Embed Size (px)
Citation preview
Anticoagulation: How Do I Pick From All the Choices?
Jeffrey H. Neuhauser, DO, FACC BHHI Primary Care Symposium
February 28, 2014
2
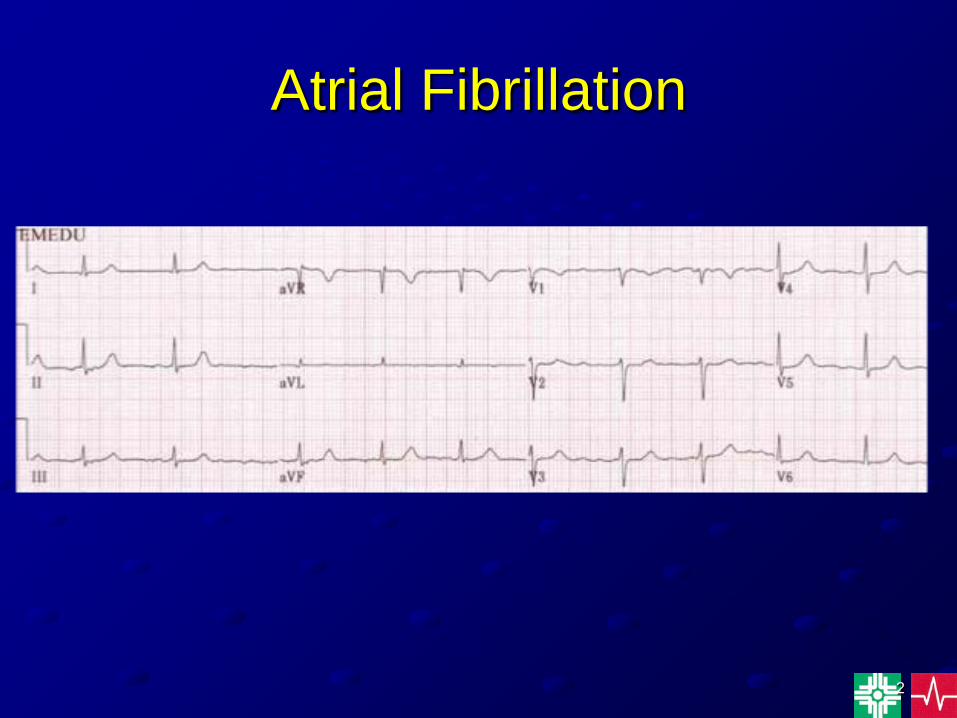
Atrial Fibrillation

3
Atrial Fibrillation
• The most common arrhythmia encountered in clinical practice.
• The prevalence increases with age.• Risk factors include HPTN, valvular heart
disease, cardiomyopathy, obesity, sleep apnea, congenital heart disease, pulmonary disease, & hyperthyroidism.
• Classified as paroxysmal, persistent, or permanent.
• Major complications include CHF & stroke.
4
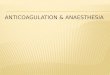
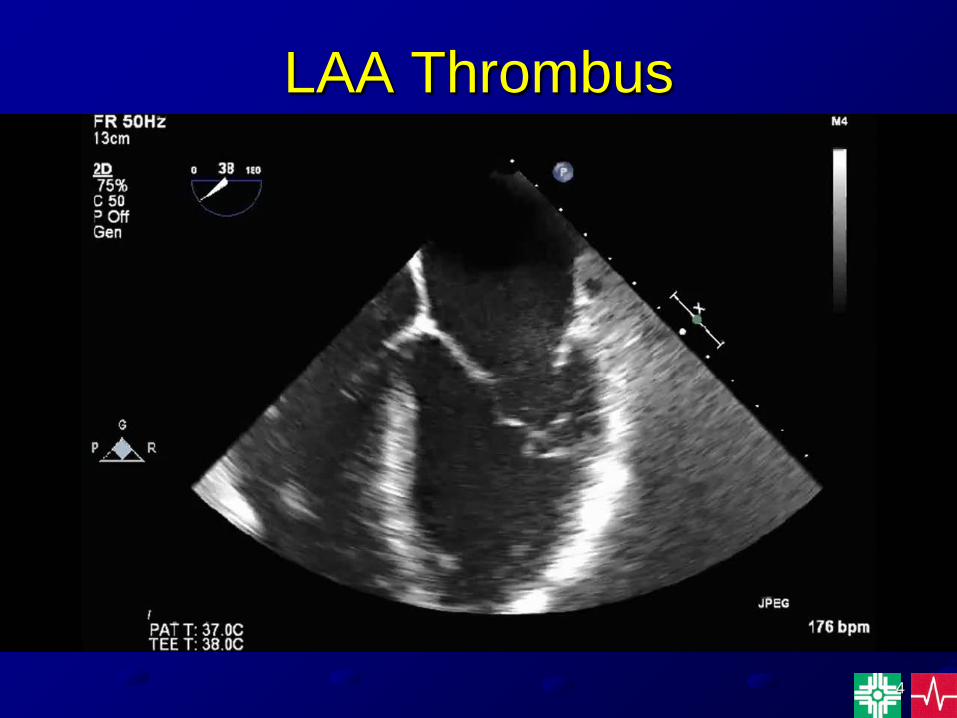
LAA Thrombus
5
AF - CASE STUDIES• 45 yr old male. No significant PMH. Develops AF while
training for a marathon. He presents to the ER & then spontaneously converts to SR after 6 hrs. Baseline ECG & Echo are normal.
• 76 yr old female with HPTN, NIDDM who presents to her PCP for an annual checkup is found to be in AF with a controlled ventricular response. She is completely unaware that she is in AF. She has a history of GI hemorrhage within the past year.
• 68 yr old male with previous CABG, CHF, HPTN, & AS presents to the ER with a 2 day history of palpitations. He is found to be in AF with a RVR. He is admitted to the hospital & started on IV diltiazem for rate control.
6
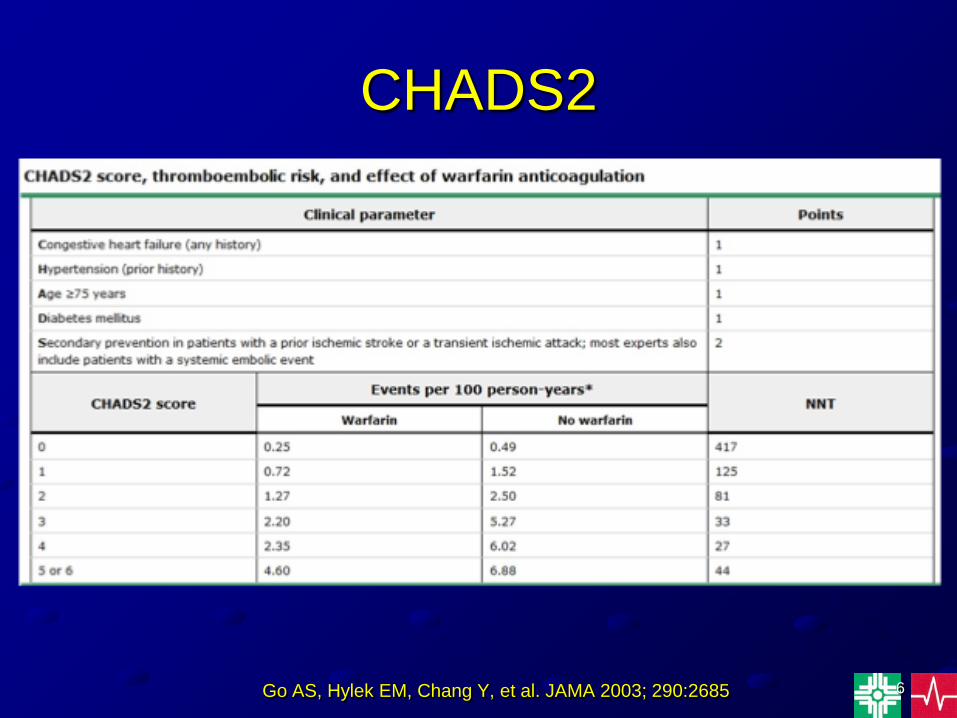
CHADS2
Go AS, Hylek EM, Chang Y, et al. JAMA 2003; 290:2685
7
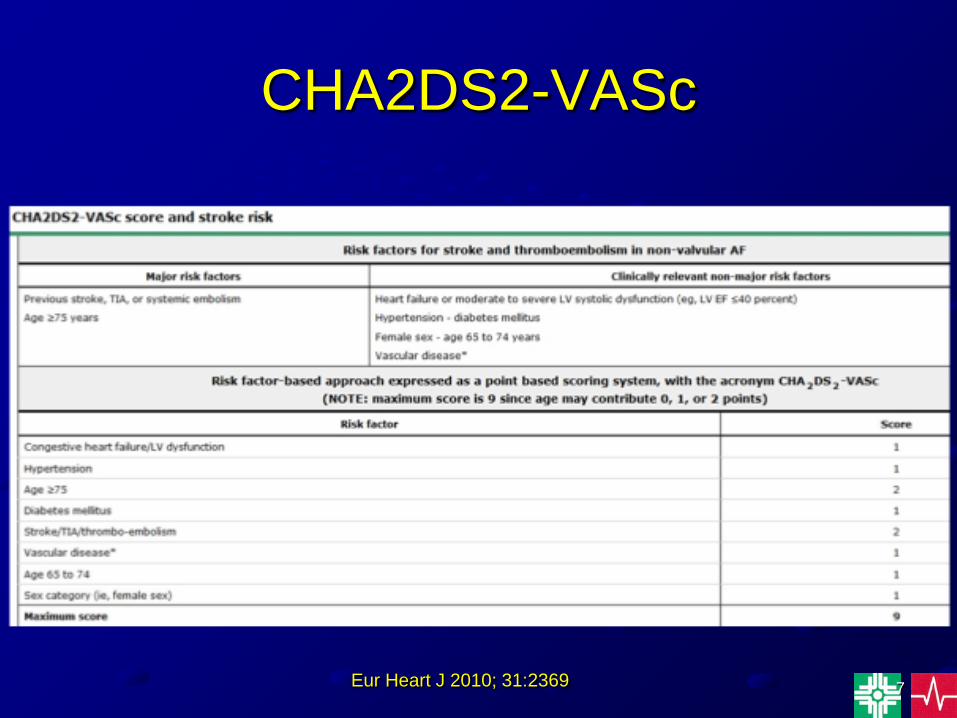
CHA2DS2-VASc
Eur Heart J 2010; 31:2369
8
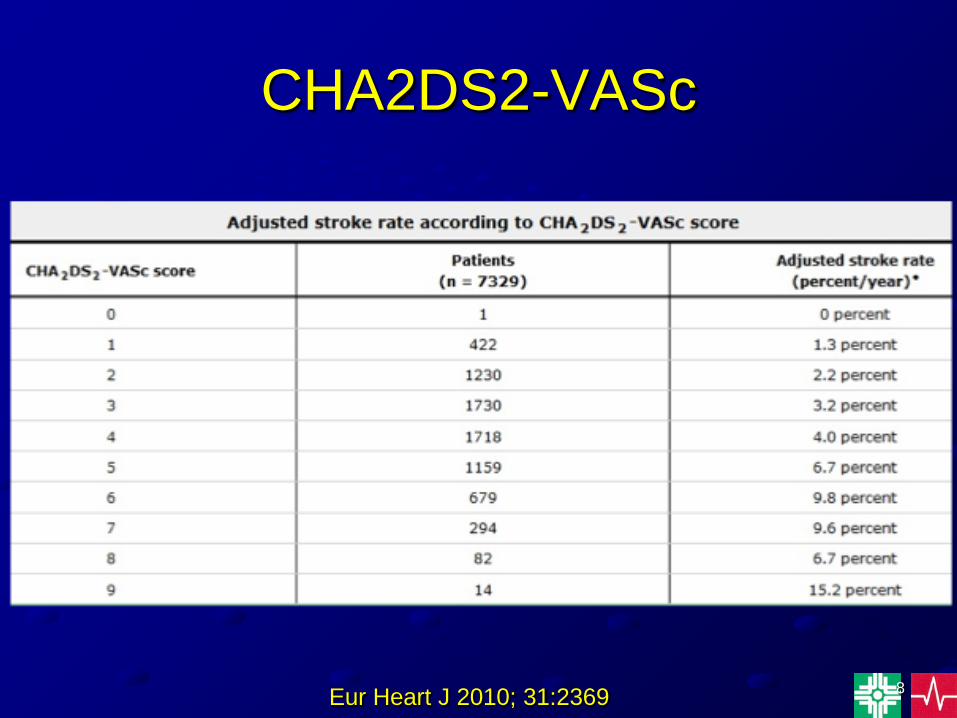
CHA2DS2-VASc
Eur Heart J 2010; 31:2369
9
Warfarin• Inhibits vit K dependent coagulation factors• Metabolism - Liver CYP450• 1/2 life 20-60h• Dose adjusted to INR 2-3• Many drug & food interactions• Common drugs that increase the INR - Quinolones,
Erythromycins, Tetracyclines antifungals, Isoniazid, Amio, Propafenone, Gemfibrizol, Niacin,Pantoprozole, Paroxitene, Rouvastatin
10
Dabigatran (Pradaxa)
• Direct thrombin inhibitor• Indicated for the prevention of stroke &
thromboembolism in nonvalvular AF• No liver CYP 450 metabolism; Primarily
urine excretion• 1/2 life 12-17 hrs• CrCl >50 ml/min - dose 150mg bid• CrCl 30-50 ml/min - dose 75 mg bid
11
Drugs that Increase Dabigatran Levels
• Cyclosporin• Dronedarone• Antifungal agents - Itraconazole & Ketoconazole• Quinidine• Verapamil
12
Drugs That Decrease Dabigatran Levels
• Carbamazepine• Rifampin• St. John’s Wort
13
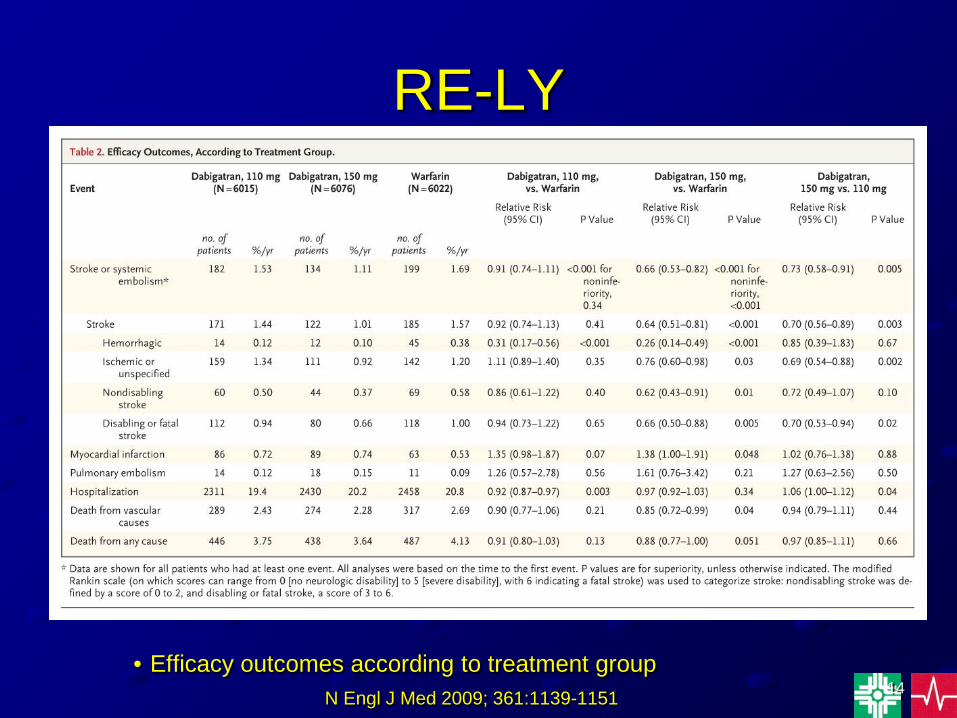
RE-LY
• Comparison of Dabigatran (150 mg bid & 110 mg bid) with warfarin in pts with nonvalvular AF & risk of stroke.
• Randomized, blinded for dabigatran, unblinded for warfarin
• Primary outcome was stroke or systemic embolization
• Median duration of F/U - 2 yearsN Engl J Med 2009; 361:1139-1151
14
RE-LY
• Efficacy outcomes according to treatment groupN Engl J Med 2009; 361:1139-1151
15
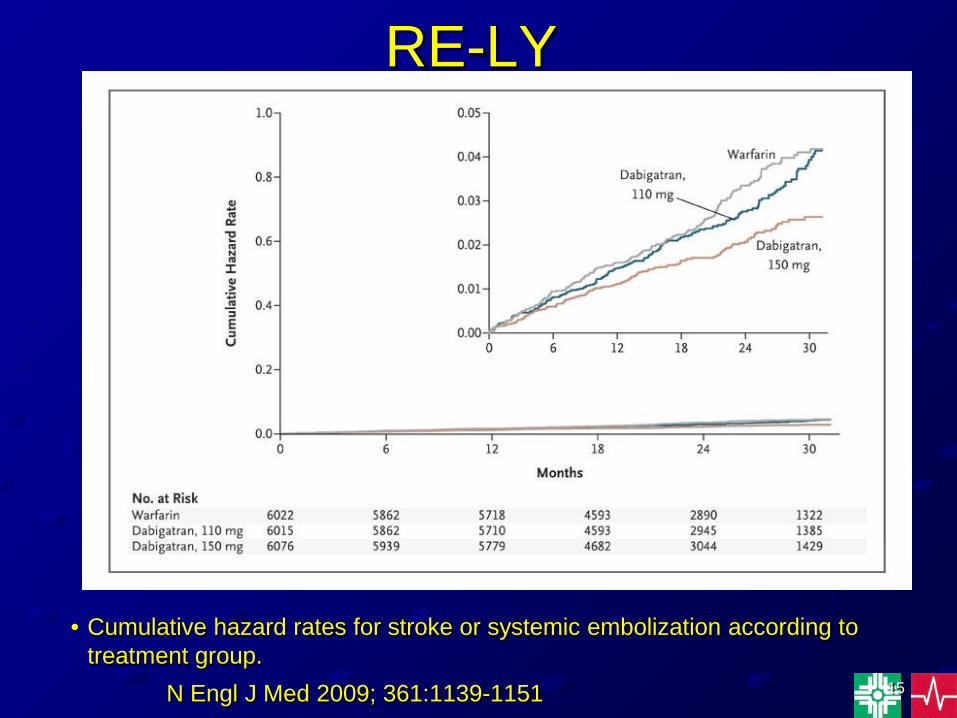
RE-LY
• Cumulative hazard rates for stroke or systemic embolization according to treatment group.
N Engl J Med 2009; 361:1139-1151
16
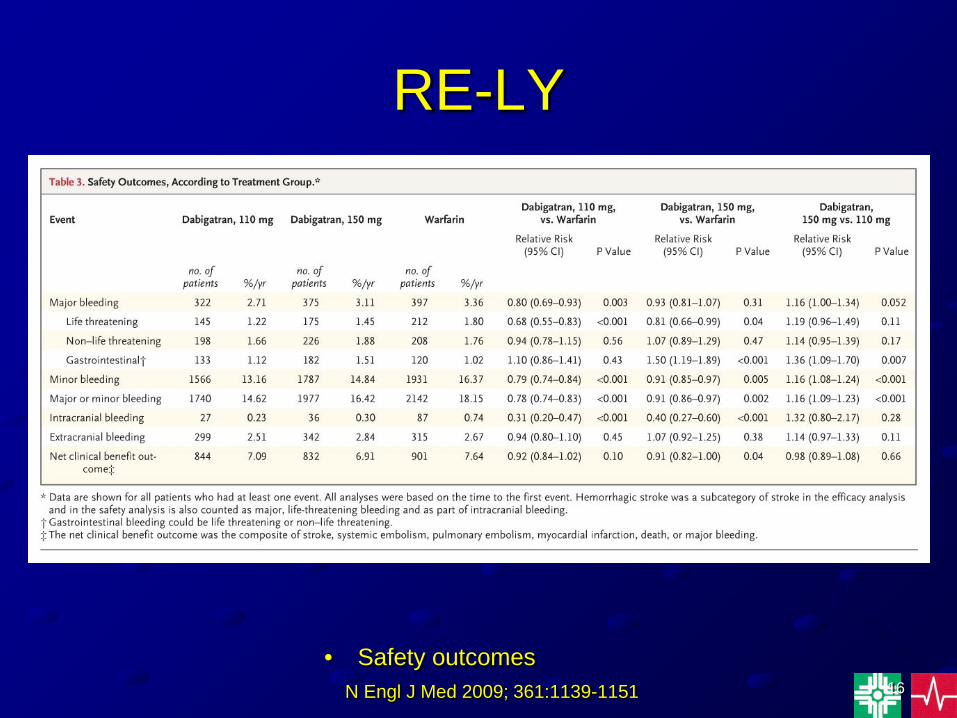
RE-LY
• Safety outcomesN Engl J Med 2009; 361:1139-1151
17
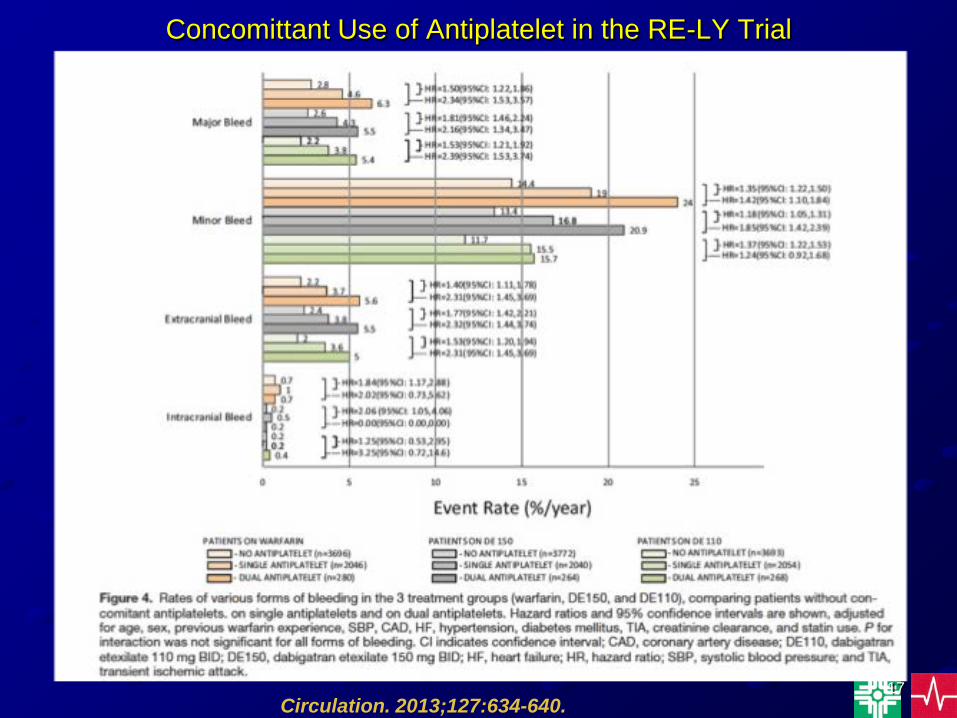
Concomittant Use of Antiplatelet in the RE-LY Trial
Circulation. 2013;127:634-640.
18
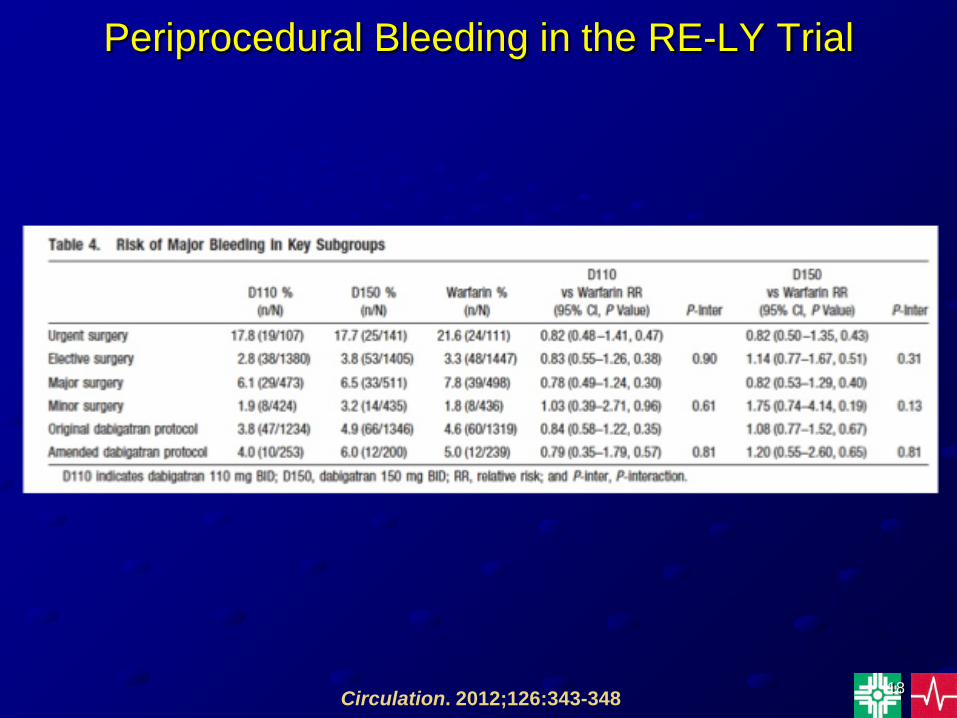
Periprocedural Bleeding in the RE-LY Trial
Circulation. 2012;126:343-348
19
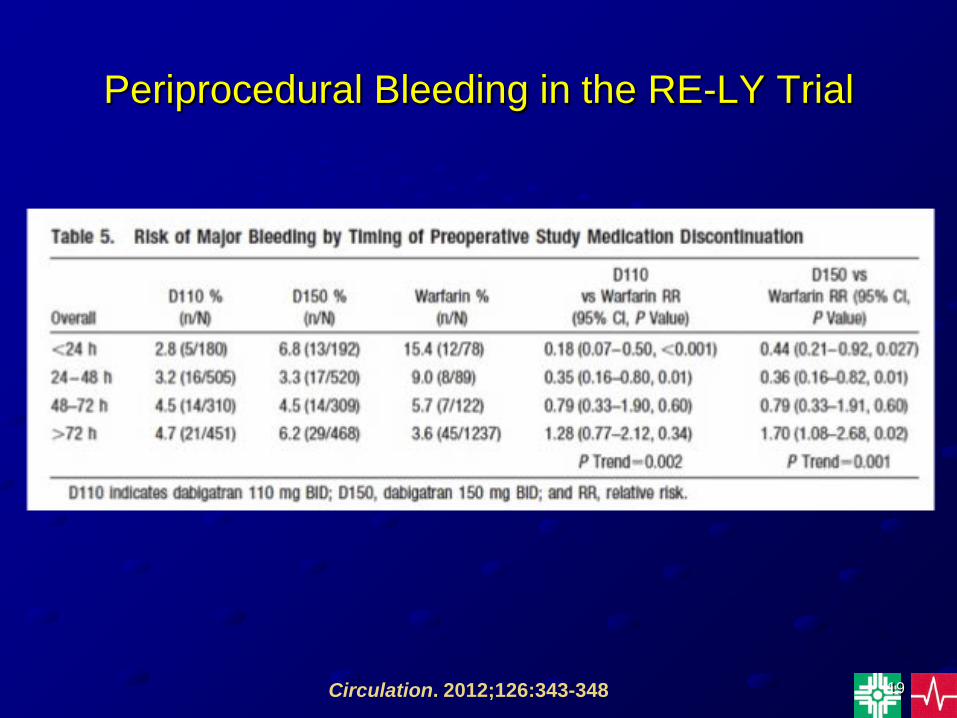
Periprocedural Bleeding in the RE-LY Trial
Circulation. 2012;126:343-348
20
RE-ALIGN
• Dabigatran vs warfarin S/P AVR & MVR within 7 days & after 3 months.
• Dabigatran dose 150, 220, 300mg bid based on renal function.
• The trial was terminated prematurely due to an excess of thromboembolic & bleeding events in the dabigatran group.
N Engl J Med 2013;369:1206-14
21
Rivaroxaban (Xarelto)
• Factor Xa inhibitor• Indicated for the prevention of stroke &
thromboembolism in nonvalvular AF. Also indicated for the prevention & tx of DVT/PE.
• Metabolism - Liver CYP450; Urinary excretion 66%
• 1/2 life 5-9 hrs; 11-13 hrs in the elderly• CrCl >50 ml/min - dose 20 mg daily• CrCl 15-50 ml/min - dose 15 mg daily
22
Drugs That Increase Rivaroxaban Levels
• Amiodarone, Dronedarone• Erythromycins• Cyclosporine• Diltiazem• Antifungal agents - Itraconazole & Ketoconazole• Phenytoin• Ranolazine• Tamoxifen• Verapamil
23
Drugs That Decrease Rivaroxaban Levels
• Carbamazepine• Phenytoin• Rifampin• St. John’s Wort
24
ROCKET AF
• Comparison of Rivaroxaban (20 mg daily) vs warfarin (INR 2-3) in pts with nonvalvular AF.
• Randomized, double blind design.• Primary endpoint - stroke or systemic
embolization.N Engl J Med 2011;365:883-91
25
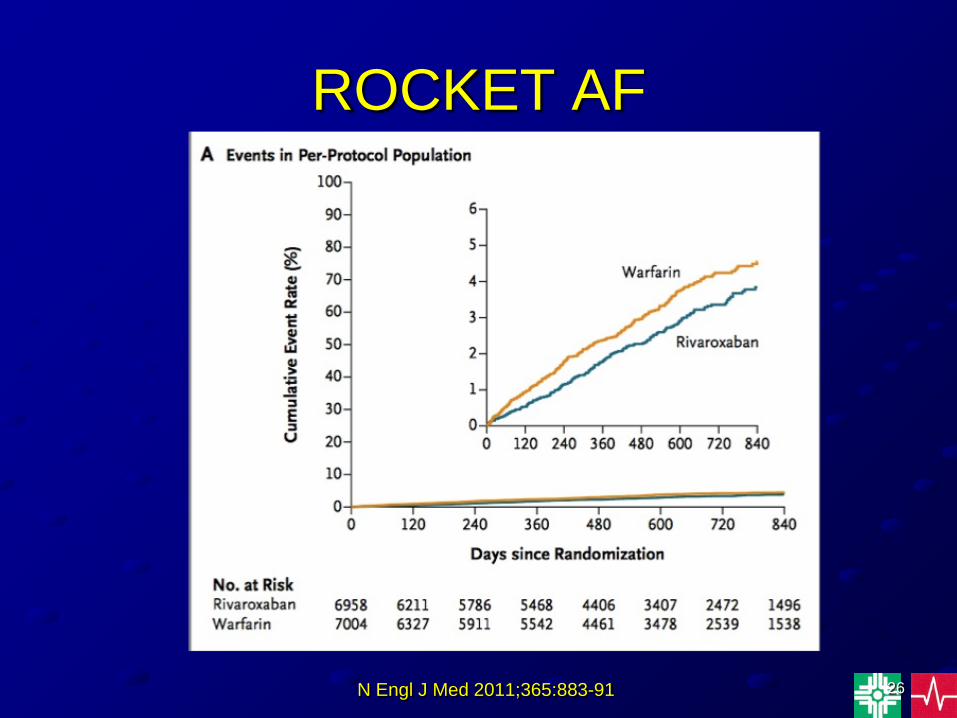
ROCKET AF
• The Rivaroxaban group had 21% reduction in stroke & systemic embolization.
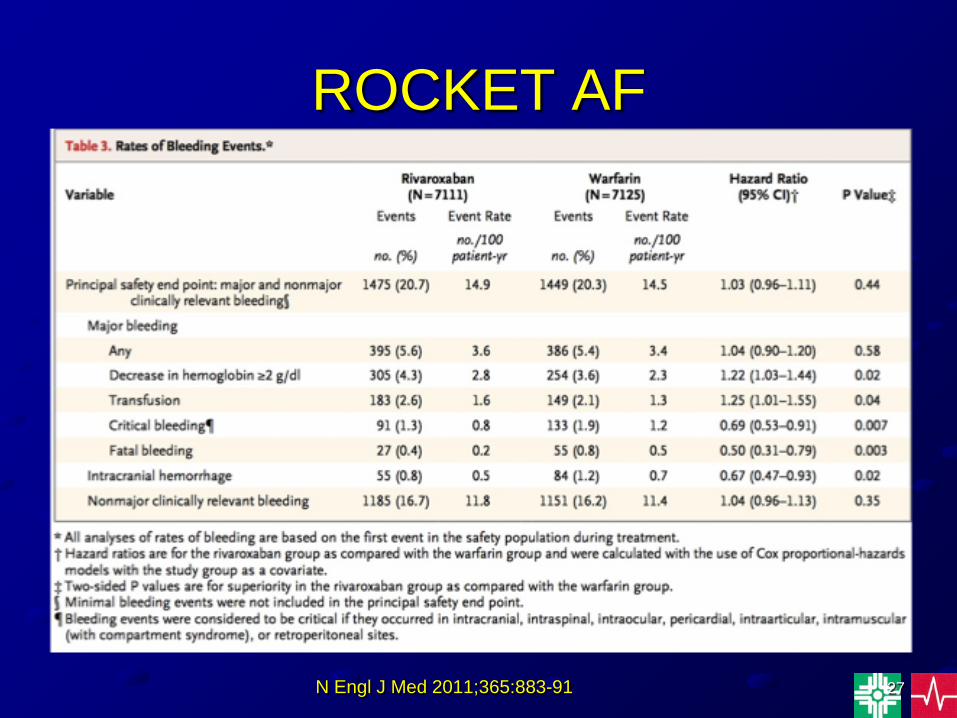
• Incidence of major bleeding was similar -Rivaroxaban (14.9%) vs warfarin (14.5%).
• The Rivaroxaban group had significantly less intracranial hemorrhage (0.5% vs 0.7%) & fatal hemorrhage (0.2% vs 0.5%).
N Engl J Med 2011;365:883-91
26
ROCKET AF
N Engl J Med 2011;365:883-91
27
ROCKET AF
N Engl J Med 2011;365:883-91
28
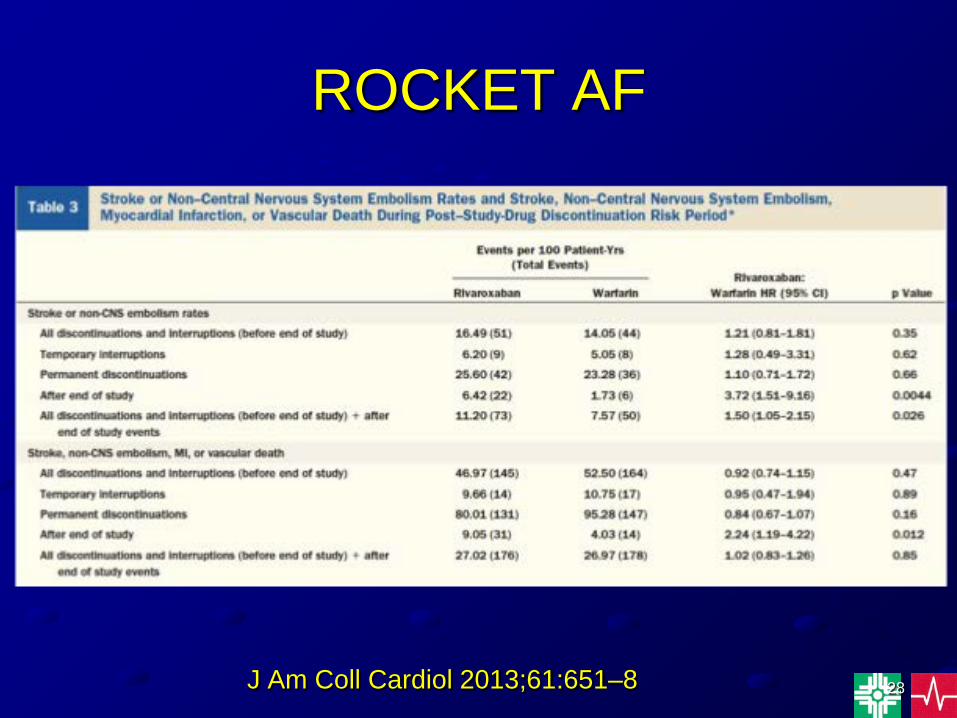
ROCKET AF
J Am Coll Cardiol 2013;61:651–8
29
ROCKET AF
• The mean time in therapeutic range in the warfarin group was 55.2%.
• The mean time with an INR <2 was 29.1%.• The mean time with an INR >3 was 15.7%.
J Am Heart Assoc. 2013;2:e000067 doi 10.1161/JAHA.112.000067
30
Apixaban (Eliquis)
• Factor Xa inhibitor• Indicated for the prevention of stroke &
thromboembolism in nonvalvular AF• Metabolism - Liver CYP450; Urine
excretion 27%• 1/2 life 12 hrs• Dose 5 mg bid• Creat >1.5, age >80, wt <60 kg - dose 2.5
mg bid
31
Drugs That Decrease Apixaban Levels
• Dexamethasone• Nafcillin• Phenobarbital• Phenytoin• Rifampin• St. John’s Wort
32
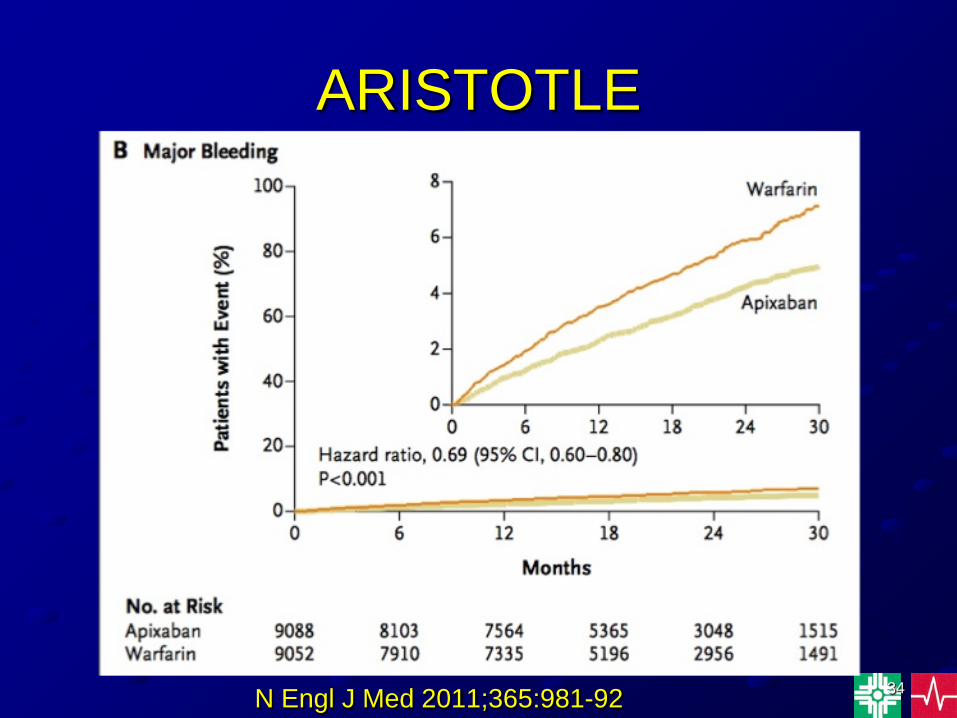
ARISTOTLE
• Apixaban vs Warfarin in pts with AF• Randomized, double blind trial design• Pts had at least 1 additional RF for stroke• Primary outcome: stroke or systemic
embolization• Median duration of F/U - 1.8 years
33
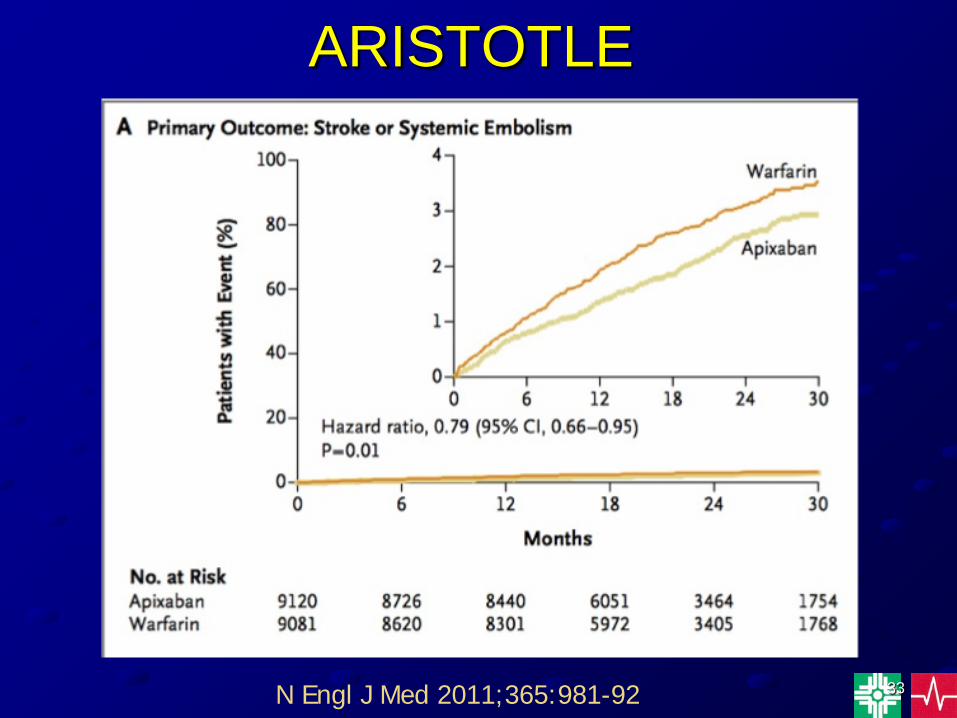
ARISTOTLE
N Engl J Med 2011;365:981-92
34
ARISTOTLE
N Engl J Med 2011;365:981-92
35
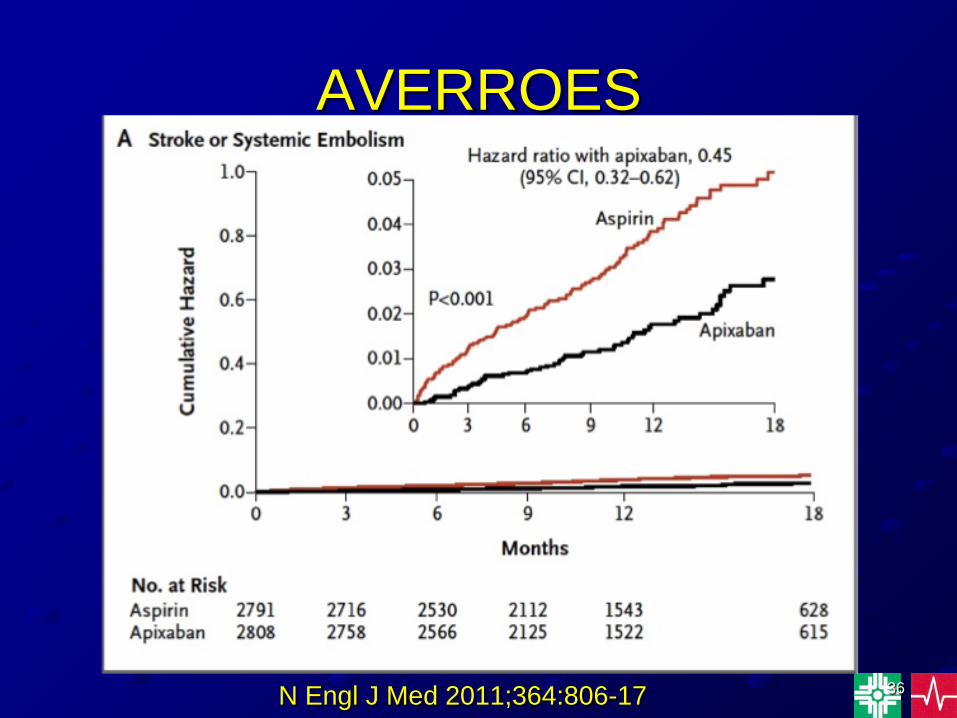
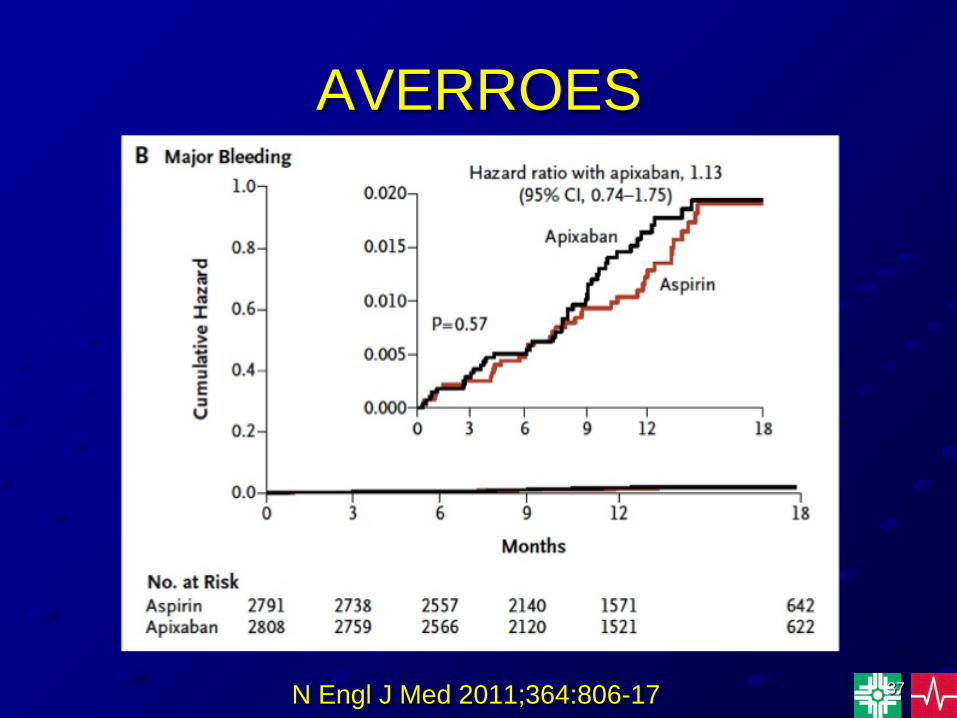
AVERROES
• Apixaban vs ASA in pts with AF• Double blind, randomized design• Mean F/U 1.1 years• The primary outcome was stroke or
systemic embolizationN Engl J Med 2011;364:806-17
36
AVERROES
N Engl J Med 2011;364:806-17
37
AVERROES
N Engl J Med 2011;364:806-17
38
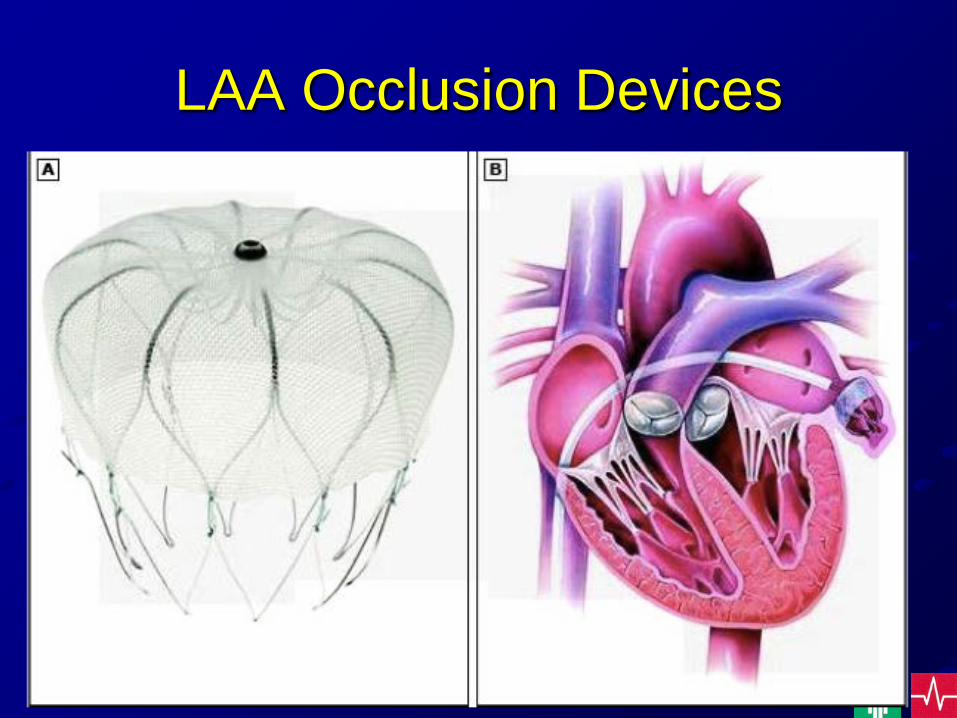
LAA Occlusion Devices
39
PROTECT AF• Comparison of a LAA closure device (Watchman) with
warfarin for the prevention of stroke & systemic embolization in pts with nonvalvular AF & at least 1 risk factor.
• After device implantation, pts received warfarin for 45 days, followed by clopidogrel for 4.5 months & then life long ASA.
• Mean F/U 2.3 yrs.• Composite endpoint - stroke, systemic embolization, &
CV death. • Primary composite endpoint in the Watchman group
(3%) was equivalent to the warfarin group (4.3%).Circulation.2013;127:720-729
40
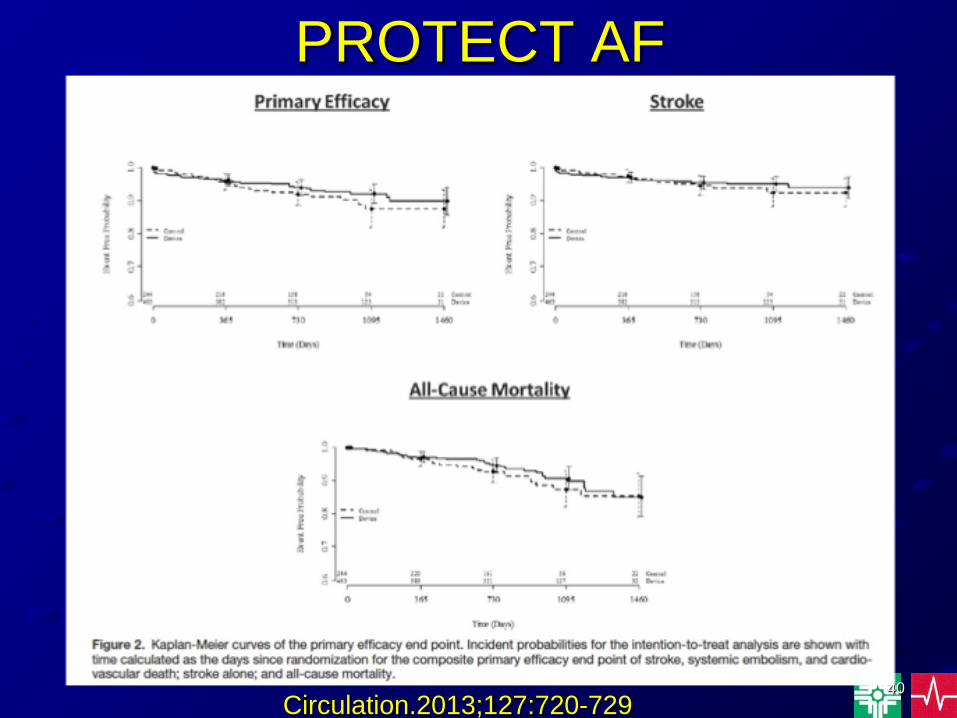
PROTECT AF
Circulation.2013;127:720-729
41
ASAP Study
• Evaluation of the Watchman LAA closure device in pts with nonvalvular AF ineligible for warfarin.
• 150 pts with nonvalvular AF & CHADS2 score at least 1
• Primary efficacy end point was the combined events of ischemic stroke, hemorrhagic stroke, systemic embolization, CV / unexplained death.
J Am Coll Cardiol 2013;61:2551–6
42
ASAP Study• Pts with LVEF <30%, intracardiac thrombus, dense
spontaneous echo contrast on TEE, PFO, significant mitral stenosis, pericardial effusion >3 mm, mobile plaque in the ascending aorta or aortic arch were excluded.
• Following implant, pts received 6 months of clopidogrel or ticlopidine followed by life long ASA.
• The mean CHADS2 score was 2.8.• Mean f/u 14.4 months.
J Am Coll Cardiol 2013;61:2551–6
43
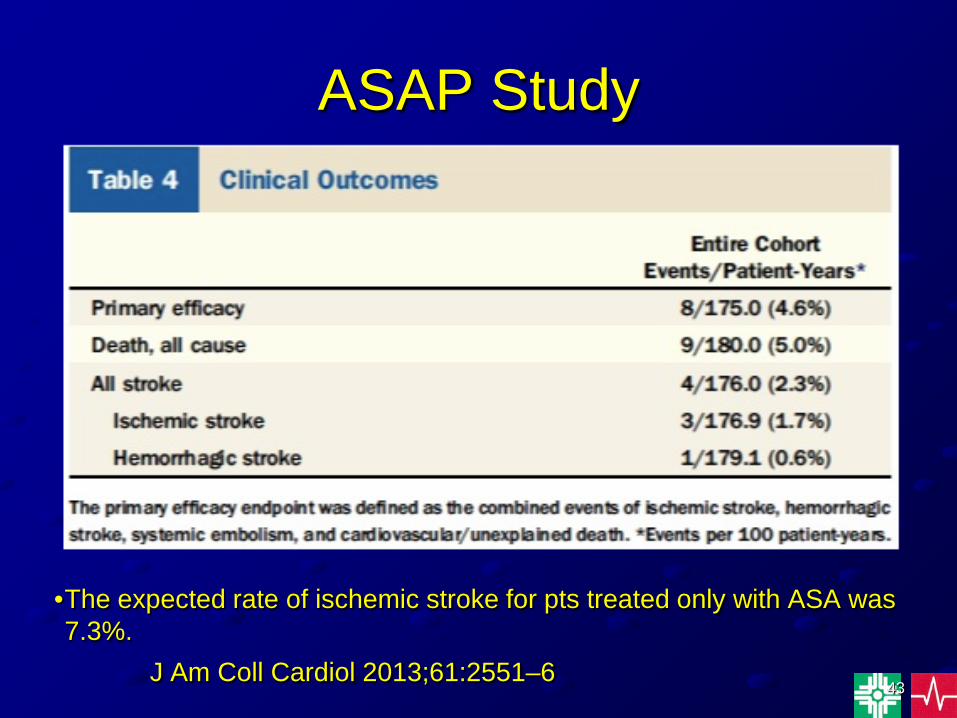
ASAP Study
•The expected rate of ischemic stroke for pts treated only with ASA was 7.3%.
J Am Coll Cardiol 2013;61:2551–6
44
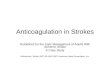
THE WATCHMAN LAA OCCLUSION DEVICE

45
Cryoablation for AF