Embed Size (px)
Citation preview

Musings on Antimicrobial Susceptibility Testingand Antibiotic Review
(AST for the bench tech)
24 Mar 17
George Kallstrom

Disclosures
None, although this is the second time in two years a volunteered SCACM talk was either altered or content restricted.

When should you tell someone about a resistant isolate?
• Vancomycin, linezolid, daptomycin resistant Gram positive organisms.
• Carbapenem or colistin resistant Gram negative organisms.
• Beta hemolytic strep resistant to any beta lactam.
• When all or nearly all tested antibiotics are resistant.
• When something does not look right.

What Gram negatives are colistin R?
• Burkholderia spp
• Ralstonia spp
• Proteus spp
• Providencia spp
• Serratia spp
• Edwardsiella spp
• Brucella spp
• Aerobic Gram negative cocci

What Gram positives are vanco R?
Lactobacillus spp
Pediococcus spp (a food additive!)
Weisiella spp
Leuconostoc spp
Erysipelothrix spp
VanC enterococci (E. gallolyticus/casseliflavus)

Did you know?
• 60-65% of monomicrobial serious infections treated with a single antibiotic testing resistant to the antibiotic will respond to therapy.
• 90% of monomicrobial infections will respond to an antibiotic if sensitive.
• Nearly all uncomplicated UTIs will respond to almost any therapy able to concentrate in urine (even if resistant).
• The inherent variability of AST testing?

• There are no great data correlating AST and clinical outcome for polymicrobial infections.
• There are no great data correlating AST and clinical outcome for infections treated with multiple antibiotics.
• There are no great data correlating clinical outcome and AST for infections treated with oral agents.
• There are no great data correlating clinical outcome and AST for infections where antibiotics do not readily achieve normal concentration (diabetic feet, pressure ulcers).
So why do we bother with all of this AST testing?
Did you know?

Minimum Inhibitory Concentration
Antibiotic MIC
Ampicillin 4
Ceazolin 1
What is the MIC of Ampicillin?
What is the MIC of Cefazolin?
Do your ID docs get concerned when an MIC goes from 1 to 2?

Minimum Inhibitory Concentrations
Lowest concentration of an antibiotic that prevents
visible evidence of growth after 20-24 h exposure = MIC
Broth Dilution

MIC
MICs are determined from steady state serum concentrations of IV drug. Great for monomicrobial BSIs, but…
– What are drug concentrations in an area where there is poor circulation (diabetic feet)?
– What is the drug concentration in a biofilm in a CF/COPD lung?
I’m sure you could think of many other scenarios.

S, I, R, NS, SDD
• Do you report SIR only?
• Do you include MIC?
• Do you report NS or SDD, how content are your providers with the information provided?
• Epidemiological cutoff (not for use in clinical medicine, but just to differentiate wt from mutants), Shigella, Propi?
• Therapy comments?

Selective Reporting vs. all
• Should you suppress drugs?
• Do you suppress non-formulary drugs?
• Should you suppress less effective drugs?
• Should you suppress broader spectrum drugs if isolates are susceptible to more narrow or better agents?

Indicator Drugs
• Tetracycline for doxycycline/minocycline
• Penicillin/oxacillin in staph
• Penicillin Enterococci
• Erythromycin for macrolides
• Levofloxacin S. pneumo
• Cefazolin is an indicator for all oral cephalosporins
• Naladixic acid for fluoroquinolones in Salmonella

Viridans streps and anginosis
• Anginosis group are considered viridans strep (even if beta hemolytic)
• Viridans Streps are generally very susceptible to beta lactam antibiotics
• Anginosis group Streps (anginosis, constellatus, intermedius) tend to form abscesses.

Bad CSF drugs
• Oral only
• 1st/2nd cephs, cephamycins
• Clinda
• Macrolides
• Tetracyclines
• FQs

Do not report
• Daptomycin on respiratory isolates • Cephalosporins, clindamycin, TMP-SXT on
Enterococcus spp• On CSF isolates
– Oral drugs– 1st and 2nd generation cephalosporins– Clindamycin– Macrolides– Tetracyclines– Fluoroquinolones

Some drugs to never report as susceptible
• Klebsiella ampicillin
• Salmonella/Shigella 1st/2nd cephs, aminoglycosides
• Ox resistant SA-beta lactams except ceftaroline
• Enterococcus-aminoglycosides (except HLR), Cephs, clinda, TMP-SXT

Bauer-Kirby testing
• Very flexible
• Easy to modify as breakpoints are changed
• Great standardization
• Can take longer than automated systems (24h vs. ~8h)

Issues with B-K testing
• Improper concentrations of divalent cationscan cause issues with AST testing.
• pH issues
• Inoculum to light/heavy

Troubleshooting
• Disks losing potency (meropenem, clavulinic acid)
• Loss of plasmid
• S. pneumo
• All zones to large (light inoculum)
• All zones to small (to heavy inoculum)
• Same disk fails with multiple strains (disk problem)
• Single strain fails with single drug (maybe strain mutation)

E-test
E-test is not suitable for Cryptococcus neoformansE test has shown limitations with regard to C. jejuni agents
KPC – carbapenemsRead all colonies; 8 μg/mL
Candida spp. – read allmacrocolonies in the ellipse,(potential hetero-resistance);1 μg/mL
Bacteriostatic drugs – read at80 % inhibition; 0.032 μg/mL

Fosfomycin
• Can ignore some colonies in zone of e-test (<=5).
• Breakpoints are only for E. coli and E. faecalis.

Drug companies
• Hey, we have these e-tests/disks we will give you for free to test our new drug.
• We have already talked to your ID docs and they really want this testing available at your institution.
• Of course this is all for epidemiological purposes. We would never tell you to test RUO reagents on patients.

Some major Vitek Limitations
• Pip/tazo Pseudomonas Serratia
• Aztreonam Pseudomonas

Vitek Advanced Expert Rules
• Proprietary system to detect mechanisms of resistance.
• From my experience it tends to overcall resistance, particularly carbapenemresistance.

Phoenix Limitations
The Phoenix system suppresses from the final report the drugs with MIC values interpreted with a dash (‘-’) (susceptibility testing is not recommended as the species is a poor target for therapy with the drug) as well as with the acronym ‘IE’, which indicates that there is insufficient evidence that the species in question is a good target for therapy with the drug. In both cases, the MIC remains visible at the laboratory level.

Microscan Limitations
• Tigecycline, Doripenem on a few GNRs.
• Some organisms required manual reading.
• Elevated MICs if overinoculated.
• Reduced MICs if underinoculated.
• Azithromycin

Broth microdilution
• Trailing growth for some bugs/drugs Gram positives Strep/Staph.

Colistin testing
• Colistin is a large molecule, unable to diffuse well.
• Colistin is absorbed by polystyrene, the material microwell plates are made of.
• Several studies have shown VMEs for colistincalling isolates sensitive when actually resistant.
EUCAST “The currently available gradient tests should be withdrawn from use!”

Colistin testing
• So what do you do for colistin testing?
– Nothing
– MIC microbroth only
– E-test
– Do you bill?
– Do you add a disclaimer?

MRSA discrepant results
• What do you do with mecA positive PCR, ox-S?
• How about fox-S, Pbp2a-pos?
• Or any other combination of discrepancy.

β-Lactam resistance
• bla genes destroy the β-Lactam ring inactivating the β-Lactam binding to the PBPs
• There are 4 classes of β-Lactamases (ABCD)
• > resistance when coupled w/ permeability and efflux mutations
• Modifications to the PBPs can cause resistance to β-Lactam antibiotics (Enterococcus faecium, S. aureus)

β-Lactam Resistance
• Penicillinase
• AmpC cephalosporinase
• Extended-spectrum β-lactamases
• Carbapenemases

Penicillin Resistance
• Staphylococcus aureus– Nearly all are pen R
• Streptococcus pneumoniae– Penicillin resistance:
• May also indicate resistant to 3rd gen. cephalo’s, so have to do MICs.
• Other streps: should not be pen resistant.– Confirm!
• Enterococcus faecium: always amp R– E. faecalis: usually sensitive

Beach test required in 2012 for confirmation of S. aureus and Pen-S
Fuzzy “beach” =β-lactamase negative Penicillin - S
Sharp “cliff” = β-lactamase positive Penicillin - R
Some question usefulness of this Test!

Mechanisms of resistance
According to CLSI-mechanism of resistance is uselessafter lowering breakpoints.
For “epidemiological” and historical perspective,let’s review quickly AmpC, ESBL, CRE as mechanism can often
be deduced from profile.

AmpC b-lactamases
• Chromosomally encoded.
• Inducible AmpC-Enterobacter spp, Citrobacter freundii, Serratia spp, Morganella spp Providencia spp
• Even E. coli (E.coli is low-level constitutive and not often derepressed).
• AmpC mutants are typically cephamycin resistant
• Several beta lactam drugs induce the AmpC gene which can drive resistance in vivo.

De-repression
• 20% of infections from non-urine Enterobacter infections can become de-repressed when on treatment with a 3rd generation cephalosporin.
• De-repressed isolates are resistant to 3rd
generation cephalosporins (ceftriaxone).
• Cefepime and the carbapenems retain activity to de-repressed AmpC strains.
Should you take a chance and treat a serious Enterobacter spp infection with a 3rd generation cephalosporin?

AmpC induction• Strong inducers include ampicillin and the
carbapenems.
• Mutations in the promoter can stably de-repress-turning production on at full speed (gas pedal to the floor).
• Third-generation cephalosporins (and beta lactamase inhibitors) are weak inducers and are susceptible to AmpC. This combination selects for mutations in the promoter to outgrow susceptible population (can occur as frequently as 10^5).

“This organism possesses an inducible beta-lactamase. For serious infections outside of the urinary tract, third generation cephalosporins may not be effective, even if test results indicate the organism is sensitive.”
AmpC comment in report
(at Summa we do not override results to R)

Citrobacter freundii antibiotic panel: a different approach
Drug Sensitivity
Ampicillin R
Cefoxitin R
Ceftazidime S
Ceftriaxone S
Cefepime S
Piperacillin/tazobactam S

Citrobacter freundii antibiotic panel: what should be reported?
Drug Sensitivity
Ampicillin R
Cefoxitin R
Ceftazidime S R
Ceftriaxone S R
Cefepime S
Piperacillin/tazobactam S
Another option to override the 3rd generation sensitivities; treatment with ceftaz orceftriaxone could lead to derepressed AmpC mutant.

ESBL
• “Extended spectrum beta-lactamase”
• Named because provide R to:
– Extended spectrum beta-lactams: 3rd gen. cephalo’s
• First appeared in early 1980’s, in E. coli and Kleb-most common, but also in all enterics.
• Despite previous CLSI recommendations

ESBL
• CTX-M Most common now-cefotaxime(ase)
• Now, CLSI has lowered breakpoints for 3rd gen. cephs
• In the past, tested by:
– Resistance to ceftazidime, with and without inhibitor
– Resistance to ceftriaxone, with and without inhibitor

• Resistance or intermediate to one or more third-generation cephalosporins.
• Cefoxitin and cefotetan susceptible.
• ESBL disk diffusion test (clavulanate inhibition)
– E-test ESBL strip or disk diffusion +/- inhibitor
– Confirmatory ESBL MIC test (Microscan)
• K. pneumoniae, K. oxytoca, E. coli, P. mirabilis
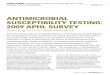
Laboratory detection of ESBLs

ESBL producer: >5 mm zone increase with inhibitor
CAZ CLA: ceftazidime with clavulanic acidCAZ: ceftazidime

ESBL comment on report
“This phenotype is suggestive of an ESBL-producing organism. Treatment with beta-lactam antibiotics other than carbapenems may not be effective. An ID consult may be warranted.”
At Summa, we override non-carbapenembeta-lactam antibiotics to R.

AmpC and ESBL comparison
AmpC ESBL
1st gen. ceph R R
2nd gen. ceph (cephamycin;cefoxitin or cefotetan)
R S
3rd gen. ceph R R
4th gen. ceph (cefepime) S S/R

Causes of carbapenem resistance in Gram-negative bacteria
• Porin (OprD) mutation +/- upregulated AmpC(Pseudomonas aeruginosa)
• Efflux + betalactamases• Metallo-beta-lactamases (MBL)
– Resistance to all carbapenems, but not monobactams– NDM, VIM, IMP
• KPC, Oxa48

Carbapenemases
• Dangerous!!!
• Usually plasmids, some chromosomal
• KPC, NDM
• R to pretty much all beta-lactamases
• Ertapenem is most sensitive indicator

Carbapenemase Classification
Molecular
ClassA B D
Aztreonam
Hydrolysis+ - -
EDTA
Inhibition- + -
Clavulanate
Inhibition
+ -

KPC• Molecular class A
• Inhibited by clavulanic acid but not by EDTA
• Confers resistance to ALL b-LACTAM antibiotics
• Plasmid-encoded
–Associated with other resistant genes (aminoglycosides, fluoroquinolones)
– Transferable

Definitive ID of a KPC Producer
PCR-The best method to confirm KPC, NDM. Some assays are including more targets, VIMs, IMPs, Oxa48 etc.
Carba-NP uses imipenem as a substrate with phenol red indicator and supernatant of suspected carbapenem strains.

Alternative Treatment for a KPC Producer
• Tigecycline
• Colistin
• Minocycline, Doxycycline
• Double carbapenems?

MBL’s
• Active site has Zn++ ions.
– Produce an oxyanionic attack on the β-lactam ring.
– Doesn’t form a covalent intermediate with the substrate (like a serine enzyme) so β-lactamaseinhibitors don’t work.
• No inhibitors of MBL’s have entered phase 1 trials in the past 20 years.

MBL’s• Substrates include all β-lactams except
monobactams.
• If resistance to azteonam is observed, it is likely due to an array of β-lactamases.

History of MBL’s
• Intrinsically found in Stenotrophomonas (L1)
• Later discovered in P. aeruginosa and Acinetobacter.
– IMP-1 first identified in P.a. in Japan in the early ’90’s.
• Now disseminating among Enterobacteriaceae.

NDM-1
• Newest MBL out of India and Pakistan (~2008).
• Plasmid that carries NDM-1 may carry resistance factors to macrolides, aminoglycosides, rifampicin, SXT.
• Found mostly in K. pneumoniae but also Enterobacteriaceae and Acinetobacter.
• Prevalence in India of NDM-1 in K. pneumo of 2-8%.

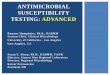
EDTA Inhibition
Erta/Mero +EDTA Erta/Mero no EDTA

Carbapenemase comment
“Suspected carbapenemase producing organism (CRE). Carbapenem drugs such as imipenem, meropenem, doripenem, and ertapenem may not be effective. An ID consult may be warranted.”
(beta-lactam drugs are overridden to R)

When to Suspect a Producer
• Resistance to extended spectrum cephalosporins (cefotaxime, ceftazidime, ceftriaxone)
• Variable susceptibility to cephamycins (cefoxitin, cefotetan)
• Meropenem >0.5 g/ml. Both Erta and Imihave some major problems overcalling at low, but elevated MICs.

Is this a carbapenemase?
E. coli
• Ampicillin S• Pip/tazo S• Cefazolin S• Cefoxitin S• Cefotaxime S• Ceftazidime S• Ceftriaxone S• Aztreonam S
• Cefepime S
• Imipenem R
• Meropenem S
• Ertapenem S
• Gentamycin S
• Ciprofloxacin S
• TMP-SXT S

PPM & Carbapenems
• Proteus, Providencia and Morganella
• Have elevated MICs to Imipenem
• Can also have slight increases in MIC to Ertapenem
• Typically not CRE

Would you consider this a suspected carbapenemase?
Providencia rettgeri
• Ampicillin R• Pip/tazo S• Cefazolin R• Cefoxitin S• Cefotaxime S• Ceftazidime S• Ceftriaxone S• Aztreonam S
• Cefepime S
• Imipenem R
• Meropenem S
• Ertapenem I
• Gentamycin R
• Ciprofloxacin S
• TMP-SXT S

ID of a KPC Producer
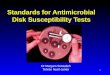
• Modified Hodge test
– 100% sensitive to detect KPC, not 100% specific!!!!!
meropenem ertapenem imipenem
pos
neg
neg
neg
pos
pos
Janet Hindler, What’s New in the 2008 CLSI Standards for (AST)?
•Streak Susceptible E. coli (ATCC 25922) to create lawn.•Place carbapenem disk in center.•Streak test isolates from edge of disk to end of plate.•Look for growth of E. coli around test isolate streak - indicates carbapenem-hydrolyzing enzyme.

De-repressed AmpC Enterobacter
produces false positive results with modified Hodge test

Inhibitors of Cell Wall Synthesis
• b-Lactam antibiotics
• Glycopeptide antibiotics
– Vancomycin

b-Lactam antibiotics
• Bind to penicillin-binding proteins of bacteria
• Cause rupture, cell death

β-Lactam antibiotics
• Inhibit cell wall synthesis.
• NAG and NAM are linked through transpeptidases called PBPs & make peptidoglycan.
• β-Lactam antibiotics inhibit transpeptidation by binding to the PBPs (bactericidal).
• Broad spectrum of activity.

Some β-Lactam antibiotics
• Penicillins• Cephalosporins• Carbapenems• Monobactamsβ-Lactamase inhibitors (suicide inhibitors-stably bind β-
Lactamases) are often used with the β-Lactam antibiotics.Clavulanate (Amox/Ticar-Calv), Sulbactam* (Amp-Sul),
Tazobactaom (Pip-Tazo, Ceftolozane-Tazo), Avibactam(Ceftaz-Avibac)
*Sulbactam alone can inhibit A. baumanii, Burkholderia spp & some Neisseria spp

Affect of Penicillin

Penicillins
Resistance often due to PENICILLINASE
• Pen G– Intramuscular or IV
– Commonly used for:
Syphilis
– Sometimes
Group A strep infections
• Pen V– Oral
– Group A strep infections
• Ampicillin– Oral or IV
– Enterococci
– Listeria monocytogenes
– Sinusitis, otitis media, urinary tract infections
• Amoxicillin– Only oral
– Sinusitis, otitis media, urinary tract infections

Penicillins
Resistance often due to PENICILLINASE
• Oxacillin– IV
– Sometimes used for S. aureus
• Piperacillin– IV
– “Extended spectrum penicillin”
• Some Gram-negative activity (Pseudomonas)

Penicillin/Inhibitor combo
Inhibitor: designed to counteract beta-lactamase
• Ampicillin/sulbactam– “Unasyn”
– IV
– Decent for:• Sensitive S. aureus
• Enterics
• Anaerobes
• Many types of infections– Soft tissue
– Human bites, animal bites
– Respiratory tract
– Urinary tract
• Amoxicillin/clavulanic acid– “Augmentin”
– Oral
– Sinus infections, otitis media, skin infections
– Human and animal bites
• Piperacillin/tazobactam“Zosyn”IVDecent for:
Enterococci, EntericsPseudomonasAnaerobesMany types of infections
Soft tissueAbdominal

Cephalosporins
Resistance due to ESBLs, AmpC beta-lactamases
• 1st generation– Staph, strep
– Some enterics (E. coli, Kleb, Proteus)
– Cefazolin: IV
– Cephalexin (Keflex): oral
• 2nd generation– More coverage against
enterics
– “Above the diaphragm”
• Cefuroxime, cefamandole
– Staph, strep, enterics, UTIs
– “Below the diaphragm”
• Cefoxitin, cefotetan
– Not for staph or strep
– Gram negative aerobes and anaerobes

Cephalosporins
Resistance due to ESBLs, AmpC beta-lactamases
• 3rd generation– Broad enteric and aerobic
GNR coverage
– Some anaerobic GNR coverage
– Ceftriaxone: IV/IM
– Cefotaxime: IV• Meningitis, pneumonia,
sepsis; many GNR including strep
– Ceftazidime• Pseudomonas infections
• 4th generation– Cefepime
• Excellent GNR coverage
– Pseudomonas
– AmpC producers
• 5th generation– Ceftaroline
• Like a 3rd generation drug with anti Staph activity, particularly MRSA

Aztreonam
• Monobactam class
• IV
• Active only against GNRs
– Includes Pseudomonas
• Useful in patients with known penicillin allergy
– Doesn’t cross react

Carbapenems
• Resistance is due to CARBAPENEMASES
• Very powerful
• Active against some Gram pos and most Gram neg
• Can cause seizures, renal problems
• May cross react with penicillin allergy
• Imipenem IV
• Meropenem IV
• Ertapenem IV/IM– Not good vs.
Pseudomonas, Acinetobacter

Enterobacter cloacae antibiotic panel: what is unusual?
Drug Sensitivity
Ampicillin R
Cefoxitin R
Ceftazidime R
Ceftriaxone R
Cefepime S
Piperacillin/tazobactam R
Meropenem R

Enterobacter cloacae antibiotic panel:
Drug Sensitivity
Ampicillin R
Cefoxitin R
Ceftazidime R
Ceftriaxone R
Cefepime S
Piperacillin/tazobactam R
Meropenem R
This is unusual. Note the Meropenem result: indicates a potential carbapenemase,would render the other beta-lactams useless. Remember E. cloacae would alsoproduce an inducible AmpC. De-repressed AmpC should retain susceptibility toCefepime (however, carbapenemase may confer resistance to cefepime).

Case
35yr old female, has recurrent UTIs that always grow out E. coli. She has received treatment 1-2 times per year. The infections clear and then recur.

E. coli susceptibility Report
• Ampicillin S• Piperacillin S• Cephalothin S• Cefoxitin S• Cefotaxime S• Ceftazidime S• Ceftriaxone S• Aztreonam S
• Cefepime S
• Pip/Tazo S
• Imipenem S
• Ciprofloxacin S
• TMP-SXT S

Continued
The patient returns to her doctor with another UTI. The physician gives her TMP-SXT as usual however, the symptoms persist and progress to include flank pain and fever. The patient is admitted to the hospital.
Urine and blood cultures are submitted and E. coli grows in both. However, this isolate does not have the same susceptibility profile as previous isolates.

E. coli susceptibility Report
• Ampicillin R• Piperacillin R• Cephalothin R• Cefoxitin S• Cefotaxime R• Ceftazidime S• Ceftriaxone R• Aztreonam I
• Cefepime S
• Pip/Tazo I
• Imipenem S
• TMP-SXT R
• Ciprofloxacin R
What is going on? What would you do?How would you report the AST?
CTX-M ESBL

E. coli ESBL susceptibility report
• Ampicillin R• Piperacillin R• Cephalothin R• Cefoxitin SR• Cefotaxime R• Ceftazidime SR• Ceftriaxone R• Aztreonam IR
• Cefepime SR
• Pip/Tazo I
• Imipenem S
• TMP-SXT R
• Ciprofloxacin R
Are you comfortable if this was you, or a loved one being treated with Ceftaz?

24yr old noticed a gradual loss of hearing in his right ear. It is determined that he has an acoustic neuroma. He is scheduled for surgery to remove the tumor. The surgery was successful. However, after surgery the patient develops hydrocephalus. A extra ventricular shunt is placed and symptoms resolve.
Cultures of CSF are collected and grow Enterobacter cloacae.
Case

Enterobacter cloacae susceptibility report
• Ampicillin R• Piperacillin R• Cephalothin R• Cefoxitin R• Cefotaxime S• Ceftazidime S• Ceftriaxone S• Aztreonam S
• Cefepime S
• Pip/Tazo R
• Imipenem S

Case (continued)
• An Infectious Disease Physician treats the infection with ceftriaxone (isolate tested sensitive).
• During microbiology plate rounds there is a discussion between the ID doc & microbiologist about ceftriaxone and inducible AmpC organisms.

Case continued
Additional cultures are collected after ceftriaxone therapy is initiated. Cultures again grow Enterobacter cloacae with the following sensitivities…

E. cloacae susceptibility report
• Ampicillin R• Piperacillin R• Cephalothin R• Cefoxitin R• Cefotaxime R• Ceftazidime I• Ceftriaxone R• Aztreonam I
• Cefepime S
• Pip/Tazo R
• Imipenem S

Case
24yr old woman 25lbs overweight attempts to obtain bariatric surgery to lose weight. She cannot find a doctor in the US willing to perform the surgery, so she goes to Brazil, where they will perform the surgery.
She returns to the US (St. Louis) and her abdomen becomes infected.
Cultures grow out Klebsiella pneumoniae.

Klebsiella pneumoniae
Ampicillin RPiperacillin RCephalothin RCefoxitin SCefotaxime RCeftazidime ICeftriaxone RAztreonam I
Cefepime SPip/Tazo RMeropenem I
• What are you thinking?• What do you do next?• Do you report out the
sensitivities?

Case
• 73-y-o male of Indian descent with a past medical history of diabetes is admitted for a right-sided ear infection.
• Infection is classified as malignant otitis externa and cultures are positive for Pseudomonas aeruginosa
• Antimicrobial susceptibility demonstrates the following resistance pattern:

Susceptibility results
Piperacillin-tazobactam R
Cefepime R
Imipenem R
Meropenem R
Aztreonam R
Ciprofloxacin R
Gentamicin R
Amikacin R
Tobramycin R
Colistin S

Things to think about
This is a very resistant organism (resistant even to the carbapenems) and the patient has a history of recent travel to India
What should we be worried about?

So did our isolate produce a MBL?
Maybe not, it was Resistant to Aztreonam.
Most likely a de-repressed AmpC plus a porin mutation (most common mechanism of carbapenem resistance in Pseudomonas aeruginosa)

Review

Which of the following antibiotics would be best to prescribe a patient with an infection of an enteric
with the derepressed AmpC phenotype?
• A: Ceftazidime
• B: Imipenem
• C: Aztreonam
• D: Cefepime
• E: Piperacillin/tazobactam

Which of the following antibiotics would be best to prescribe a patient with an infection of an enteric
with the derepressed AmpC phenotype?
• A: Ceftazidime
• B: Imipenem
• C: Aztreonam
• D: Cefepime
• E: Piperacillin/tazobactam

An E. coli isolate has the antibiotic susceptibility panel shown on the left. Which of the statements are correct?
Drug Result
Ampicillin R
Cefazolin R
Ceftriaxone R
Ceftazidime R
Cefoxitin R
Cefotetan R
Imipenem S
• A: The isolate is a carbapenemaseproducer; the imipenemresult should be changed.
• B: The isolate is probably an ESBL producer.
• C: The isolate probably produces a plasmid-mediated AmpC
• D: This is a classic efflux-mediated resistance pattern.

An E. coli isolate has the antibiotic susceptibility panel shown on the left. Which of the statements are correct?
Drug Result
Ampicillin R
Cefazolin R
Ceftriaxone R
Ceftazidime R
Cefoxitin R
Cefotetan R
Imipenem S
• A: The isolate is a carbapenemaseproducer; the imipenemresult should be changed.
• B: The isolate is probably an ESBL producer.
• C: The isolate probably produces a plasmid-mediated AmpC
• D: This is a classic efflux-mediated resistance pattern.
Note the cefoxitin and cefotetan results

Refer to the susceptibility panel for Klebsiellapneumoniae. Which of the results should be
confirmed?
Drug Sensitivity
Amikacin S
Ampicillin S
Cefazolin S
Cefoxitin S
Ceftazidime S
Cefotaxime S
Ciprofloxacin S
Levofloxacin S
Imipenem S
Piperacillin/tazobactam S
Tobramycin S
Trimethoprim-sulfamethoxazole
S

Refer to the susceptibility panel for Klebsiellapneumoniae. Which of the results should be
confirmed?
Drug Sensitivity
Amikacin S
Ampicillin S
Cefazolin S
Cefoxitin S
Ceftazidime S
Cefotaxime S
Ciprofloxacin S
Levofloxacin S
Imipenem S
Piperacillin/tazobactam S
Tobramycin S
Trimethoprim-sulfamethoxazole
S
K. pneumoniaeshould beamp resistant

The following is the sensitivity panel obtained for a Serratiamarcescens isolate from a blood culture. Which antibiotic sensitivity is
most alarming?
Drug Sensitivity
Amikacin S
Ampicillin R
Cefazolin R
Cefoxitin R
Ceftazidime R
Cefotaxime R
Ciprofloxacin R
Levofloxacin R
Meropenem R
Piperacillin/tazobactam R
Tobramycin R
Trimethoprim-sulfamethoxazole
R

The following is the sensitivity panel obtained for a Serratiamarcescens isolate from a blood culture. Which antibiotic sensitivity is
most alarming?
Drug Sensitivity
Amikacin S
Ampicillin R
Cefazolin R
Cefoxitin R
Ceftazidime R
Cefotaxime R
Ciprofloxacin R
Levofloxacin R
Meropenem R
Piperacillin/tazobactam R
Tobramycin R
Trimethoprim-sulfamethoxazole
R
Indicates acarbapenemase; bigtrouble clinically

Which of the following does not have an inducible, chromosomal ampC?
• A: Citrobacter freundii
• B: Enterobacter cloacae
• C: Escherichia coli
• D: Serratia marcescens
• E: None of the above

Which of the following does not have an inducible, chromosomal ampC?
• A: Citrobacter freundii
• B: Enterobacter cloacae
• C: Escherichia coli
• D: Serratia marcescens
• E: None of the above
Has an ampC, but it’s not inducible

The End
Any questions?