Embed Size (px)
Citation preview

Antibiotic Stewardship Where Are You?
Suzanne F. Bradley, M.D.
Professor of Internal Medicine
Division of Infectious Disease
University of Michigan Medical School
VA Ann Arbor Healthcare System
Hospital Epidemiologist, Infection Control


Antimicrobial UseUS - 2010
Fridkin S et al. MMWR 2014;63:195.


How to Combat Resistance?

Antibiotic Stewardship ProgramsCore Elements
• Leadership
Commitment
• Accountability
• Drug expertise
• Action to improve use
• Tracking
• Reporting
• Education
http://www.cdc.gov/getsmart/healthcare/evidence.html

7 Core Elements
Stewardship
Leadership
•human
• financial
• IT Resources
Accountability
•outcomes
• report committee
Drug Expertise
•pharmacist leader
Tracking
•process measures
Action
• Implement one
Reporting
• regularly to staff
Education
•optimal prescribing
Pollack et al.
CID 2014;59:S98

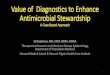
Improving Antimicrobial UseInvolves Everyone!
Reduction Antibiotic
Use
Hospitals
Patients and
Families
Post-Acute Care
Outpatient Facilities


Patient Education

Patient Education

AE, AP, AS, GU, VI data are not shown due to 7 or fewer hospital respondents but are included in the overall percentage.
*Prescribing data from 2014; population data from 2013
Source: IMS Health
7 - 33%
46 - 54%
55 - 77%
34 - 45%
48%
37%
54%
30%
33%
77%
48%
70%
63% 40%
49%
12%
33%
31%
28%
35%
41%
24%
26%
36%
43%
33%
47%
48%
24%
45%
54%51%
54%
41%
47%
47%
45% 48%
64%
56%
67%
60%
24%
59%
51%7%
27%59%67%47%58%38%60%50%
60%
40%
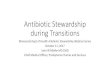
Percent of Hospitals with Antibiotic Stewardship Programs by State, 2015*
*A hospital stewardship program is defined as a program following all 7
of CDC’s Core Elements of Hospital Antibiotic Stewardship Programs.
Source: CDC’s National Healthcare Safety Network (NHSN) Survey
Nationally, 48.1% of all hospitals have stewardship programs (2,199 of 4,549); the national goal is 100% of hospitals by 2020.


VA StewardshipImpact
Kelly AA et al. ICHE 2017;38:513.
ASP program 41-89%
ASP policy 17-92%
ATB use drops 12%

Quality MeasuresHow to Define Success
• Structure to deliver high quality care?–personnel?
– resources?
–policies?
• Process for healthcare delivery?– what is the process?
– is it being done?
• Outcomes of healthcare delivery
Dodds Ashley ES et al. SHEA ASP Textbook 2018 pp 131

Antimicrobial StewardshipMeasures
• Structural– leadership commitment
–multidisciplinary protocols
–designated ASP leader
–expert pharmacist
– tracking resistance
– tracking antimicrobial use
–education staff, patients, & families
Dodds Ashley ES et al. SHEA ASP Textbook 2018 pp 131

Antimicrobial StewardshipProcess Measures
Pt Management Stewardship Program ATB Consumption
Adherence guidelines Antibiotic courses reviewed Days of therapy-DOT
Duration antibiotic therapy Electronic alerts reviewed Defined daily doses-DDD
De-escalation events Recommendations made Length of therapy
IV to PO conversion Types of interventions Doses dispensed
Dual anaerobe therapy Approval restricted ATB Antimicrobial starts
Time to appropriate therapy Excess drug use
Diagnostic utilization Device days
Orders include indication ICU days
Orders include duration
ATB free days
ID consult performed

Antimicrobial StewardshipOutcome Measures
Clinical Financial
Mortality overall & infection-
related
Drug costs
LOS overall & after ATB Hospitalization costs
Re-admission rates Overall therapy cost
ATB adverse events Cost per pt per day
ATB resistance rates Attributable infection costs
Cure & clinical or micro
response
QUALYs
Clinical failures
HAI rates

Antimicrobial StewardshipHorizontal vs Vertical Action Items
Horizontal
Formulary Restriction
Antibiotic Time Out
Alerts for Duplicative Therapy
(Ex: Double Anaerobic Coverage)
Vertical
Targeting Specific Antimicrobials
(Ex: Anti-MRSA agents)
Cellulitis Order Set
UTI Stewardship
Patel PK. ICHE 2017;38:532.

Antimicrobial StewardshipHorizontal vs Vertical

Vertical Action ItemsSyndrome-Culture Strategies
Strategy Description Benefits Challenges
Susceptibility
Reports
(low effort or $)
Select or censor
ATB to include on
culture reports
Improve ATB use Providers assume
susceptible even if
agents not
reported
Clincal Pathways &
Order Sets
( mod effort or $$)
ATB & Dx guidance Guideline Tool
Kit
Standardized care
Design & maintain
Need IT
Uptake limited
Rapid diagnostics
(mod effort or $$)
Rapid ID or
susceptibility info
Improve time to
appropriate Rx &
rapid de-escalation
May not change
ATB use alone
Add audit &
feedback
Audit & Feedback
(high effort or $$$)
Direct to providers Improve ATB
selection &
outcomes, ATB de-
escalation
Need system to ID
patients for review
Need IT resources
Adapted from Moehring RW et al. SHEA ASP Textbook 2018, pp:63-84

Horizontal Action ItemsBroad-Based Strategies
Strategy Description Benefits Challenges
Guidelines
(low effort or $)
Tailored national
recommendations,
local resistance
patterns, formulary
Standardized care
Improved selection
& outcomes
Maintain updates
Assess adherence
Education
(mod effort or $$)
Group format,
policies
Reach many
providers
Change not
sustained
Preauthorization
(high effort or $$$)
Review & approval
Restricted ATB
Improve use &
outcomes, Reduce
use & costs, Some
education
Time intensive
Skilled personnel
Loss autonomy
Use other ATB
Audit & Feedback
(high effort or $$$)
After Rx started
Feedback given
Improve use &
outcomes, Reduce
use & costs, Direct
education
Time intensive
Skilled personnel
Need IT to identify
Adherence
voluntary
Adapted from Moehring RW et al. SHEA ASP Textbook 2018, pp:63-84

Horizontal Action ItemsBroad-Based (2)
Strategy Description Benefits Challenges
Allergy initiatives
(low effort or $)
Improve allergy
assessments
Increase use first-
line drugs
Education
providers, nurses,
pharmacy, patients
Dose optimization
(mod effort or $$)
Pt & drug specific
factors
Better dosing
Improves safety
Improve drug
levels
Pharmacy
workload
Ongoing
assessments
IV to PO
Conversion
(mod effort or $$)
Automatic
conversion high
bioavailability ATB
Decrease costs
No change safety
Decrease LOS
Pharmacy
workload
Frequent review
Automatic ID
Consult
(high effort or $$$)
Eligible pts per
policy
Improve survival
Reduce
complications &
readmissions
Need ID docs
Acceptance by
non-ID docs
Adapted from Moehring RW et al. SHEA ASP Textbook 2018, pp:63-84

Horizontal Action ItemsBroad-Based (3)
Strategy Description Benefits Challenges
Antibiotic Time
Outs
(low effort or $)
Providers review &
document choice,
dose, duration,
cultures, &
indication
Increase
awareness
Use in limited
resource areas
Integrate in EMR
No data on impact
Providers may not
change decisions
Alert fatigue
Automatic Stop
Orders
(low effort or $)
Require approval
for continuation
Improve use
Decrease
resistance
ATB stopped
inappropriately
Maintain process
Peer Comparison
Feedback
(high effort or $)
Feedback data vs
other prescribers
Positive
reinforcement
good prescribers
Target education
Collect & analyze
data, Adequate
sample size, what
is appropriate
use?
High Risk Unit ASP
Routine Rounds
(high effort or $)
Target high priority
areas,
Multidisciplinary
team
Direct education
In depth pt review
Time & labor
intensive
Engaging provider
groupsAdapted from Moehring RW et al. SHEA ASP Textbook 2018, pp:63-84

Antimicrobial StewardshipSetting Priorities - Leadership
Basic Intermediate Advanced
Board Statement importance of ASP
Make top management -ASP Champion
Ensure training for ASP leaders
CEO/CMO Newsletter Facility strategic goals –include ASP
IT funding & support for ASP
Dedicate salary - ASP leaders
QI & Safety - include ASPreporting to leadership
Micro & lab data access by ASP
Specify ASP time & goals Provider education - includeASP
All departments responsible for improving antimicrobial use
Funding ASP consultants if none locally
Financial incentives for departments that improve antimicrobial use
Articulate that ATB use important hospital goal
Ensure other departments support ASP
Share stories, speakers & resources - ASPs improve outcomes
Hold providers accountable for antibiotic use
Engage pts & advocates
National Quality Partners Playbook: AS in Acute Care.

Antimicrobial StewardshipSetting Priorities -Accountability
Basic Intermediate Advanced
Appoint ASP Leader –physician +/- pharmacist
Ensure ASP training & certification
Tie measures to performance/financial incentives
NP as an alternative ASP leader accountable specific outcome measures
IT funding & support for ASP
Dedicate salary - ASP leaders
Document outcome measure in performance evaluations
Tie hospital QI, e.g., SAAR and C. diff rates, to ASP performance
Collaboration between physicians & pharmacy
ASP leader involves other disciplines in stewardshipefforts
ASP leader involved in all QI projects related to ATB
National Quality Partners Playbook: AS in Acute Care.

Antimicrobial StewardshipSetting Priorities – Drug Expertise
Basic Intermediate Advanced
Ensure pharmacist with ASP expertise
Provide pharmacist ASPtraining & certification
Ensure pharmacy leader trains other pharmacists in ASP throughout the hospital
National Quality Partners Playbook: AS in Acute Care.

Antimicrobial StewardshipSetting Priorities - Actions
Basic Intermediate Advanced
Antibiotic order review by ASP leader based on local need
ATB time out or post-prescription review 48-72 hrs by primary team or ASP
Rapid diagnostics for organisms or biomarkers to improve ATB use
Require indication, dose, duration for all orders
Guidance for automatic change IV to PO
Timely culture and transport
Provide guidance - antibiotic allergy assessment
Guidance for ATB adjustments if organ dysfunction
Improve ATB use for specific syndromes, e.g., CAP, VAP, SSI, BSI, sepsis
Develop treatment recommendations based on national guidelines & local susceptibility data
Dose optimization for Rx resistant organisms.
Improve ATB use for specific organisms, e.g., MRSA, CDI
Standardize order forms for clinical syndromes
Automatic alerts for duplicative drug therapy
Inappropriate use for contaminants, colonization
Automatic stop orders for specific antibiotics
Treatment protocols for sepsis in ICU
Pt rounds include discussions of ATB
National Quality Partners Playbook: AS in Acute Care.

Antimicrobial StewardshipSetting Priorities – Tracking/Monitoring
Basic Intermediate Advanced
Adhere documentation
policies - ATB indications &
time outs
Tracking antibiotic
resistance patterns
Track DOT-Days of Therapy
Track diagnosis, drug, dose,
duration, de-escalation
Tracking CDI rates Track DDD-defined daily
dose (grams ATB used)
Adherence facility treatment
guidelines
Readmission rates
pneumonia & CDI at 30
days
Track SAAR-standardized
antibiotic administration ratio
Adherence interventions Direct antibiotic expenditures
– purchasing costs
Accurate allergy & adverse
event reporting
National Quality Partners Playbook: AS in Acute Care.

Antimicrobial StewardshipSetting Priorities - Reporting
Basic Intermediate Advanced
Regular reports on measures tracked.
Progress reports for meeting facility goals & suggestions for improvement
Provide provider-specific data & suggestions for improvement
Submit report to stakeholders, e.g., Board, QI, Safety. P&T, Staff
Include overall use, trends, interventions, actions taken, appropriate use, & outcome measures
Provide real-time ASPmetrics for all staff by dashboard
Present to Medical Staff quarterly
Make concreterecommendations for improvement
Post data on medical staff websites & by email
Encourage early adoption NHSN modules - SAAR
Reports to leadership, staff, & PTs
Post susceptiibility & use data in news letters
Provide unit specific reports Present ASP to governing bodies
Provide to specific groups Post unit specific data invisible areas
Report to leadership with actionable items
National Quality Partners Playbook: AS in Acute Care.

Antimicrobial StewardshipSetting Priorities -Education
Basic Intermediate Advanced
Communicate ASP at least quarterly – blogs, website, intranet, newsletters
Give ASP data in grand rounds
Participate in national ASP activities
Highlight ASP goals in education programs & materials
Talk annually to key providers in person or using web-based programs
Annual staff education should include ASP information
Tell stories – physicians who change prescribing habits
Develop concise messages for ASP with clear recommendations for improvement
Patient education should include ATB information
Tell stories – pt adverse events
Educate providers on resistance data and susceptibility interpretation
Medical education & training should include ASP information
Establish an expert collaborative for coaching goals & webinars
New staff orientation should include ASP information
National Quality Partners Playbook: AS in Acute Care.

High Antimicrobial Use?How to Respond
CDC/NHSN & Pew Charitable Trust

Antimicrobial StewardshipUS Viewpoint
• Prevention of ATB resistance is important
• Reduction of antibiotic use critical
• Requires everyone to help
• Start simply!
• Multiple goals, actions, & measures
• Everyone can do something!