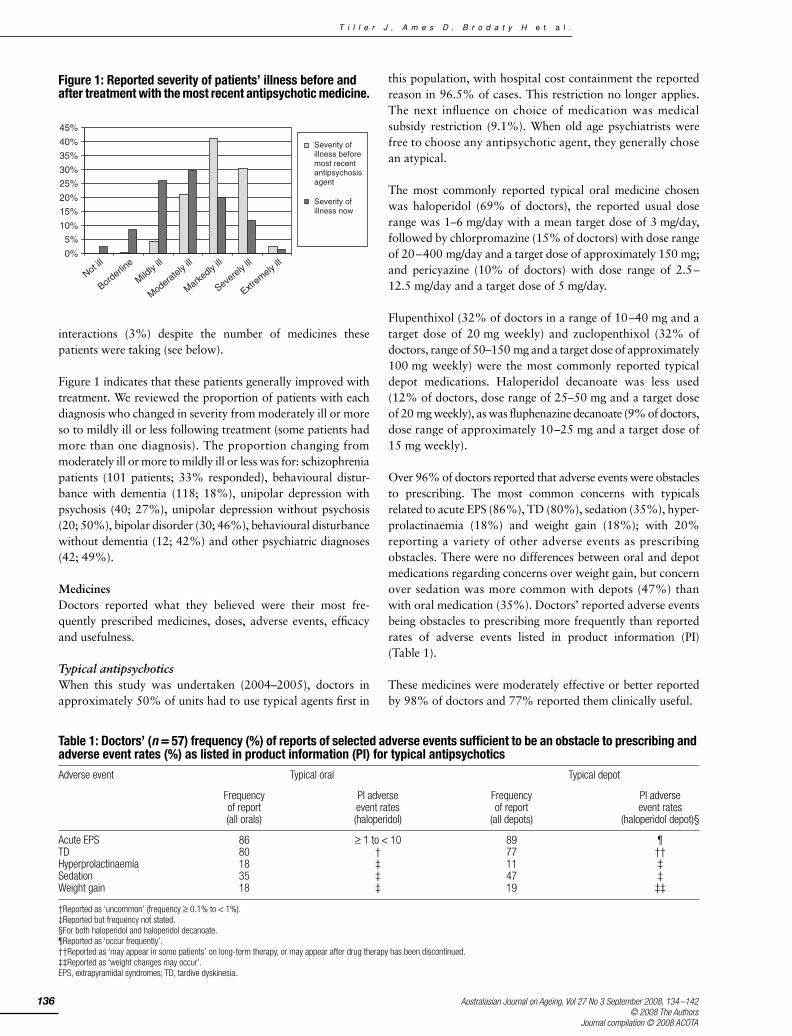
The reported usefulness of atypicals is shown in Figure 2, anddoses of atypicals recommended by participating doctors andthe range recommended in PI in Table 3.
Doctors reported adverse events as an obstacle to prescribingless frequently with atypicals than typicals (Tables 1 and 4).The impact of adverse events as obstacles to prescribing wasmuch greater for specific compounds and particular adverseevents than reported PI rates would suggest (Table 4).
Medicines where doctors had concerns over weight gain wereolanzapine (91%), clozapine (60%), oral risperidone (32%) andquetiapine (25%); overall, 32.5% of doctors reported weight gainas an obstacle to prescribe. Drugs with less weight impedimentscompared with typicals were amisulpride (7%), risperidonedepot (6%) and aripiprazole (6%). Sedation was an obstaclefor 70% of doctors for quetiapine, 69% for clozapine, 61% forolanzapine and 47% for oral risperidone, but less for depotrisperidone (13%), amisulpride (13%) and aripiprazole (2%).
Hyperprolactinaemia was a problem for 22% of doctors whenprescribing amisulpride, 38% with oral risperidone and 26%
Table 2: Percentage of doctors (n ==== 57) reporting particular obstacles in prescribing specific atypical antipsychotic medicines
Drug Frequency of perceived obstruction to prescribing (%)
PBS restrictions Unlisted in PBS Cost to patient Cost to hospital Dosing problem
Amisulpride 79.6 5.6 33.3 16.7 16.7Aripiprazole 76.0 12.0 34.0 20.0 8.0Clozapine 51.9 3.8 13.5 11.5 7.7Olanzapine 85.7 7.1 48.2 23.2 1.8Quetiapine 81.1 9.4 41.5 20.8 22.6Risperidone 81.1 7.5 39.6 17.0 1.9Risperidone depot 31.9 34.0 44.7 46.8 17.0
PBS, pharmaceutical benefits scheme.
Figure 2: Reported overall usefulness of atypical antipsychotic medicines.
aja(05)_308.fm Page 137 Saturday, July 26, 2008 9:22 AM
138
Australasian Journal on Ageing, Vol 27 No 3 September 2008, 134 –142© 2008 The Authors
Journal compilation © 2008 ACOTA
T i l l e r J , A m e s D , B r o d a t y H
e t a l .
with depot risperidone, but less with aripiprazole (12% ofdoctors), olanzapine (9%), quetiapine (8%) and clozapine (0%).
The mean percentage of doctors reporting impediments toprescribing from EPS when using atypicals was 27, and withTD was 10.
The reported usefulness of the atypical antipsychotics is shownin Figure 2. Efficacy and usefulness were generally similarfor all agents, except clozapine, which was reported to beextremely effective for 12.3% of patients, more than any otheragent. Among those who were borderline or mildly ill (
n
=
15),the proportion of times these medicines were rated asmoderately useful or more was 50%, for those moderately andmarkedly ill (
n
=
191) it was 63%, and for those as severely orextremely ill (
n
=
52) it was 51%.
Concomitant medications
Patients were taking many medications (mean 5.43, SD
=
3.13,range 0–16) with only five patients on no concomitantmedications. There were no reported adverse drug inter-actions. The 212 concomitantly prescribed non-antipsychoticmedicines covered a wide range of therapeutic classes.Concomitant medicines prescribed for disorders in othertherapeutic areas were for the central nervous system (otherthan antipsychotics) (511), cardiovascular (269), alimentarytract (219), analgesics (185), nutritional supplements andvitamins (161), endocrinological (158), ophthalmological (109),respiratory (29), immunological (18), musculoskeletal (17),genitourinary (10) and for neoplastic disorders (7). Manypatients were on multiple medications, even of the same classso that the number of medicines exceeded the number ofpatients being treated.
Table 3: Doses of atypical antipsychotic medicines (lowest and highest effective dose, and the reported usual target dose) recommended by participating doctors (n ==== 57), and dose range reported in the product information (PI)
Drug Lowest effective dose (mg/day)
Highest effective dose (mg/day)†
Usual target dose (mg/day)
Dose range in PI‡
Amisulpride 100 500 300 50–1200§Aripiprazole 9 25 15 10–30§Clozapine 100 400 250 12.5–900§Olanzapine 2.5 20 10 5–20§Quetiapine 50 500 300 50–800§Risperidone 1 4 3 1–6§Risperidone depot 12.5 25 15 25–50¶
†The highest effective dose is the dose beyond which they would expect no significant additional benefit or the occurrence of disabling adverse events. Numbers have been rounded to the nearest prescribing unit or proportion of that.‡Product information, eMIMS, 2007.§Daily dose average.¶Dose per 2 weeks.
Table 4: Doctors’ (n ==== 57) frequency of reports (%) of selected adverse events sufficient to be an obstacle to prescribing, and adverse event rates (%) as listed in product information (PI) for atypical antipsychotics
Adverse event Amisulpride Aripiprazole Clozapine Olanzapine Quetiapine Risperidone Risperidone depot
Frequency of report
PI Frequency of report
PI Frequency of report
PIa Frequency of report
PIa Frequency of report
PI Frequency of report
PIa Frequency of report
PI
Acute EPS 28 11b 20 13 6 ≥ 1 to < 10
13 ≥ 1 to < 10c
6 d 79 > 10 38 2.9–3.8
TD 2 e 6 f 2 < 0.01 5 c 6 g 23 h 26 iHyperprolactinaemia 22 j 2 k 0 – 9 – 8 – 38 – 26 < 1Sedation 13 3 2 5 69 40 61 ≥ 10 70 ≥ 10 47 l 13 > 1, < 5m
Weight gain 7 6 6 – 60 > 1 to < 10
91 ≥ 10 25 ≥ 1 to < 10
32 m 6 > 1, < 5m
aSome compounds have frequency of adverse events reported as: very common ≥ 10%, common ≥ 1 to < 10%, uncommon ≥ 0.1% to < 1%,rare 0.01–0.1%, very rare < 0.01%.bTardive dyskinesia listed as ‘rarely reported’ ≥ 0.01% to < 0.1%.cLower incidence of parkinsonism, akathisia, dyskinesia and dystonia compared with titrated doses of haloperidol.dReported as ‘no differences between the Seroquel and the placebo treatment groups’.eThere was no separate report of tardive dyskinesia from other EPS.fReported as ‘uncommon’ ≥ 0.1% to < 1%.gVery rare postmarketing cases.hMentioned, but no rate given.iOccasionally.jNo report of hyperprolactinaemia, but 3% report of galactorrhoea.kNo reference but report of breast discharge uncommon (≥ 0.1% to < 1%).lReported as ‘mild and transient’.mThis compound has these adverse events reported as > 1%, < 5%.nReported as ‘less common’.EPS, extrapyramidal syndromes.
aja(05)_308.fm Page 138 Saturday, July 26, 2008 9:22 AM

A n t i p s y c h o t i c s i n t h e e l d e r l y
Australasian Journal on Ageing, Vol 27 No 3 September 2008, 134 –142
139
© 2008 The AuthorsJournal compilation © 2008 ACOTA
The most commonly prescribed concomitant medications wereartificial tears (94), paracetamol (81), oxazepam (80), coloxyl(75), temazepam (70), aspirin (68), sodium valproate (48),lactulose (42), frusemide (41), lithium carbonate (38), omepra-zole (36), perindopril (35), venlafaxine (33) and calcium (30).
Discussion
These results, we believe, represent attitudes of psychiatrists inold age psychiatry units in Australia, in terms of antipsychoticmedicines used and doctors’ attitudes. This is particularly sogiven the broad similarity of data from each unit, even thoughthis was from a convenience sample and not from a randomsample of such units. We were surprised at the degree ofsimilarity between these widely dispersed units acrossAustralia. This may reflect the impact on prescribing practicesand attitudes from common elements in old age psychiatrists’training and continuing education.
The increased cost of atypical antipsychotic medicines overtypicals costs to hospitals materially affected prescribing forsome in that setting, despite the attendant potential toxicity oftypical antipsychotics, for example, high reported EPS and TDrates [9,10]. Since data collection, doctors now report beingable to prescribe any antipsychotic.
The use of lower doses in the elderly is consistent with otherreports [2,16]. Lower doses can have better tolerability andfewer adverse events, but efficacy may be less. Doctors may usemore than one agent rather than increase the primary anti-psychotic to an effective dose. Guidelines generally suggest oneantipsychotic medicine at a time, rather than combinations.Yet, more than 10% of these patients were prescribed two ormore antipsychotics and
<
1% had three. There shouldbe compelling medical reasons for the use of multiple anti-psychotics. One such reason is when transitioning from oneantipsychotic to another, when dosing may overlap.
Doctors’ perception of efficacy for typical agents of 98% wassimilar to atypicals and data are similar to the CATIE study[30]. In contrast, the evaluation of the clinical usefulness oftypicals (75%) was exceeded by that of atypicals (average 88%).These patients were in specialty units implying non-response toprevious treatment, or requiring additional resources. Thatmore than three-fourths of patients were mildly improved orbetter, and more than one-third moderately improved or betterwith one treatment, are positive outcomes.
The obligatory first use of typicals meant that they were morelikely to show efficacy than second choices which could reflecttreatment resistance or intolerance of medicines. All atypicalsappeared reasonably effective and useful (Fig. 2).
For most diagnoses, about one-third to half of patients movedfrom moderately or more ill to mildly ill or less, a clinically use-ful change. Though the proportion showing this degree ofchange was lower in those with behavioural disturbance withdementia than for other diagnoses, there was clearly benefit, as
almost 40% moved from markedly or more ill to moderatelyill or less. This could imply greater effectiveness for the moreseverely ill with this diagnosis than is apparent when lookingat overall improvement.
Doctors’ preference for atypicals suggests that notwithstand-ing their adverse events, they are more clinically useful thantypicals, which appears to be the most important benefit ofatypicals [5]. Doctors’ perceptions of EPS and TD were lowerwith atypicals than with typicals. With the typical agents, theaversion to prescribe because of adverse events was muchgreater than the low adverse event rates in the PIs wouldsuggest. The ability to avoid antimuscarinic agents for acuteEPS, with atypicals, reduces potential adverse effects on cognitionand on the heart (from increasing cardiac rate).
The proportion of old age psychiatrists who regarded specificadverse events as impediments to prescribe was higher than thefrequency of reported adverse events in the PIs, for both thetypical and the atypical agents. Old typical antipsychoticsstudies often express adverse events in general terms ratherthan specific percentages.
The results also highlight the fact that it is not just the frequencyof an adverse event that matters, but the nature of the event,and the clinical relevance of the event for the patient.
Adverse event rates may be higher and could have greaterimpact in the elderly who mostly have comorbidity as in thissample, than in younger populations with no comorbidity,who are usually recruited for registration studies. It is thereforeimportant to conduct studies in the elderly to obtain datarelevant to that population.
Without practice constraints, old age psychiatrists in our studysample chose to use atypical agents when an antipsychotic wasneeded. Though we cannot assume that the practices of thesedoctors will be exactly the same as those of all other old agepsychiatrists, we believe that this sample of convenience in‘real-life’ general elderly residential settings is consistent acrossAustralia and reflects current attitudes and practices.
Conclusions
The atypical antipsychotics were seen by doctors as treatmentsof choice over typicals, and as being both efficacious and clinic-ally useful with older patients. In the elderly, antipsychotics areused for disorders other than schizophrenia and behaviouraldisorder with dementia. The adverse event burden with typicalagents, especially EPS and TD, is substantial and may be higherin the elderly than in younger patients. There were no reportedadverse interactions with a wide range of concomitantmedication. Adverse events with antipsychotics were reportedas an impediment to prescribe more often than frequencieslisted in the PI, despite older patients generally having lowerantipsychotic doses. Despite these concerns, old age psychia-trists use the full repertoire of antipsychotics for a range ofmental illness (including off-label indications) in the elderly.
aja(05)_308.fm Page 139 Saturday, July 26, 2008 9:22 AM

140
Australasian Journal on Ageing, Vol 27 No 3 September 2008, 134 –142© 2008 The Authors
Journal compilation © 2008 ACOTA
T i l l e r J , A m e s D , B r o d a t y H
e t a l .
Acknowledgements
The authors wish to acknowledge Dr Paul Bennett and MsNatalia Lukaszewicz of AstraZeneca for their assistance inthis project which was supported by an unrestricted grantfrom AstraZeneca Neuroscience, Australia. Dr Karen Bermancollected data at the University of New South Wales site.
Key Points
• Atypical antipsychotics were seen as more efficaci-ous and clinically useful than typical antipsychotics.
• Doctors’ perceptions of the impact of adverse eventsas impediments to prescribe were greater thanexpected from the rates reported for the same eventsin product information.
• Doses of antipsychotics were lower in this olderpopulation than reported with younger patients;with the elderly reported as more vulnerable toadverse events.
• Doctors used the range of atypical agents, reflectingthat no one agent is suitable for all patients,while
>
20% of use was for off-label indications.
References
1 Small GW. Psychopharmacological treatment of elderly dementedpatients.
Journal of Clinical Psychiatry
1988; 49(Suppl. 5): 8–13.2 Folsom DP, Nayak GV, Jeste DV. Antipsychotic medications and the
elderly.
Primary Psychiatry
2004; 11: 47–50.3 Raskin DE. Antipsychotic medication and the elderly.
Journal of ClinicalPsychiatry
1985; 46(5, sect 2): 36–40.4 Percudani M, Barbui C, Fortino I, Petrovich L. Antipsychotic drug prescribing
in the elderly is cause for concern.
International Clinical Psychopharma-cology
2004; 19: 347–350.5 Kane JM. Tardive dyskinesia rates with atypical antipsychotics in adults:
Prevalence and incidence.
Journal of Clinical Psychiatry
2004; 65(Suppl. 9):16–20.
6 Stahl SM.
Psychopharmacology of Antipsychotics
. London: Martin DunitzLtd, 1999.
7 Woodward ND, Purdon SE, Meltzer HY, Zald DH. A meta-analysis ofneuropsychological change to clozapine, olanzapine, quetiapine, andrisperidone in schizophrenia.
International Journal of Neuropsychophar-macology
2005; 8: 457–472.8 Australian Government.
Schedule of Pharmaceutical Benefits forApproved Pharmacists and Medical Practitioners
. Barton, ACT: Common-wealth of Australia, 2006.
9 Lieberman JA, Stroup TS, McEvoy JP et al. Effectiveness of antipsychoticdrugs in patients with chronic schizophrenia.
New England Journal ofMedicine
2005; 353: 1209–1223.
10 Schneider LS, Tariot PN, Dagerman KS et al. Effectiveness of atypicalantipsychotic drugs in patients with Alzheimer’s disease.
New EnglandJournal of Medicine
2006; 355: 1525–1538.11 Miller DD, McEvoy JP, Davis SM et al. Clinical correlates of tardive
dyskinesia in schizophrenia: Baseline data from the CATIE schizophreniatrial.
Schizophrenia Research
2005; 80: 33–43.12 Sciolla A, Jeste DV. Use of antipsychotics in the elderly.
InternationalJournal of Psychiatry in Clinical Practice
1998; 2: S27–S34.13 Aizenberg D, Sigler M, Weizman A, Barak Y. Anticholinergic burden and
the risk of falls among elderly psychiatric inpatients: A 4-year case-control study.
International Journal of Psychogeriatrics
2002; 14(3):307–310.
14 Collins A, Anderson J. SIADH induced by two atypical antipsychotics.
International Journal of Geriatric Psychiatry
2000; 15: 282–285.15 McEvoy JP, Meyer JM, Goff DC et al. Prevalence of the metabolic syn-
drome in patients with schizophrenia: Baseline results from the clinicalantipsychotic trials of intervention effectiveness (CATIE) schizophrenia trialand comparison with national estimates from NHANES III.
SchizophreniaResearch
2005; 80: 19–32.16 Daniel DG. Antipsychotic treatment of psychosis and agitation in the
elderly.
Journal of Clinical Psychiatry
2000; 61(Suppl. 14): 49–52.17 van Iersel MB, Zuidema SU, Koopmans RTCM, Verhey FRJ, Olde Rikkert
MGM. Antipsychotics for behavioural and psychological problems inelderly people with dementia.
Drugs and Aging
2005; 22: 845–858.18 Brodaty H, Ames D, Snowdon J et al. A randomized placebo-controlled
trial of risperidone for the treatment of aggression, agitation, and psychosisof dementia.
Journal of Clinical Psychiatry
2003; 64: 134–143.19 Gill SS, Rochon PA, Herrmann N et al. Atypical antipsychotic drugs and
risk of ischaemic stroke: Population based retrospective cohort study.
British Medical Journal
2005; 330: 1–6.20 Liperoti R, Gambassi G, Lapane KL et al. Cerebrovascular events among
elderly nursing home patients treated with conventional or atypical anti-psychotics.
Journal of Clinical Psychiatry
2005; 66: 1090–1096.21 Herrmann N, Mamdani M, Lanctot KL. Atypical antipsychotics and risk of
cerebrovascular accidents.
American Journal of Psychiatry
2004; 161:1113–1115.
22 Hollis J, Forrester L, Brodaty H, Touyz S, Cumming RG, Grayson D. Riskof death associated with antipsychotic drug dispensing in residentialaged care facilities.
Australian and New Zealand Journal of Psychiatry
2007; 41: 751–758.23 Kuehn BM. FDA warns antipsychotic drugs may be risky for elderly.
JAMA
2005; 293: 2462.24 Schneeweiss S, Setoguchi S, Brookhart A, Dormuth C, Wang PS. Risk of
death associated with the use of conventional versus atypical antipsychoticdrugs among elderly patients.
Canadian Medical Association Journal
2007; 176: 627–632.25 Beck S, Paton C, Euba R, Goddard C. Atypical antipsychotics in the elderly.
International Journal of Psychiatry in Clinical Practice
2001; 5: 257–261.
26 Comaty JE, Advokat C. Indications for the use of atypical antipsychoticsin the elderly.
Journal of Clinical Geropsychology
2001; 7: 285–309.27 Rapoport M, Mamdani M, Shulman KI, Herrman N, Rochon PA. Antipsychotic
use in the elderly: Shifting trends and increasing costs.
InternationalJournal of Geriatric Psychiatry
2005; 20: 749–753.28 Percudani M, Barbui C. Cost outcome implications of using typical and
atypical antipsychotics in ordinary practice in Italy.
Journal of ClinicalPsychiatry
2003; 64: 1293–1299.29 Institute of Medicine
Crossing the Quality Chasm: A New Health Systemfor the 21st Century
. Washington, DC: National Academy Press, 2001.30 Lieberman JA, Stroup TS, Davis SM, the CATIE Investigator Group.
Antipsychotic drugs and schizophrenia.
New England Journal of Medicine
2006; 354: 300.
aja(05)_308.fm Page 140 Saturday, July 26, 2008 9:22 AM
A n t i p s y c h o t i c s i n t h e e l d e r l y
Australasian Journal on Ageing, Vol 27 No 3 September 2008, 134 –142
141© 2008 The AuthorsJournal compilation © 2008 ACOTA
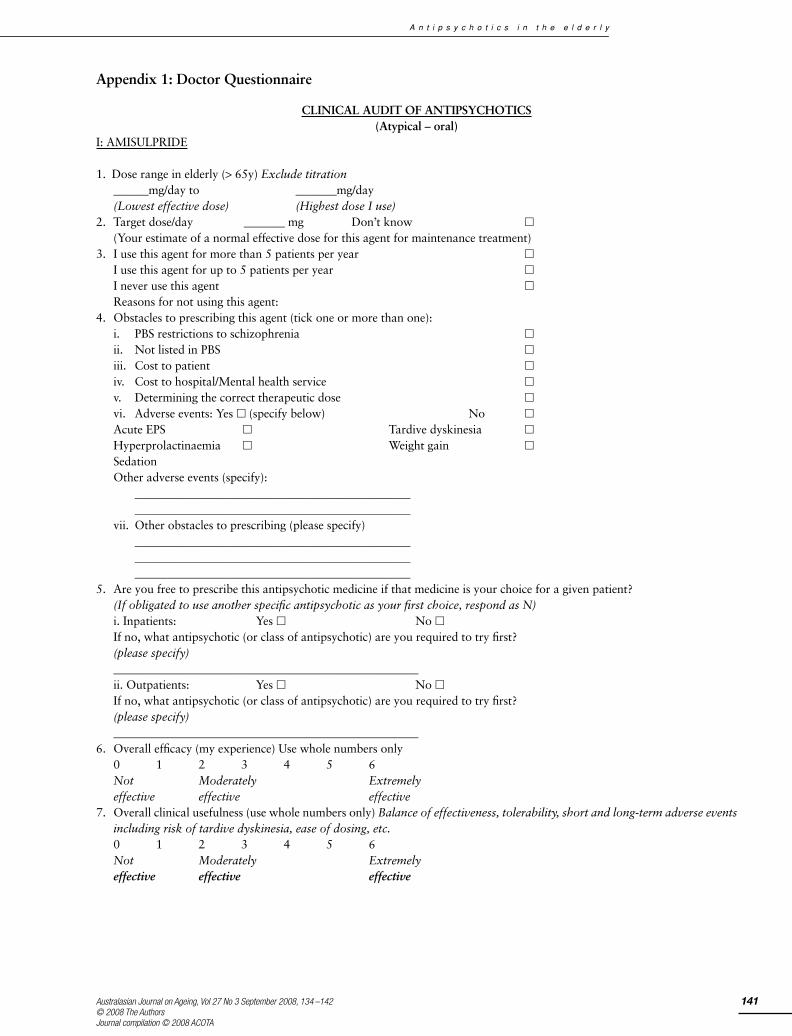
Appendix 1: Doctor Questionnaire
CLINICAL AUDIT OF ANTIPSYCHOTICS(Atypical – oral)
I: AMISULPRIDE
1. Dose range in elderly (> 65y) Exclude titration______mg/day to _______mg/day(Lowest effective dose) (Highest dose I use)
2. Target dose/day _______ mg Don’t know �
(Your estimate of a normal effective dose for this agent for maintenance treatment)3. I use this agent for more than 5 patients per year �
I use this agent for up to 5 patients per year �
I never use this agent �
Reasons for not using this agent:4. Obstacles to prescribing this agent (tick one or more than one):
i. PBS restrictions to schizophrenia �
ii. Not listed in PBS �
iii. Cost to patient �
iv. Cost to hospital/Mental health service �
v. Determining the correct therapeutic dose �
vi. Adverse events: Yes � (specify below) No �
Acute EPS � Tardive dyskinesia �
Hyperprolactinaemia � Weight gain �
SedationOther adverse events (specify):
______________________________________________________________________________________________
vii. Other obstacles to prescribing (please specify)_____________________________________________________________________________________________________________________________________________
5. Are you free to prescribe this antipsychotic medicine if that medicine is your choice for a given patient?(If obligated to use another specific antipsychotic as your first choice, respond as N)i. Inpatients: Yes � No �If no, what antipsychotic (or class of antipsychotic) are you required to try first?(please specify)____________________________________________________ii. Outpatients: Yes � No �If no, what antipsychotic (or class of antipsychotic) are you required to try first?(please specify)____________________________________________________
6. Overall efficacy (my experience) Use whole numbers only0 1 2 3 4 5 6Not Moderately Extremelyeffective effective effective
7. Overall clinical usefulness (use whole numbers only) Balance of effectiveness, tolerability, short and long-term adverse eventsincluding risk of tardive dyskinesia, ease of dosing, etc.0 1 2 3 4 5 6Not Moderately Extremelyeffective effective effective
aja(05)_308.fm Page 141 Saturday, July 26, 2008 9:22 AM
142 Australasian Journal on Ageing, Vol 27 No 3 September 2008, 134 –142© 2008 The Authors
Journal compilation © 2008 ACOTA
T i l l e r J , A m e s D , B r o d a t y H e t a l .
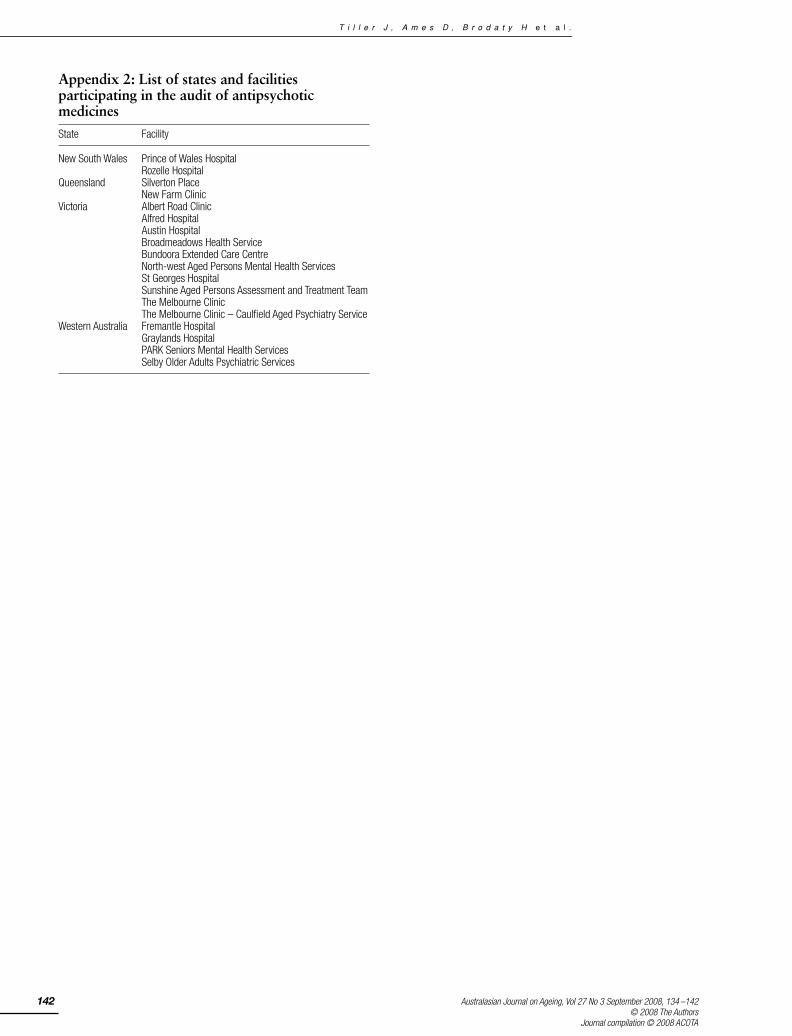
Appendix 2: List of states and facilities participating in the audit of antipsychotic medicinesState Facility
New South Wales Prince of Wales HospitalRozelle Hospital
Queensland Silverton PlaceNew Farm Clinic
Victoria Albert Road ClinicAlfred HospitalAustin HospitalBroadmeadows Health ServiceBundoora Extended Care CentreNorth-west Aged Persons Mental Health ServicesSt Georges HospitalSunshine Aged Persons Assessment and Treatment TeamThe Melbourne ClinicThe Melbourne Clinic – Caulfield Aged Psychiatry Service
Western Australia Fremantle HospitalGraylands HospitalPARK Seniors Mental Health ServicesSelby Older Adults Psychiatric Services
aja(05)_308.fm Page 142 Saturday, July 26, 2008 9:22 AM