Embed Size (px)
Citation preview

1
The population pharmacokinetic and pharmacodynamic properties of intramuscular 1
quinine in Tanzanian children with severe falciparum malaria 2
3
Running title: Intramuscular quinine population pharmacokinetics 4
5
Ilse C E Hendriksen1,2, Deogratius Maiga3, Martha M Lemnge3, George Mtove4, Samwel 6
Gesase3, Hugh Reyburn5, Niklas Lindegardh1,2, Nicholas P J Day1,2, Lorenz von Seidlein6, Arjen 7
M Dondorp1,2, Joel Tarning1,2#, Nicholas J White1,2 8
9
1. Mahidol-Oxford Tropical Medicine Research Unit, Faculty of Tropical Medicine, Mahidol 10
University, Bangkok, Thailand 11
2. Centre for Tropical Medicine, Churchill Hospital, University of Oxford, Oxford, United 12
Kingdom 13
3. National Institute for Medical Research, Tanga Medical Research Centre, Tanga, Tanzania 14
4. National Institute for Medical Research, Amani Centre, Tanga, Tanzania 15
5. London School of Tropical Medicine and Hygiene, London, United Kingdom 16
6. Menzies School of Health Research, Casuarina, NT, Australia 17
18
# Corresponding author: 19
Copyright © 2012, American Society for Microbiology. All Rights Reserved.Antimicrob. Agents Chemother. doi:10.1128/AAC.01349-12 AAC Accepts, published online ahead of print on 26 November 2012
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

2
Joel Tarning 20
Mahidol-Oxford Tropical Medicine Research Unit 21
Faculty of Tropical Medicine, Mahidol University 22
3/F, 60th Anniversary Chalermprakiat Bldg. 23
420/6 Rajvithi Rd., Rajthevee 24
Bangkok 10400 Thailand 25
Email: [email protected] 26
Tel: 66 (0) 2 203 6369 27
Fax: 66 (0) 2 354 6018 28
29 on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

3
Abstract 30
Although artesunate is clearly superior, parenteral quinine is still used widely for the treatment of 31
severe malaria. A loading dose regimen has been recommended for 30 years but is often not 32
used. 33
A population pharmacokinetic study was conducted in 75 Tanzanian children aged 4 months to 8 34
years with severe malaria receiving intramuscular quinine; 69 patients received a loading dose of 35
20 mg quinine dihydrochloride (salt)/kg. 21 patients had plasma quinine concentrations 36
detectable at baseline. A zero-order absorption model with one-compartment disposition 37
pharmacokinetics described the data adequately. Body weight was the only significant covariate 38
and was implemented as an allometric function on clearance and volume parameters. Population 39
pharmacokinetic parameter estimates (%RSE) of elimination clearance, central volume of 40
distribution, and duration of zero-order absorption were 0.977 (6.50%) L/h, 16.7 (6.39%) L and 41
1.42 (21.5%) h, respectively, for a typical patient weighing 11 kg. Quinine exposure was reduced 42
at lower body weights after a standard weight-based dosing; there was 18% less exposure over 43
24 hours in patients of 5 kg compared with those of 25 kg. Maximum plasma concentrations 44
after the loading dose were unaffected by body weight. There was no evidence of dose related 45
drug toxicity with the loading dosing regimen. 46
Intramuscular quinine is rapidly and reliably absorbed in children with severe falciparum 47
malaria. Based on these pharmacokinetic data, a loading of 20 mg salt/kg is recommended, 48
provided no loading dose was administered within 24 hours and no routine dose within 12 hours 49
of admission. 50
Keywords: Severe malaria, Quinine, Children, Pharmacokinetics, Pharmacodynamics51
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

4
Introduction 52
Malaria kills over 2000 people each day. Young children in Africa account for over 85% of the 53
malaria associated mortality worldwide (52). The case-fatality of pediatric severe malaria usually 54
exceeds 10% with the highest mortality within the first 24 hours (6, 43). Parenteral quinine has 55
been the mainstay of severe malaria treatment for much of the past century (51). Although 56
parenteral artesunate is now firmly established as the treatment of choice, availability is still 57
limited and so quinine remains very widely used (6). 58
Modern quinine dosing regimens were initially based on studies in Asian adults (46, 47) and 59
have been extrapolated to African children, although there is relatively little detailed 60
pharmacokinetic information in this important group (12, 19, 32, 40, 45). The currently 61
recommended dosing regimen is a loading dose of 20 mg quinine dihydrochloride (salt)/kg 62
followed by 10 mg/kg every eight hours, given by rate-controlled intravenous infusion or 63
intramuscular injection (51). Peak quinine concentrations are achieved within 4 hours after 64
intramuscular injection, which is more practicable and may be safer in resource limited settings 65
where intravenous infusions cannot be established or reliably monitored (19, 40, 42). 66
Quinine is metabolized primarily via the cytochrome P450 enzyme CYP3A4 and the more polar 67
metabolites are eliminated mainly by renal excretion (9, 23, 28). The major metabolite, 3-68
hydroxyquinine, contributes approximately 10% of the antimalarial activity of the parent 69
compound (24). The pharmacokinetic properties of quinine are affected by the severity of 70
infection as well as age (40, 46). The apparent volume of distribution and elimination clearance 71
are significantly reduced in proportion to increased disease severity (13, 46), partly because of 72
increased quinine binding to plasma-proteins, mainly alpha 1-acid glycoprotein (18, 34). Quinine 73
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

5
clearance is also altered by some drug interactions (44). The unbound plasma fraction of quinine 74
determines the therapeutic and toxic activity of the drug (54). In children under 2 years of age 75
with severe malaria, unbound quinine concentrations were found to be slightly higher than in 76
older children and adults (40). Although quinine is generally well tolerated, the therapeutic 77
window of unbound drug is relatively narrow and side effects include hypoglycemia (even in the 78
therapeutic range), cardiotoxicity, ototoxicity and ocular toxicity (4, 48, 49, 55). 79
Rapid achievement of therapeutic quinine concentrations while avoiding toxicity is of vital 80
importance in the treatment of severe malaria. Despite its extensive use in millions of critically 81
ill children at risk of death, there are very few detailed assessments of the pharmacokinetic 82
properties in the target population (12). The primary aim of this study was to characterize the 83
population pharmacokinetic profile of intramuscular quinine after a loading dose in children with 84
severe malaria in Tanzania. A limited pharmacodynamic assessment was included as a secondary 85
aim. 86
87
Methods 88
Study design, patients and procedures 89
This pharmacokinetic assessment of quinine was part of the ‘AQUAMAT’ trial (registration 90
number ISRCTN 50258054), a large multinational trial comparing quinine and artesunate for the 91
treatment of severe malaria, results of which have been published elsewhere (6). This substudy 92
was conducted in Teule Hospital in Muheza, Tanzania, from May 2009 to July 2010. Apart from 93
the additional blood sampling, procedures of the current study were part of the ‘AQUAMAT’ 94
study protocol. The clinical assessment is reported in full elsewhere (6). Approval for the study 95
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

6
including the pharmacokinetic substudy was obtained from Tanzania Medical Research 96
Coordinating Committee and the Oxford Tropical Research Ethics Committee. A total of 21 97
patients were co-enrolled in the ‘FEAST’ trial evaluating fluid bolus therapy in children with 98
compensated shock (17). 99
Children ≤14 years with a clinical diagnosis of severe malaria confirmed by a parasite Lactate 100
Dehydrogenase (pLDH)-based rapid diagnostic test (Optimal, Diamed, Cressier) were recruited, 101
provided written informed consent was given by their parent or guardian. Severe malaria was 102
defined as at least one of the following: coma (Glasgow Coma Scale ≤10 or Blantyre Coma 103
Scale ≤2 in preverbal children), convulsions (of duration >30 minutes or ≥2 in 24 hours before 104
admission), respiratory distress (nasal alar flaring, costal indrawing/recession or use of accessory 105
muscles, severe tachypnea) or acidotic breathing (‘deep’ breathing), shock (capillary refill time 106
≥3 sec and/or temperature gradient and/or systolic blood pressure <70 mmHg), severe 107
symptomatic anemia (hemoglobin <5 g/dL with respiratory distress), hypoglycemia (blood 108
glucose <3 mmol/L), hemoglobinuria, severe jaundice or a convincing history of anuria or 109
oliguria in older children. Patients who had received full treatment with parenteral quinine or a 110
parenteral artemisinin derivative for more than 24 hours before admission were excluded. 111
Physical examination was performed at admission and a venous blood sample was taken for 112
peripheral blood parasitemia, quantitative assessment of plasma Plasmodium falciparum 113
Histidine-Rich Protein-2 (a marker of total body parasite burden) (10), HIV serology (SD Bio-114
Line HIV 1/2 3.0, Standard Diagnostics Inc, Kyonggi-do, Korea /Determine HIV-1/2, Abbott 115
Laboratories, IL, USA), blood culture, liver function tests (AST, ALT, Gamma-GT, total 116
bilirubin, creatinine and urea, by Reflotron, Roche Diagnostics), Hematocrit (Hct), biochemistry 117
and acid-base parameters (EC8+ cartridge for i-STATTM handheld blood analyzer). Hematocrit 118
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

7
was reported from the i-STAT or, when not available, derived from hemoglobin (Hb) measured 119
by Haemocue (n=5). At discharge, a neurological examination was performed. 120
Antimalarial treatment 121
Quinine dihydrochloride (Indus Pharma, Karachi, Pakistan) was given as an intramuscular 122
injection. A loading dose (20 mg salt/kg) was given shortly after admission, followed by 10 123
mg/kg every 8 hours. In case the patient had received pretreatment with either a quinine loading 124
dose (20 mg/kg) within 24 hours or a maintenance dose (10 mg/kg) within 12 hours before 125
enrollment, quinine treatment after study enrolment was continued with 10 mg/kg (i.e. no 126
loading dose). Quinine was diluted with normal saline to a concentration of 60 mg salt/ml and 127
injected into the anterior thigh. The dosing was based on body weight and injection volumes over 128
3 ml were split and divided over both thighs. When the patient was well enough to take oral 129
medication, but after a minimum of 24 hours (3 doses) of intramuscular quinine, a full course of 130
oral artemether-lumefantrine (Co-artem®, Novartis, Basel, Switzerland) was given to complete 131
the treatment. 132
Patient management 133
The majority of patients receiving quinine received an intravenous infusion with glucose 5%. 134
Vital signs and glucose were monitored at least 6-hourly and with any deterioration in clinical 135
condition. Low blood glucose (defined here as blood glucose <3 mmol/L) was treated with an 136
i.v. 5 ml/kg 10% glucose bolus. A blood transfusion (20 ml/kg) was given to children with 137
hematocrit ≤15% or Hb <5 g/dL. All children were treated empirically with i.v. antibiotics 138
(ampicillin and gentamicin or ceftriaxone if clinically suspected of having sepsis or meningitis) 139
until blood culture results were known or changed according to antibiotic sensitivity analysis. 140
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

8
Convulsions were treated with diazepam or phenobarbitone if they persisted. A peripheral blood 141
smear was repeated after 24 hours. 142
Blood sampling 143
Blood samples (1.5 mL) were drawn from an indwelling catheter into lithium-heparin tubes 144
before the first dose (at baseline) and 4 subsequent samples taken from each patient at pre-set 145
random times in the following time-windows: 1 to 4 hours, 4 to 8 hours 12 to 16 hours and 20 to 146
24 hours after the injection of the first dose. The sampling windows were selected in order to 147
cover the whole concentration-time profile during the first 24 hours. More intensive sampling 148
was practically difficult and ethically challenging considering the clinical setting and the age and 149
disease severity of the patients. Randomization of sample times was done by computer-generated 150
randomization in STATATM, version 10 (Stata Corp., TX, USA). 151
Blood samples were centrifuged at 2,000×g for 10 minutes to obtain plasma. Duplicate plasma 152
samples (0.5 mL) were stored at -80°C and sent to AMBRELA/NIMR laboratory in Tanga, 153
Tanzania for plasma quinine quantification. Quinine drug content and quality were checked in 154
ampoules taken randomly from the purchase lots (see supplement of (6)). 155
Drug analysis 156
Total quinine was quantified in plasma samples using high-performance liquid chromatography 157
with UV-detection (22). Quinine was extracted from plasma samples by liquid-liquid extraction 158
using ethyl acetate/hexane (1:1 v/v). Separation was performed by isocratic elution from a 159
reverse phase Synergi MAX-RP (250 x 4.6 mm; 4 μ) column (Phenomenex, USA) with an acidic 160
(adjusted to pH 2.8 with o-phosphoric acid) mobile phase (25 mM KH2PO4:methanol; 80:20% 161
(v/v) + 1% (v/v) triethylamine) at a flow rate of 1.2 mL/min. Quinidine internal standard (25 µl 162
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

9
aliquot of 100 µg/ml quinidine working standard) and quinine was detected at 254 nm and 163
resolved to baseline with retention times of 9.3 minutes and 11.8 minutes, respectively. The 164
lower limit of quantification was set to 100 ng/ml. Quality control samples at 1, 10 and 20 mg/L 165
were prepared by spiking drug free plasma. Intra-assay and inter-assay coefficients of variation 166
ranged from 5.4% to 12.7%. 167
Population pharmacokinetic-pharmacodynamic analysis 168
Quinine concentrations were transformed into their natural logarithms and modeled using 169
NONMEM version 7 (ICON Development Solutions, Hanover MD) (3). Automation and model 170
diagnostics were performed using Pearl-speaks-NONMEM (PsN) and Xpose (11, 15, 16). The 171
Laplacian (pharmacodynamic model) and first-order conditional estimation method with 172
interaction (pharmacokinetic model) was used throughout modeling. The difference in objective 173
function value (∆OFV) computed by NONMEM as -2×Loglikelihood was used as statistical 174
criteria for hierarchical models (∆OFV>3.84 was considered statistically significant at p<0.05 175
with one degree of freedom difference). Goodness-of-fit plots and simulation-based diagnostics 176
were used for model evaluation. Only two post-dose concentrations were quantified to be below 177
the lower limit of quantification and were therefore omitted. 178
Population pharmacokinetic models were parameterized initially using a first-order rate constant 179
(ka) or a duration of a zero-order absorption (DUR), elimination clearance (CL/F), inter-180
compartment clearance (Q/F) and apparent volume of distribution(s) (V/F). Limited data were 181
available in the absorption phase and the injection sites were therefore considered to be a single 182
depot compartment and bioavailability (F) was assumed to be 100%. Several absorption models 183
were tried i.e. first- and zero-order absorption with or without lag time as well as a more flexible 184
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

10
transit-compartment absorption (30). Pre-dose concentrations were handled by flagging patients 185
with pre-dose concentrations to allow a baseline value to be estimated for these individuals. 186
Between-subject variability (BSV) and between-dose occasion variability (BOV) were modeled 187
exponentially. One- and two-compartment disposition models were evaluated. First-order and 188
Michaelis-Menten elimination was evaluated. A Box-Cox transformation was tried on individual 189
population parameters to assess formally the assumption that pharmacokinetic parameters are 190
log-normally distributed (27). The residual random variability was assumed to be additive since 191
data were transformed into their natural logarithms (i.e. essentially equivalent to an exponential 192
error model on an arithmetic scale). 193
The implementation of body weight as a covariate on clearance and volume of distribution in the 194
final structural model was assessed using an allometric function [individual clearance value 195
=typical clearance value × (individual body weight/median body weight in the population)EXP 196
and individual volume value = typical volume value × (individual body weight/median body 197
weight in the population)EXP]. An estimated exponent (EXP) for the allometric implementation of 198
body weight on clearance and volume parameters was tried as well as fixed exponents of 1, 3/4, 199
and 2/3 (21). An age-related enzyme-maturation effect was also investigated on clearance (1). 200
Demographic, clinical and laboratory data on admission were considered as potential covariates 201
and investigated using a stepwise forward addition and backward elimination approach. A P-202
value of 0.05 was used in the forward step and a P-value of 0.001 in the backward step to 203
compensate for the relatively small population studied. The following admission covariates were 204
investigated using the stepwise approach: age (years), weight-for-age Z-scores (5, 53), 205
temperature (⁰C), heart rate (beats/min), coma (continuous variable based on GCS/BCS coma 206
score), cerebral malaria (coma and/or convulsions), blood urea nitrogen (mg/dL), hemoglobin 207
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

11
(g/dL), base excess (mmol/L), parasitemia, (parasites/µL), plasma Plasmodium falciparum 208
Histidine-Rich Protein-2 (ng/mL) as a marker of total parasite burden (10), total bilirubin 209
(μmol/L), creatinine (high: age<1 yr ≥44.2 µmol/L, age≥1 year≥62 µmol/L, low: age<1 yr<44.2 210
µmol/L, age≥1 year>62 µmol/L), HIV co-infection, shock (compensated or decompensated), 211
fluid bolus and/or blood transfusion. 212
Numerical- and visual predictive checks were used to assess the predictive performance of the 213
final model. The final model with included variability was used to simulate 2,000 concentrations 214
at each sampling time-point and the 95% confidence interval around the simulated 5th, 50th and 215
95th percentiles were overlaid with the same percentiles of observed data to evaluate the 216
predictive power of the model (visual predictive check). The percentages of observations below 217
and above the simulated 5th and 95th percentile were also calculated for a numerical predictive 218
check. Non-parametric bootstrap diagnostics (n=2,000), stratified by median body weight (above 219
or below 11 kg), were performed for accurate relative standard errors and non-parametric 220
confidence intervals of population parameter estimates. Stratification by body weight was 221
performed to maintain an equal distribution of high and low body weights in the resampled data. 222
The final model was also used for Monte-Carlo simulations evaluating the quinine exposure in 223
children at different body weights with or without a loading dose. 224
Survival data were modeled in NONMEM using a time-to-event analysis. Patients were censored 225
at 12 hours after the last intramuscular quinine administration. The survival data were modeled 226
using a constant hazard function, Weibull-distribution hazard function, or an exponential hazard 227
function. OFV and simulation based diagnostics were used to compare models. There were 13 228
deaths in the 75 patients in this study which was too few for a formal covariate analysis on the 229
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

12
time-to-event. Drug concentration-response relationships were evaluated by a direct effect driven 230
by plasma concentrations or a delayed effect by cumulative quinine exposure. 231
232
Results 233
Clinical details 234
Seventy five (75) children were included, of whom 28 (37%) were under 2 years. Demographic, 235
clinical and laboratory characteristics are described in Table 1. Severe prostration, convulsions, 236
severe acidosis, severe anemia and coma were the most common severity criteria. None of the 18 237
patients who presented with hypoglycemia at admission and only 4 out of 7 patients with 238
hemoglobinuria had a history of quinine pretreatment. Seven (9.3%) patients had blood culture 239
confirmed bacteremia (12.5% in shocked patients versus 8.5% in non-shocked patients, 240
p=0.623). The identified organisms were non-Typhi Salmonella, Enterobacter cloacae, 241
Klebsiella spp., Escherichia coli, Burkholderia cepacia, Streptococcus Group A. HIV co-242
infection was found in 5/75 (6.7%) of patients. None of these patients was receiving 243
antiretroviral treatment. Out of 75 patients 13 (17%) died, of whom 10 (77%) died within 24 244
hours. Children who survived had no neurological sequelae at discharge. 245
Sixty nine (92%) patients received a quinine loading dose at the start of the study, and the 246
remainder started with 10 mg/kg. During the first 24 hours of admission, 37 patients received a 247
blood transfusion and 19 patients received a fluid bolus. Eleven patients (15%) developed 248
hypoglycemia after admission, including 5/18 (27.7%) of those who presented with 249
hypoglycemia at admission. Hypoglycemia occurred in 6/11 children despite intravenous 5% 250
dextrose infusion, five of whom subsequently died. 251
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

13
Coma after admission occurred in 7 (9%) patients. Geometric mean (95% CI) peripheral parasite 252
densities on admission were 31,900 (17,300-58,900) parasites/µL, and after 24 hours treatment 253
were 3,681 (1,422-10,790) parasites/µL with a median (IQR) fractional reduction of 78% (38%-254
99%) in 60 patients (1 and 14 patients with missing baseline or 24 hours parasitemia, 255
respectively, including 10 fatal cases). 256
A history of oral antimalarial treatment before admission was given for 41 (55%) patients (8 with 257
quinine, 5 with amodiaquine, 17 with artemether-lumefantrine, 10 with sulfadoxine-258
pyrimethamine and 1 with sulfadoxine-pyrimethamine followed by artemether-lumefantrine). 259
Parenteral quinine pretreatment within 24 hours prior to admission was reported for 15 patients, 260
with a maximum of 3 doses and a mean (SD) of 10 (1.8) mg/kg. Of these patients, 12 had 261
detectable baseline plasma quinine concentrations ranging from 1.56 to 17.38 mg/L. Three 262
patients treated earlier with oral quinine had baseline drug concentrations of 3.34, 5.10 and 8.26 263
mg/L. Another 6 patients without history of quinine treatment before admission had detectable 264
plasma quinine concentrations ranging from 0.85 to 14.88 mg/L (of whom 5 had baseline 265
concentrations <4.0 mg/L). 266
Population pharmacokinetic-pharmacodynamic analysis 267
Each patient contributed 1 to 5 plasma samples resulting in a total of 341 concentration-time 268
samples distributed randomly over the first 24 hours of the study. All patients were included in 269
the population pharmacokinetic analysis and pre-dose quinine concentrations were 270
accommodated by estimating a baseline concentration in these patients (median [range] 271
concentrations of 6.90 [0.976-14.9] mg/L). Post-dose plasma concentrations ranged from 0.850 272
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

14
to 33.8 mg/L. Four patients had very high plasma quinine concentrations (>25 mg/L) but no 273
serious adverse events or deaths could be attributed to these high plasma quinine concentrations. 274
A one-compartment disposition model with zero-order absorption resulted in adequate fit to the 275
observed data. None of the investigated absorption models performed better than the zero-order 276
absorption model. No additional benefit was seen with an additional peripheral disposition 277
compartment (∆OFV=-4.12, two degrees of freedom difference). There was no substantial 278
between dose occasion variability in any population parameters (∆OFV<-0.150) and this was 279
therefore not included in the final model. Michaelis-Menten elimination did not significantly 280
improve the model diagnostics (∆OFV=-2.75) compared to a first-order elimination model. A 281
Box-Cox transformation of population parameters did not significantly improve the model fit 282
(∆OFV<-1.88) compared to the usual assumed log-normal distribution. Incorporation of an off-283
diagonal element in the covariance-matrix of elimination clearance and apparent volume of 284
distribution resulted in a significant correlation (99.9%) and an improvement in model fit. 285
Between-subject variability could not be estimated reliably for the duration of zero-order 286
absorption (RSE=171%) and was therefore not retained in the final model. 287
Body weight as a fixed allometric function on elimination clearance (exponent of 3/4) and 288
apparent volume of distribution (exponent of 1) resulted in a significant improvement in model 289
fit (∆OFV=-39.0) and decreased the between-subject variability (%CV) from 47.4% to 35.9% 290
and from 61.2% to 51.3%, respectively. The exponents were also estimated and the bootstrap 291
(n=500) diagnostics resulted in 95% confidence intervals of 0.484-1.51 for elimination clearance 292
and 0.594-1.52 for apparent volume of distribution, respectively. A fixed exponent of 3/4 for 293
elimination clearance and 1 for apparent volume of volume was selected as the final model 294
considering the strong biological prior of these relationships supported by the observation that 295
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

15
the estimated confidence intervals included these fixed values (21). The following covariate 296
relationships were selected in the forward step-wise addition (p<0.05): base excess on CL/F, 297
base excess on V/F, hemoglobin on V/F and age on CL/F as a maturation model. However, none 298
of these covariates could be retained in the backward step with a more stringent statistical 299
criterion (p<0.001). The final population parameter estimates, variability estimates and post-hoc 300
estimates are summarized in Table 2. 301
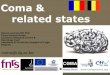
The final model described the observed data well with adequate goodness-of-fit diagnostics 302
(Figure 1) and calculated shrinkages below 15% (CL/F: 11.3%, V/F: 11.3%, Epsilon-shrinkage: 303
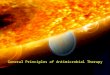
14.0%). A prediction-corrected visual predictive check of the final model resulted in no model 304
misspecification with good simulation properties (Figure 2). The numerical predictive check 305
resulted in 6.92% (95% CI. 2.08-9.00) and 2.08 (95% CI. 1.73-9.00) of observations above and 306
below the 90% prediction interval. 307
Body weight was the only significant covariate in the final model with lower body weights being 308
associated with slightly reduced exposure during the first 24 hours after the standard weight-309
based dose. There was a mean reduction of 7.19% in simulated quinine exposure during the first 310
dose (0 to 8 hours) when comparing patients weighing 5 kg with patients of 20 kg body weight 311
after a 20 mg salt/kg loading dose (data not shown). This reduction in exposure accumulated 312
with the repeated maintenance dosing of 10 mg/kg over the first 24 hours to a total mean 313
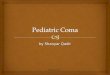
difference of 15.4% (data not shown). Peak concentrations after the first dose were unaffected by 314
body weight but accumulated to a mean difference of 15.9% lower peak concentrations for 315
patients weighing 5 kg compared to patients of 20 kg after the third dose (Figure 3a). This 316
difference (<20%) in total exposure and maximum concentration is not likely to have a 317
significant clinical impact since more than 85% of patients irrespectively of body weight reached 318
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

16
plasma quinine concentrations over the therapeutic margin of 8 mg/L after a loading dose of 20 319
mg/kg and more than 95% of patients reached the target during the first 24 hours with the 320
subsequent maintenance dose of 10 mg/kg. In absence of a loading dose, the therapeutic range 321
would only be reached in less than 30% of patients after the first dose and in 89% of patients 322
during the first 24 hours (Figure 3b). 323
A constant hazard function model with cumulative exposure implemented as an Emax function 324
modulating the hazard described the survival over time well in this study. A simulation-based 325
visual predictive check resulted in the observed survival curve being contained within the 90% 326
prediction interval of the model simulated survival curve (Figure 4). Median time to reach a 50% 327
reduction in hazard was approximately 6 hours. However, there was no significant difference in 328
post-hoc estimates of total exposure (p=0.1358) or maximum concentrations (p=0.1786) after the 329
first dose in children who died compared to children who survived (Figure 5). The exposure-330
effect relationship is likely to describe the delayed antimalarial effect of quinine but this 331
approach is biased since many patients had a pre-treatment history of quinine and a larger data 332
set would be necessary for a formal concentration-effect analysis. 333
334
Discussion 335
The therapeutic range for quinine in severe malaria has been estimated between 8 and 15 mg/L 336
based on observations in uncomplicated malaria suggesting reduced therapeutic responses when 337
serum or plasma concentrations fall below 5 mg/L and taking into account variation in parasite 338
susceptibility and the reduced free fraction observed in severe malaria. Plasma concentrations up 339
to 20 mg/L have not been associated with significant toxicity (7, 29, 35, 36, 45). 340
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

17
In the present study, intramuscular quinine was rapidly and reliably absorbed and the currently 341
recommended loading dose regimen resulted in plasma concentrations that rapidly reached the 342
therapeutic range in African children with severe malaria. A wide range of patient covariates did 343
not affect the pharmacokinetic parameters significantly suggesting that this applied to children of 344
all ages and with all forms of severe malaria. Body weight was the only significant covariate 345
affecting quinine exposure. Monte Carlo simulations resulted in a modest mean reduction of 346
7.19% in total quinine exposure after the loading dose (0 to 8 hours) in children weighing 5 kg 347
compared to that of children weighing 20 kg. This accumulated to a larger difference of 15.4% 348
over 3 doses (0 to 24 hours). This is unlikely to have a significant clinical impact since 349
therapeutic levels of 8 mg/L were reached rapidly in all weight groups (Figure 2). Dose 350
adjustment is therefore not recommended in smaller children based on this pharmacokinetic 351
difference. Simulations resulted in median (95% CI) maximum concentrations of 12.6 (5.60-352
28.4) mg/L after a loading dose of 20 mg/kg compared to 6.32 (2.80-14.2) mg/L without loading 353
dose (i.e. after 10 mg/kg). This supports that a loading dose should be used to achieve target 354
concentrations within the first dose interval. 355
An intramuscular loading dose of quinine was rapidly and reliably absorbed and patients in this 356
study reached estimated peak median (95% CI) plasma quinine concentrations of 13.4 (7.20-357
24.8) mg/L within 1.50 hours. This is in accordance with previous studies showing similar peak 358
plasma quinine concentration compared to the intravenous route with similar efficacy (13, 26, 359
31). Dilution of the quinine solution to 60 mg/mL has been reported to accelerate the absorption 360
from the intramuscular injection site (19, 42, 54), and this time to peak is shorter than reported 361
previously with injection of more concentrated injectate. 362
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

18
Pharmacokinetic estimates should be extrapolated with caution beyond the range of the studied 363
patients (i.e. elimination clearance of 3.91 L/h scaled to a 70 kg patient). However, the reported 364
median (95% CI) estimates of a quinine terminal half-life of 12.1 (9.63-14.3) hours and 365
elimination clearance of 0.0741 (0.0455-0.144) L/h/kg are in agreement with previously 366
published estimates from small conventional densely sampled pharmacokinetic studies in 367
children with severe falciparum malaria: median half-lives ranging from 8.4 to 23.5 hours and 368
clearance from 0.027 to 0.0816 L/h/kg have been reported (reviewed in (13)). Minor differences 369
between our findings with that reported in a population pharmacokinetic analysis by Krishna et 370
al (mean (SD) half-life of 19.9 (4.4) hours and elimination clearance of 0.05 L/h/kg) may be 371
explained by using different structural models (a one-compartment model versus a two-372
compartment model) (12). In this study, we sampled during the first 24 hours, which could also 373
have contributed to the difference in structural models. Thus, a two-compartment model could 374
prove to be a more appropriate structural model when enough data are collected to support a 375
differentiation between a distribution and a terminal phase. However, the terminal elimination 376
half-life estimate reported by Krishna et al is similar to that in adults with severe malaria, 377
whereas the majority of published data point to more rapid elimination in children compared 378
with adults. Body weight has not been described as a covariate for quinine pharmacokinetics 379
before but it was significant in this analysis (12, 40). Physiological processes do not scale 380
linearly with body weight and consequently children with a lower body weight will have a higher 381
body weight-normalised elimination clearance, which has been reported previously for other 382
antimalarials (2, 37). 383
In accordance with the only previous population pharmacokinetic study, we did not find any 384
other covariates explaining the between-subject variability in children with severe malaria 385
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

19
despite the different clinical presentations (12). Compared with uncomplicated malaria, patients 386
with severe disease have a smaller distribution volume and a slower clearance due in part to a 387
higher fraction of plasma-protein bound quinine (46). 388
It is reassuring that intramuscular quinine was reliably absorbed in children with impaired 389
perfusion, shock and severe anemia, although these were largely corrected for in this study with 390
supportive treatments. In addition, none of the clinical or laboratory parameters with strong 391
prognostic value such as coma, impaired renal function (elevated BUN) or acidosis affected the 392
pharmacokinetics of quinine (41). Therefore, the quinine dosing does not need to be adapted 393
according to the presentation of the disease in children with severe malaria. 394
Intramuscular quinine is painful, but local toxicity is rare when a sterile injection technique is 395
used and the quinine is diluted to 60 mg/ml (40). In our study site, all concomitant medications 396
including routinely administered antibiotics were given by IM injection in the anterior thigh. 397
However, no mobility problems were noted and all surviving children were well at discharge. 398
The neurological examination at discharge did not disclose any evidence of systemic quinine 399
toxicity such as blindness or hearing problems, even though 4/75 (5%) of children had plasma 400
quinine concentrations above 25 mg/L within the first 24 hours of treatment. Peak total plasma 401
concentrations tend to increase during the treatment of severe malaria until clinical resolution 402
(13), so it is possible that some patients might have experienced potentially toxic quinine 403
concentrations later in their treatment course. The levels of quinine associated with toxicity in 404
severe malaria are not well established, since toxicity derives from the free quinine-fraction, 405
which depends on the levels of plasma-proteins, predominantly AGP that vary substantially (18, 406
34). The pharmacokinetic study of Hensbroek et al showed that young children could be more 407
prone to quinine toxicity as evidenced by slight prolongation of QRS interval on the 408
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

20
electrocardiogram (intraventricular conduction delay), although this was not related to plasma 409
quinine concentrations (40). The main adverse effect of quinine in severe malaria is 410
hypoglycemia resulting from quinine stimulated insulin release, and this occurs with therapeutic 411
concentrations (48, 49). Otherwise given the extensive use of quinine, the widespread and often 412
unreported pre-treatment, its use in severe malaria is otherwise remarkably free from serious 413
toxicity. 414
In our study, children who died did not have higher or lower plasma quinine concentrations than 415
children who survived (Figure 5) and 12/13 of fatal cases had received a loading dose at 416
admission. The one child who died and did not receive a loading dose at admission was reported 417
to have received pretreatment with two quinine injections; however the baseline quinine 418
concentration was undetectable suggesting that the history was incorrect. Unreliability of the 419
treatment history is commonplace in malaria (33, 39). Administering a loading dose of 20 mg/kg 420
when the history is uncertain may be safest as undertreating severe malaria risks death. 421
The therapeutic benefit of the loading dose has been widely accepted, but unsubstantiated 422
toxicity concerns have long hindered its implementation in the field (47, 50). Although there is 423
no large randomized controlled trial evidence that the loading dose is life-saving, the faster fever 424
and parasite clearance times and an understanding of the basic pathobiology of severe malaria 425
suggest that it is beneficial in the treatment of severe malaria (reviewed in (14)). Importantly, the 426
loading dose does not alter the risk of hypoglycemia due to quinine-induced hyperinsulinemia 427
(14, 25). One fifth of the children in our study had already received routine dosing parenteral 428
quinine prior to admission, none of whom presented hypoglycemic at admission. Hypoglycemia 429
is an indicator of severe disease, associated with an increased case-fatality (8, 20, 25, 38). The 430
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

21
high incidence of shock and positive blood cultures suggests that concomitant sepsis might also 431
have contributed to the high mortality in our study population. 432
In conclusion, if artemisinin derivatives are unavailable and quinine is used, then a loading dose 433
should be given unless there is convincing evidence of adequate pretreatment, since the risk of 434
death of severe malaria is highest and the risk of systemic toxicity is lowest during the first 24 435
hours. Starting with the routine dose is justified in children who have already definitely received 436
a loading dose within 24 hours before admission and those who have received a routine dose 437
within 12 hours of admission, but if in doubt, a loading dose should be given. 438
439
Acknowledgements 440
We are grateful to the patients and their guardians. We thank Ben Amos from Teule Hospital in 441
Muheza for microbiology and laboratory management. Thanks also go to Paul Martine, 442
laboratory technician at AMBRELA, for assisting in the laboratory. Permission to publish this 443
work was given by the Director General, National Institute for Medical Research, Tanzania. This 444
work was supported by The Wellcome Trust of Great Britain [grant 076908 and 082541] and 445
was coordinated as part of the Mahidol-Oxford Tropical Medicine Research Programme funded 446
by the Wellcome Trust of Great Britain. 447
448
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

22
References 449
1. Anderson, B. J., and N. H. Holford. 2009. Mechanistic basis of using body size and 450
maturation to predict clearance in humans. Drug Metab. Pharmacokinet. 24:25-36. 451
2. Barnes, K. I., F. Little, P. J. Smith, A. Evans, W. M. Watkins, and N. J. White. 2006. 452
Sulfadoxine-pyrimethamine pharmacokinetics in malaria: pediatric dosing implications. Clin. 453
Pharmacol. Ther. 80:582-596. 454
3. Beal, S., Boeckman, AJ, Sheiner, LB 1992. NONMEM user’s guides, version 4. 455
NONMEM Project Group, University of California, San Francisco. 456
4. Claessen, F. A., C. J. van Boxtel, R. M. Perenboom, R. A. Tange, J. C. Wetsteijn, and P. 457
A. Kager. 1998. Quinine pharmacokinetics: ototoxic and cardiotoxic effects in healthy 458
Caucasian subjects and in patients with falciparum malaria. Trop. Med. Int. Health 3:482-459
489. 460
5. de Onis, M., A. W. Onyango, E. Borghi, A. Siyam, C. Nishida, and J. Siekmann. 2007. 461
Development of a WHO growth reference for school-aged children and adolescents. Bull. 462
World Health Organ. 85:660-667. 463
6. Dondorp, A. M., C. I. Fanello, I. C. Hendriksen, E. Gomes, A. Seni, K. D. Chhaganlal, 464
K. Bojang, R. Olaosebikan, N. Anunobi, K. Maitland, E. Kivaya, T. Agbenyega, S. B. 465
Nguah, J. Evans, S. Gesase, C. Kahabuka, G. Mtove, B. Nadjm, J. Deen, J. Mwanga-466
Amumpaire, M. Nansumba, C. Karema, N. Umulisa, A. Uwimana, O. A. Mokuolu, O. 467
T. Adedoyin, W. B. Johnson, A. K. Tshefu, M. A. Onyamboko, T. Sakulthaew, W. P. 468
Ngum, K. Silamut, K. Stepniewska, C. J. Woodrow, D. Bethell, B. Wills, M. Oneko, T. 469
E. Peto, L. von Seidlein, N. P. Day, and N. J. White. 2010. Artesunate versus quinine in 470
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

23
the treatment of severe falciparum malaria in African children (AQUAMAT): an open-label, 471
randomised trial. Lancet 376:1647-1657. 472
7. Earle, D. P., Jr., R. W. Berliner, and et al. 1948. Studies on the chemotherapy of the 473
human malarias; method for the quantitative assay of suppressive antimalarial action in 474
falciparum malaria. J. Clin. Invest. 27:75-79. 475
8. English, M., S. Wale, G. Binns, I. Mwangi, H. Sauerwein, and K. Marsh. 1998. 476
Hypoglycaemia on and after admission in Kenyan children with severe malaria. Q. J. Med. 477
91:191-197. 478
9. Hall, A. P., A. W. Czerwinski, E. C. Madonia, and K. L. Evensen. 1973. Human plasma 479
and urine quinine levels following tablets, capsules, and intravenous infusion. Clin. 480
Pharmacol. Ther. 14:580-585. 481
10. Hendriksen, I. C., J. Mwanga-Amumpaire, L. von Seidlein, G. Mtove, L. J. White, R. 482
Olaosebikan, S. J. Lee, A. K. Tshefu, C. Woodrow, B. Amos, C. Karema, S. Saiwaew, 483
K. Maitland, E. Gomes, W. Pan-Ngum, S. Gesase, K. Silamut, H. Reyburn, S. Joseph, 484
K. Chotivanich, C. I. Fanello, N. P. Day, N. J. White, and A. M. Dondorp. 2012. 485
Diagnosing Severe Falciparum Malaria in Parasitaemic African Children: A Prospective 486
Evaluation of Plasma PfHRP2 Measurement. PLoS Med. 9:e1001297. 487
11. Jonsson, E. N., and M. O. Karlsson. 1999. Xpose--an S-PLUS based population 488
pharmacokinetic/pharmacodynamic model building aid for NONMEM. Comput. Methods 489
Programs Biomed. 58:51-64. 490
12. Krishna, S., N. V. Nagaraja, T. Planche, T. Agbenyega, G. Bedo-Addo, D. Ansong, A. 491
Owusu-Ofori, A. L. Shroads, G. Henderson, A. Hutson, H. Derendorf, and P. W. 492
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

24
Stacpoole. 2001. Population pharmacokinetics of intramuscular quinine in children with 493
severe malaria. Antimicrob. Agents Chemother. 45:1803-1809. 494
13. Krishna, S., and N. J. White. 1996. Pharmacokinetics of quinine, chloroquine and 495
amodiaquine. Clinical implications. Clin. Pharmacokinet. 30:263-299. 496
14. Lesi, A., and M. Meremikwu. 2004. High first dose quinine regimen for treating severe 497
malaria. Cochrane Database Syst. Rev.:CD003341. 498
15. Lindbom, L., P. Pihlgren, and E. N. Jonsson. 2005. PsN-Toolkit--a collection of computer 499
intensive statistical methods for non-linear mixed effect modeling using NONMEM. 500
Comput. Methods Programs Biomed. 79:241-257. 501
16. Lindbom, L., J. Ribbing, and E. N. Jonsson. 2004. Perl-speaks-NONMEM (PsN)--a Perl 502
module for NONMEM related programming. Comput. Methods Programs Biomed. 75:85-503
94. 504
17. Maitland, K., S. Kiguli, R. O. Opoka, C. Engoru, P. Olupot-Olupot, S. O. Akech, R. 505
Nyeko, G. Mtove, H. Reyburn, T. Lang, B. Brent, J. A. Evans, J. K. Tibenderana, J. 506
Crawley, E. C. Russell, M. Levin, A. G. Babiker, and D. M. Gibb. 2011. Mortality after 507
fluid bolus in African children with severe infection. N. Engl. J. Med. 364:2483-2495. 508
18. Mansor, S. M., M. E. Molyneux, T. E. Taylor, S. A. Ward, J. J. Wirima, and G. 509
Edwards. 1991. Effect of Plasmodium falciparum malaria infection on the plasma 510
concentration of alpha 1-acid glycoprotein and the binding of quinine in Malawian children. 511
Br. J. Clin. Pharmacol. 32:317-321. 512
19. Mansor, S. M., T. E. Taylor, C. S. McGrath, G. Edwards, S. A. Ward, J. J. Wirima, 513
and M. E. Molyneux. 1990. The safety and kinetics of intramuscular quinine in Malawian 514
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

25
children with moderately severe falciparum malaria. Trans. R. Soc. Trop. Med. Hyg. 84:482-515
487. 516
20. Marsh, K., D. Forster, C. Waruiru, I. Mwangi, M. Winstanley, V. Marsh, C. Newton, P. 517
Winstanley, P. Warn, N. Peshu, and et al. 1995. Indicators of life-threatening malaria in 518
African children. N. Engl. J. Med. 332:1399-1404. 519
21. McLeay, S. C., G. A. Morrish, C. M. Kirkpatrick, and B. Green. 2012. The relationship 520
between drug clearance and body size: systematic review and meta-analysis of the literature 521
published from 2000 to 2007. Clin. Pharmacokinet. 51:319-330. 522
22. Mirghani, R. A., O. Ericsson, J. Cook, P. Yu, and L. L. Gustafsson. 2001. Simultaneous 523
determination of quinine and four metabolites in plasma and urine by high-performance 524
liquid chromatography. J. Chromatogr. B Biomed. Sci. Appl. 754:57-64. 525
23. Mirghani, R. A., U. Yasar, T. Zheng, J. M. Cook, L. L. Gustafsson, G. Tybring, and O. 526
Ericsson. 2002. Enzyme kinetics for the formation of 3-hydroxyquinine and three new 527
metabolites of quinine in vitro; 3-hydroxylation by CYP3A4 is indeed the major metabolic 528
pathway. Drug Metab. Dispos. 30:1368-1371. 529
24. Nontprasert, A., S. Pukrittayakamee, D. E. Kyle, S. Vanijanonta, and N. J. White. 1996. 530
Antimalarial activity and interactions between quinine, dihydroquinine and 3-531
hydroxyquinine against Plasmodium falciparum in vitro. Trans. R. Soc. Trop. Med. Hyg. 532
90:553-555. 533
25. Ogetii, G. N., S. Akech, J. Jemutai, M. Boga, E. Kivaya, G. Fegan, and K. Maitland. 534
2010. Hypoglycaemia in severe malaria, clinical associations and relationship to quinine 535
dosage. BMC Infect. Dis. 10:334. 536
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

26
26. Pasvol, G., C. R. Newton, P. A. Winstanley, W. M. Watkins, N. M. Peshu, J. B. Were, 537
K. Marsh, and D. A. Warrell. 1991. Quinine treatment of severe falciparum malaria in 538
African children: a randomized comparison of three regimens. Am. J. Trop. Med. Hyg. 539
45:702-713. 540
27. Petersson, K. J., E. Hanze, R. M. Savic, and M. O. Karlsson. 2009. Semiparametric 541
distributions with estimated shape parameters. Pharm. Res. 26:2174-2185. 542
28. Pukrittayakamee, S., S. Looareesuwan, D. Keeratithakul, T. M. Davis, P. Teja-543
Isavadharm, B. Nagachinta, A. Weber, A. L. Smith, D. Kyle, and N. J. White. 1997. A 544
study of the factors affecting the metabolic clearance of quinine in malaria. Eur. J. Clin. 545
Pharmacol. 52:487-493. 546
29. Pukrittayakamee, S., S. Wanwimolruk, K. Stepniewska, A. Jantra, S. Huyakorn, S. 547
Looareesuwan, and N. J. White. 2003. Quinine pharmacokinetic-pharmacodynamic 548
relationships in uncomplicated falciparum malaria. Antimicrob. Agents Chemother. 47:3458-549
3463. 550
30. Savic, R. M., D. M. Jonker, T. Kerbusch, and M. O. Karlsson. 2007. Implementation of a 551
transit compartment model for describing drug absorption in pharmacokinetic studies. J. 552
Pharmacokinet. Pharmacodyn. 34:711-726. 553
31. Schapira, A., T. Solomon, M. Julien, A. Macome, N. Parmar, I. Ruas, F. Simao, E. 554
Streat, and B. Betschart. 1993. Comparison of intramuscular and intravenous quinine for 555
the treatment of severe and complicated malaria in children. Trans. R. Soc. Trop. Med. Hyg. 556
87:299-302. 557
32. Shann, F., J. Stace, and M. Edstein. 1985. Pharmacokinetics of quinine in children. J. 558
Pediatr. 106:506-510. 559
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

27
33. Silamut, K., R. Hough, T. Eggelte, S. Pukrittayakamee, B. Angus, and N. J. White. 560
1995. A simple method for assessing quinine pre-treatment in acute malaria. Trans. R. Soc. 561
Trop. Med. Hyg. 89:665-667. 562
34. Silamut, K., P. Molunto, M. Ho, T. M. Davis, and N. J. White. 1991. Alpha 1-acid 563
glycoprotein (orosomucoid) and plasma protein binding of quinine in falciparum malaria. Br. 564
J. Clin. Pharmacol. 32:311-315. 565
35. Silamut, K., N. J. White, S. Looareesuwan, and D. A. Warrell. 1985. Binding of quinine 566
to plasma proteins in falciparum malaria. Am. J. Trop. Med. Hyg. 34:681-686. 567
36. Taggart, J. V., D. P. Earle, Jr., and et al. 1948. Studies on the chemotherapy of the human 568
malarias; the physiological disposition and antimalarial activity of the cinchona alkaloids. J. 569
Clin. Invest. 27:80-86. 570
37. Tarning, J., I. Zongo, F. A. Some, N. Rouamba, S. Parikh, P. J. Rosenthal, W. 571
Hanpithakpong, N. Jongrak, N. P. Day, N. J. White, F. Nosten, J. B. Ouedraogo, and N. 572
Lindegardh. 2012. Population pharmacokinetics and pharmacodynamics of piperaquine in 573
children with uncomplicated falciparum malaria. Clin. Pharmacol. Ther. 91:497-505. 574
38. Taylor, T. E., M. E. Molyneux, J. J. Wirima, K. A. Fletcher, and K. Morris. 1988. Blood 575
glucose levels in Malawian children before and during the administration of intravenous 576
quinine for severe falciparum malaria. N. Engl. J. Med. 319:1040-1047. 577
39. Tran, T. H., N. P. Day, H. P. Nguyen, T. H. Nguyen, P. L. Pham, X. S. Dinh, V. C. Ly, 578
V. Ha, D. Waller, T. E. Peto, and N. J. White. 1996. A controlled trial of artemether or 579
quinine in Vietnamese adults with severe falciparum malaria. N. Engl. J. Med. 335:76-83. 580
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

28
40. van Hensbroek, M. B., D. Kwiatkowski, B. van den Berg, F. J. Hoek, C. J. van Boxtel, 581
and P. A. Kager. 1996. Quinine pharmacokinetics in young children with severe malaria. 582
Am. J. Trop. Med. Hyg. 54:237-242. 583
41. von Seidlein, L., R. Olaosebikan, I. C. Hendriksen, S. J. Lee, O. T. Adedoyin, T. 584
Agbenyega, S. B. Nguah, K. Bojang, J. L. Deen, J. Evans, C. I. Fanello, E. Gomes, A. J. 585
Pedro, C. Kahabuka, C. Karema, E. Kivaya, K. Maitland, O. A. Mokuolu, G. Mtove, J. 586
Mwanga-Amumpaire, B. Nadjm, M. Nansumba, W. P. Ngum, M. A. Onyamboko, H. 587
Reyburn, T. Sakulthaew, K. Silamut, A. K. Tshefu, N. Umulisa, S. Gesase, N. P. Day, N. 588
J. White, and A. M. Dondorp. 2012. Predicting the clinical outcome of severe falciparum 589
malaria in african children: findings from a large randomized trial. Clin. Infect. Dis. 590
54:1080-1090. 591
42. Waller, D., S. Krishna, C. Craddock, D. Brewster, A. Jammeh, D. Kwiatkowski, J. 592
Karbwang, P. Molunto, and N. J. White. 1990. The pharmacokinetic properties of 593
intramuscular quinine in Gambian children with severe falciparum malaria. Trans. R. Soc. 594
Trop. Med. Hyg. 84:488-491. 595
43. Waller, D., S. Krishna, J. Crawley, K. Miller, F. Nosten, D. Chapman, F. O. ter Kuile, 596
C. Craddock, C. Berry, P. A. Holloway, and et al. 1995. Clinical features and outcome of 597
severe malaria in Gambian children. Clin. Infect. Dis. 21:577-587. 598
44. Wanwimolruk, S., M. Sunbhanich, M. Pongmarutai, and P. Patamasucon. 1986. Effects 599
of cimetidine and ranitidine on the pharmacokinetics of quinine. Br. J. Clin. Pharmacol. 600
22:346-350. 601
45. White, N. J. 1995. Optimal regimens of parenteral quinine. Trans. R. Soc. Trop. Med. Hyg. 602
89:462-464. 603
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

29
46. White, N. J., S. Looareesuwan, D. A. Warrell, M. J. Warrell, D. Bunnag, and T. 604
Harinasuta. 1982. Quinine pharmacokinetics and toxicity in cerebral and uncomplicated 605
falciparum malaria. Am. J. Med. 73:564-572. 606
47. White, N. J., S. Looareesuwan, D. A. Warrell, M. J. Warrell, P. Chanthavanich, D. 607
Bunnag, and T. Harinasuta. 1983. Quinine loading dose in cerebral malaria. Am. J. Trop. 608
Med. Hyg. 32:1-5. 609
48. White, N. J., K. D. Miller, K. Marsh, C. D. Berry, R. C. Turner, D. H. Williamson, and 610
J. Brown. 1987. Hypoglycaemia in African children with severe malaria. Lancet 1:708-711. 611
49. White, N. J., D. A. Warrell, P. Chanthavanich, S. Looareesuwan, M. J. Warrell, S. 612
Krishna, D. H. Williamson, and R. C. Turner. 1983. Severe hypoglycemia and 613
hyperinsulinemia in falciparum malaria. N. Engl. J. Med. 309:61-66. 614
50. WHO. 1990. Severe and complicated malaria. Trans. R. Soc. Trop. Med. Hyg. 84 (Suppl 615
2):1-65. 616
51. WHO. 2000. Severe falciparum malaria. Trans. R. Soc. Trop. Med. Hyg. 94 (Suppl 1):S1-617
90. 618
52. WHO 2008, posting date. World Malaria Report 2008. [Online.] 619
53. WHO Multicentre Growth Reference Study Group 2006, posting date. WHO Child 620
Growth Standards: Length/height-for-age, weight-for-age, weight-for-length, weight-for-621
height and body mass index-for-age: Methods and development. World Health Organization. 622
[Online.] 623
54. Winstanley, P., C. Newton, W. Watkins, E. Mberu, S. Ward, P. Warn, I. Mwangi, C. 624
Waruiru, G. Pasvol, D. Warrell, and et al. 1993. Towards optimal regimens of parenteral 625
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

30
quinine for young African children with cerebral malaria: the importance of unbound quinine 626
concentration. Trans. R. Soc. Trop. Med. Hyg. 87:201-206. 627
55. Zahn, J. R., G. F. Brinton, and E. Norton. 1981. Ocular quinine toxicity followed by 628
electroretinogram, electro-oculogram, and pattern visually evoked potential. Am. J. Optom. 629
Physiol. Opt. 58:492-498. 630
631
632
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

31
Table legends 633
634
Table 1. Demographic, clinical and laboratory characteristics of children admitted with severe 635
malaria. 636
637
Table 2. Parameter estimates of the final model describing quinine population pharmacokinetics 638
in children (n=75) with severe malaria 639
640
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

32
Figure legends 641
Figure 1. Goodness-of-fit diagnostics of the final population pharmacokinetic model of quinine 642
in children with severe malaria. Broken line, a locally weighted least-squares regression; solid 643
line, line of identity. The observed concentrations, population predictions, and individual 644
predictions were transformed into their logarithms (base 10). 645
646
Figure 2. Visual predictive check of the final model describing the population pharmacokinetics 647
of quinine in children with severe malaria. Open circles, observed data points; solid lines, 5th, 648
50th, and 95th percentiles of the observed data. Shaded area, 95% confidence interval of 649
simulated (n=2,000) 5th, 50th, and 95th percentiles. Venous plasma quinine concentrations were 650
transformed into their logarithms (base 10). 651
652
Figure 3. Predicted population pharmacokinetic profiles of quinine A) at different body weights 653
(gray solid profiles): 5 kg, (− · −), 10 kg (− −) and 20 kg (―) are highlighted in black; and B) 654
after a loading dose of 20 mg/kg (―) versus a routine dose of 10 mg/kg (− −): 10 kg are 655
highlighted in black. 656
657
Figure 4. Visual predictive check for the Kaplan-Meier survival curve. The solid black line 658
represents the observed Kaplan-Meier curve and the shaded gray area represents the 659
corresponding 90% prediction interval derived from model simulations (n=1,000) of the final 660
PK-PD model. 661
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

33
Figure 5. Predicted total quinine exposure (AUC0-8hrs) and maximum concentration (CMAX) after 662
the first dose stratified for outcome. Error bars indicate median and interquartile range. 663
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

1
Table 1. Demographic, clinical and laboratory characteristics of children admitted with
severe malaria.
Variable
Children with severe malaria
n=75
Age (yr) 2.4 (0.33 to 8.1)
Weight (kg) 11 (5.5 to 27)
Weight-for-age Z-score -1.0 (-4.1 to 1.0)
Coma 27 (36%)
Prostration 46 (61%)
Convulsions 34 (45%)
Shock a 16 (21%)
Respiratory distress 7 (9%)
Acidosis (base excess <-8 mmol/L) 32 (46%)
Hypoglycemia (glucose<3mmol/L) 18 (24%)
Anemia 27 (36%)
Black Water Fever 7 (9%)
Axillary temperature (°C) 38.2 (35.4 to 41.8)
Heart rate (beats/min) 154 (98 to 202)
Respiratory rate (breath/min) 50 (24 to 98)
Glucose (mg/dL) 95 (15 to 240)
Blood urea nitrogen (mg/dL) 13 (4 to 97)
Hemoglobin (g/dL) 7.1 (2.6 to 13.2)
pH 7.36 (7.28 to 7.42)
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

2
HCO3 (mmol/L) 17.8 (3.5 to 25.6)
Base excess (mmol/L) -8 (-28 to 2)
ASAT (U/L) 85 (7 to 3180)
ALAT (U/L) 22 (3 to 1490)
Total bilirubin (μmol/L) 38 (5 to 250)
HIV positive 5 (6.7%)
Parasitemia (parasites/µL)
(geometric mean, 95%CI) 31,900 (17,300-58,900)
Plasma PfHRP2 (ng/mL)
(geometric mean, 95%CI) 2,070 (1,470-2,900)
Data are reported as median (range) or number (%), unless otherwise stated.
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

1
Table 2. Parameter estimates of the final model describing quinine population
pharmacokinetics in children (n=75) with severe malaria
Variable
Population estimate a
(% RSE b) 95% CI. b
Fixed PK effects
CL/F (L/h) 0.792 (6.42) 0.698-0.898
V/F (L) 13.7 (6.56) 12.1-15.6
DUR (h) 1.42 (21.1) 0.486-1.70
Fixed PD effects
Baseline hazard (h-1) 0.016 (42.7%) 0.00586-0.0342
AUC50 (h×mg/L) 64.8 (96.9%) 21.8-387
Random PK effects
ηCL/F 0.128 (28.7) 0.0620-0.201
ηV/F 0.176 (25.7) 0.0927-0.262
ηCL/F ~ ηV/F 0.15 (21.5) 0.0835-0.206
σ 0.0942 (7.76) 0.0671-0.124
Post-hoc PK estimates c
CL/F (L/h/kg) 0.0741 0.0455-0.144
V/F (L/kg) 1.24 0.645-2.89
t1/2 (hours) 12.1 9.63-14.3
CMAX (mg/L) 13.4 7.20-24.8
AUC0-7.5h (h×mg/L) 78.9 42.3-148
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

2
a Computed population mean values from NONMEM are calculated for a typical patient with a
body weight of 11 kg.
b Assessed by non-parametric bootstrap method (n=1,586 successful iterations out of 2000 for
PK and n=1,532 successful iterations out of 2000 for PD) of the final model. Relative standard
error (% RSE) is calculated as 100×(standard deviation/mean value). 95% confidence interval
(95% CI.) is displayed as the 2.5 to 97.5 percentile of bootstrap estimates.
c Post-hoc estimates are displayed as median values with 2.5 to 97.5 percentiles of empirical
Bayes estimates.
CL/F = elimination clearance; V/F = volume of distribution; F = intramuscular bioavailability;
DUR = duration of zero-order absorption; Baseline hazard = baseline hazard of death per hour in
the time-to-event model; AUC50 = cumulative exposure associated with a 50% reduction in the
baseline hazard of death; η = inter-individual variability; ηCL/F ~ ηV/F = correlation of random
effects on CL/F and V/F; σ = additive residual variance error; t1/2 = terminal elimination half-life;
AUC0-7.5h = area under the concentration-time curve from time-point 0 to 7.5 hours; CMAX =
predicted peak concentration after first dose.
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

1 10
1
10
Population predictions (mg/L)
Ob
serv
ati
on
s (
mg
/L)
1 10
1
10
Individual predictions (mg/L)
Ob
serv
ati
on
s (
mg
/L)
1 10-4
-2
0
2
4
Population predictions (mg/L)
Co
nd
itio
nal w
eig
hte
d r
esid
uals
0 10 20-4
-2
0
2
4
Time (hours)
Co
nd
itio
nal w
eig
hte
d r
esid
uals
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

Time after dose (hours)
Concentr
ation (
mg/L
)
1
10
2 4 6 8
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

0 4 8 12 16 20 240
4
8
12
16
20
Time (hours)
Co
ncen
trati
on
(m
g/L
)
0 4 8 12 16 20 240
4
8
12
16
20
Time (hours)
Co
ncen
trati
on
(m
g/L
)A)
B)
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

Time (hours)
Surv
ival (%
)
50
60
70
80
90
100
0 50 100
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

Survived Died0
50
100
150
200
AU
C0-8
hr
(h´
mg
/L)
Survived Died0
10
20
30
40
CM
AX (
mg
/L)
on May 16, 2018 by guest
http://aac.asm.org/
Dow
nloaded from