Embed Size (px)
Citation preview
Antimicrobial Susceptibility
Summary 2017
Clinical Microbiology Department of Pathology & Laboratory Medicine

Antimicrobial Susceptibility Summary
Clinical Microbiology Department of Pathology and
Laboratory Medicine
UCLA Health System
2017
The information contained in this booklet can also be found at:
http://www.asp.mednet.ucla.edu/pages/
Select “Antimicrobial Susceptibility Summary” on left side of homepage

Preface This booklet contains up-to-date information to assist the clinician in making decisions concerning antimicrobial therapy and testing. These tables summarize susceptibility data obtained for organisms isolated in the UCLA Clinical Microbiology Laboratory in 2016. Percent Susceptible Data (Tables 1-12)
Emerging Resistance Trends at UCLA (Tables 13-18) Antimicrobial Testing and Reporting Policies (Tables 28–29) In order to provide the most meaningful information, the laboratory is selective in reporting antimicrobial susceptibility results. Reporting guidelines are based on:
1. Identity of the organism 2. Body site of culture 3. Overall antibiogram of the organism 4. Therapeutically relevant antimicrobials 5. Formulary status of the antimicrobial
Non-formulary drugs are not routinely reported and controlled formulary agents (Table 27) are reported only in the appropriate setting: e.g. amikacin and tobramycin if resistant to gentamicin. Results of all relevant drugs tested, including those not reported, are available upon request. We thank:
Brandy Bryant, Dept. of Quality Diane Citron, R.M. Alden Research Lab Jennifer Currello, PharmD, Dept. Pharmaceutical Services Janet A. Hindler, MT (ASCP), Sr. Specialist, Clinical
Microbiology Meganne S. Kanatani, PharmD, Dept. Pharmaceutical Services Elise Martin, MD, Division of Infectious Diseases Amy Shayne, Administrative Specialist, Brentwood Annex Daniel Uslan, MD, Division of Infectious Diseases
Guidelines for Interpretation of Minimal Inhibitory Concentrations (MICs)
MICs are interpreted as susceptible, intermediate, resistant, non-susceptible or susceptible dose dependent according to Clinical and Laboratory Standards Institute (CLSI) guidelines. When deciding whether the interpretation is meaningful, one should consider the antimicrobial pharmacokinetics, taking into account dosage and route of administration, the infecting organism and site of infection, and previous clinical experience. For antimicrobials without interpretive criteria (e.g. colistin & enterobacteriaceae), an interpretation of wild-type (no resistance genes/mutations) or non-wild-type (with resistance gene or mutation) may be reported. Consultation with Infectious Diseases strongly advised in these cases. For additional information, please call the antimicrobial testing laboratory, or Antimicrobial Stewardship hotline. Romney M. Humphries, Ph.D., D(ABMM) Section Chief, Clinical Microbiology Omai B. Garner, Ph.D., D(ABMM) Associate Director, Clinical Microbiology Cynthia Toy, M.T. (ASCP) Director of Clinical Microbiology Sylvia Miyagishima, Sr. CLS Supervisor Ruel Mirasol, M.T. (ASCP) Sr. Specialist, Clinical Microbiology Allison Tsan, CLS Sr. Specialist, Clinical Microbiology Alyssa Ziman, M.D., Director of Clinical Laboratories
Clinical Microbiology UCLA Health System Department of Pathology and Laboratory Medicine 171315
Frequently called numbers*: Antimicrobial Stewardship Hotline ........... 310-267-7567 Antimicrobial Testing Laboratory ............ 310-794-2760 Drug Information Center ........................... 310-267-8522 Infection Control (SMH-UCLA) ................. 424-259-4454 Infection Control (RRUMC) ...................... 310-794-0187 Infectious Diseases (Adult) ..................... 310-825-7225 Infectious Diseases (Pediatric) ................. 310-825-5235 Infectious Disease Pharmacist (page 92528) ......................................... 310-267-8510 Microbiology Fellow on-call .......................... page 90103
* If calling within UCLA system, dial the last 5 digits of the phone number.
Table of Contents Table ............................................................................ Page
1 Adults (>21 y.o.) Most Common Gram-negative Bacteria – Non-Urine Isolates, % Susceptible ................................. 1
2 Adults (>21 y.o.) Gram-negative Bacteria – Non-Urine Isolates, % Susceptible .................................................. 2
3 Adults (>21 y.o.) Gram-negative Bacteria – Urine Isolates, % Susceptible ......................................................... 3
4 Adults (>21 y.o.) Gram-positive Cocci, % Susceptible ...................... 4
5 Miscellaneous Gram-negative Bacteria............................................. 6
6 Pseudomonas aeruginosa – % Susceptible to One or Two Antimicrobials .............................................................. 7
7 Stenotrophomonas maltophilia – % Susceptible to One or Two Antimicrobials .............................................................. 8
8 Most Resistant Gram-negative Bacteria – Non-Urine Isolates, % Susceptible ...................................................................................... 9
9 Pediatrics (≤ 21 y.o.) Gram-negative Bacteria – Non-Urine Isolates, % Susceptible ............................................. 10
10 Pediatrics (≤ 21 y.o.) Gram-negative Bacteria – Urine Isolates, % Susceptible ........................................................ 11
11 Pediatrics (≤ 21 y.o.) Gram-positive Cocci, % Susceptible ............................................................................... 12
12 Yeasts, % Susceptible, 2014–2016 ................................................ 14
13 Emerging Resistance Concerns ...................................................... 15
14 Resistance Trends: 1990-2016 ....................................................... 19
15 Carbapenem-resistant Enterobacteriaceae (CRE): 2009-2016 ....... 22
Table of Contents Table ...................................................................... Page
16 Treatment Suggestions for Organisms for which Susceptibility Testing is Not Routinely Performed ................................................ 23
17 Blood: One Isolate per Patient, 2016 .............................................. 24
18 CSF: One Isolate per Patient, 2016 ................................................ 26
19 Mycobacteria, One Isolate per Patient per Source, 2016 ................ 27
20 Mycobacteria Antimicrobial Susceptibility Testing ........................... 28
21 California Mycobacterium tuberculosis % Resistant, 2012-2015 .... 29
22 Rapid Grower - Mycobacteria % Susceptible, 2011-2016 ............... 30
23 Anaerobic Bacteria, % Susceptible ................................................. 31
24 Antimicrobials (IV, PO), Formulary Status and Cost Reference ..... 32
25 Indications for Performing Routine Antimicrobial Susceptibility Tests – Aerobic Bacteria ............................................................... 35
26 Antimicrobial Agents Routinely Reported – Aerobic Bacteria .......... 37
27 Expected Antimicrobial Susceptibility Patterns of the Most Commonly Isolated Nocardia ........................................................ 41
28 Susceptible MIC (μg/ml) Breakpoints for Aerobic Gram-negative Bacilli ............................................................................................. 42
29 Susceptible MIC (μg/ml) Breakpoints for Aerobic Gram-positive Cocci ............................................................................................. 43
30 Antimicrobial Stewardship ............................................................... 44
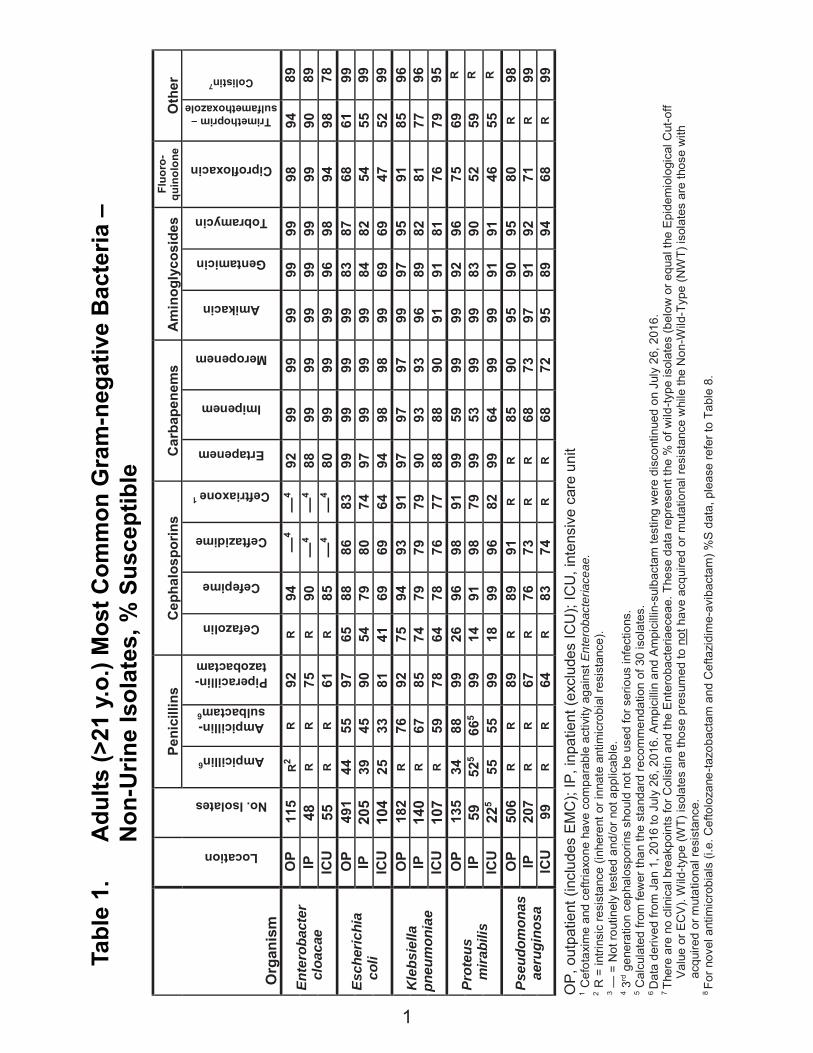
Tabl
e 1.
A
dults
(>21
y.o
.) M
ost C
omm
on G
ram
-neg
ativ
e B
acte
ria –
N
on-U
rine
Isol
ates
, % S
usce
ptib
le
Pe
nici
llins
C
epha
losp
orin
s C
arba
pene
ms
Am
inog
lyco
side
s Fl
uoro
-qu
inol
one
Oth
er
Org
anis
m
Location
No. Isolates
Ampicillin6
Ampicillin- sulbactam6
Piperacillin- tazobactam
Cefazolin
Cefepime
Ceftazidime
Ceftriaxone 1
Ertapenem
Imipenem
Meropenem
Amikacin
Gentamicin
Tobramycin
Ciprofloxacin
Trimethoprim – sulfamethoxazole
Colistin7
Ente
roba
cter
cloa
cae
OP
115
R2
R
92
R
94
—4
—4
92
99
99
99
99
99
98
94
89
IP
48
R
R
75
R
90
—4
—4
88
99
99
99
99
99
99
90
89
ICU
55
R
R
61
R
85
—4
—4
80
99
99
99
96
98
94
98
78
Esch
eric
hia
co
li
OP
491
44
55
97
65
88
86
83
99
99
99
99
83
87
68
61
99
IP
205
39
45
90
54
79
80
74
97
99
99
99
84
82
54
55
99
ICU
10
4 25
33
81
41
69
69
64
94
98
98
99
69
69
47
52
99
Kle
bsie
lla
pneu
mon
iae
OP
182
R
76
92
75
94
93
91
97
97
97
99
97
95
91
85
96
IP
140
R
67
85
74
79
79
79
90
93
93
96
89
82
81
77
96
ICU
10
7 R
59
78
64
78
76
77
88
88
90
91
91
81
76
79
95
Prot
eus
m
irabi
lis
OP
135
34
88
99
26
96
98
91
99
59
99
99
92
96
75
69
R
IP
59
525
665
99
14
91
98
79
99
53
99
99
83
90
52
59
R
ICU
22
5 55
55
99
18
99
96
82
99
64
99
99
91
91
46
55
R
Pseu
dom
onas
aeru
gino
sa
OP
506
R
R
89
R
89
91
R
R
85
90
95
90
95
80
R
98
IP
207
R
R
67
R
76
73
R
R
68
73
97
91
92
71
R
99
ICU
99
R
R
64
R
83
74
R
R
68
72
95
89
94
68
R
99
OP
, out
patie
nt (i
nclu
des
EM
C);
IP, i
npat
ient
(exc
lude
s IC
U);
ICU
, int
ensi
ve c
are
unit
1 C
efot
axim
e an
d ce
ftria
xone
hav
e co
mpa
rabl
e ac
tivity
aga
inst
Ent
erob
acte
riace
ae.
2 R
= in
trins
ic re
sist
ance
(inh
eren
t or i
nnat
e an
timic
robi
al re
sist
ance
). 3 —
= N
ot ro
utin
ely
test
ed a
nd/o
r not
app
licab
le.
4 3rd g
ener
atio
n ce
phal
ospo
rins
shou
ld n
ot b
e us
ed fo
r ser
ious
infe
ctio
ns.
5 Cal
cula
ted
from
few
er th
an th
e st
anda
rd re
com
men
datio
n of
30
isol
ates
. 6 D
ata
deriv
ed fr
om J
an 1
, 201
6 to
Jul
y 26
, 201
6. A
mpi
cilli
n an
d A
mpi
cilli
n-su
lbac
tam
test
ing
wer
e di
scon
tinue
d on
Jul
y 26
, 201
6.
7 Th
ere
are
no c
linic
al b
reak
poin
ts fo
r Col
istin
and
the
Ent
erob
acte
riaec
eae.
The
se d
ata
repr
esen
t the
% o
f wild
-type
isol
ates
(bel
ow o
r equ
al th
e E
pide
mio
logi
cal C
ut-o
ff V
alue
or E
CV
). W
ild-ty
pe (W
T) is
olat
es a
re th
ose
pres
umed
to n
ot h
ave
acqu
ired
or m
utat
iona
l res
ista
nce
whi
le th
e N
on-W
ild-T
ype
(NW
T) is
olat
es a
re th
ose
with
ac
quire
d or
mut
atio
nal r
esis
tanc
e.
8 Fo
r nov
el a
ntim
icro
bial
s (i.
e. C
efto
loza
ne-ta
zoba
ctam
and
Cef
tazi
dim
e-av
ibac
tam
) %S
dat
a, p
leas
e re
fer t
o Ta
ble
8.
1
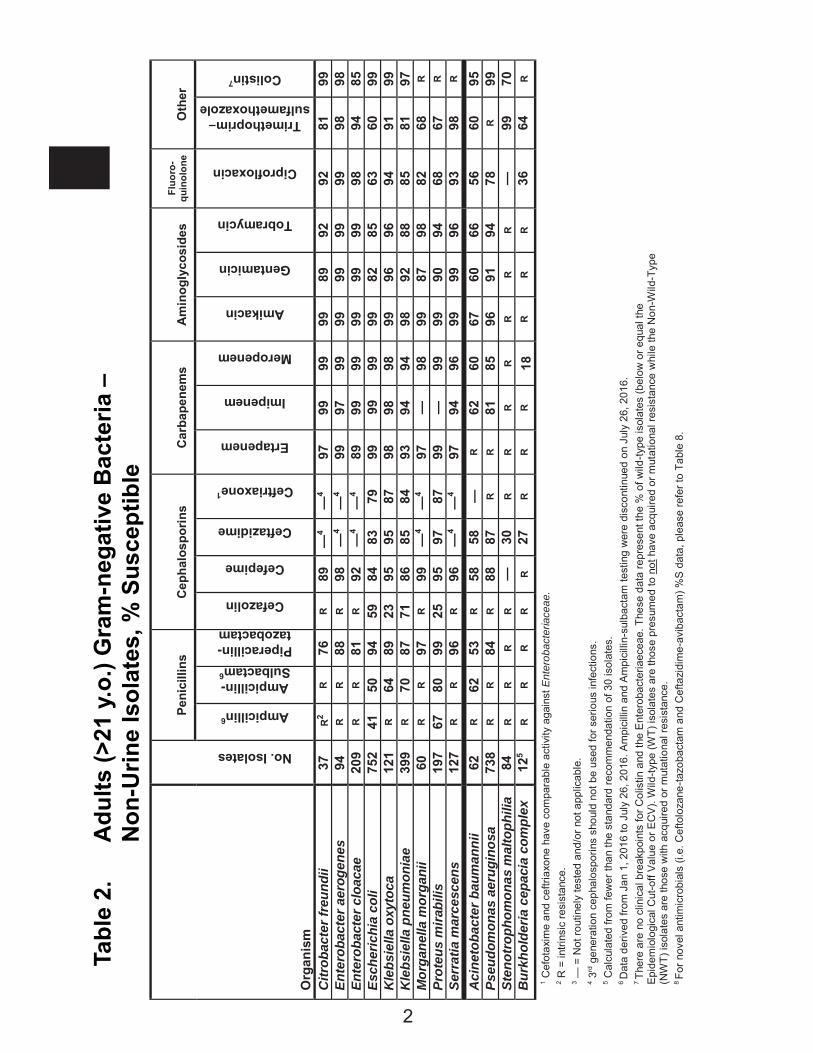
Tabl
e 2.
A
dults
(>21
y.o
.) G
ram
-neg
ativ
e B
acte
ria –
Non
-Urin
e Is
olat
es, %
Sus
cept
ible
Peni
cilli
ns
Cep
halo
spor
ins
Car
bape
nem
s A
min
ogly
cosi
des
Fluo
ro-
quin
olon
e O
ther
Org
anis
m
No. Isolates
Ampicillin6
Ampicillin- Sulbactam6
Piperacillin- tazobactam
Cefazolin
Cefepime
Ceftazidime
Ceftriaxone1
Ertapenem
Imipenem
Meropenem
Amikacin
Gentamicin
Tobramycin
Ciprofloxacin
Trimethoprim– sulfamethoxazole
Colistin7
Citr
obac
ter f
reun
dii
37
R2
R
76
R
89
—4
—4
97
99
99
99
89
92
92
81
99
Ente
roba
cter
aer
ogen
es
94
R
R
88
R
98
—4
—4
99
97
99
99
99
99
99
98
98
Ente
roba
cter
clo
acae
20
9 R
R
81
R
92
—4
—4
89
99
99
99
99
99
98
94
85
Esch
eric
hia
coli
752
41
50
94
59
84
83
79
99
99
99
99
82
85
63
60
99
Kle
bsie
lla o
xyto
ca
121
R
64
89
23
95
95
87
98
98
98
99
96
96
94
91
99
Kle
bsie
lla p
neum
onia
e 39
9 R
70
87
71
86
85
84
93
94
94
98
92
88
85
81
97
Mor
gane
lla m
orga
nii
60
R
R
97
R
99
—4
—4
97
—
98
99
87
98
82
68
R
Prot
eus
mira
bilis
19
7 67
80
99
25
95
97
87
99
—
99
99
90
94
68
67
R
Serr
atia
mar
cesc
ens
127
R
R
96
R
96
—4
—4
97
94
96
99
99
96
93
98
R
Aci
neto
bact
er b
aum
anni
i 62
R
62
53
R
58
58
—
R
62
60
67
60
66
56
60
95
Pseu
dom
onas
aer
ugin
osa
738
R
R
84
R
88
87
R
R
81
85
96
91
94
78
R
99
Sten
otro
phom
onas
mal
toph
ilia
84
R
R
R
R
—
30
R
R
R
R
R
R
R
—
99
70
Bur
khol
deria
cep
acia
com
plex
12
5 R
R
R
R
R
27
R
R
R
18
R
R
R
36
64
R
1 Cef
otax
ime
and
ceftr
iaxo
ne h
ave
com
para
ble
activ
ity a
gain
st E
nter
obac
teria
ceae
. 2 R
= in
trins
ic re
sist
ance
. 3 —
= N
ot ro
utin
ely
test
ed a
nd/o
r not
app
licab
le.
4 3rd g
ener
atio
n ce
phal
ospo
rins
shou
ld n
ot b
e us
ed fo
r ser
ious
infe
ctio
ns.
5 Cal
cula
ted
from
few
er th
an th
e st
anda
rd re
com
men
datio
n of
30
isol
ates
. 6 D
ata
deriv
ed fr
om J
an 1
, 201
6 to
Jul
y 26
, 201
6. A
mpi
cilli
n an
d A
mpi
cilli
n-su
lbac
tam
test
ing
wer
e di
scon
tinue
d on
Jul
y 26
, 201
6.
7 Th
ere
are
no c
linic
al b
reak
poin
ts fo
r Col
istin
and
the
Ent
erob
acte
riaec
eae.
The
se d
ata
repr
esen
t the
% o
f wild
-type
isol
ates
(bel
ow o
r equ
al th
e E
pide
mio
logi
cal C
ut-o
ff V
alue
or E
CV
). W
ild-ty
pe (W
T) is
olat
es a
re th
ose
pres
umed
to n
ot h
ave
acqu
ired
or m
utat
iona
l res
ista
nce
whi
le th
e N
on-W
ild-T
ype
(NW
T) is
olat
es a
re th
ose
with
acq
uire
d or
mut
atio
nal r
esis
tanc
e.
8 Fo
r nov
el a
ntim
icro
bial
s (i.
e. C
efto
loza
ne-ta
zoba
ctam
and
Cef
tazi
dim
e-av
ibac
tam
) %S
dat
a, p
leas
e re
fer t
o Ta
ble
8.
2

Tabl
e 3.
A
dults
(>21
y.o
.) G
ram
-neg
ativ
e B
acte
ria –
U
rine
Isol
ates
, % S
usce
ptib
le
Pe
nici
llin
Ce
phal
ospo
rins
Ca
rbap
enem
s Am
ino-
glyc
osde
Fl
uoro
-qu
inol
one
Oth
er
Org
anis
m
Source
No. Isolates
Ampicillin
Oral Cephalosporins1
Cefepime
Ceftriaxone 2
Ertapenem
Imipenem
Meropenem
Gentamicin
Ciprofloxacin
Nitrofurantoin
Trimethoprim – sulfamethoxazole
Ente
roba
cter
cloa
cae
O
P 14
4 R
3 R
99
—4,
5 97
99
99
97
97
46
83
IP
24
6 R
R 96
—
5 71
99
99
99
99
42
88
Esch
eric
hia
coli
O
P 65
35
55
89
—
92
99
99
99
91
78
97
74
IP
434
38
70
—
75
98
99
99
81
58
95
59
Kleb
siel
la
pneu
mon
iae
O
P 10
84
R 93
—
93
99
99
99
95
95
39
86
IP
17
3 R
81
—
81
95
97
97
91
84
36
75
Prot
eus
m
irabi
lis
OP
500
80
94
—
97
97
—
99
92
77
R 76
IP
71
78
90
—
93
97
—
99
92
72
R
72
Pseu
dom
onas
ae
rugi
nosa
7 O
P 24
3 R
R 93
R
R 86
91
93
80
R
R IP
91
R
R 83
R
R 72
78
94
77
R
R O
P, o
utpa
tient
(inc
lude
s EM
C); I
P, in
patie
nt (i
nclu
des
all u
nits
and
ICUs
) 1
Ora
l cep
halo
spor
ins
incl
ude
cefp
odox
ime
and
ceph
alex
in fo
r tre
atm
ent o
f unc
ompl
icat
ed u
rinar
y tra
ct in
fect
ions
. 2
C
efot
axim
e an
d ce
ftria
xone
hav
e co
mpa
rabl
e ac
tivity
aga
inst
Ent
erob
acte
riace
ae
3 R
= in
trins
ic re
sista
nce.
4
— =
Not
rout
inel
y te
sted
and
/or n
ot a
pplic
able
. 5
3rd g
ener
atio
n ce
phal
ospo
rins
shou
ld n
ot b
e us
ed fo
r ser
ious
infe
ctio
ns.
6 Cal
cula
ted
from
few
er th
an th
e st
anda
rd re
com
men
datio
n of
30
isol
ates
7
Cef
tazid
ime:
OP
91%
, IP
85%
, Pip
erac
illin-
tazo
bact
am: O
P 89
%, I
P 79
%
3
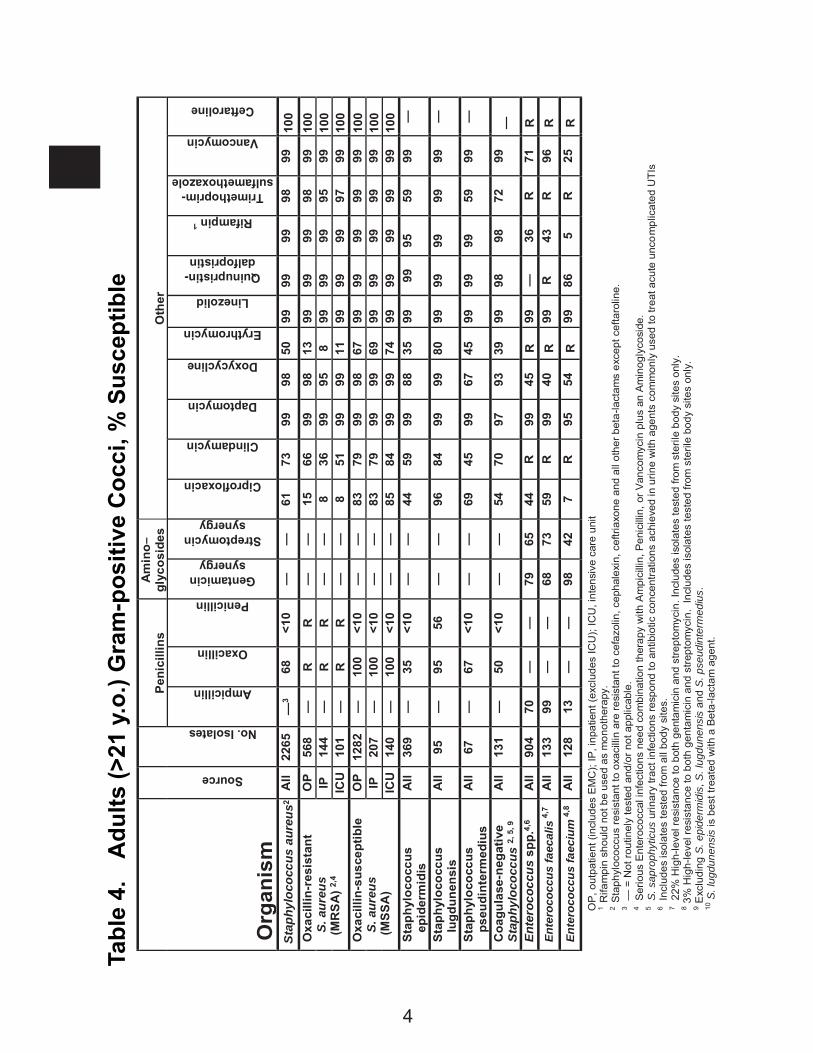
Tabl
e 4.
A
dults
(>21
y.o
.) G
ram
-pos
itive
Coc
ci, %
Sus
cept
ible
Pe
nici
llins
A
min
o–
glyc
osid
es
Oth
er
Org
anis
m
Source
No. Isolates
Ampicillin
Oxacillin
Penicillin
Gentamicin synergy
Streptomycin synergy
Ciprofloxacin
Clindamycin
Daptomycin
Doxycycline
Erythromycin
Linezolid
Quinupristin-dalfopristin
Rifampin 1
Trimethoprim-sulfamethoxazole
Vancomycin
Ceftaroline
Stap
hylo
cocc
us a
ureu
s2
All
2265
—
3 68
<1
0 —
—
61
73
99
98
50
99
99
99
98
99
10
0 O
xaci
llin-
resi
stan
t
S. a
ureu
s (
MR
SA
) 2,4
OP
568
—
R
R
—
—
15
66
99
98
13
99
99
99
98
99
100
IP
144
—
R
R
—
—
8 36
99
95
8
99
99
99
95
99
100
ICU
10
1 —
R
R
—
—
8
51
99
99
11
99
99
99
97
99
100
Oxa
cilli
n-su
scep
tible
S. a
ureu
s (
MSS
A)
OP
1282
—
10
0 <1
0 —
—
83
79
99
98
67
99
99
99
99
99
10
0 IP
20
7 —
10
0 <1
0 —
—
83
79
99
99
69
99
99
99
99
99
10
0 IC
U
140
—
100
<10
—
—
85
84
99
99
74
99
99
99
99
99
100
Stap
hylo
cocc
us
epid
erm
idis
A
ll 36
9 —
35
<1
0 —
—
44
59
99
88
35
99
99
95
59
99
—
St
aphy
loco
ccus
lu
gdun
ensi
s A
ll 95
—
95
56
—
—
96
84
99
99
80
99
99
99
99
99
—
St
aphy
loco
ccus
ps
eudi
nter
med
ius
All
67
—
67
<10
—
—
69
45
99
67
45
99
99
99
59
99
—
Coa
gula
se-n
egat
ive
St
aphy
loco
ccus
2, 5
, 9
All
131
—
50
<10
—
—
54
70
97
93
39
99
98
98
72
99
—
Ente
roco
ccus
spp
.4,6
All
904
70
—
—
79
65
44
R
99
45
R
99
—
36
R
71
R
Ente
roco
ccus
faec
alis
4,7
All
133
99
—
—
68
73
59
R
99
40
R
99
R
43
R
96
R
Ente
roco
ccus
faec
ium
4,8
All
128
13
—
—
98
42
7 R
95
54
R
99
86
5
R
25
R
OP
, out
patie
nt (i
nclu
des
EM
C);
IP, i
npat
ient
(exc
lude
s IC
U);
ICU
, int
ensi
ve c
are
unit
1 R
ifam
pin
shou
ld n
ot b
e us
ed a
s m
onot
hera
py.
2 S
taph
yloc
occu
s re
sist
ant t
o ox
acill
in a
re re
sist
ant t
o ce
fazo
lin, c
epha
lexi
n, c
eftri
axon
e an
d al
l oth
er b
eta-
lact
ams
exce
pt c
efta
rolin
e.
3 — =
Not
rout
inel
y te
sted
and
/or n
ot a
pplic
able
. 4 S
erio
us E
nter
ococ
cal i
nfec
tions
nee
d co
mbi
natio
n th
erap
y w
ith A
mpi
cilli
n, P
enic
illin
, or V
anco
myc
in p
lus
an A
min
ogly
cosi
de.
5 S. s
apro
phyt
icus
urin
ary
tract
infe
ctio
ns re
spon
d to
ant
ibio
tic c
once
ntra
tions
ach
ieve
d in
urin
e w
ith a
gent
s co
mm
only
use
d to
trea
t acu
te u
ncom
plic
ated
UTI
s 6 I
nclu
des
isol
ates
test
ed fr
om a
ll bo
dy s
ites.
7 2
2% H
igh-
leve
l res
ista
nce
to b
oth
gent
amic
in a
nd s
trept
omyc
in. I
nclu
des
isol
ates
test
ed fr
om s
teril
e bo
dy s
ites
only
. 8 3
% H
igh-
leve
l res
ista
nce
to b
oth
gent
amic
in a
nd s
trept
omyc
in.
Incl
udes
isol
ates
test
ed fr
om s
teril
e bo
dy s
ites
only
. 9 E
xclu
ding
S. e
pide
rmid
is, S
. lug
dune
nsis
and
S. p
seud
inte
rmed
ius.
10
S. l
ugdu
nens
is is
bes
t tre
ated
with
a B
eta-
lact
am a
gent
.
4
Tabl
e 4.
A
dults
(>21
y.o
.) G
ram
-pos
itive
Coc
ci, %
Sus
cept
ible
(c
ont.)
Pe
nici
llins
Ce
phal
ospo
rins
Oth
er
Org
anis
m
No. Isolates
Amoxicillin
Penicillin
Cefotaxime
Ceftriaxone
Clindamycin
Doxycycline
Erythromycin
Levofloxacin
Trimethoprim – sulfamethoxazole
Vancomycin
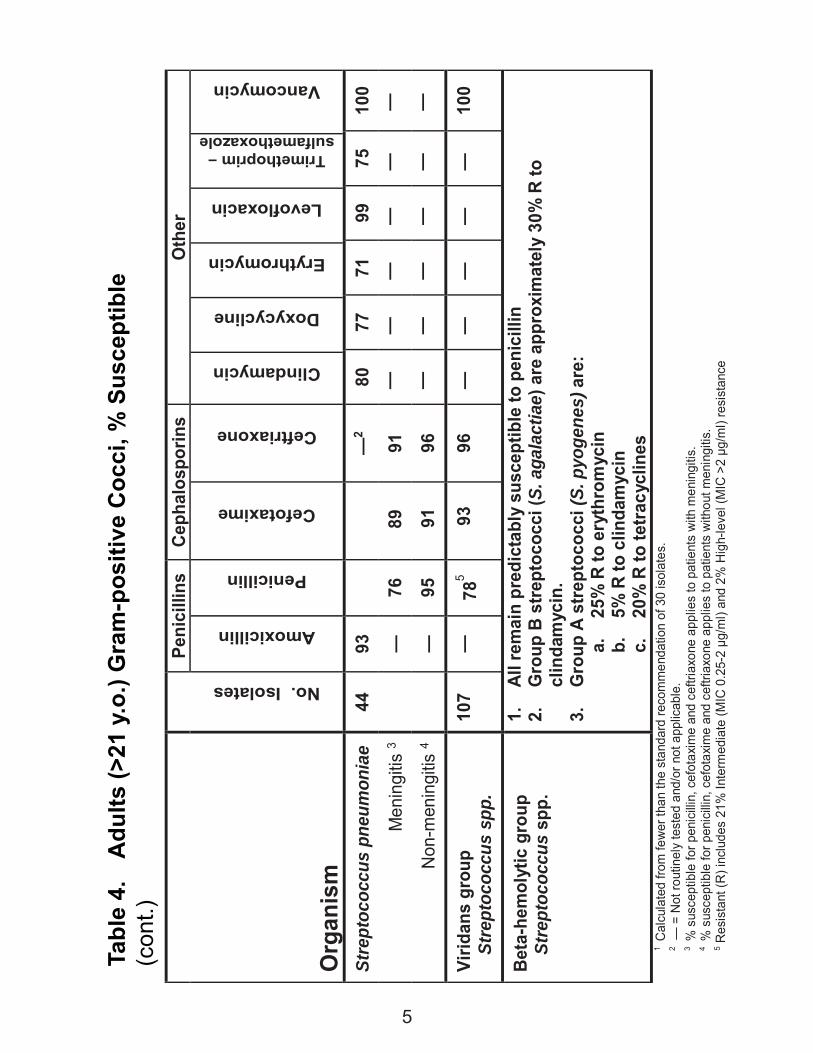
Stre
ptoc
occu
s pn
eum
onia
e 44
93
—
2 80
77
71
99
75
10
0
Men
ingi
tis 3
—
76
8
9 91
—
—
—
—
—
—
N
on-m
enin
gitis
4
—
95
91
96
—
—
—
—
—
—
Virid
ans
grou
p St
rept
ococ
cus
spp.
10
7 —
78
5 9
3 96
—
—
—
—
—
10
0
Beta
-hem
olyt
ic g
roup
St
rept
ococ
cus
spp.
1.
Al
l rem
ain
pred
icta
bly
susc
eptib
le to
pen
icill
in
2.
Gro
up B
stre
ptoc
occi
(S. a
gala
ctia
e) a
re a
ppro
xim
atel
y 30
% R
to
clin
dam
ycin
.
3.
Gro
up A
stre
ptoc
occi
(S. p
yoge
nes)
are
: a.
25
% R
to e
ryth
rom
ycin
b.
5%
R to
clin
dam
ycin
c.
20
% R
to te
tracy
clin
es
1 C
alcu
late
d fro
m fe
wer
than
the
stan
dard
reco
mm
enda
tion
of 3
0 is
olat
es.
2 — =
Not
rout
inel
y te
sted
and
/or n
ot a
pplic
able
. 3 %
sus
cept
ible
for p
enic
illin,
cef
otax
ime
and
ceftr
iaxo
ne a
pplie
s to
pat
ient
s w
ith m
enin
gitis
. 4 %
sus
cept
ible
for p
enic
illin,
cef
otax
ime
and
ceftr
iaxo
ne a
pplie
s to
pat
ient
s w
ithou
t men
ingi
tis.
5 Res
ista
nt (R
) inc
lude
s 21
% In
term
edia
te (M
IC 0
.25-
2 μg
/ml)
and
2% H
igh-
leve
l (M
IC >
2 μg
/ml)
resi
stan
ce
5
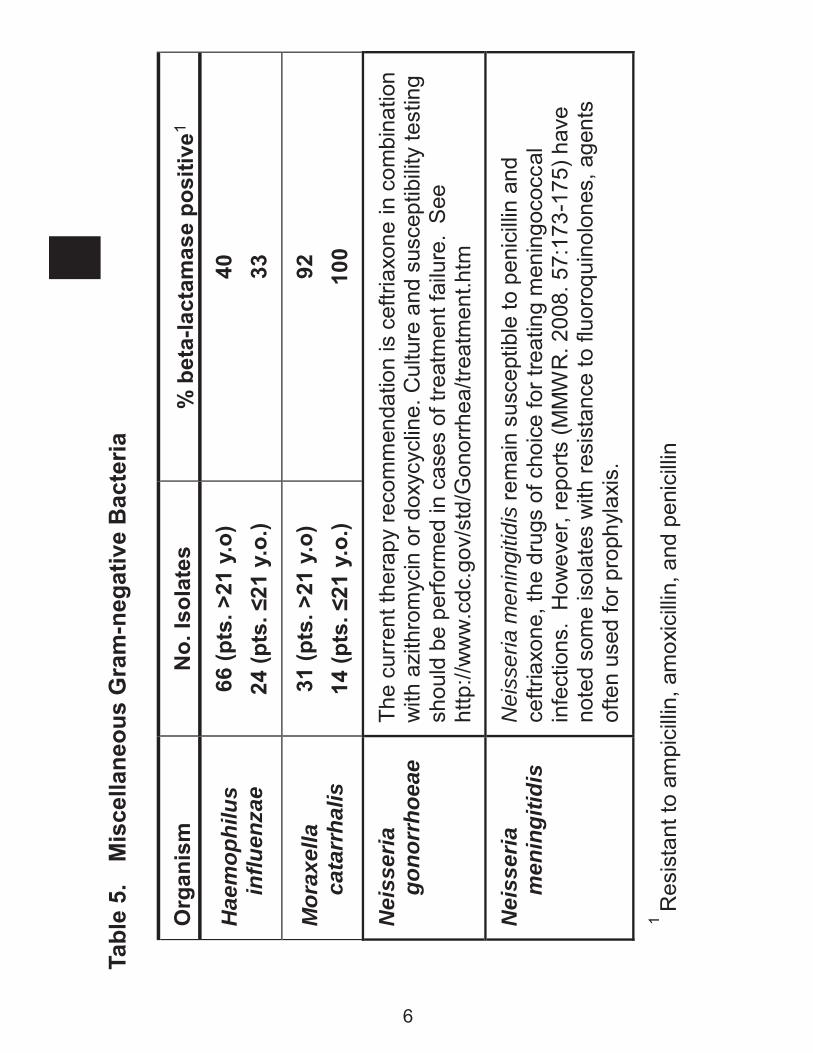
Tabl
e 5.
M
isce
llane
ous
Gra
m-n
egat
ive
Bac
teria
Org
anis
m
No.
Isol
ates
%
bet
a-la
ctam
ase
posi
tive1
Hae
mop
hilu
s in
fluen
zae
66 (p
ts. >
21 y
.o)
24 (p
ts. ≤
21 y
.o.)
40
33
Mor
axel
la
cata
rrha
lis
31 (p
ts. >
21 y
.o)
14 (p
ts. ≤
21 y
.o.)
92
100
Nei
sser
ia
gono
rrho
eae
The
curr
ent t
hera
py re
com
men
datio
n is
cef
triax
one
in c
ombi
natio
n w
ith a
zith
rom
ycin
or d
oxyc
yclin
e. C
ultu
re a
nd s
usce
ptib
ility
test
ing
shou
ld b
e pe
rform
ed in
cas
es o
f tre
atm
ent f
ailu
re. S
ee
http
://w
ww
.cdc
.gov
/std
/Gon
orrh
ea/tr
eatm
ent.h
tm
Nei
sser
ia
men
ingi
tidis
N
eiss
eria
men
ingi
tidis
rem
ain
susc
eptib
le to
pen
icill
in a
nd
ceftr
iaxo
ne, t
he d
rugs
of c
hoic
e fo
r tre
atin
g m
enin
goco
ccal
in
fect
ions
. H
owev
er, r
epor
ts (M
MW
R. 2
008.
57:
173-
175)
hav
e no
ted
som
e is
olat
es w
ith re
sist
ance
to fl
uoro
quin
olon
es, a
gent
s of
ten
used
for p
roph
ylax
is.
1 Res
ista
nt to
am
pici
llin,
am
oxic
illin
, and
pen
icill
in
6
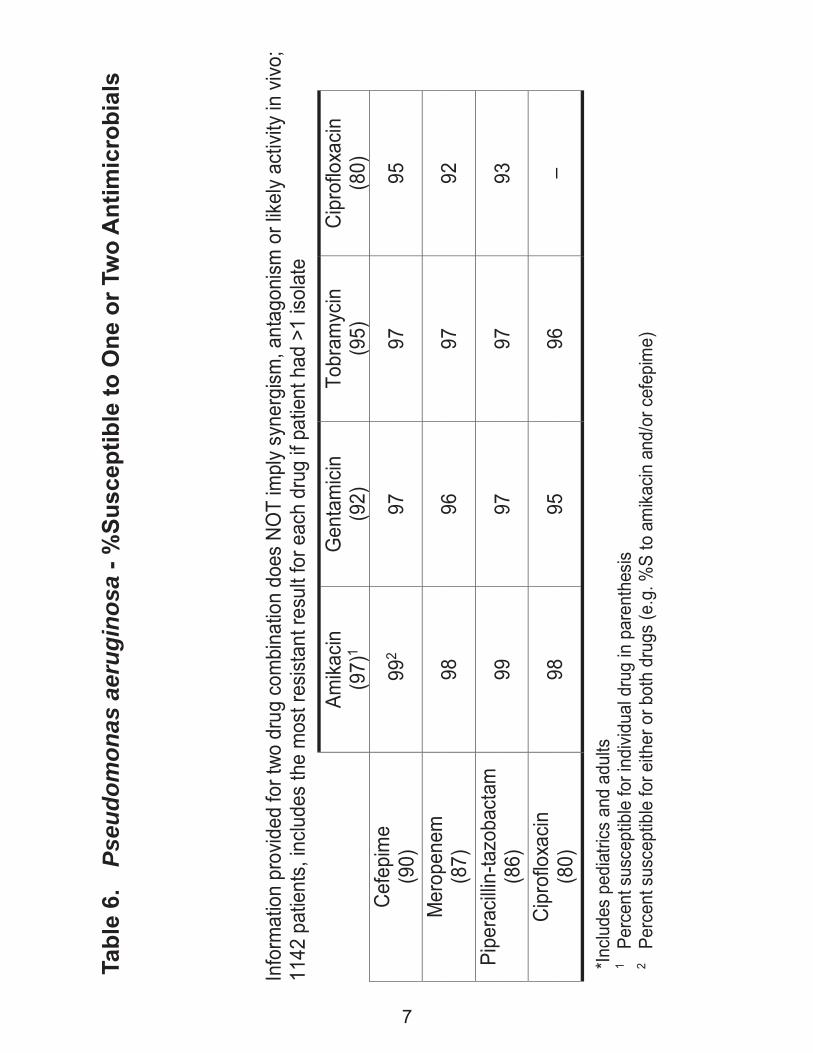
In
form
atio
n pr
ovid
ed fo
r two
dru
g co
mbi
natio
n do
es N
OT
impl
y sy
nerg
ism, a
ntag
onism
or l
ikely
activ
ity in
vivo
; 11
42 p
atie
nts,
inclu
des
the
mos
t res
istan
t res
ult f
or e
ach
drug
if p
atie
nt h
ad >
1 iso
late
Am
ikacin
(9
7)1
Gen
tam
icin
(92)
To
bram
ycin
(9
5)
Cipr
oflo
xacin
(8
0)
Cefe
pim
e 9
92 97
97
95
(9
0)
Mer
open
em
98
96
97
92
(87)
Pi
pera
cillin
-tazo
bact
am
99
97
97
93
(86)
Ci
prof
loxa
cin
98
95
96
– (8
0)
*Inclu
des
pedi
atric
s an
d ad
ults
1
Perc
ent s
usce
ptib
le fo
r ind
ividu
al d
rug
in p
aren
thes
is 2
Perc
ent s
usce
ptib
le fo
r eith
er o
r bot
h dr
ugs
(e.g
. %S
to a
mika
cin a
nd/o
r cef
epim
e)
Tabl
e 6.
Ps
eudo
mon
as a
erug
inos
a - %
Susc
eptib
le to
One
or T
wo
Ant
imic
robi
als
7
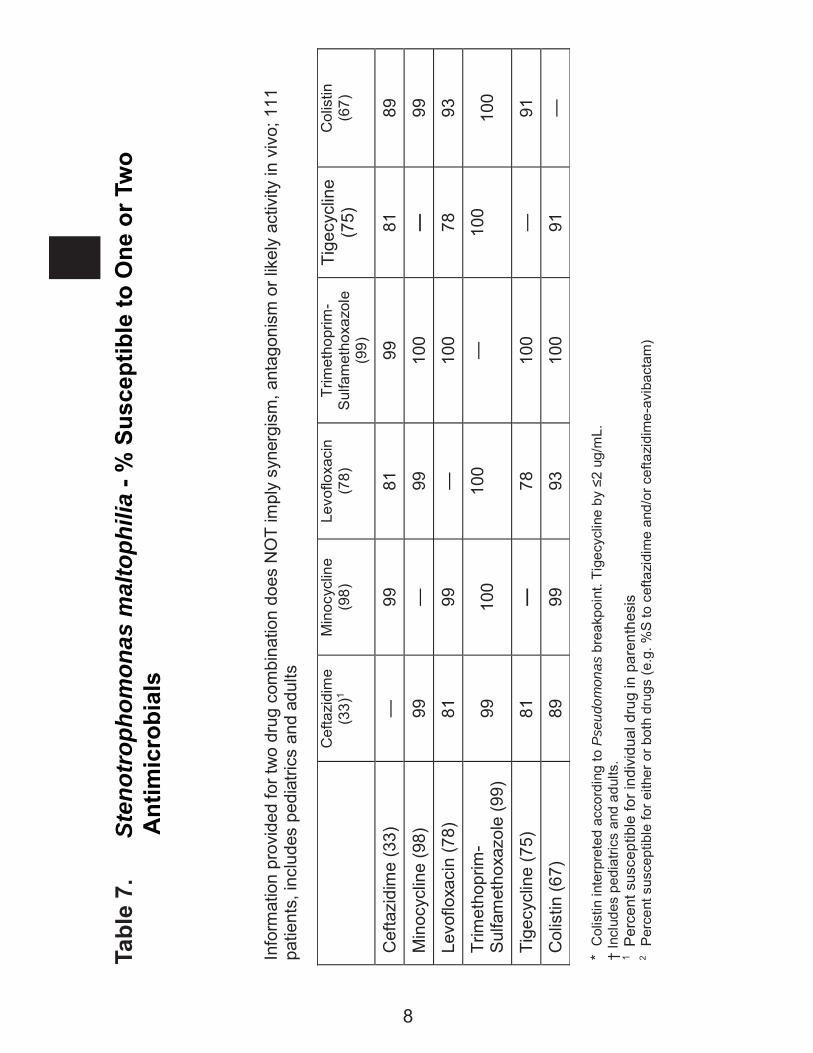
Tabl
e 7.
St
enot
roph
omon
as m
alto
phili
a - %
Sus
cept
ible
to O
ne o
r Tw
o
Ant
imic
robi
als
Info
rmat
ion
prov
ided
for t
wo
drug
com
bina
tion
does
NO
T im
ply
syne
rgis
m, a
ntag
onis
m o
r lik
ely
activ
ity in
viv
o; 1
11
patie
nts,
incl
udes
ped
iatri
cs a
nd a
dults
* C
olis
tin in
terp
rete
d ac
cord
ing
to P
seud
omon
as b
reak
poin
t. Ti
gecy
clin
e by
≤2
ug/m
L.
† In
clud
es p
edia
trics
and
adu
lts.
1 P
erce
nt s
usce
ptib
le fo
r ind
ivid
ual d
rug
in p
aren
thes
is
2 P
erce
nt s
usce
ptib
le fo
r eith
er o
r bot
h dr
ugs
(e.g
. %S
to c
efta
zidi
me
and/
or c
efta
zidi
me-
avib
acta
m)
Cef
tazi
dim
e (3
3)1
Min
ocyc
line
(98)
Le
voflo
xaci
n (7
8)
Trim
etho
prim
- S
ulfa
met
hoxa
zole
(9
9)
Tige
cycl
ine
(75)
C
olis
tin
(67)
Cef
tazi
dim
e (3
3)
—
99
81
99
81
89
Min
ocyc
line
(98)
99
—
99
10
0 —
99
Levo
floxa
cin
(78)
81
99
—
10
0 78
93
Trim
etho
prim
- S
ulfa
met
hoxa
zole
(99)
99
10
0 10
0 —
10
0 10
0
Tige
cycl
ine
(75)
81
—
78
10
0 —
91
Col
istin
(67)
89
99
93
10
0 91
—
8
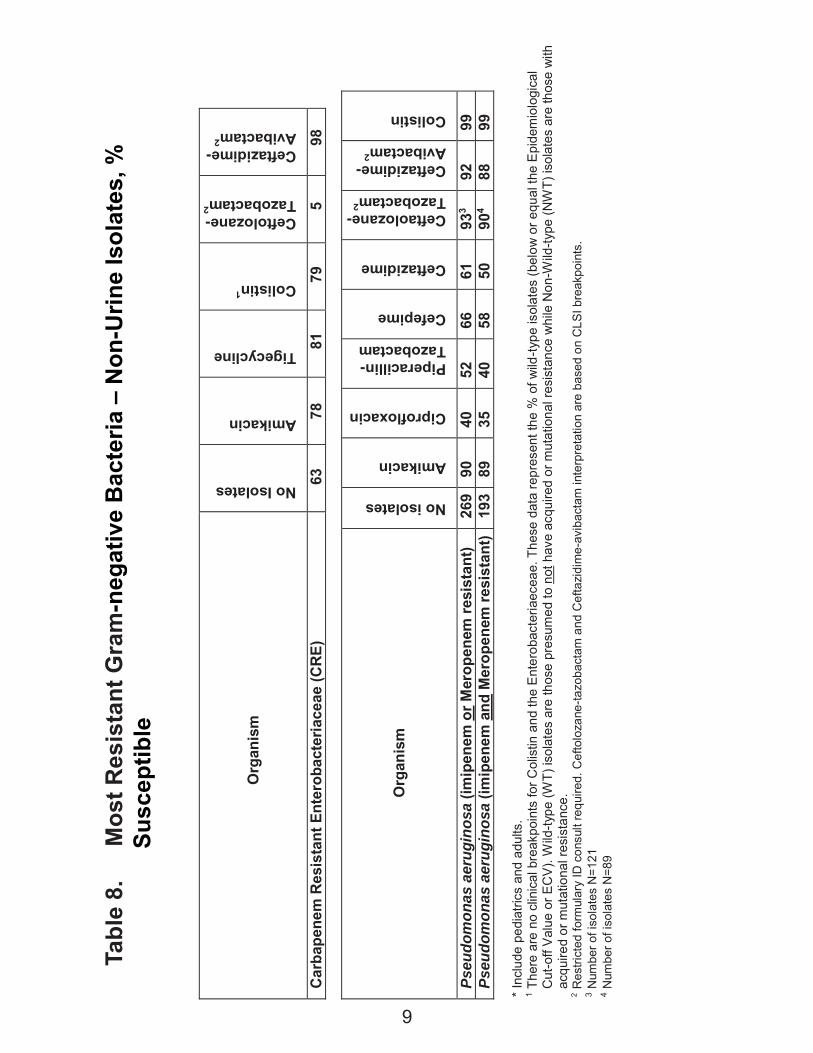
Tabl
e 8.
M
ost R
esis
tant
Gra
m-n
egat
ive
Bac
teria
– N
on-U
rine
Isol
ates
, %
Sus
cept
ible
Org
anis
m
No Isolates
Amikacin
Tigecycline
Colistin1
Ceftolozane- Tazobactam2
Ceftazidime- Avibactam2
Car
bape
nem
Res
ista
nt E
nter
obac
teria
ceae
(CR
E)
63
78
81
79
5 98
Org
anis
m
No isolates
Amikacin
Ciprofloxacin
Piperacillin- Tazobactam
Cefepime
Ceftazidime
Ceftaolozane- Tazobactam2
Ceftazidime- Avibactam2
Colistin
Pseu
dom
onas
aer
ugin
osa
(imip
enem
or M
erop
enem
resi
stan
t) 26
9 90
40
52
66
61
93
3 92
99
Ps
eudo
mon
as a
erug
inos
a (im
ipen
em a
nd M
erop
enem
resi
stan
t) 19
3 89
35
40
58
50
90
4 88
99
* I
nclu
de p
edia
trics
and
adu
lts.
1 The
re a
re n
o cl
inic
al b
reak
poin
ts fo
r Col
istin
and
the
Ent
erob
acte
riaec
eae.
The
se d
ata
repr
esen
t the
% o
f wild
-type
isol
ates
(bel
ow o
r equ
al th
e E
pide
mio
logi
cal
Cut
-off
Val
ue o
r EC
V). W
ild-ty
pe (W
T) is
olat
es a
re th
ose
pres
umed
to n
ot h
ave
acqu
ired
or m
utat
iona
l res
ista
nce
whi
le N
on-W
ild-ty
pe (N
WT)
isol
ates
are
thos
e w
ith
acqu
ired
or m
utat
iona
l res
ista
nce.
2
Res
trict
ed fo
rmul
ary
ID c
onsu
lt re
quire
d. C
efto
loza
ne-ta
zoba
ctam
and
Cef
tazi
dim
e-av
ibac
tam
inte
rpre
tatio
n ar
e ba
sed
on C
LSI b
reak
poin
ts.
3 Num
ber o
f iso
late
s N
=121
4 N
umbe
r of i
sola
tes
N=8
9
9
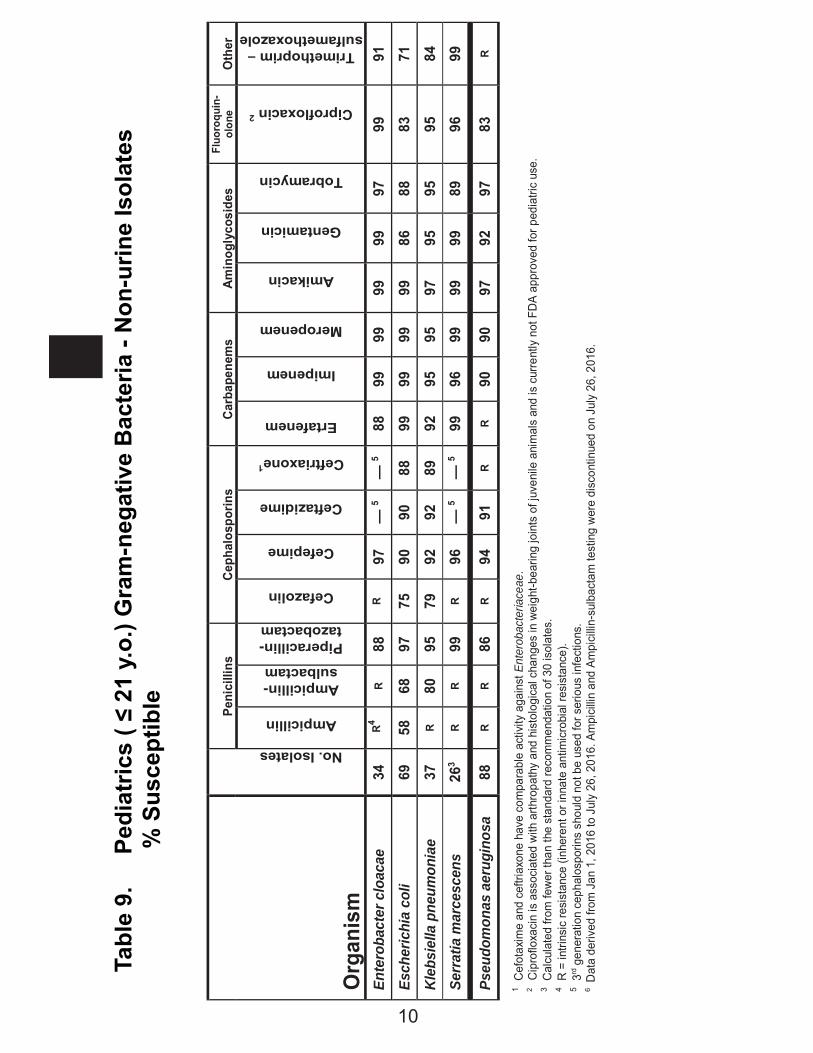
Tabl
e 9.
P
edia
tric
s ( ≤
21
y.o.
) Gra
m-n
egat
ive
Bac
teria
- N
on-u
rine
Isol
ates
% S
usce
ptib
le
Peni
cilli
ns
Ceph
alos
porin
s Ca
rbap
enem
s Am
inog
lyco
side
s Fl
uoro
quin
- ol
one
Oth
er
Org
anis
m
No. Isolates
Ampicillin
Ampicillin-sulbactam
Piperacillin-tazobactam
Cefazolin
Cefepime
Ceftazidime
Ceftriaxone1
Ertafenem
Imipenem
Meropenem
Amikacin
Gentamicin
Tobramycin
Ciprofloxacin 2
Trimethoprim – sulfamethoxazole
Ente
roba
cter
clo
acae
34
R
4 R
88
R 97
—
5 —
5 88
99
99
99
99
97
99
91
Esch
eric
hia
coli
69
58
68
97
75
90
90
88
99
99
99
99
86
88
83
71
Kleb
siel
la p
neum
onia
e 37
R
80
95
79
92
92
89
92
95
95
97
95
95
95
84
Serr
atia
mar
cesc
ens
263
R R
99
R 96
—
5 —
5 99
96
99
99
99
89
96
99
Pseu
dom
onas
aer
ugin
osa
88
R R
86
R 94
91
R
R 90
90
97
92
97
83
R
1 C
efot
axim
e an
d ce
ftria
xone
hav
e co
mpa
rabl
e ac
tivity
aga
inst
Ent
erob
acte
riace
ae.
2 C
ipro
floxa
cin
is a
ssoc
iate
d w
ith a
rthro
path
y an
d hi
stol
ogic
al c
hang
es in
wei
ght-b
earin
g jo
ints
of j
uven
ile a
nim
als
and
is c
urre
ntly
not
FD
A ap
prov
ed fo
r ped
iatri
c us
e.
3 C
alcu
late
d fro
m fe
wer
than
the
stan
dard
reco
mm
enda
tion
of 3
0 is
olat
es.
4 R
= in
trins
ic re
sist
ance
(inh
eren
t or i
nnat
e an
timic
robi
al re
sist
ance
). 5
3rd g
ener
atio
n ce
phal
ospo
rins
shou
ld n
ot b
e us
ed fo
r ser
ious
infe
ctio
ns.
6 D
ata
deriv
ed fr
om J
an 1
, 201
6 to
Jul
y 26
, 201
6. A
mpi
cillin
and
Am
pici
llin-s
ulba
ctam
test
ing
wer
e di
scon
tinue
d on
Jul
y 26
, 201
6.
10
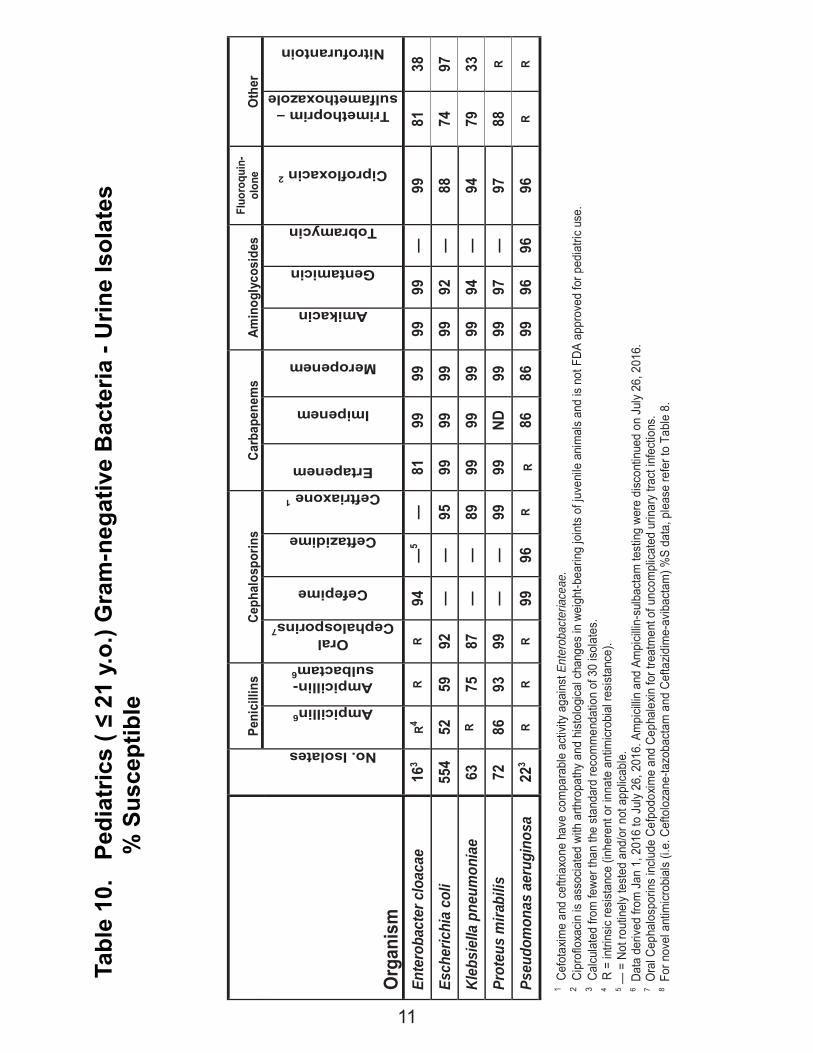
Tabl
e 10
. P
edia
tric
s ( ≤
21
y.o.
) Gra
m-n
egat
ive
Bac
teria
- U
rine
Isol
ates
% S
usce
ptib
le
Org
anis
m
Pe
nici
llins
Ceph
alos
porin
s Ca
rbap
enem
s Am
inog
lyco
side
s Fl
uoro
quin
- ol
one
Oth
er
No. Isolates
Ampicillin6
Ampicillin-sulbactam6
Oral Cephalosporins7
Cefepime
Ceftazidime
Ceftriaxone 1
Ertapenem
Imipenem
Meropenem
Amikacin
Gentamicin
Tobramycin
Ciprofloxacin 2
Trimethoprim – sulfamethoxazole
Nitrofurantoin
Ente
roba
cter
clo
acae
16
3 R4
R R
94
—5
—
81
99
99
99
99
—
99
81
38
Esch
eric
hia
coli
554
52
59
92
—
—
95
99
99
99
99
92
—
88
74
97
Kleb
siel
la p
neum
onia
e 63
R
75
87
—
—
89
99
99
99
99
94
—
94
79
33
Prot
eus
mira
bilis
72
86
93
99
—
—
99
99
ND
99
99
97
—
97
88
R
Pseu
dom
onas
aer
ugin
osa
22
3 R
R R
99
96
R R
86
86
99
96
96
96
R R
1 Cef
otax
ime
and
ceftr
iaxo
ne h
ave
com
para
ble
activ
ity a
gain
st E
nter
obac
teria
ceae
.
2 Cip
roflo
xacin
is a
ssoc
iate
d wi
th a
rthro
path
y an
d hi
stol
ogica
l cha
nges
in w
eigh
t-bea
ring
join
ts o
f juv
enile
ani
mal
s an
d is
not F
DA a
ppro
ved
for p
edia
tric
use.
3 C
alcu
late
d fro
m fe
wer t
han
the
stan
dard
reco
mm
enda
tion
of 3
0 iso
late
s.
4 R
= in
trins
ic re
sista
nce
(inhe
rent
or i
nnat
e an
timicr
obia
l res
istan
ce).
5 —
= N
ot ro
utin
ely
test
ed a
nd/o
r not
app
licab
le.
6 Dat
a de
rived
from
Jan
1, 2
016
to J
uly
26, 2
016.
Am
picil
lin a
nd A
mpi
cillin
-sul
bact
am te
stin
g we
re d
iscon
tinue
d on
Jul
y 26
, 201
6.
7 Ora
l Cep
halo
spor
ins
inclu
de C
efpo
doxim
e an
d Ce
phal
exin
for t
reat
men
t of u
ncom
plica
ted
urin
ary
tract
infe
ctio
ns.
8 For
nov
el a
ntim
icrob
ials
(i.e.
Cef
tolo
zane
-tazo
bact
am a
nd C
efta
zidim
e-av
ibac
tam
) %S
data
, ple
ase
refe
r to
Tabl
e 8.
11
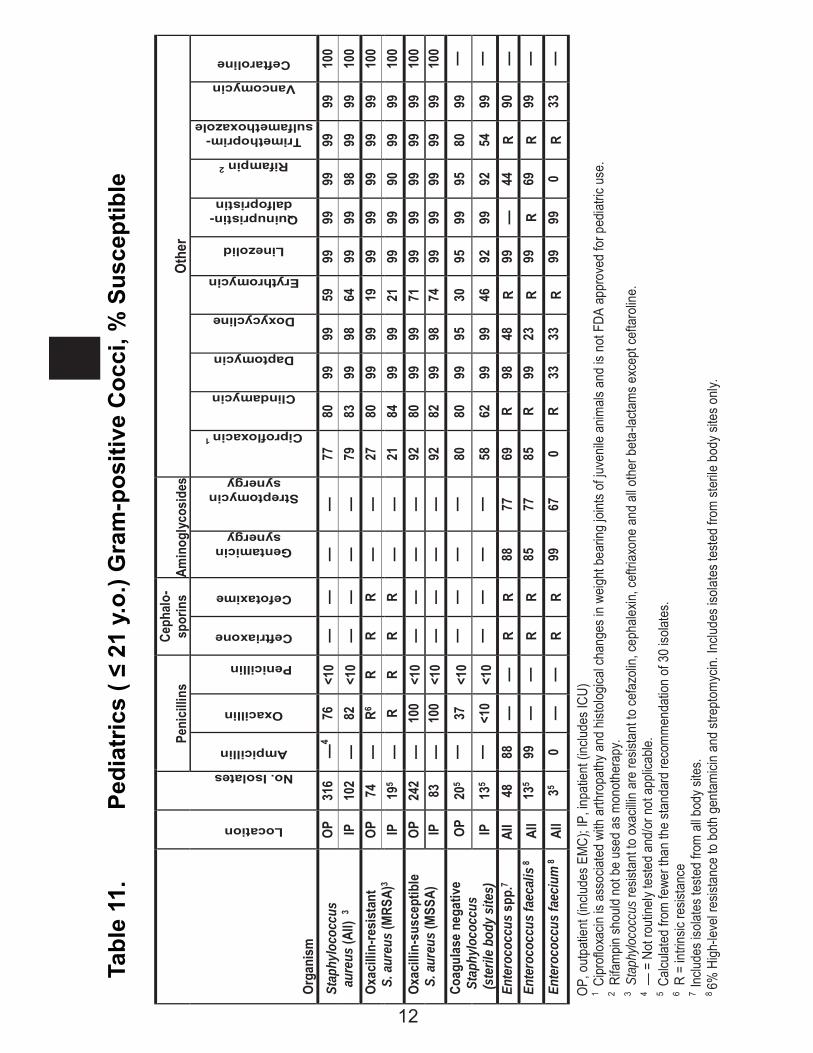
Tabl
e 11
. Pe
diat
rics
( ≤ 2
1 y.
o.) G
ram
-pos
itive
Coc
ci, %
Sus
cept
ible
Pe
nici
llins
Ce
phal
o-sp
orin
s Am
inog
lyco
side
sOt
her
Orga
nism
Location
No. Isolates
Ampicillin
Oxacillin
Penicillin
Ceftriaxone
Cefotaxime
Gentamicin synergy
Streptomycin synergy
Ciprofloxacin 1
Clindamycin
Daptomycin
Doxycycline
Erythromycin
Linezolid
Quinupristin-dalfopristin
Rifampin 2
Trimethoprim-sulfamethoxazole
Vancomycin
Ceftaroline
Stap
hylo
cocc
us
aure
us (A
ll) 3
OP
31
6 —
4 76
<1
0 —
—
—
—
77
80
99
99
59
99
99
99
99
99
10
0 IP
10
2 —
82
<1
0 —
—
—
—
79
83
99
98
64
99
99
98
99
99
10
0 Ox
acill
in-re
sist
ant
S. a
ureu
s (M
RSA)
3 OP
74
—
R6
R R
R —
—
27
80
99
99
19
99
99
99
99
99
10
0 IP
19
5 —
R
R R
R —
—
21
84
99
99
21
99
99
90
99
99
10
0 Ox
acill
in-s
usce
ptib
le
S. a
ureu
s (M
SSA)
OP
24
2 —
10
0 <1
0 —
—
—
—
92
80
99
99
71
99
99
99
99
99
10
0 IP
83
—
10
0 <1
0 —
—
—
—
92
82
99
98
74
99
99
99
99
99
10
0 Co
agul
ase
nega
tive
S
taph
yloc
occu
s
(st
erile
bod
y si
tes)
OP
205
—
37
<10
—
—
—
—
80
80
99
95
30
95
99
95
80
99
—
IP
135
—
<10
<10
—
—
—
—
58
62
99
99
46
92
99
92
54
99
—
Ente
roco
ccus
spp
.7 Al
l 48
88
—
—
R
R 88
77
69
R
98
48
R 99
—
44
R
90
—
Ente
roco
ccus
faec
alis
8 Al
l 13
5 99
—
—
R
R 85
77
85
R
99
23
R 99
R
69
R 99
—
En
tero
cocc
us fa
eciu
m 8
All
35 0
—
—
R R
99
67
0 R
33
33
R 99
99
0
R 33
—
OP
, out
patie
nt (i
nclu
des E
MC)
; IP,
inpa
tient
(inc
lude
s IC
U)
1 C
iprof
loxa
cin is
ass
ociat
ed w
ith a
rthro
path
y and
hist
olog
ical c
hang
es in
wei
ght b
earin
g jo
ints
of ju
venil
e an
imals
and
is n
ot F
DA a
ppro
ved
for p
edia
tric
use.
2 R
ifam
pin sh
ould
not
be
used
as m
onot
hera
py.
3 Sta
phylo
cocc
us re
sista
nt to
oxa
cillin
are
resis
tant
to c
efaz
olin,
ceph
alexin
, cef
triax
one
and
all o
ther
bet
a-lac
tam
s exc
ept c
efta
rolin
e.
4 — =
Not
rout
inely
teste
d an
d/or
not
app
licab
le.
5 C
alcula
ted
from
fewe
r tha
n th
e st
anda
rd re
com
men
datio
n of
30
isolat
es.
6 R =
intri
nsic
resis
tanc
e 7
Inclu
des i
solat
es te
sted
from
all b
ody s
ites.
8 6%
High
-leve
l res
istan
ce to
bot
h ge
ntam
icin
and
stre
ptom
ycin.
Inclu
des i
sola
tes t
este
d fro
m st
erile
bod
y site
s onl
y.
12
Tabl
e 11
. Pe
diat
rics
( ≤ 2
1 y.
o.) G
ram
-pos
itive
Coc
ci, %
Sus
cept
ible
(c
ont)
Peni
cilli
ns
Ceph
alos
porin
s Ot
her
Orga
nism
No. Isolates
Amoxicillin
Penicillin
Cefotaxime
Ceftriaxone
Clindamycin
Doxycycline
Erythromycin
Trimethoprim – sulfamethoxazole
Vancomycin
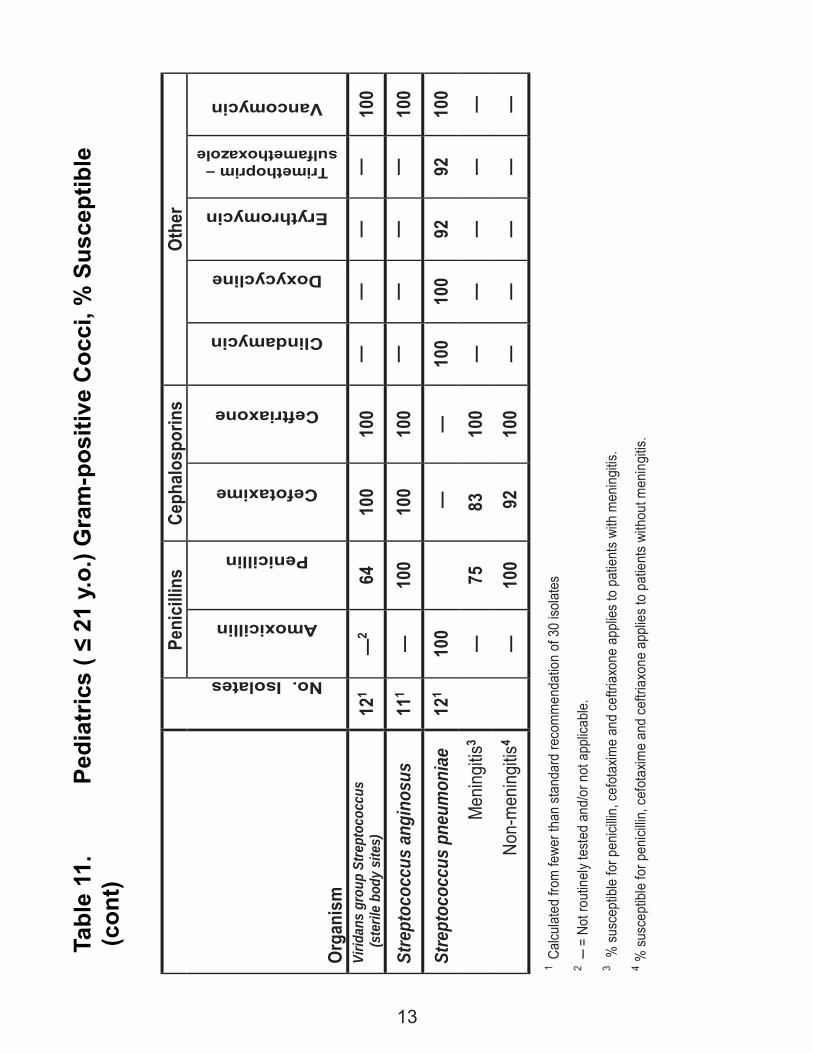
Virid
ans
grou
p St
rept
ococ
cus
(s
teril
e bo
dy s
ites)
12
1 —
2 64
10
0 10
0 —
—
—
—
10
0
Stre
ptoc
occu
s an
gino
sus
111
—
100
100
100
—
—
—
—
100
Stre
ptoc
occu
s pn
eum
onia
e 12
1 10
0
—
—
100
100
92
92
100
Men
ingi
tis3
—
75
83
10
0 —
—
—
—
—
No
n-m
enin
gitis
4
—
100
92
100
—
—
—
—
—
1 Ca
lcula
ted
from
fewe
r tha
n st
anda
rd re
com
men
datio
n of
30
isola
tes
2 ─ =
Not
rout
inel
y tes
ted
and/
or n
ot a
pplic
able
. 3 %
sus
cept
ible
for p
enici
llin, c
efot
axim
e an
d ce
ftria
xone
app
lies
to p
atie
nts
with
men
ingi
tis.
4 % s
usce
ptib
le fo
r pen
icillin
, cef
otax
ime
and
ceftr
iaxo
ne a
pplie
s to
pat
ient
s wi
thou
t men
ingi
tis.
13
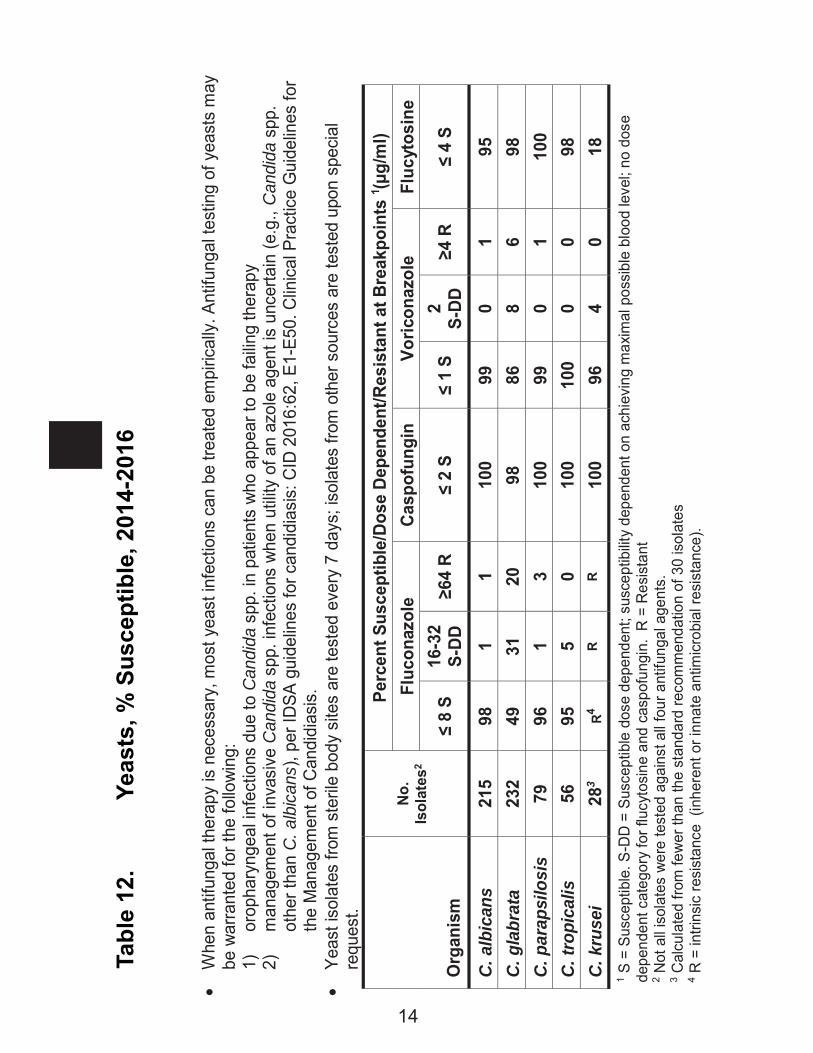
Whe
n an
tifun
gal t
hera
py is
nec
essa
ry, m
ost y
east
infe
ctio
ns c
an b
e tre
ated
em
piric
ally
. Ant
ifung
al te
stin
g of
yea
sts
may
be
war
rant
ed fo
r the
follo
win
g:
1)
orop
hary
ngea
l inf
ectio
ns d
ue to
Can
dida
spp
. in
patie
nts
who
app
ear t
o be
failin
g th
erap
y
2)
man
agem
ent o
f inv
asiv
e C
andi
da s
pp. i
nfec
tions
whe
n ut
ility
of a
n az
ole
agen
t is
unce
rtain
(e.g
., C
andi
da s
pp.
othe
r tha
n C
. alb
ican
s), p
er ID
SA g
uide
lines
for c
andi
dias
is: C
ID 2
016:
62, E
1-E5
0. C
linic
al P
ract
ice
Gui
delin
es fo
r th
e M
anag
emen
t of C
andi
dias
is.
Ye
ast i
sola
tes
from
ste
rile
body
site
s ar
e te
sted
eve
ry 7
day
s; is
olat
es fr
om o
ther
sou
rces
are
test
ed u
pon
spec
ial
requ
est.
O
rgan
ism
No
. Is
olat
es2
Perc
ent S
usce
ptib
le/D
ose
Depe
nden
t/Res
ista
nt a
t Bre
akpo
ints
1 (μg/
ml)
Fluc
onaz
ole
Casp
ofun
gin
Voric
onaz
ole
Fluc
ytos
ine
≤ 8
S 16
-32
S-DD
≥6
4 R
≤ 2
S ≤
1 S
2
S-DD
≥4
R
≤ 4
S
C. a
lbic
ans
215
98
1 1
100
99
0 1
95
C. g
labr
ata
232
49
31
20
98
86
8 6
98
C. p
arap
silo
sis
79
96
1 3
100
99
0 1
100
C. tr
opic
alis
56
95
5
0 10
0 10
0 0
0 98
C.
kru
sei
283
R4 R
R 10
0 96
4
0 18
1 S
= S
usce
ptib
le. S
-DD
= S
usce
ptib
le d
ose
depe
nden
t; su
scep
tibilit
y de
pend
ent o
n ac
hiev
ing
max
imal
pos
sibl
e bl
ood
leve
l; no
dos
e de
pend
ent c
ateg
ory
for f
lucy
tosi
ne a
nd c
aspo
fung
in.
R =
Res
ista
nt
2 Not
all
isol
ates
wer
e te
sted
aga
inst
all
four
ant
ifung
al a
gent
s.
3 Cal
cula
ted
from
few
er th
an th
e st
anda
rd re
com
men
datio
n of
30
isol
ates
4 R
= in
trins
ic re
sist
ance
(in
here
nt o
r inn
ate
antim
icro
bial
resi
stan
ce).
Tabl
e 12
. Ye
asts
, % S
usce
ptib
le, 2
014-
2016
14
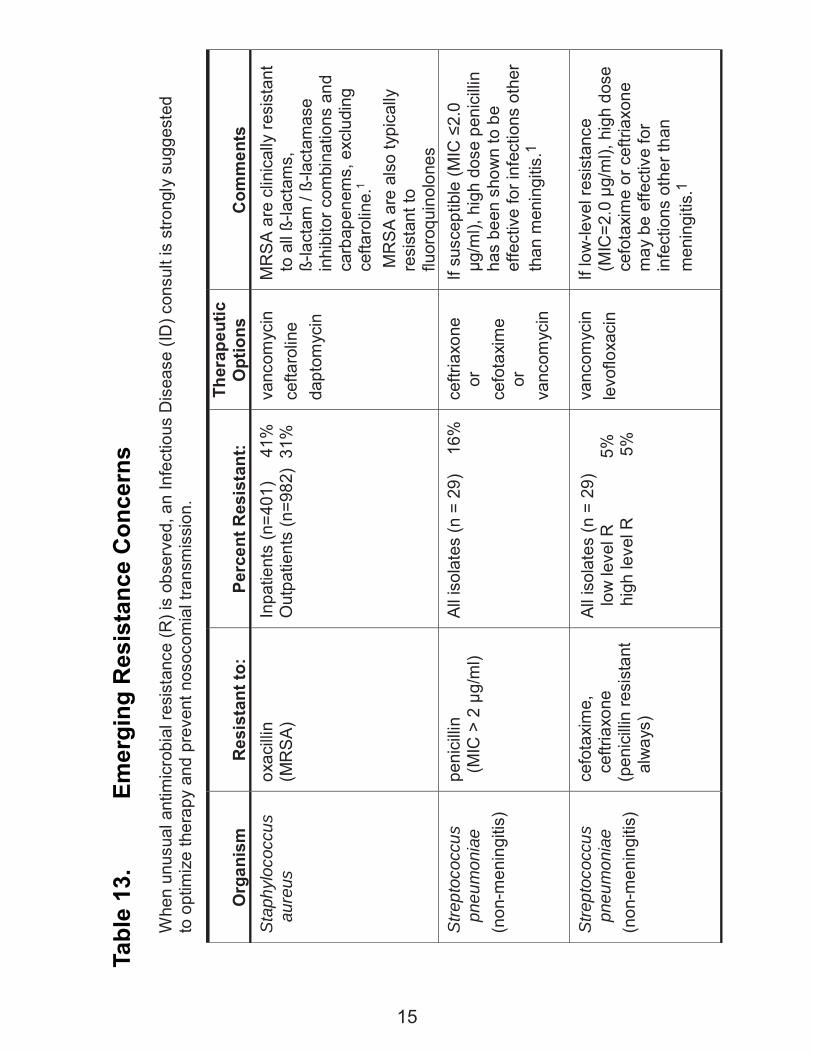
Tabl
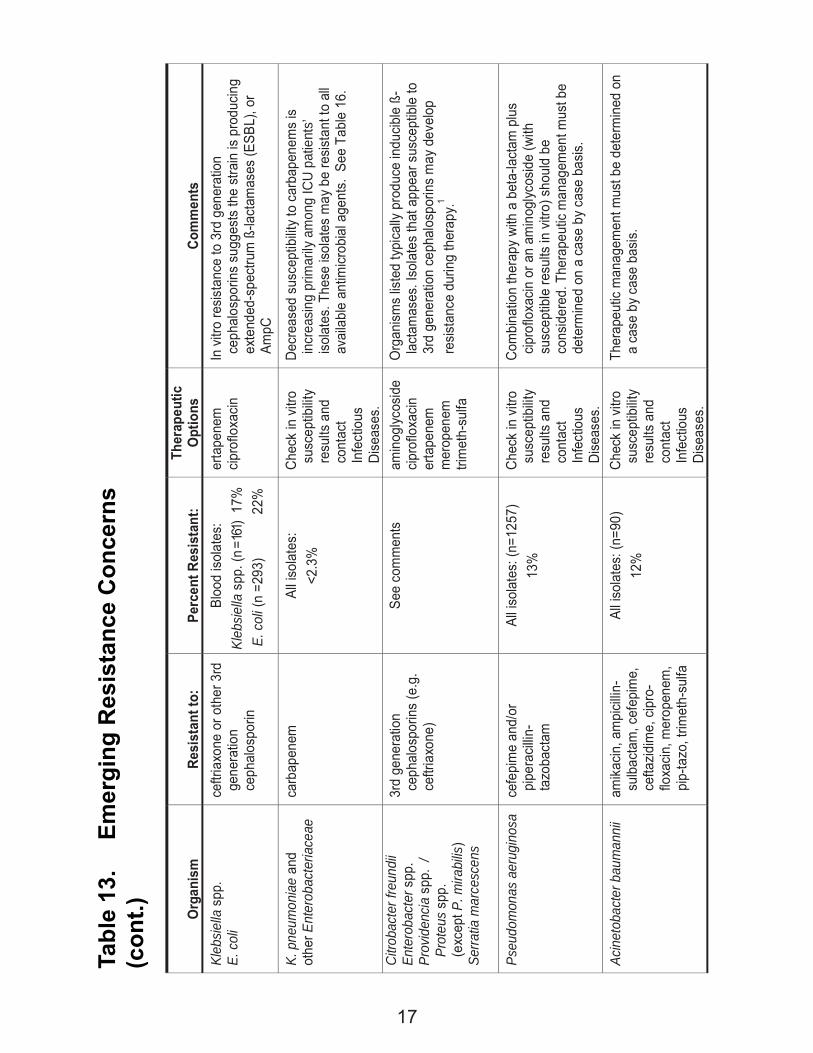
e 13
. Em
ergi
ng R
esis
tanc
e C
once
rns
Whe
n un
usua
l ant
imic
robi
al re
sist
ance
(R) i
s ob
serv
ed, a
n In
fect
ious
Dis
ease
(ID
) con
sult
is s
trong
ly s
ugge
sted
to
opt
imiz
e th
erap
y an
d pr
even
t nos
ocom
ial t
rans
mis
sion
.
O
rgan
ism
Res
ista
nt to
:
Perc
ent R
esis
tant
: Th
erap
eutic
O
ptio
ns
C
omm
ents
St
aphy
loco
ccus
au
reus
ox
acilli
n (M
RS
A)
Inpa
tient
s (n
=401
)
41%
O
utpa
tient
s (n
=982
) 31
%
vanc
omyc
in
cefta
rolin
e
dapt
omyc
in
MR
SA
are
clin
ical
ly re
sist
ant
to a
ll ß-
lact
ams,
ß-
lact
am /
ß-la
ctam
ase
inhi
bito
r com
bina
tions
and
ca
rbap
enem
s, e
xclu
ding
ce
ftaro
line.
1
MR
SA
are
also
typi
cally
re
sist
ant t
o flu
oroq
uino
lone
s St
rept
ococ
cus
pneu
mon
iae
(non
-men
ingi
tis)
peni
cilli
n (M
IC >
2 μ
g/m
l)
All i
sola
tes
(n =
29)
1
6%
ceftr
iaxo
ne
or
cefo
taxi
me
or
vanc
omyc
in
If su
scep
tible
(MIC
≤2.
0 μg
/ml),
hig
h do
se p
enic
illin
has
been
sho
wn
to b
e ef
fect
ive
for i
nfec
tions
oth
er
than
men
ingi
tis.1
St
rept
ococ
cus
pneu
mon
iae
(non
-men
ingi
tis)
cefo
taxi
me,
ce
ftria
xone
(p
enic
illin
resi
stan
t al
way
s)
All i
sola
tes
(n =
29)
lo
w le
vel R
5%
hi
gh le
vel R
5%
vanc
omyc
in
levo
floxa
cin
If lo
w-le
vel r
esis
tanc
e (M
IC=2
.0 μ
g/m
l), h
igh
dose
ce
fota
xim
e or
cef
triax
one
may
be
effe
ctiv
e fo
r in
fect
ions
oth
er th
an
men
ingi
tis.1
15
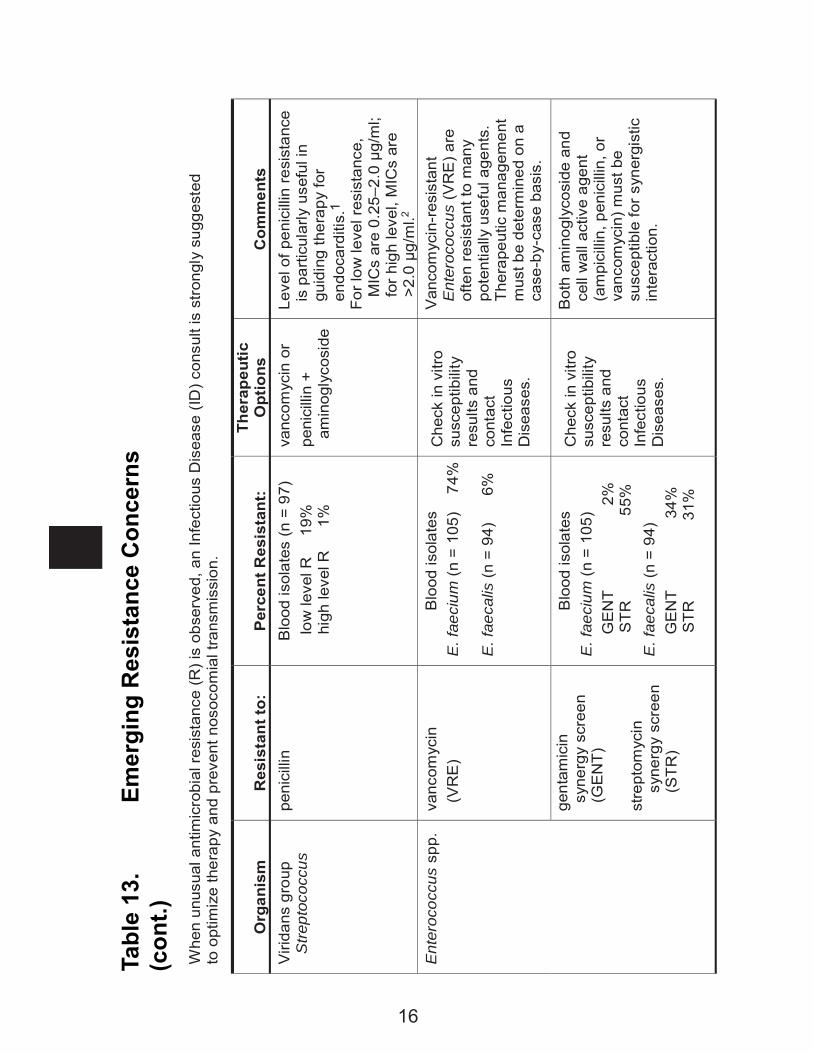
Tabl
e 13
. Em
ergi
ng R
esis
tanc
e C
once
rns
(con
t.)W
hen
unus
ual a
ntim
icro
bial
resi
stan
ce (R
) is
obse
rved
, an
Infe
ctio
us D
isea
se (I
D) c
onsu
lt is
stro
ngly
sug
gest
ed
to o
ptim
ize
ther
apy
and
prev
ent n
osoc
omia
l tra
nsm
issi
on.
O
rgan
ism
Res
ista
nt to
:
Per
cent
Res
ista
nt:
Ther
apeu
tic
Opt
ions
Com
men
ts
Viri
dans
gro
up
Stre
ptoc
occu
s pe
nici
llin
Blo
od is
olat
es (n
= 9
7)
l
ow le
vel R
19
%
h
igh
leve
l R
1%
vanc
omyc
in o
r pe
nici
llin
+ am
inog
lyco
side
Leve
l of p
enic
illin
resi
stan
ce
is p
artic
ular
ly u
sefu
l in
guid
ing
ther
apy
for
endo
card
itis.
1 Fo
r low
leve
l res
ista
nce,
M
ICs
are
0.25
–2.0
μg/
ml;
for h
igh
leve
l, M
ICs
are
>2.0
μg/
ml.2
Ent
eroc
occu
s sp
p.
va
ncom
ycin
(
VR
E)
Blo
od is
olat
es
E. f
aeci
um (n
= 1
05)
74%
E
. fae
calis
(n =
94)
6%
Che
ck in
vitr
o su
scep
tibili
ty
resu
lts a
nd
cont
act
Infe
ctio
us
Dis
ease
s.
Van
com
ycin
-res
ista
nt
Ent
eroc
occu
s (V
RE
) are
of
ten
resi
stan
t to
man
y po
tent
ially
use
ful a
gent
s.
Ther
apeu
tic m
anag
emen
t m
ust b
e de
term
ined
on
a ca
se-b
y-ca
se b
asis
.
gent
amic
in
syne
rgy
scre
en
(GE
NT)
st
rept
omyc
in
syne
rgy
scre
en
(STR
)
Blo
od is
olat
es
E. f
aeci
um (n
= 1
05)
G
EN
T
2%
STR
55%
E
. fae
calis
(n =
94)
GE
NT
34
%
S
TR
31
%
Che
ck in
vitr
o su
scep
tibili
ty
resu
lts a
nd
cont
act
Infe
ctio
us
Dis
ease
s.
Bot
h am
inog
lyco
side
and
ce
ll w
all a
ctiv
e ag
ent
(am
pici
llin,
pen
icill
in, o
r va
ncom
ycin
) mus
t be
susc
eptib
le fo
r syn
ergi
stic
in
tera
ctio
n.
16
Tabl
e 13
. Em
ergi
ng R
esis
tanc
e C
once
rns
(con
t.)
O
rgan
ism
Resi
stan
t to:
Perc
ent R
esis
tant
: Th
erap
eutic
O
ptio
ns
Co
mm
ents
Kl
ebsie
lla s
pp.
E. c
oli
ceftr
iaxo
ne o
r oth
er 3
rd
gene
ratio
n ce
phal
ospo
rin
Bloo
d is
olat
es:
Kleb
siella
spp
. (n =
161)
17%
E.
col
i (n
=293
)
22%
erta
pene
m
cipro
floxa
cin
In v
itro
resis
tanc
e to
3rd
gen
erat
ion
ceph
alos
porin
s su
gges
ts th
e st
rain
is p
rodu
cing
exte
nded
-spe
ctru
m ß
-lact
amas
es (E
SBL)
, or
AmpC
K. p
neum
onia
e an
d ot
her E
nter
obac
teria
ceae
carb
apen
em
All is
olat
es:
<2.3
%
Chec
k in
vitr
o su
scep
tibilit
y re
sults
and
co
ntac
t In
fect
ious
Di
seas
es.
Decr
ease
d su
scep
tibilit
y to
car
bape
nem
s is
incr
easin
g pr
imar
ily a
mon
g IC
U pa
tient
s’ iso
late
s. T
hese
isol
ates
may
be
resis
tant
to a
ll av
aila
ble
antim
icrob
ial a
gent
s. S
ee T
able
16.
Citro
bact
er fr
eund
ii En
tero
bact
er s
pp.
Prov
iden
cia
spp.
/
Prot
eus
spp.
(e
xcep
t P. m
irabi
lis)
Serra
tia m
arce
scen
s
3rd
gene
ratio
n ce
phal
ospo
rins
(e.g
. ce
ftria
xone
)
See
com
men
ts
amin
oglyc
osid
e cip
roflo
xacin
er
tape
nem
m
erop
enem
tri
met
h-su
lfa
Org
anism
s lis
ted
typi
cally
pro
duce
indu
cible
ß-
lact
amas
es. I
sola
tes
that
app
ear s
usce
ptib
le to
3r
d ge
nera
tion
ceph
alos
porin
s m
ay d
evel
op
resis
tanc
e du
ring
ther
apy.
1
Pseu
dom
onas
aer
ugin
osa
cefe
pim
e an
d/or
pi
pera
cillin
-ta
zoba
ctam
All is
olat
es: (
n=12
57)
13%
Ch
eck
in v
itro
susc
eptib
ility
resu
lts a
nd
cont
act
Infe
ctio
us
Dise
ases
.
Com
bina
tion
ther
apy
with
a b
eta-
lact
am p
lus
cipro
floxa
cin o
r an
amin
oglyc
osid
e (w
ith
susc
eptib
le re
sults
in v
itro)
sho
uld
be
cons
ider
ed. T
hera
peut
ic m
anag
emen
t mus
t be
dete
rmin
ed o
n a
case
by
case
bas
is.
Acin
etob
acte
r bau
man
nii
amik
acin
, am
picil
lin-
sulb
acta
m, c
efep
ime,
ce
ftazid
ime,
cip
ro-
floxa
cin,
mer
open
em,
pip-
tazo
, trim
eth-
sulfa
All is
olat
es: (
n=90
) 12
%
Chec
k in
vitr
o su
scep
tibilit
y re
sults
and
co
ntac
t In
fect
ious
Di
seas
es.
Ther
apeu
tic m
anag
emen
t mus
t be
dete
rmin
ed o
n a
case
by
case
bas
is.
17
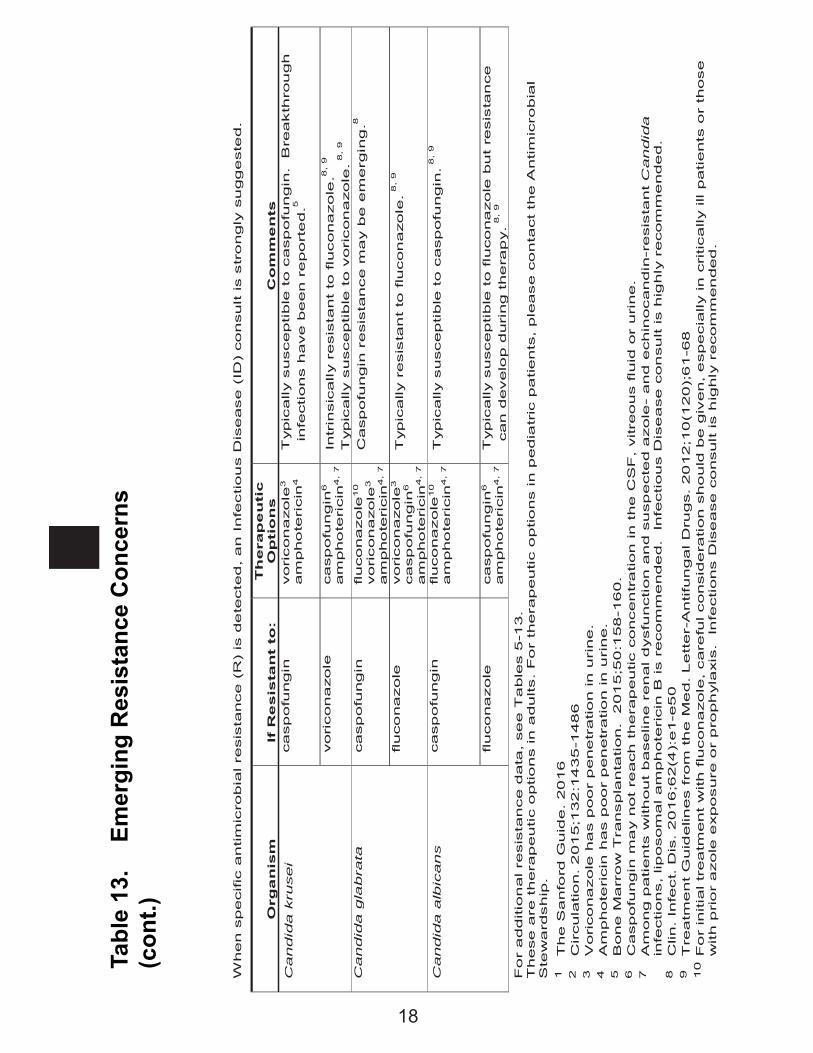
Tabl
e 13
. Em
ergi
ng R
esis
tanc
e C
once
rns
(con
t.)
When s
pecific
antim
icro
bia
l re
sis
tance (
R)
is d
ete
cte
d, a
n I
nfe
ctiou
s D
ise
ase
(ID
) co
nsult is s
tro
ngly
su
gg
este
d.
O
rga
nis
m
If
Re
sis
tan
t to
: T
hera
pe
uti
c
Op
tio
ns
Co
mm
en
ts
Candid
a k
rusei
casp
ofu
ngin
voricon
azole
3
am
pho
teri
cin
4
Typic
ally s
usceptible
to c
asp
ofu
ngin
. B
reakth
rou
gh
in
fections h
ave b
een r
epo
rte
d.5
voricon
azole
casp
ofu
ngin
6
am
pho
teri
cin
4,
7
Intr
insic
ally r
esis
tant
to flu
cona
zole
.8,
9
Typic
ally s
usceptible
to v
oricon
azole
. 8, 9
Candid
a g
labra
ta
casp
ofu
ngin
fluco
na
zole
10
voricon
azole
3
am
pho
teri
cin
4,
7
Casp
ofu
ngin
resis
tance m
ay b
e e
merg
ing
.8
fluco
na
zole
voricon
azole
3
casp
ofu
ngin
6
am
pho
teri
cin
4,
7
Typic
ally r
esis
tan
t to
flu
con
azole
. 8,
9
Candid
a a
lbic
an
s
casp
ofu
ngin
fluco
na
zole
10
am
pho
teri
cin
4,
7
Typic
ally s
usceptible
to c
asp
ofu
ngin
. 8,
9
fluco
na
zole
casp
ofu
ngin
6
am
pho
teri
cin
4,
7
Typic
ally s
usceptible
to flu
co
na
zole
but
resis
tan
ce
can d
evelo
p d
uri
ng t
he
rap
y. 8
, 9
Fo
r a
dditio
nal re
sis
tance d
ata
, se
e T
able
s 5
-13.
These a
re t
hera
peutic o
ptio
ns in
adults.
Fo
r th
era
peutic o
ptio
ns in p
edia
tric
pa
tients
, ple
ase c
onta
ct th
e A
ntim
icro
bia
l S
tew
ard
ship
. 1
T
he S
anfo
rd G
uid
e.
20
16
2
Circula
tio
n. 2
01
5;1
32
:14
35
-148
6
3
Vorico
na
zole
ha
s p
oo
r p
ene
tratio
n in u
rine
. 4
A
mphote
ricin
has p
oo
r p
en
etr
atio
n in
uri
ne.
5
Bone M
arr
ow
Tra
nspla
nta
tion.
201
5;5
0:1
58
-16
0.
6
Casp
ofu
ngin
ma
y n
ot
reach
th
era
peutic c
oncen
tra
tion
in t
he
CS
F,
vitre
ous flu
id o
r uri
ne.
7
Am
ong p
atients
with
out
baseline r
en
al d
ysfu
nction a
nd s
usp
ecte
d a
zole
- and
echin
ocandin
-resis
tant C
andid
a
infe
ctions, lip
osom
al am
ph
ote
ricin
B is r
ecom
me
nde
d.
Infe
ctious D
ise
ase c
on
sult is h
ighly
recom
me
nde
d.
8
Clin.
Infe
ct. D
is.
20
16
;62(4
):e1-e
50
9
T
reatm
ent G
uid
elin
es f
rom
th
e M
ed. L
etter-
Antifu
ngal D
rugs.
20
12;1
0(1
20);
61
-68
1
0 F
or
initia
l tr
ea
tment
with f
lucon
azole
, care
ful consid
era
tion s
ho
uld
be
giv
en,
especia
lly in
critically ill p
atients
or
those
w
ith p
rio
r a
zole
exposure
or
pro
ph
yla
xis
. In
fections D
ise
ase
co
nsult is h
ighly
recom
men
ded
.
18
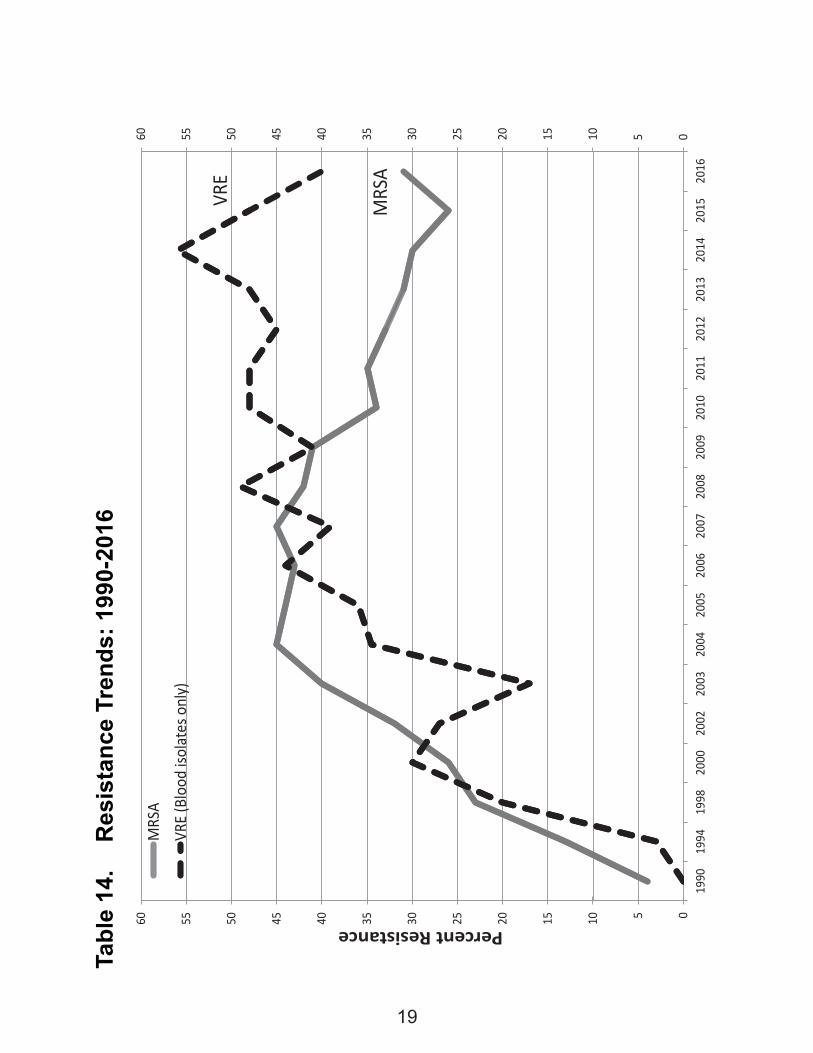
Tabl
e 14
. R
esis
tanc
e Tr
ends
: 199
0-20
16
051015202530354045505560
051015202530354045505560
1990
1994
1998
2000
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
Percent Resistance
MRS
A
VRE
(Blo
od is
olat
es o
nly)
VRE
MRS
A
19
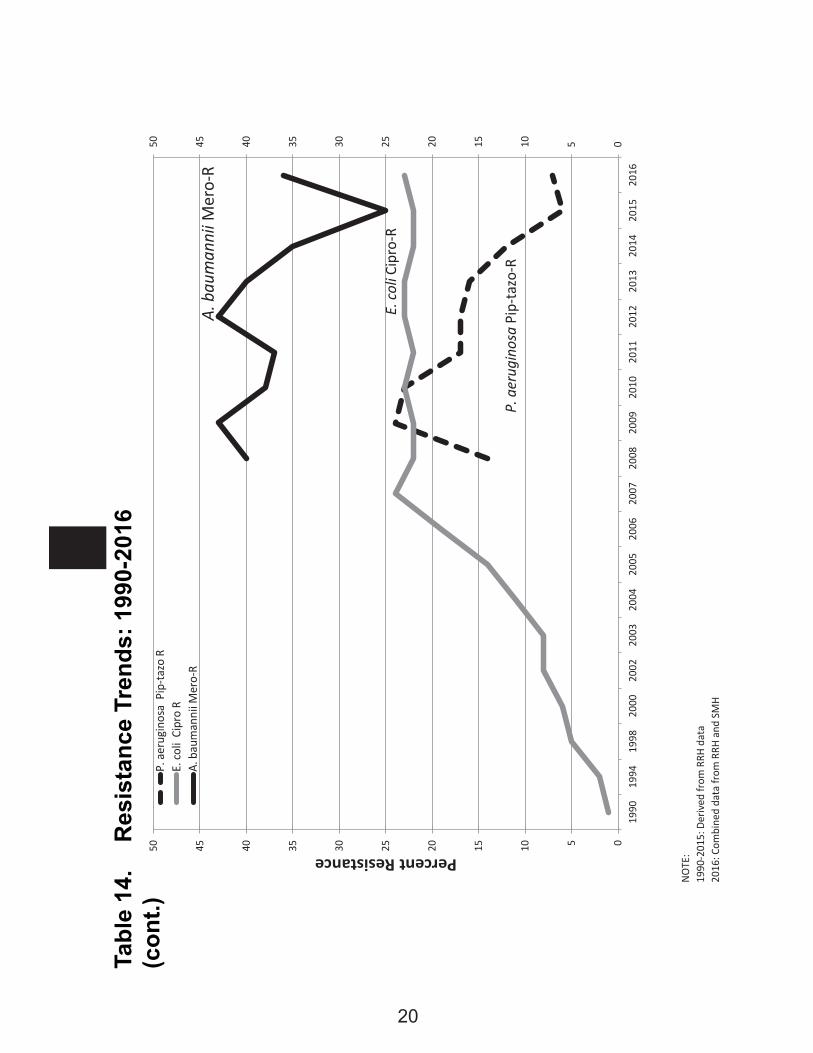
Tabl
e 14
. R
esis
tanc
e Tr
ends
: 199
0-20
16(c
ont.)
NOTE
:19
90-2
015:
Der
ived
from
RRH
dat
a20
16: C
ombi
ned
data
from
RRH
and
SM
H
05101520253035404550
05101520253035404550
1990
1994
1998
2000
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
Percent Resistance
P. a
erug
inos
a P
ip-ta
zo R
E. co
li C
ipro
RA.
bau
man
nii M
ero-
R
E.co
li Ci
pro-
R
P. a
erug
inos
a Pi
p-ta
zo-R
A.ba
uman
nii M
ero-
R
20
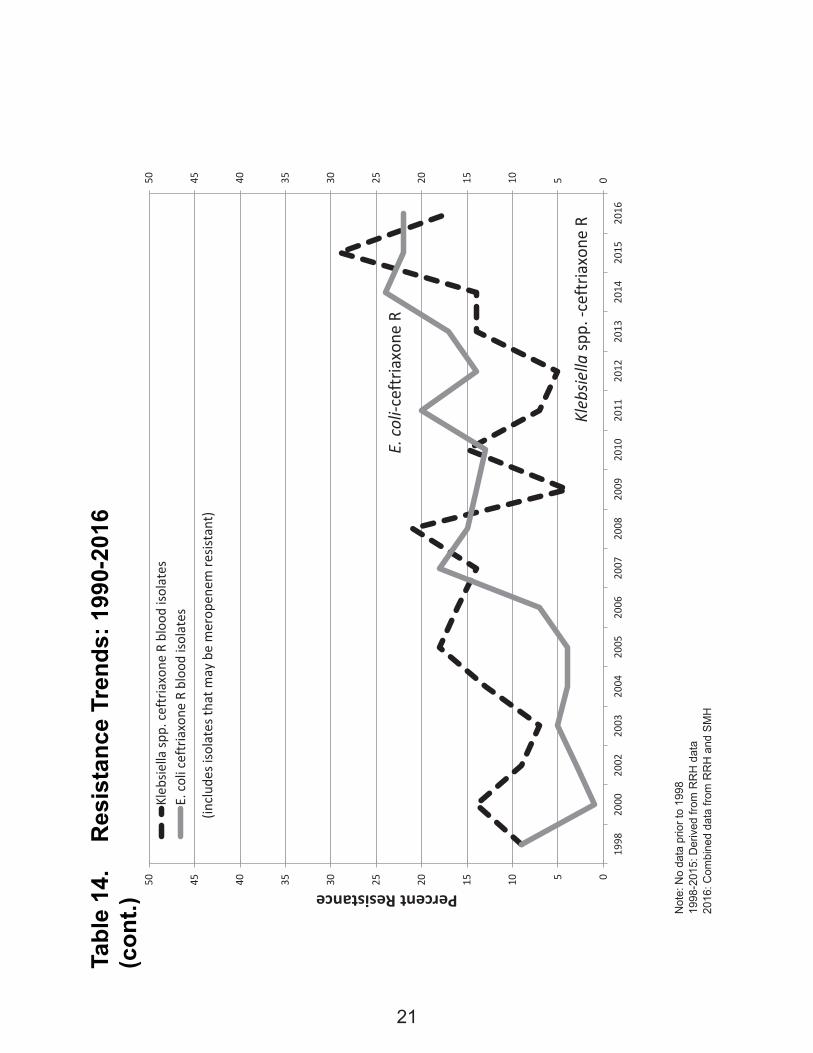
Tabl
e 14
. R
esis
tanc
e Tr
ends
: 199
0-20
16(c
ont.) N
ote:
No
data
prio
r to
1998
1998
-201
5: D
eriv
ed fr
om R
RH
dat
a20
16: C
ombi
ned
data
from
RR
H a
nd S
MH
05101520253035404550
05101520253035404550
1998
2000
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
Percent ResistanceKl
ebsie
lla sp
p. ce
ftria
xone
R b
lood
isol
ates
E. co
li ce
ftria
xone
R b
lood
isol
ates
E.coli-
ceftr
iaxo
ne R
Klebsie
llasp
p.-c
eftr
iaxo
ne R
(incl
udes
isola
tes t
hat m
ay b
e m
erop
enem
resis
tant
)
21
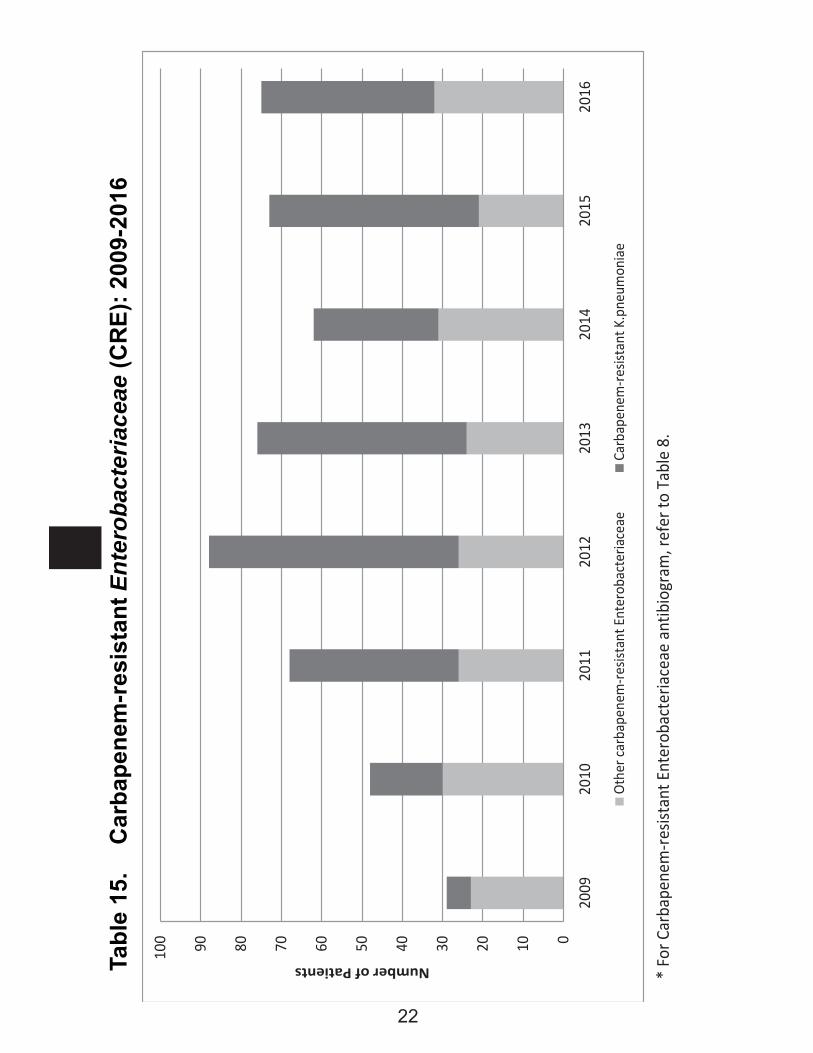
Tabl
e 15
. C
arba
pene
m-r
esis
tant
Ent
erob
acte
riace
ae (C
RE)
: 200
9-20
16
*
For
Car
bape
nem
-resis
tant
Ent
erob
acte
riace
ae a
ntib
iogr
am, r
efer
to T
able
8.
0102030405060708090100
2009
2010
2011
2012
2013
2014
2015
2016
Number of Patients
Othe
r car
bape
nem
-resis
tant
Ent
erob
acte
riace
aeCa
rbap
enem
-resis
tant
K.p
neum
onia
e
22
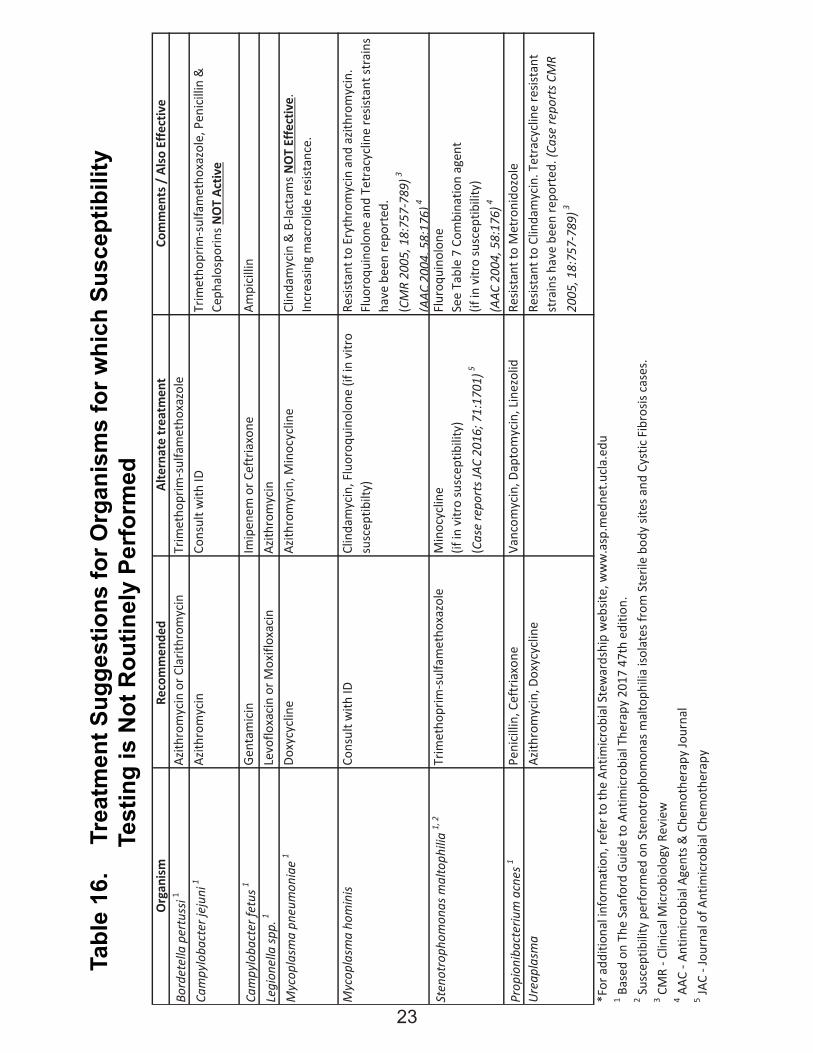
Tabl
e 16
. Tr
eatm
ent S
ugge
stio
ns fo
r Org
anis
ms
for w
hich
Sus
cept
ibili
ty
Tes
ting
is N
ot R
outin
ely
Perf
orm
ed
O
rgan
ismRe
com
men
ded
Alte
rnat
e tr
eatm
ent
Com
men
ts /
Also
Effe
ctiv
eBo
rdet
ella
per
tuss
i1Az
ithro
myc
in o
r Cla
rithr
omyc
inTr
imet
hopr
im-s
ulfa
met
hoxa
zole
Cam
pylo
bact
er je
juni
1Az
ithro
myc
inCo
nsul
t with
IDTr
imet
hopr
im-s
ulfa
met
hoxa
zole
, Pen
icilli
n &
Ce
phal
ospo
rins N
OT
Activ
e
Cam
pylo
bact
er fe
tus1
Gent
amici
nIm
ipen
em o
r Cef
tria
xone
Ampi
cillin
Legi
onel
la sp
p.1
Levo
floxa
cin o
r Mox
iflox
acin
Azith
rom
ycin
Myc
opla
sma
pneu
mon
iae
1Do
xycy
clin
eAz
ithro
myc
in, M
inoc
yclin
eCl
inda
myc
in &
B-la
ctam
s NO
T Ef
fect
ive.
In
crea
sing
mac
rolid
e re
sista
nce.
Myc
opla
sma
hom
inis
Cons
ult w
ith ID
Clin
dam
ycin
, Flu
oroq
uino
lone
(if i
n vi
tro
susc
eptib
ilty)
Resis
tant
to E
ryth
rom
ycin
and
azit
hrom
ycin
.Fl
uoro
quin
olon
e an
d Te
trac
yclin
e re
sista
nt st
rain
s ha
ve b
een
repo
rted
. (C
MR
2005
, 18:
757-
789)
3
(AAC
2004
,58:
176)
4
Sten
otro
phom
onas
mal
toph
ilia
1, 2
Trim
etho
prim
-sul
fam
etho
xazo
leM
inoc
yclin
e(if
in v
itro
susc
eptib
ility
)(C
ase
repo
rts J
AC 2
016;
71:
1701
)5
Flur
oqui
nolo
neSe
e Ta
ble
7 Co
mbi
natio
n ag
ent
(if in
vitr
o su
scep
tibili
ty)
(AAC
200
4, 5
8:17
6)4
Prop
ioni
bact
eriu
m a
cnes
1Pe
nicil
lin, C
eftr
iaxo
neVa
ncom
ycin
, Dap
tom
ycin
, Lin
ezol
idRe
sista
nt to
Met
roni
dozo
leUr
eapl
asm
aAz
ithro
myc
in, D
oxyc
yclin
eRe
sista
nt to
Clin
dam
ycin
. Tet
racy
clin
e re
sista
nt
stra
ins h
ave
been
repo
rted
. (Ca
se re
port
s CM
R 20
05, 1
8:75
7-78
9)3
*For
add
ition
al in
form
atio
n, re
fer t
o th
e An
timicr
obia
l Ste
war
dshi
p w
ebsit
e, w
ww
.asp
.med
net.u
cla.e
du1 B
ased
on
The
Sanf
ord
Guid
e to
Ant
imicr
obia
l The
rapy
201
7 47
th e
ditio
n.2 S
usce
ptib
ility
per
form
ed o
n St
enot
roph
omon
as m
alto
phili
a iso
late
s fro
m S
teril
e bo
dy si
tes a
nd C
ystic
Fib
rosis
cas
es.
3 CM
R - C
linica
l Micr
obio
logy
Rev
iew
4 AAC
- An
timicr
obia
l Age
nts &
Che
mot
hera
py Jo
urna
l5 JA
C - J
ourn
al o
f Ant
imicr
obia
l Che
mot
hera
py
23
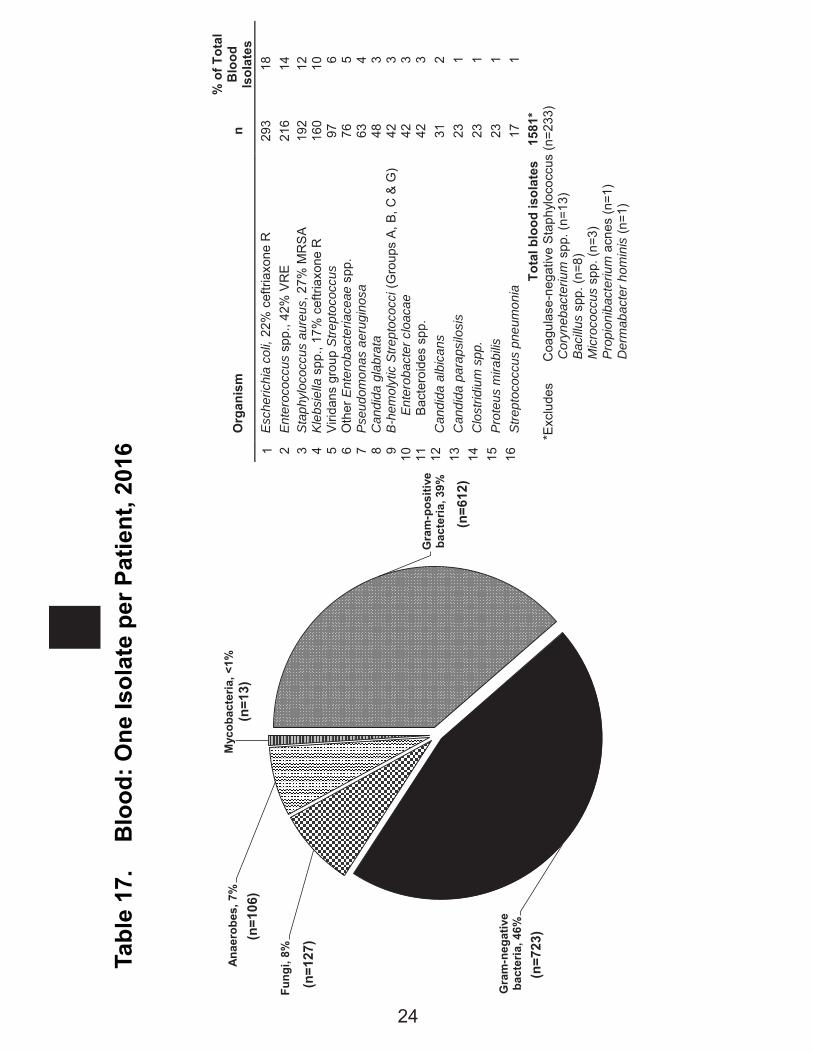
Tabl
e 17
. B
lood
: One
Isol
ate
per P
atie
nt, 2
016
Gra
m-p
ositi
ve
bact
eria
, 39%
Gra
m-n
egat
ive
bact
eria
, 46%
Fung
i, 8%
Anae
robe
s, 7
%M
ycob
acte
ria, <
1%(n
=13)
(n=1
06)
(n=1
27)
(n=7
23)
(n=6
12)
O
rgan
ism
n
% o
f Tot
al
Blo
od
Isol
ates
1
Esc
heric
hia
coli,
22%
cef
triax
one
R
293
18
2 En
tero
cocc
us s
pp.,
42%
VR
E
216
14
3 S
taph
yloc
occu
s au
reus
, 27%
MR
SA
19
2 12
4
Kleb
siel
la s
pp.,
17%
cef
triax
one
R
160
10
5 Vi
ridan
s gr
oup
Stre
ptoc
occu
s 97
6
6 O
ther
Ent
erob
acte
riace
ae s
pp.
76
5 7
Pseu
dom
onas
aer
ugin
osa
63
4 8
Can
dida
gla
brat
a 48
3
9 B
-hem
olyt
ic S
trept
ococ
ci (G
roup
s A,
B, C
& G
) 42
3
10
Ent
erob
acte
r clo
acae
42
3
11
Bact
eroi
des
spp.
42
3
12
Can
dida
alb
ican
s 31
2
13
Can
dida
par
apsi
losi
s 23
1
14
Clo
strid
ium
spp
. 23
1
15
Prot
eus
mira
bilis
23
1
16
Stre
ptoc
occu
s pn
eum
onia
17
1
To
tal b
lood
isol
ates
15
81*
*E
xclu
des
C
oagu
lase
-neg
ativ
e S
taph
yloc
occu
s (n
=233
) C
oryn
ebac
teriu
m s
pp. (
n=13
) Ba
cillu
s sp
p. (n
=8)
Mic
roco
ccus
spp
. (n=
3)
Pro
pion
ibac
teriu
m a
cnes
(n=1
) D
erm
abac
ter h
omin
is (n
=1)
24
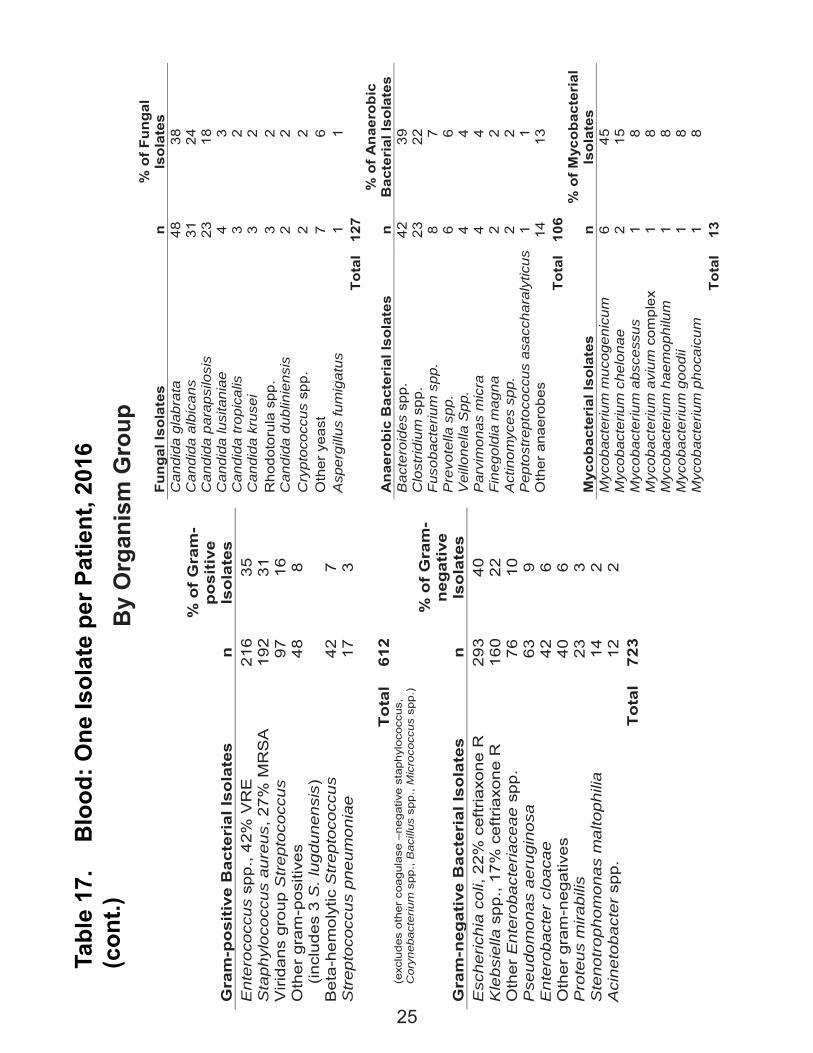
Tabl
e 17
. B
lood
: One
Isol
ate
per P
atie
nt, 2
016
(con
t.)
Gra
m-p
osi
tive
Bac
teri
al Is
ola
tes
n
% o
f G
ram
-p
osi
tive
Is
ola
tes
Ent
eroc
occu
s sp
p., 4
2% V
RE
21
6 35
S
taph
yloc
occu
s au
reus
, 27%
MR
SA
19
2 31
V
irida
ns g
roup
Str
epto
cocc
us
97
16
Oth
er g
ram
-pos
itive
s
(incl
udes
3 S
. lug
dune
nsis
) 48
8
Bet
a-he
mol
ytic
Str
epto
cocc
us
42
7 S
trep
toco
ccus
pne
umon
iae
17
3
T
ota
l 61
2
(exc
lude
s ot
her
coag
ulas
e –n
egat
ive
stap
hylo
cocc
us,
Cor
yneb
acte
rium
spp
., B
acill
us s
pp.,
Mic
roco
ccus
spp
.)
Gra
m-n
egat
ive
Bac
teri
al Is
ola
tes
n
% o
f G
ram
-n
egat
ive
Iso
late
s E
sche
richi
a co
li, 2
2% c
eftr
iaxo
ne R
29
3 40
K
lebs
iella
spp
., 17
% c
eftr
iaxo
ne R
16
0 22
O
ther
Ent
erob
acte
riace
ae s
pp.
76
10
Pse
udom
onas
aer
ugin
osa
63
9 E
nter
obac
ter
cloa
cae
42
6 O
ther
gra
m-n
egat
ives
40
6
Pro
teus
mira
bilis
23
3
Ste
notr
opho
mon
as m
alto
phili
a 14
2
Aci
neto
bact
er s
pp.
12
2 T
ota
l 72
3
Fung
al Is
olat
es
n %
of F
unga
l Is
olat
es
Can
dida
gla
brat
a 48
38
C
andi
da a
lbic
ans
31
24
Can
dida
par
apsi
losi
s 23
18
C
andi
da lu
sita
niae
4
3 C
andi
da tr
opic
alis
3
2 C
andi
da k
ruse
i 3
2 R
hodo
toru
la s
pp.
3 2
Can
dida
dub
linie
nsis
2
2 C
rypt
ococ
cus
spp.
2
2 O
ther
yea
st
7 6
Asp
ergi
llus
fum
igat
us
1 1
Tota
l 12
7
Ana
erob
ic B
acte
rial
Isol
ates
n
% o
f A
naer
obic
B
acte
rial
Isol
ates
B
acte
roid
es s
pp.
42
39
Clo
strid
ium
spp
. 23
22
F
usob
acte
rium
spp
. 8
7 P
revo
tella
spp
. 6
6 V
eillo
nella
Spp
. 4
4 P
arvi
mon
as m
icra
4
4 F
ineg
oldi
a m
agna
2
2 A
ctin
omyc
es s
pp.
2 2
Pep
tost
rept
ococ
cus
asac
char
alyt
icus
1
1 O
ther
ana
erob
es
14
13
Tota
l 10
6
Myc
obac
teri
al Is
olat
es
n %
of M
ycob
acte
rial
Is
olat
es
Myc
obac
teriu
m m
ucog
enic
um
6 45
M
ycob
acte
rium
che
lona
e 2
15
Myc
obac
teriu
m a
bsce
ssus
1
8 M
ycob
acte
rium
avi
um c
ompl
ex
1 8
Myc
obac
teriu
m h
aem
ophi
lum
1
8 M
ycob
acte
rium
goo
dii
1 8
Myc
obac
teriu
m p
hoca
icum
1
8 To
tal
13
By
Org
anis
m G
roup
25
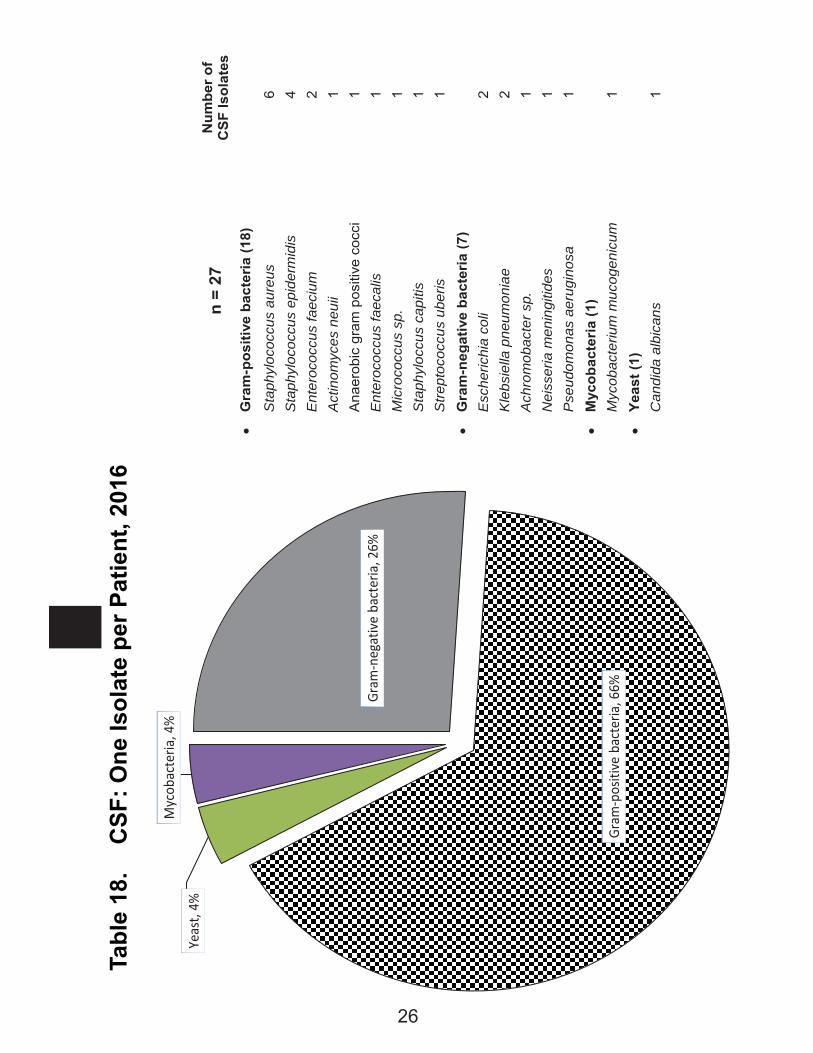
Tabl
e 18
. C
SF: O
ne Is
olat
e pe
r Pat
ient
, 201
6
Gram
-neg
ativ
e ba
cter
ia, 2
6%
Gram
-pos
itive
bac
teria
, 66%
Yeas
t, 4%
Myc
obac
teria
, 4%
n =
27
Num
ber o
f C
SF Is
olat
es
G
ram
-pos
itive
bac
teria
(18)
Sta
phyl
ococ
cus
aure
us
6 S
taph
yloc
occu
s ep
ider
mid
is
4 E
nter
ococ
cus
faec
ium
2
Act
inom
yces
neu
ii 1
Ana
erob
ic g
ram
pos
itive
coc
ci
1 E
nter
ococ
cus
faec
alis
1
Mic
roco
ccus
sp.
1
Sta
phyl
occu
s ca
pitis
1
Stre
ptoc
occu
s ub
eris
1
G
ram
-neg
ativ
e ba
cter
ia (7
)
Esc
heric
hia
coli
2 K
lebs
iella
pne
umon
iae
2
Ach
rom
obac
ter s
p.
1 N
eiss
eria
men
ingi
tides
1
Pse
udom
onas
aer
ugin
osa
1
Myc
obac
teri
a (1
)
Myc
obac
teriu
m m
ucog
enic
um
1
Yeas
t (1)
Can
dida
alb
ican
s 1
26
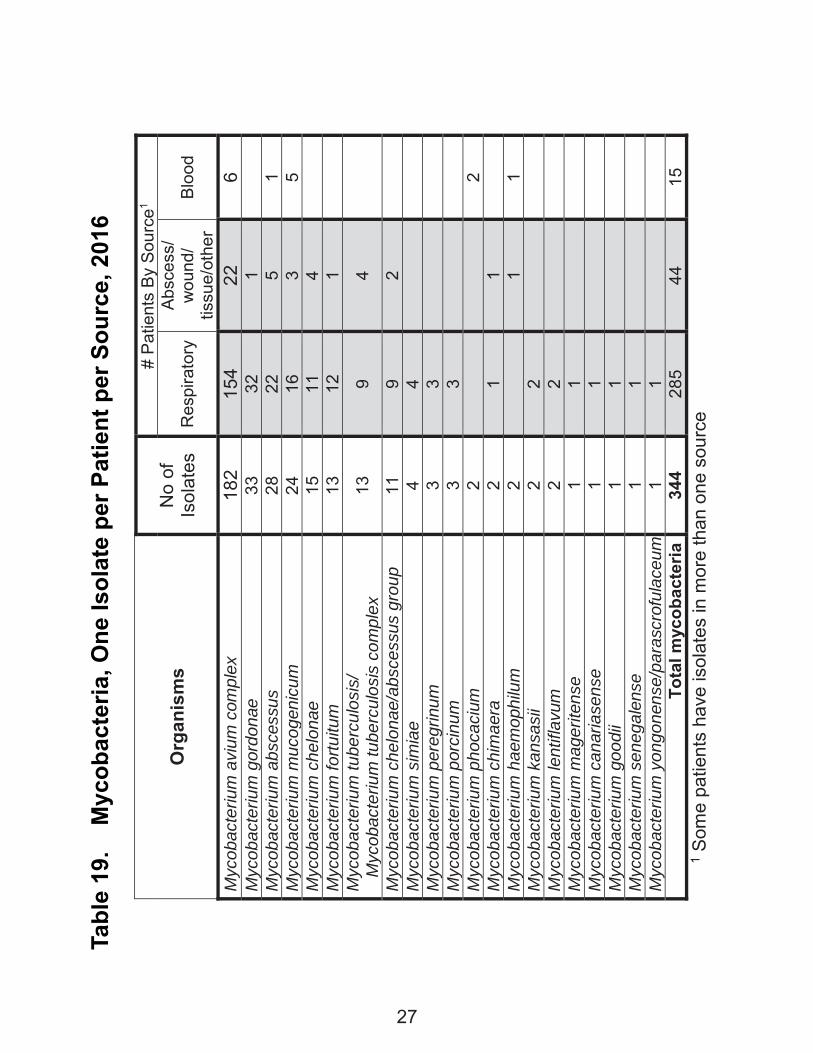
Tabl
e 19
. M
ycob
acte
ria, O
ne Is
olat
e pe
r Pat
ient
per
Sou
rce,
201
6
Org
anis
ms
No
of
Isol
ates
# P
atie
nts
By
Sou
rce1
R
espi
rato
ry
Abs
cess
/ w
ound
/ tis
sue/
othe
r B
lood
Myc
obac
teriu
m a
vium
com
plex
18
2 15
4 22
6
Myc
obac
teriu
m g
ordo
nae
33
32
1
M
ycob
acte
rium
abs
cess
us
28
22
5 1
Myc
obac
teriu
m m
ucog
enic
um
24
16
3 5
Myc
obac
teriu
m c
helo
nae
15
11
4
Myc
obac
teriu
m fo
rtuitu
m
13
12
1
Myc
obac
teriu
m tu
berc
ulos
is/
Myc
obac
teriu
m tu
berc
ulos
is c
ompl
ex
13
9 4
Myc
obac
teriu
m c
helo
nae/
absc
essu
s gr
oup
11
9 2
M
ycob
acte
rium
sim
iae
4 4
Myc
obac
teriu
m p
ereg
rinum
3
3
M
ycob
acte
rium
por
cinu
m
3 3
Myc
obac
teriu
m p
hoca
cium
2
2 M
ycob
acte
rium
chi
mae
ra
2 1
1
Myc
obac
teriu
m h
aem
ophi
lum
2
1
1 M
ycob
acte
rium
kan
sasi
i 2
2
M
ycob
acte
rium
lent
iflav
um
2 2
Myc
obac
teriu
m m
ager
itens
e 1
1
M
ycob
acte
rium
can
aria
sens
e 1
1
M
ycob
acte
rium
goo
dii
1 1
Myc
obac
teriu
m s
eneg
alen
se
1 1
Myc
obac
teriu
m y
ongo
nens
e/pa
rasc
rofu
lace
um
1 1
Tota
l myc
obac
teria
34
4 28
5 44
15
1 S
ome
patie
nts
have
isol
ates
in m
ore
than
one
sou
rce
27
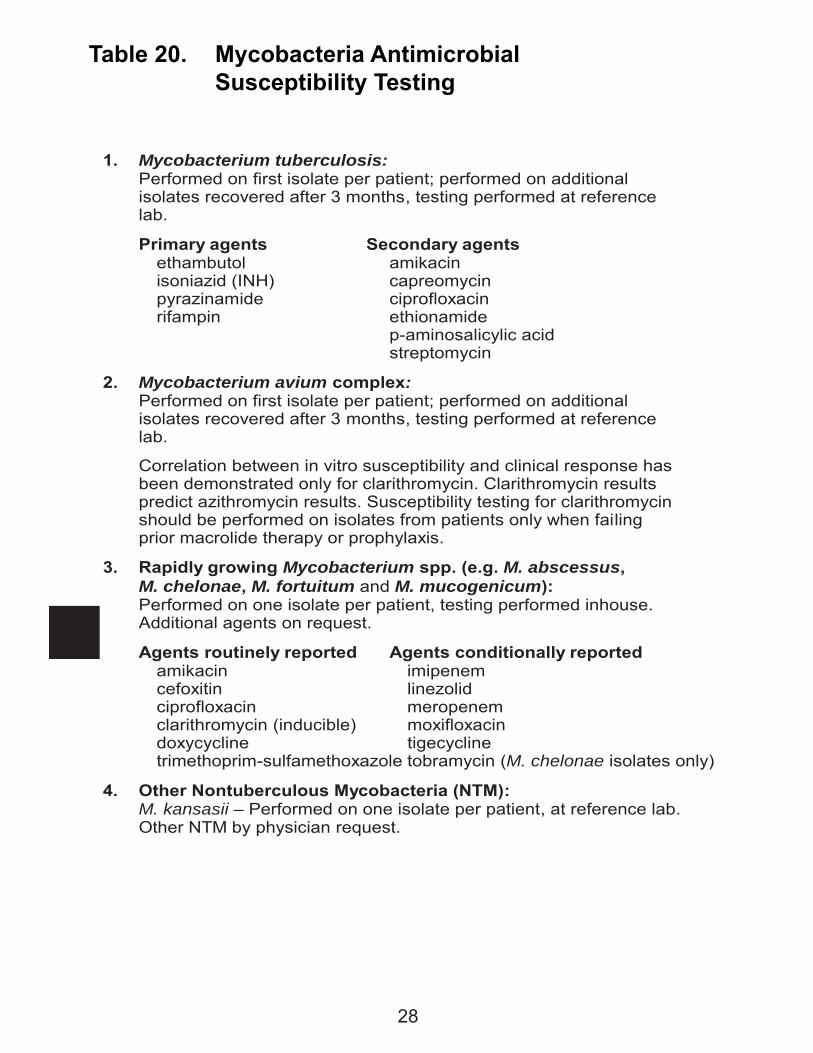
Table 20. Mycobacteria Antimicrobial Susceptibility Testing
1. Mycobacterium tuberculosis: Performed on first isolate per patient; performed on additional isolates recovered after 3 months, testing performed at reference lab.
Primary agents Secondary agents ethambutol amikacin isoniazid (INH) capreomycin pyrazinamide ciprofloxacin rifampin ethionamide p-aminosalicylic acid streptomycin
2. Mycobacterium avium complex: Performed on first isolate per patient; performed on additional isolates recovered after 3 months, testing performed at reference lab.
Correlation between in vitro susceptibility and clinical response has been demonstrated only for clarithromycin. Clarithromycin results predict azithromycin results. Susceptibility testing for clarithromycin should be performed on isolates from patients only when failing prior macrolide therapy or prophylaxis.
3. Rapidly growing Mycobacterium spp. (e.g. M. abscessus, M. chelonae, M. fortuitum and M. mucogenicum):
Performed on one isolate per patient, testing performed inhouse. Additional agents on request.
Agents routinely reported Agents conditionally reported amikacin imipenem cefoxitin linezolid ciprofloxacin meropenem clarithromycin (inducible) moxifloxacin doxycycline tigecycline trimethoprim-sulfamethoxazole tobramycin (M. chelonae isolates only)
4. Other Nontuberculous Mycobacteria (NTM): M. kansasii – Performed on one isolate per patient, at reference lab. Other NTM by physician request.
28

Tabl
e 21
. C
alifo
rnia
Myc
obac
teriu
m tu
berc
ulos
is
%
Res
ista
nt, 2
012-
2015
Antim
icro
bial
Age
nt20
1120
1220
1320
1420
15Is
onia
zid10
.9%
10.0
%10
.6%
9.8%
10.9
%Ri
fam
pin
2.2%
0.9%
1.8%
1.3%
1.4%
Etha
mbu
tol
1.6%
0.9%
1.1%
0.8%
0.7%
Pyra
zinam
ide
7.0%
6.7%
6.7%
5.5%
5.1%
Stre
ptom
ycin
10.3
%11
.3%
10.7
%7.
1%9.
7%M
ulti-
drug
Res
istan
t Tu
berc
ulos
is ra
tes1
2.0%
0.8%
1.6%
1.1%
1.3%
Num
ber o
f Cas
es
1840
1738
1756
1719
1762
* Bas
ed o
n Ca
liforn
ia D
epar
tmen
t of P
ublic
Hea
lth A
nnua
l rep
ort "
Repo
rt on
Tub
ercu
losis
in C
alifo
rnia
"1 M
DR =
Res
istan
t to
Ison
iazid
and
Rifa
mpi
n
29
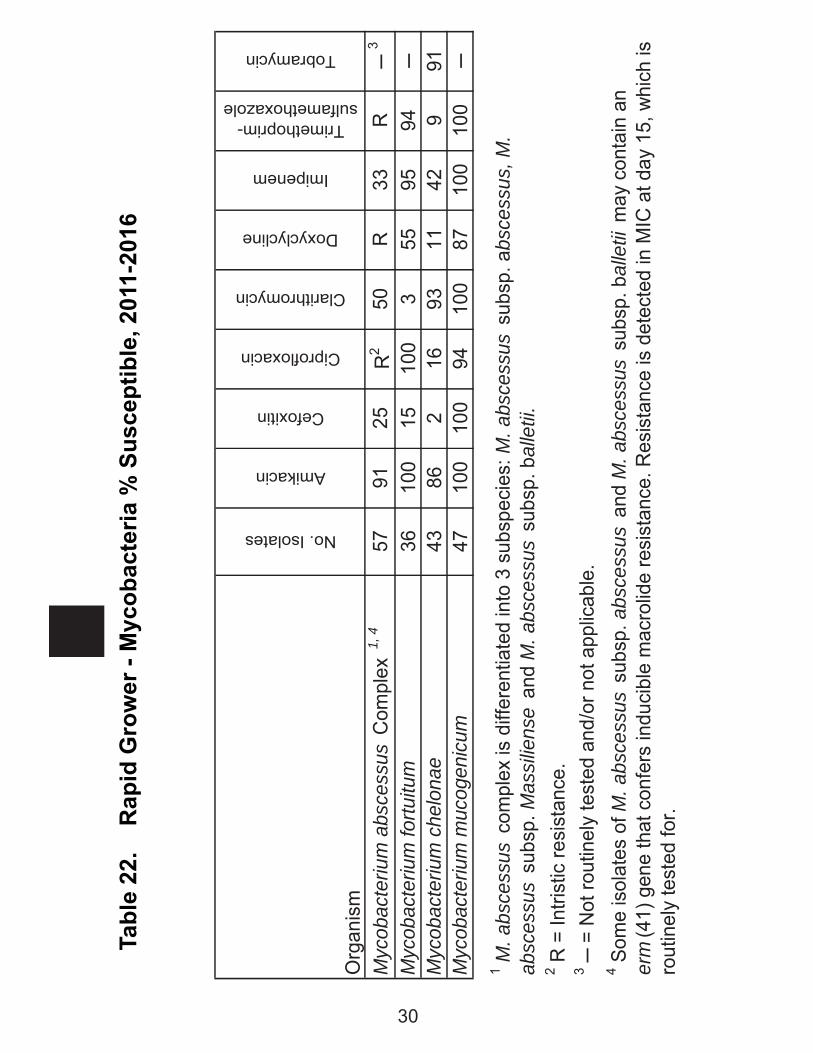
Tabl
e 22
. R
apid
Gro
wer
- M
ycob
acte
ria %
Sus
cept
ible
, 201
1-20
16
Org
anis
m
No. Isolates
Amikacin
Cefoxitin
Ciprofloxacin
Clarithromycin
Doxyclycline
Imipenem
Trimethoprim-sulfamethoxazole
Tobramycin
Myc
obac
teriu
m a
bsce
ssus
Com
plex
1, 4
5791
25R
250
R33
R ─
3
Myc
obac
teriu
m fo
rtuitu
m36
100
1510
03
5595
94─
Myc
obac
teriu
m c
helo
nae
4386
216
9311
429
91M
ycob
acte
rium
muc
ogen
icum
4710
010
094
100
8710
010
0─
2 R =
Intri
stic
resi
stan
ce.
3 ─ =
Not
rout
inel
y te
sted
and
/or n
ot a
pplic
able
.
1 M. a
bsce
ssus
com
plex
is d
iffer
entia
ted
into
3 s
ubsp
ecie
s: M
. abs
cess
us s
ubsp
. abs
cess
us, M
. ab
sces
sus
subs
p. M
assi
liens
e an
d M
. abs
cess
us s
ubsp
. bal
letii
.
4 Som
e is
olat
es o
f M. a
bsce
ssus
sub
sp. a
bsce
ssus
and
M. a
bsce
ssus
sub
sp. b
alle
tii m
ay c
onta
in a
n er
m(4
1) g
ene
that
con
fers
indu
cibl
e m
acro
lide
resi
stan
ce. R
esis
tanc
e is
det
ecte
d in
MIC
at d
ay 1
5, w
hich
is
rout
inel
y te
sted
for.
30
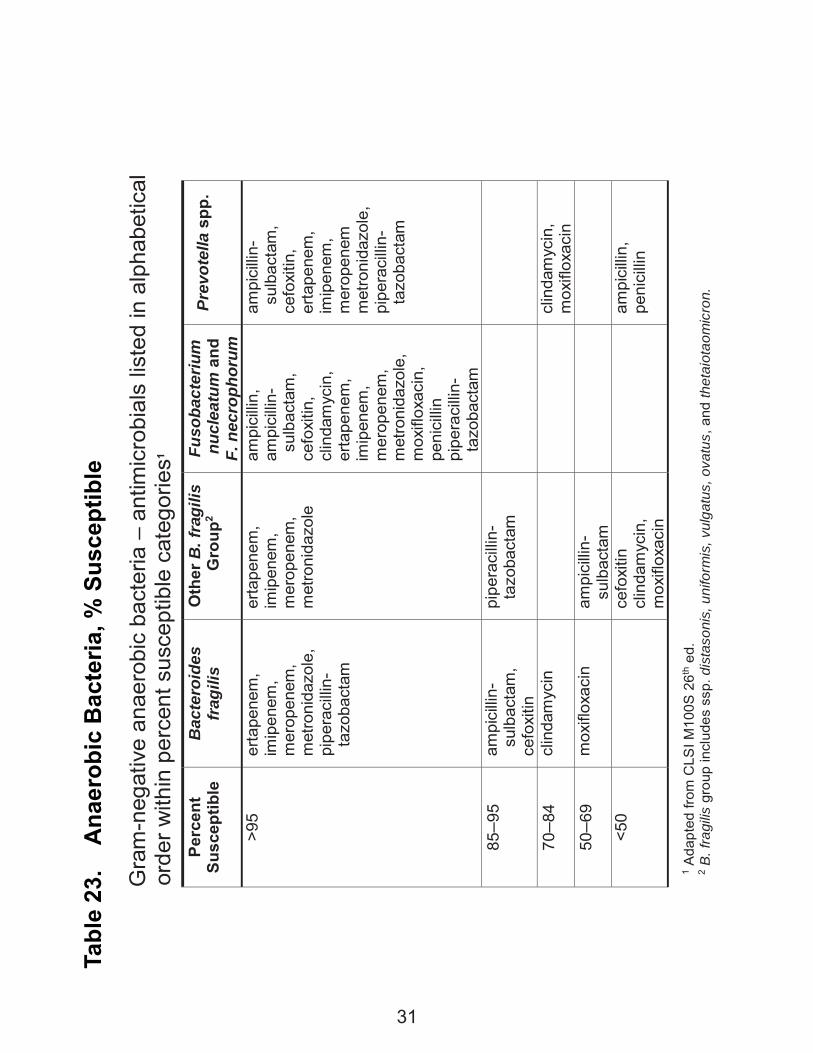
Tabl
e 23
. A
naer
obic
Bac
teria
, % S
usce
ptib
le
G
ram
-neg
ativ
e an
aero
bic
bact
eria
– a
ntim
icro
bial
s lis
ted
in a
lpha
betic
al
o
rder
with
in p
erce
nt s
usce
ptib
le c
ateg
orie
s1 Pe
rcen
t Su
scep
tible
B
acte
roid
es
frag
ilis
Oth
er B
. fra
gilis
G
roup
2 Fu
soba
cter
ium
n
ucle
atum
and
F.
nec
roph
orum
Prev
otel
la s
pp.
>95
erta
pene
m,
imip
enem
, m
erop
enem
, m
etro
nida
zole
, pi
pera
cilli
n-
taz
obac
tam
erta
pene
m,
imip
enem
, m
erop
enem
, m
etro
nida
zole
ampi
cilli
n,
ampi
cilli
n-
sul
bact
am,
ce
foxi
tin,
clin
dam
ycin
,
erta
pene
m,
imip
enem
, m
erop
enem
, m
etro
nida
zole
, m
oxifl
oxac
in,
peni
cilli
n pi
pera
cilli
n-
taz
obac
tam
ampi
cilli
n-
sul
bact
am,
cefo
xitin
, er
tape
nem
, im
ipen
em,
mer
open
em
met
roni
dazo
le,
pipe
raci
llin-
t
azob
acta
m
85–9
5 am
pici
llin-
s
ulba
ctam
, ce
foxi
tin
pipe
raci
llin-
t
azob
acta
m
70–8
4 cl
inda
myc
in
clin
dam
ycin
, m
oxifl
oxac
in
50–6
9 m
oxifl
oxac
in
ampi
cilli
n-
sul
bact
am
<50
ce
foxi
tin
clin
dam
ycin
, m
oxifl
oxac
in
am
pici
llin,
pe
nici
llin
1 A
dapt
ed fr
om C
LSI M
100S
26th
ed.
2 B. f
ragi
lis g
roup
incl
udes
ssp
. dis
taso
nis,
uni
form
is, v
ulga
tus,
ova
tus,
and
thet
aiot
aom
icro
n.
31
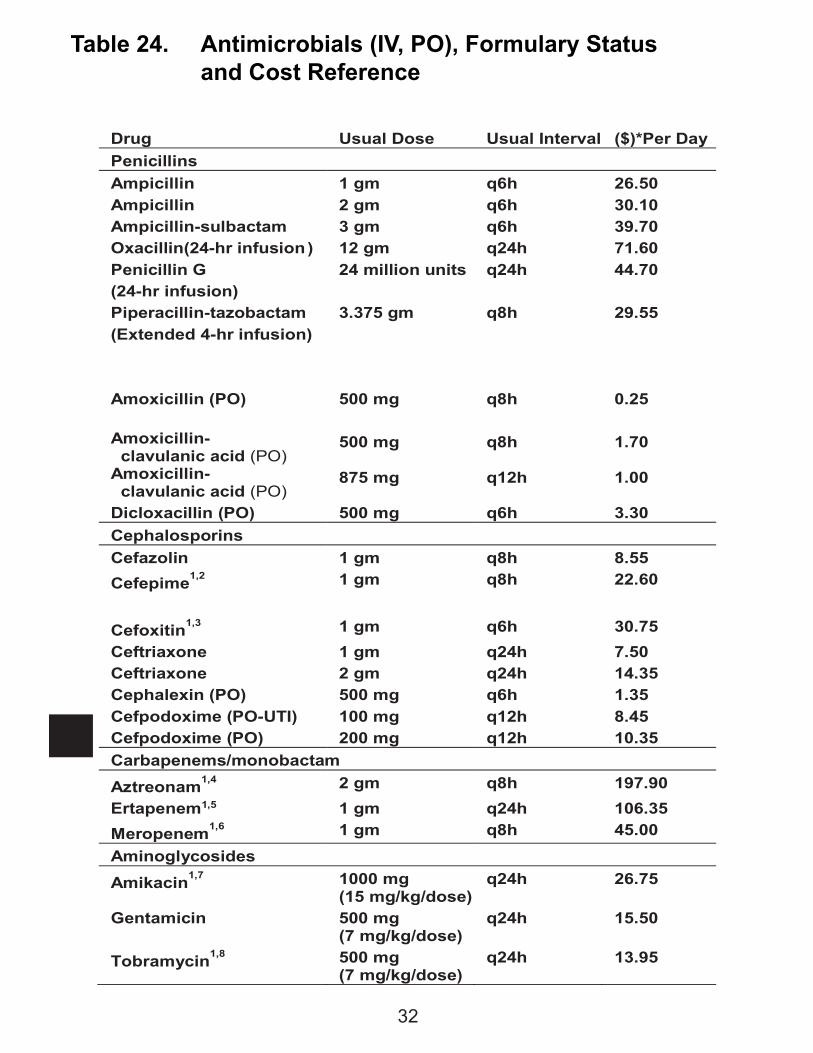
Table 24. Antimicrobials (IV, PO), Formulary Status and Cost Reference
Drug Usual Dose Usual Interval ($)*Per Day Penicillins Ampicillin 1 gm q6h 26.50 Ampicillin 2 gm q6h 30.10 Ampicillin-sulbactam 3 gm q6h 39.70 Oxacillin(24-hr infusion ) 12 gm q24h 71.60 Penicillin G (24-hr infusion)
24 million units q24h 44.70
Piperacillin-tazobactam (Extended 4-hr infusion)
3.375 gm q8h 29.55
Amoxicillin (PO) 500 mg q8h 0.25 Amoxicillin- clavulanic acid (PO)
500 mg q8h 1.70
Amoxicillin- clavulanic acid (PO)
875 mg q12h 1.00
Dicloxacillin (PO) 500 mg q6h 3.30 Cephalosporins Cefazolin 1 gm q8h 8.55 Cefepime1,2 1 gm q8h 22.60 Cefoxitin1,3 1 gm q6h 30.75 Ceftriaxone 1 gm q24h 7.50 Ceftriaxone 2 gm q24h 14.35 Cephalexin (PO) 500 mg q6h 1.35 Cefpodoxime (PO-UTI) 100 mg q12h 8.45 Cefpodoxime (PO) 200 mg q12h 10.35 Carbapenems/monobactam Aztreonam1,4 2 gm q8h 197.90 Ertapenem1,5 1 gm q24h 106.35 Meropenem1,6 1 gm q8h 45.00 Aminoglycosides Amikacin1,7 1000 mg
(15 mg/kg/dose) q24h 26.75
Gentamicin 500 mg (7 mg/kg/dose)
q24h 15.50
Tobramycin1,8 500 mg (7 mg/kg/dose)
q24h 13.95
32
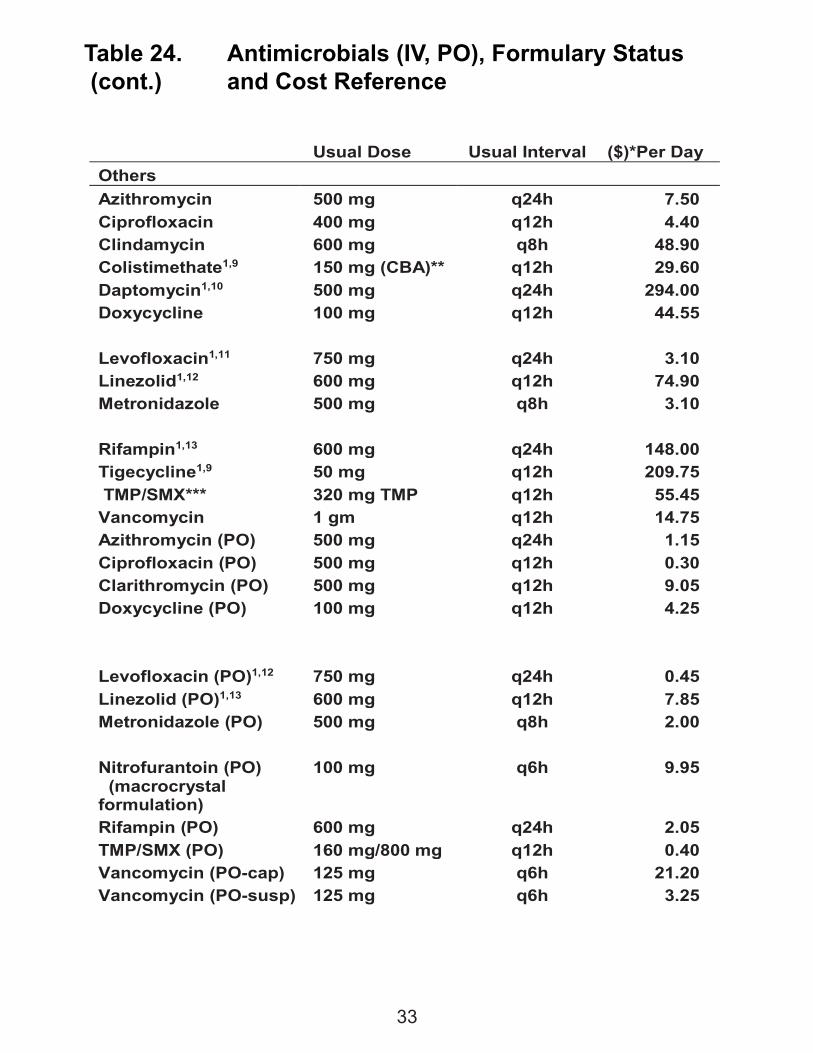
Table 24. Antimicrobials (IV, PO), Formulary Status (cont.) and Cost Reference
Usual Dose Usual Interval ($)*Per Day Others Azithromycin 500 mg q24h 7.50 Ciprofloxacin 400 mg q12h 4.40 Clindamycin 600 mg q8h 48.90 Colistimethate1,9 150 mg (CBA)** q12h 29.60 Daptomycin1,10 500 mg q24h 294.00 Doxycycline 100 mg q12h 44.55 Levofloxacin1,11 750 mg q24h 3.10 Linezolid1,12 600 mg q12h 74.90 Metronidazole 500 mg q8h 3.10 Rifampin1,13 600 mg q24h 148.00 Tigecycline1,9 50 mg q12h 209.75 TMP/SMX*** 320 mg TMP q12h 55.45 Vancomycin 1 gm q12h 14.75 Azithromycin (PO) 500 mg q24h 1.15 Ciprofloxacin (PO) 500 mg q12h 0.30 Clarithromycin (PO) 500 mg q12h 9.05 Doxycycline (PO) 100 mg q12h 4.25 Levofloxacin (PO)1,12 750 mg q24h 0.45 Linezolid (PO)1,13 600 mg q12h 7.85 Metronidazole (PO) 500 mg q8h 2.00 Nitrofurantoin (PO) (macrocrystal formulation)
100 mg q6h 9.95
Rifampin (PO) 600 mg q24h 2.05 TMP/SMX (PO) 160 mg/800 mg q12h 0.40 Vancomycin (PO-cap) Vancomycin (PO-susp)
125 mg 125 mg
q6h q6h
21.20 3.25
33
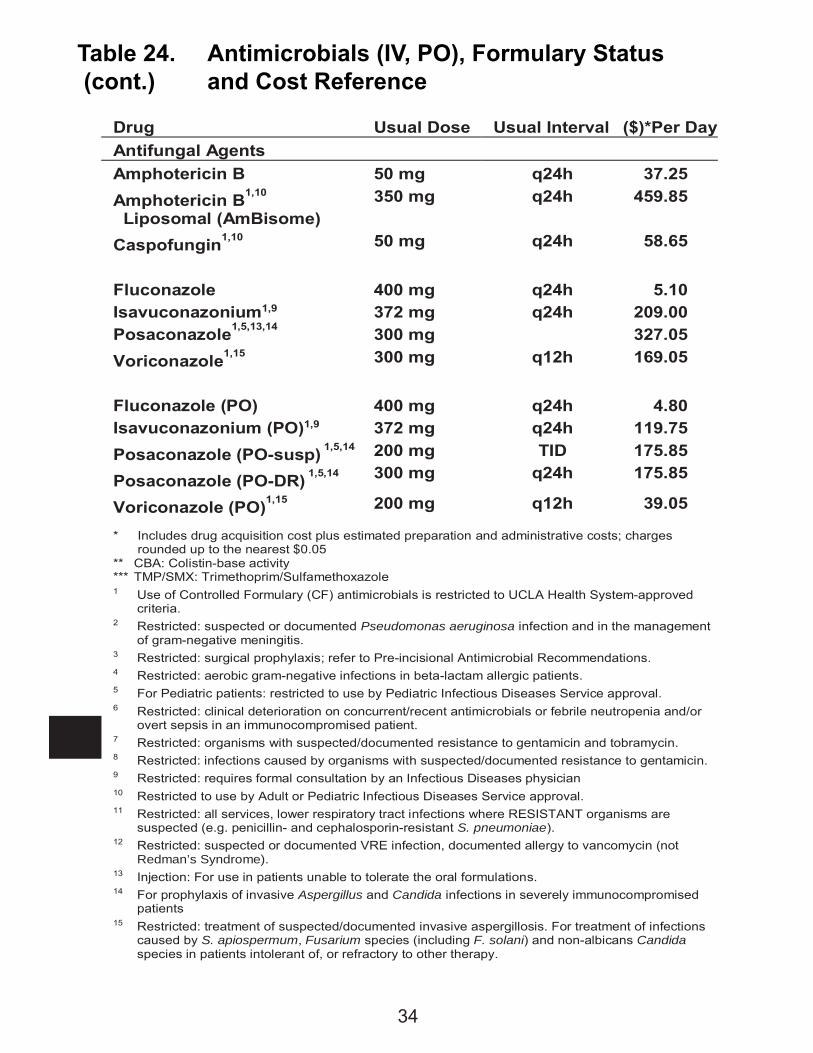
Table 24. Antimicrobials (IV, PO), Formulary Status (cont.) and Cost Reference
Drug Usual Dose Usual Interval ($)*Per Day Antifungal Agents Amphotericin B 50 mg q24h 37.25 Amphotericin B1,10 Liposomal (AmBisome)
350 mg q24h 459.85
Caspofungin1,10 50 mg q24h 58.65 Fluconazole Isavuconazonium1,9 Posaconazole1,5,13,14
400 mg 372 mg 300 mg
q24h q24h
5.10 209.00 327.05
Voriconazole1,15 300 mg q12h 169.05 Fluconazole (PO) Isavuconazonium (PO)1,9
400 mg 372 mg
q24h q24h
4.80 119.75
Posaconazole (PO-susp) 1,5,14 Posaconazole (PO-DR) 1,5,14
200 mg 300 mg
TID q24h
175.85 175.85
Voriconazole (PO)1,15 200 mg q12h 39.05
* Includes drug acquisition cost plus estimated preparation and administrative costs; charges rounded up to the nearest $0.05
** CBA: Colistin-base activity *** TMP/SMX: Trimethoprim/Sulfamethoxazole 1 Use of Controlled Formulary (CF) antimicrobials is restricted to UCLA Health System-approved
criteria. 2 Restricted: suspected or documented Pseudomonas aeruginosa infection and in the management
of gram-negative meningitis. 3 Restricted: surgical prophylaxis; refer to Pre-incisional Antimicrobial Recommendations. 4 Restricted: aerobic gram-negative infections in beta-lactam allergic patients. 5 For Pediatric patients: restricted to use by Pediatric Infectious Diseases Service approval. 6 Restricted: clinical deterioration on concurrent/recent antimicrobials or febrile neutropenia and/or
overt sepsis in an immunocompromised patient. 7 Restricted: organisms with suspected/documented resistance to gentamicin and tobramycin. 8 Restricted: infections caused by organisms with suspected/documented resistance to gentamicin. 9 Restricted: requires formal consultation by an Infectious Diseases physician 10 Restricted to use by Adult or Pediatric Infectious Diseases Service approval. 11 Restricted: all services, lower respiratory tract infections where RESISTANT organisms are
suspected (e.g. penicillin- and cephalosporin-resistant S. pneumoniae). 12 Restricted: suspected or documented VRE infection, documented allergy to vancomycin (not
Redman’s Syndrome). 13 Injection: For use in patients unable to tolerate the oral formulations. 14 For prophylaxis of invasive Aspergillus and Candida infections in severely immunocompromised
patients 15 Restricted: treatment of suspected/documented invasive aspergillosis. For treatment of infections
caused by S. apiospermum, Fusarium species (including F. solani) and non-albicans Candida species in patients intolerant of, or refractory to other therapy.
34
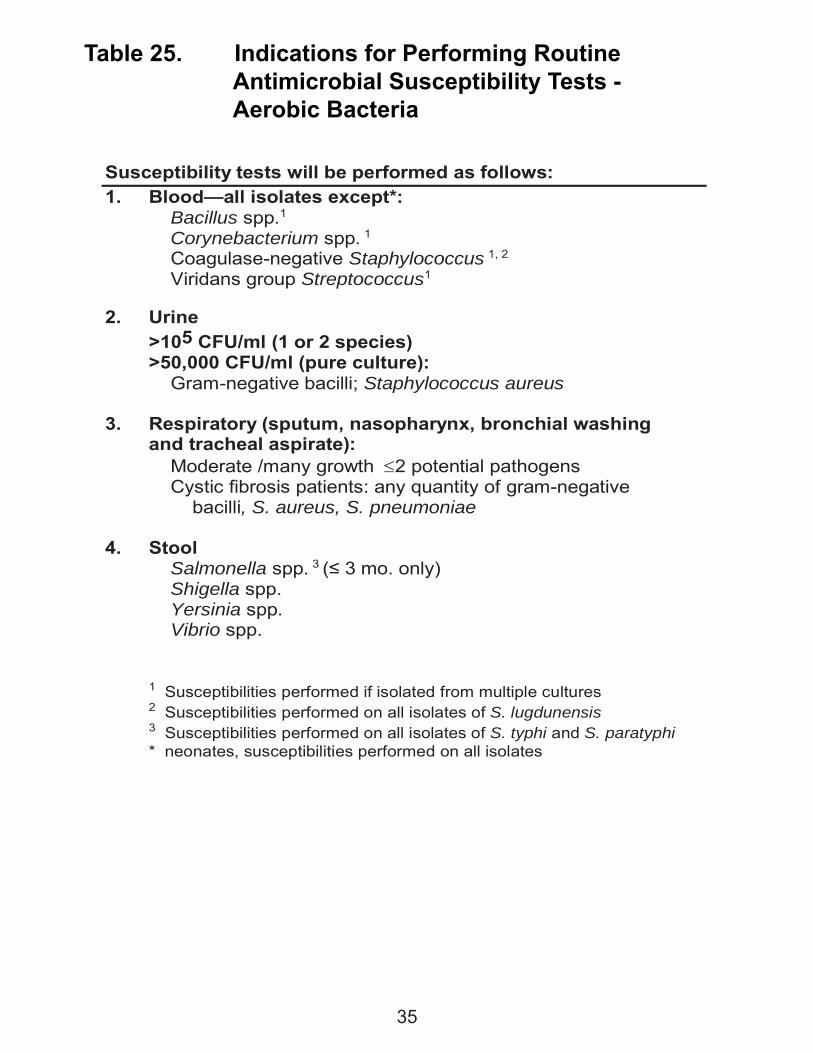
Table 25. Indications for Performing Routine Antimicrobial Susceptibility Tests - Aerobic Bacteria
Susceptibility tests will be performed as follows: 1. Blood—all isolates except*:
Bacillus spp.1 Corynebacterium spp. 1 Coagulase-negative Staphylococcus 1, 2 Viridans group Streptococcus1
2. Urine >105 CFU/ml (1 or 2 species) >50,000 CFU/ml (pure culture):
Gram-negative bacilli; Staphylococcus aureus
3. Respiratory (sputum, nasopharynx, bronchial washing and tracheal aspirate):
Moderate /many growth 2 potential pathogens Cystic fibrosis patients: any quantity of gram-negative
bacilli, S. aureus, S. pneumoniae
4. Stool Salmonella spp. 3 (≤ 3 mo. only) Shigella spp. Yersinia spp. Vibrio spp.
1 Susceptibilities performed if isolated from multiple cultures 2 Susceptibilities performed on all isolates of S. lugdunensis 3 Susceptibilities performed on all isolates of S. typhi and S. paratyphi * neonates, susceptibilities performed on all isolates
35
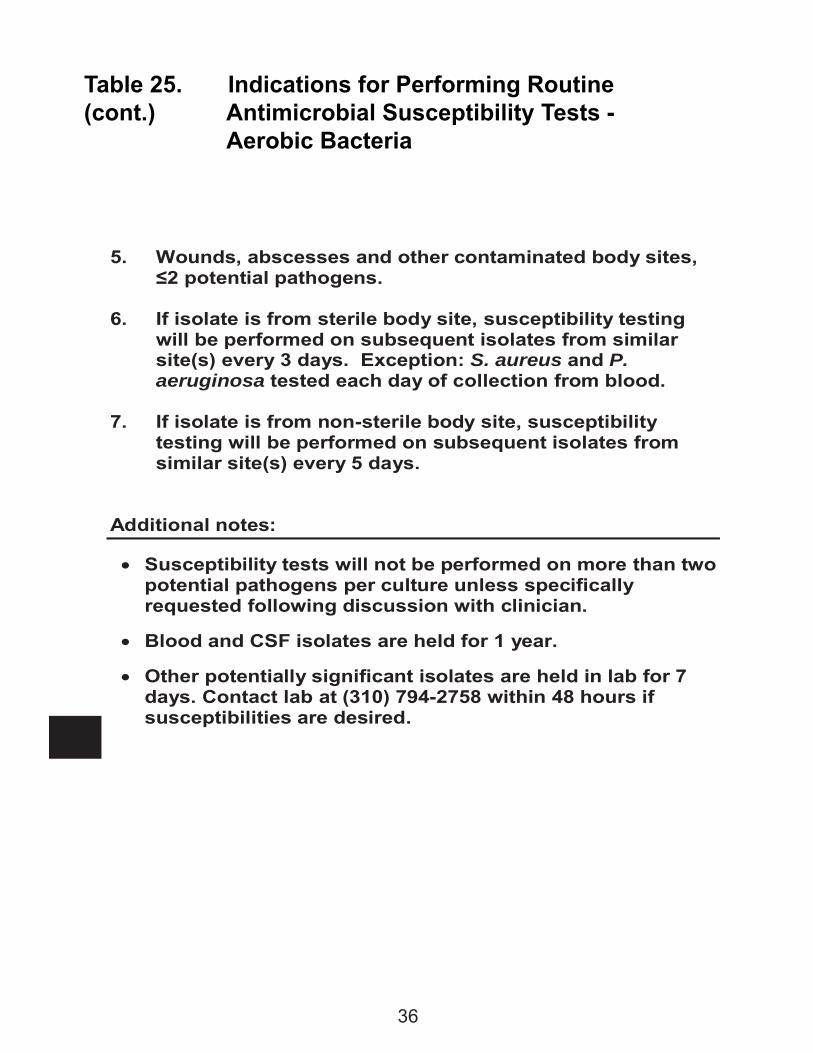
Table 25. Indications for Performing Routine(cont.) Antimicrobial Susceptibility Tests - Aerobic Bacteria
5. Wounds, abscesses and other contaminated body sites, ≤2 potential pathogens.
6. If isolate is from sterile body site, susceptibility testing
will be performed on subsequent isolates from similar site(s) every 3 days. Exception: S. aureus and P. aeruginosa tested each day of collection from blood.
7. If isolate is from non-sterile body site, susceptibility
testing will be performed on subsequent isolates from similar site(s) every 5 days.
Additional notes:
Susceptibility tests will not be performed on more than two potential pathogens per culture unless specifically requested following discussion with clinician.
Blood and CSF isolates are held for 1 year.
Other potentially significant isolates are held in lab for 7 days. Contact lab at (310) 794-2758 within 48 hours if susceptibilities are desired.
36
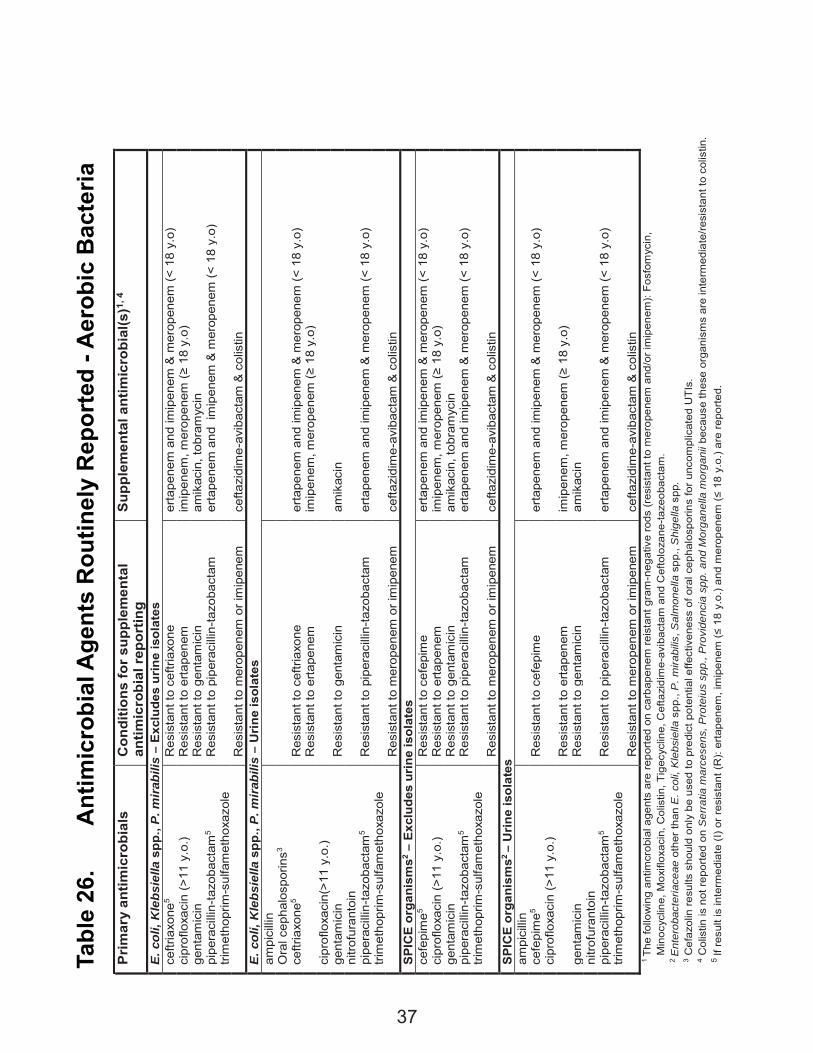
Tabl
e 26
.
Ant
imic
robi
al A
gent
s R
outin
ely
Rep
orte
d - A
erob
ic B
acte
ria
Pri
mar
y an
timic
robi
als
Con
ditio
ns fo
r su
pple
men
tal
antim
icro
bial
rep
ortin
g S
uppl
emen
tal a
ntim
icro
bial
(s)1,
4
E. c
oli,
Kle
bsie
lla s
pp.,
P. m
irab
ilis
– E
xclu
des
urin
e is
olat
es
ceftr
iaxo
ne5
Res
ista
nt to
cef
triax
one
erta
pene
m a
nd im
ipen
em &
mer
open
em (˂
18
y.o)
ci
prof
loxa
cin
(>11
y.o
.) R
esis
tant
to e
rtape
nem
im
ipen
em, m
erop
enem
(≥ 1
8 y.
o)
gent
amic
in
Res
ista
nt to
gen
tam
icin
am
ikac
in, t
obra
myc
in
pipe
raci
llin-
tazo
bact
am5
Res
ista
nt to
pip
erac
illin
-tazo
bact
am
erta
pene
m a
nd i
mip
enem
& m
erop
enem
(˂ 1
8 y.
o)
trim
etho
prim
-sul
fam
etho
xazo
le
R
esis
tant
to m
erop
enem
or i
mip
enem
ce
ftazi
dim
e-av
ibac
tam
& c
olis
tin
E. c
oli,
Kle
bsie
lla s
pp.,
P. m
irab
ilis
– U
rine
isol
ates
am
pici
llin
Ora
l cep
halo
spor
ins3
ceftr
iaxo
ne5
Res
ista
nt to
cef
triax
one
erta
pene
m a
nd im
ipen
em &
mer
open
em (˂
18
y.o)
Res
ista
nt to
erta
pene
m
imip
enem
, mer
open
em (≥
18
y.o)
ci
prof
loxa
cin(
>11
y.o.
)
ge
ntam
icin
R
esis
tant
to g
enta
mic
in
amik
acin
ni
trofu
rant
oin
pipe
raci
llin-
tazo
bact
am5
Res
ista
nt to
pip
erac
illin
-tazo
bact
am
erta
pene
m a
nd im
ipen
em &
mer
open
em (˂
18
y.o)
tri
met
hopr
im-s
ulfa
met
hoxa
zole
Res
ista
nt to
mer
open
em o
r im
ipen
em
cefta
zidi
me-
avib
acta
m &
col
istin
S
PIC
E o
rgan
ism
s2 – E
xclu
des
urin
e is
olat
es
cefe
pim
e5 R
esis
tant
to c
efep
ime
erta
pene
m a
nd im
ipen
em &
mer
open
em (˂
18
y.o)
ci
prof
loxa
cin
(>11
y.o
.) R
esis
tant
to e
rtape
nem
im
ipen
em, m
erop
enem
(≥ 1
8 y.
o)
gent
amic
in
Res
ista
nt to
gen
tam
icin
am
ikac
in, t
obra
myc
in
pipe
raci
llin-
tazo
bact
am5
Res
ista
nt to
pip
erac
illin
-tazo
bact
am
erta
pene
m a
nd im
ipen
em &
mer
open
em (˂
18
y.o)
tri
met
hopr
im-s
ulfa
met
hoxa
zole
Res
ista
nt to
mer
open
em o
r im
ipen
em
cefta
zidi
me-
avib
acta
m &
col
istin
S
PIC
E o
rgan
ism
s2 –
Urin
e is
olat
es
ampi
cilli
n
ce
fepi
me5
Res
ista
nt to
cef
epim
e er
tape
nem
and
imip
enem
& m
erop
enem
(˂ 1
8 y.
o)
cipr
oflo
xaci
n (>
11 y
.o.)
R
esis
tant
to e
rtape
nem
im
ipen
em, m
erop
enem
(≥ 1
8 y.
o)
gent
amic
in
Res
ista
nt to
gen
tam
icin
am
ikac
in
nitro
fura
ntoi
n
pi
pera
cilli
n-ta
zoba
ctam
5 R
esis
tant
to p
iper
acill
in-ta
zoba
ctam
er
tape
nem
and
imip
enem
& m
erop
enem
(˂ 1
8 y.
o)
trim
etho
prim
-sul
fam
etho
xazo
le
R
esis
tant
to m
erop
enem
or i
mip
enem
ce
ftazi
dim
e-av
ibac
tam
& c
olis
tin
1 Th
e fo
llow
ing
antim
crob
ial a
gent
s ar
e re
porte
d on
car
bape
nem
reis
tant
gra
m-n
egat
ive
rods
(res
ista
nt to
mer
open
em a
nd/o
r im
ipen
em):
Fosf
omyc
in,
Min
ocyc
line,
Mox
iflox
acin
, Col
istin
, Tig
ecyc
line,
Cef
tazi
dim
e-av
ibac
tam
and
Cef
tolo
zane
-taze
obac
tam
.
2 E
nter
obac
teria
ceae
oth
er th
an E
. col
i, K
lebs
iella
spp
., P
. mira
bilis
, Sal
mon
ella
spp
., S
hige
lla s
pp.
3 C
efaz
olin
resu
lts s
houl
d on
ly b
e us
ed to
pre
dict
pot
entia
l effe
ctiv
enes
s of
ora
l cep
halo
spor
ins
for u
ncom
plic
ated
UTI
s.
4 C
olis
tin is
not
repo
rted
on S
erra
tia m
arce
sens
, Pro
teiu
s sp
p., P
rovi
denc
ia s
pp. a
nd M
orga
nella
mor
gani
i bec
ause
thes
e or
gani
sms
are
inte
rmed
iate
/resi
stan
t to
colis
tin.
5 If
resu
lt is
inte
rmed
iate
(I) o
r res
ista
nt (R
): er
tape
nem
, im
ipen
em (≤
18
y.o.
) and
mer
open
em (≤
18
y.o.
) are
repo
rted.
37
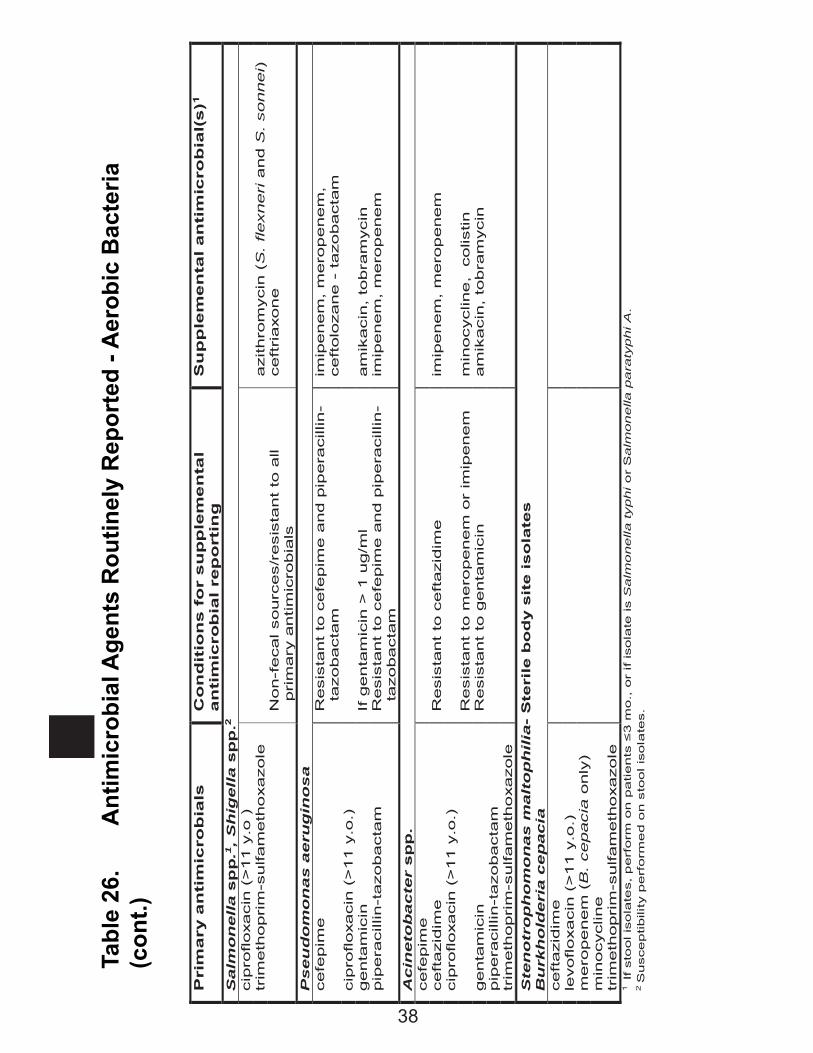
Tabl
e 26
.
Ant
imic
robi
al A
gent
s R
outin
ely
Rep
orte
d - A
erob
ic B
acte
ria
(con
t.)
Pri
ma
ry a
nti
mic
rob
ials
C
on
dit
ion
s f
or
su
pp
lem
en
tal
an
tim
icro
bia
l re
po
rtin
g
Su
pp
lem
en
tal a
nti
mic
rob
ial(
s)1
Salm
on
ell
a s
pp
.1,
Sh
igell
a s
pp
.2
cip
rofloxacin
(>
11 y
.o )
tr
imeth
opri
m-s
ulfam
eth
oxazole
azithro
mycin
(S
. flexneri
and S
. sonnei)
Non-f
ecal sourc
es/r
esis
tant
to a
ll
pri
mary
antim
icro
bia
ls
ceft
riaxon
e
Pseu
do
mo
nas a
eru
gin
os
a
cefe
pim
e
Resis
tant
to c
efe
pim
e a
nd p
ipera
cill
in-
ta
zobacta
m
imip
enem
, m
ero
penem
, ceft
olo
zane -
tazo
bacta
m
cip
rofloxacin
(>
11 y
.o.)
genta
mic
in
If g
enta
mic
in >
1 u
g/m
l am
ikacin
, to
bra
mycin
pip
era
cill
in-t
azobacta
m
Resis
tant
to c
efe
pim
e a
nd p
ipera
cill
in-
ta
zobacta
m
imip
enem
, m
ero
penem
Acin
eto
ba
cte
r sp
p.
cefe
pim
e
ceft
azid
ime
Resis
tant
to c
eft
azid
ime
im
ipenem
, m
ero
penem
cip
rofloxacin
(>
11 y
.o.)
Resis
tant
to m
ero
penem
or
imip
enem
m
inocyclin
e,
colis
tin
genta
mic
in
Resis
tant
to g
enta
mic
in
am
ikacin
, to
bra
mycin
pip
era
cill
in-t
azobacta
m
trim
eth
opri
m-s
ulfam
eth
oxazole
S
ten
otr
op
ho
mo
nas m
alt
op
hil
ia-
Ste
rile
bo
dy s
ite i
so
late
s
Bu
rkh
old
eri
a c
ep
acia
ceft
azid
ime
levoflo
xacin
(>
11 y
.o.)
m
ero
pe
nem
(B
. cepacia
only
)
m
inocyclin
e
trim
eth
opri
m-s
ulfam
eth
oxazole
1 If s
tool is
ola
tes, p
erf
orm
on p
atients
≤3 m
o., o
r if isola
te is S
alm
onella typhi o
r S
alm
on
ella
pa
raty
phi A
. 2 S
usceptibili
ty p
erf
orm
ed o
n s
tool is
ola
tes.
38
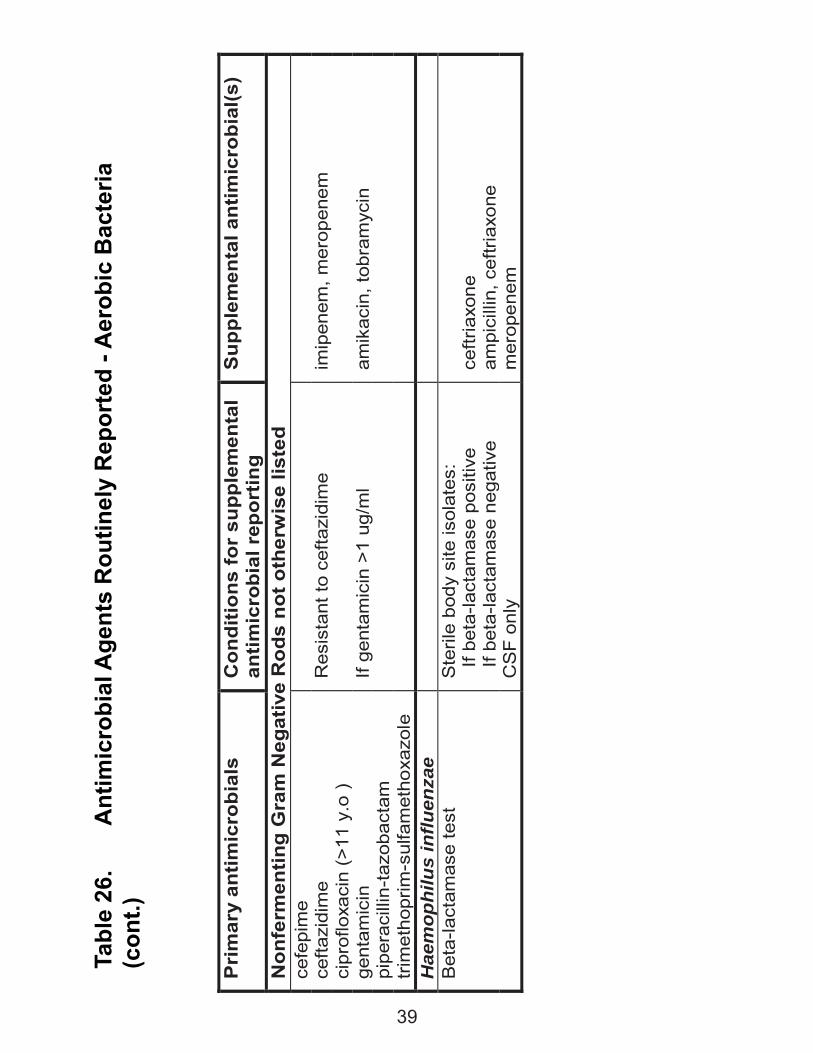
Tabl
e 26
.
Ant
imic
robi
al A
gent
s R
outin
ely
Rep
orte
d - A
erob
ic B
acte
ria
(con
t.)
Pri
mar
y an
timic
robi
als
Con
ditio
ns fo
r su
pple
men
tal
antim
icro
bial
rep
ortin
g S
uppl
emen
tal a
ntim
icro
bial
(s)
Non
ferm
entin
g G
ram
Neg
ativ
e R
ods
not o
ther
wis
e lis
ted
ce
fepi
me
cefta
zidi
me
Res
ista
nt to
cef
tazi
dim
e
imip
enem
, mer
open
em
cipr
oflo
xaci
n (>
11 y
.o )
ge
ntam
icin
If
gent
amic
in >
1 ug
/ml
amik
acin
, tob
ram
ycin
pi
pera
cilli
n-ta
zoba
ctam
tr
imet
hopr
im-s
ulfa
met
hoxa
zole
H
aem
ophi
lus
influ
enza
e
B
eta-
lact
amas
e te
st
Ste
rile
body
site
isol
ates
: I
f bet
a-la
ctam
ase
posi
tive
If b
eta-
lact
amas
e ne
gativ
e
ceftr
iaxo
ne
ampi
cilli
n, c
eftri
axon
e
CS
F on
ly
mer
open
em
39
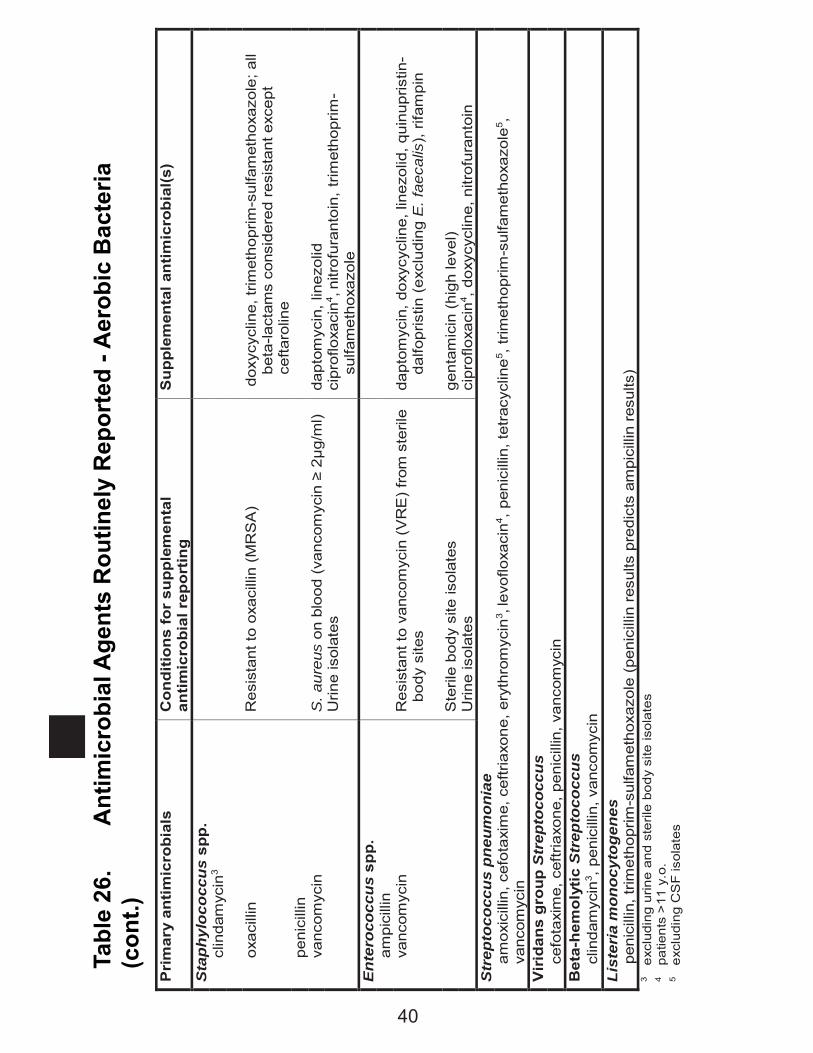
Tabl
e 26
.
Ant
imic
robi
al A
gent
s R
outin
ely
Rep
orte
d - A
erob
ic B
acte
ria
(con
t.)
Pri
mar
y an
timic
robi
als
Con
ditio
ns fo
r su
pple
men
tal
antim
icro
bial
rep
ortin
g S
uppl
emen
tal a
ntim
icro
bial
(s)
Sta
phyl
ococ
cus
spp.
cl
inda
myc
in3
ox
acill
in
Res
ista
nt to
oxa
cilli
n (M
RS
A)
do
xycy
clin
e, tr
imet
hopr
im-s
ulfa
met
hoxa
zole
; all
beta
-lact
ams
cons
ider
ed r
esis
tant
exc
ept
cefta
rolin
e pe
nici
llin
vanc
omyc
in
S. a
ureu
s on
blo
od (
vanc
omyc
in ≥
2μg
/ml)
dapt
omyc
in, l
inez
olid
Urin
e is
olat
es
ci
prof
loxa
cin4 ,
nitr
ofur
anto
in, t
rimet
hopr
im-
sulfa
met
hoxa
zole
E
nter
ococ
cus
spp.
am
pici
llin
vanc
omyc
in
Res
ista
nt to
van
com
ycin
(V
RE
) fr
om s
teril
e bo
dy s
ites
dapt
omyc
in, d
oxyc
yclin
e, li
nezo
lid, q
uinu
pris
tin-
dalfo
pris
tin (
excl
udin
g E
. fae
calis
), r
ifam
pin
S
teril
e bo
dy s
ite is
olat
es
gent
amic
in (
high
leve
l)
Urin
e is
olat
es
cipr
oflo
xaci
n4 , d
oxyc
yclin
e, n
itrof
uran
toin
S
trep
toco
ccus
pne
umon
iae
amox
icill
in, c
efot
axim
e, c
eftr
iaxo
ne, e
ryth
rom
ycin
3 , le
voflo
xaci
n4 , p
enic
illin
, tet
racy
clin
e5 , tr
imet
hopr
im-s
ulfa
met
hoxa
zole
5 ,
vanc
omyc
in
Vir
idan
s gr
oup
Str
epto
cocc
us
c
efot
axim
e, c
eftr
iaxo
ne, p
enic
illin
, van
com
ycin
B
eta-
hem
olyt
ic S
trep
toco
ccus
clin
dam
ycin
3 , p
enic
illin
, van
com
ycin
Li
ster
ia m
onoc
ytog
enes
pen
icill
in, t
rimet
hopr
im-s
ulfa
met
hoxa
zole
(pe
nici
llin
resu
lts p
redi
cts
ampi
cilli
n re
sults
) 3
exc
ludi
ng u
rine
and
ster
ile b
ody
site
isol
ates
4
pat
ient
s >
11 y
.o.
5 e
xclu
ding
CS
F is
olat
es
40
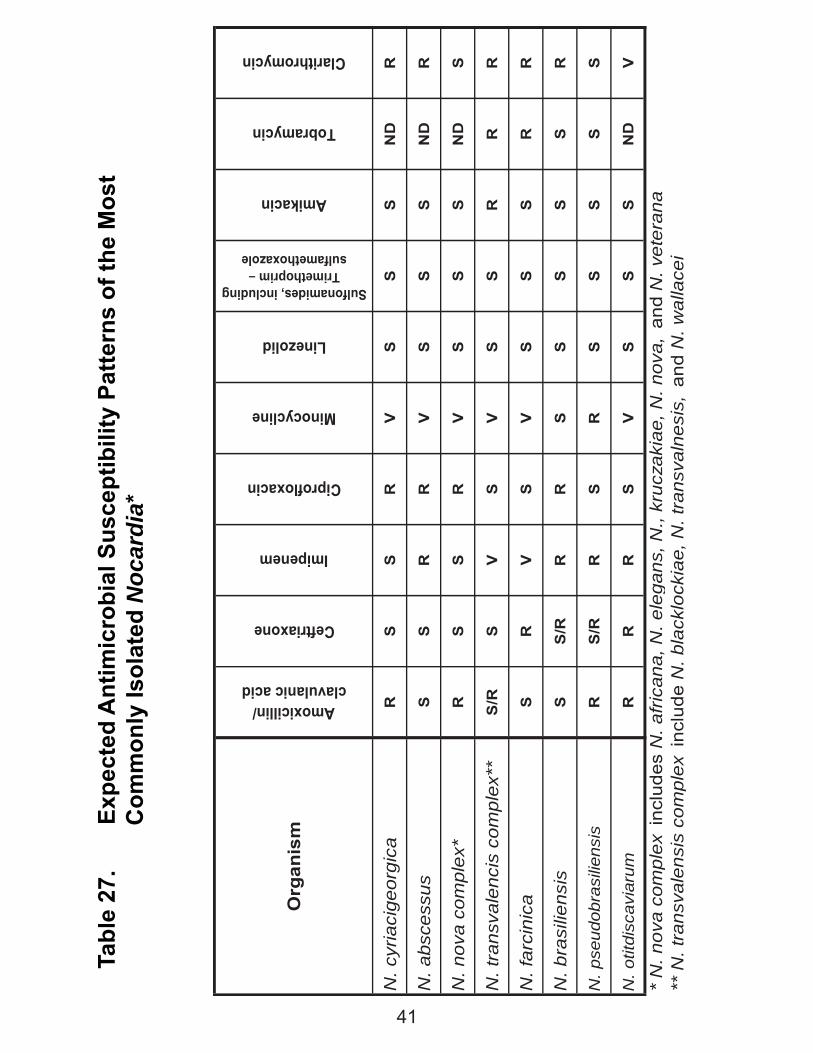
Tabl
e 27
.
Exp
ecte
d A
ntim
icro
bial
Sus
cept
ibili
ty P
atte
rns
of th
e M
ost
C
omm
only
Isol
ated
Noc
ardi
a*
Org
anis
m
Amoxicillin/ clavulanic acid
Ceftriaxone
Imipenem
Ciprofloxacin
Minocycline
Linezolid
Sulfonamides, including Trimethoprim –
sulfamethoxazole
Amikacin
Tobramycin
Clarithromycin
N. c
yria
cige
orgi
caR
SS
RV
SS
SN
DR
N. a
bsce
ssus
SS
RR
VS
SS
ND
R
N. n
ova
com
plex
*R
SS
RV
SS
SN
DS
N. t
rans
vale
ncis
com
plex
**S
/RS
VS
VS
SR
RR
N. f
arci
nica
SR
VS
VS
SS
RR
N. b
rasi
liens
isS
S/R
RR
SS
SS
SR
N. p
seud
obra
silie
nsis
RS
/RR
SR
SS
SS
S
N. o
titdi
scav
iaru
mR
RR
SV
SS
SN
DV
* N
. nov
a co
mpl
ex i
nclu
des
N. a
fric
ana,
N. e
lega
ns, N
., kr
ucza
kiae
, N. n
ova,
and
N. v
eter
ana
** N
. tra
nsva
lens
is c
ompl
ex i
nclu
de N
. bla
cklo
ckia
e, N
. tra
nsva
lnes
is,
and
N. w
alla
cei
41
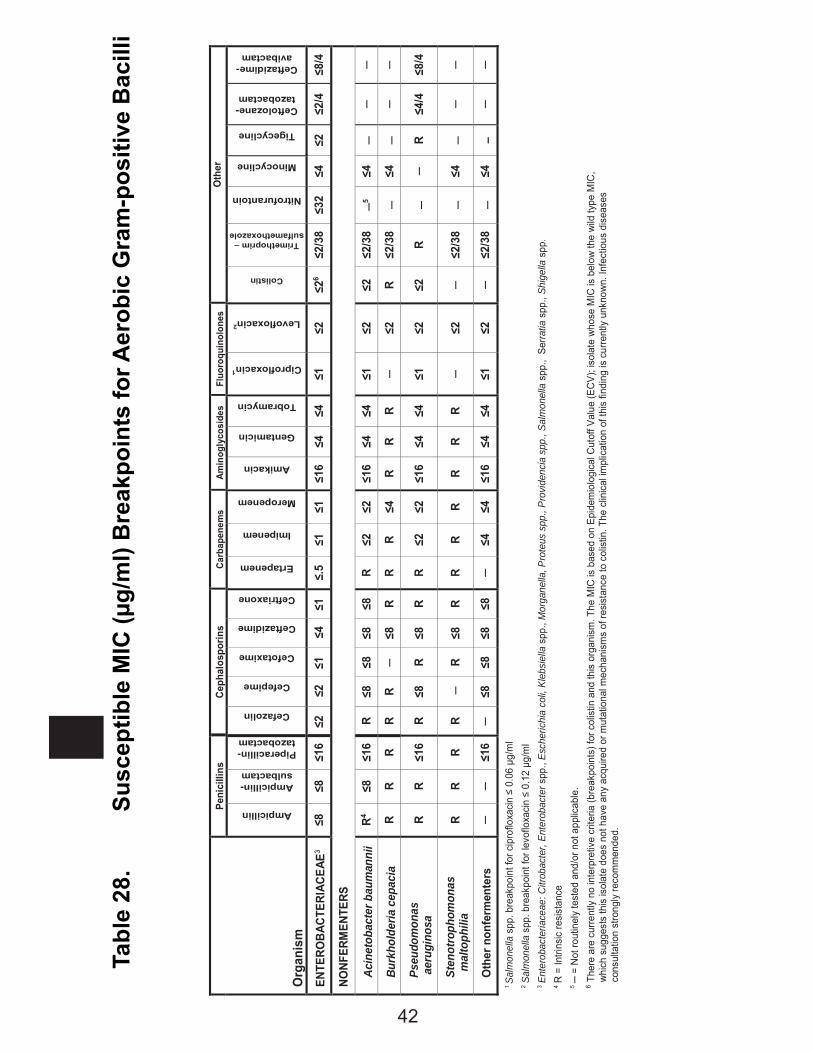
Tabl
e 28
.
S
usce
ptib
le M
IC (μ
g/m
l) B
reak
poin
ts fo
r Aer
obic
Gra
m-p
ositi
ve B
acill
i
Org
anis
m
Peni
cilli
ns
Ceph
alos
porin
s Ca
rbap
enem
s Am
inog
lyco
side
s Fl
uoro
quin
olon
es
Oth
er
Ampicillin
Ampicillin-sulbactam
Piperacillin-tazobactam
Cefazolin
Cefepime
Cefotaxime
Ceftazidime
Ceftriaxone
Ertapenem
Imipenem
Meropenem
Amikacin
Gentamicin
Tobramycin
Ciprofloxacin1
Levofloxacin2
Colistin
Trimethoprim – sulfamethoxazole
Nitrofurantoin
Minocycline
Tigecycline
Ceftolozane-tazobactam
Ceftazidime-avibactam
ENTE
ROBA
CTER
IACE
AE3
≤8
≤8
≤16
≤2
≤2
≤1
≤4
≤1
≤.5
≤1
≤1
≤16
≤4
≤4
≤1
≤2
≤26
≤2/3
8 ≤3
2 ≤4
≤2
≤2
/4
≤8/4
NONF
ERM
ENTE
RS
Ac
inet
obac
ter b
aum
anni
i R4
≤8
≤16
R ≤8
≤8
≤8
≤8
R
≤2
≤2
≤16
≤4
≤4
≤1
≤2
≤2
≤2/3
8 ─5
≤4
─ ─
─
Burk
hold
eria
cep
acia
R
R R
R R
─ ≤8
R
R R
≤4
R R
R ─
≤2
R ≤2
/38
─ ≤4
─
─ ─
Ps
eudo
mon
as
aer
ugin
osa
R R
≤16
R ≤8
R
≤8
R R
≤2
≤2
≤16
≤4
≤4
≤1
≤2
≤2
R ─
─ R
≤4/4
≤8
/4
St
enot
roph
omon
as
m
alto
phili
a R
R R
R ─
R ≤8
R
R R
R R
R R
─ ≤2
─
≤2/3
8 ─
≤4
─ ─
─
O
ther
non
ferm
ente
rs
─ ─
≤16
─ ≤8
≤8
≤8
≤8
─
≤4
≤4
≤16
≤4
≤4
≤1
≤2
─ ≤2
/38
─ ≤4
–
─ ─
1 Sa
lmon
ella
spp
. bre
akpo
int f
or c
ipro
floxa
cin ≤
0.06
μg/
ml
2 Sal
mon
ella
spp
. bre
akpo
int f
or le
voflo
xaci
n ≤
0.12
μg/
ml
3 Ent
erob
acte
riace
ae: C
itrob
acte
r, En
tero
bact
er s
pp.,
Esch
eric
hia
coli,
Kle
bsie
lla s
pp.,
Mor
gane
lla, P
rote
us s
pp.,
Prov
iden
cia
spp.
, Sal
mon
ella
spp
., S
erra
tia s
pp.,
Shig
ella
spp
. 4 R
= In
trins
ic re
sist
ance
5 ─
= N
ot ro
utin
ely
test
ed a
nd/o
r not
app
licab
le.
6 The
re a
re c
urre
ntly
no
inte
rpre
tive
crite
ria (b
reak
poin
ts) f
or c
olis
tin a
nd th
is o
rgan
ism
. The
MIC
is b
ased
on
Epid
emio
logi
cal C
utof
f Val
ue (E
CV)
; iso
late
who
se M
IC is
bel
ow th
e wi
ld ty
pe M
IC,
whi
ch s
ugge
sts
this
isol
ate
does
not
hav
e an
y ac
quire
d or
mut
atio
nal m
echa
nism
s of
resi
stan
ce to
col
istin
. The
clin
ical
impl
icat
ion
of th
is fi
ndin
g is
cur
rent
ly u
nkno
wn.
Infe
ctio
us d
isea
ses
cons
ulta
tion
stro
ngly
reco
mm
ende
d.
42
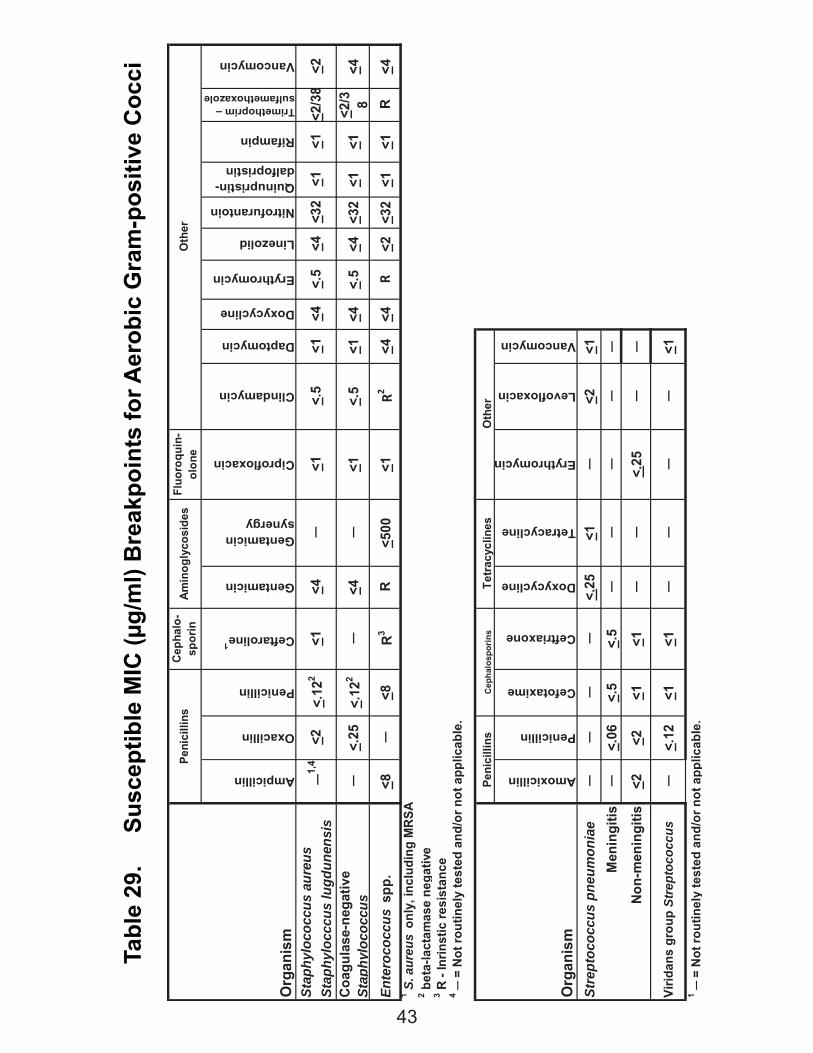
Tabl
e 29
.
Susc
eptib
le M
IC (μ
g/m
l) B
reak
poin
ts fo
r Aer
obic
Gra
m-p
ositi
ve C
occi
Fluo
roqu
in-
olon
e
Org
anis
mAmpicillin
Oxacillin
Penicillin
Ceftaroline1
Gentamicin
Gentamicin synergy
Ciprofloxacin
Clindamycin
Daptomycin
Doxycycline
Erythromycin
Linezolid
Nitrofurantoin
Quinupristin-dalfopristin
Rifampin
Trimethoprim – sulfamethoxazole
Vancomycin
Stap
hylo
cocc
us a
ureu
sSt
aphy
locc
cus
lugd
unen
sis
Coa
gula
se-n
egat
ive
Stap
hylo
cocc
us─
<.25
<.12
2─
<4─
<1<.
5<1
<4<.
5<4
<32
<1<1
<2/3 8
<4
Ente
roco
ccus
spp
.<8
─<8
R3
R<5
00<1
R2<4
<4R
<2<3
2<1
<1R
<4
2 bet
a-la
ctam
ase
nega
tive
Org
anis
m
Amoxicillin
Penicillin
Cefotaxime
Ceftriaxone
Doxycycline
Tetracycline
Erythromycin
Levofloxacin
Vancomycin
Stre
ptoc
occu
s pn
eum
onia
e─
──
─<.
25<1
─<2
<1 M
enin
gitis
─<.
06<.
5<.
5─
──
──
N
on-m
enin
gitis
<2<2
<1<1
──
<.25
──
Virid
ans
grou
p St
rept
ococ
cus
─<.
12<1
<1─
──
─<1
1 ─ =
Not
rout
inel
y te
sted
and
/or n
ot a
pplic
able
.
Ceph
alos
porin
s
1 S. a
ureu
s on
ly, i
nclu
ding
MR
SA
<.5
Peni
cilli
nsC
epha
lo-
spor
in
Peni
cilli
ns
─
1,4
Oth
er
<1<4
<2<4
<.5
<4<3
2<1
Tetr
acyc
lines
Oth
er
<2
Amin
ogly
cosi
des
4 ─ =
Not
rout
inel
y te
sted
and
/or n
ot a
pplic
able
.
<1<1
<1<2
/38
<.12
2─
3 R -
Inrin
stic
resi
stan
ce
43
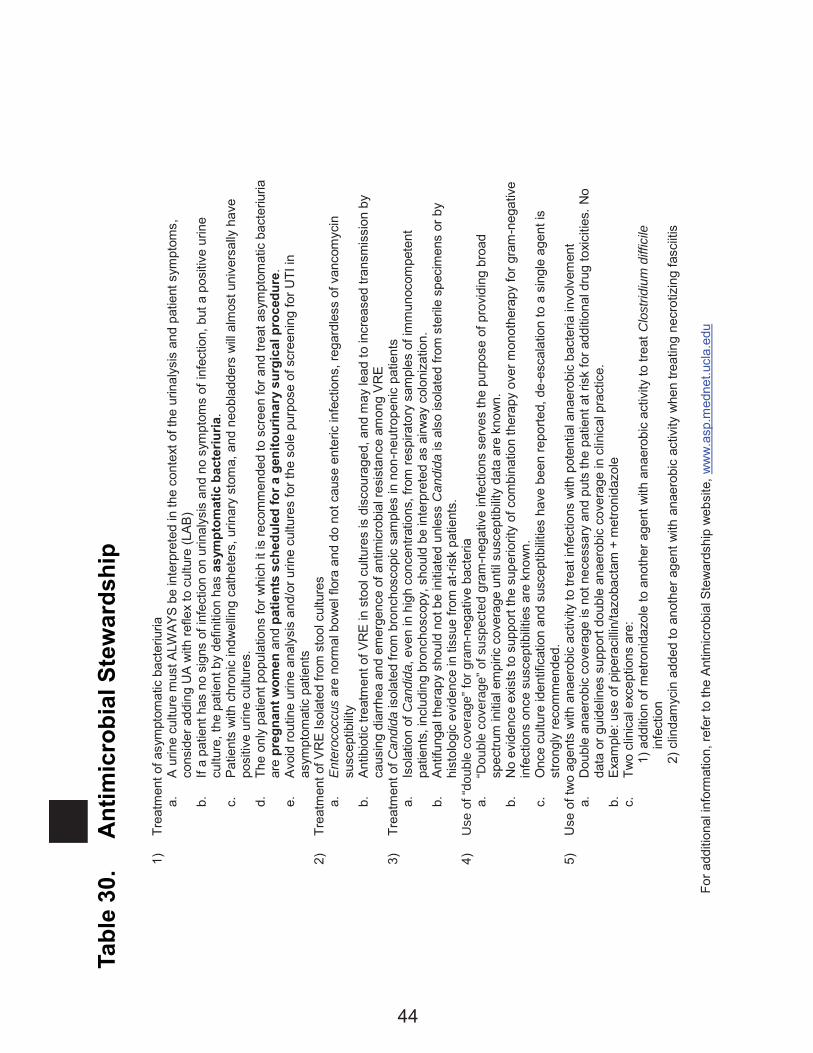
Tabl
e 30
.
Ant
imic
robi
al S
tew
ards
hip
1)
Tr
eatm
ent o
f asy
mpt
omat
ic b
acte
riuria
a.
A
urin
e cu
lture
mus
t ALW
AYS
be
inte
rpre
ted
in th
e co
ntex
t of t
he u
rinal
ysis
and
pat
ient
sym
ptom
s,
cons
ider
add
ing
UA
with
refle
x to
cul
ture
(LA
B)
b.
If a
patie
nt h
as n
o si
gns
of in
fect
ion
on u
rinal
ysis
and
no
sym
ptom
s of
infe
ctio
n, b
ut a
pos
itive
urin
e cu
lture
, the
pat
ient
by
defin
ition
has
asy
mpt
omat
ic b
acte
riuria
. c.
P
atie
nts
with
chr
onic
indw
ellin
g ca
thet
ers,
urin
ary
stom
a, a
nd n
eobl
adde
rs w
ill a
lmos
t uni
vers
ally
hav
e po
sitiv
e ur
ine
cultu
res.
d.
Th
e on
ly p
atie
nt p
opul
atio
ns fo
r whi
ch it
is re
com
men
ded
to s
cree
n fo
r and
trea
t asy
mpt
omat
ic b
acte
riuria
ar
e pr
egna
nt w
omen
and
pat
ient
s sc
hedu
led
for a
gen
itour
inar
y su
rgic
al p
roce
dure
. e.
A
void
rout
ine
urin
e an
alys
is a
nd/o
r urin
e cu
lture
s fo
r the
sol
e pu
rpos
e of
scr
eeni
ng fo
r UTI
in
asym
ptom
atic
pat
ient
s 2)
Tr
eatm
ent o
f VR
E Is
olat
ed fr
om s
tool
cul
ture
s a.
E
nter
ococ
cus
are
norm
al b
owel
flor
a an
d do
not
cau
se e
nter
ic in
fect
ions
, reg
ardl
ess
of v
anco
myc
in
susc
eptib
ility
b.
Ant
ibio
tic tr
eatm
ent o
f VR
E in
sto
ol c
ultu
res
is d
isco
urag
ed, a
nd m
ay le
ad to
incr
ease
d tra
nsm
issi
on b
y ca
usin
g di
arrh
ea a
nd e
mer
genc
e of
ant
imic
robi
al re
sist
ance
am
ong
VR
E
3)
Trea
tmen
t of C
andi
da is
olat
ed fr
om b
ronc
hosc
opic
sam
ples
in n
on-n
eutro
peni
c pa
tient
s a.
Is
olat
ion
of C
andi
da, e
ven
in h
igh
conc
entra
tions
, fro
m re
spira
tory
sam
ples
of i
mm
unoc
ompe
tent
pa
tient
s, in
clud
ing
bron
chos
copy
, sho
uld
be in
terp
rete
d as
airw
ay c
olon
izat
ion.
b.
A
ntifu
ngal
ther
apy
shou
ld n
ot b
e in
itiat
ed u
nles
s C
andi
da is
als
o is
olat
ed fr
om s
teril
e sp
ecim
ens
or b
y hi
stol
ogic
evi
denc
e in
tiss
ue fr
om a
t-ris
k pa
tient
s.
4)
Use
of “
doub
le c
over
age”
for g
ram
-neg
ativ
e ba
cter
ia
a.
“Dou
ble
cove
rage
” of s
uspe
cted
gra
m-n
egat
ive
infe
ctio
ns s
erve
s th
e pu
rpos
e of
pro
vidi
ng b
road
sp
ectru
m in
itial
em
piric
cov
erag
e un
til s
usce
ptib
ility
data
are
kno
wn.
b.
N
o ev
iden
ce e
xist
s to
sup
port
the
supe
riorit
y of
com
bina
tion
ther
apy
over
mon
othe
rapy
for g
ram
-neg
ativ
e in
fect
ions
onc
e su
scep
tibilit
ies
are
know
n.
c.
Onc
e cu
lture
iden
tific
atio
n an
d su
scep
tibilit
ies
have
bee
n re
porte
d, d
e-es
cala
tion
to a
sin
gle
agen
t is
stro
ngly
reco
mm
ende
d.
5)
Use
of t
wo
agen
ts w
ith a
naer
obic
act
ivity
to tr
eat i
nfec
tions
with
pot
entia
l ana
erob
ic b
acte
ria in
volv
emen
t a.
D
oubl
e an
aero
bic
cove
rage
is n
ot n
eces
sary
and
put
s th
e pa
tient
at r
isk
for a
dditi
onal
dru
g to
xici
ties.
No
data
or g
uide
lines
sup
port
doub
le a
naer
obic
cov
erag
e in
clin
ical
pra
ctic
e.
b.
Exa
mpl
e: u
se o
f pip
erac
illin
/tazo
bact
am +
met
roni
dazo
le
c.
Two
clin
ical
exc
eptio
ns a
re:
1) a
dditi
on o
f met
roni
dazo
le to
ano
ther
age
nt w
ith a
naer
obic
act
ivity
to tr
eat C
lost
ridiu
m d
iffic
ile
infe
ctio
n
2) c
linda
myc
in a
dded
to a
noth
er a
gent
with
ana
erob
ic a
ctiv
ity w
hen
treat
ing
necr
otiz
ing
fasc
iitis
For a
dditi
onal
info
rmat
ion,
refe
r to
the
Ant
imic
robi
al S
tew
ards
hip
web
site
, ww
w.a
sp.m
edne
t.ucl
a.ed
u
44

UCLA Form 3819 (6/17)
Resources at UCLA through the Antimicrobial Stewardship Program
(ASP) The Antimicrobial Stewardship Program (ASP) has made resources available for the sole purpose of improving clinical outcomes of patients with infections. Questions and guidance on interpretation of culture reports (contaminant/pathogen), drug dosing, etc. are welcome. The ASP can be contacted numerous ways, depending on the urgency and clinical needs: ASP helpdesk: (310) 267-7567 Email: [email protected] Website: http://www.asp.mednet.ucla.edu Note that the website has a guidebook, with detailed information about specific clinical syndromes, interpretation of microbiology reports, and guidelines for treatment. eConsult: http://www.asp.mednet.ucla.
edu/pages/econsult We encourage you to reach out to the program with questions. The program is staffed by Dr. Daniel Uslan (ID), Dr. Elise Martin (ID), Dr. Christine Pham (Pharm – SM ), Dr. Jennifer Curello (Pharm – RR), and Dr. Meganne Kanatani (Pharm – RR).
Tables 1-4 Adults Tables 5-8 Adults/Peds
Tables 9-11 Peds
Tables 12 Yeasts
Tables 13-16 Emerging Restist. Concerns
Tables 17-23 Misc
Tables 24-29 Lab Info
Table 30 Antimicrobial Stewardship Program
RapidReference