1. CDC; Antibiotic resistance threats in the United States,
2013 ANTIBIOTIC STEWARDSHIP 2
2. National Center for Emerging and Zoonotic Infectious
Diseases Division of Healthcare Quality Promotion Used with
permission from: Centers for Disease Control and Prevention; CDC
24/7: Savings Lives, Protecting People TM
3. Mission- Get Smart for Healthcare To optimize the use of
antimicrobial agents in in- patient healthcare settings.
4. Antibiotics are misused in hospitals It has been recognized
for several decades that up to 50% of antimicrobial use is
inappropriate. IDSA/SHEA Guidelines for Antimicrobial Stewardship
Programs
http://www.journals.uchicago.edu/doi/pdf/10.1086/510393
5. Why we need to improve in-patient antibiotic use Antibiotics
are misused in hospitals Antibiotic misuse adversely impacts
patients and society Improving antibiotic use improves patient
outcomes and saves money Improving antibiotic use is a public
health imperative
6. Antibiotics are misuse in a variety of ways Given when they
are not needed Continued when they are no longer necessary Given at
the wrong dose Broad spectrum agents are used to treat very
susceptible bacteria The wrong antibiotic is given to treat an
infection
7. Antibiotic misuse adversely impacts patients- C. difficile
Antibiotic exposure is the single most important risk factor for
the development of Clostridium difficile associated disease
(CDAD).1 Up to 85% of patients with CDAD have antibiotic exposure
in the 28 days before infection.1 1. Chang HT et al. Infect Control
Hosp Epidemiol 2007; 28:926931.
8. Antibiotic exposure increases the risks of resistance
Pathogen and Antibiotic Exposure Increased Risk Carbapenem
Resistant Enterobactericeae and Carbapenems 15 fold 1 ESBL
producing organisms and Cephalosoprins 6- 29 fold 3,4 Patel G et
al. Infect Control Hosp Epidemiol 2008;29:1099-1106 Zaoutis TE et
al. Pediatrics 2005;114:942-9 Talon D et al. Clin Microbiol Infect
2000;6:376-84
9. Antibiotic misuse adversely impacts patients- resistance
Increasing use of antibiotics increases the prevalence of resistant
bacteria in hospitals. Antibiotic resistance increases mortality.
Getting an antibiotic increases a patients chance of becoming
colonized or infected with a resistant organism.
10. Antibiotic misuse adversely impacts patients - adverse
events In 2008, there were 142,000 visits to emergency departments
for adverse events attributed to antibiotics.1 National estimates
for in-patient adverse events are not available, but there are many
reports of serious adverse events (aside from C. difficile
infection) from in-patient antibiotic use. 1 Shehab N et al.
Clinical Infectious Diseases 2008; 15:735-43
11. Clinical outcomes better with antimicrobial management
program 0 20 40 60 80 100 Appropriate Cure Failure AMP UP RR 2.8
(2.1-3.8) RR 1.7 (1.3-2.1) RR 0.2 (0.1-0.4) Percent AMP =
Antibiotic Management Program UP = Usual Practice Fishman N. Am J
Med. 2006;119:S53.
12. Improving antibiotic use saves money Comprehensive programs
have consistently demonstrated a decrease in antimicrobial use with
annual savings of $200,000 - $900,000 IDSA/SHEA Guidelines for
Antimicrobial Stewardship Programs
http://www.journals.uchicago.edu/doi/pdf/10.1086/510393
13. Improving antibiotic use is a public health imperative
Antibiotics are the only drug where use in one patient can impact
the effectiveness in another. If everyone does not use antibiotics
well, we will all suffer the consequences. Antibiotics are a shared
resource, (and becoming a scarce resource). Using antibiotics
properly is analogous to developing and maintaining good
roads.
14. Goals- Get Smart for Healthcare Improve patient safety
through better treatment of infections. Reduce the emergence of
anti-microbial resistant pathogens and Clostridium difficile.
Heighten awareness of the challenges posed by antimicrobial
resistance in healthcare and encourage better use of antimicrobials
as one solution.
15. Development of the National Action Plan 16
16. Development of the National Action Plan The National Action
Plan was developed in response to Executive Order 13676: Combating
Antibiotic - Resistant Bacteria which was issued by President
Barack Obama on September 18, 2014 in conjunction with the National
Strategy for Combating Antibiotic- Resistant Bacteria. 17
17. The goals of the National Action Plan Significant Outcomes
of Goal 1 Reduction of inappropriate antibiotic use by 50% in
outpatient settings and by 20% in inpatient settings. 18
18. The goals of the National Action Plan 1. Slow the emergence
of resistant bacteria and prevent the spread of resistant
infections. 2. Strengthen national One-Health Surveillance efforts
to combat resistance. 19
19. The goals of the National Action Plan 3. Advance
development and use of rapid and innovative diagnostic tests for
identification and characterization of resistant bacteria. 20
20. The goals of the National Action Plan 4. Accelerate basic
and applied research and development for new antibiotics, other
therapeutics and vaccines. 5. Improve international collaboration
and capacities for antibiotic-resistance prevention, surveillance,
control, and antibiotic research and development. 21
21. The goals of the National Action Plan Sub-Objective 1.1.1B:
Get Smart: Know When Antibiotics Work. Many antibiotics prescribed
in doctors offices, clinics, and other outpatient settings are not
needed. This program focuses on appropriate antibiotic prescribing
and use for common illnesses in children and adults. 22
22. The goals of the National Action Plan Sub-Objective 1.1.1B:
Get Smart for Healthcare. Many patients in hospitals, nursing
homes, and other healthcare facilities receive antibiotics to fight
infections, but these drugs are often prescribed incorrectly.
23
23. The goals of the National Action Plan Sub-Objective 1.1.1B:
Get Smart for Healthcare. This program helps clinicians prescribe
the right drugs for the right patients at the right doses and
times. 24
24. Antibiotic Stewardship Antibiotics 25
25. Antibiotics Myth 1. They can cure colds and the flu. Not
so. Antibiotics work against only bacterial infections, not viral
ones such as colds, the flu, most sore throats, and many sinus and
ear infections. 26 STOP SUPERBUGS NOW; Myths about antibiotics; No,
they won't help with the cold or flu, and other common
misconceptions. Teresa Carr; Consumer Reports; Published: June 25,
2015
26. Antibiotics Myth 2. They have few side effects. Almost 1 in
5 emergency-room visits for drug side effects stems from
antibiotics. In children, the drugs are the leading cause of such
visits. 27 STOP SUPERBUGS NOW; Myths about antibiotics; No, they
won't help with the cold or flu, and other common misconceptions.
Teresa Carr; Consumer Reports; Published: June 25, 2015
27. Antibiotics Those side effects include diarrhea, yeast
infections, and in rare cases, nerve damage, torn tendons. Allergic
reactions that include rashes, swelling of the face or throat, and
breathing problems. 28 STOP SUPERBUGS NOW; Myths about antibiotics;
No, they won't help with the cold or flu, and other common
misconceptions. Teresa Carr; Consumer Reports; Published: June 25,
2015
28. Antibiotics The drugs can kill off good bacteria,
increasing the risk of some infections, including C. difficile. At
least 250,000 people a year now develop C. diff. infections linked
to antibiotic use, and 14,000 die as a result. 4 29 STOP SUPERBUGS
NOW; Myths about antibiotics; No, they won't help with the cold or
flu, and other common misconceptions. Teresa Carr; Consumer
Reports; Published: June 25, 2015
29. Antibiotics Myth 3. A full course lasts at least a week.
Not always. A shorter course can work for some infections, such as
certain urinary tract, ear, and sinus infections. So ask your
doctor for the shortest course and lowest dose of antibiotics
necessary to treat your infection. 30 STOP SUPERBUGS NOW; Myths
about antibiotics; No, they won't help with the cold or flu, and
other common misconceptions. Teresa Carr; Consumer Reports;
Published: June 25, 2015
30. Antibiotics Myth 4. Its OK to take leftover medication.
Nope. First, you may not need an antibiotic at all. And if you do,
the leftovers may not be the right type or dose for your infection.
31 STOP SUPERBUGS NOW; Myths about antibiotics; No, they won't help
with the cold or flu, and other common misconceptions. Teresa Carr;
Consumer Reports; Published: June 25, 2015
31. Antibiotics Taking them could allow the growth of harmful
and resistant bacteria. Return unused antibiotics to the pharmacy
or mix them with coffee grounds or cat litter and toss in the
trash. 32 STOP SUPERBUGS NOW; Myths about antibiotics; No, they
won't help with the cold or flu, and other common misconceptions.
Teresa Carr; Consumer Reports; Published: June 25, 2015
32. Antibiotics Myth 5. All bacterial infections require drugs.
Mild ones sometimes clear up on their own. So ask your doctor
whether you could try waiting it out. 33 STOP SUPERBUGS NOW; Myths
about antibiotics; No, they won't help with the cold or flu, and
other common misconceptions. Teresa Carr; Consumer Reports;
Published: June 25, 2015
33. Antibiotics Myth 6. The more bacteria a drug kills, the
better. Wrong. So-called broad-spectrum drugs, such as ceftriaxone,
cipro- floxacin and levofloxacin, should be reserved for
hard-to-treat infections. 34 STOP SUPERBUGS NOW; Myths about
antibiotics; No, they won't help with the cold or flu, and other
common misconceptions. Teresa Carr; Consumer Reports; Published:
June 25, 2015
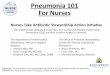
34. Pathogen Cases Streptococcus pneumoniae 20-60% Haemophilus
influenza 3-10% Staphylococcus aureus 3-5% Gram-negative bacilli
3-10% Legionella species 2-8% Mycoplasma pneumoniae 1-6% Chlamydia
pneumoniae 4-6% Viruses 2-15% Aspiration 6-10% Others 3-5% Adapted
from Mandell LA, Bartlett JG, Dowell SF, et al: Update of practice
guidelines for the management of community-acquired pneumonia in
immunocompetent adults. Clin Infect Dis 2003;37:1405-1433. Many
pathogens: Which to treat? 35
35. Methods Used Today 36
36. Medical history Physical exam Chest x-rays Blood tests
Blood culture Sputum collection CT chest computed tomography
Current methods to determine if patients have pneumonia 37 Current
methods to determine if patients have pneumonia
37. Thoracentesis Pleural fluid culture Pulse oximetry Nasal
swab Throat swab Urine antigen Bronchoscopy - BAL Current methods
to determine if patients have pneumonia 38 Current methods to
determine if patients have pneumonia
38. Specimens are very often contaminated from the upper
respiratory resulting in many false positives. This leads to broad
antibiotic treatment because the actual pathogen causing the
pneumonia is usually never identified. 39 Current sampling data is
not reliable or accurate
39. Chest x-rays can reveal areas of opacity (seen as white)
which represent consolidation. Pneumonia is not always seen on x-
rays, either because the disease is only in its initial stages, or
because it involves a part of the lung not easily seen by x-ray.
X-rays cannot identify pathogens. Routine chest x-rays 40
40. PneumoniaChecktm 41
41. Glossary Disruptive technology: Introducing new technology
to current technology which will change the way things are done.
42
42. The Need 43
43. The Need Pneumonia is a leading cause of death in children
worldwide. Over 2 million children die from pneumonia each year and
one child dies every 20 seconds. The problem with current diagnosis
methods is one of sampling. Mouth and nose samples have
contaminating bacteria, which result in many false positives.
44
44. The Need Additionally, the samples are unable to identify
the pathogen; hospital stays are lengthened increasing the chances
that cases will become complicated. Since the pathogen cannot be
identified, patients receive broad- spectrum antibiotics, which are
often unnecessary and can cause antibiotic resistance. 45
45. The Need Other methods, such as a chest x-ray, can identify
fluid in the lungs, but cannot identify the specific pathogen
causing the pneumonia. 46
46. The Need Antibiotic resistance is one of the world's most
pressing public health threats. Antibiotics are the most important
tool we have to combat life- threatening bacterial disease, but
using antibiotics can also result in side effects. 47
47. The Need Antibiotic use leads to new drug- resistant germs
and increased risks to patients. Patients, healthcare providers,
hospital administrators and policy makers must work together to
employ safe and effective strategies for improving antibiotic use
ultimately saving lives. 48
48. The Need Antimicrobial resistance is one of our most
serious health threats. Infections from resistant bacteria are now
too common, and some pathogens have even become resistant to
multiple types or classes of antibiotics. Dr. Tom Frieden, MD, MPH
Director, U.S. Centers for Disease Control and Prevention Meeting
the Challenges of Drug-Resistant Diseases in Developing Countries
Committee on Foreign Affairs Subcommittee on Africa, Global Health,
Human Rights, and International Organizations United States House
of Representatives April 23, 2013 49
49. The Solution 50
50. Pneumonia kills more children than any other disease.
Unfortunately, the pathogen cannot be identified in most patients.
Thepathogens causing pneumonia are difficult to identify because a
high quality specimen from the lower lung is difficult to obtain
due to contamination of the sample. Development of PneumoniaCheck
51
51. PneumoniaCheck was developed and designed to collect
aerosolspecimens selectively from the lower lung generated during
deep cough. This technology allows PneumoniaCheck to effectively
separate the upper respiratory tract from the aerosols in the lung
by >90%. Development of PneumoniaCheck 52
52. PneumoniaCheck utilizes a separation reservoir and
specially designed mouthpiece to segregate contents from the upper
airway and the lower lungs. Development of PneumoniaCheck 53
53. PneumoniaCheck includes several specially designed features
to exclude oral contaminants from the sample and a filter to
collect theaerosolized pathogens from the lower lungs. The filter
can collect >99.97% of virus and bacteria sized particles from
the sampled lower lung aerosols. Development of PneumoniaCheck
54
54. PC saves time and money diagnosing pneumonia; however, it
is NOT a diagnostic device. Development of PneumoniaCheck 55
55. PneumoniaCheck - The Device 56
56. The Device PneumoniaCheck uses fluid mechanics to separate
the upper airway particles from the lower airway particles. The
separation means that only a lung specimen is captured on the
filter media at the end of the device. 57
57. The Device This filter can then be analyzed using
traditional microbiology methods or more sensitive molecular DNA
analysis to identify the specific pathogen causing pneumonia, or
other lower respiratory infections. 58
58. The Device The ability to identify the specific pathogen
will allow for more targeted antibiotic treatment or none at all if
viral, which should reduce antibiotic resistance and other
complications. 59
59. The Device PneumoniaCheck is an easy-to-use, noninvasive,
disposable solution for collecting respiratory specimens to help
reduce one of the worlds largest health problems. PneumoniaCheck
may be used on patients three feet and taller. 60
60. 61
61. To use PneumoniaCheck, a patient simply coughs deeply into
the mouthpiece and expels the remaining air in his or her lungs.
This action can be repeated as many times as necessary to collect a
sufficient sample of lower respiratory aerosolized pathogens.
Recommend collecting 10 coughs 62
62. The air from the upper respiratory is collected in a
reservoir, and aerosols from the lower respiratory are captured on
a microbial filter. The filter can then be sent to a laboratory to
be tested for the presence of various pathogens. 63
63. PneumoniaCheck uses fluid mechanics to isolate lung
pathogens onto the filter. Fluid mechanics is the branch of physics
that studies fluids (liquids, gases, and plasmas) and the forces on
them. 64
64. 65
65. 66
66. 67
67. The air from the upper respiratory is collected in a
reservoir, and aerosols from the lower respiratory are captured on
a microbial filter. PneumoniaCheck is then sent to a laboratory to
be tested for the presence of various pathogens. 68
68. The link from diagnosis to treatment 69
69. 70
70. Questions? ARC Medical Inc. PneumoniaCheck arcmedical.com
71