-
7/31/2019 Anticancer Agents 1
1/20
Antineoplastic Agents and Biologic Response Modifiers
Antineoplastic Agents
Anticancer/AntineoplasticDrugs
Introduction___________________
In the United States cancer the second
leading cause of death- second only to heart disease. It is the
leading cause of
death in women. In children between ages 1 and 15 years, cancer
is the leading
cause of death after accidents. The most common types of cancer
in men are
prostate, lung, and colorectal cancer. In women, common types
include breast,
lung, and colorectal cancer.
Cancer results from alterations in the deoxyribonucleic acid
(DNA) within
the cell. DNA is the genetic substance in the body cells. In
addition, DNA
transfers information necessary for the production of enzymes
and protein
synthesis.
Anti-cancer drugs, also called cancer chemotherapeutic agents
or
antineoplastic drugs were introduced in the treatment of cancer
in the 1940s.
The first antineoplastic drugs included estrogen for prostatic
cancer and the
nitrogen mustard drug mechlorethamine hydrochloride (Mustargen).
Many of theearly anticancer drugs such as methotrexate,
5-flourouracil, 6-mercaptopurine,
and cyclophosphamide, are still in use. Since the early 1970s
more anticancer
drugs have been marketed, and drug protocols (detailed plans)
using
combinations of drugs have been proven effective in curing
specific leukemias
and Hodgkins disease. Anticancer drugs are given for several
reasons, including
-
7/31/2019 Anticancer Agents 1
2/20
Antineoplastic Agents and Biologic Response Modifiers
cure, control, and palliation. Chemotherapy may be used as the
sole treatment of
cancer or in conjunction with radiation and surgery.
Cancer Chemotherapy_____________________________
It is difficult for anticancer drugs to be selective in killing
tumor cells and
not normal cells. If large anticancer doses are given to kill
malignant cells, normal
cells usually are also killed; thus the death of the client
could result.
There are various protocols for successful chemotherapy. If
the
chemotherapy is extended too long or the doses are too high,
toxicity is likely to
occur. Eliminating every cancer cell can be difficult. When
symptoms disappear;
it had once been thought that malignant cells were eradicated
but this is
generally not true, because 1 million cells could remain when
there are no
symptoms. It is still not known how long cancer therapy should
be continued.
With continuous research and protocol drug therapy, an answer is
anticipated
soon.
Drug Resistance__________________________________
Tumor resistance can develop against an anticancer drug because
the
drug is used too infrequently or the tumors location limits the
effectiveness of the
drug. Brain tumors respond poorly to anticancer drugs because
most drugs do
not cross the blood brain barrier. Nitrosoureas, however, do
cross the blood-brain
barrier. Intraarterial infusion of drugs at the site may be
necessary.
Changes in DNA are major cause of drug resistance and mutation
of
cancer cells is also a factor in drug resistance. As the tumor
ages, cancer cells
mutate as they multiply; thus the cancer cells are no longer
identical. The
mutated cells may differ in response to drug therapy.
-
7/31/2019 Anticancer Agents 1
3/20
Antineoplastic Agents and Biologic Response Modifiers
Combination Chemotherapy________________________
To achieve the best tumor kill, chemotherapy needs to target
cells in all
phases of the cell cycle. Combining chemotherapy drugs makes
this possible.CCS and CCNS are often combined to maximize cell
death.
Classifications of Anticancer Drugs
1. Alkylating Drugs
- It belongs to CCNS category and kills cells by forming
cross-links on the DNA
strands
Cyclophosphamide (Cytoxan)______________________________
Pharmacokinetics
Cyclophosphamide is well absorbed from the GI tract. Its
half-life is
moderate, and it is moderately protein-bound. The drug is
metabolized by the
liver, and less than 50% is excreted unchanged in the urine.
Pharmacodynamics
The onset of the action begins within hours; however, the
desired effect
may take several days. It is one of the anticancer drugs that
can be administered
orally.
Several drug interactions may occur with cyclophosphamide:
thiazides
and allopurinol can increase bone marrow depression; the effect
of digoxin
decreases; and the effect of insulin increases, causing
hypoglycaemia.
-
7/31/2019 Anticancer Agents 1
4/20
Antineoplastic Agents and Biologic Response Modifiers
Phenobarbital and rifampin may increase cyclophosphamide
toxicity. Adverse
reactions should be observed and reported.
Uses and Considerations
For treatment of progressive carcinoma of prostate. Consists of
estrogen
and nitrogen mustard.
Side Effects
Nausea
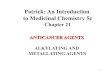
Peripheral edema
Thrombophlebitis
Breast tenderness
2. Antimetabolites
- They are classified as CCS and affect S phase (DNA synthesis
and
metabolism) of the cell cycle. Many of the antimetabolites drugs
resemble natural
metabolites; thus they disrupt the metabolic processes and some
of the agents
inhibit enzyme synthesis.
Fluorouracil_____________________________________________
Pharmacokinetics
Fluorouracil is administered IV for carcinoma and topically for
superficial
basal cell carcinoma. Protein-binding is less than 10% and the
half-life for the IV
route is short (10 to 20 minutes). A small amount of the drug is
excreted in the
urine, and up to 80% is excreted by the lungs as carbon
dioxide.
Peripheral Edema (Feet)
-
7/31/2019 Anticancer Agents 1
5/20
Antineoplastic Agents and Biologic Response Modifiers
Pharmacodynamics
Fluorouracil, a CCS drug, blocks the enzyme action necessary for
DNA
and ribonucleic acid (RNA) synthesis. The drug has a low
therapeutic index.
Fluorouracil can be used alone or in a combination with other
anticancer drugs.
Fluorouracil can cross the blood-brain barrier. Its duration of
action is 30 days.
Uses and Considerations
To treat advanced or metastatic adenocarcinoma of the pancreas.
Acts at
the S phase of cell cycle. To monitor leukocytes and platelet
count; reduce dose
if these values are extremely low.
Side Effects
Anorexia
Nausea
Vomiting
Diarrhea
Stomatitis
Alopecia
Photosensitivity
Increased pigmentation
Rash
Erythema
Bone marrow suppression
-
7/31/2019 Anticancer Agents 1
6/20
Antineoplastic Agents and Biologic Response Modifiers
3. Antitumor Antibiotics
- Inhibit protein and RNA synthesis and bind DNA, causing
fragmentation.
Doxorubicin and Plicamycin_______________________________
Pharmacokinetics
Doxorubicin and plicamycin are administered IV. Doxorubicin
is
metabolized in the liver to active and inactive metabolites. The
various
metabolites affect the half-life; the initial phase of the
doxorubicin is 12 minutes,
the intermediate phase is 3.5 hours, and the final phase is 30
hours.
Pharmacodynamics
The primary effects of doxorubicin and plicamycin differ
although they are
classified as antitumor antibiotics. Doxorubicin is prescribed
in combination with
other anticancer agents for the treatment of breast cancer,
ovaries, lung, and
bladder and, leukemias and lymphomas. Plicamycin may be used in
combination
with other anticancer agents for the treatment of testicular
carcinoma. Its primary
use is for correction of hypercalcemia.
Because plicamycin affects bleeding time, use of aspirin,
anticoagulants,
and thrombolytic agents should be avoided. The use of
cyclophosphamide with
doxorubicin can increase the chance of haemorrhagic
cystitis.
Uses and Considerations
Doxorubicin
To treat breast, bladder, ovarian, and lung cancers; leukemias;
lymphomas
-
7/31/2019 Anticancer Agents 1
7/20
Antineoplastic Agents and Biologic Response Modifiers
Plicamycin
To correct hypercalcemia, and hypercaliciuria; to treat
testicular carcinoma
Side Effects
Doxorubicin
Alopecia
Nausea
Vomiting
Stomatitis
Leukopenia
Thrombocytopenia
Rash
Plicamycin
Dizziness
Weakness
Headache
Mental depression
4. Mitotic Inhibitors
- They block cell division at the M phase of the cell cycle.
They are extracted
from plants and tree substances such as periwinkle tree, needles
and bark of the
yew tree and mandrake plant.
A. Vinca Alkaloids Group
Vinblastine Sulfate (Velban)_______________________________
- used for treating breast cancer, testicular, and kidney and
for treatment of
lymphomas, lumphosarcomas, and nueroblastomas. Check CBC before
dosing.
Alopecia (Hair loss) Stomatitis
-
7/31/2019 Anticancer Agents 1
8/20
Antineoplastic Agents and Biologic Response Modifiers
Adverse Effects
Nausea
Vomiting
Partial to Complete Alopecia
Leukopenia
Stomatitis
Neurotoxicity
B. Antimicrotubule / Taxanes Group
Docetaxel (Taxotore)_____________________________________
- used to treat advanced or metastatic breast cancer. It
inhibits mitosis in the
cells. Has a greater antitumor activity with lower toxicity
effect than paclitaxel
(Taxol). Monitor WBC and platelet count; if low, dose may need
to be decreased.
Stages of Cell Mitosis
-
7/31/2019 Anticancer Agents 1
9/20
Antineoplastic Agents and Biologic Response Modifiers
Adverse Effects
Alopecia
Diarrhea
Nausea
Vomiting
Peripheral neuropathy
Stomatitis
Fever
Fluid retention
C. Topoisomerase I inhibitors Group
Irinotecan Hydrochloride (Camptosar)_______________________
- used for advanced and metastatic carcinoma of the colon and
rectum. Inhibits
the topoisomerase enzyme that is needed for DNA and RNA
synthesis.
Increased fluid intake is necessary. Monitor WBC count.
Adverse Effects
Alopecia
Constipation
Nausea and vomiting
Peripheral neuropathy
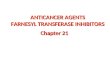
Peripheral Neuropathy Stages. A. Nerve's myelin
sheeth begins to degenerate. B. Separation of the
axon. C. Degeneration of the rest of the nerve
parts.
Peripheral Neuropathy (Foot)
-
7/31/2019 Anticancer Agents 1
10/20
Antineoplastic Agents and Biologic Response Modifiers
D. Topoisomerase II Derivatives Group
Etoposide (VePesid, VP-16)________________________________
- used for treating refractory testicular tumors, small cell
lung carcinoma,Hodgkins and non-Hodgkins lymphomas, and acute
myelogenous leukemia.
Has standard chemotherapy side effects. Has long duration of
action.
Adverse Effects
Alopecia
Anorexia
Nausea and vomiting
5. Hormones (Steroids), Hormone Antagonists, and
Enzymes
The anticancer hormones have 2 major actions:
1. As agonists that inhibit tumor cell growth
e.g. estrogen, progestins, androgens, and
adrenocorticosteroids
2. As antagonists that compete with endogenous hormone
e.g. aminoglutethimide, flutamide, goserelin, acetate, and
tamoxifen
-
7/31/2019 Anticancer Agents 1
11/20
Antineoplastic Agents and Biologic Response Modifiers
A. Hormone (Steroid)
Testolactone (Teslac)_____________________________________- used
for palliative treatment of breast carcinoma in postmenopausal
women.
Serum calcium levels should periodically be checked. Voice may
deepen and
facial hair may occur.
B. Hormonal Antagonist
Aminoglutethimide (Cytadren)_____________________________
- used for treating adrenal carcinoma, ectopic
adrenocorticotropic hormone
(ACTH)-producing tumors. Drug supresses adrenal activity. May be
used in
breast cancer therapy. Treatment usually used for 3 months.
C. Enzyme
L-asparaginase (Elspar)___________________________________- used
for treating acute lymphocytic leukemia. Used in combination with
another
anticancer drug. Common side effects include nausea, vomiting,
anorexia,
leukopenia, and impaired pancreatic function.
-
7/31/2019 Anticancer Agents 1
12/20
Antineoplastic Agents and Biologic Response Modifiers
Biologic Response Modifiers
Biologic Response Modifiers (BRMs)
- class of agents used to enhance the bodys immune system.
Two Advances in Production of BRMs_______________________
A. Recombinant DNA
- genetic engineering process that produces mass quantities of
human proteins
B. Hybridoma Technology
- process that uses mice to mass produce monoclonal
antibodies
Functions of BRM:
1. Enhance immunologic function (immunomodulation)
2. Destroy or interfere with tumor activities
(cytotic/cystostatic effects)
3. Promote differentiation of stem cells
-
7/31/2019 Anticancer Agents 1
13/20
Antineoplastic Agents and Biologic Response Modifiers
Different Biologic Response Modifiers_______________
1. Interferons (IFNs)
- family of naturally occurring proteins
Three Major Types:
1. Alpha IFN-
2. Beta IFN-
3. Gamma IFN-
Interferon-______________________________________
- Produced by B cells, T cells, macrophages, and null cells in
response to the
presence of viruses or tumor cells. It has been known to have
antiviral,
antiproliferative, and immunomodulatory effects which means that
it inhibits
intracellular replication of viral DNA, interferes with tumor
cell growth, and
enhances natural killer cell (antitumor) activity. Recombinant
IFN- is
manufactured as Roferon-A and Intron A.
-
7/31/2019 Anticancer Agents 1
14/20
Antineoplastic Agents and Biologic Response Modifiers
Pharmacokinetics
IFN- is metabolized by the liver and filtered by the kidney. The
body,
however, absorbs approximately 80% of the dose. Peak serum
concentrations
are reached 4-8 hours after administration. IFN- can be ,
administered
subcutaneously (SC), intramuscularly (IM), and intravenously
(IV), although SC
or IM administration is preferred. SC administration is
recommended for clients
with platelet count below 50, 000.
Side Effects
Flulike syndrome (chills, fever, malaise, fatigue and
myalgias)
GI: nausea, vomiting, diarrhea, anorexia, taste alterations,
xerostomia (dry
mouth)
Neurologic reversible side effects: mild confusion, somnolence
(sleepiness),
irritability, poor concentrations, seizures, transient aphasia
(temporary loss of
ability to speak), hallucinations, paranoia and psychoses
Cardiopulmonary: tachycardia, pallor, cyanosis, tachypnea,
nonspecificelectrocardiographic changes, rare myocardial
infarction, and orthostatic
hypotension
Renal and Hepatic: increased blood urea nitrogen (BUN) and
creatinine levels,
proteinuria, and elevated transaminase
Hematologic: neutropenia (decreased number of neutrophils in the
blood),
Thrombocytopenia
Dermatological: maculopapular rashes of the trunk and
extremities, pruritus,
irritation at the injection site, desquamation, and alopecia
-
7/31/2019 Anticancer Agents 1
15/20
Antineoplastic Agents and Biologic Response Modifiers
2. Colony-Stimulating Factors (CSFs)
- Hematopoietic colony-stimulating factors (CSFs) are proteins
that stimulate or
regulate the growth, maturation, and differentiation of bone
marrow stem cells;
manufactured through recombinant DNA techniques.
Uses of CSFs
1. Decrease the length of posttreatment neutropenia (the length
of time the
neutrophils [a type of white blood cell) are decreased secondary
to
therapy)
2. Reduce bone marrow recovery time after bone marrow
transplantation
3. Enhance macrophage or granulocyte tumor-, virus-, and
fungus-
destroying ability
4. Prevent severe thrombocytopenia after myelosuppressive
chemotherapy
Erythropoietin (EPO) (Procrit)______________________________
- A glycoprotein produced by the kidney that stimulates red
blood cell production
in response to hypoxia. It also stimulates the division and
differentiation of
committed red blood cell progenitors (parent cells destined to
become circulating
red blood cells) in the bone marrow.
Pharmacokinetics
EPO can be administered IV (IV push) or SC. According to the
manufacturer, EPO administered by IV is eliminated at a rate
consistent with first-
order kinetics (process by which the drug is eliminated in part
by the hepatic andrenal blood flow). It has a circulating half-life
ranging from approximately 4 to 13
hours in clients with CRF. Plasma levels of EPO have been
detected for at least
24 hours. After SC administration of EPO to CRF clients, peak
serum levels are
achieved with 5 to 24 hours. The half-life of IV-administered
EPO is
-
7/31/2019 Anticancer Agents 1
16/20
Antineoplastic Agents and Biologic Response Modifiers
approximately 20% shorter in normal clients without CRF than in
clients with
CRF. Pharmacokinetic studies have not been done with
HIV-infected clients.
Side Effects
Hypertension
Headache
Arthralgia
Nausea
Edema
Fatigue
Diarrhea
Vomiting
Chest pain
Injection site skin reaction
Asthenia (weakness)
Dizziness
Seizures
Thrombosis
Allergic reactions
Granulocyte Colony-Stimulating Factor (G-CSF)______________
- marketed as filgrastrim (Neupogen), is a human granulocyte
(type of white
blood cell responsible for fighting infection)
colony-stimulating factor produced by
monocytes, fibroblasts, and endothelial cells. It regulates
production of
neutrophils within the bone marrow.
Pharmacokinetics
Filgastrim administration results in a two-phase neutrophil
response. An
early response is seen within 24 hours of administration.
Following the
chemotherapy-induced nadir (low point), a second peak in
circulating neutrophils
is observed. The proliferation-induced increase in neutrophils
usually begins 4 to
5 days after administration is initiated but timing may vary
based on the type and
dose and prior to treatment history. The elimination half-life
of G-CSF in both
normal clients and those with cancer is 3.5 hours. Clearance
rates are
approximately 0.5 to 0.7 ml/min/kg.
-
7/31/2019 Anticancer Agents 1
17/20
Antineoplastic Agents and Biologic Response Modifiers
Side Effects
Nausea
Vomiting
Skeletal pain
Alopecia
Diarrhea
Neutropenia
Fever
Mucositis
Fatigue
Anorexia
Dyspnea
Headache
Cough
Skin rash
Chest pain
Generalized weakness
Sore throat
Stomatitis
Constipation
Pain of unspecified origin
3. Neumega (Oprelvekin )
- is recombinant interleukin- 11, which is a platelet growth
factor. It can potentially
prevent recurrent severe chemotherapy-induced thrombocytopenia.
Oprelvekin
as an active ingredient stimulates megakaryocyte and thrombocyte
production.
Pharmacokinetics
Neumega is available for SC administration in single-use vials
containing
5 mg of oprelvekin as a sterile, lyophilized powder. When
reconstituted with 1 ml
-
7/31/2019 Anticancer Agents 1
18/20
Antineoplastic Agents and Biologic Response Modifiers
of sterile water for injection, the resulting solution has a pH
of 7.0 and a
concentration of 5mg/ml.
Product doing should begin 6 to 24 hours after the completion
of
chemotherapy. SC dosing for 14 days increases the platelet count
in a dose-
dependent way. Platelet counts begin to increase between 5 to 9
days after the
start of Neumega administration. After use of the product is
stopped, platelet
counts continued to increase for up to 7 days and then return to
baseline within
14 days.
The kidney is the primary route of elimination, although most of
the
product is metabolized before excretion. Neumega is
contraindicated with clients
with history of hypersensitivity to the product or any of its
components.
Side Effects
Fluid retention
Cardiovascular events (Arrythmia)
Ophthalmologic effects (Blurry vision) Allergic reactions
(Rash)
4. Interleukins
- are a group of proteins produced by the bodys WBCsthe
lymphocytes.
Because interleukins are monelike glycoproteins manufactured by
the
lymphocytes, they are sometime called lymphokines.
IL-2 is produced commercially through recombinant DNA
technology. It is
marketed as aldesleukin (Proleukin) for use in the treatment of
metastatic renal
cell carcinoma.
Pharmacokinetics
-
7/31/2019 Anticancer Agents 1
19/20
Antineoplastic Agents and Biologic Response Modifiers
IL-2, administered either by IV infusion or SC injection, and is
rapidly
distributed to the extravascular, extracellular space and
eliminated from the body
by metabolism in the kidney. The serum half-life of IL-2 is
short. Because of this
rapid clearance, IL-2 is administered in frequent, short
infusions.
Side Effects
Hypotension
Nausea
Vomiting
Diarrhea
Mental status changes
Oliguria/anuria
Anemia
Thrombocytopenia
Fever
Chills
Sinus tachycardia
Pulmonary congestion
Dyspnea
Pain at injection site
Fatigue
Weakness
Malaise
Elevated liver function test
5. Monoclonal Antibody
Transtuzumab (Herceptin)_________________________________
- is a recombinant humanized monoclonal antibody approved by the
FDA for solo
treatment of metastatic breast cancer in clients whose condition
is refractory to
chemotherapy or in combination with paclitaxel (Taxol) for
first-line treatment of
metastatic breast cancer.
Pharmacokinetics
-
7/31/2019 Anticancer Agents 1
20/20
Antineoplastic Agents and Biologic Response Modifiers
The metabolism and elimination of transtuzumab is unknown.
Following IV
infusion, the half-life is dose dependent; the half-life is
about 6 days with a
weekly maintenance dose of 2mg/kg. The initial dose is 4mg/kg IV
over 1.5 hours
followed by weekly maintenance doses of 2 mg/kg over half an
hour. The
estimated cost for 23 weeks of treatment for a 120-pound woman
is about $14,
000.
Side Effects
Fever
Chills
Nausea
Vomiting
Headache
Asthenia
Pain
Reference:
Kee, J.L., & Hayes, E. R. (2003). Pharmacology: A nursing
process approach
(4th ed.). W. B. Saunders Co.
A diagram showing a monoclonal antibody attached into a
cell.