Embed Size (px)
Citation preview

Antiplatelet Therapy: Stents, Strokes, MIs, and Prevention - 1, 2 or 3 Drugs - What is a
Clinician to do?
Marc P. Bonaca, MD, MPHVascular Section, Cardiovascular Division
Investigator TIMI Study GroupBrigham and Women’s Hospital
Assistant Professor, Harvard Medical School
ASPC 2016 Congress on Atherosclerotic Cardiovascular Disease Prevention

0
4
8
12
16
20
24
CADOnly
CVDOnly
PADOnly
>1 Bed
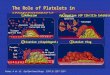
CV Death, MI, Strokeor Hosp for Atherothrombosis
54% 20% 6% 20%
Steg et al. JAMA 2007; 297:1197-1206.
5.31
14.4
0
4
8
12
16
20
24
Multiple RiskFactors
EstablishedDisease
CV Death, MI, Strokeor Hosp for Atherothrombosis
%
Outcomes in Patients with Atherosclerotic Disease
REACH Registry (1 Year Outcomes) 64,977 pts ≥ 45 YO

Marc P. Bonaca, and Mark A. Creager Circulation Research. 2015;116:1579-1598
Copyright © American Heart Association, Inc. All rights reserved.
Targets for Antithrombotic Therapy

Aspirin in Primary and Secondary Prevention
ATT Meta-analysis, Lancet 2009

Primary Prevention
Low dose aspirin
• Reduces serious vascular events by ~12% at a cost of bleeding
• Not just for prevention of ischemic events, cancer prevention
• Benefit based on life expectancy and 10-yr CVD risk
• Bleeding risk needs to be assessed (history of GI/intracranial bleeding, concomitant NSAIDs or AC, liver disease, renal disease, bleeding disorder) and modified (e.g. H. Pylori)
• Need to balance ischemic benefit against risk of bleeding and weighing outcomes is complex
• Differences in US and European Guidelines

Primary Prevention
Halvorsen et al. JACC 2014

CAPRIE Steering Committee. Lancet 1996
Thienopyridine Monotherapy
Clopidogrel versus ASA (325 mg) in 19,185 patients (6,452 with PAD)
No difference in Amputations52 with clopidogrel vs 47 with ASA

CURE: benefit of DAPT with aspirin and clopidogrel after ACS
Prop
ortio
n Ev
ent-F
ree
.90
.92
.94
.96
.98
1.00
Week 0 1 2 3 4
RRR: 21% 95% CI, 0.67–0.92 P=.003
Clopidogrel
Placebo
CV Death, MI, or Stroke First 30 Days
No. at Risk5981 5481 4742 4004 3180 24185954 5390 4639 3929 3159 2388
Clopidogrel 6259 6145 6070 6026 5990Placebo 6303 6159 6048 5993 5965
No. at Risk
Prop
ortio
n Ev
ent-F
ree
RRR: 18% 95% CI, 0.70–0.95 P=.009
Clopidogrel
Placebo
CV Death, MI, or Stroke >30 Days–1 Year
Month 1 4 6 8 10 12.90
.92
.94
.96
.98
1.00
Yusuf S, et al. Circulation. 2003;107:966-972.
12,562 Patients with NSTEACS (mostly conservatively managed)

8,688
8,763
0 10 20 30
8
6
4
2
0
CV
Dea
th, M
I, or
Stro
ke (%
)
Clopidogrel
Ticagrelor
4.775.43
HR 0.88 (95% CI 0.77–1.00), p=0.045
No. at risk
Clopidogrel
Ticagrelor
9,291
9,333
8,875
8,942
8,763
8,827
Days after randomisation
31 90 150 210 270 330
8
6
4
2
0
Clopidogrel
Ticagrelor
5.28
6.60
8,688
8,673
8,286
8,397
6,379
6,480
Days after randomisation*
HR 0.80 (95% CI 0.70–0.91), p<0.001
8,437
8,543
6,945
7,028
4,751
4,822
CV
Dea
th, M
I, or
Stro
ke (%
)
Efficacy of ticagrelor vs clopidogrel over time
*Excludes patients with any primary event during the first 30 days
18,624 Patients w/in 24 hrs of onset of ACS (64% underwent PCI)

CHARISMA: DAPT with ASA and Clopidogrel in Secondary Prevention
*All patients received ASA 75-162 mg/day
Placebo + ASA*7.3%
Clopidogrel + ASA*6.8%
RRR: 7.1% [95% CI: -4.5%, 17.5%]P=0.22
Months since randomization
0
2
4
6
8
0 6 12 18 24 30
Dea
th, M
I, or
Str
oke
(%)
Bhatt DL, Fox KA, Hacke W, NEJM 2006
ASA vs. ASA + Clopidogrel in 1º and 2º Atherothrombosis Prevention
N=15,603
12% Reduction in SymptomaticRR 0.88 (0.77 – 0.998, p=0.046)
23% reduction in prior MI

Dual Antiplatelet Therapy in Patients with Symptomatic PAD after Bypass
• 851 patients undergoing unilateral below-knee bypass grafting for atherosclerotic PAD
• ASA (75 mg – 100 mg) + clopigogrel vs. ASA alone
• Primary endpoint composite of index-graft occlusion, revascularization, amputation, or death
Belch et al. Journal of Vascular Sugery. 2010
Benefit in subgroup with prosthetic grafts?

Intracranial Hemorrhage with Long-Term Intensive Antithrombotic Therapy in Stroke Patients
1.4%
1.0%
0.0%
0.5%
1.0%
1.5%
ASA+ERDP Clopidogrel
PROFESS HR 1.42 (1.11 –1.83)
1.0%
0.6%
0.0%
0.5%
1.0%
1.5%
ASA+Clopidogrel Clopidogrel
MATCHRR 1.89 (1.05 –3.40)
2.30%
0.30%0.00% 0.30%0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
History of Stroke Overall
prasugrel clopidogrelTRITON-TIMI 38
P=0.02
Diener H. et al. Lancet 2004 Sacco RL. et al. NEJM 2008, Wiviott SD. et al. NEJM 2007
SPS3 – Lacunar Stroke0.28%
0.15%
0.00%0.05%0.10%0.15%0.20%0.25%0.30%
ASA+Clopidogrel ASA
HR 1.92 (0.82 – 4.54)

Challenge to the Broad Application of Potent Antiplatelet Strategies for Secondary Prevention
MI PAD Stroke
• DAPT beneficial in ACS and more potent agents are superior
• Long-term DAPT may be helpful for secondary prevention of new spontaneous events
• Monotherapybeneficial in symptomatic but benefit unclear in asymptomatic
• Uncertain benefit of DAPT (short or long-term) – does not appear to modify limb ischemic risk
• Monotherapybeneficial
• Long-term DAPT harmful in broad stroke populations

Vorapaxar in Stable Patients with Prior MI, Prior Stroke, or PAD
CV Death, MI, or Stroke
9.3%
10.5%
Hazard Ratio 0.87p < 0.001
N = 26449Mean f/u: 2.5 years Placebo
Vorapaxar
BleedingGUSTO Mod/Sev at 3 yrs
4.2 v. 2.5%, HR 1.66, p<0.001
Morrow DA, Braunwald E, Bonaca MP, et al. N Engl J Med. 2012; 366: 1404-1413

Major Bleeding EndpointsOverall Population
3-yr KM rate (%)Prior Stroke
n = 5746No Hx of Stroke
n = 20699
Morrow et al. NEJM 2012; 366: 1404-1413
ARD 2.0% HR 1.87 P<0.001
ARD 1.5% HR 2.55 P<0.001
ARD 0.2% HR 1.48 P=0.46
ARD 0.2% HR 1.55 P=0.049
ARD 0.1% HR 1.44 P=0.30
ARD 0.7% HR 1.35 P=0.005

Efficacy of PAR-1 Inhibition Independent of P2Y12 Inhibition
Bohula et al. Circulation 2015

Limb Ischemic Events in PADHospitalization for Acute Limb IschemiaPre-specified, adjudicated
2.3%
3.9%
Hazard Ratio 0.5895% CI 0.39 to 0.86
p = 0.006
Placebo
Vorapaxar
N = 3767
Days from randomization
Peripheral RevascularizationPrespecified, Investigator
18.4%
22.2%
Hazard Ratio 0.84;95% CI 0.73 to 0.97
p = 0.017
Bonaca et al. Circulation 2012

Challenge to the Broad Application of Potent Antiplatelet Strategies for Secondary Prevention
MI PAD Stroke
• DAPT beneficial in ACS and more potent agents are superior
• Long-term DAPT may be helpful for secondary prevention of new spontaneous events
• Monotherapybeneficial in symptomatic but benefit unclear in asymptomatic
• Uncertain benefit of DAPT (short or long-term) – does not appear to modify limb ischemic risk
• Monotherapybeneficial
• Long-term DAPT harmful in broad stroke populations
PAR-1 antagonismMACE and limb ischemic
risk reduction

Randomized trials of dual antiplatelettreatment duration after drug-eluting stents
Randomized trials of dual antiplatelettreatment duration after drug-eluting stents
Trial Total DESRandomized
Treatment Duration
Bleeding HR (95% CI)
Stent ThrombosisHR (95% CI)
Myocardial Infarction HR (95% CI)
REAL + ZEST LATE 2701 24 vs. ~12 2.96 (0.31-28.46) 1.23 (0.33-4.58) 1.41 (0.54-3.71)
PRODIGY 1357 24 vs 6 2.17 (1.44-3.22) 0.87 (0.41-1.81) 0.94 (0.61-1.45)
EXCELLENT 1443 12 vs 6 2.0 (0.37-11.11) 0.17 (0.02-1.39) 0.54 (0.21-1.35)
OPTIMIZE 3120 12 vs 3 1.41 (0.63-3.13) 0.95 (0.42-2.04) 0.85 (0.57-1.29)
ARCTIC‐Interruption 1259
Continued DAPT vs.
ASA6.94 (0.85-56.61) 0 vs 3 events* 1.04 (0.41-26.2)
ITALIC 1850 12 vs 6 3 vs. 0 events* 0 vs. 3 events* 0.67 (0.19-2.38)
ISAR‐SAFE 4005 12 vs 6 1.25 (0.34-4.76)0.80 (0.21-3.03)
9 events1.08 (0.51-2.27)
27 events
20
Park, et al. N Eng J Med 2010; 362:15.Valgimigli, et al. Circulation 2012;125:2015. Gwon, et al. Circulation 2012;125:505.Feres, et al. JAMA 2013; 310:510.
Collet, et al. Lancet 2014;384:1577.Gillard, et al. J Am Coll Card Nov 2104.Schultz-Schupke, et al. EHJ Jan 25, 2015.

Mauri et al. NEJM 2014
~ 46% with history of MI
Death, MI or stroke
DAPT: Withdrawal of Thienopyridine 12 Months after Coronary Stenting

DAPT: Prior MI and Efficacy for MACE
Yeh et al. JACC 2015

An Academic Research Organization of Brigham and Women’s Hospital and Harvard Medical School
Months from Randomization
Ticagrelor 60 mgHR 0.84 (95% CI 0.74 – 0.95)
P=0.004
CV
Dea
th, M
I, or
Str
oke
(%)
3 6 9 120 15 18 21 24 27 30 33 36
Ticagrelor 90 mgHR 0.85 (95% CI 0.75 – 0.96)
P=0.008
Placebo (9.0%)
Ticagrelor 90 (7.8%)Ticagrelor 60 (7.8%)
21,162 Patients with Prior MI
6
5
4
3
10
9
8
7
2
1
0
N = 21,162Median follow-up 33 months
Bonaca MP et al. NEJM 2015;372:1791-800

An Academic Research Organization of Brigham and Women’s Hospital and Harvard Medical School
Primary Endpoint – Landmark (ITT)
0%
1%
2%
3%
4%
5%
6%
7%
0 90 180 270 3600%
1%
2%
3%
4%
5%
6%
7%
366 456 546 636 726 816 906 996 1086
CVD
/MI/S
trok
e (%
)
Time from Index MI
3.2%2.8%2.7%
5.9%
5.2%5.1%
First Year of Treatment Subsequent Two Years of Treatment
Ticagrelor 60 mgHR 0.82
(95% CI 0.67 – 0.99)P=0.037
Ticagrelor 90 mgHR 0.86
(95% CI 0.71 – 1.03)P=0.10
Ticagrelor 60 mgHR 0.85
(95% CI 0.73 – 0.998)P=0.047
Ticagrelor 90 mgHR 0.85
(95% CI 0.72 – 0.99)P=0.036
Median 1.7 yrs(1.2 – 2.3)
Median 2.7 yrs(2.2 – 3.3)
Median 4.7 yrs(4.2 – 5.3)
3.1%
2.8%2.5%

An Academic Research Organization of Brigham and Women’s Hospital and Harvard Medical School
0.0%
0.5%
1.0%
1.5%
2.0%
0 90 180 270 360 450 540 630 720 810 900 990 1080
Effect of Ticagrelor on STEMI
Ticagrelor 60 mgHR 0.62
(95% CI 0.45 – 0.86)P=0.00016
Ticagrelor 90 mgHR 0.57
(95% CI 0.41 – 0.79)P=0.0008
Placebo
Ticagrelor 90Ticagrelor 60
Days from Randomization
STEM
I (%
)

An Academic Research Organization of Brigham and Women’s Hospital and Harvard Medical School
Major Adverse Limb Events with TicagrelorAc
ute
Lim
b Is
chem
ia o
r Pe
riphe
ral R
evas
cula
rizat
ion
for I
sche
mia
(%)
Days from Randomization
0.0%
0.2%
0.4%
0.6%
0.8%
1.0%
0 180 360 540 720 900 1080
0.71%
0.46%
HR 0.6595% CI (0.44 – 0.95)
P=0.026
Number at RiskPlacebo
Ticagrelor7067
140956988
139296912
137896701
134256077
1218645189154
21234296

An Academic Research Organization of Brigham and Women’s Hospital and Harvard Medical School
0.0%
0.2%
0.4%
0.6%
0.8%
1.0%
1.2%
1.4%
0 180 360 540 720 900 1080
Thro
mbo
tic C
ompl
icat
ions
(%)
Days from Randomization
PlaceboN=105
Ticagrelor 60 mgHR 0.68 (0.47 – 0.99)
P=0.041 Ticagrelor 60 mg N=47
N=14,112 patientsMedian FUP of 33 months
VENOUS AND INTRACARDIAC THROMBOSIS WITH TICAGRELOR

Outcomes with Continued DAPT after MI
6.4
2.3
3.5
1.40.6
7.5
2.6
4.4
1.7 1.4
0123456789
10
MACE CV Death MI Stroke StentThrombosis(Def/Prob)
Even
t Rat
e (%
)
Extended DAPTAspirin Alone
RR 0.78P = 0.001
RR 0.85P = 0.03
RR 0.70P = 0.003
RR 0.81P = 0.02 RR 0.50
P = 0.02
Udell JA, Bonaca MP et al. Eur Heart J 2015 at eurheartj.oxfordjournals.org.

An Academic Research Organization of Brigham and Women’s Hospital and Harvard Medical School
0.1 0.2 0.5 1 2 5 10
P<0.001
0.1 0.2 0.5 1 2 5 10
Stroke Reduction with Intensive AP Therapy
Stroke
Favors More Intensive AP Therapy
Favors Less Intensive AP Therapy
Ischemic Stroke
P<0.001
Trial N n Intervention Background RR 95% CICHARISMA 3,846 75 Clopidogrel ASA 0.75 0.48-1.81
TRA°2P-TIMI 50 16,897 164 Vorapaxar ASA±clopidogrel 0.62 0.45-0.85
DAPT 9,961 80 Clopidogrel ASA 0.80 0.51-1.25
PEGASUS-TIMI 54 14,112 213 Ticagrelor 60 ASA 0.75 0.57-0.98
Overall 44,816 532 28% 0.72 0.60-0.85
Trial N n Intervention Background RR P-valueCHARISMA 3,846 65 Clopidogrel ASA 0.76 0.47-1.25
TRA2°P-TIMI 50 16,897 136 Vorapaxar ASA±clopidogrel 0.51 0.36-0.72
DAPT 9,961 58 Clopidogrel ASA 0.68 0.40-1.16
PEGASUS-TIMI 54 14,112 181 Ticagrelor 60 ASA 0.76 0.56-1.03
Overall 442 34% 0.66 0.54-0.81
Favors More Intensive AP Therapy
Favors Less Intensive AP Therapy
Bonaca MP et al. Circulation 2016

All Cause Mortality with Prolonged Intensive Antiplatelet Therapy after MI
~11% rededication in all cause mortality– ~17% reduction in CV Mortality (about 60% of deaths)– No excess in non-CV Mortality (about 40% of deaths)
Bonaca MP and Sabatine MS. JAMA Cardiology 2016

1.9
0.4 0.1
1.7
4.0
1.10.3 0.2
1.6
4.2
0123456789
10
MajorBleeding
ICH FatalBleeding
Non-CVDeath
All-CauseDeath
Even
t Rat
e (%
)
Extended DAPTAspirin Alone
RR 1.73P = 0.004
P = NS
RR 1.03P = NS
RR 0.92P = NS
P = NS
Udell JA, et al. Eur Heart J 2015 at eurheartj.oxfordjournals.org.
Safety of Continued DAPT after MI

Prolonged Antiplatelet Therapy and Bleeding
Mauri et al. NEJM 2014
1.6% 1.7%
1.1%0.9%
1.1% 1.1%0.8%
0.4%
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
CHARISMA DAPT TRA2P-TIMI 50 MIon DAPT
TRA2P-TIMI 50 MIon ASA
Treatment Placebo
Slide by Bonaca MP
P < 0.001 for all comparisons at full follow upGUSTO Moderate or Severe
Annualized Rates
Clopidogrel 75 mg daily vs Placebo
Vorapaxar 2.5 mg daily vs Placebo
+ 0.5% + 0.6%
+ 0.3% + 0.5%
Bohula et al. Circ 2015
Vorapaxar“Triple”
Vorapaxar“Dual”
Clopidogrel“Dual”
Berger et al. Circ 2010

Selection of Post-MI Patients for Long-Term Potent Antiplatelet Therapy
High Bleeding Risk
High Ischemic Risk

An Academic Research Organization of Brigham and Women’s Hospital and Harvard Medical School
CVD
/MI/S
trok
e (%
)
Days from Randomization
9.9%
8.0%
7.4%
Placebo
Ticagrelor 60 mg BID Ticagrelor 90 mg BIDHR 0.75
(95% CI 0.61 – 0.92)P=0.0064
HR 0.70(95% CI 0.57 – 0.87)
P=0.0009
MACE at 3 Years with Ticagrelor in Patients with P2Y12Inhibitor Withdrawal ≤ 30 Days from Randomization
NNT=40
NNT=53
0%
2%
4%
6%
8%
10%
12%
0 90 180 270 360 450 540 630 720 810 900 990 1080
Bonaca et al. EHJ 2015

An Academic Research Organization of Brigham and Women’s Hospital and Harvard Medical School
Efficacy of ticagrelor by eGFR
HR 95% CI0.81 (0.68 – 0.96)
ARR = 2.70%NNT 37
HR 95% CI0.88 (0.77 – 1.00)
ARR = 0.63%
Primary Endpoint: CV death, MI, stroke
Months since randomization12 24 36
eGFR < 60 Placebo (N = 1,649)eGFR < 60 Ticagrelor Pooled (N = 3,200)eGFR ≥ 60 Placebo (N = 5,336)eGFR ≥ 60 Ticagrelor Pooled (N = 10,713)
13.99%
11.29%
7.43%
6.80%
3-yr
KM
%
0
2
0
6
12
10
8
16
14
4
Magnani G et al. and Bonaca MP EHJ 2015

4
12
8
16
Incid
ence
(%)
7.9%
6.8%
12 24Time (Months)
36
15.7%
12.6%
HR 0.77 p=0.004
ARD -3.1NNT=30 95% CI 19, 92
HR 0.83 p=0.005
ARD -1.1 NNT=76 95% CI 47, 247
Efficacy of Vorapaxar in Patients w/ Prior MI Based on Diabetes History
CV Death, MI, or stroke (%)
PlaceboVorapaxar DM
No DM
0
p-int 0.51
Cavender et al. Circulation 2015;131:1047-53
Net Clinical Outcome(All‐Cause‐Mortality/MI/CVA/
GUSTO Severe Bleeding)HR: 0.77 (0.65‐0.93)
p = 0.006

An Academic Research Organization of Brigham and Women’s Hospital and Harvard Medical School
CV
Dea
th, M
I, or
Str
oke
(%)
Days from Randomization
0%
5%
10%
15%
20%
25%
0 90 180 270 360 450 540 630 720 810 900 990 1080
19.3%
15.2%
8.4%7.4%
PADHR 0.75
95% (CI 0.55 – 1.01) ARR 4.1%NNT 25
No PADHR 0.86
95% (CI 0.77 – 0.96)
P-interaction 0.41
Ticagrelor(pooled doses)
Placebo
ARR 1.0%NNT 100
MACE with Ticagrelor by PAD at Baseline
Bonaca et al. JACC 2016

Risk Scores – Common Themes
Baber et al. JACC 2016
DAPT PARIS TIMI PEGASUS-TIMI 54
Diabetes Mellitus ▲Ischemic Risk ▲Ischemic Risk ▲Ischemic Risk ▲Ischemic Risk
Prior MI/ACS ▲Ischemic Risk ▲Ischemic Risk ▲Ischemic Risk ▲Ischemic Risk
Prior CABG / MVD ▲Ischemic Risk ▲Ischemic Risk ▲Ischemic Risk ▲Ischemic Risk
Renal Dysfunction ▲Ischemic Risk ▲Ischemic Risk ▲Ischemic Risk
Current Smoking ▲Ischemic Risk ▲Ischemic Risk ▲Ischemic Risk
PAD ▲Ischemic Risk ▲Ischemic Risk
CHF or low EF ▲Ischemic Risk ▲Ischemic Risk
Age ▲Bleeding Risk ▲Bleeding Risk ▲Ischemic Risk ▲Ischemic Risk
Prior stroke ▲Ischemic Risk
Hypertension ▲Ischemic Risk
Prior PCI ▲Ischemic Risk ▲Ischemic Risk
Stent Diameter ▲Ischemic Risk
Paclitaxel Stent ▲Ischemic Risk
Yeh et al. JAMA 2016 Bohula et al. Circ 2016Slide by Marc Bonaca

An Approach to Long-Term DAPT/TAPT after MI
Who
• Patients with prior MI at high risk:
• Diabetes mellitus• Multiple prior MIs• Renal dysfunction• MVD / prior CABG• PAD• Smoker• CHF / low EF
• Not at high risk for bleeding
• Prior/risk of ICH• Recent major
Bleeding• Bleeding diathesis• On anticoagulation• Low BMI / anemia
When
• Continue after started for MI and re-evaluate at each visit:
• Recent bleeding?
• Are they tolerating?
• Are they adherent?
• Contraindications (e.g. new dx of AF requiring anticoagulation)
Why
• To reduce long-term ischemic risk including:
• New spontaneous MI including STEMI
• Ischemic stroke including disabling events
• Limb ischemic events in PAD
• CV mortality as predominant cause of death
Slide by Marc Bonaca

1, 2, 3 Drugs – which drugs and for how long?
Slide by Marc Bonaca
CAD PAD AtherothrmoboticStroke
AP Monotherapy No prior MI or recent stenting
Symptomatic PAD notat high-risk for
MACE/ALI, consider in asymptomatic
Prior stroke (excluding AF/embolic)
ASA+ clopidogrel
Limited duration after elective
stenting or ACS and needs anticoagulant
Limited duration after elective stenting
Selected patients with acute stroke for short
duration
Monotherapy+ vorapaxar
Prior MI with highischemic risk and low bleeding risk (e.g. DM, MVD)
Symptomatic PAD with MACE or ALI
risk (e.g. prior ALI or revascularization)
Contraindicated
ASA+ticagrelor
ASA+clopiodgrel+vorapaxar
Prior MI with highischemic risk and low bleeding risk
Net benefit in high risk (e.g. DM, MVD)
Caution with ASA + potent P2Y12
Vorapaxar contraindicated