Embed Size (px)
Citation preview
Antifungal therapy in ICU prophylaxis pre-emptive and targeted
Is it applicablewhen how
Antifungal de-escalation
The case for antifungal stewardship
bull Dr Rafael Zaragoza
Conflicts
bull Pfizer
bull Astellas
bull MSD
bull Gilead
bull Cephalon
SECOND RECOMMENDATION
bull Enjoy City of
Sciences and arts
ndash Opera house
ndash Hemisferic
ndash Sciences museum
ndash Agora
Allaacute vamoshellip
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
Antimicrobial optimization strategies in ICU
GuidelinesProtocols
Restricting the hospital formulary
Scheduled changes in antibiotic
Combining antibiotic therapy
Antibiotic rotation
Area-specific antimicrobial therapy
Antimicrobial de-escalation
Kollef MH Crit Care 20015 189-95
INTRODUCTION Antimicrobial stewardship (AMS) has overwhelmingly focussed on antibiotics
while antifungal agents have been largely neglected despite the few published audits of antifungal drug use demonstrating clear deficiencies in prescibing behavior
Invasive fungal diseases (IFDs) have a lower institutional incidence relative to infections caused by multiresistant bacteria but their health and economic burden are substantial
Pharmacy costs inclusive of antifungal agents are a major determinant of IFD-attributable hospital cost High drug costs and the toxicities of antifungal agents are the principal rationale for AFS while antifungal resistance is an emerging but less prevalent issue
Nonculture-based tests may enhance AFS but refinement of both target populations and clinical pathways incorporating their use is required Performance indicators including structural process and outcome measures are integral for demonstrating the value of AFS programmes
Ananda-Rajah MR Slavin MA Thursky KT
Curr Opin Infect Dis 2012 Feb25(1)107-15
De-escalation of antibiotic therapy Concept
ldquoCould be considered as a strategy to balance the need to provide adequate initial antibiotic treatment of high risk patients with the avoidance of unnecessary antibiotic utilization which promotes resistancerdquo
Inadequate empirical antibitibic therapy and ICU-Bacteremia
6229
0
50
100
I EAT NO I EAT
I nhospital
Mortality
Ibrahim et al Chest 2000 118 146-155
N= 492 Candida spp VRE meticilin resistant S aureus CNS Pseudomonas aeruginosa
IEAT= 299
plt 0001
Inadequate empirical antibitibic therapy and ICU-Bacteremia
30235
0
10
20
30
I EAT NO-I EAT Related
mortality
N= 166 CNS Acinetobacter baumannii Pseudomonas aeruginosa Candida spp
Zaragoza R et al Clin Microbiol Infect 2003 May 9(5)412-418
IEAT= 235
pgt005
APPROACH TO ANTIFUNGAL TREATMENT
Pre-emptive and Empirical Therapy ICCd
iquestPrevious azol`s use +- clinical unstable (MOF severe sepsis) +- suspected or previous infection by C krusei o C glabrata +- multiple colonization by no-C albicans spp +- ICU stay and risk factors (drug-interactions kind of patient pe transplantation peritonitis)
-Fluconazole 400-800 mg IVd If possible switching to oral therapy (400 mgd)
We must considered AF rapid broad spectrum and PKPD
optimized
Yes NO
-Anidulafungin 200 mg24 (d1)+100 mg d -Caspofungin 70 mg24 h (d1) + 50 mg d -Micafungina 150 mg24 hs - Amphotericin B-Lipidic Complex 3-5 mgkgd - Amphotericin B- Lipossomal 3 mgkgd - Voriconazol e iv 6 mgkg12h (d1) + 4 mgkg12h
EVEN POSSIBLE DE-ESCALATION
Zaragoza R Pemaacuten J J Invasive Fungal Infect 2007150-58
Antifungal de-escalation strategy
Initially a broad spectrum antitungal treatment is administrated until the agent of infection was identified
Echinocandins AMPHOTERICINS
Microbiogical data
Patientacutes physician criteria
Maintenance of broad spectrum combination
DT Switching to a narrow spectrum
Guery ICM2008
Candidemia pacientes no-neutropenicos De-escalation IDSA 2008
De-escalation even it`s possible (I-A)
Targeted Treatment of Candidaemia
Echinocandins
Compound SoR QoE Reference Comment
Anidulafungin
200100
A I Reboli NEJM 2007 bull Broad spectrum
bull Resistance rare
bull Fungicidal
bull Local epidemiology
bull C parapsilosis C krusei
bull Safety profile
bull Less drug-drug interactions
than caspofungin
Caspofungin
7050
A I Mora-Duarte NEJM 2002
Pappas CID 2007
bull Largely as above
Micafungin
100
A I Kuse Lancet 2007
Pappas CID 2007
bull Largely as above
bull Consider EMA warning label
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
Conflicts
bull Pfizer
bull Astellas
bull MSD
bull Gilead
bull Cephalon
SECOND RECOMMENDATION
bull Enjoy City of
Sciences and arts
ndash Opera house
ndash Hemisferic
ndash Sciences museum
ndash Agora
Allaacute vamoshellip
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
Antimicrobial optimization strategies in ICU
GuidelinesProtocols
Restricting the hospital formulary
Scheduled changes in antibiotic
Combining antibiotic therapy
Antibiotic rotation
Area-specific antimicrobial therapy
Antimicrobial de-escalation
Kollef MH Crit Care 20015 189-95
INTRODUCTION Antimicrobial stewardship (AMS) has overwhelmingly focussed on antibiotics
while antifungal agents have been largely neglected despite the few published audits of antifungal drug use demonstrating clear deficiencies in prescibing behavior
Invasive fungal diseases (IFDs) have a lower institutional incidence relative to infections caused by multiresistant bacteria but their health and economic burden are substantial
Pharmacy costs inclusive of antifungal agents are a major determinant of IFD-attributable hospital cost High drug costs and the toxicities of antifungal agents are the principal rationale for AFS while antifungal resistance is an emerging but less prevalent issue
Nonculture-based tests may enhance AFS but refinement of both target populations and clinical pathways incorporating their use is required Performance indicators including structural process and outcome measures are integral for demonstrating the value of AFS programmes
Ananda-Rajah MR Slavin MA Thursky KT
Curr Opin Infect Dis 2012 Feb25(1)107-15
De-escalation of antibiotic therapy Concept
ldquoCould be considered as a strategy to balance the need to provide adequate initial antibiotic treatment of high risk patients with the avoidance of unnecessary antibiotic utilization which promotes resistancerdquo
Inadequate empirical antibitibic therapy and ICU-Bacteremia
6229
0
50
100
I EAT NO I EAT
I nhospital
Mortality
Ibrahim et al Chest 2000 118 146-155
N= 492 Candida spp VRE meticilin resistant S aureus CNS Pseudomonas aeruginosa
IEAT= 299
plt 0001
Inadequate empirical antibitibic therapy and ICU-Bacteremia
30235
0
10
20
30
I EAT NO-I EAT Related
mortality
N= 166 CNS Acinetobacter baumannii Pseudomonas aeruginosa Candida spp
Zaragoza R et al Clin Microbiol Infect 2003 May 9(5)412-418
IEAT= 235
pgt005
APPROACH TO ANTIFUNGAL TREATMENT
Pre-emptive and Empirical Therapy ICCd
iquestPrevious azol`s use +- clinical unstable (MOF severe sepsis) +- suspected or previous infection by C krusei o C glabrata +- multiple colonization by no-C albicans spp +- ICU stay and risk factors (drug-interactions kind of patient pe transplantation peritonitis)
-Fluconazole 400-800 mg IVd If possible switching to oral therapy (400 mgd)
We must considered AF rapid broad spectrum and PKPD
optimized
Yes NO
-Anidulafungin 200 mg24 (d1)+100 mg d -Caspofungin 70 mg24 h (d1) + 50 mg d -Micafungina 150 mg24 hs - Amphotericin B-Lipidic Complex 3-5 mgkgd - Amphotericin B- Lipossomal 3 mgkgd - Voriconazol e iv 6 mgkg12h (d1) + 4 mgkg12h
EVEN POSSIBLE DE-ESCALATION
Zaragoza R Pemaacuten J J Invasive Fungal Infect 2007150-58
Antifungal de-escalation strategy
Initially a broad spectrum antitungal treatment is administrated until the agent of infection was identified
Echinocandins AMPHOTERICINS
Microbiogical data
Patientacutes physician criteria
Maintenance of broad spectrum combination
DT Switching to a narrow spectrum
Guery ICM2008
Candidemia pacientes no-neutropenicos De-escalation IDSA 2008
De-escalation even it`s possible (I-A)
Targeted Treatment of Candidaemia
Echinocandins
Compound SoR QoE Reference Comment
Anidulafungin
200100
A I Reboli NEJM 2007 bull Broad spectrum
bull Resistance rare
bull Fungicidal
bull Local epidemiology
bull C parapsilosis C krusei
bull Safety profile
bull Less drug-drug interactions
than caspofungin
Caspofungin
7050
A I Mora-Duarte NEJM 2002
Pappas CID 2007
bull Largely as above
Micafungin
100
A I Kuse Lancet 2007
Pappas CID 2007
bull Largely as above
bull Consider EMA warning label
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
SECOND RECOMMENDATION
bull Enjoy City of
Sciences and arts
ndash Opera house
ndash Hemisferic
ndash Sciences museum
ndash Agora
Allaacute vamoshellip
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
Antimicrobial optimization strategies in ICU
GuidelinesProtocols
Restricting the hospital formulary
Scheduled changes in antibiotic
Combining antibiotic therapy
Antibiotic rotation
Area-specific antimicrobial therapy
Antimicrobial de-escalation
Kollef MH Crit Care 20015 189-95
INTRODUCTION Antimicrobial stewardship (AMS) has overwhelmingly focussed on antibiotics
while antifungal agents have been largely neglected despite the few published audits of antifungal drug use demonstrating clear deficiencies in prescibing behavior
Invasive fungal diseases (IFDs) have a lower institutional incidence relative to infections caused by multiresistant bacteria but their health and economic burden are substantial
Pharmacy costs inclusive of antifungal agents are a major determinant of IFD-attributable hospital cost High drug costs and the toxicities of antifungal agents are the principal rationale for AFS while antifungal resistance is an emerging but less prevalent issue
Nonculture-based tests may enhance AFS but refinement of both target populations and clinical pathways incorporating their use is required Performance indicators including structural process and outcome measures are integral for demonstrating the value of AFS programmes
Ananda-Rajah MR Slavin MA Thursky KT
Curr Opin Infect Dis 2012 Feb25(1)107-15
De-escalation of antibiotic therapy Concept
ldquoCould be considered as a strategy to balance the need to provide adequate initial antibiotic treatment of high risk patients with the avoidance of unnecessary antibiotic utilization which promotes resistancerdquo
Inadequate empirical antibitibic therapy and ICU-Bacteremia
6229
0
50
100
I EAT NO I EAT
I nhospital
Mortality
Ibrahim et al Chest 2000 118 146-155
N= 492 Candida spp VRE meticilin resistant S aureus CNS Pseudomonas aeruginosa
IEAT= 299
plt 0001
Inadequate empirical antibitibic therapy and ICU-Bacteremia
30235
0
10
20
30
I EAT NO-I EAT Related
mortality
N= 166 CNS Acinetobacter baumannii Pseudomonas aeruginosa Candida spp
Zaragoza R et al Clin Microbiol Infect 2003 May 9(5)412-418
IEAT= 235
pgt005
APPROACH TO ANTIFUNGAL TREATMENT
Pre-emptive and Empirical Therapy ICCd
iquestPrevious azol`s use +- clinical unstable (MOF severe sepsis) +- suspected or previous infection by C krusei o C glabrata +- multiple colonization by no-C albicans spp +- ICU stay and risk factors (drug-interactions kind of patient pe transplantation peritonitis)
-Fluconazole 400-800 mg IVd If possible switching to oral therapy (400 mgd)
We must considered AF rapid broad spectrum and PKPD
optimized
Yes NO
-Anidulafungin 200 mg24 (d1)+100 mg d -Caspofungin 70 mg24 h (d1) + 50 mg d -Micafungina 150 mg24 hs - Amphotericin B-Lipidic Complex 3-5 mgkgd - Amphotericin B- Lipossomal 3 mgkgd - Voriconazol e iv 6 mgkg12h (d1) + 4 mgkg12h
EVEN POSSIBLE DE-ESCALATION
Zaragoza R Pemaacuten J J Invasive Fungal Infect 2007150-58
Antifungal de-escalation strategy
Initially a broad spectrum antitungal treatment is administrated until the agent of infection was identified
Echinocandins AMPHOTERICINS
Microbiogical data
Patientacutes physician criteria
Maintenance of broad spectrum combination
DT Switching to a narrow spectrum
Guery ICM2008
Candidemia pacientes no-neutropenicos De-escalation IDSA 2008
De-escalation even it`s possible (I-A)
Targeted Treatment of Candidaemia
Echinocandins
Compound SoR QoE Reference Comment
Anidulafungin
200100
A I Reboli NEJM 2007 bull Broad spectrum
bull Resistance rare
bull Fungicidal
bull Local epidemiology
bull C parapsilosis C krusei
bull Safety profile
bull Less drug-drug interactions
than caspofungin
Caspofungin
7050
A I Mora-Duarte NEJM 2002
Pappas CID 2007
bull Largely as above
Micafungin
100
A I Kuse Lancet 2007
Pappas CID 2007
bull Largely as above
bull Consider EMA warning label
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
Allaacute vamoshellip
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
Antimicrobial optimization strategies in ICU
GuidelinesProtocols
Restricting the hospital formulary
Scheduled changes in antibiotic
Combining antibiotic therapy
Antibiotic rotation
Area-specific antimicrobial therapy
Antimicrobial de-escalation
Kollef MH Crit Care 20015 189-95
INTRODUCTION Antimicrobial stewardship (AMS) has overwhelmingly focussed on antibiotics
while antifungal agents have been largely neglected despite the few published audits of antifungal drug use demonstrating clear deficiencies in prescibing behavior
Invasive fungal diseases (IFDs) have a lower institutional incidence relative to infections caused by multiresistant bacteria but their health and economic burden are substantial
Pharmacy costs inclusive of antifungal agents are a major determinant of IFD-attributable hospital cost High drug costs and the toxicities of antifungal agents are the principal rationale for AFS while antifungal resistance is an emerging but less prevalent issue
Nonculture-based tests may enhance AFS but refinement of both target populations and clinical pathways incorporating their use is required Performance indicators including structural process and outcome measures are integral for demonstrating the value of AFS programmes
Ananda-Rajah MR Slavin MA Thursky KT
Curr Opin Infect Dis 2012 Feb25(1)107-15
De-escalation of antibiotic therapy Concept
ldquoCould be considered as a strategy to balance the need to provide adequate initial antibiotic treatment of high risk patients with the avoidance of unnecessary antibiotic utilization which promotes resistancerdquo
Inadequate empirical antibitibic therapy and ICU-Bacteremia
6229
0
50
100
I EAT NO I EAT
I nhospital
Mortality
Ibrahim et al Chest 2000 118 146-155
N= 492 Candida spp VRE meticilin resistant S aureus CNS Pseudomonas aeruginosa
IEAT= 299
plt 0001
Inadequate empirical antibitibic therapy and ICU-Bacteremia
30235
0
10
20
30
I EAT NO-I EAT Related
mortality
N= 166 CNS Acinetobacter baumannii Pseudomonas aeruginosa Candida spp
Zaragoza R et al Clin Microbiol Infect 2003 May 9(5)412-418
IEAT= 235
pgt005
APPROACH TO ANTIFUNGAL TREATMENT
Pre-emptive and Empirical Therapy ICCd
iquestPrevious azol`s use +- clinical unstable (MOF severe sepsis) +- suspected or previous infection by C krusei o C glabrata +- multiple colonization by no-C albicans spp +- ICU stay and risk factors (drug-interactions kind of patient pe transplantation peritonitis)
-Fluconazole 400-800 mg IVd If possible switching to oral therapy (400 mgd)
We must considered AF rapid broad spectrum and PKPD
optimized
Yes NO
-Anidulafungin 200 mg24 (d1)+100 mg d -Caspofungin 70 mg24 h (d1) + 50 mg d -Micafungina 150 mg24 hs - Amphotericin B-Lipidic Complex 3-5 mgkgd - Amphotericin B- Lipossomal 3 mgkgd - Voriconazol e iv 6 mgkg12h (d1) + 4 mgkg12h
EVEN POSSIBLE DE-ESCALATION
Zaragoza R Pemaacuten J J Invasive Fungal Infect 2007150-58
Antifungal de-escalation strategy
Initially a broad spectrum antitungal treatment is administrated until the agent of infection was identified
Echinocandins AMPHOTERICINS
Microbiogical data
Patientacutes physician criteria
Maintenance of broad spectrum combination
DT Switching to a narrow spectrum
Guery ICM2008
Candidemia pacientes no-neutropenicos De-escalation IDSA 2008
De-escalation even it`s possible (I-A)
Targeted Treatment of Candidaemia
Echinocandins
Compound SoR QoE Reference Comment
Anidulafungin
200100
A I Reboli NEJM 2007 bull Broad spectrum
bull Resistance rare
bull Fungicidal
bull Local epidemiology
bull C parapsilosis C krusei
bull Safety profile
bull Less drug-drug interactions
than caspofungin
Caspofungin
7050
A I Mora-Duarte NEJM 2002
Pappas CID 2007
bull Largely as above
Micafungin
100
A I Kuse Lancet 2007
Pappas CID 2007
bull Largely as above
bull Consider EMA warning label
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
Antimicrobial optimization strategies in ICU
GuidelinesProtocols
Restricting the hospital formulary
Scheduled changes in antibiotic
Combining antibiotic therapy
Antibiotic rotation
Area-specific antimicrobial therapy
Antimicrobial de-escalation
Kollef MH Crit Care 20015 189-95
INTRODUCTION Antimicrobial stewardship (AMS) has overwhelmingly focussed on antibiotics
while antifungal agents have been largely neglected despite the few published audits of antifungal drug use demonstrating clear deficiencies in prescibing behavior
Invasive fungal diseases (IFDs) have a lower institutional incidence relative to infections caused by multiresistant bacteria but their health and economic burden are substantial
Pharmacy costs inclusive of antifungal agents are a major determinant of IFD-attributable hospital cost High drug costs and the toxicities of antifungal agents are the principal rationale for AFS while antifungal resistance is an emerging but less prevalent issue
Nonculture-based tests may enhance AFS but refinement of both target populations and clinical pathways incorporating their use is required Performance indicators including structural process and outcome measures are integral for demonstrating the value of AFS programmes
Ananda-Rajah MR Slavin MA Thursky KT
Curr Opin Infect Dis 2012 Feb25(1)107-15
De-escalation of antibiotic therapy Concept
ldquoCould be considered as a strategy to balance the need to provide adequate initial antibiotic treatment of high risk patients with the avoidance of unnecessary antibiotic utilization which promotes resistancerdquo
Inadequate empirical antibitibic therapy and ICU-Bacteremia
6229
0
50
100
I EAT NO I EAT
I nhospital
Mortality
Ibrahim et al Chest 2000 118 146-155
N= 492 Candida spp VRE meticilin resistant S aureus CNS Pseudomonas aeruginosa
IEAT= 299
plt 0001
Inadequate empirical antibitibic therapy and ICU-Bacteremia
30235
0
10
20
30
I EAT NO-I EAT Related
mortality
N= 166 CNS Acinetobacter baumannii Pseudomonas aeruginosa Candida spp
Zaragoza R et al Clin Microbiol Infect 2003 May 9(5)412-418
IEAT= 235
pgt005
APPROACH TO ANTIFUNGAL TREATMENT
Pre-emptive and Empirical Therapy ICCd
iquestPrevious azol`s use +- clinical unstable (MOF severe sepsis) +- suspected or previous infection by C krusei o C glabrata +- multiple colonization by no-C albicans spp +- ICU stay and risk factors (drug-interactions kind of patient pe transplantation peritonitis)
-Fluconazole 400-800 mg IVd If possible switching to oral therapy (400 mgd)
We must considered AF rapid broad spectrum and PKPD
optimized
Yes NO
-Anidulafungin 200 mg24 (d1)+100 mg d -Caspofungin 70 mg24 h (d1) + 50 mg d -Micafungina 150 mg24 hs - Amphotericin B-Lipidic Complex 3-5 mgkgd - Amphotericin B- Lipossomal 3 mgkgd - Voriconazol e iv 6 mgkg12h (d1) + 4 mgkg12h
EVEN POSSIBLE DE-ESCALATION
Zaragoza R Pemaacuten J J Invasive Fungal Infect 2007150-58
Antifungal de-escalation strategy
Initially a broad spectrum antitungal treatment is administrated until the agent of infection was identified
Echinocandins AMPHOTERICINS
Microbiogical data
Patientacutes physician criteria
Maintenance of broad spectrum combination
DT Switching to a narrow spectrum
Guery ICM2008
Candidemia pacientes no-neutropenicos De-escalation IDSA 2008
De-escalation even it`s possible (I-A)
Targeted Treatment of Candidaemia
Echinocandins
Compound SoR QoE Reference Comment
Anidulafungin
200100
A I Reboli NEJM 2007 bull Broad spectrum
bull Resistance rare
bull Fungicidal
bull Local epidemiology
bull C parapsilosis C krusei
bull Safety profile
bull Less drug-drug interactions
than caspofungin
Caspofungin
7050
A I Mora-Duarte NEJM 2002
Pappas CID 2007
bull Largely as above
Micafungin
100
A I Kuse Lancet 2007
Pappas CID 2007
bull Largely as above
bull Consider EMA warning label
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
Antimicrobial optimization strategies in ICU
GuidelinesProtocols
Restricting the hospital formulary
Scheduled changes in antibiotic
Combining antibiotic therapy
Antibiotic rotation
Area-specific antimicrobial therapy
Antimicrobial de-escalation
Kollef MH Crit Care 20015 189-95
INTRODUCTION Antimicrobial stewardship (AMS) has overwhelmingly focussed on antibiotics
while antifungal agents have been largely neglected despite the few published audits of antifungal drug use demonstrating clear deficiencies in prescibing behavior
Invasive fungal diseases (IFDs) have a lower institutional incidence relative to infections caused by multiresistant bacteria but their health and economic burden are substantial
Pharmacy costs inclusive of antifungal agents are a major determinant of IFD-attributable hospital cost High drug costs and the toxicities of antifungal agents are the principal rationale for AFS while antifungal resistance is an emerging but less prevalent issue
Nonculture-based tests may enhance AFS but refinement of both target populations and clinical pathways incorporating their use is required Performance indicators including structural process and outcome measures are integral for demonstrating the value of AFS programmes
Ananda-Rajah MR Slavin MA Thursky KT
Curr Opin Infect Dis 2012 Feb25(1)107-15
De-escalation of antibiotic therapy Concept
ldquoCould be considered as a strategy to balance the need to provide adequate initial antibiotic treatment of high risk patients with the avoidance of unnecessary antibiotic utilization which promotes resistancerdquo
Inadequate empirical antibitibic therapy and ICU-Bacteremia
6229
0
50
100
I EAT NO I EAT
I nhospital
Mortality
Ibrahim et al Chest 2000 118 146-155
N= 492 Candida spp VRE meticilin resistant S aureus CNS Pseudomonas aeruginosa
IEAT= 299
plt 0001
Inadequate empirical antibitibic therapy and ICU-Bacteremia
30235
0
10
20
30
I EAT NO-I EAT Related
mortality
N= 166 CNS Acinetobacter baumannii Pseudomonas aeruginosa Candida spp
Zaragoza R et al Clin Microbiol Infect 2003 May 9(5)412-418
IEAT= 235
pgt005
APPROACH TO ANTIFUNGAL TREATMENT
Pre-emptive and Empirical Therapy ICCd
iquestPrevious azol`s use +- clinical unstable (MOF severe sepsis) +- suspected or previous infection by C krusei o C glabrata +- multiple colonization by no-C albicans spp +- ICU stay and risk factors (drug-interactions kind of patient pe transplantation peritonitis)
-Fluconazole 400-800 mg IVd If possible switching to oral therapy (400 mgd)
We must considered AF rapid broad spectrum and PKPD
optimized
Yes NO
-Anidulafungin 200 mg24 (d1)+100 mg d -Caspofungin 70 mg24 h (d1) + 50 mg d -Micafungina 150 mg24 hs - Amphotericin B-Lipidic Complex 3-5 mgkgd - Amphotericin B- Lipossomal 3 mgkgd - Voriconazol e iv 6 mgkg12h (d1) + 4 mgkg12h
EVEN POSSIBLE DE-ESCALATION
Zaragoza R Pemaacuten J J Invasive Fungal Infect 2007150-58
Antifungal de-escalation strategy
Initially a broad spectrum antitungal treatment is administrated until the agent of infection was identified
Echinocandins AMPHOTERICINS
Microbiogical data
Patientacutes physician criteria
Maintenance of broad spectrum combination
DT Switching to a narrow spectrum
Guery ICM2008
Candidemia pacientes no-neutropenicos De-escalation IDSA 2008
De-escalation even it`s possible (I-A)
Targeted Treatment of Candidaemia
Echinocandins
Compound SoR QoE Reference Comment
Anidulafungin
200100
A I Reboli NEJM 2007 bull Broad spectrum
bull Resistance rare
bull Fungicidal
bull Local epidemiology
bull C parapsilosis C krusei
bull Safety profile
bull Less drug-drug interactions
than caspofungin
Caspofungin
7050
A I Mora-Duarte NEJM 2002
Pappas CID 2007
bull Largely as above
Micafungin
100
A I Kuse Lancet 2007
Pappas CID 2007
bull Largely as above
bull Consider EMA warning label
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
INTRODUCTION Antimicrobial stewardship (AMS) has overwhelmingly focussed on antibiotics
while antifungal agents have been largely neglected despite the few published audits of antifungal drug use demonstrating clear deficiencies in prescibing behavior
Invasive fungal diseases (IFDs) have a lower institutional incidence relative to infections caused by multiresistant bacteria but their health and economic burden are substantial
Pharmacy costs inclusive of antifungal agents are a major determinant of IFD-attributable hospital cost High drug costs and the toxicities of antifungal agents are the principal rationale for AFS while antifungal resistance is an emerging but less prevalent issue
Nonculture-based tests may enhance AFS but refinement of both target populations and clinical pathways incorporating their use is required Performance indicators including structural process and outcome measures are integral for demonstrating the value of AFS programmes
Ananda-Rajah MR Slavin MA Thursky KT
Curr Opin Infect Dis 2012 Feb25(1)107-15
De-escalation of antibiotic therapy Concept
ldquoCould be considered as a strategy to balance the need to provide adequate initial antibiotic treatment of high risk patients with the avoidance of unnecessary antibiotic utilization which promotes resistancerdquo
Inadequate empirical antibitibic therapy and ICU-Bacteremia
6229
0
50
100
I EAT NO I EAT
I nhospital
Mortality
Ibrahim et al Chest 2000 118 146-155
N= 492 Candida spp VRE meticilin resistant S aureus CNS Pseudomonas aeruginosa
IEAT= 299
plt 0001
Inadequate empirical antibitibic therapy and ICU-Bacteremia
30235
0
10
20
30
I EAT NO-I EAT Related
mortality
N= 166 CNS Acinetobacter baumannii Pseudomonas aeruginosa Candida spp
Zaragoza R et al Clin Microbiol Infect 2003 May 9(5)412-418
IEAT= 235
pgt005
APPROACH TO ANTIFUNGAL TREATMENT
Pre-emptive and Empirical Therapy ICCd
iquestPrevious azol`s use +- clinical unstable (MOF severe sepsis) +- suspected or previous infection by C krusei o C glabrata +- multiple colonization by no-C albicans spp +- ICU stay and risk factors (drug-interactions kind of patient pe transplantation peritonitis)
-Fluconazole 400-800 mg IVd If possible switching to oral therapy (400 mgd)
We must considered AF rapid broad spectrum and PKPD
optimized
Yes NO
-Anidulafungin 200 mg24 (d1)+100 mg d -Caspofungin 70 mg24 h (d1) + 50 mg d -Micafungina 150 mg24 hs - Amphotericin B-Lipidic Complex 3-5 mgkgd - Amphotericin B- Lipossomal 3 mgkgd - Voriconazol e iv 6 mgkg12h (d1) + 4 mgkg12h
EVEN POSSIBLE DE-ESCALATION
Zaragoza R Pemaacuten J J Invasive Fungal Infect 2007150-58
Antifungal de-escalation strategy
Initially a broad spectrum antitungal treatment is administrated until the agent of infection was identified
Echinocandins AMPHOTERICINS
Microbiogical data
Patientacutes physician criteria
Maintenance of broad spectrum combination
DT Switching to a narrow spectrum
Guery ICM2008
Candidemia pacientes no-neutropenicos De-escalation IDSA 2008
De-escalation even it`s possible (I-A)
Targeted Treatment of Candidaemia
Echinocandins
Compound SoR QoE Reference Comment
Anidulafungin
200100
A I Reboli NEJM 2007 bull Broad spectrum
bull Resistance rare
bull Fungicidal
bull Local epidemiology
bull C parapsilosis C krusei
bull Safety profile
bull Less drug-drug interactions
than caspofungin
Caspofungin
7050
A I Mora-Duarte NEJM 2002
Pappas CID 2007
bull Largely as above
Micafungin
100
A I Kuse Lancet 2007
Pappas CID 2007
bull Largely as above
bull Consider EMA warning label
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
De-escalation of antibiotic therapy Concept
ldquoCould be considered as a strategy to balance the need to provide adequate initial antibiotic treatment of high risk patients with the avoidance of unnecessary antibiotic utilization which promotes resistancerdquo
Inadequate empirical antibitibic therapy and ICU-Bacteremia
6229
0
50
100
I EAT NO I EAT
I nhospital
Mortality
Ibrahim et al Chest 2000 118 146-155
N= 492 Candida spp VRE meticilin resistant S aureus CNS Pseudomonas aeruginosa
IEAT= 299
plt 0001
Inadequate empirical antibitibic therapy and ICU-Bacteremia
30235
0
10
20
30
I EAT NO-I EAT Related
mortality
N= 166 CNS Acinetobacter baumannii Pseudomonas aeruginosa Candida spp
Zaragoza R et al Clin Microbiol Infect 2003 May 9(5)412-418
IEAT= 235
pgt005
APPROACH TO ANTIFUNGAL TREATMENT
Pre-emptive and Empirical Therapy ICCd
iquestPrevious azol`s use +- clinical unstable (MOF severe sepsis) +- suspected or previous infection by C krusei o C glabrata +- multiple colonization by no-C albicans spp +- ICU stay and risk factors (drug-interactions kind of patient pe transplantation peritonitis)
-Fluconazole 400-800 mg IVd If possible switching to oral therapy (400 mgd)
We must considered AF rapid broad spectrum and PKPD
optimized
Yes NO
-Anidulafungin 200 mg24 (d1)+100 mg d -Caspofungin 70 mg24 h (d1) + 50 mg d -Micafungina 150 mg24 hs - Amphotericin B-Lipidic Complex 3-5 mgkgd - Amphotericin B- Lipossomal 3 mgkgd - Voriconazol e iv 6 mgkg12h (d1) + 4 mgkg12h
EVEN POSSIBLE DE-ESCALATION
Zaragoza R Pemaacuten J J Invasive Fungal Infect 2007150-58
Antifungal de-escalation strategy
Initially a broad spectrum antitungal treatment is administrated until the agent of infection was identified
Echinocandins AMPHOTERICINS
Microbiogical data
Patientacutes physician criteria
Maintenance of broad spectrum combination
DT Switching to a narrow spectrum
Guery ICM2008
Candidemia pacientes no-neutropenicos De-escalation IDSA 2008
De-escalation even it`s possible (I-A)
Targeted Treatment of Candidaemia
Echinocandins
Compound SoR QoE Reference Comment
Anidulafungin
200100
A I Reboli NEJM 2007 bull Broad spectrum
bull Resistance rare
bull Fungicidal
bull Local epidemiology
bull C parapsilosis C krusei
bull Safety profile
bull Less drug-drug interactions
than caspofungin
Caspofungin
7050
A I Mora-Duarte NEJM 2002
Pappas CID 2007
bull Largely as above
Micafungin
100
A I Kuse Lancet 2007
Pappas CID 2007
bull Largely as above
bull Consider EMA warning label
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
Inadequate empirical antibitibic therapy and ICU-Bacteremia
6229
0
50
100
I EAT NO I EAT
I nhospital
Mortality
Ibrahim et al Chest 2000 118 146-155
N= 492 Candida spp VRE meticilin resistant S aureus CNS Pseudomonas aeruginosa
IEAT= 299
plt 0001
Inadequate empirical antibitibic therapy and ICU-Bacteremia
30235
0
10
20
30
I EAT NO-I EAT Related
mortality
N= 166 CNS Acinetobacter baumannii Pseudomonas aeruginosa Candida spp
Zaragoza R et al Clin Microbiol Infect 2003 May 9(5)412-418
IEAT= 235
pgt005
APPROACH TO ANTIFUNGAL TREATMENT
Pre-emptive and Empirical Therapy ICCd
iquestPrevious azol`s use +- clinical unstable (MOF severe sepsis) +- suspected or previous infection by C krusei o C glabrata +- multiple colonization by no-C albicans spp +- ICU stay and risk factors (drug-interactions kind of patient pe transplantation peritonitis)
-Fluconazole 400-800 mg IVd If possible switching to oral therapy (400 mgd)
We must considered AF rapid broad spectrum and PKPD
optimized
Yes NO
-Anidulafungin 200 mg24 (d1)+100 mg d -Caspofungin 70 mg24 h (d1) + 50 mg d -Micafungina 150 mg24 hs - Amphotericin B-Lipidic Complex 3-5 mgkgd - Amphotericin B- Lipossomal 3 mgkgd - Voriconazol e iv 6 mgkg12h (d1) + 4 mgkg12h
EVEN POSSIBLE DE-ESCALATION
Zaragoza R Pemaacuten J J Invasive Fungal Infect 2007150-58
Antifungal de-escalation strategy
Initially a broad spectrum antitungal treatment is administrated until the agent of infection was identified
Echinocandins AMPHOTERICINS
Microbiogical data
Patientacutes physician criteria
Maintenance of broad spectrum combination
DT Switching to a narrow spectrum
Guery ICM2008
Candidemia pacientes no-neutropenicos De-escalation IDSA 2008
De-escalation even it`s possible (I-A)
Targeted Treatment of Candidaemia
Echinocandins
Compound SoR QoE Reference Comment
Anidulafungin
200100
A I Reboli NEJM 2007 bull Broad spectrum
bull Resistance rare
bull Fungicidal
bull Local epidemiology
bull C parapsilosis C krusei
bull Safety profile
bull Less drug-drug interactions
than caspofungin
Caspofungin
7050
A I Mora-Duarte NEJM 2002
Pappas CID 2007
bull Largely as above
Micafungin
100
A I Kuse Lancet 2007
Pappas CID 2007
bull Largely as above
bull Consider EMA warning label
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
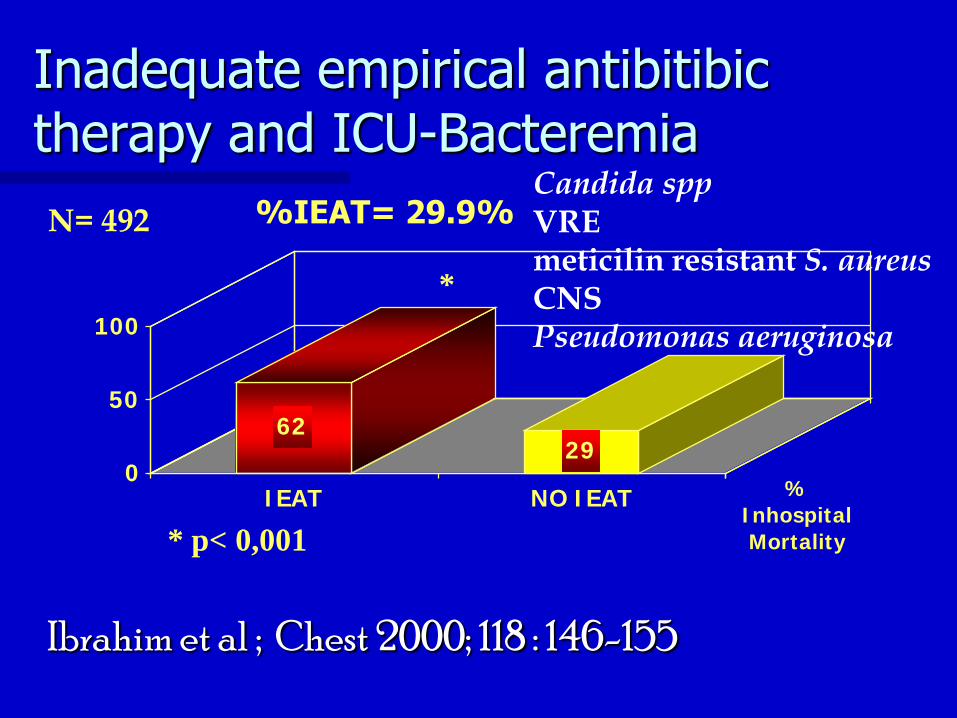
Inadequate empirical antibitibic therapy and ICU-Bacteremia
30235
0
10
20
30
I EAT NO-I EAT Related
mortality
N= 166 CNS Acinetobacter baumannii Pseudomonas aeruginosa Candida spp
Zaragoza R et al Clin Microbiol Infect 2003 May 9(5)412-418
IEAT= 235
pgt005
APPROACH TO ANTIFUNGAL TREATMENT
Pre-emptive and Empirical Therapy ICCd
iquestPrevious azol`s use +- clinical unstable (MOF severe sepsis) +- suspected or previous infection by C krusei o C glabrata +- multiple colonization by no-C albicans spp +- ICU stay and risk factors (drug-interactions kind of patient pe transplantation peritonitis)
-Fluconazole 400-800 mg IVd If possible switching to oral therapy (400 mgd)
We must considered AF rapid broad spectrum and PKPD
optimized
Yes NO
-Anidulafungin 200 mg24 (d1)+100 mg d -Caspofungin 70 mg24 h (d1) + 50 mg d -Micafungina 150 mg24 hs - Amphotericin B-Lipidic Complex 3-5 mgkgd - Amphotericin B- Lipossomal 3 mgkgd - Voriconazol e iv 6 mgkg12h (d1) + 4 mgkg12h
EVEN POSSIBLE DE-ESCALATION
Zaragoza R Pemaacuten J J Invasive Fungal Infect 2007150-58
Antifungal de-escalation strategy
Initially a broad spectrum antitungal treatment is administrated until the agent of infection was identified
Echinocandins AMPHOTERICINS
Microbiogical data
Patientacutes physician criteria
Maintenance of broad spectrum combination
DT Switching to a narrow spectrum
Guery ICM2008
Candidemia pacientes no-neutropenicos De-escalation IDSA 2008
De-escalation even it`s possible (I-A)
Targeted Treatment of Candidaemia
Echinocandins
Compound SoR QoE Reference Comment
Anidulafungin
200100
A I Reboli NEJM 2007 bull Broad spectrum
bull Resistance rare
bull Fungicidal
bull Local epidemiology
bull C parapsilosis C krusei
bull Safety profile
bull Less drug-drug interactions
than caspofungin
Caspofungin
7050
A I Mora-Duarte NEJM 2002
Pappas CID 2007
bull Largely as above
Micafungin
100
A I Kuse Lancet 2007
Pappas CID 2007
bull Largely as above
bull Consider EMA warning label
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
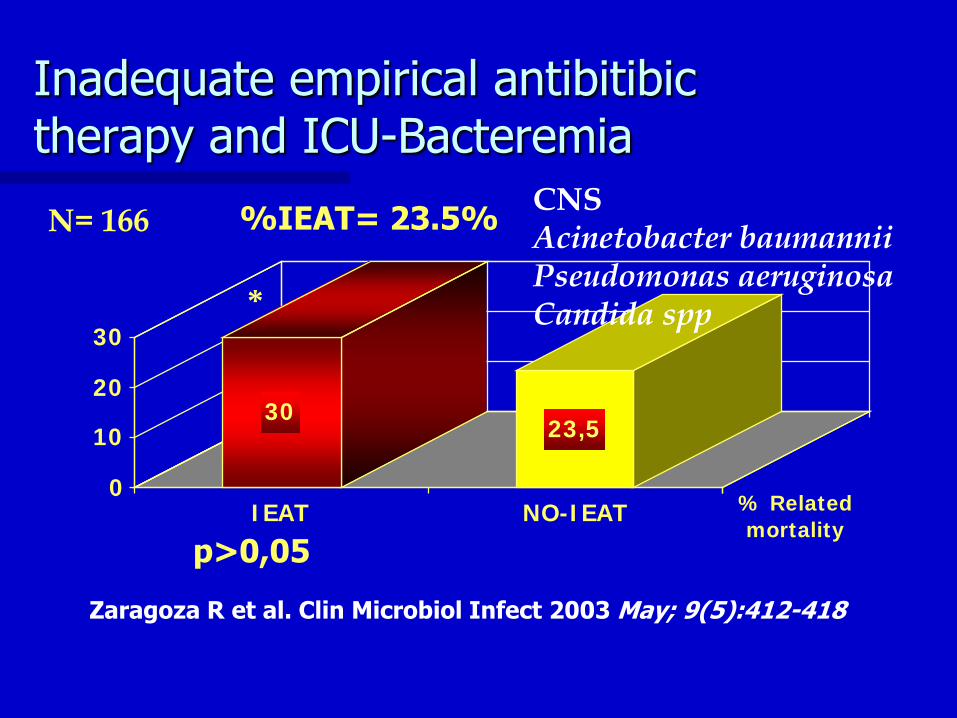
APPROACH TO ANTIFUNGAL TREATMENT
Pre-emptive and Empirical Therapy ICCd
iquestPrevious azol`s use +- clinical unstable (MOF severe sepsis) +- suspected or previous infection by C krusei o C glabrata +- multiple colonization by no-C albicans spp +- ICU stay and risk factors (drug-interactions kind of patient pe transplantation peritonitis)
-Fluconazole 400-800 mg IVd If possible switching to oral therapy (400 mgd)
We must considered AF rapid broad spectrum and PKPD
optimized
Yes NO
-Anidulafungin 200 mg24 (d1)+100 mg d -Caspofungin 70 mg24 h (d1) + 50 mg d -Micafungina 150 mg24 hs - Amphotericin B-Lipidic Complex 3-5 mgkgd - Amphotericin B- Lipossomal 3 mgkgd - Voriconazol e iv 6 mgkg12h (d1) + 4 mgkg12h
EVEN POSSIBLE DE-ESCALATION
Zaragoza R Pemaacuten J J Invasive Fungal Infect 2007150-58
Antifungal de-escalation strategy
Initially a broad spectrum antitungal treatment is administrated until the agent of infection was identified
Echinocandins AMPHOTERICINS
Microbiogical data
Patientacutes physician criteria
Maintenance of broad spectrum combination
DT Switching to a narrow spectrum
Guery ICM2008
Candidemia pacientes no-neutropenicos De-escalation IDSA 2008
De-escalation even it`s possible (I-A)
Targeted Treatment of Candidaemia
Echinocandins
Compound SoR QoE Reference Comment
Anidulafungin
200100
A I Reboli NEJM 2007 bull Broad spectrum
bull Resistance rare
bull Fungicidal
bull Local epidemiology
bull C parapsilosis C krusei
bull Safety profile
bull Less drug-drug interactions
than caspofungin
Caspofungin
7050
A I Mora-Duarte NEJM 2002
Pappas CID 2007
bull Largely as above
Micafungin
100
A I Kuse Lancet 2007
Pappas CID 2007
bull Largely as above
bull Consider EMA warning label
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
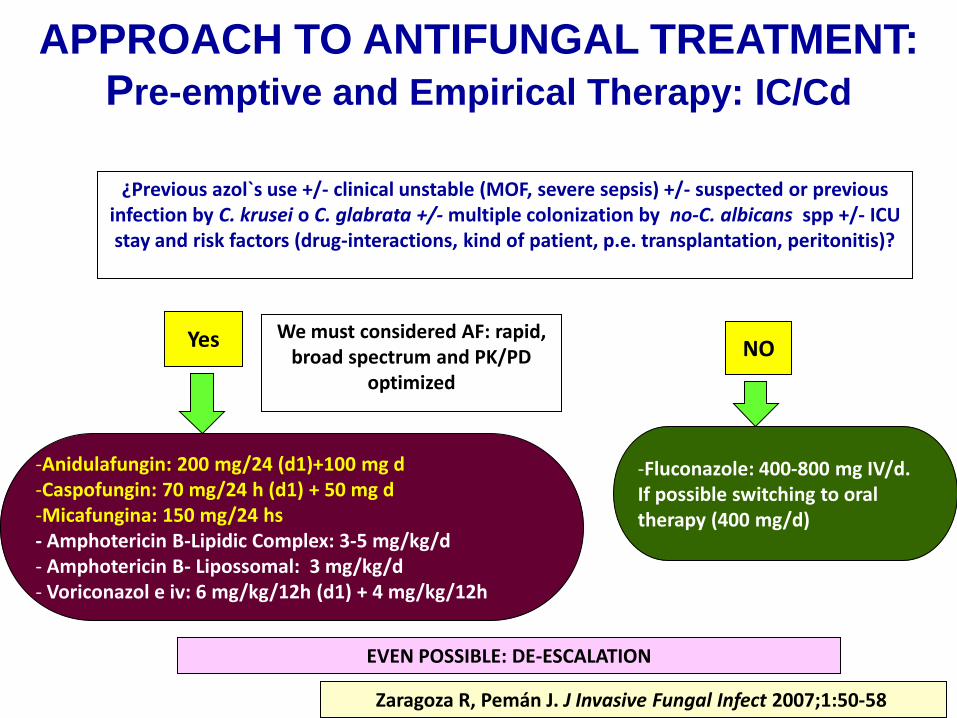
Antifungal de-escalation strategy
Initially a broad spectrum antitungal treatment is administrated until the agent of infection was identified
Echinocandins AMPHOTERICINS
Microbiogical data
Patientacutes physician criteria
Maintenance of broad spectrum combination
DT Switching to a narrow spectrum
Guery ICM2008
Candidemia pacientes no-neutropenicos De-escalation IDSA 2008
De-escalation even it`s possible (I-A)
Targeted Treatment of Candidaemia
Echinocandins
Compound SoR QoE Reference Comment
Anidulafungin
200100
A I Reboli NEJM 2007 bull Broad spectrum
bull Resistance rare
bull Fungicidal
bull Local epidemiology
bull C parapsilosis C krusei
bull Safety profile
bull Less drug-drug interactions
than caspofungin
Caspofungin
7050
A I Mora-Duarte NEJM 2002
Pappas CID 2007
bull Largely as above
Micafungin
100
A I Kuse Lancet 2007
Pappas CID 2007
bull Largely as above
bull Consider EMA warning label
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
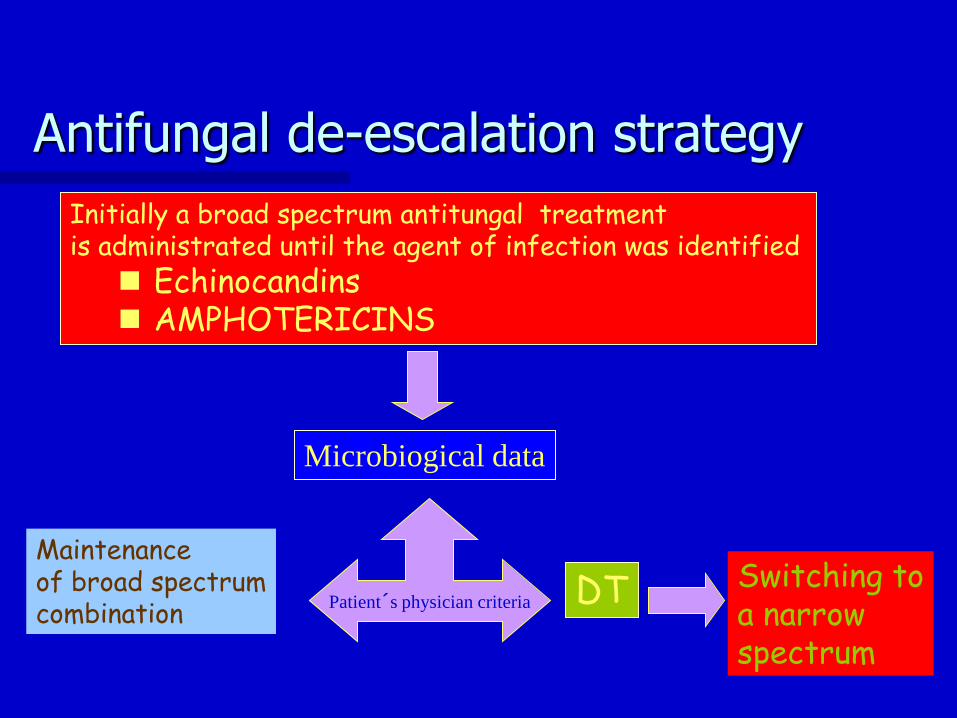
Guery ICM2008
Candidemia pacientes no-neutropenicos De-escalation IDSA 2008
De-escalation even it`s possible (I-A)
Targeted Treatment of Candidaemia
Echinocandins
Compound SoR QoE Reference Comment
Anidulafungin
200100
A I Reboli NEJM 2007 bull Broad spectrum
bull Resistance rare
bull Fungicidal
bull Local epidemiology
bull C parapsilosis C krusei
bull Safety profile
bull Less drug-drug interactions
than caspofungin
Caspofungin
7050
A I Mora-Duarte NEJM 2002
Pappas CID 2007
bull Largely as above
Micafungin
100
A I Kuse Lancet 2007
Pappas CID 2007
bull Largely as above
bull Consider EMA warning label
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
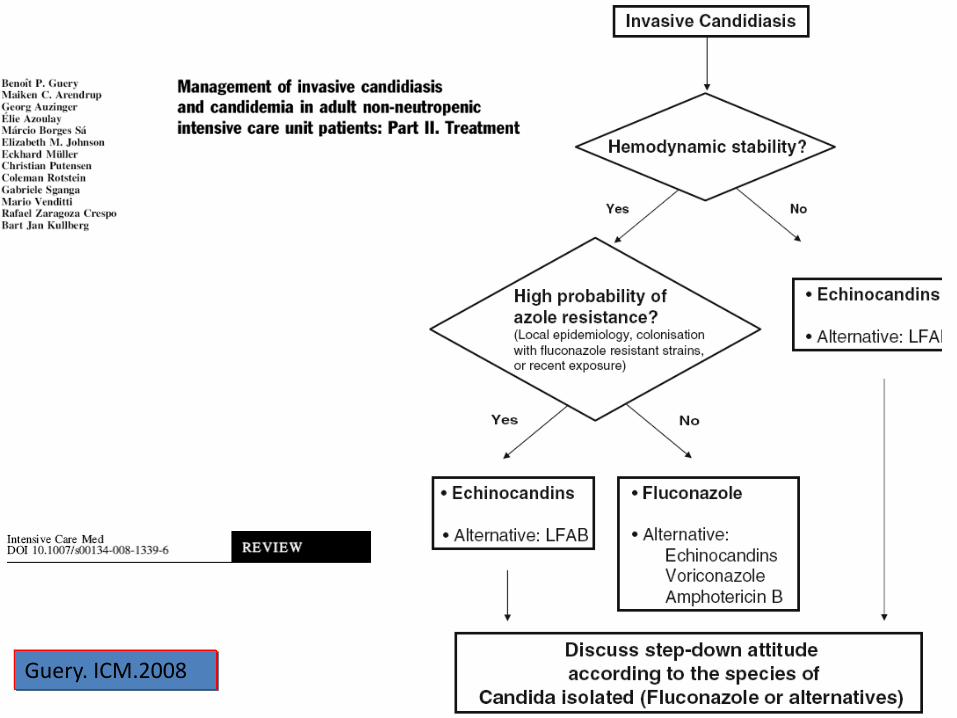
Candidemia pacientes no-neutropenicos De-escalation IDSA 2008
De-escalation even it`s possible (I-A)
Targeted Treatment of Candidaemia
Echinocandins
Compound SoR QoE Reference Comment
Anidulafungin
200100
A I Reboli NEJM 2007 bull Broad spectrum
bull Resistance rare
bull Fungicidal
bull Local epidemiology
bull C parapsilosis C krusei
bull Safety profile
bull Less drug-drug interactions
than caspofungin
Caspofungin
7050
A I Mora-Duarte NEJM 2002
Pappas CID 2007
bull Largely as above
Micafungin
100
A I Kuse Lancet 2007
Pappas CID 2007
bull Largely as above
bull Consider EMA warning label
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
Targeted Treatment of Candidaemia
Echinocandins
Compound SoR QoE Reference Comment
Anidulafungin
200100
A I Reboli NEJM 2007 bull Broad spectrum
bull Resistance rare
bull Fungicidal
bull Local epidemiology
bull C parapsilosis C krusei
bull Safety profile
bull Less drug-drug interactions
than caspofungin
Caspofungin
7050
A I Mora-Duarte NEJM 2002
Pappas CID 2007
bull Largely as above
Micafungin
100
A I Kuse Lancet 2007
Pappas CID 2007
bull Largely as above
bull Consider EMA warning label
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
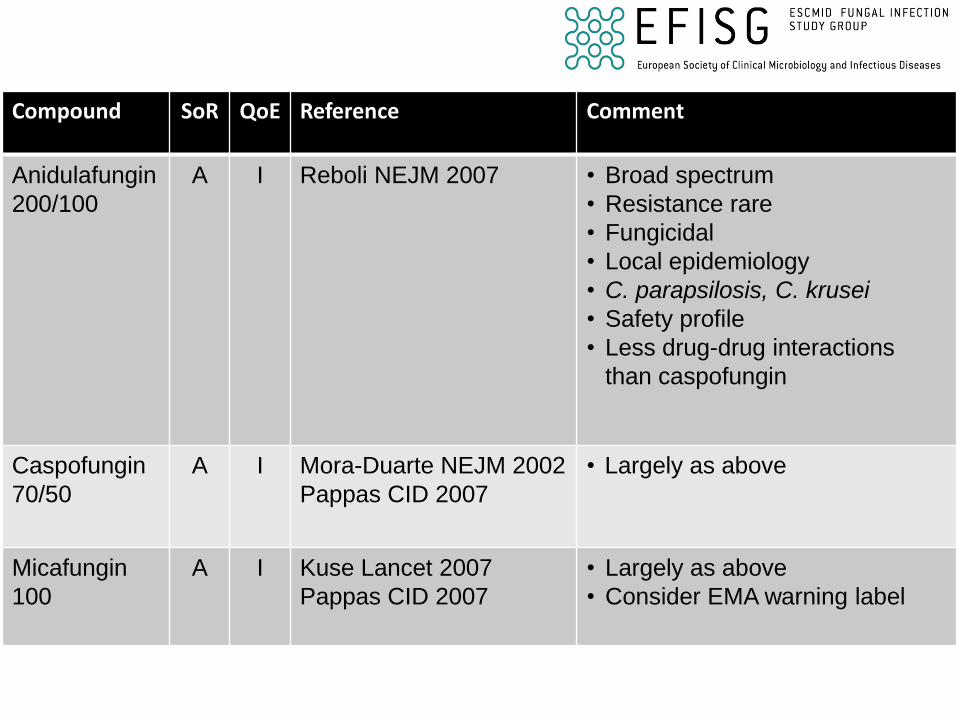
Search for
Limits PreviewIndex History Clipboard Details
1 ORIGINAL
ARTICLE found
DE ESCALATION THERAPY AND CANDIDIASIS
0Pb8X13qPubMedpubmedGoSearch4DocSum200
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
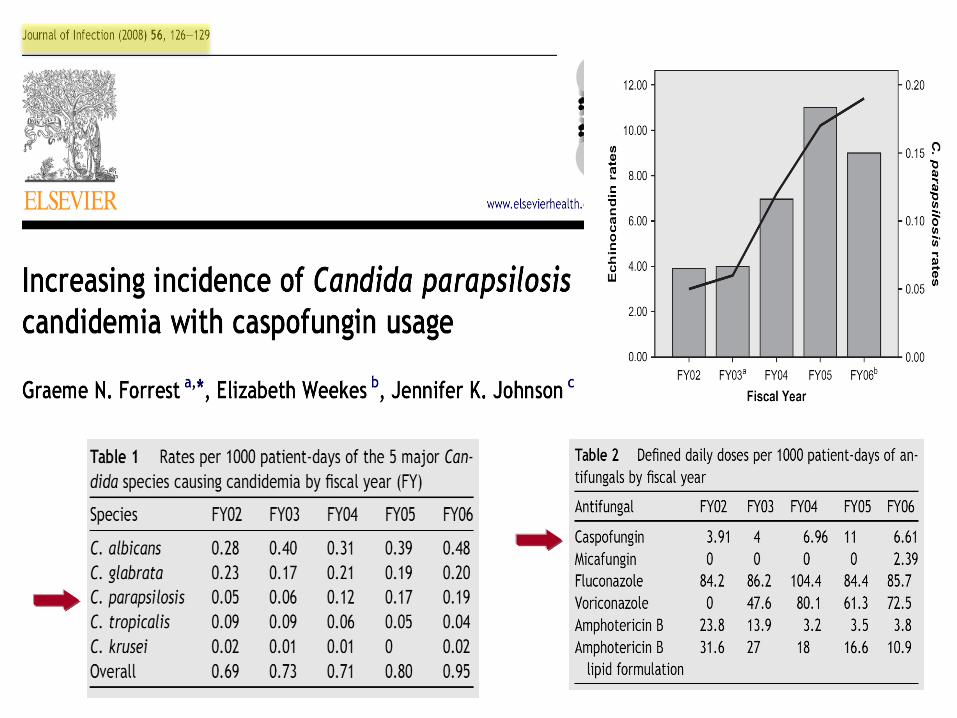
DESESCALADA ARTIacuteCULO
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
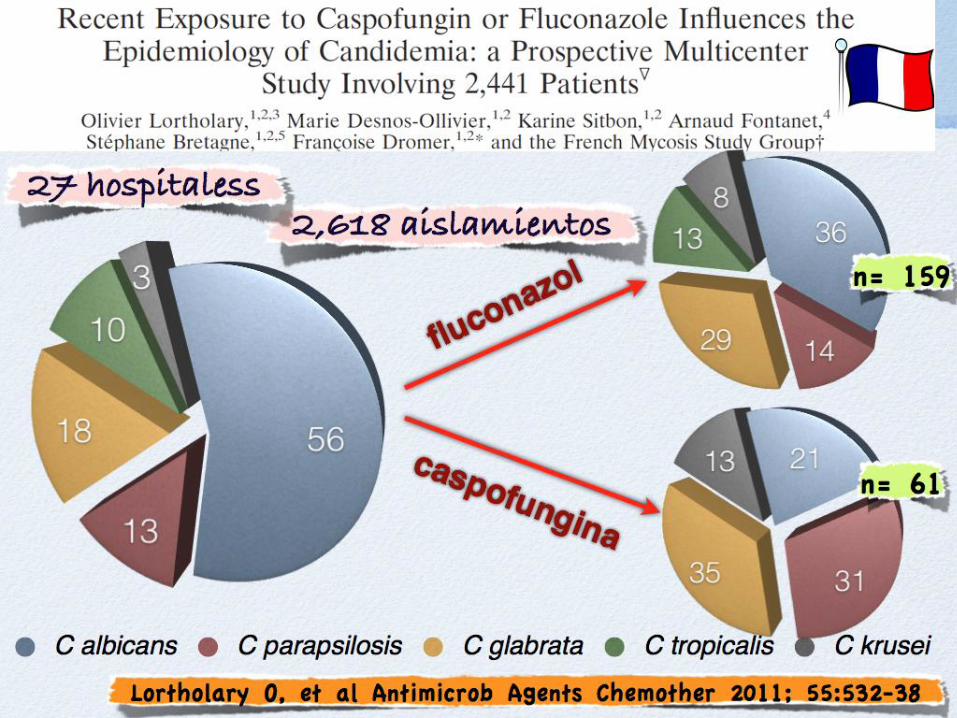
What did happen in tle last trials
WAY OF DE-ESCALATION
ICE STUDY Patients could be switched
to oral voriconazole or fluconazole at the discretion of the investigator after a minimum of 10 daysrsquo anidulafungin treatment if they had 2 subsequent negative blood cultures and resolution of CIC signs and symptoms
REBOLI STUDY All patients could
receive oralfluconazole (400 mg daily) at the investigatorsrsquodiscretion after at least 10 days of intravenoustherapy if the patients were able to tolerate oralmedication if they had been afebrile for at least24 hours if the most recent blood culture wasnegative for candida species and if there wasclinical improvement
IMPLEMENTATION
ICE STUDY53 patients were switched to
an oral azole 41 to fluconazole (mean duration 117 days range 3-44) and 12 to voriconazole (mean duration 112 days range 5-20)
REBOLI STUDY 33 patients FROM
EACH GROUP were switched to an oral FLUCONAZOLE
34
26-28
Reboli A et al NEJM 2007
Ruhnke M et al CMI in press
Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk

Is early treatment needed for Invasive Candidiasis in critically ill patients
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
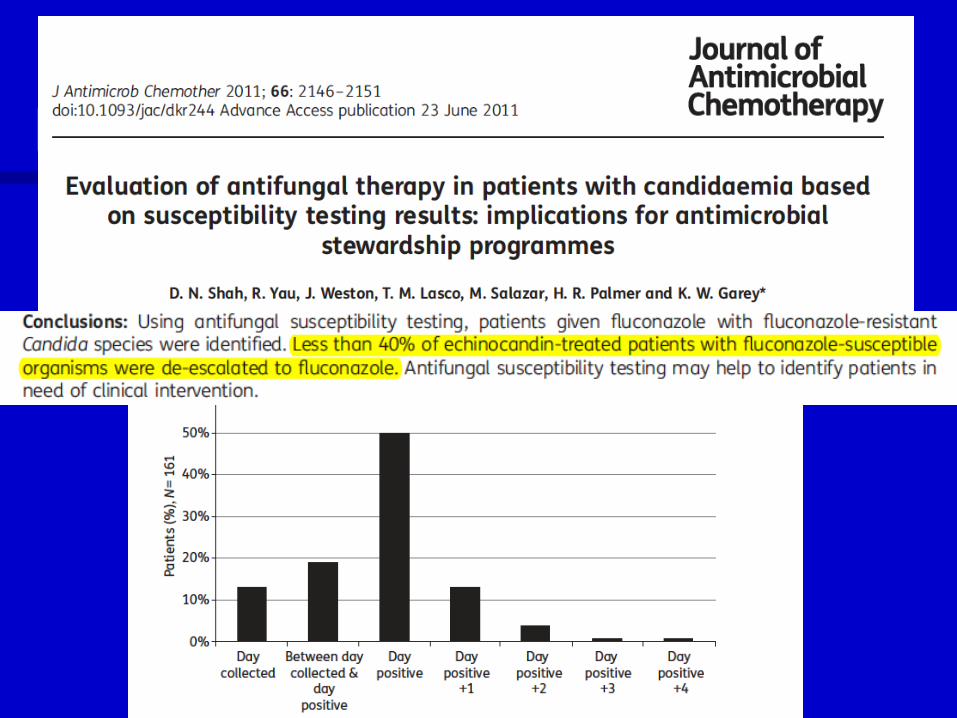
Yeshellipof coursehelliphellip
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
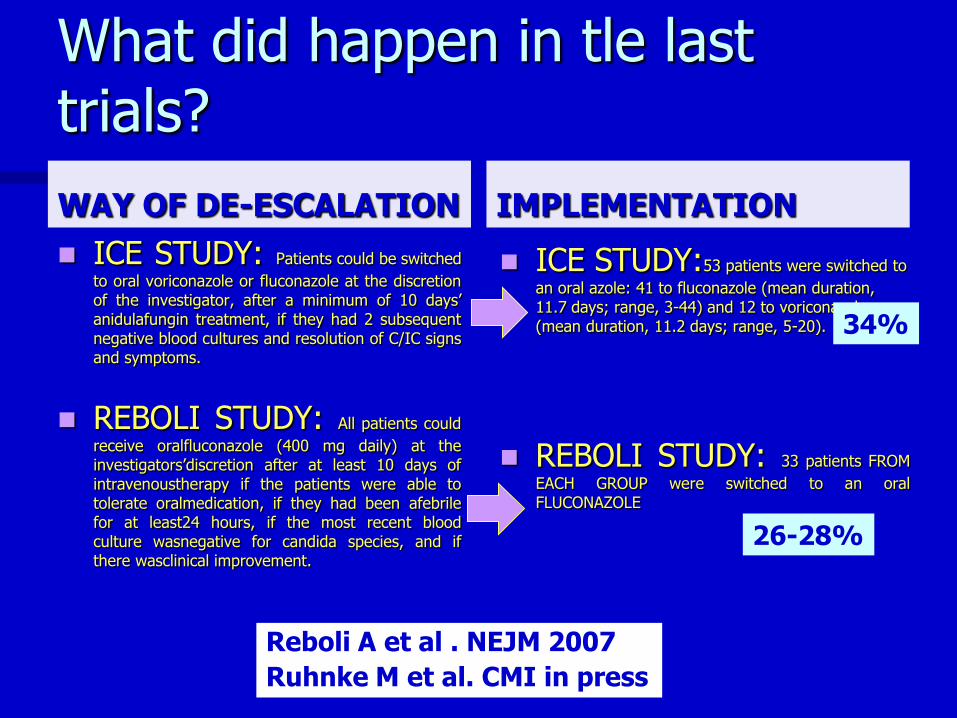
Difficulties in Establishing a
Diagnosis for Candidemia
No disease CulturesAntigen Signs and
symptoms
Cultures
histopathology Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality
40
Treatment Morbidity
Mortality
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
Delaying the Empiric Treatment of Candidemia An Independent Risk Factor for Hospital Mortality
lt12 lt 24 gt24 gt48
0
5
10
15
20
25
30
35
H
ospital M
ort
alit
y
Delay in Start of Antifungal
Therapy (days)
Variable OR 95 CI P
APACHE II 124 (118-131) lt0001
Prior antibiotics 405 (214-765) 0028
Delay in antifungal 209 (153-284) 0018
therapy
Multivariate analysis of independent risk
factors for hospital mortality
Morrell et al Antimicrob Agent Chemother 2005493640
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
Garey KW Clin Infect Dis 2006 4325-31
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
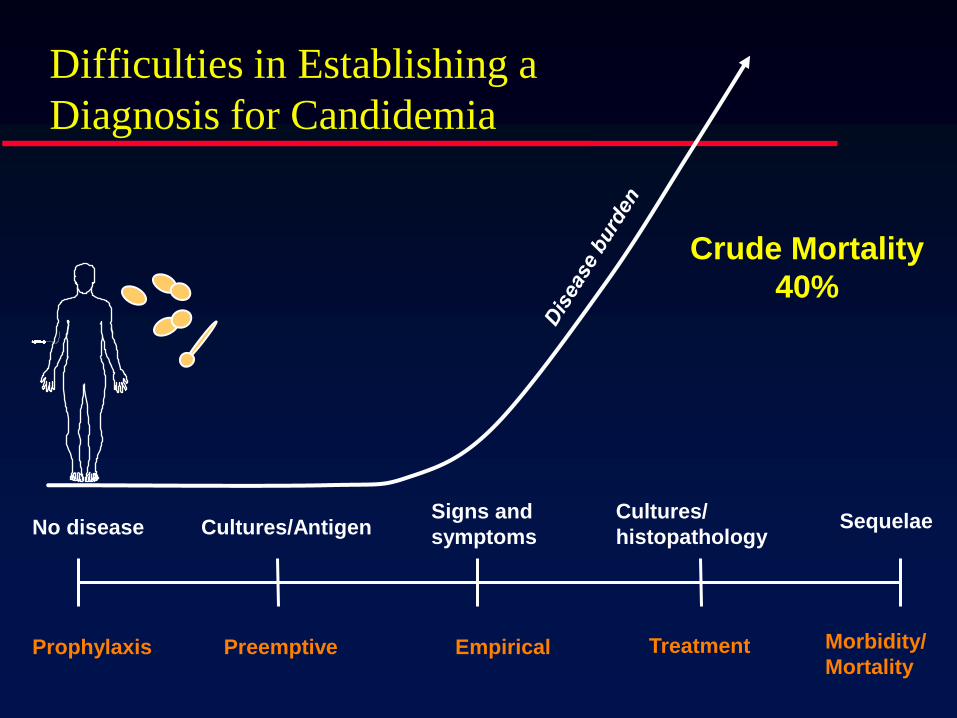
The Effect of Time to Antifungal Therapy on Mortality in Candidemia associated Septic Shock
Patel GP et al Am J Therapeutics 2009
Septic shock developed in 23 (31 of 135) patients with CBSI
In-hospital mortality was 68
Appropriate antifungal therapy was
administered to 24 patients 15 (63)
of these patients died
Patients who received appropriate
antifungal therapy within 15 hours of
collecting the first positive Candida
blood culture had improved survival
(P = 003)
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
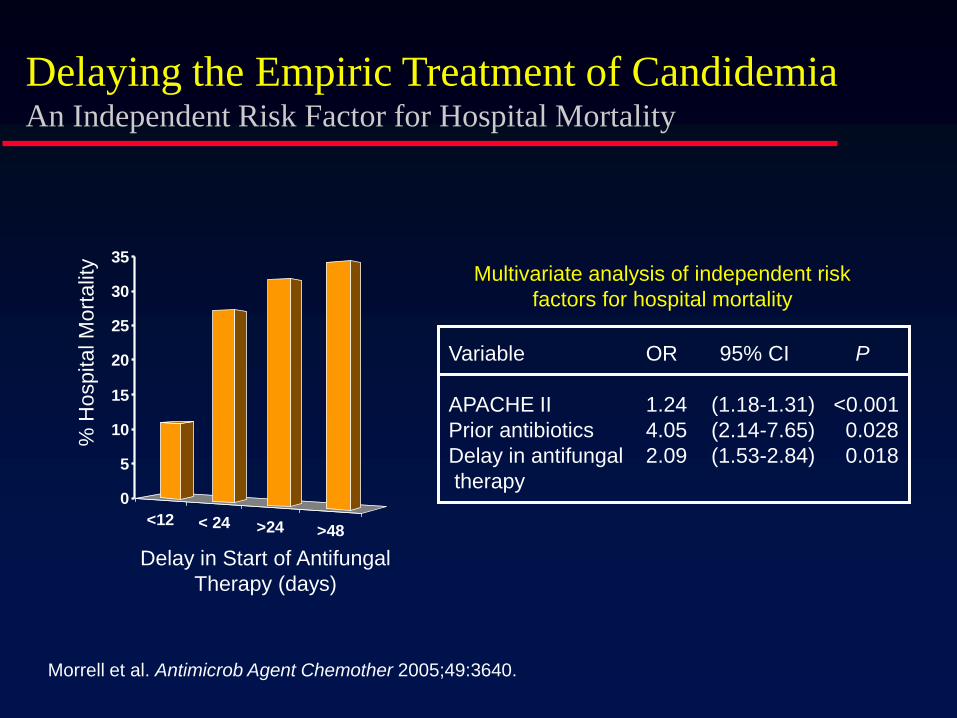
Caspo velocidad
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
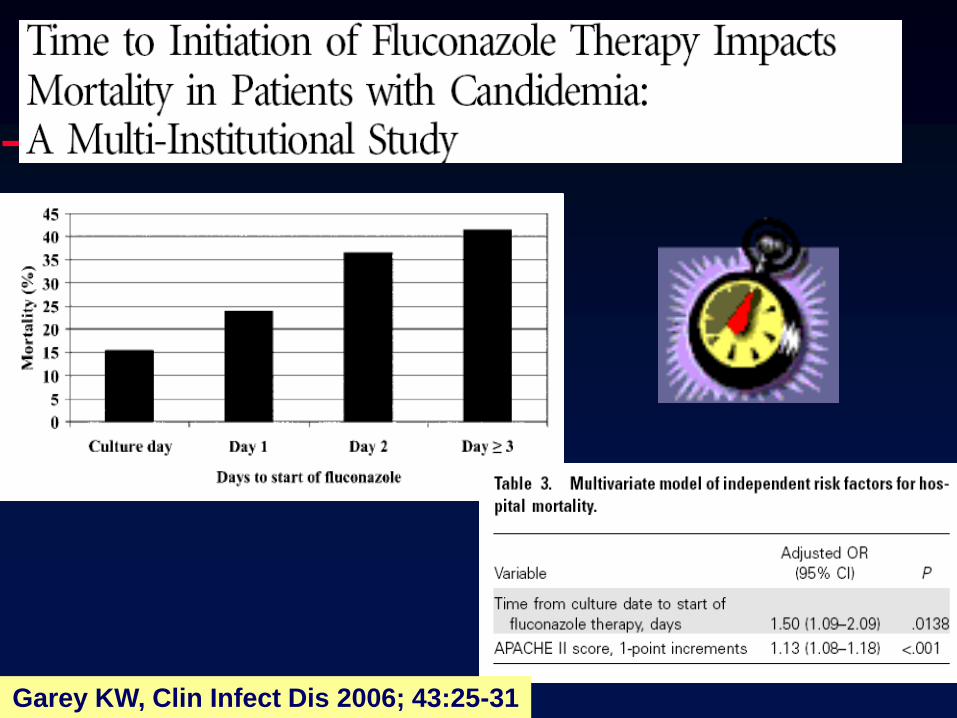
Relationship between ldquoCandida scorerdquo and risk for developing IC in surgical patients
C Leon et al Crit Care Med 2009 371624 ndash1633
0
5
10
15
20
25
30
35
CSlt3 CSgt3 CS=3
Abdominal surgery
No abdominalsurgery
P lt005
IC in surgical patients according CS
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
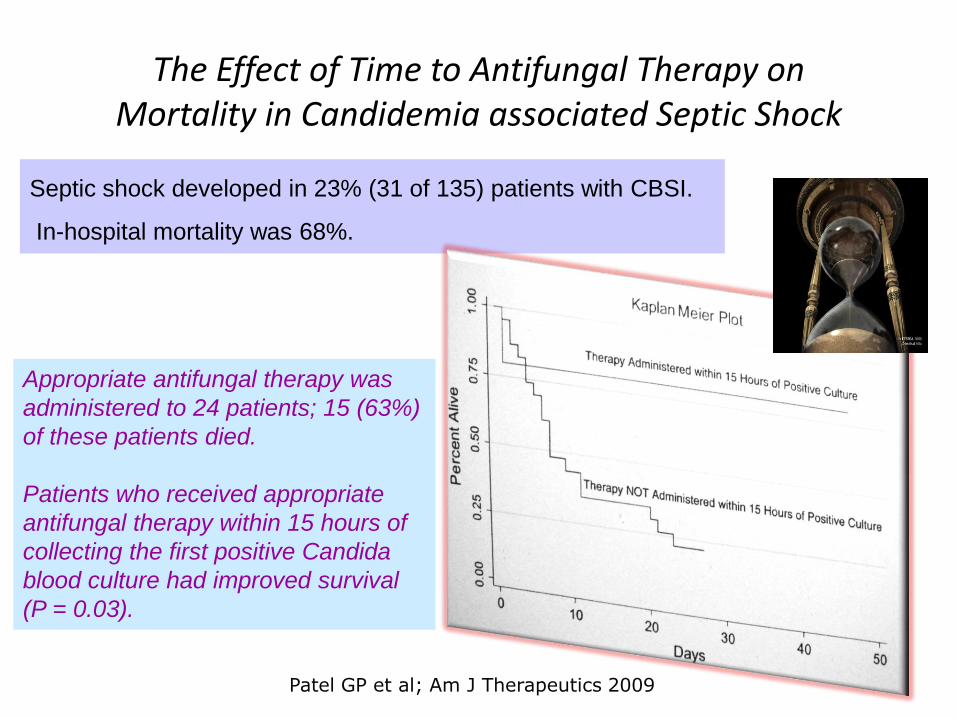
NCMT NCMT
Non-culture microbiological tools [(13)-
b-D-glucan Candida albicans germ tube
antibodies or PCR
Mycoses 2010
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
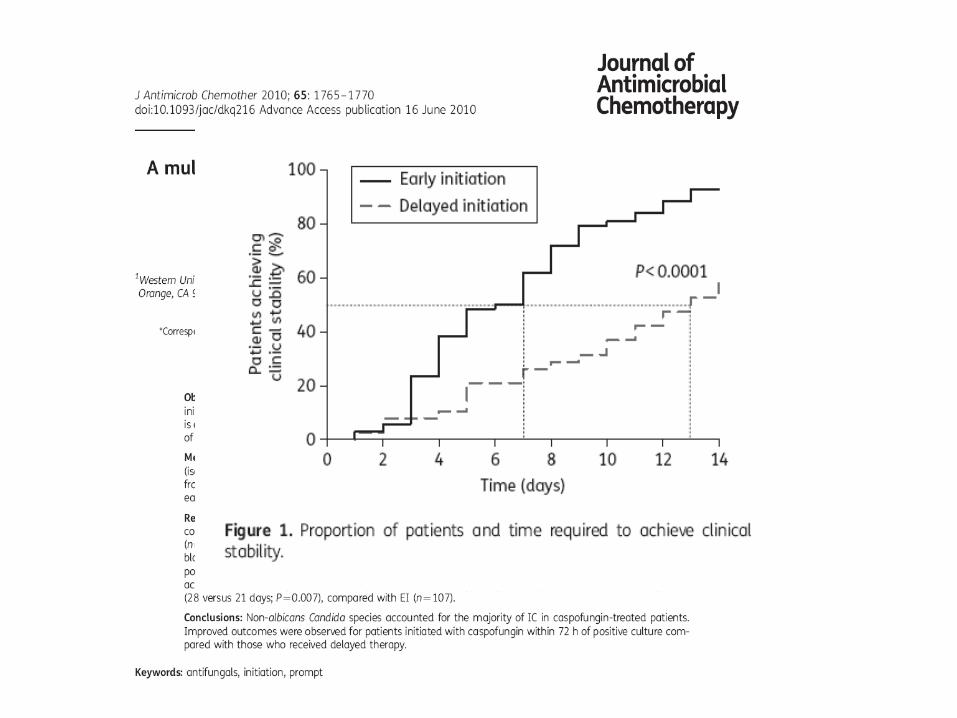
Fluconazole To be or not to be
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
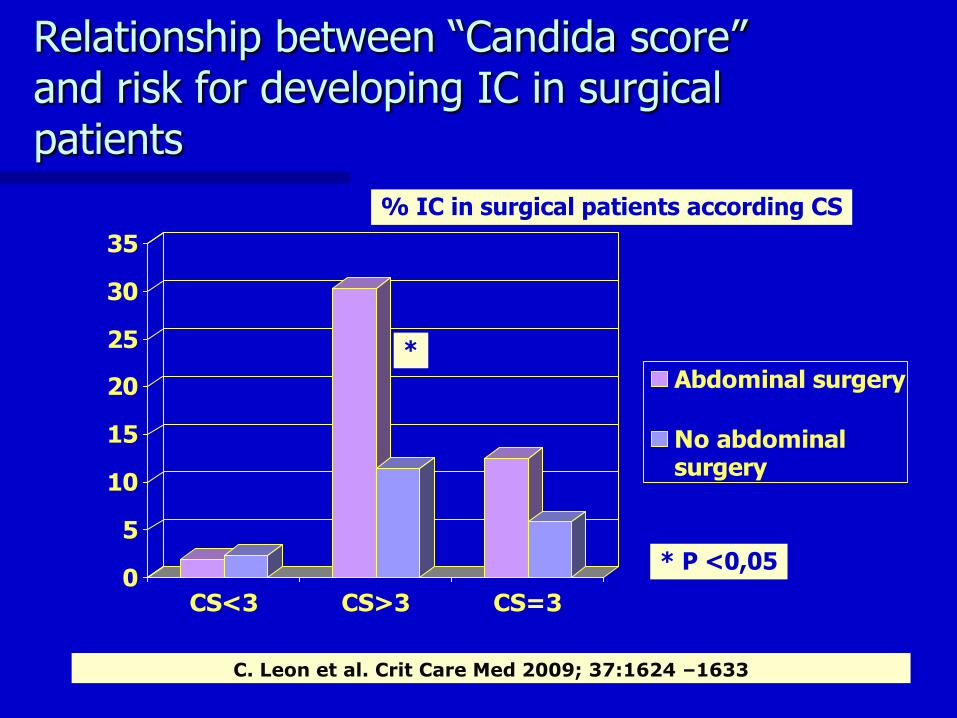
Jacobs et al CCM 312003
71 septic shock patients (Pneumonia=37 y Intrabadominal=34) Randomized (32 pts) 200 mg fluconazole iv vs (39 pts) placebo
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
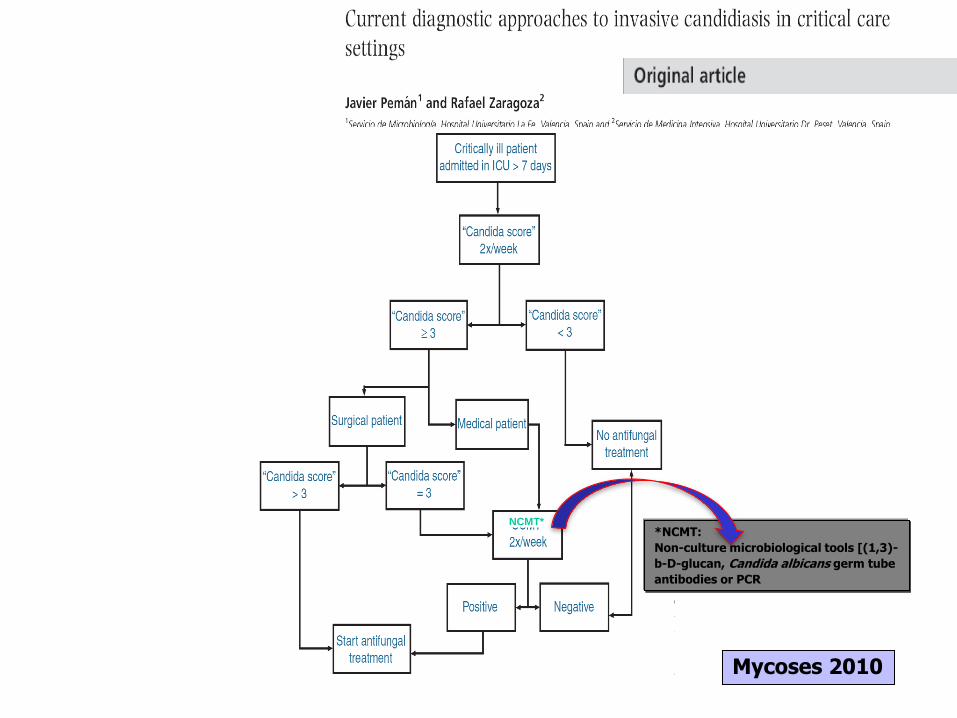
Epidemiological trends in nosocomial
candidemia in intensive care
Bassetti M et al BMC Infectious Diseases 2006680
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
Candidemias in ICU
HUDP 1996-2007
5
95
Candidemias Bacteriemias
48
23
10
19
Candida albicans Candida glabrata Candida parapsilopsis Otras
N =397 N = 31
Mortality in C no albicans episodes
gt Calbicans (125 vs 466 p= 003)
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
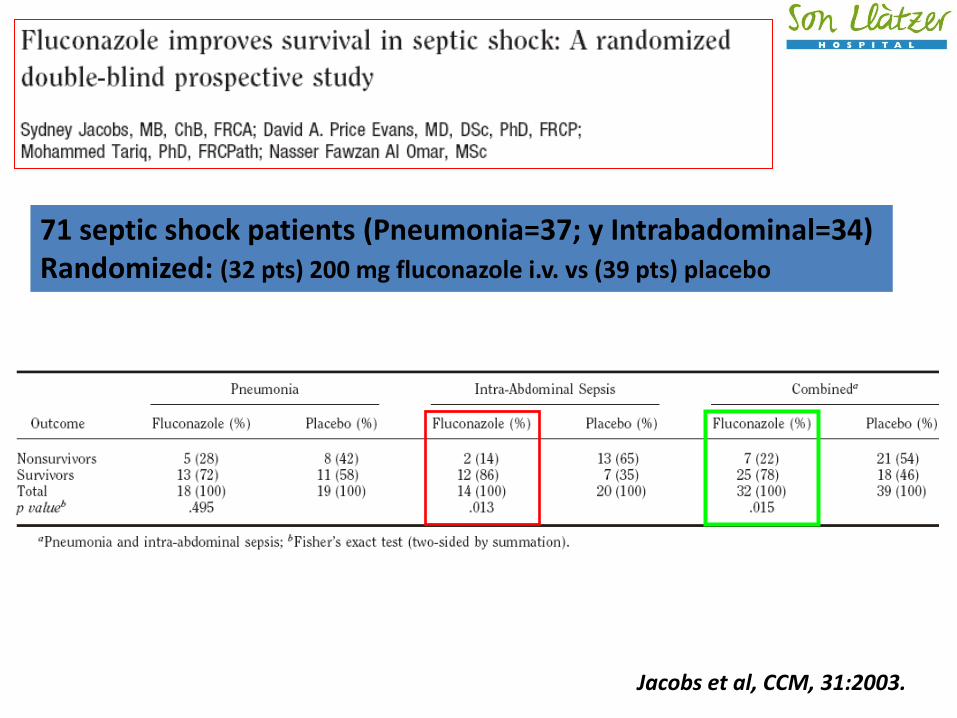
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
57
8
8
17 5
5
Candida albicans Candida glabrata Candida parapsilopsis
Candida krusei Ctropicalis Otras
N =271
Leroy O et al Crit Care Med 2009
Reduced susceptibility to fluconazole 171
Desescalated 371
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
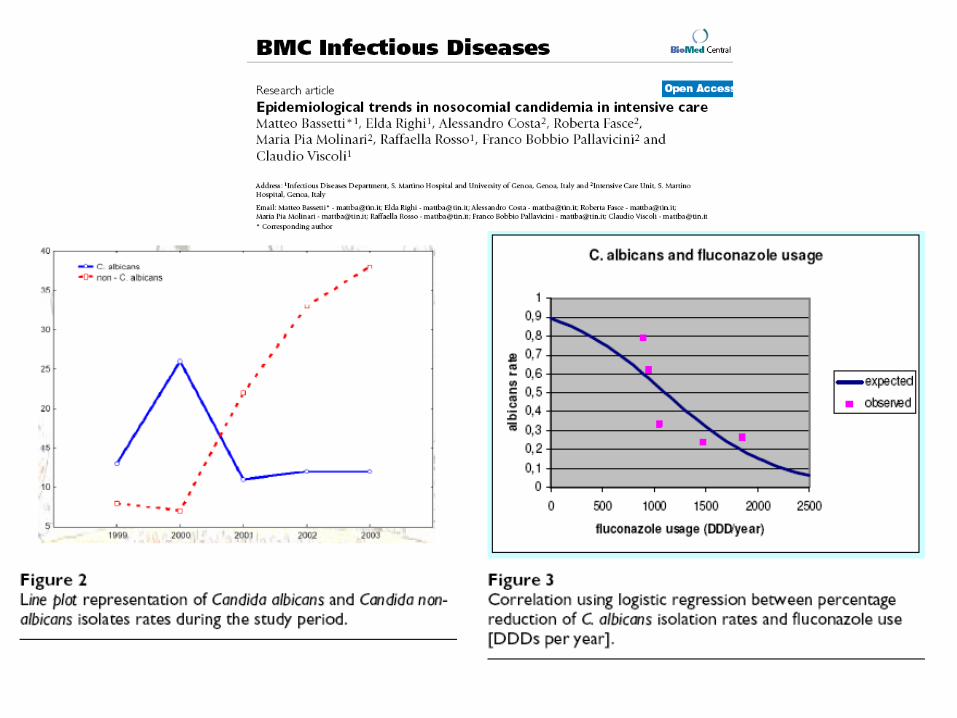
Epidemiology management and risk factors for death of invasive Candida infections in critical care A multicenter prospective observational study in France (2005ndash2006)
Leroy O et al Crit Care Med 2009
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
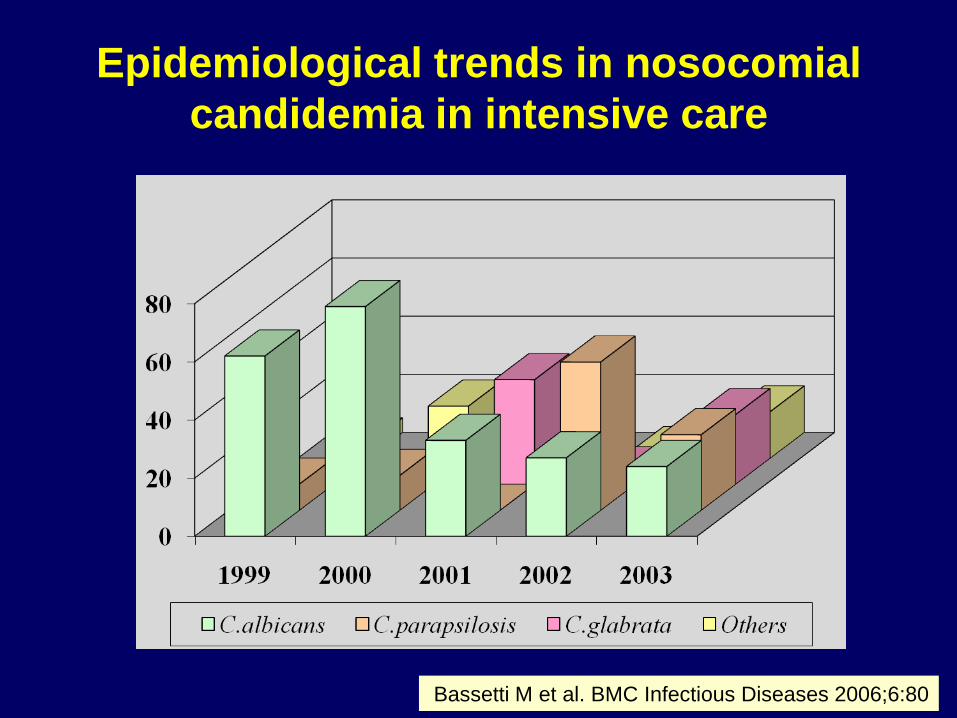
CANDIPOP Study ( 752 episodes)
12 months of candidemias in Spain (2010-2011)
Overall rate of fluconazole resistance (MICgt4 μgml) was 146
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
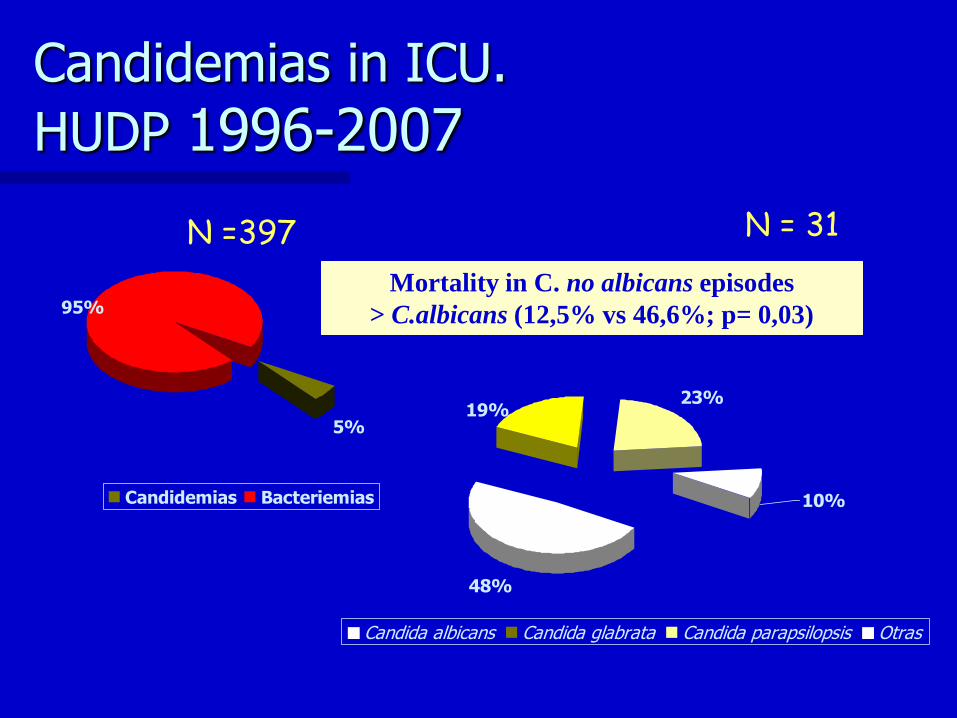
Risk factors for fluconazole-resistant
Candida glabrata bloodstream infections
76 C glabrata R fluconazole
68 C glabrata S fluconazole
512 controls
Lee I et al Arch Intern Med 2009 Feb 23169(4)379-83
Fluco R OR (95IC ) Previos use of fluconazol 23 (13-42)
Previos use of linezolid 46 ( 22-93)
Fluco S OR (95IC) Previous use of cefepime 22 (12-39)
Previous use of metronidazol
2 ( 11-35)
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
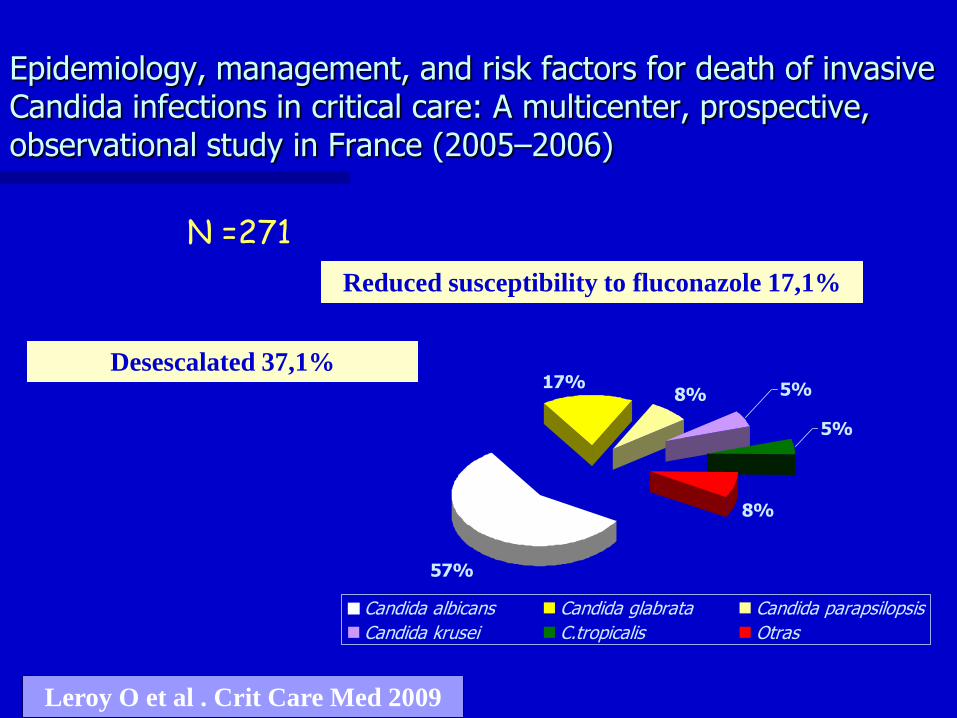
Risk Factors for Fluconazole-Resistant Candidemia
bull Prospective study including adult patients with candidemia (226 episodios)
ndash Non-albicans 53
ndash Potentially fluconazole resistant 18
bull Isolates microbiologically confirmed fluconazole resistance 13
J Garnacho et al Antimicrob Agents Chemother 2010
Previous fluconazole exposure is an independent risk factor for candidemia caused by microbiologically
confirmed fluconazole resistant species but not for bloodstream infection caused by non-albicans Candida
spp or by potentially fluconazole-resistant Candida spp (C glabrata and C krusei) Our findings may be of
value for selecting empirical antifungal therapy
INDEPENDENT PREDICTORS OR
Neutropenia 494
Chronic renal disease 482
Previous Fluconazole exposure 509
C glabrata (14) C krusei (14)
C tropicalis (2)
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
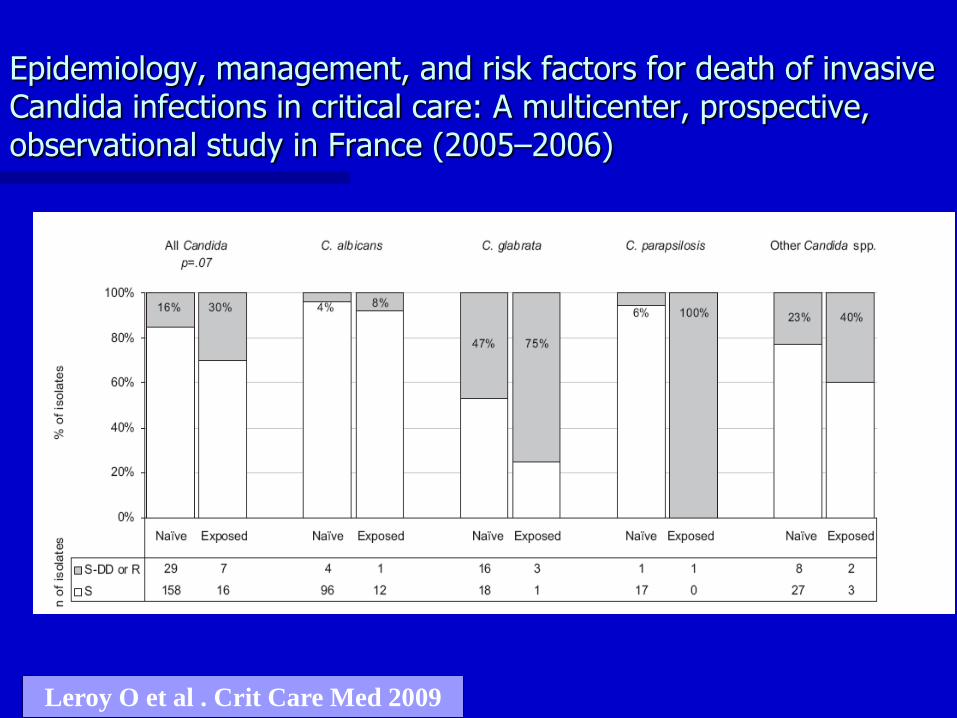
Baddley
p=0009
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
Global mortality 28 (n=84)
0
5
10
15
20
25
R Fluconazole
Alive
Dead
p = 002
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
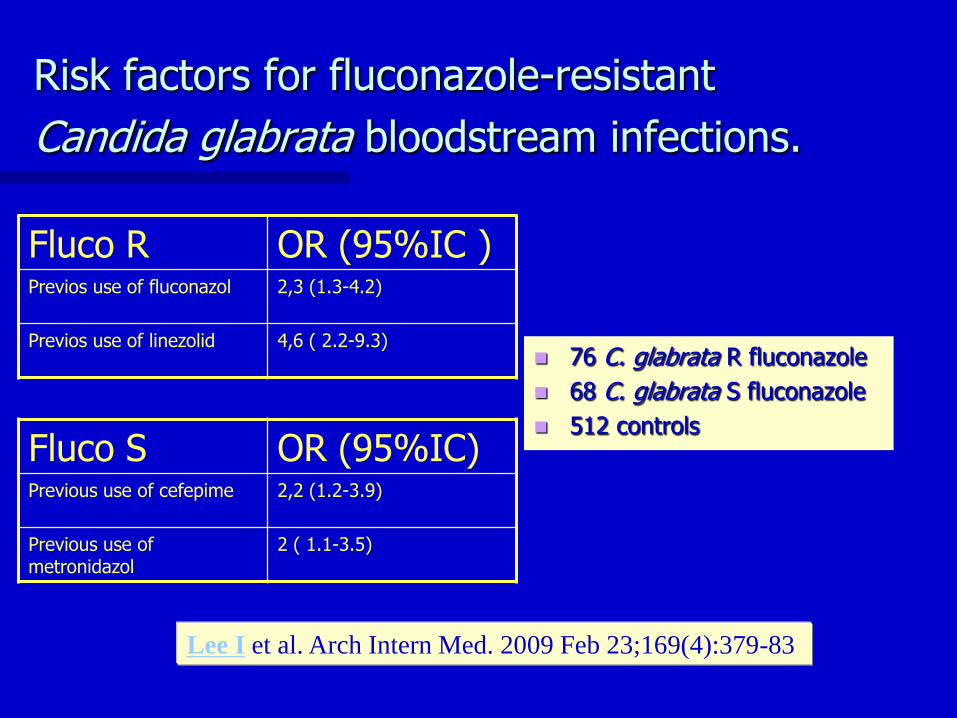
Association of Fluconazole AUCMIC and DoseMIC Ratios
with Mortality in Non-neutropenic Patients with
Candidemia
0
5
10
15
Survivors Non
Survivors
Dose MI C
p = 003
Pai M et al Antimicrob Agents Chemother 2007 51 35
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
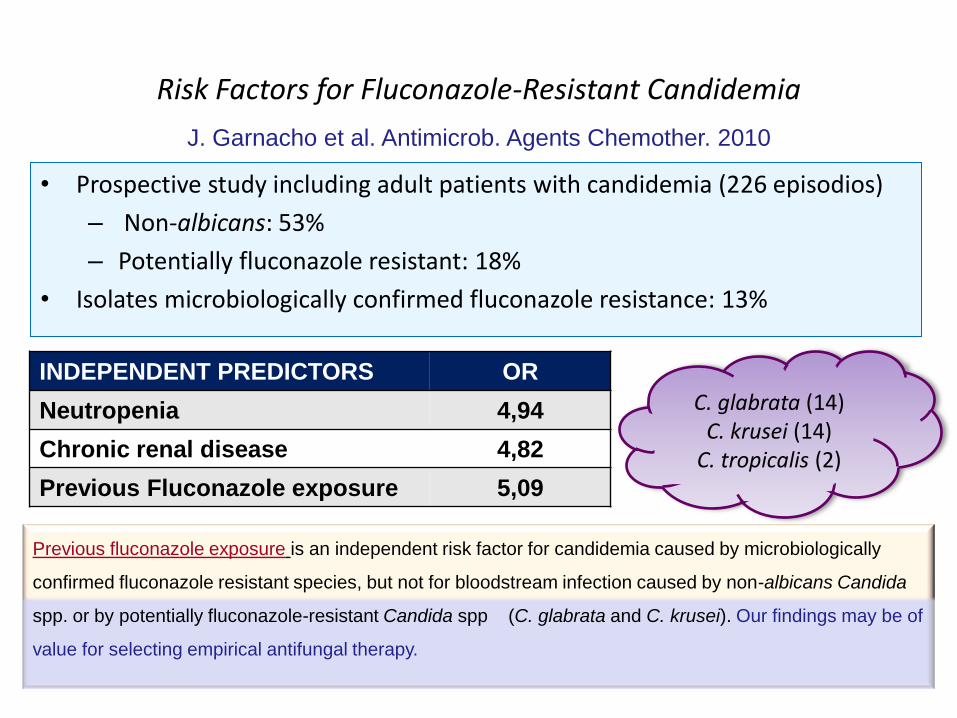
A new schemehellip Invasive Candidiasis in ICU
The case for antifungal stewardship
bull httpwwwdisfrutalogratiscomcochesoporto2jpg
bull Introduction and definition
How to do it
bull Is de-escalation a real practise
bull Is an early broad spectrum
antifungal treatment needed
bull Do we need it Fluconazole
bull Which situations
bull NEVER
bull SOMETIMES
bull ALWAYS
bull When can we step down
ndash If case of proven IC
ndash If IC are not proven
bull Take home messages
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
NEVER USE DE-ESCALATION STRATEGY NEVER STEP DOWN TO FLUCONAZOLEhellipif
CRRT
AVOID INTERACTIONS specially with
inmunossupresive agents
Hepatic failure
C glabrata amp C krusei ETIOLOGY
Personal opinion
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
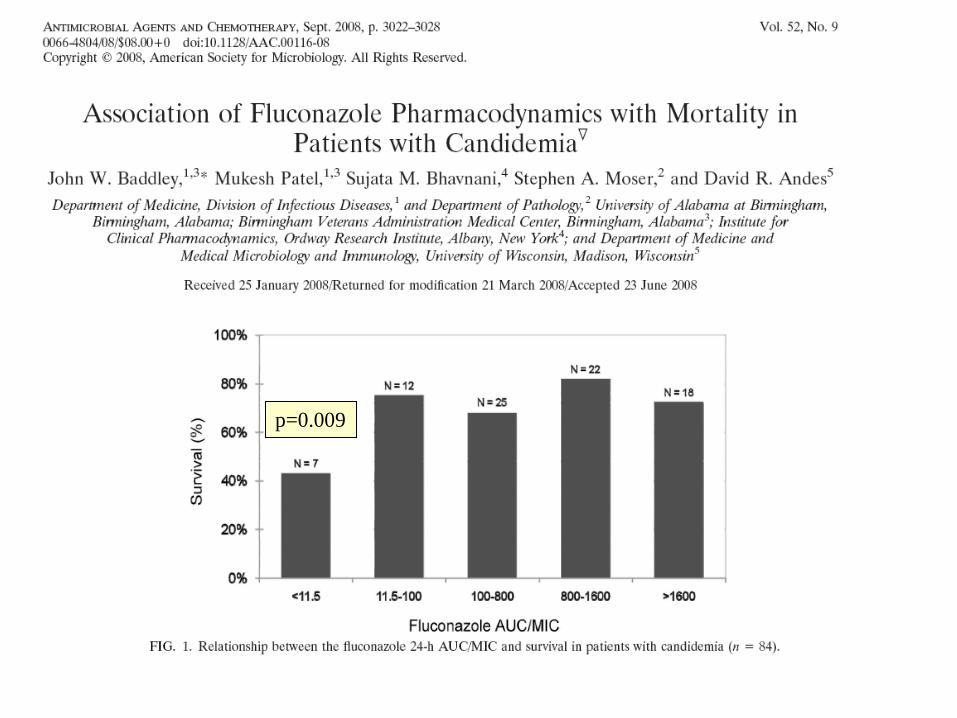
TIME TO STEP DOWN
5 DAYS
10 DAYS
I DO NOT KNOW BUT PROBABLYhellip
Personal opinion
IDSA VS ESCMID
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
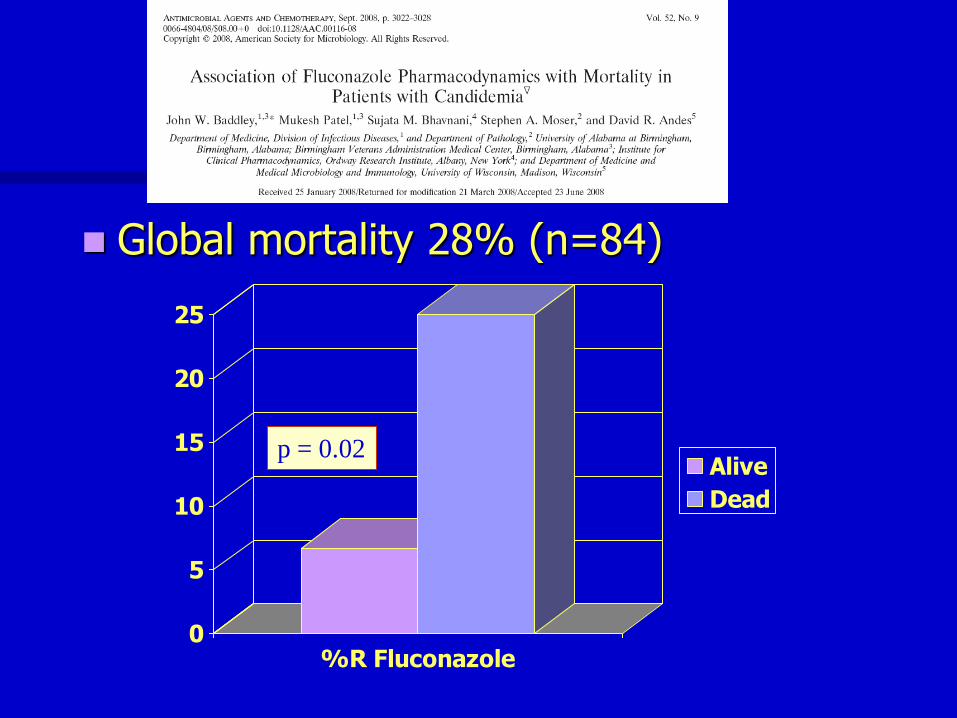
USE DE-ESCALATION STRATEGY WITHDRAW ANY ANTIFUNGAL DRUG hellipif
Personal opinion
Documentation of another etiology Or Documentation of other sources of infection Or No positive result of Platelia after 10 days and improvement of scores PCT gt 55 ngml on day 5
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
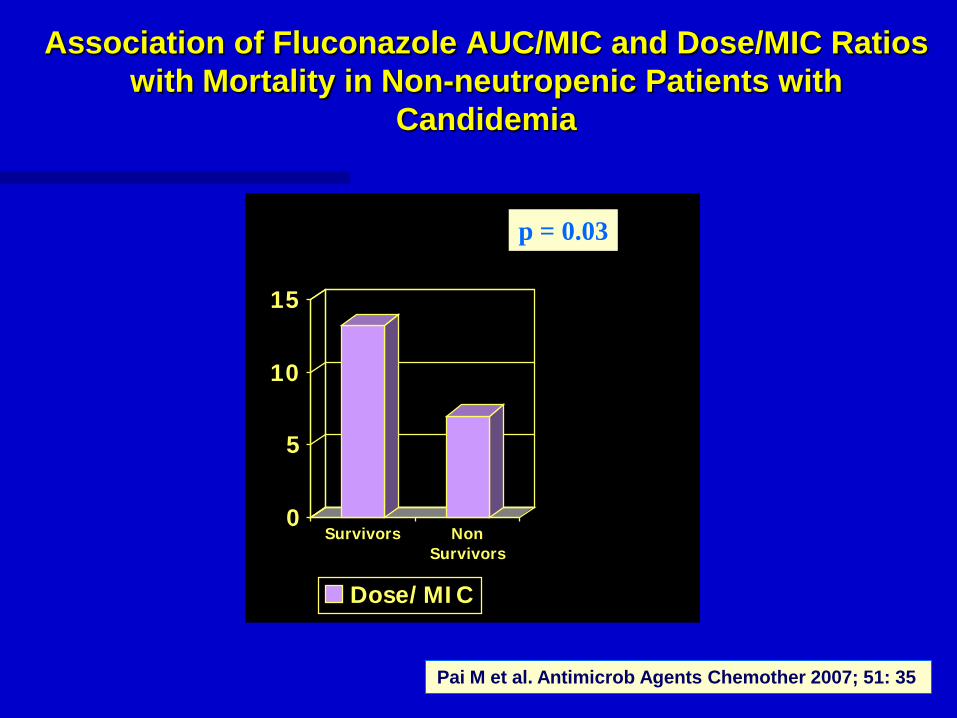
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
Personal opinion
If invasive candidiasis is confirmed by positive blood culture or sterile site after knowing susceptibility to fluconazole and the patient has recovered from MOF
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
Blood cultures= 50 sensitivity
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
iquest What can we do
PROFILAXIS Tratamiento
anticipado Tratamiento
empiacuterico
Tratamiento
dirigido
Zaragoza R et al Clin Ther Risk Man 2008 Dec
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
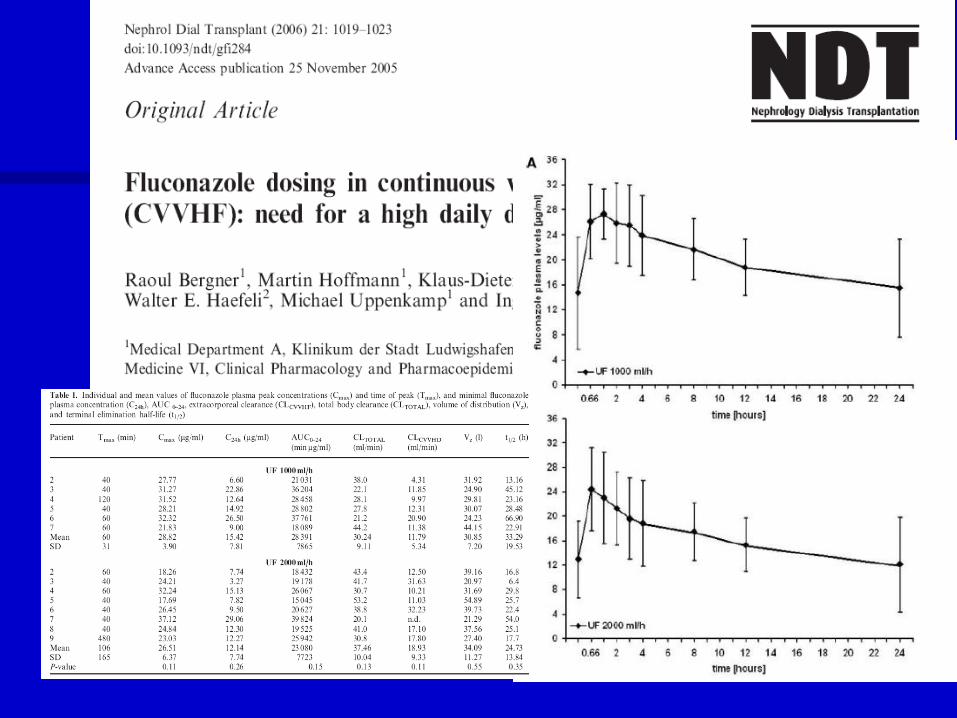
Charles PE et al Intensive Care Med 2006 32 1577-1583
Retrospective study
50 bloodstream infections 15 candidemias (11 patients) y 35 bacteremias (33
patients)
PCT gt 55 ngml NPV for candidemia
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-
Zeichner prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
Multidisciplinary approach to the treatment of invasive fungal infections in adult patients Prophylaxis empirical preemptive or targeted therapy which is the best in the different hosts Rafael Zaragoza Javier Pemaacuten Miguel Salavert Aacutengel Viudes Amparo Soleacute Isidro Jarque Emilio Monte Eva Romaacute Emilia Cantoacuten
Clin Ther Risk Man 2008 Dec
Strategy Antifungal agent References
Prophylaxis No generally recommended Patients with upper
gastrointestinal perforation heavy Candida
colonization or with severe acute pancreatitis
might be benefit
Fluconazole (Pelz et al 2001) (Garbino et al
2002) (De Waele et al
2003Piarroux et al 2004)
Empirical Use of ldquoCandida scorerdquo or the Ostrosky-Zeichner
prediction rule
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Leon et al 2006Ostrosky-
Zeichner et al 2007)
Pre-emptive Based on detection of galactomannan (13)--d-
glucan or C albicans germ tube antibodies or
PCR
De-escalation therapy ()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient
(Meersseman et al
2008Ostrosky-Zeichner et al
2005Zaragoza et al 2006)
Targeted Based on sterile site culture results De-escalation therapy()
the choice of antifungal
drug must be based on the
individual characteristics
of the patient ()
(Kullberg et al 2005Kuse et al
2007Mora-Duarte et al
2002Pappas et al 2007Phillips
et al 1997Rex et al
1994Zaragoza amp Peman 2006)
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
FUNGAL BIOMARKERS
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
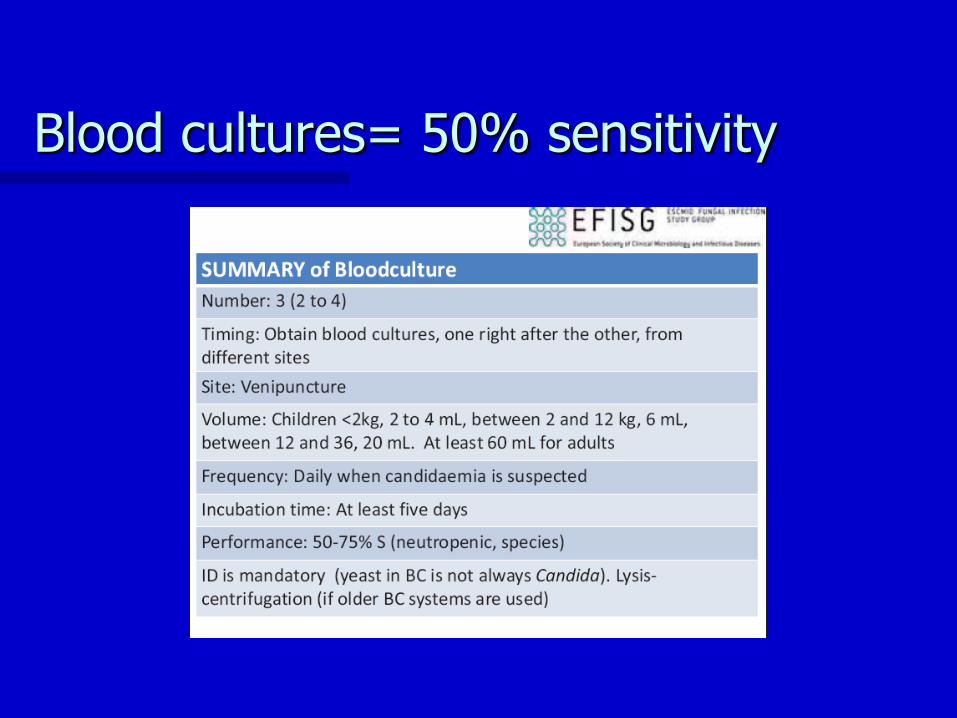
Kinetic Patterns of Candida albicans Germ Tube
Antibody (CAGTA) in Critically Ill Patients Influence
on Mortality
0
66
143
307
0
10
20
30
40
50
60
70
Treated
patients
All patients
Mortality
IncreasingCAGTA
No increasingCAGTA
2253 CAGTA +
318 Increasing titers
364 Decreasing titers
228 No change
p = 008 p = 004
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
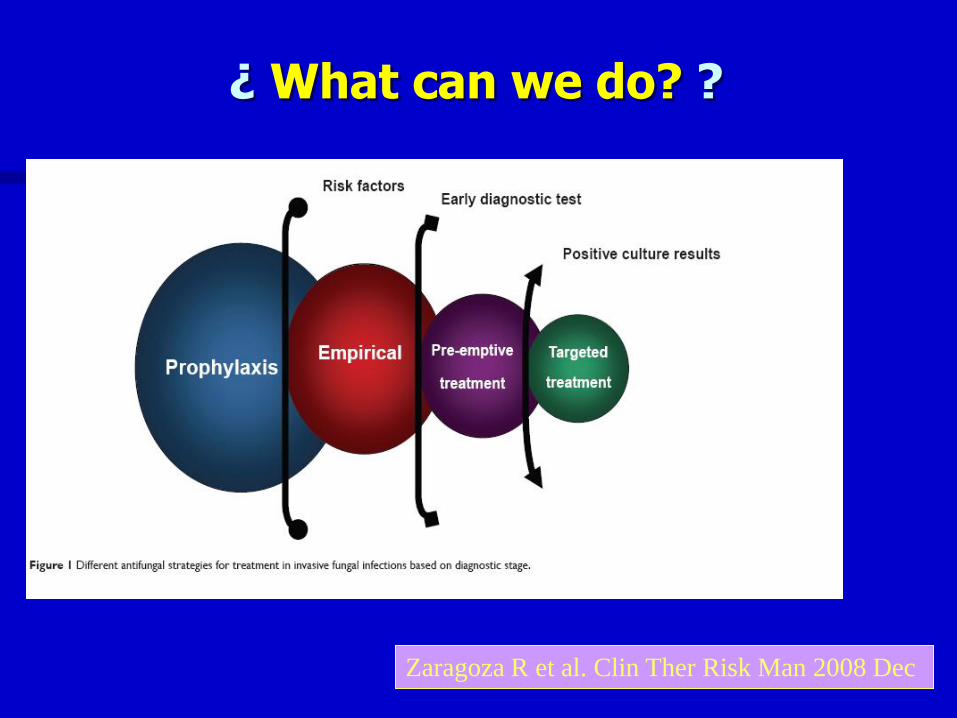
CAGTA
Monitorizing the treatment
Iruretagoyena JR Reguacutelez P Quindoacutes G Pontoacuten J Rev Iberoam Micol 2006 Mar23(1)50-3
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
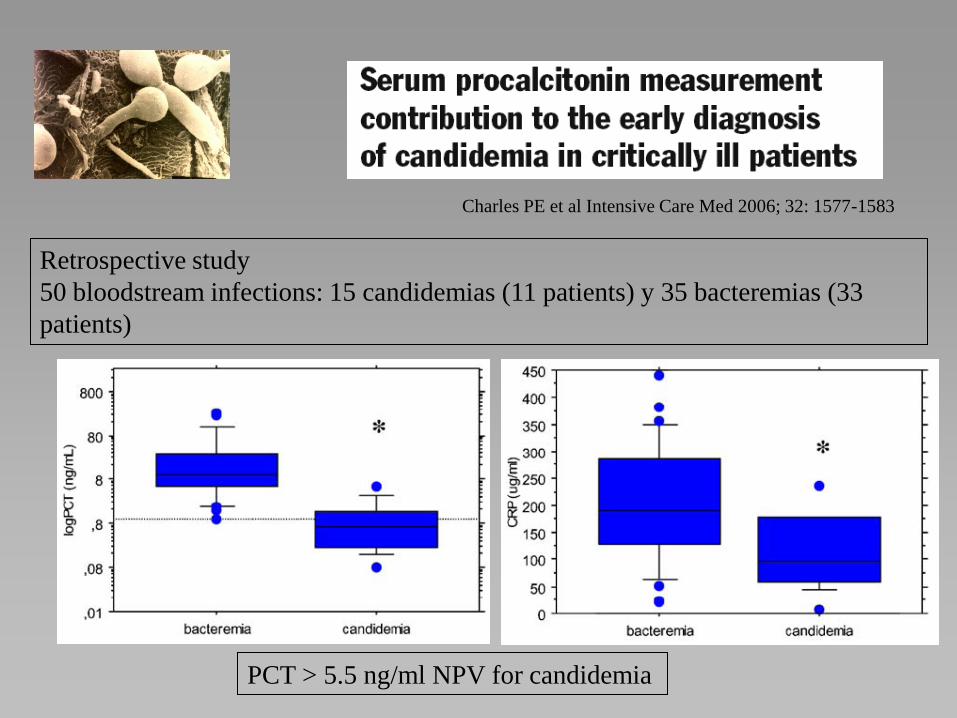
USE DE-ESCALATION STRATEGY STEPING DOWN TO FLUCONAZOLEhellipif
If IC is not confirmed (one of them)
Improvement of scores (SOFA and CS)
Negative result of Platelia (if any previous
sample was positive) or another biomarker
No positive result of Platelia on days 5 or 10 or
another biomarker
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
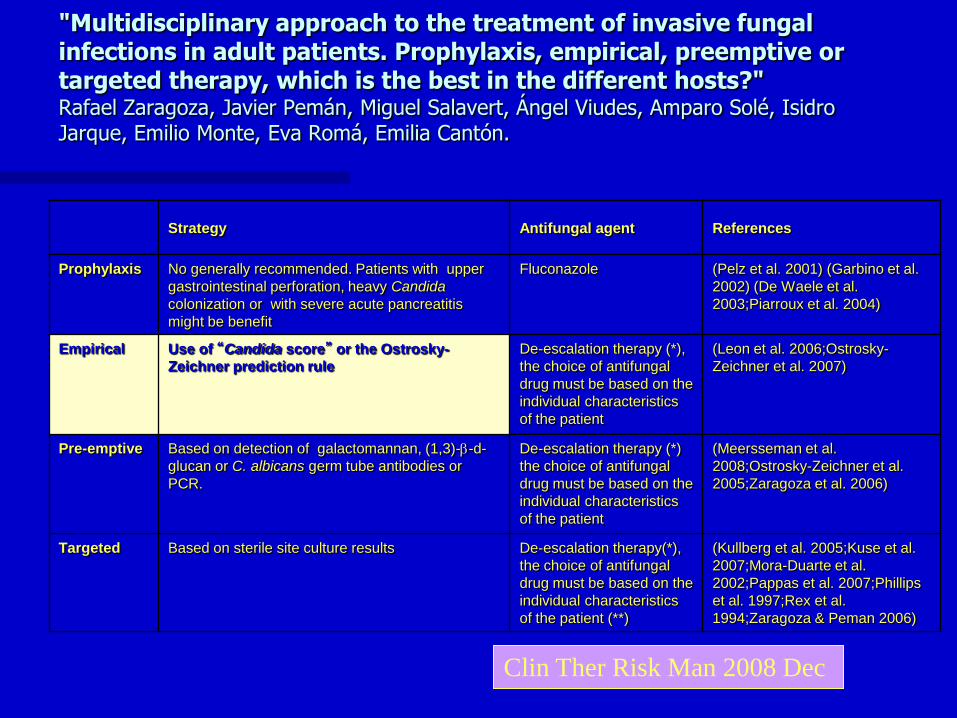
TAKE HOME MESSAGES
1 TREAT AS SOON AS POSSIBLE WITH A BROAD
SPECTRUM ANTIFUNGAL DRUG
2 FOLLOW A DE-ESCALATION PROTOCOL
COMBINE CLINICAL AND MICROBIOLOGICAL
DATA
3 DO NOT WORRY ABOUT WITHDRAW IF YOU ARE
SURE
4 USE FLUCONAZOLE WHEN THE SITUATION
OFTHE PATIENT ALLOW YOU TO DO IT
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
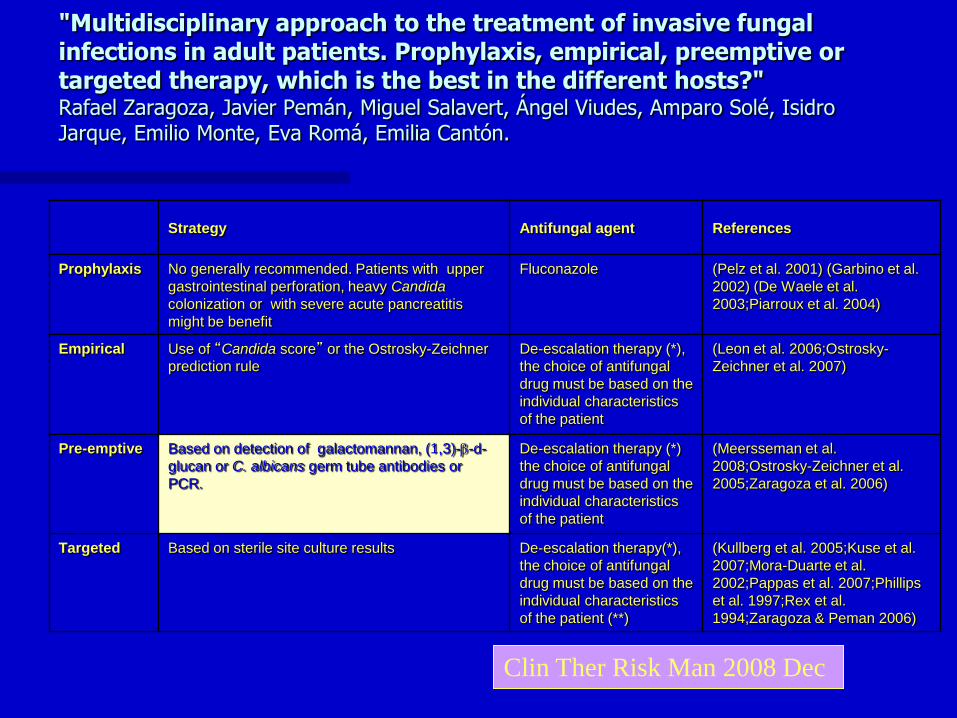
Nike
I HOPE YOU AGREE WITH ME
Fith recommendation
bull Do not wait for last talk
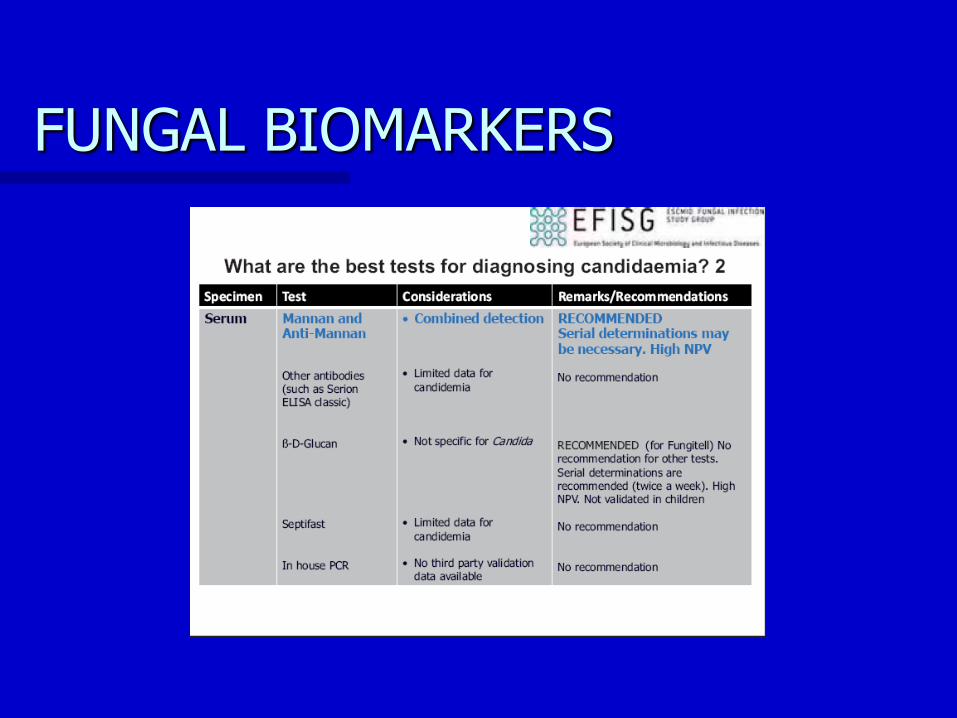
Fith recommendation
bull Do not wait for last talk